Rani Khatib
Consultant Pharmacist in Cardiology and Cardiovascular Research, Leeds Teaching Hospitals NHS Trust, and Visiting Associate Professor, University of Leeds
Medicines Management & Pharmacy Services, Leeds Teaching Hospitals NHS Trust, Great George Street, Leeds, LS1 3EX
Some healthcare professionals may see the idea of ‘joint working’ between NHS Trusts and pharmaceutical companies as anathema – a bridge too far in the direction of private interests perhaps? However, when the needs of patients, the health system and the company are aligned, it can bring significant benefits for everyone.
At the Leeds Teaching Hospitals NHS Trust (LTHT), we have recently entered into a joint working partnership with Boehringer Ingelheim.1 This arrangement is helping us to develop a patient-centred clinic specifically focused on reducing cardiovascular (CV) risk in individuals with diabetes recently discharged from LTHT following a myocardial infarction (MI). Initiated in September 2021, the clinic is run jointly by the cardiology department at Leeds General Infirmary and the diabetes services at the Trust. It is shared funded by the Trust and by Boehringer Ingelheim.
Meeting patient needs
Dr Rani Khatib
Previously, individuals with CV disease and type 2 diabetes in our area were treated by two separate specialty teams. However, it is now well-established that there is significant interplay between CV and metabolic disease, as well as renal disorders.2,3 Thus, we have come to believe that the management of complex post-MI Cardio–Renal–Metabolic or ‘CaReMe’ cases requires a more holistic care model. In this way, we can ensure that patients gain easy access to all required risk and medicine optimisation, and other forms of care, in line with current treatment guidelines, and individually tailored to their personal circumstances.
Our CaReMe service is built around a pharmacist-led clinic scheduled for six to eight weeks after the patient’s MI. Eligible individuals are first triaged by our advanced cardiology pharmacists, then sent a newly modified version of our ‘MYMEDS’, a self-reporting tool for assessing current secondary prevention medicines (SPMs), practical concerns and (modifiable) adherence barriers; this tool was developed from the broader MYMEDS questionnaire that we have used for many years with post-MI patients regardless of diabetes status.4 The ‘MYMEDS-Diabetes’ questionnaire includes exploration of diabetes medicines, knowledge about risk factors and diabetes distress, as well as other elements related to providing CaReMe consultation. We use the information gained from the pre-clinic MYMEDS-Diabetes as the baseline for a comprehensive, virtual or in-person, patient-centred review of their CV, diabetes and renal management needs. This includes:
Analysis of key risk factors/markers, e.g. cholesterol, blood pressure, glycosylated haemoglobin (HbA1c), urine albumin:creatinine ratio, estimated glomerular filtration rate (eGFR)
Post-MI secondary prevention, e.g. antithrombotics, antihypertensives, lipid-lowering treatments, etc.
Diabetes management, including lifestyle advice and medicines prescription
Other relevant comorbidities.
The clinic is a ‘one-stop shop’ for these highly comorbid individuals. Although run primarily by a consultant pharmacist and, in the future, by advanced cardiology pharmacists, patients have access to consultant cardiologists and diabetologists, when required. Dietary and weight management support is also available, so it is truly multi-disciplinary.
The model aligns with the comprehensive guidance on medicines optimisation from the National Institute for Health and Care Excellence (NICE), which highlights the centrality of a holistic patient-centred approach when delivering medicines optimisation, led by a pharmacist within their specialty.5 However, the focus of the clinic goes well beyond medicines optimisation, with the aim of fostering healthy behaviours and building adherence to both better lifestyle modifications and medicines. Action plans are developed in collaboration with patients and shared with their wider care teams.
A clinic model that works
We have extensive experience of delivering pharmacist-led, multi-disciplinary CV clinics at LTHT.6,7 Indeed, the specialist CaReMe service was developed from our original, ‘all comers’ post-MI service, which has been operating successfully since 2015.6 That clinic has led to reduced waiting times from discharge to first outpatient cardiology review, enhanced SPM optimisation, and significant reductions in rates of non-adherence to SPMs of 43–71% at three to six months post-clinic; patient satisfaction with the model is high.6 Furthermore, the pharmacist-led approach has freed up cardiology outpatient clinic space and created more capacity.
Then, in February 2017, we initiated a centralised, pharmacist-led proprotein convertase subtilisin/kexin type 9 inhibitor (PCSK9i) and lipids management clinic to help improve the usage of novel medicines and provide tailored support for lipids optimisation. This service has yielded significant improvements in cholesterol levels, has been well received by patients, and is considered cost-effective by service commissioners.7
Benefits of joint working
The proof-of-concept phase of our original (2015) post-MI service development programme was partly funded by AstraZeneca within a joint working framework. The success of that phase led to the clinic being fully commissioned by the Leeds Clinical Commissioning Groups, and it has subsequently become the standard service offered to patients with MI in Leeds. Given our previous success with joint working, it felt natural to do so again with the CaReMe service. Although only recently initiated, the clinic has already begun to identify important adherence barriers and concerns. Early outcomes and patient feedback are promising – and we intend to collect and publish complete data in the future.
It should be noted that ‘joint working’ is not a catch-all term for any form of pharmaceutical involvement in National Health Service (NHS) funding. It is instead a specific type of collaboration defined by the Department of Health and Social Care as: “Situations where, for the benefit of patients, NHS and industry organisations pool skills, experience and/or resources for the joint development and implementation of patient-centred projects and share a commitment to successful delivery”.8 The main beneficiary must always be patients.
For us at LTHT, joint working is facilitating redesign of the care pathway. However, there are many other ways in which this type of model can be deployed – for example in increasing the treatment capacity of the system, identifying uncontrolled patients, economic analysis, or generating patient experience data.9 Joint working arrangements must always be non-promotional, and ideally should be underpinned by a written agreement outlining clear milestones, the ’exit strategy’, and methods for measuring outcomes, so that successful programmes can be replicated and scaled across the country when appropriate.9
Apart from our own experiences, other recent, successful joint working collaborations have included:
A project in the West of England aimed at stroke prevention in individuals with atrial fibrillation through improved medicines management in primary care, which has successfully reduced the number of strokes and yielded significant cost savings
The ‘All Wales Haematological Malignancy Data Solution’, capturing real-world evidence for improving patient outcomes in myeloma
A programme in London attempting to improve the detection and treatment of heart failure and educate patients on home management of their condition.9
Conclusion
Joint working between the NHS and pharma can bring significant benefits, most importantly for patients – for example, fewer hospital appointments, better information and/or a better experience of the healthcare system. There can also be important advantages for the NHS (e.g. higher-quality care configured around patient needs, improved health outcomes, and better use of resources) and for the pharma company (e.g. increased appropriate use of medicines aligned with guidelines, and improved internal understanding of the challenges facing the health system).9
Thus, used appropriately, joint working can be a win–win–win. Our experience of hospital–pharma partnerships to develop novel clinics is leading to improved care. Rather than a bridge too far, these collaborations have instead been a bridge to better healthcare provision.
Conflicts of interest
The author is the lead for both the Boehringer Ingelheim and AstraZeneca joint working projects.
Funding
The project is funded by both the Leeds Teaching Hospitals NHS Trust and Boehringer Ingelheim as part of a joint working arrangement.
Acknowledgements
Thanks to Professor Steve Wheatcroft and Professor Ramzi Ajjan of Leeds Teaching Hospitals and LICAMM, University of Leeds, for their support in this project.
2. Mata-Cases M, Franch-Nadal J, Real J, Cedenilla M, Mauricio D. Prevalence and coprevalence of chronic comorbid conditions in patients with type 2 diabetes in Catalonia: a population-based cross-sectional study. BMJ Open 2019;9:e031281. https://doi.org/10.1136/bmjopen-2019-031281
4. Khatib R, Patel N, Hall AS. The my experience of taking medicines (MYMEDS) questionnaire for assessing medicines adherence barriers in post-myocardial infarction patients: development and utility. BMC Cardiovasc Disord 2020;20:46. https://doi.org/10.1186/s12872-020-01362-y
5. National Institute for Health and Care Excellence. Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes. NG5. London: NICE, 2015. Available from: https://www.nice.org.uk/guidance/ng5
6. Khatib R, Patel N, Laverty U et al. Re-engineering the post-myocardial infarction medicines optimisation pathway: a retrospective analysis of a joint consultant pharmacist and cardiologist clinic model. Open Heart 2018;5:e000921. https://doi.org/10.1136/openhrt-2018-000921
7. Khatib R, Khan M, Barrowcliff A et al. Innovative, centralised, multidisciplinary medicines optimisation clinic for PCSK9 inhibitors. Open Heart 2022;9:e001931. https://doi.org/10.1136/openhrt-2021-001931
9. Association of the British Pharmaceutical Industry. Joint working. A toolkit for industry and the NHS. London: ABPI, September 2019. Available from: https://www.abpi.org.uk/publications/joint-working
Dual antiplatelet therapy is recommended for secondary prevention of ischaemic events in coronary artery disease. Some patients, who may be at high bleed risk if other factors are present, should be considered for gastroprotection. In our survey, we assessed whether gastroprotection was prescribed for hospital inpatients, especially high-risk patients, who were receiving dual antiplatelet therapy at discharge, and the type of gastroprotection prescribed. We found that over 13 months, a total of 1,693 patient episodes were prescribed dual antiplatelet therapy at discharge, of which 71% also received gastroprotection. Of the patient episodes who were not prescribed gastroprotection, 46% (223/483) met the criterion of age as a risk factor for gastroprotection. A further 30 episodes met other risk criteria of certain concomitant drugs or prior comorbidity. There is a need among clinicians and pharmacy teams within the hospital for recognition and management of this opportunity to improve the care of these patients.
Introduction
Dual antiplatelet therapy (DAPT), a combination of aspirin and either clopidogrel, prasugrel or ticagrelor, is recommended for secondary prevention of ischaemic events in coronary artery disease in both patients managed medically and those undergoing percutaneous coronary intervention (PCI). Patients taking DAPT may be at high bleed risk if other factors are present, such as older age, kidney and/or liver disease, active cancer, anaemia, low platelet count, previous stroke, prior bleeding, recent trauma or surgery, and use of oral anticoagulants and/or non-steroidal anti-inflammatory drugs (NSAIDs).1 Gastrointestinal (GI) bleeding is a particularly serious DAPT-related complication, and gastroprotection with a proton-pump inhibitor (PPI) or H2-receptor antagonist should be considered for certain groups of patients, though guidance on which groups should receive gastroprotection is variable.
Box 1. Risk factors for gastrointestinal (GI) bleed
High dose of aspirin
Older age, especially aged over 70 years
History of gastroduodenal ulcer, GI bleeding, or gastroduodenal perforation
Helicobacter pylori infection
Concomitant use of medicines that are known to increase the risk of GI bleeds, such as anticoagulants
European guidelines recommend a PPI for all patients, whereas American guidance is more targeted at high-risk patients.2,3 As a concise summary to be followed in England, National Institute for Health and Care Excellence (NICE) Clinical Knowledge Summaries identify people at high risk of GI adverse effects with antiplatelet treatment if the risk factors in box 1 are present.4 Gastroprotection reduces this bleeding risk by 70% or more, and COGENT (Clopidogrel and the Optimization of Gastrointestinal Events Trial) showed that the addition of omeprazole 20 mg daily to aspirin–clopidogrel dual therapy in patients with a median age of 69 years reduced overt gastroduodenal bleeding from an absolute 0.6% down to 0.1% at 180 days after randomisation.5 A post-hoc analysis of the COGENT trial evaluated the safety and efficacy of PPI therapy in the post-acute coronary syndrome (ACS) group. This study, in a cohort of high-risk patients, showed significant benefit with bleeding reduced from 1.2% to 0.24% at 180-day follow-up.6 Others have shown that PPIs are superior to H2-receptor antagonists for gastroprotection in patients on DAPT, though this review included trials using low and high doses of each class of drug.7
Some patients (e.g. those with existing atrial fibrillation or those who develop atrial fibrillation after PCI, coronary artery bypass graft or ACS) are prescribed triple therapy – an anticoagulant in addition to DAPT – which further increases the risk of bleeding. These patients should automatically be considered for gastroprotection. For instance, our acute hospital trust policy notes that compared with oral anticoagulation therapy alone, the addition of DAPT to oral anticoagulation therapy results in at least a two- to threefold increase in bleeding complications, and that routine use of PPIs is recommended.8 Though not mentioned in the policy, current practice recognises there are cautions when considering use of a PPI, such as electrolyte abnormalities.
However, various studies from across the globe have reported that patients on DAPT and at high risk of bleeding have not received concomitant gastroprotection. One Danish study examined 46,301 patients on DAPT after a myocardial infarction.9 Only 35% of patients at higher risk of upper GI bleeding received the recommended treatment with a PPI to reduce bleeding risk related to PCI based on the 2015 European Society of Cardiology (ESC) guideline criteria, which are broader than those factors described in box 1, including a lower age threshold of ≥65 years.10 An American study from 2011, using an age risk factor ≥75 years, noted that in a sample of 250 hospital patients the use of GI prophylaxis was appropriate in only 48% of patients.11 A UK study from 2008 found that less than half of 370 ACS patients at high bleeding risk taking DAPT were provided with GI prophylaxis and, in particular, of the ≥75 years cohort only 50% received such GI prophylaxis.12 Interestingly, all the above studies apparently examined only the presence or absence of concomitant GI prophylaxis and did not look at the dose prescribed.
As well as the association between DAPT and increased GI bleeding,13 adverse drug reactions due to antiplatelets have been associated with hospital admission, including preventable admissions.14-16 One specific area of medicines safety – measuring the number of patients aged 18 years and over currently prescribed aspirin and another antiplatelet without a gastroprotective medicine – was identified in the Investment and Impact Fund (IIF) 2020/21 for primary care in England.17 This IIF, which is a financial incentive scheme, supports primary care networks in England to deliver high-quality care to their population, as well as supporting the delivery of priority objectives in the National Health Service (NHS) Long Term Plan. Primary care networks consist of GP practices working together with community, mental health, social care, pharmacy, hospital and voluntary services in their local areas in groups of practices. The indicators in the IIF domain of delivering better outcomes for patients on medication focused on improved prescribing to support a reduction in medicines-related harm, and the IIF metric for the number of patients on DAPT and a gastroprotective is reported on the NHS Business Services Authority medicines safety dashboard at various levels including practice, and primary care network.18
Aims and objectives
The main aim of this review was to assess whether gastroprotection was prescribed for hospital inpatients, especially high-risk patients, who were receiving DAPT at discharge, and the type of gastroprotection prescribed.
Method
Study design and setting
This was a descriptive, retrospective study in a 750-bed acute hospital in the south-west of England serving a population of 450,000, which doubles over the summer holiday period.
Data collection and processing
Patient episodes involving prescription of DAPT (aspirin plus concomitant use of clopidogrel, ticagrelor or prasugrel) upon discharge between April 2020 and April 2021 were included in the data extraction from the hospital e-prescribing system (Wellsky International, Basildon, UK). The electronic prescribing records of the identified patients were also searched for co-prescription of gastroprotection, either PPI or H2 antagonist, and if there was a documented contraindication to gastroprotection. This prescribing database was also analysed to ascertain if patients on DAPT should have been on gastroprotection using risk factors of age 71 years and over, some concomitant medication (selective serotonin reuptake inhibitor [SSRI], NSAID, prednisolone, nicorandil or an anticoagulant), and also if patients were on triple therapy (dual antiplatelets and an anticoagulant). A list of diagnostic codes was generated for those patients not prescribed gastroprotection identifying the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) administrative code, if present, in primary or secondary position in hospital episode statistics for the episode of care. This identified patients with the following diagnostic codes: gastrointestinal haemorrhage, unspecified (K92.2); gastric ulcer, unspecified as acute or chronic, without haemorrhage or perforation (K25.9); personal history of diseases of the digestive system (Z87.1). Demographic details were also recorded, as were any potential biochemical abnormalities that might influence the use of a PPI as gastroprotection. Data were entered into Microsoft Excel for analysis.
Results
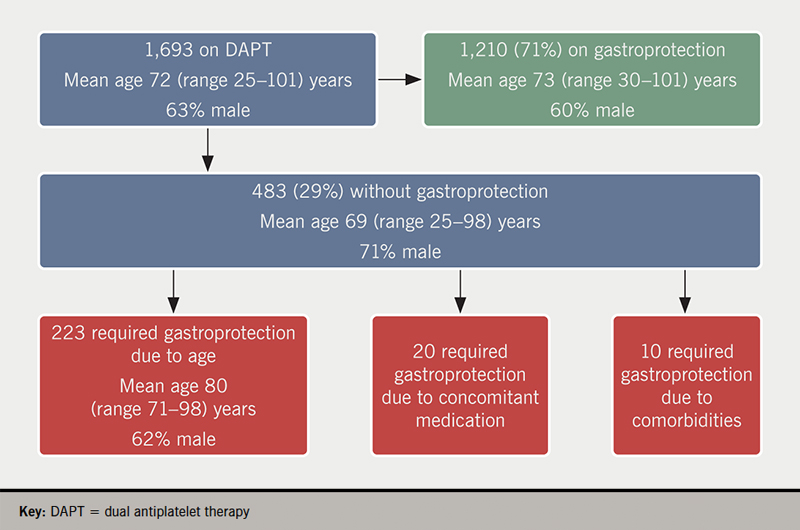
Over this 13-month period there was a total of 1,693 patient episodes (mean age 72 years, 63% male) prescribed DAPT at discharge, of which 1,210 (71%) also received gastroprotection (figure 1). Of the 483 patient episodes who were not prescribed gastroprotection, 223 (46%) met the criterion of age as a risk factor for gastroprotection.
Figure 1. Flow of patients
There were 20 episodes (mean age 61 years, range 38–69, 80% male) of patients aged under 71 years not on gastroprotection but receiving a SSRI, NSAID, prednisolone, nicorandil or an anticoagulant. In one of these episodes a patient received nicorandil and an anticoagulant in addition to DAPT and so was very much at high bleeding risk. There were a further 10 patient spells without gastroprotection but with an ICD code of previous history of GI ulcer/bleed, and all these were younger than 71 years of age. Hence, we identified that gastroprotection was potentially missing in a total of 15% (n=253) of DAPT patient episodes. Of those 253 episodes where we would have expected patients to be prescribed gastroprotection but were not, we observed 47 unique episodes where a patient had either an abnormal value, as defined by our clinical chemistry department, of a serum magnesium level <0.7 mmol/L or a serum sodium level <133 mmol/L during that spell. In these patients, our clinical staff consider that use of a PPI, though desirable, is inappropriate. The remaining 206 episodes had no such abnormal electrolyte contraindication.
