We present a rare case of cardiac arrest caused by torsades de pointes in relation to severe hypothyroidism, which highlights the importance of thyroid replacement therapy compliance.
Background
Hypothyroidism is a common endocrine disorder, which has a variety of effects on the cardiovascular system including decreased cardiac output, increased systemic vascular resistance, accelerated atherosclerosis and rhythm disturbances, such as sinus bradycardia, conduction defects or non-specific ST changes.1,2 Hypothyroidism can also cause prolongation of the QTc interval and ventricular arrhythmias.1
Case presentation
A 76-year-old woman was admitted to our hospital with a collapse, and while in the emergency department she sustained a witnessed cardiac arrest secondary to torsades de pointes (TdP) (figure 1). This was terminated with direct current electrical cardioversion followed by magnesium and potassium infusions. Over the next 48 hours she had four further short runs of self-terminating TdP. Our patient had a background of primary hypothyroidism, type 2 diabetes mellitus and stable angina. Her medications included: aspirin, levothyroxine, bisoprolol, furosemide, nitrazepam, tramadol, gliclazide, atorvastatin and lansoprazole.

The initial electrocardiogram (ECG) showed sinus bradycardia, PR interval of 200 ms, prolonged QTc interval (640 ms, Bazzet’s formula) and T-wave inversions in lateral and anterior leads (figure 2). Her ECG from one year ago showed a normal QTc interval. Blood tests revealed hypokalaemia of 2.7 mmol/L, normal magnesium (0.82 mmol/L) and adjusted calcium levels (2.53 mmol/L). Potassium levels normalised within a few hours after potassium infusion. Her thyroid function tests showed severe hypothyroidism with high thyroid stimulating hormone (>150 mIU/L, normal range 0.3–5.5 mIU/L) and low free T4 (2.6 pmol/L, normal range 11.5–22.7 pmol/L).
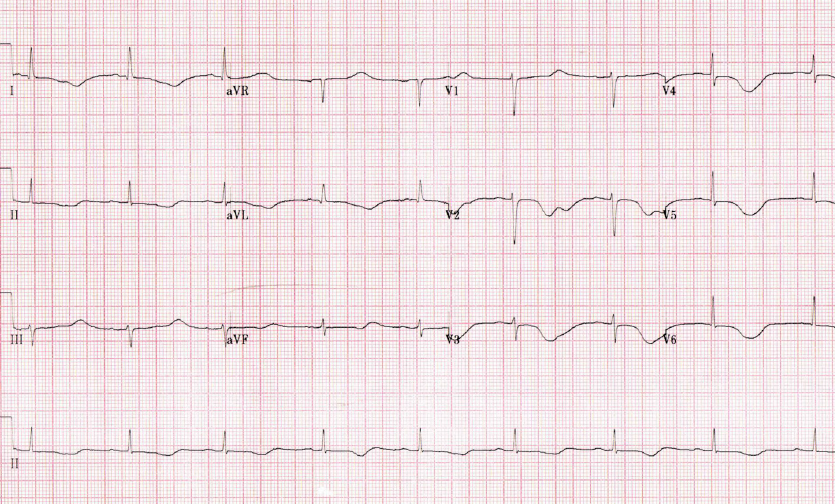
200 ms, prolonged QTc interval (640 ms, Bazzet’s formula) and T-wave inversions in
lateral and anterior leads
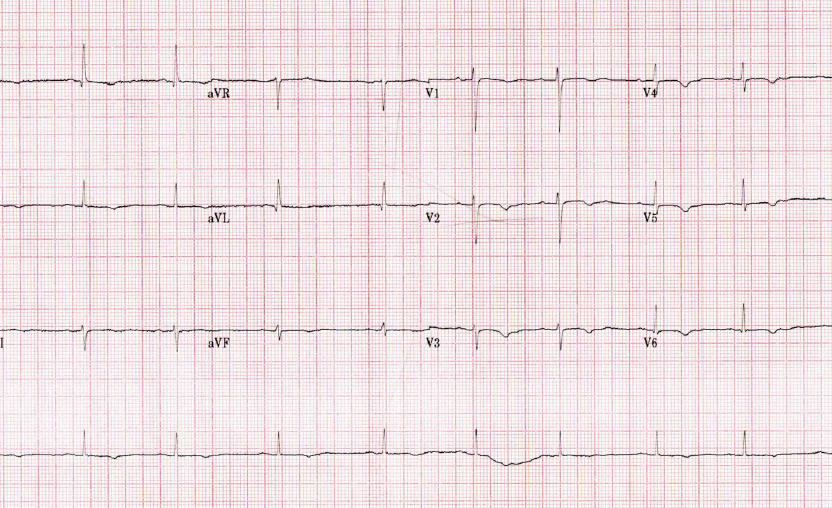
After further discussion, it transpired that our patient was not compliant with her thyroid replacement therapy. Levothyroxine was slowly re-introduced and serial ECGs showed a gradual shortening of QT interval with QTc of 444 ms six days after initial admission (figure 3).
Discussion
TdP is a type of polymorphic ventricular tachycardia that can occur in the setting of a prolonged QT/QTc interval and may lead to a sudden cardiac death.3 There are a variety of identified causes of acquired QT/QTc prolongation, such as drugs, electrolyte imbalance, bradycardia, cocaine use, myocardial ischaemia, subarachnoid haemorrhage, autonomic neuropathy or human immunodeficiency virus disease.4 However, TdP secondary to severe hypothyroidism is rare,1 with a limited number of cases reported in the literature.5-7
Our case shows that severe hypothyroidism can indeed lead to life-threatening arrhythmias, and it is likely that hypokalaemia contributed to the clinical picture. More importantly, however, it highlights the need for medical professionals to ensure thyroid replacement therapy compliance and inform patients regarding the possible risks associated with non-adherence, including rarer, but potentially life-threatening, ones
Conflict of interest
None declared.
References
1. Klein I, Sanzi S. Thyroid disease and the heart. Circulation 2007;116:1725–35. http://dx.doi.org/10.1161/CIRCULATIONAHA.106.678326
2. Almandoz JP, Gharib H. Hypothyroidism: etiology, diagnosis and management. Med Clin North Am 2012;96:203–21. http://dx.doi.org/10.1016/j.mcna.2012.01.005
3. Zipes DP, Camm AJ, Borggrefe M et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Europace 2006;8:146–837. http://dx.doi.org/10.1093/eurheartj/ehl199
4. Khan IA. Long QT syndrome: diagnosis and management. Am Heart J 2002;143:7–14. http://dx.doi.org/10.1067/mhj.2002.120295
5. Schenck JB, Rizvi AA, Lin T. Severe primary hypothyroidism manifesting with torsades de pointes. Am J Med Sci 2006;331:154–6. http://dx.doi.org/10.1097/00000441-200603000-00008
6. Shojaie M, Eshraghian A. Primary hypothyroidism presenting with torsades de pointes type tachycardia: a case report. Cases J 2008;1:298. http://dx.doi.org/10.1186/1757-1626-1-298
7. Kandan SR, Saha M. Severe primary hypothyroidism presenting with torsades de pointes. BMJ Case Rep 2012:published online September 17. http://dx.doi.org/10.1136/bcr.12.2011.5306
