Dr James Rosengarten reports highlights from the European Heart Rhythm Association (EHRA) Europace 2013 meeting held recently in Athens, Greece.
With the number of patients with atrial fibrillation (AF) set to double by 2050, appropriate anticoagulation for this growing condition was highlighted in a special session at the meeting – a ‘State of The Art Lecture’. Professor Stefan H Hohnloser (JW Goethe University, Frankfurt, Germany) described how stroke in Europe costs an estimated €38 billion per year, with 20% attributable to AF. Yet a decade ago, around 40% of AF patients did not receive appropriate anticoagulation. Of those receiving therapy, only around 50% of time in therapeutic range (TTR) is seen. With this in mind, novel oral anticoagulants (NOACs) are non-inferior to warfarin at reducing stroke risk, but also remove many of the therapeutic difficulties seen with oral anticoagulant therapy. The benefits of NOACs are seen even in those with previous stroke or impaired renal function.
Many of the difficulties with vitamin K antagonists (VKAs), such as warfarin, were seen in the past as good reason to avoid anticoagulation in all but the highest risk patients. Professor Gregory Y H Lip (University of Birmingham Centre for Cardiovascular Sciences, City Hospital, Birmingham) believes we need to change the culture of under-prescribing thromboprophylaxis in AF. The focus has been on identifying those highest risk patients in whom benefits were believed to outweigh risks. However, a culture change is needed. NOACs now represent a more convenient and, in many respects, a safer option to VKA for stroke prophylaxis. The 2012 focussed update of the European Society of Cardiology (ESC) guidelines for the management of atrial fibrillation1 recommend all but the lowest risk patients are indicated for oral anticoagulation. Attention should now be focussed on identifying these truly low risk individuals, scoring 0 or 1 on the CHA2DS2-VASc score.
Professor Lip also considered bleeding risk: the HAS-BLED score is a now well-validated score to identify those at risk of bleeding with oral anticoagulation. A score >3 is indicative of regular review and follow up, but should not be used as a reason for avoiding anticoagulation. In fact, patients with a high HAS-BLED score derive a higher net clinical benefit when balancing ischaemic stroke and intracranial bleeding.
Once you have identified your patient is at risk of stroke, which anticoagulant should you choose? The ESC guidelines recommend either a VKA with a high TTR, or a NOAC. A new scoring system – SAMe-TT2R2 (Sex female, Age less than 60, Medical history, Treatment strategy [rhythm control], Tobacco use [doubled] and race [doubled]) – can predict those who will do well with a VKA (a score of 0-1) or those who are likely to have poor anticoagulation control with a VKA (a score ≥2) and where a NOAC could be a better option.2
It is acknowledged that licensed indications and experience develops more quickly than guidelines can be updated. For this reason EHRA has published a Practical Guide on the use of NOACs in patients with non-valvular AF.3 This addresses many of the practical concerns relating to these novel agents, including initiation and follow up, drug interactions, dosing issues, bleeding and administration in patients requiring urgent surgery, or suffering with acute coronary events, or stroke.
James Rosengarten
Wessex Electrophysiology Fellow and BJCA Deanery Representative
([email protected])
Camm AJ, Lip GY, De Caterina R et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation–developed with the special contribution of the European Heart Rhythm Association. Europace 2012;14:1385-413. http://dx.doi.org/10.1093/europace/eus305
Apostolakis S, Sullivan RM, Olshansky B, Lip GY. Factors affecting quality of anticoagulation control amongst atrial fibrillation patients on warfarin: the SAMe-TT2R2 (Sex female, Age less than 60, Medical history, Treatment strategy [rhythm control], Tobacco use [doubled], Race [doubled]) score. Chest 2013; http://dx.doi.org/10.1378/chest.13-0054
Heidbuchel H, Verhamme P, Alings M et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace 2013;15:625-51. http://dx.doi.org/10.1093/europace/eut083
Dr James Rosengarten reports highlights from the European Heart Rhythm Association (EHRA) Europace 2013 meeting held recently in Athens, Greece.
Data on the trends in management of patients with AF in five European countries were presented in a Late Breaking Clinical Trials session at the meeting. PREFER AF (Prevention of Thromboembolic Events –European Registry in Atrial Fibrillation) found that oral anticoagulation is now used in over 85% of patients with AF eligible for therapy.
PREFER AF provides a ‘snapshot’ of clinical practice across five European countries taken in 2012. It revealed that NOACs are now used by 6.1% of AF patients and that use of rhythm control interventions and catheter ablations have increased.
“PREFER AF illustrates changes in management of patients with AF since the last ESC guidelines. The registry shows that oral anticoagulant therapy is now much more widely used than in the German Competence Network on Atrial Fibrillation (AFNET) and the Euro Heart Survey registries on AF and suggests that European clinicians are using guidelines well. The rapid uptake of new oral anticoagulants suggests that these drugs are filling a therapeutic gap,” said Professor Paulus Kirchhof (School of Clinical and Experimental Medicine, University of Birmingham).
The investigators believe the study represents the largest European registry on AF to date. The ESC guidelines for the management of AF, published in 2010, incorporated several ‘evolutionary’ changes in the management of AF. These included the concept of active AF screening to initiate therapy before complications had occurred and, furthermore, emphasised that continuous oral anticoagulation was indicated for the majority of AF patients since almost all are at increased risk of stroke.
Between January 2012 and January 2013, the PREFER AF registry enrolled consecutive patients with AF from 461 centres in France, Germany, Italy, Spain and UK. Altogether 42% of patients were office based and 53% hospital based, with 89% treated by cardiologists. “Since practice patterns can be influenced by the type of physicians, we felt it was important to recruit patients from a number of different settings,” said Professor A Kirchhof.
Results showed that of the 7,243 evaluable patients enrolled, 30% had paroxysmal AF, 24% persistent AF, 7.2% long-standing persistent AF, and 38.8% had permanent AF.
When medications were examined it was found that 66.3% of patients (4,799) received a VKA as monotherapy; 9.9% of patients (720) received VKA and an antiplatelet agent in combination; and 6.1% received NOACs (dabigatran, rivaroxaban or apixaban). Furthermore, antiplatelet agents alone were given to 11.2% of patients (808) while 6.5% of patients (474) received no antithrombotic therapy at all. Altogether, 78.6% of patients were adequately rate controlled, using a mean heart rate of 60 to 100 bpm as the definition.
Rhythm control therapy was deployed in 66.7% of patients, consisting of DC cardioversion in 18.1% of patients; pharmacological conversion in 19.5%; amiodarone in 24.1%; flecainide in 10.5%; sotalol in 5.5%; dronedarone in 4.0%; other antiarrhythmic drugs in 3.1%; and catheter ablation in 5.0%.
Over 80% of patients still suffered from AF symptoms despite good rate control.
“We were surprised and puzzled by the high number of patients who suffer from AF despite good rate control,” said Professor Kirchhof. “This indicates that we have more work to do to develop tools to better prevent AF and possibly to better maintain sinus rhythm in the future.” The ongoing EAST (Early Treatment of Atrial Fibrillation for Stroke Prevention Trial) study (www.easttrial.org) is currently testing whether early use of rhythm control therapy can prevent adverse cardiovascular outcomes in patients with AF compared to usual care.
James Rosengarten
Wessex Electrophysiology Fellow and BJCA Deanery Representative
([email protected])
Dr James Rosengarten reports highlights from the European Heart Rhythm Association (EHRA) Europace 2013 meeting held recently in Athens, Greece.
Patients with paroxysmal AF rate their heath-related quality of life (HRQoL) lower than their physicians do, according to results from the ANTIPAF (Angiotensin II Antagonist in Paroxysmal Atrial Fibrillation) trial. The study found these patients show signs of depression, sleeping disorders and low levels of physical activity even in the absence of significant concomitant cardiac disease.