Of those 1,210 episodes of patients receiving gastroprotection, a PPI was prescribed in 1,171 instances. There were 49% (n=587) prescriptions for lansoprazole, 48% (n=564) omeprazole (of which 34 were for the 10 mg strength), and 10 each of esomeprazole, and rabeprazole. A H2 antagonist was prescribed in 39 instances, of which 72% (n=28) were for famotidine, and 11 ranitidine. For the 28 patient episodes of famotidine prescribed as gastroprotection, 13 of these instances were recorded as due to the patient being unable to receive a PPI due to low sodium and/or low magnesium.
Discussion
In this retrospective observational study, we found that gastroprotection was not prescribed during the hospital admission for 29% (n=483) of 1,693 patient episodes receiving DAPT. Approximately half (253) of those who did not receive gastroprotection, equivalent to 15% of the total cohort of episodes, were classified as at high risk for GI bleed based on age, or a selection of concomitant medication, or specific limited comorbidities. In one English study, GI bleeding was identified as the single greatest cause of hospital admission or death due to adverse drug reactions, largely caused by prescribed antithrombotics.19 A recent systematic review and meta-analysis found that the use of PPIs was associated with a reduced risk of GI bleeding in patients treated with DAPT after PCI or ACS.20 Hence, consideration of gastroprotection, certainly for high-risk patients, is an important aspect of the pharmaceutical care of these patients.
The inclusion in the English NHS IIF for general practice potentially has implications for hospitals.17 This IIF metric measures the percentage of patients aged 18 years or over prescribed aspirin and another antiplatelet in the three months to 1 April 2022, who in the three months to 1 April 2023 were either (i) no longer prescribed aspirin and/or no longer prescribed an antiplatelet or (ii) prescribed a gastroprotective in addition to both aspirin and another antiplatelet. There are thresholds for payment to general practice of 75% as the lower threshold and 90% as the upper threshold. Although this IIF metric does not directly apply to what is happening in English hospitals, our observed value of 71% of our cohort of patient episodes on DAPT receiving gastroprotection may attract scrutiny from primary care wanting to see a higher proportion of patients discharged on gastroprotection. This may be especially relevant as primary care prescribing across Cornwall is shown to be higher than the England average for having patients on DAPT but not receiving gastroprotection, with Cornwall having approximately 4,000 patients in the final quarter of 2020/2021 compared with an expected value of 3,000.18
Though antiplatelets are listed as high-risk medicines and seen as a candidate for prioritisation for a medication review in hospitals, it is not clear from the literature if this is solely because of the risk of GI bleeding and the need for gastroprotection, or other reasons, such as appropriate indication or duration for treatment.21-23 Our age threshold for increased risk was 71 years and over, and we note that other studies use a different age threshold for high-risk prescribing of DAPT.24,25 For instance, a Canadian study of cardiology outpatients found that 57.1% (n=68) of 119 patients aged over 60 years on DAPT were receiving a PPI.26
When considering newly initiated gastroprotection when one of the antiplatelet agents is clopidogrel, the choice of PPI may be a consideration, though up to now our trust has not been overly concerned about the theoretical interaction between clopidogrel and omeprazole.27 However, the Care Quality Commission, which monitor, inspect and regulate general practice services to make sure they meet fundamental standards of quality and safety, now scrutinise how general practitioners manage this potential interaction.28 Therefore, it is expected to become more of an issue for hospitals discharging patients on this combination. In fact, of the 574 patient spells in our study when omeprazole or esomeprazole was co-prescribed, clopidogrel was the antiplatelet used in combination with aspirin in 261/574 (45%) of cases.
PPIs are not without risk and are associated with slight increased risk of bone fractures and pneumonia, and an association with vitamin B deficiency, and with Clostridium difficile infection in hospitalised patients. PPIs are also known to have adverse effects, such as low sodium and low magnesium,29 which may be a reason for considering a H2 antagonist. The European guidelines advise that impaired magnesium absorption with PPIs has been reported only from studies in which patients had received a PPI for at least one year.2 However, a recent review of PPI adverse effects found that most putative adverse outcomes associated with PPI use may not be supported by high-quality evidence and are likely to have been affected by underlying confounding factors.30 We found that in 19% (47/243) instances, the reason for not prescribing a PPI appeared to be low sodium or low magnesium.
Strengths and limitations
This is a large cross-sectional study that collected data on all patients with prescribed DAPT over a 13-month period. There are, however, limitations. First, it was conducted in a single centre in England; this might restrict the generalisability of our findings. Second, the retrospective nature of this may introduce bias or other uncertainties. Third, we did not ascertain the indication for DAPT nor confirm if the PPI or H2 antagonist was actually for gastroprotection or another indication, nor if patients came in on these drugs as opposed to being started during their admission. Fourth, we did not check risk factors for gastroprotection other than age, selected concomitantly prescribed drugs, and selected comorbidities. Finally, we did not check if those not prescribed gastroprotection had significant contraindications other than electrolyte abnormalities.
Conclusion
We identified that 15% of patients on DAPT were at high risk for GI bleed and, yet, did not receive appropriate GI prophylaxis. There is a need among clinicians and pharmacy teams within the hospital for recognition and management of this opportunity to improve the care of these patients. This will include updating local guidelines to incorporate the recommendation on gastroprotection in patients on dual antiplatelets and at risk of GI bleeding.
Key messages
Dual antiplatelet therapy (DAPT) is a risk factor for gastrointestinal bleeding and concomitant gastroprotection is recommended to reduce the risk of bleeding if there are various patient risk factors
We assessed whether gastroprotection was prescribed for hospital inpatients, especially high-risk patients, who were receiving DAPT at discharge, and the type of gastroprotection prescribed
Over 13 months, a total of 1,693 patient episodes were prescribed DAPT at discharge, of which 71% (1,210) also received gastroprotection. Of the patient episodes who were not prescribed gastroprotection, 46% (223/483) met the criterion of age as a risk factor for gastroprotection. A further 30 episodes met other risk criteria of certain concomitant drugs or prior comorbidity
Our study provides further evidence on the possible suboptimal management of the use of gastroprotective therapy in hospitalised patients who are receiving DAPT
Conflicts of interest
None declared.
Funding
None.
Study approval
This study was categorised as a service evaluation, not requiring NHS Research Ethics Committee approval. This study was approved locally as a Clinical Effectiveness Project. As data collection occurred within standard clinical care, routinely provided at the study site, patient consent was neither sought nor required. Patient data were used in accordance with local NHS Trust Policy and in line with general data protection regulations.
References
1. Tersalvi G, Biasco L, Cioffi GM et al. Acute coronary syndrome, antiplatelet therapy, and bleeding: a clinical perspective. J Clin Med 2020;9:2064. https://doi.org/10.3390/jcm9072064
2. Valgimigli M, Bueno H, Byrne RA et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2018;39:213–60. https://doi.org/10.1093/eurheartj/ehx419
3. Abraham NS, Hlatky MA, Antman EM et al. ACCF/ACG/AHA 2010 expert consensus document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use. Circulation 2010;122:2619–33. https://doi.org/10.1161/CIR.0b013e318202f701
5. Bhatt DL, Cryer BL, Contant CF et al.; on behalf of the COGENT Investigators. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med 2010;363:1909–17. https://doi.org/10.1056/NEJMoa1007964
6. Vaduganathan M, Cannon CP, Cryer BL et al.; on behalf of the COGENT Investigators. Efficacy and safety of proton-pump inhibitors in high-risk cardiovascular subsets of the COGENT trial. Am J Med 2016;129:1002–05. https://doi.org/10.1016/j.amjmed.2016.03.042
7. Almufleh A, Ramirez FD, So D et al. H2 receptor antagonists versus proton pump inhibitors in patients on dual antiplatelet therapy for coronary artery disease: a systematic review. Cardiology 2018;140:115–23. https://doi.org/10.1159/000489165
8. Royal Cornwall Hospitals NHS Trust. Management of acute chest pain of suspected cardiac origin (unstable angina/NSTEMI) in Cornwall Policy. June 2020.
9. Sehested TSG, Carlson N, Hansen PW et al. Reduced risk of gastrointestinal bleeding associated with proton pump inhibitor therapy in patients treated with dual antiplatelet therapy after myocardial infarction. Eur Heart J 2019;40:1963–70. https://doi.org/10.1093/eurheartj/ehz104
10. Roffi M, Patrono C, Collet JP et al. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2016;37:267–315. https://doi.org/10.1093/eurheartj/ehv320
11. Morneau KM, Reaves AB, Martin JB et al. Analysis of gastrointestinal prophylaxis in patients receiving dual antiplatelet therapy with aspirin and clopidogrel. J Manag Care Pharm 2014;20:187–93. https://doi.org/10.18553/jmcp.2014.20.2.187
13. Nishtala PS, Jamieson HA, Hanger HC et al. Examining the risks of major bleeding events in older people using antithrombotics. Cardiovasc Drugs Ther 2019;33:323–9. https://doi.org/10.1007/s10557-019-06867-z
14. Howard RL, Avery AJ, Slavenburg S et al. Which drugs cause preventable admissions to hospital? A systematic review. Br J Clin Pharmacol 2006;63:136–47. https://doi.org/10.1111/j.1365-2125.2006.02698.x
15. Lghoul-Oulad Saïd F, Hek K, Flinterman LE et al. Prevalence and incidence rate of hospital admissions related to medication between 2008 and 2013 in The Netherlands. Pharmacoepidemiol Drug Saf 2020;29:1659–68. https://doi.org/10.1002/pds.5122
16. Mejía G, Saiz-Rodríguez M, Gómez de Olea B et al. Urgent hospital admissions caused by adverse drug reactions and medication errors – a population-based study in Spain. Front Pharmacol 2020;11:734. https://doi.org/10.3389/fphar.2020.00734
19. Pirmohamed M, James S, Meakin S et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 2004;329:15–19. https://doi.org/10.1136/bmj.329.7456.15
20. Guo H, Ye Z, Huang R. Clinical outcomes of concomitant use of proton pump inhibitors and dual antiplatelet therapy: a systematic review and meta-analysis. Front Pharmacol 2021;12:694698. https://doi.org/10.3389/fphar.2021.694698
21. Otero MJ, Moreno-Gómez AM, Santos-Ramos B et al. Developing a list of high-alert medications for patients with chronic diseases. Eur J Intern Med 2014;25:900–08. https://doi.org/10.1016/j.ejim.2014.10.021
22. Otero MJ, Guzmán MDT, Galván-Banqueri M et al. Utility of a trigger tool (TRIGGER-CHRON) to detect adverse events associated with high-alert medications in patients with multimorbidity. Eur J Hosp Pharm 2021;28(suppl 2):s41–s46. https://doi.org/10.1136/ejhpharm-2019-002126
23. Alshakrah MA, Steinke DT, Tully PM et al. Development of the adult complexity tool for pharmaceutical care (ACTPC) in hospital: a modified Delphi study. Res Social Adm Pharm 2021;17:1907–22. https://doi.org/10.1016/j.sapharm.2021.02.009
24. Wallis KA, Elley CR, Moyes S, Kerse N. Safer Prescribing and Care for the Elderly (SPACE): a pilot study in general practice. BJGP Open 2018;2:bjgpopen18X101594. https://doi.org/10.3399/bjgpopen18X101594
25. Peek N, Gude W, Keers RN et al. Evaluation of a pharmacist-led actionable audit and feedback intervention for improving medication safety in UK primary care: an interrupted time series analysis. PLoS Med 2020;17:e1003286. https://doi.org/10.1371/journal.pmed.1003286
26. Shen H, Sestier M, Soltani I et al. Gastroprotection in patients on antithrombotic therapy: a quality improvement study. Can J Cardiol 2021;37:S37–S38. https://doi.org/10.1016/j.cjca.2021.07.080
29. Makunts T, Cohen IV, Awdishu L et al. Analysis of postmarketing safety data for proton-pump inhibitors reveals increased propensity for renal injury, electrolyte abnormalities, and nephrolithiasis. Sci Rep 2019;9:2282. https://doi.org/10.1038/s41598-019-39335-7
30. Veettil SK, Sadoyu S, Bald EM et al. Association of proton-pump inhibitor use with adverse health outcomes: a systematic umbrella review of meta-analyses of cohort studies and randomised controlled trials. Br J Clin Pharmacol 2022;88:1551–66. https://doi.org/10.1111/bcp.15103
We report the case of an elderly woman with recent hip replacement surgery that presented with cardiogenic shock. The initial echocardiogram was suggestive of mid-ventricular Takotsubo cardiomyopathy, which was later confirmed due to absence of severe coronary artery disease and complete resolution of the patient’s cardiac systolic dysfunction. Fluid and inotrope administration in the acute phase, and guideline-directed medical therapy for heart failure, thereafter, led to full recovery.
Introduction
Takotsubo cardiomyopathy (TTCM) is an often reversible injury of the myocardium caused by catecholamine excess, usually after a stressor.1 The first case series were described by Tsuchihashi et al. three decades ago, and it was named due to the resemblance of the left ventricle (LV) in ventriculography to a Japanese pot used to catch octopuses. It usually affects post-menopausal women and has a typical form involving the mid and apical segments of the LV (apical ballooning), and atypical forms (mid, basal and focal TTCM).2 Mid-ventricular TTCM is a rare variant that affects the mid-segments of the LV, and accounts for 14.6% of patients presenting with this syndrome.3
Case presentation
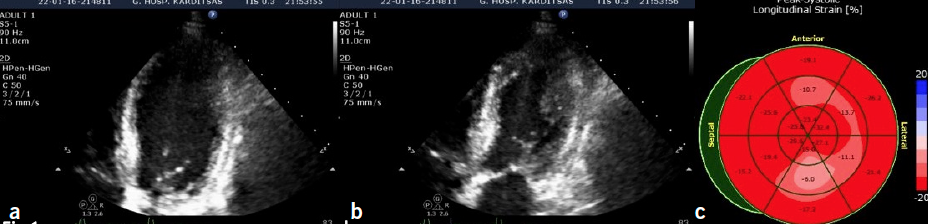
A 71-year-old woman that underwent total hip arthroplasty the day before, after falling from a standing position, presented with hypotension (80/45 mmHg), tachypnoea, and signs of poor peripheral perfusion. The patient’s only pertinent medication included irbesartan 150 mg daily for arterial hypertension. Cardiology consultation was requested. Upon cardiac auscultation an S3 was audible in the left precordium along with bi-basal lung crackles. A transthoracic echocardiogram (TTE) was deemed necessary in order to unveil the mechanism behind the cardiovascular haemodynamic collapse in a previously well patient with no history of heart failure (figure 1).
Figure 1. 2D echocardiographic still images of the apical four-chamber view of the heart focusing on the left ventricle (LV) in: diastole (a) and systole (b) showing akinesis (no systolic thickening) of the mid-diaphragmatic and mid-lateral segments of the LV; (c) mildly abnormal global longitudinal strain, especially of the mid-ventricular segments
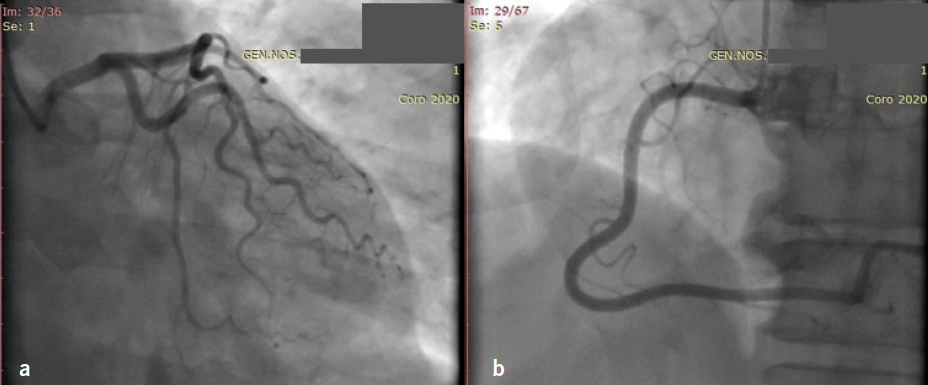
The patient was then transferred to the cardiac care unit with fluid boluses and inotropic support, as no LV outflow obstruction was noted. When haemodynamic stability was ensured, guideline-directed medical therapy commenced, and the patient underwent coronary angiography due to the, presumed new, LV wall motion abnormalities and low troponin rise (figure 2). Surprisingly, the patient’s electrocardiogram (ECG) remained grossly normal throughout her hospital stay.
Figure 2. Basic views on coronary angiography: right anterior oblique (RAO) caudal view of the left coronary system without significant stenoses (a) and RAO cranial view of the right coronary system without stenoses (b)
Keeping in mind the patient’s demographics, physical and emotional stressors, echocardiographic appearance of the LV, low troponin rise and absence of severe coronary artery disease, mid-ventricular TTCM was the final diagnosis, with a probability of 98.8% according to the International Takotsubo registry score (InterTAK score).
The patient was asymptomatic and well, and discharged on carvedilol and ramipril. A re-examination was scheduled three weeks later. A new echocardiogram was performed showing complete resolution of the regional wall motion abnormalities (figure 3).
Figure 3. 2D echocardiographic still images of the apical four-chamber view of the heart focusing on the LV: in diastole (a) and systole (b) showing normal systolic thickening of the previously affected segments; (c) normal global longitudinal strain
Discussion
TTCM is known to typically manifest in elderly female patients presenting with chest pain or new-onset heart failure after an emotional stressor. The majority of patients in many series are postmenopausal women between the ages of 60 and 80 years, although younger women and men are also affected.4 The advanced age and risk factors for coronary artery disease in these patients make the diagnosis difficult. One of the main characteristics of this syndrome are the physical or emotional triggers that preclude the presentation of symptoms, making TTCM widely known as ‘broken-heart syndrome’.5,6 Typical anginal chest pain, dyspnoea, syncope or arrythmias are the main symptoms of TTCM,7 which, if combined with ST-segment elevation or depression on the ECG and a, usually modest, rise in cardiac troponin, make the diagnosis of acute coronary syndrome very likely at first glance.8 New-onset ischaemic ECG changes are reported to be present in about two-thirds of affected patients in many registries,8 while Tsuchihashi et al. reported ST elevation in 90%.7 Those findings often lead to activation of the cath-lab and, traditionally, epicardial artery stenoses <50% are needed for the diagnosis of TTCM, according to the well-known Mayo clinic criteria.9 However, this remains an area of debate because significant atherosclerotic disease does not exlude TTCM, and those patients may be misdiagnosed as having a myocardial infarction. Acute therapy for TTCM consists of beta-blockade when outflow tract obstruction is present. Use of inotropes are an area of conflict, given the deleterious effects of catecholamines on the heart muscle of those affected. Oral medication is no different to that used for heart failure, and is usually stopped when LV function is restored, due to the low incidence of reccurence.10
Key messages
This case illustrates the significance of echocardiography in the assessment of patients with acute haemodynamic instability
In the echocardiographic examination of a severely ill patient, the cardiologist must have a high suspicion for cardiac manifestations of systemic disease, such as catecholamine surge in Takotsubo
Regional wall motion abnormalities, especially if not in the distribution of an epicardial vessel, should arouse suspicion of Takotsubo cardiomyopathy
Conflicts of interest
None declared.
Funding
None.
Patient consent
Written consent for publication was obtained from the patient.
2. Ghadri JR, Wittstein IS, Prasad A et al. International expert consensus document on Takotsubo syndrome (part I): clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J 2018;39:2032–46. https://doi.org/10.1093/eurheartj/ehy076
3. Templin C, Ghadri JR, Diekmann J et al. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. N Engl J Med 2015;373:929–38. https://doi.org/10.1056/NEJMoa1406761
4. Pilgrim TM, Wyss TR. Takotsubo cardiomyopathy or transient left ventricular apical ballooning syndrome: a systematic review. Int J Cardiol 2008;124:283–92. https://doi.org/10.1016/j.ijcard.2007.07.002
5. Sharkey SW, Windenburg DC, Lesser JR et al. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol 2010;55:333–41. https://doi.org/10.1016/j.jacc.2009.08.057
6. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J 2006;27:1523–9. https://doi.org/10.1093/eurheartj/ehl032
7. Tsuchihashi K, Ueshima K, Uchida T et al. Angina pectoris-myocardial infarction investigations in Japan. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol 2001;38:11–18. https://doi.org/10.1016/S0735-1097(01)01316-X
8. Dib C, Asirvatham S, Elesber A, Rihal C, Friedman P, Prasad A. Clinical correlates and prognostic significance of electrocardiographic abnormalities in apical ballooning syndrome (Takotsubo/stress-induced cardiomyopathy). Am Heart J 2009;157:933–8. https://doi.org/10.1016/j.ahj.2008.12.023
Disparities in cardiovascular morbidity and mortality are among the leading health and social care concerns in the UK. The disruption of the COVID-19 pandemic to health services has further placed cardiovascular care and the respective patient communities at the sharp end, not least in exacerbating existing health inequalities across service interfaces and patients’ health outcomes. While the pandemic engenders unprecedented constraints within established cardiology services, it conduces to a unique opportunity to embrace novel transformative approaches within the way we deliver patient care in maintaining best practices during and beyond the crisis. As the first step in navigating toward the ‘new norm’, a clear recognition of the challenges inherent in cardiovascular health inequalities is critical, primarily in preventing the widening of extant inequalities as cardiology workforces continue to build back fairer. We may consider the challenges through the lens of health services’ diverse facets, including the aspects of universality, interconnectivity, adaptability, sustainability, and preventability. This article explores the pertinent challenges and provides a focused narration concerning potential measures to foster equitable and resilient cardiology services that are patient centred in the post-pandemic landscape.
Introduction
Dr Cong Ying Hey
Disparities in cardiovascular (CV) morbidity and mortality are among the major health and social care concerns in our modern society. In the UK, people living in the most deprived areas are four times more likely to die prematurely from CV disease (CVD) than those living in the least deprived areas.1 To address the disparities in CV outcomes, it is imperative to recognise the presence of inequalities at different interfaces of cardiology services. This article, therefore, aims to provide a focused discussion concerning potential measures to reduce health inequalities in cardiology through the lens of the challenges: “Universality, interconnectivity, adaptability, sustainability, and preventability.”
Universality
Despite universal healthcare services and standardised treatment guidelines in the UK, the morbidity and mortality outcomes across different ethnic populations during the pandemic demonstrated that all is not equal with regard to universality and clinical outcomes. Recently, an article in Lancet Public Health investigated the England-wide general practice patient survey, which reported substantial ethnic inequalities in health-related quality of life among older adults, particularly in women. Further, there was a greater likelihood in patients from ethnic minority populations to report a poorer experience than their white British counterparts in using health services.2 Such observation portrays that universal access to healthcare services may not necessarily lead to the same clinical outcomes in all patient groups. This leads us to consider the concept of proportionate universalism (delivering universal services while providing targeted support for vulnerable groups) as a model of care to address health inequalities.
Given the complex interplay between coronavirus severity, CVD and the broader determinants of health, there has never been a better time in exploring novel care delivery in cardiology that capitalises on the concept described above as we emerge from the pandemic. In the multi-ethnic British population, cardiology services need to culturally tailor local facilities to reduce health inequities across communities that are disproportionately affected by the CVD burden. Linguistic barriers can often be an impediment to patients’ understanding of disease-related information and treatment adherence as a result, especially when some cardiology terminologies can be technical and confusing for patients with limited English proficiency.3 This can be compounded by systems-level barriers, including, but not limited to, short allocated clinic time for such patients. To ensure equitable cardiology care, we need to optimise language concordance between physician and patient, ease of access to professional interpreting facilities and availability of translated documents, such as patient information sheets and culturally adapted healthy living handbooks. Some of the systems-level barriers can be anticipated and reduced by implementing proactive screening for such cohorts in advance of clinic allocation. In addition, several studies have attested to the positive impact of workforce diversity on the inclusiveness in population health management.4,5 As such, we need to foster a diverse and inclusive cardiology workforce in pursuit of equitable healthcare for the under-served.
Interconnectivity
Interconnectivity in healthcare empowers a culture of shared decision-making via the accessible and actionable clinical information exchange between the public, public health, health services, voluntary sector partners and local authorities. The unprecedented pandemic has showcased the potential of trans-sectoral collaborative ventures in addressing health inequalities in a short period. To take on health inequalities in CV care, strategic partnerships with local and voluntary sector partners, public health and the Office for National Statistics, could offer a platform to investigate:
The geographical pattern of the post-pandemic backlog in CV services
Understand the public health behaviours across different socio-economic backgrounds
Track outcomes of disease management with the help of the census data.
The data can then be utilised to guide targeted health campaigns and funding distribution to supplement affected CV services.
Not limiting to organisational partnerships, a close collaboration with patients, both clinically and in research, is equally paramount in addressing disparities in service experience and clinical outcomes. Community-based studies have previously been reported and shown to be effective in addressing gaps in patients’ needs and wants.6-8 Therefore, CV research needs to foster a culture of patient and public involvement in clinical research activities. Direct public/patient advocate involvement in the research planning and execution can improve the likelihood of developing culturally pertinent research questions and sustainable strategies in tackling multi-faceted CV health inequalities.
Adaptability and sustainability
The adoption of telemedicine and remote home monitoring have allowed cardiology services to maintain the standard of care during the pandemic. Remote care, however, is not a new concept in CV care, in that its role was prominently studied in the chronic heart failure (CHF) cohort since the 2000s. While a meta-analysis of remote care in the CHF cohort concluded promising treatment effects, the heterogeneity of individual studies reminds us to be judicious in selecting patient groups for remote care medicine.9 A blanket adoption of virtual care may exacerbate the intrinsic health inequality gap in disadvantaged cohorts with high CV risk and low digital literacy.10,11 To prevent the exacerbation of such inequalities, cardiology services need to refine triage system models as they look to maintain the uptake of virtual care beyond the pandemic. Cardiology specialists and their local foundation trusts need to establish a safe and equitable framework to risk-stratify patients according to their digital literacy, the status of CV diagnosis and the severity of CVD burden in long-term service planning. Besides service refinement, cardiology societies should proactively embed the topic of digital health equity in their educational curriculum to support current physicians, as well as the next generation of trainees.
Preventability
Fundamental to achieving preventable disparities in CVD outcomes, the cardiology workforce needs to give equal consideration to optimising patient access to guideline-directed treatments. A prominent example is the significant regional variation in the uptake of prognostically beneficial guideline-directed medical therapy (GDMT) and access to cardiac rehabilitation programmes (CR)12 in CHF cohorts. Leaders in cardiology services should support junior trainees and encourage local quality improvement projects to optimise patient access to GDMT in CHF cohorts. CHF can be complex in its disease process and management for many patients, as such, inequitable access to CR can further widen inequalities in this cohort, with high mortality burden. Low uptake of CR in CHF cohorts can be attributed to several reasons, including missed opportunity, lack of regional access and inadequate recognition of CR as evidence-based management. For instance, there remains no CR for CHF cohorts across Norfolk in 2021. Cardiology leaders from such areas need to proactively advocate for the cause and secure funding to establish the service for the local population. If centre-based options are limited, cardiology centres can now consider an evidence-based CR for use at home to cater for patients who may be limited by geographic barriers.13
Conclusion
Although the pandemic has exacerbated inherent health inequalities, it brought about a unique opportunity to embrace novel transformative approaches in CV services. Redefining the concept of health equality in the post-pandemic UK has never been more pertinent. Multi-sectorial stakeholders and the wider health services need to proactively reach out to our patients to create equitable and resilient CV services that are patient centred as we continue to build back better and fairer.
Key messages
Disparities in cardiovascular morbidity and mortality remain significant despite universal access to healthcare services in the UK
The concept of proportionate universalism may serve as an alternative care delivery model for addressing health inequalities within cardiology services
Shared decision-making and partnerships with patients remain paramount in cultivating relevant and sustainable solutions for inequalities within cardiovascular care after the pandemic
Cardiology services should refine remote care frameworks to safeguard equitable access to best practices, while preventing the exacerbation of intrinsic gaps in the disadvantaged cohorts, who are already burdened with high cardiovascular risk and modest digital literacy
Conflicts of interest
None declared.
Funding
None.
Editors’ note
This article was the prize-winning essay in the National Essay Prize 2021 of the British Junior Cardiologists’ Association (BJCA).
2. Watkinson RE, Sutton M, Turner AJ. Ethnic inequalities in health-related quality of life among older adults in England: secondary analysis of a national cross-sectional survey. Lancet Public Health 2021;6:e145–e154. https://doi.org/10.1016/S2468-2667(20)30287-5
3. Herbert BM, Johnson AE, Paasche-Orlow MK, Brooks MM, Magnani JW. Disparities in reporting a history of cardiovascular disease among adults with limited English proficiency and angina. JAMA Netw Open 2021;4:e2138780. https://doi.org/10.1001/jamanetworkopen.2021.38780
4. Johnson AE, Birru Talabi M, Bonifacino E et al. Considerations for racial diversity in the cardiology workforce in the United States of America. J Am Coll Cardiol 2021;77:1934–7. https://doi.org/10.1016/j.jacc.2021.02.043
6. Ekezie W, Czyznikowska BM, Rohit S et al. The views of ethnic minority and vulnerable communities towards participation in COVID-19 vaccine trials. J Public Health (Oxf) 2020;43:e258–e260. https://doi.org/10.1093/pubmed/fdaa196
7. Khunti K, Routen A, Patel K et al. Focused action is required to protect ethnic minority populations from COVID-19 post-lockdown. Br J Gen Pract 2020;71:37–40. https://doi.org/10.3399/bjgp21X714581
8. Highton PJ, Hadjiconstantinou M, Schreder S, Seidu S, Davies M, Khunti K. COVID-19, ethnicity and cardiometabolic disease self-management in UK primary care. Diabetes Metab Syndr 2020;14:2241–3. https://doi.org/10.1016/j.dsx.2020.11.013
9. Inglis SC, Clark RA, Dierckx R, Prieto-Merino D, Cleland JGF. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Syst Rev 2015;2015:CD007228. https://doi.org/10.1002/14651858.CD007228.pub3
10. Neves AL, van Dael J, O’Brien N et al. Use and impact of virtual primary care on quality and safety: the public’s perspectives during the COVID-19 pandemic. J Telemed Telecare 2021:[online first]. https://doi.org/10.1177/1357633X211066235
11. Vas V, North S, Rua T et al. Delivering outpatient virtual clinics during the COVID-19 pandemic: early evaluation of clinicians’ experiences. BMJ Open Qual 2022;11:e001313. https://doi.org/10.1136/bmjoq-2020-001313
13. Dalal HM, Taylor RS, Jolly K et al. The effects and costs of home-based rehabilitation for heart failure with reduced ejection fraction: the REACH-HF multicentre randomized controlled trial. Eur J Prev Cardiol 2018;26:262–72. https://doi.org/10.1177/2047487318806358
Nutrition is underrepresented in the medical curriculum; this has always been the case, but recently there has been a focus on trying to change this. A ‘call for action’ by the independent organisation Nutritank CIC and the Nutrition Implementation Coalition has led the way for this. New recommendations for curriculum changes have been proposed, but no mandatory changes are yet in place.
Current situation
The General Medical Council (GMC) publishes guidelines on the competencies expected from UK medical schools, however, there are no set quantities or qualities for nutrition education. Interestingly, a recent study found that 95% of participants (medical students and doctors) believed that doctors play an important role in providing nutrition care, yet 70% reported receiving fewer than two hours of nutrition teaching while at medical school.1 Lack of knowledge has been reported as the most common barrier to providing nutrition advice for patients, but a comprehensive review is required to really understand where the gaps in nutrition education lie.2 The NHS Long Term Plan states that “we will ensure nutrition has a greater place in professional education training”.3 Across many organisations there is an appreciation that nutrition is fundamental for good health, however, this has not been translated into meaningful practices in the education of medical professionals.
Consequences
Malnourished patients see their GP twice as often, have three times the number of hospital admissions and stay in hospital on average around three days longer than non-malnourished patients.4 National Institute for Health and Care Excellence (NICE) guidelines state that “all healthcare professionals who are directly involved in patient care should receive education, and training, relevant to their post, on the importance of providing adequate nutrition”.5 However, we know from the research that the education is not adequate for doctors.
Notably, tobacco smoking has reduced in the UK, however, globally, poor diet and sedentary lifestyle are now the leading modifiable risk factors associated with morbidity and mortality.6 NICE recommends that lifestyle interventions, including dietary modification, are first-line in the prevention and management of common chronic medical conditions, including type 2 diabetes (T2DM), cardiovascular disease, heart failure, and hypertension.7 When trained healthcare professionals advise patients on diet modification this can lead to sustained improved health outcomes in T2DM patients.8
Dietitians and registered nutritionists are paramount in championing this cause. However, with only 9,000 registered dietitians in the UK, they can only be a small voice in the vast healthcare system, and they are also sparsely distributed across the National Health Service (NHS).9 Nonetheless, integrating dietitians into multi-disciplinary teams and on the wards will help to increase the profile of nutrition in healthcare. It is not about educating doctors to the level in which dietitians are then replaced, but as doctors are commonly the gatekeepers of the NHS, it is essential to educate them to recognise when further support is required and generate appropriate onward referrals.
Who are Nutritank?
Nutritank is a non-profit organisation and innovative information hub for food, nutrition and lifestyle medicine. It is on a mission – promoting the need for greater education in medical training around nutrition and lifestyle medicine. It functions as a network and think-tank. Nutritank was created in 2017 by two medical students (now junior doctors) Dr Iain Broadley and Dr Ally Jaffee. They were both frustrated by the lack of nutrition in their curriculum while studying at Bristol University, and decided to take action.
Nutritank now has 22 medical school branches with over 1,500 medical students and junior doctors signed up to support the cause. They aim to provide their network with evidence-based information on nutrition and lifestyle to enable them to advise patients on making sustainable self-care behaviour changes to improve their health. The branches have organised over 300 education events and contributed to two annual conferences in collaboration with the Royal Society of Medicine. Additionally, Nutritank’s junior doctor network aims to implement nutrition and lifestyle medicine education within hospital core training, the food environment, grand rounds and input to research projects such as quality improvement projects (QIPs) and audits. In 2018, Nutritank worked alongside TV chef Jamie Oliver and his campaign team in creating the social media campaign #nutrition4medics, this was instrumental in adding a clause to the NHS Long Term Plan on a commitment to increasing nutrition education for healthcare professionals. Nutritank’s overall mission is to equip healthcare professionals with the knowledge and communicative tools to help reverse the trend in rising diet and lifestyle related chronic disease. Anecdotally, Nutritank medical students and doctors have witnessed that the most common ‘lifestyle’ advice clinicians provide patients with is to ‘lose weight,’ largely, this can be unhelpful, sometimes harmful, and unlikely leads to beneficial behaviour change or improved outcomes. Significantly, patients experience the majority of their weight stigma from medical doctors.10 A more effective approach to clinical management could be self-care activation incorporating advice on nutrition, movement, sleep and stress management, alongside pharmacology. If clinically important, asking permission if the patient is willing to discuss their weight, and if they are motivated to lose weight, the clinician could provide helpful resources on managing their metabolic health or referral to specialist services.
How is Nutritank trying to get more nutrition into medical schools?
In October 2021, after three years of development, the new Association for Nutrition (AfN) Undergraduate Curriculum in Nutrition for Medical Doctors was launched.11 Nutritank was proud to work alongside a wide-ranging inter-professional working group (including medical schools, royal colleges, medical and nutrition organisations, professionals and students). The new curriculum is designed to be incorporated within the core curriculum of undergraduate medical students. Integrating nutrition into current modules, rather than a standalone module, allows students to appreciate the relevance of nutrition and its application across different clinical specialties. This is not mandatory for medical schools to implement, therefore, Nutritank is using its local branches to encourage and advocate this to their individual medical school faculty.
Since its publication, Nutritank has been working alongside the Nutrition Implementation Coalition in organising workshops with faculty members from UK medical schools to advise on how to implement further nutrition teaching into their curricula. To date, 11 medical schools have now sought advice on how to implement further nutrition teaching into their curricula, which is positive progress.
Vision for the future
Nutritank are already driving changes to the curriculum and policy, and hope to be at the forefront of conversations and action around the intersection between food, lifestyle and health, and ultimately become the go-to hub for information and community engagement.
While the new curriculum indicates real progress and potential in pushing nutrition to the forefront, is this going to be enough to get the systemic changes needed? Focusing on medical students is an effective first step, but we need to see top-down changes throughout clinical specialties. Nutrition interventions can prevent chronic disease and manage chronic disease once onset, across the entire life-course. Therefore, it is time for action and to provide medical professionals with sufficient education to address this issue. This needs to start in medical schools, but we should not neglect the need for postgraduate nutrition education throughout medical professionals’ careers.
We call upon the UK cardiology profession to join our campaign for greater nutrition education within medical training for both undergraduate and postgraduate doctors. Being from such a well-regarded profession, your added voice to this educational movement will help innovate medical training, clinical practice and ultimately benefit patients’ health outcomes and society as a whole.
Conflicts of interest
IB and AJ work voluntarily for Nutritank CIC. They are employed by their respective NHS hospital trusts. RW is employed part-time by Nutritank CIC.
Funding
Nutritank CIC has recently received a grant from the AIM Foundation Grant Fund.