Researchers led by Professor Karl Ladwig (Helmholtz Centre, Munich, Germany) analysed data from patients enrolled in the ANTIPAF trial, which examined discordance between AF patients and their doctors. Between February 2004 and September 2008, 334 patients (41% female and 59% male) with paroxysmal AF, without significant concomitant heart disease, and their physicians from 43 participating centres were asked to rate the patients’ HRQoL.
Results show physicians rated their patients’ HRQoL higher than patients, both for the mental component score and physical component score. In the regression analyses, depression was significantly associated with discord in the mental component score and the physical component score. Furthermore, sleeping disorders were associated with discord in the mental component score and physical activity with discord in the physical component score.
“Electrophysiologists (EPs) generally decide whether to take a more or less aggressive treatment approach according to the patient’s disease burden. Here, not only physical symptoms need to be taken into consideration, but also the patient’s mental health and quality of life in general. If EPs don’t know that their patients are suffering from depression they may not be offering them optimum treatments,” said Professor Ladwig. “Good communication between physicians and patients is of paramount importance for adherence to medications and long term prognosis,” he added.
James Rosengarten
Wessex Electrophysiology Fellow and BJCA Deanery Representative
([email protected])
Dr James Rosengarten reports highlights from the European Heart Rhythm Association (EHRA) Europace 2013 meeting held recently in Athens, Greece.
A website for AF patients AFib Matters (www.afibmatters.org) was introduced by the EHRA at the meeting.
The site outlines what AF is, symptoms, complications, types of drugs, and the need for stroke prevention. A section is devoted to frequently asked questions.
Professor Gregory YH Lip, who was Chairman of the Task Force responsible for the development of the website, said: “Patients with AF often have questions or misconceptions about their condition, such as whether they can travel, should they avoid certain foods, what can interact with their medication, and what is the risk of treatments. All of these questions are answered on the website.”
“The website also highlights the latest developments in the treatment and management of AF including the new oral anticoagulant drugs, ablation and devices. It is the authoritative website on AF and will be updated at regular intervals with relevant and timely information,” Professor Lip added.
James Rosengarten
Wessex Electrophysiology Fellow and BJCA Deanery Representative
([email protected])
Dr James Rosengarten reports highlights from the European Heart Rhythm Association (EHRA) Europace 2013 meeting held recently in Athens, Greece.
Details of two biomarker discovery programmes were presented by myself and other colleagues from Southampton.The early results were generated by our team, headed by Professor John Morgan, and build on several years of collaboration between cardiologists at the University Hospitals Southampton and scientists at the University of Southampton. The work hopes to advance sudden cardiac death risk stratification and ultimately move towards a more personal selection of interventions, such as implantable defibrillators.
Traditional risk stratification markers, such as left ventricular function or QRS width, fail to identify those at greatest risk, or merely demonstrate those with advanced heart failure who will go on to die regardless of what intervention is offered. This variation in response may, in part, be due to the genetic variability and response to, for example, ischaemic insult. Measuring this variability is challenging: gene expression does not accurately reflect functional protein expression. Proteomics is an emerging field in which this protein fingerprint can be sequenced directly.
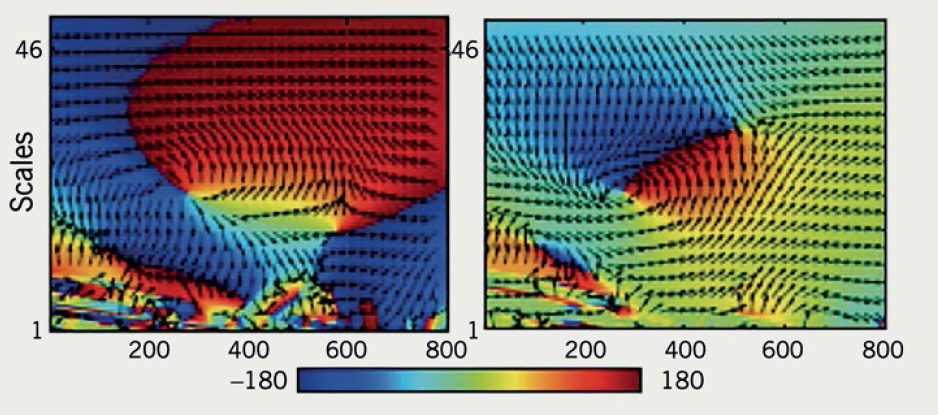
Figure 1. Protein cluster map demonstrating differential protein expression
Our team have exploited these techniques, most frequently used in cancer sciences where solid tissue is readily available, to look for differences in protein expression of the whole serum proteome. We have taken serum samples from 243 patients with implantable cardiac devices, who were followed-up for 40 months for the occurrence of death, ventricular arrhythmia or survival without arrhythmia.1 Following pooling and sample preparation, mass spectrometry was used to demonstrate differential expression between groups (figure 1), generating over 90 proteins that were associated with arrhythmia and not survival.
Generating candidate biomarkers in this fashion means that whole panels of proteins can be rapidly selected for testing. Usually, serum biomarkers are chosen based upon only a limited understanding of cellular mechanisms, whereas this technique enables unbiased selection without preconceptions.
An emerging risk stratification tool in recent years has been the use of cardiac magnetic resonance imaging (MRI) to quantify myocardial scar. Although the association between myocardial scar and ventricular arrhythmogenesis has been well reported, cardiac MRI is resource and time limited, making it unsuitable as a screening tool.
Our Southampton group looked at whether the resting ECG could be a surrogate for myocardial scar but found traditional ECG parameters were poor at detecting scar accurately.2 Manual assessment of the ECG is time consuming and limited to those parameters that can be visually appraised. We know that the ECG signal contains much more information but extracting that data and processing large volumes requires a fresh approach. By working with biomedical signal engineers, the team sought to develop a novel algorithm that was capable of classifying scar. Standard 12-lead ECGs were recorded from over 150 patients undergoing cardiac MRI with scar assessment. Time, frequency and phase domain features were then ‘extracted’ from the digitally acquired signal and used in a ‘machine learning’ experiment to train the algorithm to classify ECGs with known scar burden (see figure 2). This classifier was then tested on the ECGs of over 80 patients; the algorithm correctly identified scar with 81% sensitivity and 73% specificity.
Figure 2. ECG image giving an example of a classification parameter: wavelet phase coherence. Left panel shows scar beat; right panel shows no scar
As more data are processed this type of approach can be endlessly refined. The classifier could be valuable in population screening before referral for more costly complex investigations, such as MRI scanning.
James Rosengarten
Wessex Electrophysiology Fellow and BJCA Deanery Representative
([email protected])
Rosengarten JA, Scott PA, Larkin SE et al. High resolution multidimensional proteomics detects candidate arrhythmia biomarkers. Presented at Europace 2013, Athens, Greece. Europace 2013;15(suppl 2):ii11. http://dx.doi.org/10.1093/europace/eut194
Rosengarten JA, Dima SM, Panagiotou C et al. Novel non-invasive detection of arrhythmia substrate using supervised learning support vector machine. Presented at Europace 2013, Athens, Greece. Europace 2013;15(suppl 2):ii118. http://dx.doi.org/10.1136/heartjnl-2013-304019.72
Dr James Rosengarten reports highlights from the European Heart Rhythm Association (EHRA) Europace 2013 meeting held recently in Athens, Greece.
The 2013 ESC Guidelines on Cardiac Pacing and Cardiac Resynchronisation Therapy1 developed in collaboration with the EHRA, were launched at the meeting and also published simultaneously in the European Heart Journal and EP Europace. They have been redesigned to offer a more accessible format with greater emphasis on a practical ‘how to’ approach, which is targetted at generalists, including general practitioners and geriatricians, as well as cardiologists and electrophysiologists.
“By taking this user friendly approach we hope to get our messages out to the wider medical community, which ultimately should allow more patients to benefit from the latest evidence-based medicine,” explained Professor Michele Brignole (Ospedali del Tigullio, Italy), Chairperson of the Guidelines on Cardiac Pacing and Cardiac Resynchronisation Therapy Task Force.