2. Xie JY, Abramovich N, Burridge J, Jaffee A, Broadley I. Nutrition education in core medical curricula: a call to action from tomorrow’s doctors. Future Healthc J 2021;8:19–21. https://doi.org/10.7861/fhj.2020-0207
4. Guest JF, Panca M, Baeyens JP et al. Health economic impact of managing patients following a community-based diagnosis of malnutrition in the UK. Clin Nutr 2011;30:422–9. https://doi.org/10.1016/j.clnu.2011.02.002
5. National Institute for Health and Care Excellence. Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. CG32. London: NICE, 2006. Available from: https://www.nice.org.uk/guidance/cg32
7. National Institute for Health and Care Excellence. Type 2 diabetes in adults: management. NG28. London: NICE, 2015. Available from: https://www.nice.org.uk/guidance/ng28
8. Taylor R, Ramachandran A, Yancy WS Jr, Forouhi NG. Nutritional basis of type 2 diabetes remission. BMJ 2021;374:n1449. Erratum in: BMJ 2021;374:n1752. https://doi.org/10.1136/bmj.n1449
This audit compared the management of patients with heart failure with reduced ejection fraction (HFrEF) admitted to a district general hospital (DGH) during comparative eight month periods before and during the COVID-19 pandemic. The periods studied were from 1 February 2019 to 30 September 2019 and between the same dates in 2020. We investigated differences in mortality and patient characteristics (age, gender and new or prior diagnosis). For patients who survived to discharge and who were not referred to palliative care, we also investigated whether there were differences in rates of echocardiography and prescription of angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists and beta blockers.
We found that the number of cases was lower during the pandemic and there was a lower mortality rate that was not statistically significant. There was a higher proportion of new cases (odds ratio [OR] 2.21, 95% confidence interval [CI] 1.24 to 3.94, p=0.008) and of female patients (OR 2.03, 95%CI 1.14 to 3.61, p=0.019). For survivors, there was a non-significant decrease in prescription rates for ACE inhibitors and angiotensin II receptor antagonists (81.6% vs. 71.4%, p=0.137) that was not seen for beta blockers. The length of stay was increased and there was also an increase in the interval between admission and echocardiography in patients who were newly diagnosed. Regardless of time period, the time before echocardiography was significantly associated with length of stay.
Background
Heart failure is a common cause of hospital admission in the UK, and the leading cause of admission in people aged 65 years or older.1 Treatment with angiotensin-converting enzyme (ACE) inhibitors (ACEi), angiotensin-receptor blockers (ARB) and beta blockers are associated with reduced morbidity and mortality, while prompt imaging with a transthoracic echocardiogram (TTE) enables earlier diagnosis and appropriate management.2 It has been recommended that a TTE should be done within 48 hours of admission.
Coronavirus disease 2019 (COVID-19) was declared as a global pandemic on 11 March 2020,3 and the UK had 491,805 cases by 30 September 2020.4 The pandemic had a huge impact on NHS services. The British Cardiovascular Society (BCS) and British Society for Heart Failure (BSH) released a statement with regards to prioritisation of heart failure service provision during the pandemic.5 In brief, there was a focus on avoiding face-to-face consultations and increased use of community-based teams. The aim was to reduce pressure on likely stretched hospital services and to keep vulnerable patients away from potential sources of infection. TTE guidelines during the pandemic likely led to inpatient delays because of factors such as the requirement to wear personal protective equipment and to decontaminate equipment between cases.6 For all admitted patients, there was a requirement for COVID-19 testing, and the wait for such results often meant a delay for other investigations. We did a comparative audit of heart failure with reduced ejection fraction (HFrEF) patients admitted to hospital before and during the pandemic period. The aim of the audit was to assess the overall effect of the pandemic on inpatient diagnosis and treatment.
Method
We selected patients from the National Heart Failure Audit (NHFA)7 who had heart failure with reduced ejection fraction ≤40% and were admitted to St. Richard’s Hospital, Chichester with one of the following ICD-10 (International classification of diseases version 10) codes in the first diagnostic position – I11.0, I25.5, I42.0, I42.9, I50.0, I50.1 and I50.9. The pre-pandemic cohort consisted of all patients admitted between 1 February 2019 and 30 September 2019, while the pandemic cohort was admitted between 1 February 2020 and 30 September 2020.
We compared age, gender, mortality and diagnosis (new case or prior diagnosis). For patients who survived and who were not referred to palliative care, we compared the use of ACEi/ARB and beta blockers. We considered that drugs had been prescribed even if they were subsequently withdrawn. We compared hospital length of stay and the interval between admission and inpatient TTE. We assessed a multiple linear regression model where length of stay was the dependent variable and interval before TTE, pandemic period, age and diagnosis were independent variables.
All statistics were performed using JMP®, version 16.2.0, SAS Institute Inc. The Anderson-Darling test was used to assess whether data had a normal distribution. Data that were not normally distributed were summarised as median and interquartile range (IQR) and compared with the Wilcoxon rank-sum test. Results were presented as mean and standard deviation (SD) for continuous variables and as number (%) for categorical variables. Categorical variables were compared with Fisher’s exact test.
Results
There was a 36.8% reduction in cases during the pandemic (table 1) with an increase in the proportion of patients with a diagnosis of new HFrEF and who were female. The mortality rate was lower, but this was not statistically significant. Mortality was associated with age, and for all patients, the odds ratio (OR) for those aged over 80 years was 4.07 (95% confidence interval [CI] 1.64 to 10.10, p=0.003). There was also a non-significant reduction in patients on ACEi/ARB that was not seen for those on beta blockers. The length of stay was increased.
Table 1. Number of patients during pre-pandemic and pandemic periods
Pre-pandemic period
Pandemic period
OR (95%CI)
p
All patients
Number
125
79
Median age (IQR), years
80.9 (70.3 to 86.9)
80.9 (73.1 to 88.4
0.409
Mean age (SD), years
78.0 (12.0)
79.5 (11.9)
Female, n (%)
42 (33.6%)
40 (50.6%)
2.03 (1.14 to 3.61)
0.019
Died, n (%)
23 (18.4%)
9 (11.4%)
0.57 (0.25 to 1.31)
0.236
New HFrEF, n (%)
41 (32.8%)
41 (51.9%)
2.21 (1.24 to 3.94)
0.008
Survivors
Number
98
70
Median age (IQR), years
78.3 (68.1 to 85.5)
80.3 (72.9 to 86.1)
0.202
Mean age (SD), years
76.0 (12.1)
78.5 (11.5)
Female, n (%)
33 (33.7%)
37 (52.9%)
2.21 (1.18 to 4.14)
0.017
New HFrEF, n (%)
29 (29.6%)
37 (61.7%)
2.67 (1.41 to 5.05)
0.004
ACEi/ARB, n (%)
80 (81.6%)
50 (71.4%)
0.56 (0.27 to 1.17)
0.137
Beta blocker, n (%)
88 (89.8%)
63 (90%)
1.02 (0.37 to 2.83)
1.000
Median length of stay (IQR), days
5 (3 to 11)
10 (5.75 to 16)
0.001
Mean length of stay (SD), days
8.73 (10.47)
12.01 (9.18)
Inpatient TTE, n (%)
New HFrEF
27 (93.1%)
36 (97.3%)
2.67 (0.23 to 30.95)
0.578
Known HFrEF
27 (39.1%)
14 (42.4%)
1.15 (0.49 to 2.66)
0.830
Inpatient TTE within 2 days, n (%)
New HFrEF
22 (75.9%)
19 (51.4%)
0.36 (0.12 to 0.98)
0.073
Known HFrEF
15 (21.7%)
7 (21.2%)
1.03 (0.38 to 2.84)
1.000
TTE within previous 12 months or inpatient TTE, n (%)
87 (88.8%)
67 (95.7%)
2.82 (0.76 to 10.52)
0.157
Days between admission and TTE – median (IQR)
New HFrEF
1 (0 to 2)
2 (1 to 4)
0.003
Known HFrEF
2 (1 to 3)
4 (1 to 7.25)
0.426
Key: ACEi = angiotensin-converting enzyme inhibitor; ARB = angiotensin-receptor blocker; CI = confidence interval; HFrEF = heart failure with reduced ejection fraction; IQR = interquartile range; OR = odds ratio; SD = standard deviation; TTE = transthoracic echocardiography
Patients with a new diagnosis were more likely to have inpatient TTE, while a significant proportion with known HFrEF had had a TTE within the preceding 12 months. The time before inpatient TTE was shorter for new cases and this increased during the pandemic.
In our multiple-regression model, only the time interval between admission and TTE was significantly associated with the length of stay (parameter estimate 0.93, SD 0.24, p=0.0002, R2=0.16).
Discussion
Our main findings were that the pandemic was associated with a lower number of cases and a higher proportion of patients who had a new diagnosis of HFrEF and who were female. There was reduced prescribing of ACEi and ARB that was not seen for beta blockers. The length of stay was increased, and for new cases, the interval before inpatient TTE was increased. Length of stay was strongly associated with interval before inpatient TTE, regardless of period.
The 36.8% drop in cases is consistent with reports that hospital admissions fell significantly during the first wave of the pandemic,8 and patients may have been less likely to seek help from medical services. It is possible that some known HFrEF cases were managed by the community heart failure nurses to avoid admission. An increase in new cases may partly be due to COVID-19 infection. However, myocarditis related to vaccination is rare, affecting mainly young males,9 and one study with case validation reported an incidence of COVID associated myocarditis of only 2.4 per 1,000 hospitalisations, with male preponderance.10 We are uncertain why the proportion of female patients was increased.
At the beginning of the pandemic, there were concerns that the use of ACEi and ARB may be associated with higher rates for COVID-19 infection and adverse outcomes. This may explain the non-significant reduction in their use. Current data suggest that use of these drugs is actually associated with reduced risk.11
Locally, a likely important contributory factor for the longer wait for TTE for new cases was a requirement that all patients had to be tested for COVID-19, with samples being sent off-site, and COVID-19 negative patients were scanned first.
Conclusion
A lower prescription rate for ACEi/ARB is most likely a historical problem, whereas longer waits for TTE could be an exacerbation of a pre-existing problem. It seems that shortening waits is important as it contributes to length of stay. There continues to be an emphasis on investigating and managing patients in the community, and collecting data on these patients will give a more comprehensive understanding of the management of heart failure.
Conflicts of Interest
None declared.
Funding
None.
Study approval
Permission for this audit was given by the hospital audit committee with no requirement to seek ethical approval.
Key messages
The proportion of new cases of heart failure with reduced ejection fraction (HFrEF) was increased during the COVID-19 pandemic. The proportion of female patients was also increased
The proportion of patients on angiotensin-converting enzyme inhibitors (ACEi) and angiotensin-receptor blockers (ARB) was lower during the pandemic, with no change for those on beta blockers
During the pandemic, the length of stay was prolonged and, for patients with a new diagnosis of HFrEF, the interval between admission and echocardiography was increased. Regardless of time period, the waiting time for an echo was strongly associated with length of stay
References
1. National Institute for Health and Care Excellence. Acute heart failure: diagnosis and management. CG187. London: NICE, 2021. Available from: https://www.nice.org.uk/guidance/cg187
8. Reschen ME, Bowen J, Novak A et al. Impact of the COVID-19 pandemic on emergency department attendances and acute medical admissions. BMC Emerg Med 2021;21:143. https://doi.org/10.1186/s12873-021-00529-w
10. Ammirati E, Lupi L, Palazzini M et al. Prevalence, characteristics, and outcomes of COVID-19 associated acute myocarditis. Circulation 2022;145:1123–39. https://doi.org/10.1161/CIRCULATIONAHA.121.056817
11. Hippisley-Cox J, Young D, Coupland C et al. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: cohort study including 8.3 million people. Heart 2020;106:1503–11. https://doi.org/10.1136/heartjnl-2020-317393
SARS-CoV-2 is an emerging cause of viral myocarditis that generates multiple complications, such as dilated cardiomyopathy. We describe a young, obese male patient with severe myocardial involvement by the SARS-CoV-2 virus, who presented with chest pain, elevated cardiac enzymes, non-specific electrocardiographic findings, echocardiogram with evidence of dilated heart disease with reduced ejection fraction, and subsequent verification using magnetic resonance imaging (MRI). The results of the cardiac MRI were typical of viral myocarditis. The patient did not respond to a short course of systemic steroids and the standard management for heart failure, had multiple re-admissions, and, unfortunately, died.
Introduction
Since its appearance in December 2019 in Wuhan (Hubei, China), more than 300 million people worldwide have been infected with the SARS-CoV-2 virus1 (which generates multi-systemic involvement and is an emerging cause of myocardial compromise). This article presents an illustrative case of dilated cardiomyopathy as a complication of viral myocarditis due to SARS-CoV-2.
The patient was a 36-year-old man with a body mass index (BMI) of 35 kg/m2. The patient presented at the hospital with general malaise, fever, nausea and dyspnoea; vital signs included normal blood pressure, tachycardia, tachypnoea, desaturation and bi-basilar crackles. Laboratory testing showed leukocytosis with neutrophilia, mild elevation of transaminases, positive troponin I and elevated inflammatory markers (table 1). Thoracic computed tomography (CT) scan showed areas with limited extension of ground-glass opacification towards the lung apices. The patient was confirmed positive for SARS-CoV-2 by reverse transcriptase polymerase chain reaction (RT-PCR) and, therefore, an immunomodulatory management with dexamethasone dosage of 6 mg every 24 hours for 10 days was given, expecting improvement.
During his hospital stay, he presented with thoracic pain, electrocardiographic (ECG) findings of sinus tachycardia, premature ventricular complexes, left atrial abnormality and positive troponin I. Transthoracic echocardiogram revealed dilated cardiomyopathy with a left ventricular (LV) ejection fraction of 20%. Chagas serology was negative. The management of heart failure was improved with dapagliflozin, sacubitril/valsartan, spironolactone and metoprolol succinate.
The stress myocardial perfusion imaging showed a moderated ischaemia (approximately 15%) in the inferolateral and inferior wall. The coronary angiography revealed epicardial arteries without lesions.
Figure 1. Cardiac resonance image in four-chamber view in which marked dilation is observed in both atria and ventriclesFigure 2. Cardiac magnetic resonance image in short-axis view at the level of the ventricles in ‘black blood’ sequence in which significant oedema of the lateral and inferolateral meso and epicardial walls is observedFigure 3. Cardiac magnetic resonance image in short-axis view, with late-phase gadolinium, showing enhancement that compromises the meso and epicardium of the interventricular septum, lateral, inferolateral, and inferior walls
Finally, cardiac magnetic resonance imaging (MRI) showed severe dilation of the four chambers with severe biventricular dysfunction, presence of oedema, late gadolinium enhancement (LGE), extensive fibrosis of the meso and lateral epicardium of inferolateral and inferior wall, tricuspid regurgitation and dilation of the pulmonary artery (figures 1, 2 and 3), which confirmed the diagnosis of myocarditis. After the initial consultation the patient had multiple hospitalisations, was monitored over time and treated for heart failure. Unfortunately, the patient developed decompensated heart failure and died.
Discussion
Viral myocarditis has been identified as one of the most frequent causes of dilated cardiomyopathy. Historically, it has been linked to several viral strains, with SARS-CoV-2 currently the most common global cause of myocardial dysfunction. This virus enters the cells through the angiotensin-converting 2 enzyme (ACE 2) receptor generating an inflammatory response with injury to multiple systems, including the cardiovascular system.2
Most patients are asymptomatic; however, respiratory symptomatology is the most common pathology (as described in this patient). The risk of complications is more significant in those with pre-existing cardiovascular diseases; in this patient, obesity was found as a comorbidity.3
SARS-CoV-2 infection, manifesting in acute cardiac injury, has been well documented. The mechanism of such injury may be multi-factorial, including ischaemia, toxicity of viral injury stress, inflammation, microvascular dysfunction, or atheromatous plaque rupture. It has been documented that arrhythmias, such as sustained ventricular tachycardia and ventricular fibrillation, heart failure, myocardial dysfunction, severe cases of cardiogenic shock and fulminant myocarditis; with a reduction in left ventricular systolic function (in the absence of obstructive coronary disease) produce a high rate of mortality in these patients.4-6
Echocardiographic findings are non-specific for the diagnosis of myocarditis, although they may demonstrate regional or global dysfunction and, occasionally, pericardial effusion. The standard test for the diagnosis of myocarditis is an endomyocardial biopsy, which is considered an invasive test. However, a non-invasive test that allows the diagnosis of acute myocarditis is a cardiac MRI. In this case, the patient was given a cardiac MRI which revealed significant oedema and delayed gadolinium enhancement, showing an extensive area of fibrosis, all of which is consistent with myocarditis.7,8
Conclusion
The case illustrated in this article represents an unusual case of dilated cardiomyopathy due to viral myocarditis triggered by SARS-CoV-2 with a fatal outcome. Emphasis is placed on the findings and utility of the cardiac MRI in the diagnosis of the described pathology.
Conflicts of interest
None declared.
Funding
None.
Patient consent
For the publication of this case, we have the endorsement of the ethics committee of San José Hospital Universitario de Popayán, Colombia, instead of the consent of the relatives because contact with them was not achieved after patient’s death.
Disclaimer
The data and opinions expressed in the article are those of the authors and not an official position of the institution.
2. Atri D, Siddiqi HK, Lang JP, Nauffal V, Morrow DA, Bohula EA. COVID-19 for the cardiologist: basic virology, epidemiology, cardiac manifestations, and potential therapeutic strategies. JACC Basic Transl Sci 2020;5:518–36. https://doi.org/10.1016/j.jacbts.2020.04.002
3. Huang C, Wang Y, Li X et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395:497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
4. Soumya RS, Unni TG, Raghu KG. Impact of COVID-19 on the cardiovascular system: a review of available reports. Cardiovasc Drugs Ther 2021;35:411–25. https://doi.org/10.1007/s10557-020-07073-y
5. Guo T, Fan Y, Chen M et al. Cardiovascular Implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol 2020;5:811–18. https://doi.org/10.1001/jamacardio.2020.1017
6. Bernal-Torres W, Herrera-Escandón Á, Hurtado-Rivera M, Plata-Mosquera CA. COVID-19 fulminant myocarditis: a case report. Eur Heart J Case Rep 2020;4(FI1):1–6. https://doi.org/10.1093/ehjcr/ytaa212
7. Friedrich MG, Sechtem U, Schulz-Menger J et al. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009;53:1475–87. https://doi.org/10.1016/j.jacc.2009.02.007
8. Abdelazeem B, Borcheni M, Alnaimat S, Mallikethi-Reddy S, Sulaiman A. Persistent cardiac magnetic resonance imaging features of myocarditis detected months after COVID-19 infection. Cureus 2021;13:e14250. https://doi.org/10.7759/cureus.14250
Dr Tiffany Kemp
Cardiology (Devices and Heart Failure) ST7
Worthing Hospital, University Hospitals Sussex [email protected]
First published online 30th August 2022
One of the most difficult challenges presented to healthcare professionals during the COVID-19 pandemic has been maintaining standards of care in non-COVID related chronic illness. Many members of our heart failure multidisciplinary (MDT) teams were redeployed and, while many have returned to their original positions, the impact of COVID-19 will be felt for years. It was, therefore, particularly poignant that in its 25th year, the British Society of Heart Failure (BSH) hosted a two-day immersive programme focusing on the heart failure MDT. Held at the Golden Jubilee Conference Hotel in Glasgow, on 12th May 2022, the meeting gave heart failure enthusiasts the opportunity to ‘reconnect in the real world’. Dr Tiffany Kemp reports on the highlights of the meeting.
President of the BSH, Professor Roy Gardner opened the meeting asking where his ‘mute button’ had gone to silence the excited chatter after two years of predominantly virtual meetings. He recognised the room was full of professionals with a passion for caring for patients with heart failure, and encouraged everyone to share their knowledge and continue to promote heart failure awareness.
Why do people develop heart failure?
The first session explored some of the many reasons patients can develop heart failure. Dr Caroline Coates (University of Glasgow) highlighted the importance of taking a thorough family history to identify an inherited cardiac condition (ICC) as a cause. While genetic testing is very important, the results are not black and white and, therefore, it is vital to take a holistic approach when making a diagnosis of an ICC. She explored the impact of a genetic diagnosis, including the likelihood of improvement in cardiac function with treatment1, decision making regarding early implantation of cardiac devices, and the consequences of the result on family members. It is vital that ICC services are joined up with heart failure services in order to provide best care for patients. With the huge rise in the consumer market for genetic testing, the importance of this relationship will only increase.
Arrhythmias
Dr Derek Connelly (Golden Jubilee National Hospital, Glasgow) explored the relationship between arrhythmia and heart failure. With new onset acute fibrillation doubling the risk of hospitalisation and mortality in those with heart failure with reduced ejection fraction (HFrEF)2, heart failure specialists must consider which patients may benefit from ablation, and Dr Connelly noted the European Society of Cardiology (ESC) guidelines on management of arrhythmia in heart failure will soon be updated.
Valve disease
Valvular disease can cause a highly abnormal haemodynamic state, and Dr Alison Duncan (Royal Brompton Hospital, London) took the meeting on a whistle-stop tour on how different valvular pathologies can contribute to heart failure. She discussed how specialists should strongly consider structural intervention for aortic stenosis even if already in heart failure with HFrEF, and that the impending new guidelines will support this providing the patient has a prognosis of over 12 months. Newer options such as MitraClip™ (transcatheter mitral valve repair) and transcatheter edge-to-edge mitral valve repair (TMVR) have been shown to improve symptoms and survival for selected patients with HFrEF and severe secondary mitral regurgitation despite optimal medical therapy.3
Ischaemia
Coronary artery disease is often forgotten when treating heart failure, particularly in younger patients, according to Professor Mark Petrie (University of Glasgow). The STICH (Surgical Treatment for Ischemic Heart Failure) study is the only trial focusing on patients with both severe left ventricular systolic impairment (left ventricular ejection fraction <35%) and severe coronary artery disease. While the results can be complex to interpret, the study shows benefit in revascularisation surgery at 10 years; therefore young patients are likely to benefit more. We do not yet have firm evidence regarding percutaneous coronary intervention (PCI) in HFrEF patients, as many trials exclude ejection fraction; but trials are ongoing.
Managing emergencies
There are several scenarios that will scare most heart failure specialists and session two aimed to educate the meeting in order to reduce this fear.
Cardiogenic shock
Dr Robyn Smith (Golden Jubilee National Hospital, Glasgow) presented a pragmatic approach in managing patients with cardiogenic shock, starting with ‘ABC and beyond.’ There are four main causes of shock (distributive, hypovolaemic, cardiogenic and obstructive), but the cause is not always clear. With a logical approach and remembering the key five variables (cardiac output, heart rate and rhythm, preload, afterload and contractility), it is possible to implement supportive measures, including medications targeted towards the problem area.
Left ventricular assist device
Dr Jane Cannon (Golden Jubilee National Hospital, Glasgow) explained how the left ventricular assist device (LVAD) is surgically implanted into the left ventricular apex and then pulls blood from the left ventricle into the motorised Impella® and then out into the ascending aorta. Patients with an LVAD may not have a palpable pulse or recordable blood pressure using standard methods, so it is important to assess the patient clinically and also perform a Doppler blood pressure reading where possible. The most frequent issues in LVAD patients include infection of the drive line, thrombus in the motor and bleeding due to ‘warfarinisation’. Clinicians are advised to contact the ventricular advice device (VAD) centre early should patients present elsewhere with any VAD issues.
Adult congenital heart disease
Dr Niki Walker (University of Glasgow) is an adult congenital heart disease (ACHD) expert and she highlighted the importance in asking patients about their own baseline parameters, including oxygen saturations. ACHD is an increasing specialty, particularly in the number of patients surviving to adulthood with complex congenital conditions. Those hospitalised with heart failure and ACHD currently have a one-year mortality after hospital admission, and thus an admission should be seen as an opportunity to improve care. The main precipitants for decompensated heart failure in this group are arrhythmia, infection, endocrine abnormalities, and structural change. Young adults with ACHD may present more insidiously with heart failure and so specialists need to look for it carefully, and escalate to ACHD and advanced heart failure services where necessary.
Pregnancy
Approximately 80–90% of those who die in pregnancy of cardiac disease had no known cardiac diagnosis prior to this devastating event. Dr Lorna Swann (Golden Jubilee National Hospital, Glasgow) showed the two peaks in morbidity and mortality are at 23–24 weeks of gestation and at delivery. This earlier peak is particularly challenging as it is the grey zone for foetal viability and, therefore, can make decision making about management even more difficult. Symptoms of heart failure and normal pregnancy can overlap, but symptoms such as chronic cough, orthopnoea, atrial fibrillation, cyanosis, diastolic murmur and loud systolic murmur should trigger high suspicion for heart failure. It is important to involve all the right specialists early when managing a pregnant patient with cardiac disease, including intensive care, obstetricians and the labour ward, neonatologists, the cardio-obstetric team, the transplant and mechanical circulatory support team, and pharmacy.
Breakout sessions
Devices
Dr Parin Shah (Golden Jubilee National Hospital, Glasgow), Dr Phil Matthews (Golden Jubilee National Hospital, Glasgow) and Dr Zaheer Yousef (University Hospital of Wales) worked alongside device industry experts to run a workshop on cardiac devices, including a practical approach to device decision making, as well as implantation, monitoring and deactivation. It is important to consider each patient individually when deciding if device implantation is appropriate, and which device they should receive. Additionally, for those heart failure patients who receive a defibrillator implant, it is imperative to start talking about device deactivation early, prior to the stage where a patient may deteriorate. As heart failure becomes more advanced the probability of sudden cardiac death (SCD) from cardiac arrhythmia decreases, and thus it may be appropriate to deactivate the defibrillator. MERIT-HF (Metoprolol CR/XL randomised intervention trial in congestive heart failure)showed that 64% of those who died with New York Heart Association (NYHA) class II died of sudden cardiac death versus 27% of those with NYHA IV.
Imaging
This breakout session focused on the use of imaging in heart failure and was run by Dr Alison Duncan (The Royal Brompton, London) and Dr Lisa Anderson (St George’s Hospital, London). Constrictive and restrictive cardiomyopathy can be challenging to differentiate, but echocardiography can be used alongside clinical signs to make a diagnosis non-invasively. While echocardiography is the first-line investigation in suspected heart failure, cardiac magnetic resonance imaging can supply additional information about the aetiology and prognosis of heart failure, due to the ability to characterise myocardial tissue and to provide simultaneous imaging of the thorax.
Psychological support and safety
Support for patients and their families
Dr Annabel Farnood (University of Glasgow) spoke about heart failure online health information and specifically about what patients with heart failure want to know and how this can be provided. She highlighted online forums that can be used as a source of support for patients with heart failure, but that sometimes can contain misleading information. It is, therefore, important that patients are given the opportunity to discuss information they have found online. The audience benefited from hearing from two service users, Mr Laurence Humphreys-Davies and Mrs Wendy Panton who reported the benefits of a multidisciplinary team and the need for signposting to support groups.
Psychotropic drugs
A presentation from principal pharmacist Dr Siobhan Gee (South London and Maudsley NHS Foundation Trust) about psychotropic drugs in patients with comorbid physical illness was particularly well received. About one in five patients with heart failure meet the diagnostic criteria for depression, so it is vital that heart failure specialists screen carefully for depression. For patients with heart failure and depression alone, sertraline is recommended as the first-line treatment, however in certain patients, sertraline and other serotonin receptor inhibitors can increase the risk of bleeding, particularly in those on dual antiplatelets due to inhibiting platelet aggregation. Other psychotropic medications such as mirtazapine and agomelatine may need to be considered.
HFpEF in the real world
Professor John McMurray (University of Glasgow) gave an impassioned overview of heart failure with preserved ejection fraction (HFpEF) evidence and the challenges in its management. Recent studies, such as EMPEROR-Preserved (Empagliflozin outcome trial in patients with cohort failure with preserved ejection fraction) give some hope for evidence, although the updated ESC guidelines for HFpEF management were published prior to EMPEROR-Preserved reporting and thus sodium-glucose co-transporter-2 (SGLT-2) inhibitors were only given a class IIa recommendation by the ESC, which means they may be considered. Diuretic therapy in HFpEF remains an IC recommendation, which means the benefits appear to outweigh the risks. Professor McMurray also advised that based on the TRED-HF (Therapy withdrawal in recovered dilated cardiomyopathy – heart failure) trial, prognostic heart failure medication should be continued in those who recover their ejection fraction, and the DELIVER (Dapagliflozin evaluation to improve the lives of patients with preserved ejection fraction heart failure) trial will also report on this. The FINEARTS-HF (Finerenone in heart failure patients) study is currently recruiting and will look at the impact of adding finereone in those with LVEF >40%.
Infiltrative cardiomyopathy
Storage and infiltrative cardiomyopathies can cause HFpEF. Dr Joanna Simpson (University of Glasgow) described the diverse group of diseases that can have overlapping phenotypes, although most initially cause increased left ventricular wall thickness with preserved ejection fraction, but can then relate in dilatation and impaired function. A diagnosis of amyloid is often difficult, and patients can be known to several specialties without a unifying cause being identified until the late stages of the condition. Fabry’s disease is an uncommon, but treatable cause of cardiomyopathy, and must be considered in unexplained left ventricular hypertrophy.
Multidisciplinary team and service models
Dr Sue Piper (King’s College, London) noted heart failure is a multi-morbid complex condition, with a mean patient age of 77 years. This means heart failure specialists must consider each patient holistically, and work closely with the MDT, including other specialties. The patient should be placed at the heart of the multidisciplinary team, particularly now patient care is becoming more complex and in a wider range of settings. The National Institute of Clinical Excellence (NICE) and the ESC both give IA levels of support that a heart failure MDT improves care for the patient, as it is backed up with data from multiple randomised clinical trials. Furthermore, the National Confidential Enquiry into Patient Outcome and Death report, Failure to function, Getting it right first time4 report both state the need for an effective heart failure multidisciplinary team.
Nurse-led medication initiation
Miss Norma Caples (Waterford, Ireland) presented her groundbreaking nurse-led medication initialisation service, where she starts patients on the four pillars of heart failure therapy (angiotensin-converting enzyme [ACE] inhibitors, angiotensin receptor neprilysin inhibitor [ARNI], beta blocker, mineralocorticoid receptor antagonists [MRA], SGLT-2 inhibitors) within a four-week period.This is based on Packer and McMurray’s paper recommended rapid sequencing5. She managed to establish 90% of her patients on all four pillars within four weeks, and found the average BNP fell from 2230 before to 1398 afterwards. Additionally, many patients reported an improvement in functional class, and her re-admission rate fell from 13% locally (25% nationally) to 3.7%.
Advanced heart failure assessment
Dr Jonathan Dalzell (Scottish National Advanced Heart Failure Service) talked about features that he would encourage clinicians to see as a prompt for referral, including inotrope dependency, NYHA III-IV, end organ dysfunction, reducing ejection fraction, defibrillator therapy, escalating diuretic need, and hypotension. Mechanical circulatory support (MCS) such as LVAD can be used as a bridge to transplant or bridge to candidacy for transplant in those who have other issues that need to be addressed prior to being eligible for transplant listing. Advanced heart failure services can provide a full workup for MCS and/or transplant and patients should be referred early for consideration.
Cardiotoxicity
Dr Ninian Lang (University of Glasgow) told the meeting that cancer survival has doubled since the 1970s, and therefore cardiac consequences of successful cancer treatment must be identified. The two main types of cardiotoxicity are divided into myocardial damage, which is usually reversible (type 1) and irreversible myocardial injury (type 2). Immune checkpoint inhibitor usage is rapidly increasing for malignancy and associated myocarditis should be treated by stopping the agent and giving five days of IV methylprednisolone.
Much-needed opportunity
This meeting was a much-needed opportunity to assemble face to face and to re-establish links between heart failure specialists. The multidisciplinary focus enabled dynamic and diverse discussion between attendees, and new connections and plans have been made that will further benefit the wider heart failure specialist community, and thus improve the care for heart failure patients.
References
1. Escobar-Lopez et al. (2021); ‘Association of genetic variants with outcomes in patients with non-ischaemic dilated cardiomyopathy’ Journal of the American College of Cardiology 2021 Oct 26;78(17):1682-1699
2. Mogensen UM, Jhund PS, Abraham WT, Desai AS, Dickstein K, Packer M, Rouleau JL, Solomon SD, Swedberg K, Zile MR, et al. (2017) ‘Type of atrial fibrillation and outcomes in patients with heart failure and reduced ejection fraction.’ Journal of the American College Cardiology. 2017;70(20):2490–2500
3. Stone G, Lindfield K, Abraham W et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med 2018;379:2307–18. https://doi.org/10.1056/NEJMoa1806640
5. Packer and Murray (2021) ‘Rapid evidence based sequencing of foundational drugs for heart failure and a reduced ejection fraction.’ Euorpean Journal of Heart Failure 2021;23(6):882-894
Authors: John P Sheppard, Suvasini Lakshmanan, Seth J Lichtenstein, Matthew J Budoff, Sion K Roy
John P Sheppard
Resident Physician
Department of Internal Medicine, Yale New Haven Hospital, 20 York Street, New Haven, Connecticut, 06510, USA
Suvasini Lakshmanan Physician Fellow
Division of Cardiovascular Medicine, University of Iowa Hospitals & Clinics, 200 Hawkins Drive, Iowa City, Iowa, 52242, USA
Seth J Lichtenstein Physician Fellow
Matthew J Budoff Professor of Medicine, David Geffen School of Medicine at UCLA, Investigator, Lundquist Institute, and Program Director and Director of Cardiac CT
Sion K Roy Associate Program Director and Director of Inpatient Cardiac CT
Harbor-UCLA Medical Center, 1000 West Carson Street, Torrance, California, 90502, USA
Correspondence to: Professor M J Budoff, Lundquist Institute, 1124 West Carson Street, Torrance, CA 90502, USA ([email protected])
First published online 19th July 2022
The coronary artery calcium (CAC) score is a marker of advanced coronary atherosclerosis. Numerous prospective cohorts have validated CAC as an independent marker that improves prognostication in atherosclerotic cardiovascular disease (ASCVD) beyond traditional risk factors. Accordingly, CAC is now incorporated into international cardiovascular guidelines as a tool to inform medical decision-making. Particular interest concerns the significance of zero CAC score (CAC=0). While many studies report CAC=0 to virtually exclude obstructive coronary artery disease (CAD), non-negligible rates of obstructive CAD despite CAC=0 are reported in certain populations. Overall, the current literature supports the power of zero CAC as a strong downward risk classifier in older patients, whose CAD burden predominantly involves calcified plaque. However, with their higher burden of non-calcified plaque, CAC=0 does not reliably exclude obstructive CAD in patients under 40 years. Illustrating this point, we present a cautionary case of a 31-year-old patient found to have severe two-vessel CAD despite CAC=0. We highlight the value of coronary computed tomography angiography (CCTA) as the gold-standard non-invasive imaging modality when the diagnosis of obstructive CAD is in question.
Introduction
Since its inception by Agatston and Janowitz in 1990, coronary artery calcium (CAC) scoring has blossomed from a novel imaging tool to an internationally accepted biomarker of cardiovascular risk included in current preventive atherosclerotic cardiovascular disease (ASCVD) guidelines.1-7 With its growing adoption, debate has emerged over the proper use of CAC scores in risk stratification, with controversy surrounding its role in excluding obstructive disease in symptomatic patients. Presently, we focus on the role of CAC in risk stratification for coronary heart disease (CHD). We review the overwhelming evidence validating CAC as a diagnostic and prognostic indicator in older adults but highlight its unreliability in younger patients under 40 years. We conclude with a cautionary case of a 31-year-old man admitted to our hospital who was found to have severe two-vessel coronary artery disease (CAD) despite zero CAC score.
Clinical overview
CAC as a CHD risk marker: the view from clinical end point studies
A nascent field of clinical imaging research investigating CAC grew throughout the 1990s,8 and culminated in the publication of foundational end point studies over the subsequent decade, establishing CAC’s utility as a marker of CHD (table 1).1,2,9-14 This work established, not only a proportional relationship between CAC score and incident CHD risk, but demonstrated CAC’s ability to improve CHD prediction independent of traditional risk factors, such as those included in the Framingham risk score (FRS).15 Greenland et al. found a 3–9% increase in 10-year coronary event risk beyond FRS criteria in individuals with CAC score over 300.14 The Rotterdam study found CAC scores improved prediction of incident CHD, ASCVD, and all-cause mortality beyond traditional risk factors among 1,795 asymptomatic adults over 70 years.10 The multi-ethnic study of atherosclerosis (MESA) extended these findings to a diverse cohort including Black (28%), Hispanic (22%), Chinese (12%), and White (39%) patients.13 MESA found an 18–39% increase in coronary event risk associated with each doubling of the CAC score, without major differences between ethnic groups.13 The Framingham Offspring study further validated these observations among 3,486 descendants of the original Framingham Heart Study.16 Again, CAC improved CHD prediction beyond Framingham risk factors, and correctly reclassified 85% of patients initially deemed at intermediate risk for CHD.16 Notable cohort studies establishing the value of CAC in ASCVD risk assessment are summarised in table 1.