The guidelines explore:
indications for pacing in patients who have cardiac arrhythmias
indications for cardiac resynchronisation therapy (CRT) in heart failure
indications for pacing in specific conditions, such as acute MI, pacing after cardiac surgery, transcatheter aortic valve implantation (TAVI) and heart transplantation, and pacing in children and individuals with congenital heart diseases
complications of pacing and CRT implantation
management considerations, such as re-implantation after device explantation for infection, MRI in patients with implanted cardiac devices, emergency (transvenous) temporary pacing and remote management of arrhythmias and devices.
The Guidelines take into account whether the patient has a persistent or intermittent problem, and whether it has been documented with electrocardiographic evidence (ECG documented) or not (ECG-undocumented).
The new ESC Guidelines have also created a new classification system for bradyarrhythmias according to mechanisms rather than aetiology.
Until now, guidelines have classified bradyarrhythmias according to aetiology, for example whether the problem has been caused by sinus node dysfunction, MI, or bundle branch block.
“One of the big innovations of these guidelines is the development of a logical decision tree displaying the different pacing modes according to different clinical situations. In effect these guidelines take the clinician by the hand and lead them through a series of three or four questions,” explained Professor Perry Elliott (The Heart Hospital, London), a member of the Guidelines Committee.
Pacemaker or ICD?
With over 90 major studies on pacing and resynchronisation published since the last guidelines, the Task Force went to considerable efforts to integrate the latest research. In areas where evidence is open to more than one interpretation, the guidelines provide information to help clinicians make a decision. For example, in patients with heart failure and poorly controlled symptoms, where choices have to be made between CRT pacemakers and CRT defibrillators, trials have had little to add to the decision-making process. “Clinicians have to consider factors such as expected life expectancy and comorbidities when choosing between pacemaker and defibrillator therapy,” said Professor Elliott.
James Rosengarten
Wessex Electrophysiology Fellow and BJCA Deanery Representative
([email protected])
Brignole M, Auricchio A, Baron-Esquivias G et al. for the Task Force on cardiac pacing and resynschronisation therapy of the European Society of Cardiology. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronisation therapy Eur Heart J 2013; http://dx.doi.org/10.1093/eurheartj/eht150 and Europace 2013; http://dx/doi.org/10.1093/europace/eut206
Authors: Francis C Wells
Publisher: Springer, London 2013
ISBN: 9781447145301
Price: £126.00
Just occasionally you come across a book which captivates your mind, one you know you will still be picking up and learning from in years to come, and a book that will be handed on to future generations, holding great historical interest. This slim yet detailed volume was researched and written by one of my surgical colleagues, Mr Francis Wells, whose interest in the heart has taken him from the cutting edge diagnostic and therapeutic surgical tools of the modern era, back to the 1500s and the heart studies of Leonardo da Vinci – a true ‘meeting of the minds’.
The Royal Collection holds the finest of Leonardo’s drawings, and this book – with a foreword by HRH Prince Charles, The Prince of Wales – features all those of the heart, describing its anatomy and functioning with extraordinary precision. These are accompanied by translations of the accompanying text, transcribed from the mirror image in which Leonardo wrote! Illustrations are compared with contemporary dissections, images from modern magnetic resonance scanners, and high definition ultrasound. Francis Wells provides a modern interpretation as a clinician, in a way that will be meaningful to cardiologists, medical specialists, anatomists, historians, and the general public.
This is a truly exceptional book. You will be amazed by what you have read, and struggle to put it down. Highly recommended, and excellent value for money!
Dr Sarah C Clarke
Vice President Education and Research
British Cardiovascular Society, 9 Fitzroy Square, London, W1T 5HW
Muslims worldwide represent a diverse and heterogeneous population varying widely in terms of geographical distribution, language, lifestyle, habits, customs, tradition, dietary habits and, above all, socio-economic status, which has a major influence on all other factors.1
The heart is extensively described in multiple Qur’anic verses and prophetic traditions as both an organ of psyche, intelligence and emotion, as well as an important organ that can be harmed by several factors.2 The prophet Muhammad, Peace Be Upon Him (PBUH), stated: “Beware! There is a piece of flesh in the body if it remains healthy the whole body becomes healthy, and if it is diseased, the whole body becomes diseased. Beware, it is the heart”.3 This tradition holds true if taken either literally or spiritually.
Fasting Ramadan and performing Hajj (Pilgrim) may pose problems to patients with cardiovascular disease, hence, it is important for the physician to have some sort of guidelines to help him in decision making when consulted about these matters.
Fasting Ramadan
Dr Hassan Chamsi-Pasha
Despite the fact that fasting in Ramadan is practised by more than a billion Muslims worldwide, there is yet no clear scientific consensus on its effects on cardiovascular disease.
During this month, participating Muslims refrain from eating, drinking, smoking and sex from dawn until sunset. As the month of Ramadan follows the lunar calendar, the fasting month is brought forward by about 10 days each year. For the next decade Ramadan will fall in the summer in the northern hemisphere. As daylight hours vary considerably between summer and winter months in non-equatorial countries, the length of the fast (which lasts from dawn to sunset) increases in the summer (to about 16–20 hours).4 Moreover, the already diverse dietary habits undergo further significant alteration during Ramadan fasting among the global Muslim population.
Although the Qur’an exempts sick people from the duty of fasting, a significant number of patients with heart disease insist on fasting despite the physician’s medical advice. Physicians do not always know how to advise such patients regarding fasting during Ramadan.
You could give your life a whole new path and light by opting for the experience of psychic readings from one the top psychic reading online websites where you get live psychic readings then and there. One can find a new solution and a new path with the help of experts.
A few studies have been published on the effects of fasting in cardiac patients.5-7 Fasting during the month of Ramadan does not increase the burden of acute cardiac illness. Temizhan et al.5 compared the incidence of acute heart disease events (acute myocardial infarction [AMI] and unstable angina) in Ramadan to one month before and after Ramadan in 1,655 patients, treated between the years 1991 and 1997 at their institution. The investigators reported no significant differences in the incidence of AMI and angina in Ramadan when compared with the other two periods, however, their study had many limitations, including the fact that it was not a population-based study, and only included a small number of patients.
What about patients with heart failure? A retrospective analysis of clinical data of 2,160 Qatari patients hospitalised with heart failure during a period of 10 years (January 1991 through December 2001) showed that there was no significant difference in the number of hospitalisations for heart failure during Ramadan when compared with the non-fasting months.6
A recent review of Medline English literature published between January 1980 and September 2012 revealed that the effects of fasting during Ramadan on stable patients with cardiac disease are minimal, and that patients with stable cardiac illness can fast during Ramadan, provided they comply with the recommended dietary and medication regimens.1
The conclusions from these studies cannot be extrapolated to patients with worse functional classes or those who are unstable.1,7 Of note, most of these studies were performed in the Middle East and Gulf area, and, therefore, such conclusions may not be extrapolated to patients living in North European countries, where the duration of daily fasting could be 2–3 hours longer.
Fasting does not apply to all Muslims. If it is considered to be detrimental to an individual’s health then the Qur’an states fasting should be avoided. “….Allah intends every facility for you; He does not want to put you to difficulties.”8 It is entirely left to the discretion of the treating physician to decide whether his patient is allowed to fast or not.
In their review, Salim et al.1 found that cardiovascular risk factors showed a trend towards improvement in patients fasting during Ramadan with stable cardiac disease, metabolic syndrome, dyslipidaemia and systemic hypertension, provided that unhealthy dietary patterns are avoided. The lipid profile of diabetic patients, however, deteriorated significantly during Ramadan fasting.