Table 1. Notable studies establishing coronary artery calcium (CAC) as a biomarker in atherosclerotic cardiovascular disease (ASCVD) risk assessment
Study
Year
Country
Patients
Population
Age, years
Follow-up, years
Key findings
Rotterdam10
2005
Netherlands
1,795
Asymptomatic adults
71 (62–85)
3.3 ± 0.8
Adding CAC score to FRS improved CHD risk prediction
Prospective Army Coronary Calcium (PACC) Project9
2005
USA
2,000
Asymptomatic active-duty military
42.9 ± 2.8 (40–50)
3.0 ± 1.6 (1–6)
Hazard ratio increase of 4.3 for incident CAD per CAC tertile. CAC>0 in men associated with relative risk of 12 for
incident CAD
Cooper Clinic Cohort11
2005
USA
10,746
Asymptomatic adults
53.8 ± 9.9 (22–96)
3.5 ± 1.4
Dose-dependent relationship between CAC score and incident CHD surviving adjustment for traditional risk factors. CAC associated with CHD in both younger (<40) and older (>65) patients
St. Francis Heart Study12
2005
USA
4,903
Asymptomatic adults
59 ± 6
4.3
CAC predicted incident CAD better than FRS
MESA13
2008
USA
6,722
Asymptomatic multi-ethnic adults
62.2 ± 10.2 (45–84)
3.8
Doubling of CAC score associated with 15–35% increased risk of major coronary event and 14% relative increase in incident ASCVD
Heinz Nixdorf Recall Study19
2010
Germany
4,129
Asymptomatic adults without known CAD
59 ± 8 (45–75)
5.1 ± 0.3
Reclassifying intermediate risk patients based on FRS to low risk (if CAC<100) or high risk (if CAC≥400) categories improved prediction of incident coronary events
Dallas Heart Study69
2015
USA
2,084
Multi-ethnic adults without diabetes or CVD
44.4 ± 9.0
9.2 ± 1.3
CAC score improved CHD risk classification in younger adults
BioImage63
2016
USA
5,805
Adults without known CVD
68.9 ± 6.0
2.7
CAC-guided reclassification of CHD risk achieved a 22% improvement in specificity with no loss in sensitivity, driven by down-classifying risk among patients with CAC=0
Jackson Heart Study70
2016
USA
2,944
African-American adults
60 (21–64)
–
Adding CAC score to FRS improved prediction of CVD prevalence
Framingham Offspring16
2016
USA
3,486
Men ≥35 y, Women ≥40 y
50 ± 10
8
CAC improved prediction of incident CHD beyond traditional risk factors and accurately reclassified 2/3 of intermediate-risk patients
CARDIA71
2017
USA
5,115
Black and White younger adults
40.3 ± 3.6 (at study year 15)
12.5
CAC>0 associated with 5-fold increase in CHD incidence after adjustment for baseline risk. CVD risk factors in early adult life identified patients who later developed CAC
CAC Consortium72
2020
USA
66,636
Adults without known CHD
54 ± 11
12.5
CAC associated with CHD-attributable, CVD-attributable and all-cause mortality in a dose-dependent manner
CAC’s prognostic power to improve cardiovascular risk classification had major implications. Among end point studies, excellent cardiovascular outcomes were noted among patient subgroups with zero detectable CAC (CAC=0). Composite analysis of 16,106 asymptomatic patients with CAC=0 spanning 13 early observational studies found an annual coronary event rate of 0.027%, translating to a negative predictive value (NPV) of 98.1% over a mean follow-up of 4.7 years.17 Other major studies reported annual event rates as low as 0.06–0.16% in asymptomatic adults without detectable CAC.9,12,18-20 Initial results from the CAC Consortium cohort found yearly all-cause mortality of 0.87% among 19,898 asymptomatic middle-age adults with CAC=0,21 and risk of all-cause mortality doubled in patients with even the lowest levels of detectable calcium (i.e. CAC score of 1–10). At 12-year follow-up, incident CHD-attributable mortality among patients with CAC=0 was only 0.17%.22 Subsequent analysis of the MESA cohort found CAC=0 to be the greatest downward indicator of 10-year CHD and overall ASCVD risk among 13 other laboratory, imaging, and clinical risk markers.23
The profound differences observed in cardiovascular events among patients at either CAC score extreme allow for more accurate reclassification of ASCVD risk. This approach has been validated in numerous studies and is of relevance for patients estimated to be at intermediate, borderline, or even low ASCVD risk based on the pooled cohort equations (PCE).5 For instance, among 2,966 MESA patients who were eligible for statin therapy per the contemporary US cholesterol guidelines, 44% had zero detectable CAC.24,25 Among this subset, the observed 10-year ASCVD event rate was only 4.2 per 1,000 person-years, and CAC=0 reclassified 49% of statin-eligible patients to a 10-year ASCVD risk <5%, below the suggested risk threshold for statin therapy.24 Valenti et al. even proposed a 15-year ‘warranty period’ among asymptomatic adults with CAC=0 who were already at low or intermediate risk by PCE, noting a survival rate of 95.1% after mean follow-up of 14.6 years.26 Ultimately, this prognostic power has led to CAC’s inclusion in the current European guidelines as a cardiovascular risk modifier for asymptomatic patients.27 CAC scoring is also incorporated in the current US cholesterol guidelines as a class IIa recommendation to inform decision-making regarding statin therapy in adults over 40 years at borderline risk,4 although debate remains as to CAC’s role in de-escalating pharmacotherapy.28
CT-based screening for obstructive CAD in the symptomatic patient
While much effort has focused on CAC’s use in asymptomatic populations from a preventive health standpoint, its diagnostic applications in patients with chest pain has also garnered considerable interest. Safe and cost-effective risk stratification of chest pain presents a major challenge in both the ambulatory and emergency setting. Chest pain accounts for over six million emergency room visits in the US annually, with three million patients ultimately discharged with non-cardiac diagnoses.29
Excluding obstructive CAD is of cardinal interest in any patient with chest pain, and particularly in those whose presentation raises suspicion for acute coronary syndrome (ACS). From a non-invasive imaging standpoint, coronary computed tomography angiography (CCTA) is unrivaled in the diagnosis of CAD and grading of coronary luminal stenosis. The ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial reported sensitivity of 94–95% and NPV of 99% for excluding moderate (≥50%) or severe (≥70%) coronary stenosis with CCTA compared with angiography.30 Subsequent studies consistently demonstrated >90% sensitivity and superior performance with CCTA compared with myocardial perfusion imaging for detecting obstructive CAD.31,32
Increasingly, CCTA has been adopted by emergency departments (EDs) in the US to facilitate decision-making in patients undergoing ACS rule-out and, potentially, defer formal angiography. In the ROMICAT-II (Rule Out Myocardial Ischemia/Infarction Using Computer Assisted Tomography) trial, 1,000 patients presenting to the ED with acute chest pain and suspicion for ACS despite negative cardiac enzymes and lack of electrocardiogram (ECG) changes were randomised to undergo early CCTA or standard evaluation.33 Patients who underwent early CCTA benefited from shorter length of stay and higher rates of direct ED discharge, and no cases of ACS went undetected (i.e. no re-presentations at 72 hours post-discharge with subsequent positive work-up).
CCTA’s role as a screening tool for chest pain syndrome is also well-validated in the outpatient setting. The PROMISE (Prospective Multicenter Imaging Study for Evaluation of Chest Pain) trial randomised patients with stable chest pain and intermediate pre-test probability to undergo either CCTA or functional testing.34 Incidence of the primary end point (death, myocardial infarction, or hospitalisation for unstable angina) at follow-up was lower in patients who underwent CCTA (0.9%) versus functional testing (2.1%), despite lower prevalence of normal test results in the CCTA arm (33% vs. 78%). CCTA had superior discriminative ability in event prediction (c-statistic 0.72 vs. 0.64) and higher diagnostic yield compared with functional testing.35 Of note, the SCOT-HEART (Scottish COmputed Tomography of the HEART) trial randomised 4,146 outpatients with stable chest pain to either standard care or standard care plus early CCTA.36 Patients undergoing early CCTA had lower incidence of the composite end point of non-fatal myocardial infarction (MI) or CHD-attributable mortality at five-year follow-up. In terms of resource utilisation, there was no difference in five-year rates of angiography or revascularisation procedures, but patients referred to CCTA were more likely to be initiated on preventive or anti-anginal therapies.36
Many large-scale studies have examined the reliability of CAC in patients with chest pain, and have yielded favourable results. Meta-analysis across 32,477 symptomatic patients found that presence of CAC (CAC>0) was strongly associated with cardiovascular event risk, with pooled risk ratios (RR) of 6.1 for incident ASCVD and 7.9 for all-cause mortality.37Table 2 lists several well-powered cohort studies evaluating the reliability of CAC=0; many data are derived from studies of symptomatic patients undergoing both CAC scoring and CCTA.38 The CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: An InteRnational Multicenter Registry) study examined 10,037 symptomatic patients without known CAD who underwent both CAC scoring and CCTA, and found that CAC=0 excluded obstructive CAD with NPV of 96.5% for ≥50% stenosis and 98.6% for ≥70% stenosis.39 The PROMISE trial also included 4,209 patients who underwent CCTA and CAC scoring.34 Among 1,457 patients with CAC=0, only 22 patients (1.5%) had ≥50% stenosis and only seven (0.5%) had ≥70% stenosis on CCTA, corresponding to NPV of 98.5% and 99.5%, respectively.34
Table 2. Notable CAC=0 studies*
Study
Year
Country
Patients
Population
Age, years
Follow-up, years
Confirmatory imaging modality
Findings in CAC=0 patients
Knez68
2004
Germany
2,115
Symptomatic adults
62 ± 19
–
ICA
NPV of 100% (≥50% stenosis)
Rubinshtein54
2007
Israel
668
Symptomatic adults
54 ± 12
–
CCTA
NPV of 93% (≥50% stenosis)
CONFIRM39
2011
International
10,037
Symptomatic adults
57 ± 12
2.1
CCTA
NPV of 96.5% (≥50% stenosis), 98.6% (≥70% stenosis)
Chang58
2011
USA
1,049
Acute chest pain, suspected ACS
48.1
30 days
CCTA
NPV of 77.6% (>50% stenosis). 4/17 patients with CAC=0 and obstructive CAD had AMI. Age <50 70% more likely to have obstructive CAD with CAC=0
Kim73
2012
Korea
2,088
Symptomatic adults
58 ± 10
2.8
CCTA
NPV of 95.7% (≥50% stenosis)
Hulten74
2014
USA
1,145
Symptomatic adults
55 ± 12
2.4
CCTA
NPV of 99% (≥50% stenosis), 99.6% (≥70% stenosis)
Valenti26
2015
USA
9,715
Asymptomatic adults
53.4 ± 10.5
14.6
–
15-year warranty period against mortality in individuals at low-to-intermediate risk regardless of age or sex
PROMISE34
2017
North America
4,209
Symptomatic adults at intermediate risk
60.6 ± 8.2
2.2
CCTA
NPV of 98.5% (≥50% stenosis), 99.5% (≥70% stenosis)
Mittal48
2017
UK
2,730
Symptomatic adults
56.9 ± 12.4
5.2
CCTA
NPV of 99.5% (≥70% stenosis)
Walter Reed75
2018
USA
13,644
Active-duty military, no prior CVD
50 ± 8
9.4
–
NNT of 3,571 to prevent MACE with 10 years of statin therapy (NNT=12 for CAC>100)
Wang43
2019
UK
1,753
Symptomatic adults, suspected stable CAD
56.8 ± 12.0
2.2
CCTA
NPV of 98.1% (≥50% stenosis)
Mortensen60
2020
Denmark
23,759
Symptomatic adults
58
4.3
CCTA
CAC=0 prevalence of 93% (age <40) vs. 5%
(age >70). Likelihood ratio of ≥50% stenosis given CAC=0 of 0.68 (age <40) vs. 0.18 (age >70)
*Expanded from Gagel et al.2 Included studies are limited to cohorts including ≥500 patients. Key: ACS = acute coronary syndrome; AMI = acute myocardial infarction; CAC = coronary artery calcium; CAD = coronary artery disease; CCTA = coronary computed tomography angiography; CVD = cardiovascular disease; ICA = invasive coronary angiography; MACE = major adverse cardiovascular event; NNT = number needed to treat; NPV = negative predictive value
The CRESCENT (Calcium Imaging and Selective CT Angiography in Comparison to Functional Testing for Suspected Coronary Artery Disease) trial evaluated a tiered approach to anatomic testing among 350 patients with stable CAD.40 Patients randomised to the anatomic testing arm first underwent CAC scoring and proceeded to CCTA only if estimated pre-test probability for obstructive CAD was >70%, or if CAC was present on computed tomography (CT). Among 242 patients randomised to anatomic testing, 98 patients had CAC=0 and none sustained major adverse cardiovascular events (MACE) or required further testing after one year of follow-up.40 The tiered anatomic testing approach was associated with reduced need for further diagnostic testing, lower cumulative testing costs, and shorter time to final diagnosis relative to a functional testing-based strategy.38,40 Similar results were obtained in the CRESCENT-II trial, with zero of 45 patients with CAC=0 suffering MACE or subsequently diagnosed with obstructive disease at follow-up.38,41 Low rates of obstructive CAD among patients with CAC=0 were also found in post-hoc analysis of the SCOT-HEART trial,38,42 with only around 1% MACE incidence after five years of follow-up.42 Wang et al. reported outcomes in a prospective series of 1,753 symptomatic patients with stable CAD.43 CAC=0 achieved a NPV of 98.1% for excluding ≥50% stenosis on CCTA. At two-year follow-up, MACE incidence was only 0.6% (five patients) among 751 patients with CAC=0.43 Sixty-three patients (8.4%) with CAC=0 had subclinical non-calcified plaque on CCTA, but there was zero MACE incidence among this subgroup.43
A subset of studies focused specifically on the reliability of CAC for excluding ACS in the emergency setting. Early case series pointed to the promise of CAC=0, reporting sensitivity of 97–100% for excluding ACS in patients with chest pain.44-46 Bittner et al. reviewed 826 consecutive patients presenting to the ED with acute chest pain.38,47 Among 444 patients with CAC=0, rates of obstructive CAD were very low, with NPV of 99.5% for ≥50% stenosis and 99.8% for ≥70% stenosis;47 however, the exclusion of patients with positive initial cardiac enzymes reduced pre-test probability with an overall ACS rate of only 7.9%.47 Mittal et al. evaluated incidence of obstructive CAD in an observational ED cohort including 2,730 patients undergoing CCTA.48 Among the 52.5% of patients with CAC=0, NPV of 98.3% and 99.5% were achieved for excluding ≥50% or ≥70% stenosis, respectively.48 All 24 patients with ≥50% stenosis on CCTA underwent formal angiography, with flow-limiting stenoses ultimately found in only four patients. Patients with CAC=0 had an annual all-cause mortality of only 0.3%, with zero reported coronary events across over five years of mean follow-up.38,48 Furthermore, the presence of non-calcified plaque on subsequent imaging had no association with mortality among patients with CAC=0.48
While the accuracy of CAC score in predicting obstructive CAD is generally excellent, some studies have reported less favourable results. As noted in the CONFIRM study,39 other early reported rates of obstructive CAD were as high as 7–38% in patients with CAC=0, although these data originated from small retrospective case series.49-54 Even the CONFIRM authors concluded that CAC=0 did not reliably exclude CAD in their symptomatic cohort, given that 3.5% of this subgroup still had ≥50% stenosis on CCTA.39 A meta-analysis by Sarwar et al. found CAC=0 excluded obstructive disease (>50% stenosis) with pooled sensitivity of 98% and NPV of 93% across 18 studies of symptomatic patients undergoing CAC scoring and invasive angiography.55 While promising, such error rates preclude deferring CCTA if reasonable suspicion exists for underlying obstructive disease.
Value of CAC=0 across the lifespan
Discrepant results in the literature raise the question of whether zero CAC score is equally meaningful in all patients. The use of CAC=0 to down-classify obstructive CAD risk is debated, especially in younger symptomatic patients with pre-test risk factors for disease. Evidence increasingly points to age as a critical factor in interpreting CAC score. The biological rationale is intuitive: atherosclerosis progresses over decades,56,57 with intimal calcification occurring late in its course.58,59 Older adults with CAD have accumulated calcified plaque over many decades of life, explaining higher average CAC scores and higher prevalence of detectable CAC relative to younger patients.60 As CAC specifically detects calcified plaque, it is unsurprising that CAC=0 excludes clinical disease more accurately in older patients.
Relative to older patients, most coronary plaque in younger patients with CAD is non-calcified.61 This is supported by MESA and related studies that demonstrate the subsequent appearance and progression of CAC over years on serial CT, in a manner correlating with cardiovascular risk factors, in patients with CAC=0 on their baseline scan.62 As a fraction of total coronary plaque, non-calcified plaque is more prevalent in younger populations,63 particularly in patients presenting with ACS in the absence of stable CAD.64 Specific cardiovascular risk factors, including diabetes and hyperlipidaemia, are also linked with higher burden of non-calcified plaque and are critical to consider in younger patients.61,65,66
The importance of age in CAC score interpretation is supported by literature findings.67 An early prospective study by Knez et al. evaluated 2,115 symptomatic patients with chest pain referred for formal angiography (mean age 62 years). Among 326 patients with CAC=0, none had significant CAD defined as ≥50% luminal stenosis.68 Among 1,247 patients with any degree of angiographically confirmed stenosis, only eight had CAC=0 (0.6%), seven of whom were under age 45 years.68 While the rate of subclinical stenosis in symptomatic adults over age 45 years with CAC=0 was only ~0.05%, the rate in adults under 45 years was ~2-5%, up to 100-fold higher.68 In another notable study, Chang et al. reported a prospective series of 1,049 patients (median age 48 years) presenting to an ED with acute chest pain and suspicion for ACS. Obstructive CAD was found in 17 of 76 patients with CAC=0 (NPV=77.6%), four of whom suffered a cardiovascular event within 30 days.58 The authors found that patients under 50 years were 70% more likely to have obstructive CAD with CAC=0.58 Cademartiri and colleagues reported ≥50% stenosis in 14.6% of 279 patients selected on the basis of suspected CAD, despite CAC=0.49 Although these numbers were driven by high pre-test probability in terms of symptoms and risk profile (including known ischaemic changes on stress testing in many patients), it bears mention that mean age across this cohort was only 48 years. Akram et al. also published a series of 210 patients referred for CAC scoring and CCTA, and reported >70% stenosis in four of 49 (8.2%) symptomatic patients on CCTA, despite CAC=0; three of these four patients were under age 45 years.50
Recently, the age-dependent relationship between CAC scores and risk of obstructive CAD has been rigorously examined in a well-conducted study by Mortensen et al.60 Mortensen and colleagues examined data from 23,759 patients aged 18 years or older from the Western Denmark Heart Registry. Among 13,496 patients with CAC=0 (57%), 725 patients (5.7%) had obstructive CAD on CCTA, corresponding to an NPV of 94.3%. Prevalence of CAC=0, however, varied markedly with age. CAC=0 was observed in 93% (1,278 of 1,372) of patients under 40 years, compared with only 51% (11,493 of 22,387) of patients over 40 years. Younger patients with obstructive CAD were much more likely to have non-calcified plaque. Among patients with obstructive CAD, CAC=0 was observed in 58% (39/68) of patients <40 years compared with only 14% (686/4,975) of patients >40 years, and 5% (52/964) of patients >70 years. Moreover, the diagnostic value of CAC=0 in reclassifying obstructive CAD risk increased steadily with age. After adjusting for age, sex, smoking, diabetes, and symptom characteristics, the risk-adjusted diagnostic likelihood ratio of obstructive CAD for CAC=0 ranged from 0.68 (32% lower CAD likelihood) in patients aged 18–39 years down to 0.18 (82% lower CAD likelihood) for patients >70 years. These findings corroborate the existing literature and demonstrate the age-dependent value of a zero CAC score.