The improvement in plasma lipid levels, especially 30% to 40% improvement in high-density lipoprotein (HDL) levels, as reported in some studies, appear promising and should be explored further to gain insight into management of low-HDL dyslipidaemia.1 Diabetic patients should be carefully monitored during Ramadan fasting.4
Cardiac patient and Hajj
Hajj, the pilgrimage to Mecca, Saudi Arabia, is the largest and most long-standing annual mass gathering event on earth. Approximately two to three million Muslims from over 160 countries travel to Saudi Arabia each year for Hajj. These pilgrims are typically older adults with a spectrum of comorbid conditions and of various ethnicities. Approximately 25,000 British pilgrims perform Hajj each year. Performance of Hajj and its rites is physically very demanding. Extreme physical stressors such as heat, sun exposure, thirst, crowding, traffic congestions, steep inclines and rough ground underfoot increase the risk of communicable diseases, particularly respiratory infections, in those with certain pre-existing health conditions such as heart disease, renal disease, chronic lung disease and other conditions including diabetes mellitus.9
Cardiac patients planning for the Hajj should consult their doctor as Hajj is arduous even for healthy adults – for those with pre-existing cardiac disease, the physical stress can easily precipitate ischaemia. The onus is on the pilgrim to avoid the Hajj if their cardiac status is precarious, and clinicians must encourage this preventative stance. Cardiac patients planning for the Hajj should consult with their doctors before the journey; ensure sufficient supply of, and compliance with, medications. They should avoid crowds, perform some rituals by proxy, and report to the closest health centre for any symptom indicating cardiac decompensation.10
Cardiovascular risk factors
Although not outwardly mentioned in the Qur’an and prophetic traditions, the lifestyle that the Qur’an encourages drastically decreases the chances of individuals developing cardiovascular diseases via the following ways: engaging in spiritual activities, moderate eating, physical labour, and abstention from forbidden foods and drinks.11 Overeating has been strongly condemned and prohibited in the Qur’an. “Eat and drink, but be not excessive. Indeed, He does not like those who commit excess.”12
Furthermore, the prophet Muhammad (PBUH) encouraged the consumption of foods, such as olive oil and whole-grain bread: “Eat olive oil and anoint it upon your bodies since it is of the blessed tree”;13 and we currently know that olive oil consumption and Mediterranean diet is associated with a decreased risk of cardiovascular mortality, and overall mortality.14
Though we do not find much in the Qur’an about specific exercise recommendation, Islamic teachings encourage Muslims to teach their children swimming, archery and horse riding.
The Islamic prayer is performed at least five times a day and consists of a series of movements entailing standing, prostrating and sitting. When performing prayer, the Qur’an discourages lazily performing prayer as performed by the Hypocrites;2 thus, a lethargic and careless approach to prayer neither obtains any spiritual nor physical benefit to the state of health.
The physical movements during prayer with repetitive standing-sitting actions throughout the day also help prevent deep vein thrombi.
The lifestyle prescribed by these Islamic traditions promotes longevity of life, prevention of cardiovascular diseases, and discourages risk factors associated with such diseases.
In addition, the Qur’an states: “Truly it is in the remembrance of God that the hearts find peace”15.
Conflict of interest
None declared.
References
Salim I, Al Suwaidi J, Ghadban W, Alkilani H, Salam AM. Impact of religious Ramadan fasting on cardiovascular disease: a systematic review of the literature. Curr Med Res Opin 2013;29:343–54. http://dx.doi.org/10.1185/03007995.2013.774270
Al-Bukhari MI. The English Translation of Sahih Al Bukhari with the Arabic Text. Translated by Muhammad Muhsin Khan. Al-Saadawi Publications, 1996, Book 2 hadeeth 49.
Hui E, Bravis V, Hassanein M et al. Management of people with diabetes wanting to fast during Ramadan. Br Med J 2010;340:1407–11. http://dx.doi.org/10.1136/bmj.c3053
Temizhan A, Donderici O, Oguz D, Demirbas B. Is there any effect of Ramadan fasting on acute coronary heart disease events? Int J Cardiol 1999;70:149–53. http://dx.doi.org/10.1016/S0167-5273(99)00082-0
Al Suwaidi J, Bener A, Hajar HA, Numan MT.Does hospitalization for congestive heart failure occur more frequently in Ramadan: a population-based study (1991–2001).Int J Cardiol 2004;96:217–21. http://dx.doi.org/10.1016/j.ijcard.2003.06.018
Chamsi-Pasha H, Ahmed WH. The effect of fasting in Ramadan on patients with heart disease. Saudi Med J 2004;25:47–51.
Al-Hilali MT, Khan MM. The translation of the meanings of the Noble Quran 2:185. Madina (KSA): King Fahd Complex for the printing of The Holy Quran, 2005.
Al-Hilali MT, Khan MM. The translation of the meanings of the Noble Quran 7:31. Madina (KSA): King Fahd Complex for the printing of The Holy Quran, 2005.
Tirmizi Muhammad bin Eisa. Hadith no. 1852, in Sunan al-tirmizi. Dar Alfikr, Beirut 2001.
Buckland G, Mayén AL, Agudo A et al. Olive oil intake and mortality within the Spanish population (EPIC-Spain). Am J Clin Nutr 2012;96:142–9. http://dx.doi.org/10.3945/ajcn.111.024216
Al-Hilali MT, Khan MM. The translation of the meanings of the Noble Quran 13:28. Madina (KSA): King Fahd Complex for the printing of The Holy Quran, 2005.
Authors: John Soong, Anjali Balasanthiran, Donald C MacLeod, Derek Bell
John Soong
RCP Clinical Quality Improvement Research Fellow
Anjali Balasanthiran
Clinical Research Fellow and Specialist Registrar in Diabetes and Endocrinology
Derek Bell
Professor of Acute Medicine at Imperial College London, and Programme Director NIHR CLAHRC for Northwest London
NIHR CLAHRC for Northwest London Team, 4th Floor, Lift Bank D, Imperial College London, Chelsea & Westminster Hospital NHS Foundation Trust, 369 Fulham Road, London, SW10 9NH
Donald C MacLeod
Consultant Physician and Cardiologist
Western General Hospital, Crewe Road, Edinburgh, EH4 2XU
Atrial fibrillation (AF) is the most common cardiac dysrrhythmia. The evidence base and expert consensus opinion for management have been summarised in several international guidelines. Recent studies suggest a disparity between contemporary practice and perceived best practice.
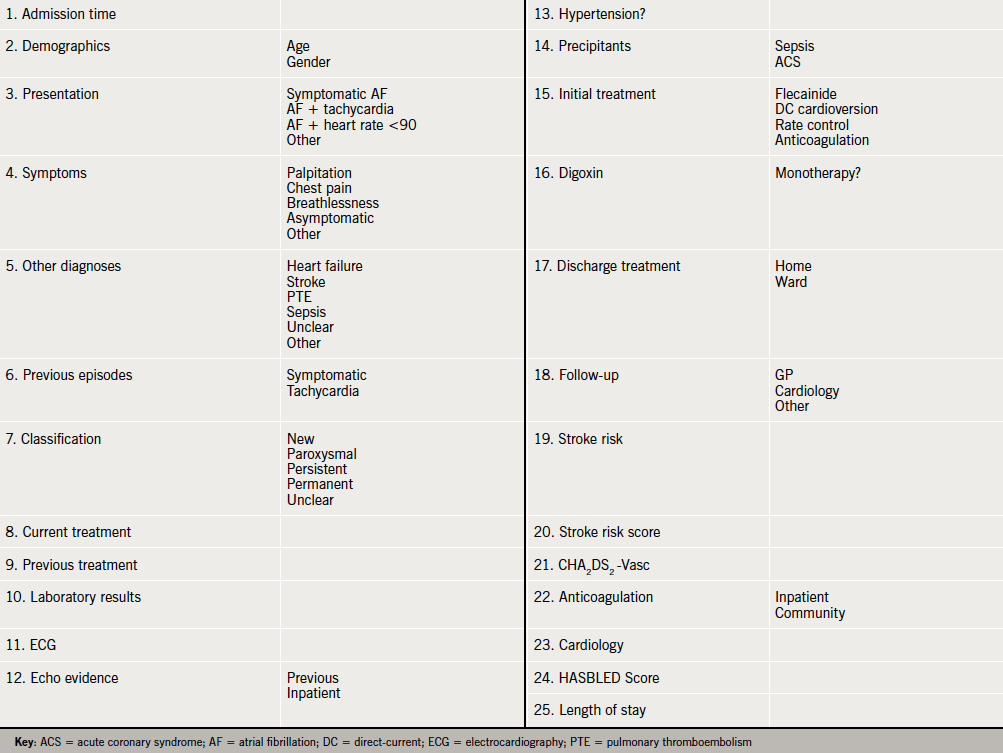
An electronic questionnaire was constructed to capture details of patient demographics and current practice, including risk assessment for stroke and major bleeding. All patients >18 years with AF as a primary or secondary diagnosis admitted from midday on the 14th September 2011 to midday on the 15th September 2011, were included in the survey. Participating units were recruited from the Society for Acute Medicine registry, and provided with an electronic link and password to enter data for individual patient episodes.
The electronic questionnaire was completed for 149 patient episodes from 31 acute medical units (AMUs) across the UK. The typical patient with AF presenting to the AMU is older, has important medical comorbidities (sepsis in almost a third) and frequently presents out of hours. Initial management was digoxin alone in 22% and 23% had a documented stroke risk assessment, not in-keeping with current guidelines.
This relatively simple methodology yields valuable insight into the real world management of AF, providing an additional evidence base.
Introduction
Atrial fibrillation (AF) is the most common cardiac dysrrhythmia, whose sequelae include stroke, heart failure and poor quality of life.1 In parallel with an ageing population, the prevalence of AF is increasing, with persistent or permanent forms affecting 10–15% of the population over the age of 75 years.2-6
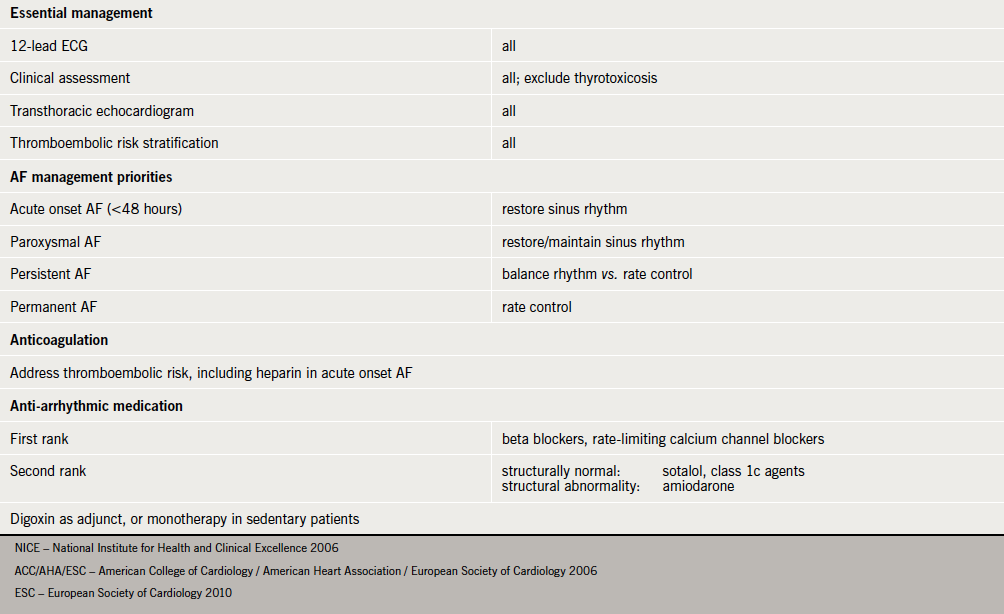
The effective management of AF has been a source of recurring debate, leading to the publication of combined American College of Cardiology/American Heart Association/European Society of Cardiology (ACC/AHA/ESC), and National Institute for Health and Clinical Excellence (NICE) guidelines in 2006.7,8 In addition to evidence-based strategies for rhythm and rate control, an important issue addressed in these guidelines was that of thrombotic risk assessment and management. This was further prioritised in the 2010 ESC document.9 Recent studies have suggested that both primary10 and secondary11 care may not follow guidelines for the management of AF.
Acute medical units (AMUs) represent the first
point of assessment and care for the majority of medical inpatients. Hospital episode statistic data suggest that, of the 5,287,032 emergency admissions in England from 1st April 2010 to 30th March 2011, 57,898 (1.1%) had a primary diagnosis of AF.
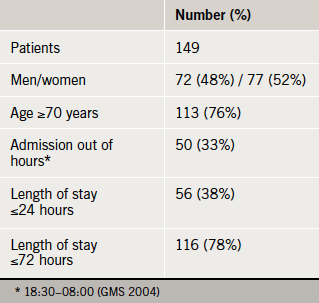
Table 1. Survey cohort demographics
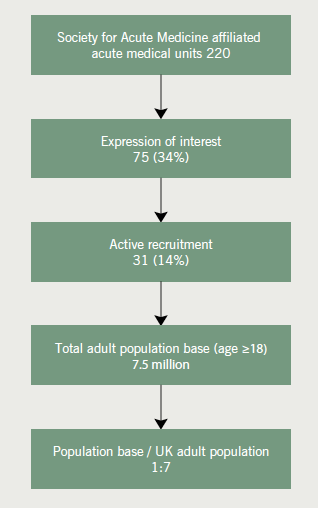
The number of AMUs affiliated with the Society of Acute Medicine (SAM) has steadily increased since its inception in the millennium, and now stands at 220.12 These units serve a substantive UK population base, creating considerable potential for collaborative research into current medical practice.
The Acute Medical Research Network of SAM, in association with the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC) for Northwest London, commissioned a survey to examine contemporary management of AF within AMUs in the UK. We report the findings of this survey and its implications.
Methods
An electronic questionnaire was constructed with fields including risk assessment for stroke and major bleeding, citing widely used scoring systems (see Appendix 1).
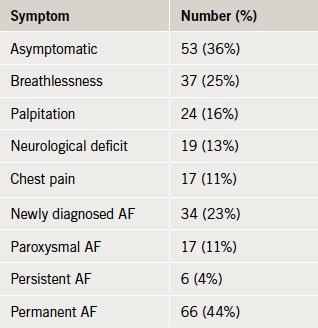
Table 2. Symptoms and atrial fibrillation (AF) status
All patients >18 years with AF as a primary or secondary diagnosis admitted over a specific 24-hour time period (midday on 14th September to midday on 15th September 2011) were included in the survey. Participating AMUs were provided with a link and password to enter data for each patient episode into the survey. Units were advised to nominate an individual to coordinate participation at a local level to prevent duplication of data entry.
Results
Of the 220 AMUs initially canvassed, 31 eventually provided patient data, representing a population base of more than seven and a half million adult UK residents (figure 1). The electronic questionnaire was completed for 149 patients (table 1). The symptom profile and AF status of the patients is displayed in table 2.
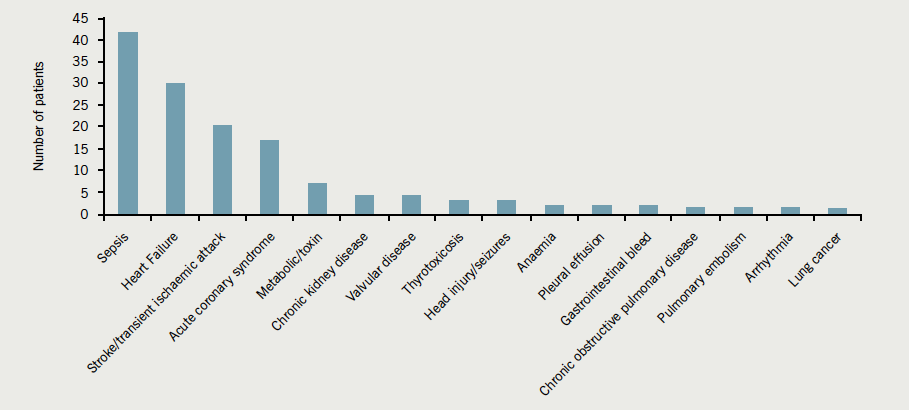
Sepsis was the principal associated diagnosis present in almost a third, followed by heart failure and cerebrovascular events (figure 2). The hierarchy of associated diagnoses was different for the elderly, where cerebrovascular events ranked highest, together with sepsis and heart failure accounting for 70% of presentations (figure 3).
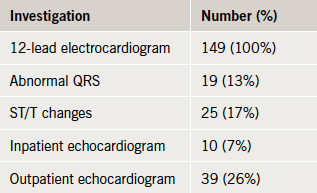
Cardiac investigations
In line with NICE guidelines, all patients received a resting 12-lead electrocardiogram (ECG). Abnormal QRS morphology, predominantly left bundle branch block, was noted in 17%, and repolarisation changes were seen in 13% (table 3).
Stroke risk assessment
Less than a quarter of the study population (23%) had any form of stroke risk assessment (NICE, CHADS2, CHA2DS2-Vasc) (Appendix 2). Retrospective CHA2DS2-Vasc scores for those who were not risk stratified averaged 3.5, and the mean age of this subgroup was 77 years. Of note, 73 (80%) patients with a significant risk for thromboembolic stroke (retrospective CHA2DS2-Vasc score >2) were not prescribed anticoagulation therapy at time of discharge. The risk of stroke needs to be balanced with the risk of major haemorrhage. Despite this, only 36% (n=54) of patients with a CHA2DS2-Vasc score >2, had a HAS-BLED score of ≥3 (8.7 major bleeds per 100 patient-years). In addition, 24% (n=15) of patients at risk of major haemorrhage (HAS-BLED score of ≥3) were discharged on anticoagulation therapy. Four of this group were concomitantly discharged on antiplatelet therapy.
Figure 2. Diagnosis reported in association with AF
Figure 3. Diagnosis reported in association with AF in patients aged 80–89 years
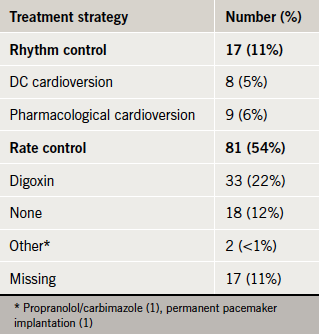
Initial AF treatment strategies
Table 3. Cardiac investigations
Rate control was the principal form of initial management, but one in five patients received digoxin alone (table 4).
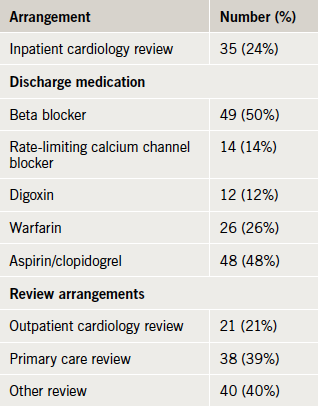
Discharge planning, medication and follow-up
At the time of data collection, information was available for 99 discharged patients (table 5). One in five was offered inpatient or outpatient cardiology review and most were prescribed rate-limiting medication. Half were discharged on aspirin or clopidogrel, and a quarter on warfarin, with the remainder receiving neither an antiplatelet nor an antithrombotic agent.
Table 4. AF treatment strategies
Out of hours
In total, 49 (33%) of patients presented out of normal working hours (defined as from 6.30 p.m. to 8.00 a.m. on weekdays, the whole of weekends, bank holidays and public holidays).13 Documentation of stroke risk was performed less frequently in patients who presented with AF out of hours, though this was not statistically significant (18.4% vs. 27.2%; Fishers exact p=0.29). Patients who presented with AF out of hours tended not to be discharged within 24 hours (28.6% of patients presenting out of hours vs. 45.7% of patients during normal working hours; Fishers exact p=0.06).
Discussion
The ideal database to study this population would contain the following features:
Table 5. Discharge planning and review arrangements
Retain the ability for longitudinal study across primary and secondary care
Continuous data collection direct from clinical records (less sampling bias and case ascertainment issues; reduce duplication/copy error)
Embedded data validation processes
Low cost (financial and human resource)
Ability for rapid feedback to participating organisations
Reproducible.
There is no existing database that fulfils all these parameters.
Clinical audits and registries have been successfully used to drive quality improvement. Routinely collected data (e.g. hospital episode statistics [HES]) have been used to explore trends in patient outcome. It is estimated that the average cost of running a national clinical audit is £250,000 per year. These audits have reasonably lengthy duration of set up, data collection and analysis, with consequent delay in feedback to participating Trusts. Poor coding practices have also given rise to doubt as to the accuracy of HES data.
We describe the piloting of an electronic survey driven, in part, by the expanding infrastructure of SAM. Our survey was designed to incur low cost and be quick to administer, facilitating rapid data analysis and feedback to participants. Additionally, the methodology allows for ease of replication, allowing time series data to be captured following local improvements. Two thirds of AMUs approached did not express interest in participation, and the eventual contribution rate was low at 14% of the total, but nonetheless, the population base accessed was considerable. We suggest that this model, readily adaptable to different conditions and presentations, has powerful potential as a research tool in acute medical practice.
Our survey suggests that the current management of individuals with AF in the acute medical environment is falling short of national standards7-9 in a number of areas (see Appendix 3).
First, in only a minority did the extended clinical assessment include echocardiography when that information was not already available. Second, a thromboembolic risk assessment was recorded for less than one in four patients. Patients with intermittent or sustained non-valvular AF have similar risks of thromboembolic events.14 Previous studies15 have shown considerable variation in decision-making processes between clinicians with regards to stroke and bleeding risks, as well as choice of antithrombotic therapy, leading to significantly different treatment choices. Findings from RealiseAF, a cross-sectional, international study of >10,000 patients seen over 800 sites, demonstrated that of patients with a CHA2DS2-Vasc score meeting criteria for anticoagulation, the percentage of patients actually receiving anticoagulation were 37.7%, 54.4% and 59.0% for paroxysmal, persistent and permanent AF, respectively.16
Reasons for recalcitrance in antithrombotic therapy in the elderly (who paradoxically are at higher risk of thromboembolic events) stem from safety concerns relating to the risk of falls and major bleeding.17 Several large randomised-controlled trials18,19 have confirmed the efficacy and safety of antithrombotic therapy in this population. The recent systematic review and health economics model of Hughes et al.20 demonstrated that stroke risk stratification models were able to discriminate between different categories of stroke risk (at least 95% confidence interval), and that anticoagulation of high-risk patients was cost-effective. Balancing the risk of stroke in AF with that of major bleeding, Pisters et al.21 have devised a novel bleeding risk score (see Appendix 4), which was validated by Lip et al.22 on a large patient cohort from the Stroke Prevention Using an Oral Thrombin Inhibitor in Atrial Fibrillation (SPORTIF) III and V trials.
Third, digoxin was the first choice for rate control. Rate control with digoxin is as effective as beta blockers or calcium channel blockers for control of ventricular rate at rest. Beta23 and calcium channel blockers,24 however, have the added advantage of providing effective rate control in exertion (hyperadrenergic state).7,25 In addition, beta blockers have proven efficacy if the patient suffers from concomitant ischaemic heart disease, and diltiazem has been shown to be superior to digoxin in acute AF.26 It is also important to note that while rate control in permanent AF provides alleviation of symptoms, it does not reduce thromboembolic risk.
Fourth, although not expressly stated in the guidelines, but recommended by inference, four out of five patients did not receive a cardiology opinion. EuroHeart, a large scale study (n=5,333) of ambulatory and hospitalised patients with AF seen in cardiology centres across 132 countries demonstrated excellent outcomes.27 Of note, a relatively high proportion of this population (34%) underwent cardioversion at enrolment and 94% had an echocardiogram at least once over the course of a year.