Illustrative case
A 31-year-old man presented to our hospital with intermittent left-sided chest pain and radiation to his left arm. Associated symptoms included shortness of breath and diaphoresis. He described experiencing similar symptoms in recent months. Medical history was pertinent for obesity, uncontrolled diabetes, and hypertension. Laboratory values revealed a glycosylated haemoglobin (HbA1c) of 14.1% and lipid profile significant for total cholesterol of 364 mg/dL, high-density lipoprotein (HDL) 24 mg/dL, and triglycerides of 1,146 mg/dL. ECG showed normal sinus rhythm without evidence of ischaemia, infarction, or hypertrophy. Echocardiogram was structurally normal, with normal ejection fraction and wall motion. Troponin I levels were intermediate (peak 0.24 ng/mL) and he was assessed as having intermediate-risk chest pain.
As part of a protocol at our hospital, patients with chest pain and an intermediate risk profile proceed directly to CCTA to exclude obstruction. The patient had a CAC score of zero (figure 1), but CCTA revealed severe two-vessel disease with total occlusion of the mid-left anterior descending (LAD) and proximal first obtuse marginal (OM1) arteries (figure 2). Coronary angiography confirmed complete mid-LAD occlusion with reconstituted distal flow supplied via right-to-left collaterals, and 80% proximal stenosis of the OM1. He underwent successful revascularisation with two-vessel coronary artery bypass grafting and was discharged in stable condition.
Figure 2. A. Axial CT angiography image demonstrating occlusions of the mid-left anterior descending (mLAD) and first obtuse marginal (OM1). B. Mid-LAD total occlusion in coronal view. C. OM1 occlusion in axial view
Conclusion
In this paper, we review the strong evidence supporting CAC as a diagnostic and prognostic marker of ASCVD. We consider the diagnostic implications of a zero CAC score, with attention to its age-dependent limitations. In older adults, CAC=0 is a validated biomarker portending low risk of cardiovascular events.55 However, as reflected in our illustrative case, CAC=0 does not reliably exclude obstructive CAD in younger patients, who are known to have a higher burden of non-calcified plaque. Here, CCTA is irreplaceable for guiding decision-making in both emergency and outpatient settings. When the diagnosis is in question, adults under 40 years with chest pain and an intermediate risk profile should proceed directly to CCTA. Future work will further expand our understanding of CAC scores across the demographic spectrum, facilitating optimal integration of this tool to best evaluate risk and guide interventions in the individual patient.
Key messages
The coronary artery calcium (CAC) score is a powerful, well-validated biomarker that reliably predicts risk burden in atherosclerotic cardiovascular disease
In older adults, CAC score of zero reliably down-stratifies risk of obstructive coronary artery disease (CAD)
In adults under 40 years, zero CAC score does not reliably exclude obstructive CAD due to higher prevalence of non-calcified plaque
Younger patients with chest pain and risk factors raising suspicion for CAD should proceed directly to coronary computed tomography angiography (CCTA)
Conflicts of Interest
MJB is a consultant for General Electric. JP, SL, SJL, SKR: none declared.
Funding
This work was supported by funding from the National Heart, Lung, and Blood Institute (NHLBI) of the United States National Institutes of Health (NIH) under award number NIHR01HL146666.
Patient consent
Informed patient consent was obtained for the clinical case included in this manuscript.
References
1. Nasir K, Cainzos-Achirica M. Role of coronary artery calcium score in the primary prevention of cardiovascular disease. BMJ 2021;373:n776. https://doi.org/10.1136/bmj.n776
3. Mach F, Baigent C, Catapano AL et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J 2019;41:111–88. https://doi.org/10.1093/eurheartj/ehz455
4. Grundy SM, Stone NJ, Bailey AL et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;139:e1082–e1143. https://doi.org/10.1161/CIR.0000000000000698
5. Arnett DK, Blumenthal RS, Albert MA et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;140:e596–e646. https://doi.org/10.1161/CIR.0000000000000725
6. Piepoli MF, Abreu A, Albus C et al. Update on cardiovascular prevention in clinical practice: a position paper of the European Association of Preventive Cardiology of the European Society of Cardiology. Eur J Prev Cardiol 2020;27:181–205. https://doi.org/10.1177/2047487319893035
7. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr., Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990;15:827–32. https://doi.org/10.1016/0735-1097(90)90282-T
8. Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc 1999;74:243–52. https://doi.org/10.4065/74.3.243
9. Taylor AJ, Bindeman J, Feuerstein I, Cao F, Brazaitis M, O’Malley PG. Coronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors: mean three-year outcomes in the Prospective Army Coronary Calcium (PACC) project. J Am Coll Cardiol 2005;46:807–14. https://doi.org/10.1016/j.jacc.2005.05.049
10. Vliegenthart R, Oudkerk M, Hofman A et al. Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation 2005;112:572–7. https://doi.org/10.1161/CIRCULATIONAHA.104.488916
11. LaMonte MJ, FitzGerald SJ, Church TS et al. Coronary artery calcium score and coronary heart disease events in a large cohort of asymptomatic men and women. Am J Epidemiol 2005;162:421–9. https://doi.org/10.1093/aje/kwi228
12. Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD. Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol 2005;46:158–65. https://doi.org/10.1016/j.jacc.2005.02.088
13. Detrano R, Guerci AD, Carr JJ et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med 2008;358:1336–45. https://doi.org/10.1056/NEJMoa072100
14. Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA 2004;291:210–15. https://doi.org/10.1001/jama.291.2.210
15. Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation 1998;97:1837–47. https://doi.org/10.1161/01.CIR.97.18.1837
16. Hoffmann U, Massaro JM, D’Agostino RB Sr., Kathiresan S, Fox CS, O’Donnell CJ. Cardiovascular event prediction and risk reclassification by coronary, aortic, and valvular calcification in the Framingham Heart Study. J Am Heart Assoc 2016;5:e003144. https://doi.org/10.1161/JAHA.115.003144
17. Shareghi S, Ahmadi N, Young E, Gopal A, Liu ST, Budoff MJ. Prognostic significance of zero coronary calcium scores on cardiac computed tomography. J Cardiovasc Comput Tomogr 2007;1:155–9. https://doi.org/10.1016/j.jcct.2007.10.001
18. Raggi P, Callister TQ, Cooil B et al. Identification of patients at increased risk of first unheralded acute myocardial infarction by electron-beam computed tomography. Circulation 2000;101:850–5. https://doi.org/10.1161/01.CIR.101.8.850
19. Erbel R, Mohlenkamp S, Moebus S et al. Coronary risk stratification, discrimination, and reclassification improvement based on quantification of subclinical coronary atherosclerosis: the Heinz Nixdorf Recall study. J Am Coll Cardiol 2010;56:1397–406. https://doi.org/10.1016/j.jacc.2010.06.030
20. Budoff MJ, Shaw LJ, Liu ST et al. Long-term prognosis associated with coronary calcification: observations from a registry of 25,253 patients. J Am Coll Cardiol 2007;49:1860–70. https://doi.org/10.1016/j.jacc.2006.10.079
21. Blaha M, Budoff MJ, Shaw LJ et al. Absence of coronary artery calcification and all-cause mortality. JACC Cardiovasc Imaging 2009;2:692–700. https://doi.org/10.1016/j.jcmg.2009.03.009
22. Blaha MJ, Cainzos-Achirica M, Dardari Z et al. All-cause and cause-specific mortality in individuals with zero and minimal coronary artery calcium: a long-term, competing risk analysis in the Coronary Artery Calcium Consortium. Atherosclerosis 2020;294:72–9. https://doi.org/10.1016/j.atherosclerosis.2019.11.008
23. Blaha MJ, Cainzos-Achirica M, Greenland P et al. Role of coronary artery calcium score of zero and other negative risk markers for cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 2016;133:849–58. https://doi.org/10.1161/CIRCULATIONAHA.115.018524
24. Nasir K, Bittencourt MS, Blaha MJ et al. Implications of coronary artery calcium testing among statin candidates according to American College of Cardiology/American Heart Association cholesterol management guidelines: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol 2015;66:1657–68. https://doi.org/10.1016/j.jacc.2015.07.066
25. Stone NJ, Robinson JG, Lichtenstein AH et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63(25 Pt B):2889–934. https://doi.org/10.1161/01.cir.0000437738.63853.7a
26. Valenti V, Hartaigh BO, Heo R et al. A 15-year warranty period for asymptomatic individuals without coronary artery calcium: a prospective follow-up of 9,715 individuals. JACC Cardiovasc Imaging 2015;8:900–09. https://doi.org/10.1016/j.jcmg.2015.01.025
27. Knuuti J, Wijns W, Saraste A et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020;41:407–77. https://doi.org/10.1093/eurheartj/ehz425
29. Fernandez-Friera L, Garcia-Alvarez A, Guzman G, Garcia MJ. Coronary CT and the coronary calcium score, the future of ED risk stratification? Curr Cardiol Rev 2012;8:86–97. https://doi.org/10.2174/157340312801784989
30. Budoff MJ, Dowe D, Jollis JG et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008;52:1724–32. https://doi.org/10.1016/j.jacc.2008.07.031
31. Neglia D, Rovai D, Caselli C et al. Detection of significant coronary artery disease by noninvasive anatomical and functional imaging. Circ Cardiovasc Imaging 2015;8:e002179. https://doi.org/10.1161/CIRCIMAGING.114.002179
32. Budoff MJ, Li D, Kazerooni EA, Thomas GS, Mieres JH, Shaw LJ. Diagnostic accuracy of noninvasive 64-row computed tomographic coronary angiography (CCTA) compared with myocardial perfusion imaging (MPI): the PICTURE study, a prospective multicenter trial. Acad Radiol 2017;24:22–9. https://doi.org/10.1016/j.acra.2016.09.008
33. Hoffmann U, Truong QA, Schoenfeld DA et al. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med 2012;367:299–308. https://doi.org/10.1056/NEJMoa1201161
34. Budoff MJ, Mayrhofer T, Ferencik M et al. Prognostic value of coronary artery calcium in the PROMISE study (Prospective Multicenter Imaging Study for Evaluation of Chest Pain). Circulation 2017;136:1993–2005. https://doi.org/10.1161/CIRCULATIONAHA.117.030578
35. Hoffmann U, Ferencik M, Udelson JE et al. Prognostic value of noninvasive cardiovascular testing in patients with stable chest pain: insights from the PROMISE trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain). Circulation 2017;135:2320–32. https://doi.org/10.1161/CIRCULATIONAHA.116.024360
36. Investigators S-H, Newby DE, Adamson PD et al. Coronary CT angiography and 5-year risk of myocardial infarction. N Engl J Med 2018;379:924–33. https://doi.org/10.1056/NEJMoa1805971
37. Abuzaid A, Saad M, Addoumieh A et al. Coronary artery calcium score and risk of cardiovascular events without established coronary artery disease: a systemic review and meta-analysis. Coron Artery Dis 2021;32:317–28. https://doi.org/10.1097/MCA.0000000000000974
38. Mahmood T, Shapiro MD. Coronary artery calcium testing in low-intermediate risk symptomatic patients with suspected coronary artery disease: an effective gatekeeper to further testing? PloS One 2020;15:e0240539. https://doi.org/10.1371/journal.pone.0240539
39. Villines TC, Hulten EA, Shaw LJ et al. Prevalence and severity of coronary artery disease and adverse events among symptomatic patients with coronary artery calcification scores of zero undergoing coronary computed tomography angiography: results from the CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) registry. J Am Coll Cardiol 2011;58:2533–40. https://doi.org/10.1016/j.jacc.2011.10.851
40. Lubbers M, Dedic A, Coenen A et al. Calcium imaging and selective computed tomography angiography in comparison to functional testing for suspected coronary artery disease: the multicentre, randomized CRESCENT trial. Eur Heart J 2016;37:1232–43. https://doi.org/10.1093/eurheartj/ehv700
41. Lubbers M, Coenen A, Kofflard M et al. Comprehensive cardiac CT with myocardial perfusion imaging versus functional testing in suspected coronary artery disease: the multicenter, randomized CRESCENT-II trial. JACC Cardiovasc Imaging 2018;11:1625–36. https://doi.org/10.1016/j.jcmg.2017.10.010
42. Williams MC, Moss AJ, Dweck M et al. Coronary artery plaque characteristics associated with adverse outcomes in the SCOT-HEART study. J Am Coll Cardiol 2019;73:291–301. https://doi.org/10.1016/j.jacc.2018.10.066
43. Wang X, Le EPV, Rajani NK et al. A zero coronary artery calcium score in patients with stable chest pain is associated with a good prognosis, despite risk of non-calcified plaques. Open Heart 2019;6:e000945. https://doi.org/10.1136/openhrt-2018-000945
44. Laudon DA, Behrenbeck TR, Wood CM et al. Computed tomographic coronary artery calcium assessment for evaluating chest pain in the emergency department: long-term outcome of a prospective blind study. Mayo Clin Proc 2010;85:314–22. https://doi.org/10.4065/mcp.2009.0620
45. McLaughlin VV, Balogh T, Rich S. Utility of electron beam computed tomography to stratify patients presenting to the emergency room with chest pain. Am J Cardiol 1999;84:327–8, A8. https://doi.org/10.1016/S0002-9149(99)00286-6
46. Georgiou D, Budoff MJ, Kaufer E, Kennedy JM, Lu B, Brundage BH. Screening patients with chest pain in the emergency department using electron beam tomography: a follow-up study. J Am Coll Cardiol 2001;38:105–10. https://doi.org/10.1016/S0735-1097(01)01364-X
47. Bittner DO, Takx RAP, Staziaki PV et al. Identification of coronary artery calcification can optimize risk stratification in patients with acute chest pain. Int J Cardiol 2017;249:473–8. https://doi.org/10.1016/j.ijcard.2017.06.119
48. Mittal TK, Pottle A, Nicol E et al. Prevalence of obstructive coronary artery disease and prognosis in patients with stable symptoms and a zero-coronary calcium score. Eur Heart J Cardiovasc Imaging 2017;18:922–9. https://doi.org/10.1093/ehjci/jex037
49. Cademartiri F, Maffei E, Palumbo A et al. Diagnostic accuracy of computed tomography coronary angiography in patients with a zero calcium score. Eur Radiol 2010;20:81–7. https://doi.org/10.1007/s00330-009-1529-9
50. Akram K, O’Donnell RE, King S, Superko HR, Agatston A, Voros S. Influence of symptomatic status on the prevalence of obstructive coronary artery disease in patients with zero calcium score. Atherosclerosis 2009;203:533–7. https://doi.org/10.1016/j.atherosclerosis.2008.07.008
51. Gottlieb I, Miller JM, Arbab-Zadeh A et al. The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography. J Am Coll Cardiol 2010;55:627–34. https://doi.org/10.1016/j.jacc.2009.07.072
52. Haberl R, Tittus J, Bohme E et al. Multislice spiral computed tomographic angiography of coronary arteries in patients with suspected coronary artery disease: an effective filter before catheter angiography? Am Heart J 2005;149:1112–19. https://doi.org/10.1016/j.ahj.2005.02.048
53. Henneman MM, Schuijf JD, Pundziute G et al. Noninvasive evaluation with multislice computed tomography in suspected acute coronary syndrome: plaque morphology on multislice computed tomography versus coronary calcium score. J Am Coll Cardiol 2008;52:216–22. https://doi.org/10.1016/j.jacc.2008.04.012
54. Rubinshtein R, Gaspar T, Halon DA, Goldstein J, Peled N, Lewis BS. Prevalence and extent of obstructive coronary artery disease in patients with zero or low calcium score undergoing 64-slice cardiac multidetector computed tomography for evaluation of a chest pain syndrome. Am J Cardiol 2007;99:472–5. https://doi.org/10.1016/j.amjcard.2006.08.060
55. Sarwar A, Shaw LJ, Shapiro MD et al. Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging 2009;2:675–88. https://doi.org/10.1016/j.jcmg.2008.12.031
56. Dzaye O, Dardari ZA, Cainzos-Achirica M et al. Warranty period of a calcium score of zero: comprehensive analysis from MESA. JACC Cardiovasc Imaging 2021;14:990–1002. https://doi.org/10.1016/j.jcmg.2020.06.048
57. Otsuka F, Sakakura K, Yahagi K, Joner M, Virmani R. Has our understanding of calcification in human coronary atherosclerosis progressed? Arterioscler Thromb Vasc Biol 2014;34:724–36. https://doi.org/10.1161/ATVBAHA.113.302642
58. Chang AM, Le J, Matsuura AC, Litt HI, Hollander JE. Does coronary artery calcium scoring add to the predictive value of coronary computed tomography angiography for adverse cardiovascular events in low-risk chest pain patients? Acad Emerg Med 2011;18:1065–71. https://doi.org/10.1111/j.1553-2712.2011.01173.x
60. Mortensen MB, Gaur S, Frimmer A et al. Association of age with the diagnostic value of coronary artery calcium score for ruling out coronary stenosis in symptomatic patients. JAMA Cardiology 2022;7:36–44. https://doi.org/10.1001/jamacardio.2021.4406
61. Kral BG, Becker LC, Vaidya D et al. Noncalcified coronary plaque volumes in healthy people with a family history of early onset coronary artery disease. Circ Cardiovasc Imaging 2014;7:446–53. https://doi.org/10.1161/CIRCIMAGING.113.000980
62. Budoff MJ, Young R, Lopez VA et al. Progression of coronary calcium and incident coronary heart disease events: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol 2013;61:1231–9. https://doi.org/10.1016/j.jacc.2012.12.035
63. Mortensen MB, Fuster V, Muntendam P et al. A simple disease-guided approach to personalize ACC/AHA-recommended statin allocation in elderly people: the BioImage study. J Am Coll Cardiol 2016;68:881–91. https://doi.org/10.1016/j.jacc.2016.05.084
64. Pundziute G, Schuijf JD, Jukema JW et al. Evaluation of plaque characteristics in acute coronary syndromes: non-invasive assessment with multi-slice computed tomography and invasive evaluation with intravascular ultrasound radiofrequency data analysis. Eur Heart J 2008;29:2373–81. https://doi.org/10.1093/eurheartj/ehn356
65. Scholte AJ, Schuijf JD, Kharagjitsingh AV et al. Prevalence of coronary artery disease and plaque morphology assessed by multi-slice computed tomography coronary angiography and calcium scoring in asymptomatic patients with type 2 diabetes. Heart 2008;94:290–5. https://doi.org/10.1136/hrt.2007.121921
66. Santos RD. Calcified and noncalcified coronary plaques and atherosclerotic cardiovascular events in patients with severe hypercholesterolemia-moving forward with risk stratification and therapy. JAMA Netw Open 2022;5:e2148147. https://doi.org/10.1001/jamanetworkopen.2021.48147
67. Akram K, Voros S. Influence of symptoms and age on the predictive value of coronary artery calcium scanning. J Am Coll Cardiol 2008;52:2214; author reply 2214. https://doi.org/10.1016/j.jacc.2008.07.070
68. Knez A, Becker A, Leber A et al. Relation of coronary calcium scores by electron beam tomography to obstructive disease in 2,115 symptomatic patients. Am J Cardiol 2004;93:1150–2. https://doi.org/10.1016/j.amjcard.2004.01.044
69. Paixao AR, Ayers CR, El Sabbagh A et al. Coronary artery calcium improves risk classification in younger populations. JACC Cardiovasc Imaging 2015;8:1285–93. https://doi.org/10.1016/j.jcmg.2015.06.015
70. Sung JH, Yeboah J, Lee JE et al. Diagnostic value of coronary artery calcium score for cardiovascular disease in African Americans: the Jackson Heart Study. Br J Med Med Res 2016;11:BJMMR/2016/21449. https://doi.org/10.9734/BJMMR/2016/21449
71. Carr JJ, Jacobs DR Jr., Terry JG et al. Association of coronary artery calcium in adults aged 32 to 46 years with incident coronary heart disease and death. JAMA Cardiol 2017;2:391–9. https://doi.org/10.1001/jamacardio.2016.5493
72. Grandhi GR, Mirbolouk M, Dardari ZA et al. Interplay of coronary artery calcium and risk factors for predicting CVD/CHD mortality: the CAC consortium. JACC Cardiovasc Imaging 2020;13:1175–86. https://doi.org/10.1016/j.jcmg.2019.08.024
73. Kim YJ, Hur J, Lee HJ et al. Meaning of zero coronary calcium score in symptomatic patients referred for coronary computed tomographic angiography. Eur Heart J Cardiovasc Imaging 2012;13:776–85. https://doi.org/10.1093/ehjci/jes060
74. Hulten E, Bittencourt MS, Ghoshhajra B et al. Incremental prognostic value of coronary artery calcium score versus CT angiography among symptomatic patients without known coronary artery disease. Atherosclerosis 2014;233:190–5. https://doi.org/10.1016/j.atherosclerosis.2013.12.029
75. Mitchell JD, Fergestrom N, Gage BF et al. Impact of statins on cardiovascular outcomes following coronary artery calcium scoring. J Am Coll Cardiol 2018;72:3233–42. https://doi.org/10.1016/j.jacc.2018.09.051
A retrospective study of 322 patient experiences of post-operative pain, short term and long term, following a cardiac implantable electronic device (CIED) procedure. Pain from pacemaker and ICD (implantable cardioverter-defibrillator) implant surgery remains a problem both in terms of severity and longevity. There is a subset of patients receiving implants that have severe pain that may be of a long duration. Patient advice needs to be appropriate to these findings.