The survey’s demographic findings are in keeping with previous epidemiological data suggesting a higher prevalence of AF in the elderly.28 The typical patient also frequently presents out of hours. Accordingly, the most relevant specialties, cardiology and stroke medicine, are unlikely to be involved in initial, or indeed downstream, management. The primary focus for acute medicine is often an important associated or precipitating diagnosis, such as sepsis. This is in contrast to other national and international studies of AF where chronic comorbidities are more frequently reported, often in ambulatory settings.29
Other management challenges for the acute medical environment include potential hypotensive and negative inotropic effects of beta and calcium channel blockers. ECG monitoring may be standard in acute medical units, but is not commonly accompanied by the nurse to patient ratios that would support aggressive cardiovascular management. In contrast, one study demonstrated that metoprolol was frequently prescribed (in 67.6% of cases) to patients treated for AF in emergency departments within the UK.30
Where acute medicine could undoubtedly improve is in the assessment of thromboembolic risk, particularly with the availability of CHA2DS2-Vasc, a rapid user-friendly scoring system with prognostic power. This said, taking the time to assess risk and translate this to treatment may be challenging in high intensity, rapid turnover units.
Within the different setting of general practice, the percentage of patients prescribed anticoagulants increased from 20 to 34% in men and 17 to 25% in women over four years.31 It is worth noting that general practice databases also hold a large amount of valuable information. This information may be selectively harnessed to aid anticoagulation decision making by using tools such as GRASP-AF. When used alongside data from the Global Anticoagulation Registry in the Field (GARFIELD), an international registry of patients with AF at risk of stroke, GRASP-AF may improve anticoagulation uptake for appropriate patients in the acute medical setting.32
We recognise that this study design has a number of limitations. It is a measurement at a single point of time, with little facility to compensate for variation. It consists of self-reported data, with no ability for external validation. The need to distinguish zero admissions from non-participation became evident at the end of the pilot, as did the need for contextual data (e.g. size of AMU). The dataset is rich with clinical information and process measures, but the design makes clinical outcome measures difficult to measure. Relatively low participation rates limit generalisability of the results.
Despite this, we suggest that this relatively simple study offers valuable insights into the real world management of an important and common condition, and highlights the challenges faced in delivering best evidence into practice, particularly within an acute medical setting •
Acknowledgements
We would like to thank the Society for Acute Medicine for distribution of the electronic survey, all participating units and Dr David Ward, Consultant Physician in Acute Medicine at Queen Elizabeth Hospital, South London Healthcare NHS Trust, for contributing to design of the electronic survey.
Conflict of interest
JS Clinical Research Fellowship is funded by the Royal College of Physicians. AB, DB, DCM: none declared.
Disclaimer
This article presents independent research commissioned by the National Institute for Health Research (NIHR) under the Collaborations for Leadership in Applied Health Research and Care (CLAHRC) programme for North West London. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Key messages
The first national survey examining the management of atrial fibrillation (AF) within acute medical units in the UK
Almost a quarter of patients with permanent AF were prescribed digoxin as initial monotherapy. The rationale for this treatment decision was only documented in a third of cases and was not in keeping with national standards
Stroke risk score was infrequently documented (23%) and retrospective analysis suggests 80% of patients with a significant risk for thromboembolic stroke (CHA2DS2-Vasc score >2) did not receive anticoagulation
Real world practice differs from national recommendations, further work examining barriers to implementation is crucial
Appendix 1. Electronic questionnaire fields
Appendix 2. Thromboembolic risk assessment
Appendix 3. Core recommendations for the management of AF: NICE, ACC/AHA/ESC, ESC
Miyasaka Y, Barnes ME, Gersh BJ et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–25. http://dx.doi.org/10.1161/CIRCULATIONAHA.105.595140
Heeringa J, van der Kuip DAM, Hofman A et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J 2006;27:949. http://dx.doi.org/10.1093/eurheartj/ehi825
Lip GY, Golding DJ, Nazir M, Beevers DG, Child DL, Fletcher RI. A survey of atrial fibrillation in general practice: the West Birmingham Atrial Fibrillation Project. Br J Gen Pract 1997;47:285–9.
Stewart S, Hart CL, Hole DJ, McMurray JJV. Population prevalence, incidence, and predictors of atrial fibrillation in the Renfrew/Paisley study. Heart 2001;86:516–21. http://dx.doi.org/10.1136/heart.86.5.516
Go AS, Hylek EM, Phillips KA et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285:2370–5. http://dx.doi.org/10.1001/jama.285.18.2370
National Institute for Health and Clinical Excellence. Atrial fibrillation: the management of atrial fibrillation. CG36. London: NICE, 2006. Available from: http://www.nice.org.uk/CG36
Fuster V, Rydén LE, Cannom DS et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation – executive summary. Circulation 2006;114:e257–e354. http://dx.doi.org/10.1161/CIRCULATIONAHA.106.177292
Camm JA, Kirchhof P, Lip GYH et al. Guidelines for the management of atrial fibrillation. The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology. Euro HeartJ 2010;31:2369–429. http://dx.doi.org/10.1093/eurheartj/ehq278
Loo B, Parnell C, Brook G, Southall E, Mahy I. Atrial fibrillation in a primary care population: how close to NICE guidelines are we? Clin Med 2009;9:219–23.
Lim JCES, Suri A, Sornalingham S, Chua TP, Lim J. Audit of management of atrial fibrillation at a district general hospital. Br J Cardiol 2010;17:89–92.
Lambourne A, Percival F, Ward D, Laverty AA, Bell D. An evaluation of consultant input into acute medical admissions management in England. Report of: Hospital service patterns versus clinical outcomes in England. London: Royal College of Physicians, 2012.
The National Health Service (General Medical Services Contracts) Regulations 2004. 2013.
Hart RG, Pearce LA, Rothbart RM, McAnulty JH, Asinger RW, Halperin JL. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy. J Am Coll Cardiol 2000;35:183–7. http://dx.doi.org/10.1016/S0735-1097(99)00489-1
Anderson N, Fuller R, Dudley N. ‘Rules of thumb’ or reflective practice? Understanding senior physicians’ decision-making about anti-thrombotic usage in atrial fibrillation. QJM 2007;100:263–9. http://dx.doi.org/10.1093/qjmed/hcm016
Chiang CE, Naditch-Brule L, Murin J et al. Distribution and risk profile of paroxysmal, persistent, and permanent atrial fibrillation in routine clinical practice: insight from the real-life global survey evaluating patients with atrial fibrillation international registry. Circ Arrhythm Electrophysiol 2012;5:632–9. http://dx.doi.org/10.1161/CIRCEP.112.970749
Mant J, Hobbs F, Fletcher K et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet 2007;370:493–503. http://dx.doi.org/10.1016/S0140-6736(07)61233-1
Rash A, Downes T, Portner R, Yeo WW, Morgan N, Channer KS. A randomised controlled trial of warfarin versus aspirin for stroke prevention in octogenarians with atrial fibrillation (WASPO). Age Ageing 2007;36:151–6. http://dx.doi.org/10.1093/ageing/afl129
Hughes M, Lip G. Risk factors for anticoagulation-related bleeding complications in patients with atrial fibrillation: a systematic review. QJM 2007;100:599–607. http://dx.doi.org/10.1093/qjmed/hcm076
Pisters R, Lane DA, Nieuwlaat R, De Vos CB, Crijns HJGM, Lip GYH. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation. Chest 2010;138:1093–1100. http://dx.doi.org/10.1378/chest.10-0134
Lip GYH, Nieuwlaat R, Pisters R, Lane DA, Crijns HJGM. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach. Chest 2010;137:263–72. http://dx.doi.org/10.1378/chest.09-1584
DiBianco R, Morganroth J, Freitag JA, Ronan JA, Lindgren KM. Effects of nadolol on the spontaneous and exercise-provoked heart rate of patients with chronic atrial fibrillation receiving stable dosages of digoxin. Am Heart J 1984;108:1121–7. http://dx.doi.org/10.1016/0002-8703(84)90592-1
Lundstrom T, Rydén L. Ventricular control and exercise performance in chronic atrial fibrillation: effects of diltiazem verapamil. J Am Coll Cardiol 1990;16:86–90. http://dx.doi.org/10.1016/0735-1097(90)90461-W
Lim HS, Hamaad A, Lip G. Clinical review: clinical management of atrial fibrillation-rate control versus rhythm control. Critical Care 2004;8:271–9. http://dx.doi.org/10.1186/cc2827
Schreck DM, Rivera AR, Tricarico VJ. Emergency management of atrial fibrillation and flutter: intravenous diltiazem versus intravenous digoxin. Ann Emerg Med 1997;29:135–40. http://dx.doi.org/10.1016/S0196-0644(97)70319-6
Pisters R, Nieuwlaat R, Prins MH et al. Clinical correlates of immediate success and outcome at 1-year follow-up of real-world cardioversion of atrial fibrillation: the Euro Heart Survey. Europace 2012;14:666–74. http://dx.doi.org/10.1093/europace/eur406
Hobbs FDR, Fitzmaurice D, Mant J et al. A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study. Health Technol Assess 2005;9:iii–iv, ix–x, 1–74.
Freestone B, Rajaratnam R, Hussain N, Lip GYH. Admissions with atrial fibrillation in a multiracial population in Kuala Lumpur, Malaysia. Int J Cardiol 2003;91:233–8. http://dx.doi.org/10.1016/S0167-5273(03)00031-7
Rogenstein C, Kelly AM, Mason S et al. An international view of how recent-onset atrial fibrillation is treated in the emergency department. Acad Emerg Med 2012;19:1255–60. http://dx.doi.org/10.1111/acem.12016
Majeed A, Moser K, Carroll K et al. Trends in the prevalence and management of atrial fibrillation in general practice in England and Wales, 1994–1998: analysis of data from the general practice research database. Heart 2001;86:284–8. http://dx.doi.org/10.1136/heart.86.3.284
Kakkar AK, Mueller I, Bassand JP et al. International longitudinal registry of patients with atrial fibrillation at risk of stroke: Global Anticoagulant Registry in the FIELD (GARFIELD). Am Heart J 2012;163:13.e1–9.e1. http://dx.doi.org/10.1016/j.ahj.2011.09.011
Charlotte Manisty
NIHR Academic Clinical Lecturer and Imaging fellow, Imperial College NHS Trust and Imaging Fellow, The Heart Hospital, University College London
Imperial College NHS Trust, Hammersmith Hospital, Du Cane Road, London, W12 0HS
James C Moon Reader and Honorary Consultant Cardiologist
The Heart Hospital, 16–18 Westmoreland Street, London W1G 8PH
As UK cardiologists, we might be forgiven for assuming acceptance of cardiovascular magnetic resonance (CMR). The past decade has seen CMR in the UK change from an ancillary research/specialist patient populations tool to an evidence-based imaging modality for use in all spheres of cardiovascular disease. Within the wider medical community and overseas, however, the advantages of CMR remain opaque.
That CMR is the gold standard for heart size and function, and for congenital and inherited heart disease is little disputed. The additional benefit of CMR for tissue characterisation has gained widespread acceptance, particularly now with convincing prognostic data across a wide variety of disorders,1 and the large EuroCMR registry (27,000 patients, 15 countries),2 showing that CMR entirely changed diagnosis in nearly 10% of subjects. CMR adoption as a ‘workhorse’ for ischaemia and viability testing has, however, been slower, with continued calls for cost-effectiveness and head-to-head comparison data with other modalities. These data are now available,3,4 and UK guidelines support perfusion CMR for the investigation of chest pain, but detractors point out that, despite the higher image quality and better diagnostic capabilities, little evidence of translation to better patient outcomes exists.
Growth in the UK
As Ripley et al. outline in their article, there has been recent substantial, and likely sustained, UK growth of CMR. Currently, there are several centres within the UK scanning some of the largest volumes worldwide – the Heart Hospital Imaging Centre in London recently scanned its 10,000th patient in the 37 months since opening. The by-product (or potentially the driver) of this is that the UK leads CMR education and training, and attracts significant numbers of international cardiologists and radiologists to train. Systems are well-codified, including attention to ‘educating the referrer’, as well as potential service providers, with a well-developed network of regular regional CMR meetings such as the quarterly London CMR meeting. From a research perspective, the UK is a dominant force with five top international research centres pioneering many techniques and conducting major clinical trials. The future also looks promising – 60% of the Young Investigator finalists at Society for Cardiovascular Magnetic resonance (SCMR) and EuroCMR 2013 were UK based.
Despite these positives, the CMR community still has a way to go to divest itself of the label ‘advanced imaging modality’ and to be considered mainstream. CMR specialists should communicate its unique strengths (such as tissue characterisation), but acknowledge both the value of other techniques (for example echocardiography for valvular assessment) and the reducing yield if referral thresholds lower too far.
Worldwide, CMR remains a minority player for ischaemia; there are 44 single-photon emission computed tomography (SPECT) scans performed for every CMR in the USA, with a (scarcely believable) 9.5% of all insured adults having one radiation-based cardiac imaging study over a three-year period.5 This entrenched pattern in the USA is not going to be easy to reverse because of the reimbursement streams, the nature of US healthcare, and the perception of CMR as an expensive, specialist technique. Even within the UK, CMR funding remains potentially fragile with an evolving commissioning landscape.
Responsibility with growth
For CMR, with growth comes responsibility. Quality must be maintained; expertise cannot be ‘diluted’ by opening large numbers of small-volume centres. Combined, the top 12 centres perform 66% of all UK CMR scans; the bottom 28 centres only 13%. Because 15%4 of CMR requests are for ‘1% diseases’, such as iron overload, arrhythmogenic right ventricular cardiomyopathy (ARVC), pericardial diseases and masses, and perhaps the same again are for common diseases in rare manifestations, low-volume centres struggle to develop expertise to maintain incremental value – and trusted techniques, when they get it wrong, harm more. We would agree with Ripley et al. that the ideal model to fulfil projected service expansion and maintain quality may be a ‘hub and spoke’. Scans of less common conditions could be either centrally verified, or referred for both scanning and reporting to ensure more specialised sequences are acquired. This should improve educational opportunities available in the smaller centres, and allow greater transparency for quality control, audit and discrepancy meetings. There is a need for workforce planning – over 10% of all current cardiology trainees aim to subspecialise in CMR imaging,6 meaning there are more current trainees than CMR centres – a serious bubble.
Nevertheless, UK cardiology and patients benefit from UK CMR. This benefit – with nurturing – is likely to be maintained and grow. A more obvious example of the openness of the UK to innovation at all levels is hard to find and the benefits are now clear for all to see.
1. Flett AS, Westwood MA, Moon JC et al. The prognostic implications of cardiovascular magnetic resonance. Circ Cardiovasc Imag 2009;2:243– 50. http://dx.doi.org/10.1161/CIRCIMAGING.108.840975
2. Bruder O, Wagner A, Lombardi M et al. European Cardiovascular Magnetic Resonance (EuroCMR) registry – multi national results from 57 centers in 15 countries. J Cardiovasc Magn Reson 2013;15:9. http://dx.doi.org/10.1186/1532-429X-15-9
3. Greenwood JP, Maredia N, Younger JF et al. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CEMARC): a prospective trial. Lancet 2012;379:453–60. http://dx.doi.org/10.1016/S0140-6736(11)61335-4
4. Walker S, Girardin F, McKenna C et al. Cost-effectiveness of cardiovascular magnetic resonance in the diagnosis of coronary heart disease: an economic evaluation using data from the CEMARC study. Heart 2013;99:873– 81. http://dx.doi.org/10.1136/heartjnl-2013-303624
5. Chen J, Einstein AJ, Fazel R et al. Cumulative exposure to ionizing radiation from diagnostic and therapeutic cardiac imaging procedures. J Am Coll Cardiol 2010;56:702–11. http://dx.doi.org/10.1016/j.jacc.2010.05.014