This study illustrates a need for better pain management by physicians, support, and realistic communication with their patients.
Introduction
Dr Selwyn Brendon Goldthorpe
Indications for the use of pacemakers and implantable cardioverter-defibrillators (ICDs) have become more defined over time, resulting in many more patients receiving these devices.1 Cardiac implantable electronic device (CIED) procedure is the term used to encompass pacemaker and ICD implant surgery.
As of 2016, it was estimated that there were about 1.14 million pacemakers globally. By the year 2023, that number is expected to increase to 1.43 million units.2 Many nations are now keeping records of the implant complication rate for pacemakers and ICDs.3-6 As in any surgical procedure, a complication rate is to be expected from device implantation.7-9 Unfortunately, complication definition is a medical categorisation. Pain can be mentioned as a complication: “Minor wound pain is expected after device implantation, almost always controlled with simple analgesia”.10
Post-operative implant pain has been acknowledged and managed more robustly.11-13 It was concluded by Lee et al.11 that “Post-operative opioid prescription rate after CIED procedures was 20.2%, with most patients being opioid naïve. Among opioid naïve patients who received opioids, 9.4% had subsequent opioid refills. This finding suggests that peri-operative pain management in CIED procedures warrants meticulous attention.” Furthermore, patient advice may still be inadequate with regard to pain expectation. The current UK National Health Service (NHS) information to patients states, “You may feel some pain or discomfort during the first 48 hours and will be given pain-relieving medication”.14
Method
A retrospective study of 322 patient experiences of post-operative pain, short term and long term (<1 week to >5 years, mean 1.72 years), exacerbating factors and relieving factors.
An online, anonymised, retrospective survey was undertaken using pacemaker and ICD support sites. The Pacemaker Club online support group now claims to have over 40,500 members (https://www.pacemakerclub.com), and the Facebook groups Pacemaker Support and Living with an ICD, have 20,000 members (https://www.facebook.com/groups/952659304852414, and https://www.facebook.com/groups/icdsupport), representing approximately 4.5% of those worldwide with pacemakers and ICDs, making such members a large, but self-selected, group of the world’s total number of CIED recipients. Members of both sites voluntarily register their interest in belonging to such online support groups. Both sites are English speaking and accept members worldwide.
Appendix. The questions reported on
Age in years
Gender
Age when received last implant
Number of implants ever
Type of implant (pacemaker/ICD)
Skin closure method
Duration of last implant
Site of pain, if any
Duration of pain, if any pain
Pain score scale (0–10) 0 being none, 10 being worst ever
Character of pain, if any
Medical complications of surgery
Pain relief method
What exacerbated the pain, if any pain?
Complications from the surgery
Co-morbidity (single choice)
Height
Weight
Comments
Anecdotal evidence from these support groups suggests that there is a group of implant recipients with long-term problems of pain, related to their implant, and that they are medically difficult to manage. These English-speaking support sites represent personal experiences worldwide, rather than from any specific country. Participants were given a brief summary of why the survey was taking place and the content of the survey, and were invited to take part on the understanding that their participation was entirely voluntary and their answers would be anonymised. Participants were self-selected, consenting to take part in this online survey by clicking onto a link taking them to the survey. This invitation was repeated weekly on the site’s message board by the person responsible for participant communication liaison. Responses were predominantly recorded between June 2021 and December 2021. There were 322 questionnaires (consisting of 19 questions – Appendix) returned.
Participants could opt out of answering questions, resulting in not all 19 questions being answered fully. The last question, ‘Any comments’, gave latitude for participants to express themselves as they wished. Text replies and comments were grouped into emerging themes in order to obtain grounded outcomes.
Results
Of the 322 support group respondents, the median age was 60 years (range 6–91 years): 217 (67.8%) were female, 103 male (32.2%). Two respondents opted out of their gender statement. The number of support group respondents with pacemakers was 212. The number with ICDs was 110.
The median number of years of having had their last device was one (mean 1.72 years). The frequency spread of implant duration is shown in figure 1.
Figure 1. Numbers reporting various durations of last implant (n=322)
Half (50%) of the support group respondents had had their present implant for less than one year. Of respondents, 85% had received one implant, 10% had received two implants, 2% had received three implants, and 3% had received four implants. No respondent had received more than four implants. The duration of last implant was not associated with gender (mean 1.97 years for males, mean for females 1.58 years; t-test 0.79, p=0.22, not significant as p>0.05).
Of our support group respondents, 208 of the 322 participants (64.8%) reported pain for one week or more: 32 people had pain for six months or more (10.0% of respondents). Duration of pain for over two months represented 24% (95% confidence interval [CI] ±9.8%) of those responding to this question – almost one in four of those replying.
Participants were asked, ‘Using any number from 0 to 10, score your pain, where 0 is none and 10 is the worst possible pain, what number would you use to rate your pain? (slide pointer to insert value).’ The sliding pointer was to the nearest integer. Figure 2 shows the frequency of response for pain scores.
Figure 2. Frequency of people reporting pain by integer interval scale of 0–10, where 0 was no pain, and 10 was the worst pain possible (n=314)
The median pain score was five. The mean pain score was found to be 4.5 (95%CI 4.2 to 4.8). The data are not normally distributed being skewed towards pain scores <6 (Kolmogorov-Smirnov test of normality D=0.093, p=0.04). The majority (62.7%) found the pain to be not of great severity (score <6, as defined by this study scale). Over a third of respondents (37.3%) found the pain to be severe (score >5), 2% describing the pain as the worst possible (i.e. score 10).
Table 1. Site of pain after implant. There were 437 sites of pain mentioned by 322 respondents
Site of pain
Number
Percentage
Incision pain
116
26.5%
Implant/pocket pain
86
19.7%
No pain or no answer
56
12.8%
Shoulder pain
51
11.7%
Localised chest pain
45
10.3%
Upper arm/arm not specified
31
7.1%
Axillary pain
13
3.0%
Central chest pain
12
2.7%
Neck/jaw pain
11
2.5%
Scapular/back pain
8
1.8%
Lower arm pain
7
1.6%
Elsewhere pain
1
0.2%
Pain experienced is certainly not confined to the pacemaker site (incision and implant, pocket pain), 178 other sites of pain were reported by 258 people experiencing pain (69.0% of those having pain). Responses were themed by anatomical sites (table 1). The character of the pain was said to be sharp by 33% of respondents, dull by 32% of respondents, and burning by 19%. Aching, tingling, and general soreness were also described.
Pain relief was categorised by 281 support group respondents: 122 people used paracetamol for pain relief, 56 people used ice, 45 people used non-steroidal anti-inflammatory drugs (NSAIDs), and 22 people used opiates. Other forms of pain relief used were heat, alcohol, marijuana, oil of oregano, turmeric, and gabapentin/pregabalin. No pain relief was required by 17.1% (48) of the 281 respondents. Careful positioning at night was said to be helpful. Many respondents mentioned multiple medications.
Critical comments were received from support group respondents, some of which are reproduced below:
“It would have been helpful if they had sent me home with something for pain – they didn’t.”
“I needed a sleep medication to sleep through the pain the first night because I was offered only Tylenol which did nothing. When I got home, ice was my friend!”
“It was a squeezing pressure and all over body pain that required Percocet every 4 hours for 8–10 days. I cried when nurse said the doctor forgot to order it. Unbearable discomfort.”
“The only pain relief my cardiologist approves of is Tylenol, and it does not help much.”
“Since my doctors won’t prescribe more than 3 days of pain meds, we are forced to find alternatives. Oil of Oregano.”
“Being sent home 5 hours after lung re-inflated without high dose pain med like morphine. It is inhumane and medically wrong.”
The complication rate reported by those support group members responding to this survey was 38.5% (124 reported individuals of 322 participants). The expected complication rate would be around 2–13% according to the pooled data from various centres.3-6,15-17
Table 2. Medical complications reported by participants (n=322)
Medical complication
Number
Device movement from initial site
18
Lead placement problem
16
Wound infection
13
Device preventing arm movement
12
Excessive bruising or blood clot at the implant site
11
Lead fracture
7
Cosmetically unacceptable
6
Badly placed device
4
Skin break
3
Other
34
Total complications
124
What is classified as a medical complication varies between centres. Medical complications reported here were themed by groups, that were mentioned by the participants (n=322) of this survey; these are shown in table 2. ‘Other’ complications (27% of the total complications) included: excessive pain during and after procedure, myocardium perforation, thoracotomy, haematoma, intravenous (IV) infusion-related swelling at the site, pneumothorax shoulder pain/frozen shoulder, psychological problems, leads badly placed, tissue glue allergy, pleural effusion, and exacerbation of hypertension.
Comparing the pain scores of those with complications and those without complications, using Mann-Whitney U-Test, no significance was found in the reported pain scores (z-score 1.15, p=0.25; the scores were approximately normally distributed). The mean pain score for the complication group was 4.26, and for the non-complication group 4.64.
Of those (n=124) reporting complications, one person had pain of 6–12 months’ duration, and two had pain of 1–2 years’ duration; 56 reported pain from one week to two months’ duration. Long-term pain does not seem to be associated with complication rates in this study.
‘Major complications’ (pre-defined and adjudicated by a committee) have been reported to be higher with implantable ICDs compared with pacemaker replacements.18 This was not found to be the case in this retrospective survey’s reported complication rate in these groups (Chi-square statistic 0.66, p=0.42, not significant).
Discussion
This worldwide, English-speaking, survey of online support group members showed a relatively high proportion (38.5%) of the 322 support group respondents having complications from their implant. This depends on how you define ‘complications’. This is especially a problem when a survey is patient-orientated (as this survey), and includes complications such as cosmetically unacceptable, or badly placed device (these two complications accounting for 10% of reported complications), compared with ‘medical complications’ reported in medical literature.15-17 Pain is not necessarily seen as a complication of a CIED procedure.3-6 The responses obtained are from a group of CIED recipients finding the need for self-support. We should, as healthcare professionals, ask why this form of support is needed?
The advice that, ‘minor wound pain is expected after device implantation, almost always controlled with simple analgesia’,10 would seem to be inappropriate, as found by this study when the duration of pain for over two months, represented 24% (95%CI ±9.8%) of those responding to this question – almost one in four of those replying.
Furthermore, the pain severity was for over a third of respondents (37.3%) found to be severe (score >5), 2% describing the pain as the worst possible (score 10). This adds support to previous findings by Lee et al.,11 that peri-operative pain management in CIED procedures warrants meticulous attention. Pain from pacemaker and ICD implant surgery remains a problem both in terms of severity and longevity.
Our respondents are a self-selected group seeking support from each other, mostly outside of medical professionals. Personal experience may not transfer into generality. However, comments received related to a number of disturbing physician findings:
“I had to beg the doctor for pain medication after the procedure.”
“My doctor keeps saying it should only be mild discomfort, which makes me feel like they are dismissing my pain/experience. Not everyone has the same experience, pain level, etc. My pain is real.”
“The doctors were no help. Once they put it in, they were done.”
“Some members of my medical team belittled my pain concerns and refused to give me pain meds. It was an awful experience.”
“Most doctors underestimate the amount of pain post-procedure.”
“I wish doctors would make it clear about getting a pacemaker and the complications that come with it.”
There would appear to be a need for better information given to patients, as found by this survey, and summed up by this comment:
“I found the literature about pacemakers misleading, as they said most people are fine after a day and back to work in a week. My boss expected this too. But I was uncomfortable, tired and emotional, and felt a failure for not being back to normal in a week as suggested. More realistic info needed.”
This worldwide survey, of those English-speaking CIED patients seeking a self-help group, highlights a need for better medical communication to CIED patients. Advice to patients, and the literature they receive at the time of the procedure, needs to change. It should now be seen that pain from pacemaker and ICD implant surgery remains a problem for some patients, both in terms of severity and longevity. This should be clear to both patient and physician. Severe pain and enduring pain needs to be recorded as a complication on follow-up of CIED patients. This should then act as a stimulus for further studies to better explore why such pain occurs and what is the best management for such pain.
Key messages
Pain from pacemaker and implantable cardioverter-defibrillator (ICD) implant surgery remains a problem both in terms of severity and longevity for some patients
In the assessment of the patient experience of pain following implantation of cardiac pacemakers and ICDs, there was found to be a need for better pain management and realistic communication with patients belonging to self-help groups
Further research is needed into the problems of chronic and severe pain associated with these procedures
Conflicts of interest
None declared.
Funding
None.
Study approval
Ethical approval for this study was obtained from the moderator of the Pacemaker Club (https://www.pacemakerclub.com).
3. Shakya S, Matsui H, Fushimi K, Yasunaga H. In-hospital complications after implantation of cardiac implantable electronic devices: analysis of a national inpatient database in Japan. J Cardiol 2017;70:405–10. https://doi.org/10.1016/j.jjcc.2017.02.013
4. Khanal J, Poudyal RR, Devkota S, Thapa S, Dhungana RR. Clinical profile and early complications after single and dual chamber permanent pacemaker implantation at Manmohan Cardiothoracic Vascular and Transplant Centre, Kathmandu, Nepal. J Nepal Health Res Counc 2015;13:138–43. Available from: https://www.jnhrc.com.np/index.php/jnhrc/article/view/638/497
5. Møller M, Arnsbo P, Asklund M et al. Quality assessment of pacemaker implantations in Denmark. Europace 2002;4:107–12. https://doi.org/10.1053/eupc.2002.0234
6. Gadler F, Valzania C, Linde C. Current use of implantable electrical devices in Sweden: data from the Swedish pacemaker and implantable cardioverter-defibrillator registry. Europace 2015;17:69–77. https://doi.org/10.1093/europace/euu233
7. Pavia S, Wilkoff B. The management of surgical complications of pacemaker and implantable cardioverter-defibrillators. Curr Opin Cardiol 2001;16:66–71. https://doi.org/10.1097/00001573-200101000-00010
8. Ludwig S, Theis C, Wolff C, Nicolle E, Witthohn A, Götte A. Complications and associated healthcare costs of transvenous cardiac pacemakers in Germany. J Comp Eff Res 2019;8:589–97. https://doi.org/10.2217/cer-2018-0114
10. Schiariti M, Cacciola M, Puddu PE. Chapter 15. Complications of pacemaker implantation. In: Das MM (ed.). Modern Pacemakers – Present and Future. London: IntechOpen, 2011; pp. 271. https://doi.org/10.5772/556
11. Lee JZ, Pasha AK, Glasgow AE et al. Postoperative opioid prescription patterns and new opioid refills following cardiac implantable electronic device procedures. Heart Rhythm 2019;16:1841–8. https://doi.org/10.1016/j.hrthm.2019.08.011
12. Lee JZ, Glasgow AE, Habermann EB et al. Liposomal bupivacaine during subcutaneous implantable cardioverter defibrillator implantation for pain management. Pacing Clin Electrophysiol 2021;44:513–18. https://doi.org/10.1111/pace.14175
13. Yang JK, Char DS, Motonaga KS et al. Pectoral nerve blocks decrease postoperative pain and opioid use after pacemaker or implantable cardioverter-defibrillator placement in children. Heart Rhythm 2020;17:1346–53. https://doi.org/10.1016/j.hrthm.2020.03.009
16. van Rees JB, de Bie MK, Thijssen J et al. Implantation-related complications of implantable cardioverter-defibrillators and cardiac resynchronization therapy devices: a systematic review of randomized clinical trials. J Am Coll Cardiol 2011;58:995–1000. https://doi.org/10.1016/j.jacc.2011.06.007
17. Pakarinen S, Oikarinen L, Toivonen L. Short-term implantation-related complications of cardiac rhythm management device therapy: a retrospective single-centre 1-year survey. Europace 2010;12:103–08. https://doi.org/10.1093/europace/eup361
18. Poole JE, Gleva MJ, Mela T, Chung MK. Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures. Circulation 2010;122:1553–61. https://doi.org/10.1161/CIRCULATIONAHA.110.976076
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits