In response to the article by Acharya and Mariscalco on the diagnosis and acute management of type A aortic dissection,1 I would like to expand on the role of pulmonary embolism (PE). The differential diagnosis of type A aortic dissection includes, not only PE, as stated by the authors in table 2 of the article,1 but, also, the co-existence of PE and dissecting aneurysm of the aorta (DAA).2–14
A literature search in Pubmed and Google scholar disclosed 13 examples of the association of type A aortic dissection and PE (table 1).2–14
Table 1. Co-existence of aortic dissection and pulmonary embolism
First author
Age
Sex
CP
BKP
ARG
PRP
BPD
MDS
SOB
HPTY
DVT
EFF
ARP
Antithrombotic treatment
Cruz2
71
F
✓
–
–
✓
–
–
✓
–
✓
–
–
OAC
Radwan3
66
F
✓
–
–
–
–
–
–
–
–
–
✓
Information not available
Kagawa4
71
F
–
✓
–
–
–
✓
–
–
✓
✓
–
IVC filter, UFH, OAC, elastic stocking
Herera5
47
F
–
–
✓
–
–
–
✓
–
✓
–
✓
IVC filter, OAC
Fernandes6
81
M
✓
✓
–
–
–
–
–
–
✓
–
✓
LMWH
Ramponi7
75
M
✓
✓
✓
–
–
✓
✓
–
–
–
✓
Pulmonary embolectomy, OAC
Bodian8
66
M
✓
✓
✓
–
✓
✓
✓
✓
–
–
–
None
Morimoto9
60
M
✓
✓
–
–
–
✓
–
–
✓
✓
–
IVC filter
Tudoran10
70
M
✓
–
✓
–
–
–
✓
–
✓
–
✓
UFH, OAC
Volvovitch11
73
F
✓
–
–
–
–
–
–
–
–
–
✓
Pulmonary embolectomy, OAC
Thiam12
31
F
✓
–
–
–
–
✓
✓
✓
–
–
–
OAC
Leu13
59
F
–
–
–
–
–
–
✓
–
–
–
–
Heparin
Fukuizumi14
81
F
–
✓
–
–
–
✓
✓
–
–
–
–
Embolectomy, IVC filter, OAC
Key: ✓ = presence of that parameter; – = absence of that parameter; ARG = aortic regurgitation; ARP = aortic repair; BKP = back pain; BPD = inter-arm blood pressure difference; CP = chest pain; DVT = deep vein thrombosis; EFF = pleural effusion; F = female; HPTY = haemoptysis; IVC = inferior vena cava; LMWH = low-molecular-weight heparin; M = male; MDS = mediastinal enlargement; OAC = oral anticoagulants; PRP = paraplegia paraparesis; SOB = shortness of breath; UFH = unfractionated heparin
Combination of DAA and PE stigmata suggestive of co-existence of DAA and PE
What seemed to be the most likely combination of DAA stigmata and PE stigmata indicative of the co-existence of DAA and PE was documented in the following patients:
A patient who had chest pain, back pain, and deep vein thrombosis.6
A patient who had chest pain, back pain, inter-arm blood pressure difference, breathlessness and haemoptysis, as well as mediastinal enlargement.8
A patient who had back pain, mediastinal enlargement and deep vein thrombosis.9
A patient who had chest pain, aortic regurgitation, breathlessness and deep vein thrombosis.10
A patient who had back pain, mediastinal enlargement, breathlessness, and floating right heart thrombus.14
Caveats and diagnostic traps
In Bhat et al., a 21-year-old man presented with severe chest pain and mild dyspnoea. Computed tomographic angiography (CTA) showed, not only stigmata of DAA, but, also, apparent filling defects in the right and left pulmonary arteries. However, during operative repair of the aorta, the pulmonary arteries were also opened and explored, and were found to be completely free of thrombus. In this instance, the angiographic signs suggestive of PE were, in fact, attributable to DAA-related compression of the pulmonary artery.15
Conversely, in Neri et al., DAA-related compression of the pulmonary artery did result in thrombotic occlusion of the pulmonary artery. Subsequent operative intervention involved operative aortic repair as well as pulmonary artery thrombectomy.16
Treatment strategies for DAA
Seven patients were managed without aortic repair,2,4,8,9,12–14 three of whom subsequently died.8,12,13 Among the four survivors of conservative DAA management was an 81-year-old patient in whom co-existing thromboembolism was managed by surgical embolectomy involving extraction of a floating right heart thrombus located in the right atrium, and subsequent oral anticoagulation using warfarin.14 Also managed without aortic repair was a 71-year-old woman in whom PE was managed by insertion of an inferior vena cava filter followed by oral anticoagulation.4
Six patients were managed by aortic repair,3,5–7,10,11 two of whom died.6,10 Among the survivors were two patients who were managed by the combined operative strategy of aortic repair (for DAA) and pulmonary embolectomy (for PE).7,11
Treatment strategies for PE
The range of treatment strategies included intravenous unfractionated heparin, vitamin K antagonists, insertion of inferior vena cava filter, and pulmonary embolectomy. There was one patient who did not receive any of those treatment strategies. That patient died soon after the dual diagnosis of DAA and PE was made.8 In one other instance, information about prescription, or absence of prescription, of antithrombotic measures was not available.3
Take home message
Clinicians should be vigilant for the co-existence of DAA and PE so that measures can be taken to mitigate the risk of a potential PE-related fatal outcome.
Conflicts of interest
None declared.
Funding
None.
Acknowledgement
I am indebted to Peter Laws for compiling table 1.
References
1. Acharya M, Mariscalco G. Diagnosis and acute management of type A aortic dissection. Br J Cardiol 2023;30:62–8. https://doi.org/10.5837/bjc.2023.012
2. Cruz I, Caldeira D, Stuart B et al. A case of pulmonary thromboembolism and aortic dissection: the role of echocardiography. Rev Port Cardiol 2013;32:549–50. https://doi.org/10.1016/j.repc.2012.12.010
3. Radwan K, Peszek-Przbyla E, Gruszka A, Sonsowski M, Buszman P. Acute aortic dissection imitating ST elevation myocardial infarction with accompanying pulmonary embolism. Cardiol J 2007;14:595–6. Available from: https://journals.viamedica.pl/cardiology_journal/article/view/21658
4. Kagawa Y, Ota S, Hoshino K et al. Acute pulmonary thromboembolism and deep vein thrombosis during the medical treatment of acute aortic dissection was successfully treated by the combination of inferior vena cava installation and anticoagulant therapy: a case report. Ann Vasc Dis 2015;8:36–9. https://doi.org/10.3400/avd.cr.14-00083
5. Herrera RN, Miott JA, Perreyra AS et al. Marfan syndrome associated with aortic dissection, venous thromboembolism and hyperhomocysteinemia [article in Spanish]. Medicina (B Aires) 2012;72:478–80. Available from: https://www.medicinabuenosaires.com/PMID/23241291.pdf
6. Fernandes S, Rodrigues M, Barreiros C et al. An incident of a massive pulmonary embolism following acute aortic dissection. J Crit Care Med 2021;7:67–72. https://doi.org/10.2478/jccm-2021-0001
7. Ramponi F, Papps T, Edwards J. Successful repair of concomitant acute type A aortic dissection and saddle pulmonary embolism. Aorta (Stamford) 2018;6:34–6. https://doi.org/10.1055/s-0038-1639345
8. Bodian M, Guindo AS, Aw F et al. Double emergency associating acute aortic dissection and pulmonary embolism of fatal evolution: about a case. J Clin Exp Cardiol 2018;9:12. https://doi.org/10.4172/2155-9880.1000617
9. Moromoto S, Izumi T, Sakurai T et al. Pulmonary embolism and deep vein thrombosis complicating acute aortic dissection during medical treatment. Intern Med 2007;46:477–80. https://doi.org/10.2169/internalmedicine.46.6215
10. Tudoran M, Tudoran C. High-risk pulmonary embolism in a patient with acute dissecting aortic aneurysm. Niger J Clin Pract 2016;19:831–3. https://doi.org/10.4103/1119-3077.181355
11. Volvovitch D, Ram E, Cohen H et al. Acute pulmonary embolism following acute type A dissection in a patient with COVID-19. J Card Surg 2012;36:1566–8. https://doi.org/10.1111/jocs.15389
12. Thiam C, Sonfo B, Camara Y et al. Double emergency pulmonary embolism and aortic dissection: about a clinical case. World J Cardiovasc Dis 2020;10:550–7. https://doi.org/10.4236/wjcd.2020.108054
14. Fikuizumi A, Akutsu K, Tokita Y et al. Surgical thrombectomy for right heart thrombus with acute aortic dissection. Ann Thorac Cardiocasc Surg 2014;20(suppl):937–40. https://doi.org/10.5761/atcs.cr.13-00218
15. Bhatt K, Navia J, Flamm S, Bolen M. Type A aortic dissection mimicking a saddle pulmonary embolus on computed tomography angiography. Circulation 2014;129:2180–2. https://doi.org/10.1161/CIRCULATIONAHA.114.008819
Authors: Ahmet Fuat, Chris Gale, Guy Lloyd, Helen Williams, Jim Moore, Trudie Lobban, Vijay Kunadian, Wajid Hussain
Sponsorship Statement:
The Bayer Cardiovascular Exchange Summit 2022 was organised and fully funded by Bayer plc, in partnership with the British Cardiovascular Society (BCS) and the Primary Care Cardiovascular Society (PCCS). This report has been endorsed by the Arrhythmia Alliance.
Faculty members receiving an honorarium are declared in the ‘Conflicts of interests statement’. LCW Consulting and the Bayer medical team were involved in the generation and approval of this report. Bayer acknowledges that the workshop feedback outlined in the report has been contributed to by delegates in attendance at the meeting who were not paid an honorarium. The Bayer medical team have not influenced the editorial outputs of this report but have medicolegally reviewed the document for compliance with the ABPI Code of Practice and for technical accuracy.
RP-UN-CAR-GB-0158 | October 2023
A post-meeting report from the Bayer 2022 Cardiovascular Exchange Summit ‘Inspire change’
Faculty
Faculty member
Affiliation
Professor Ahmet Fuat
PCCS Council Member and GPSI Cardiology, County Durham
Professor Chris Gale
Professor of Cardiovascular Medicine and Honorary Consultant Cardiologist, University of Leeds
Dr Guy Lloyd
Consultant Cardiologist, Barts Heart Centre and Honorary Secretary, BCS
Helen Williams
National Specialty Adviser for CVD Prevention, NHSE & NHSI and Consultant Pharmacist for CVD, SE London CCG and UCL Partners
Dr Jim Moore
President of the PCCS and GPSI Cardiology, Gloucestershire
Trudie Lobban, MBE
Founder of the AF Association
Professor Vijay Kunadian
Professor of Interventional Cardiology, Newcastle University and Honorary Consultant Interventional Cardiologist, Freeman Hospital Newcastle upon Tyne Hospitals NHS Foundation Trust
Dr Wajid Hussain
Consultant Cardiologist & Chief Clinical Information Officer, Royal Brompton and Harefield Hospitals
Key: AF= atrial fibrillation; BCS = British Cardiovascular Society; CCG = clinical commissioning group; CVD = cardiovascular disease; GPSI = general practitioner with a special interest; NHS = National Health Service; NHSE & NHSI = National Health Service England and National Health Service Improvement; PCCS = Primary Care Cardiovascular Society; SE = south-east; UCL = University College London
Abstract
The Bayer Cardiovascular Exchange Summit 2022 was organised in partnership with the British Cardiovascular Society (BCS) and the Primary Care Cardiovascular Society (PCCS). This meeting provided a platform for the exchange of clinical and patient expertise and innovation across the field of cardiovascular disease (CVD). It aimed to highlight opportunities to improve CVD management and to address the excess post-pandemic cardiovascular (CV) mortality. The meeting was centralised around three core areas: collaborative working between the National Health Service (NHS), pharmaceutical industry and patient advocates; synergistic working across primary and secondary care; and opportunities for healthcare digitalisation.
Joint working between the NHS and the pharmaceutical industry can help to bridge gaps in skills, contribute to quality improvement (QI) and provide learnings for future projects. Good clinical governance is key and collaborations between the NHS and multiple industry partners may overcome the risk of perceived bias. Patients should be central to all NHS-industry projects and all projects should include a patient voice by including the right patient at all times. Their perspective and views should be considered when creating CVD policies or during clinical research to allow transformation of CVD diagnostic and management services. Enriching partnerships between health care professionals (HCPs) and a diverse group of patient advocates is vital to improve patient management. Patient advocates can raise awareness of CVD and engage more patients to better understand their condition.
Improved communication, awareness of expectations and collaborative working between primary and secondary care services can facilitate optimum patient care. However, challenges exist at the primary-secondary care interface, such as long waiting lists for referrals and miscommunication. End-to-end pathways for health, social care, voluntary and community services should be mapped across the healthcare system nationally, with importance placed on integrated care via integrated clinical leadership. There is an inverse care pyramid in relation to investment, which is often top-heavy, aimed at secondary and tertiary care. Investing more resources in primary care services for public health promotion may reduce the CVD burden. More effective utilisation of annual CVD reviews, upskilling primary care teams on CVD and provision of expertise across each locality in the form of a CVD lead may optimise CVD management.
Digital healthcare technologies can provide opportunities to identify high-risk CVD patients through the use of artificial intelligence, NHS electronic health records (EHR) and digital diagnostic tools. Currently available data can innovatively be used at scale to develop pathways that allow early detection of CVD such as atrial fibrillation (AF). However, it is important to consider who will be responsible for undertaking the work and funding digital initiatives. Digital innovation can be seen with the advent of patient portals and mobile applications. New digital technologies must be supported by robust evidence, be cost-effective, allow an improvement in safety outcomes and increase productivity. They can be used to support patients with managing their condition by inducing behavioural change and facilitate communication between HCPs and patients in a timely and flexible manner. However, patient consent is essential, and it is important to note that digital tools may not suit every patient; these groups should not be disadvantaged and non-digital options should be readily available for such groups.
The outputs of the Bayer Cardiovascular Exchange Summit 2022 included valuable expertise from stakeholders involved in CVD management, including HCPs working across primary and secondary care and patient representatives. Greater partnerships between the NHS, pharmaceutical industry and patient advocacy groups with better communications across primary and secondary care services and adoption of digital innovations is vital for improving CVD management.
Introduction
The 2022 Bayer Cardiovascular Exchange Summit was run in partnership with the British Cardiovascular Society (BCS) and the Primary Care Cardiovascular Society (PCCS) with an aim to encourage scientific dialogue through the exchange of clinical expertise from specialists with an interest in the management of cardiovascular disease (CVD) and healthcare service delivery in the UK.
The meeting objectives were:
To update delegates on the latest advances in CVD clinical research
To highlight present and future challenges in CVD management
To provide a forum to discuss opportunities within CVD management for collaborative working with the pharmaceutical industry and patient advocates and synergistic working between primary and secondary care
To address unmet clinical needs in CVD care and service delivery
The meeting addressed three key topics:
Collaborative working between the National Health Service (NHS), pharmaceutical industry and patient advocates
Synergistic working between primary and secondary care
Healthcare digitalisation
Each topic was covered by plenary presentations, delivered by clinical expert speakers or a patient group expert representative, followed by workshops, chaired and facilitated by a faculty of clinical experts within cardiovascular (CV) medicine, which involved discussions between the expert faculty and attending delegates.
Both the BCS and PCCS are committed to working in partnership with patients, the pharmaceutical industry and relevant organisations with aligned strategic aims to identify the current challenges in CVD management within the NHS and to identify solutions to address these.
This report summarises the key messages from the meeting.
Collaborative working between the NHS, pharmaceutical industry and patient advocates
Quality improvement involves systematically using tools to continuously improve the quality of care delivered and outcomes for patients. It should be a key consideration when redesigning healthcare services.1
There are five different NHS and pharmaceutical industry models of working (see table 1), providing valuable opportunities for CVD management through collaborative work. Some of these models of working can be complex and so there is a need for a clear, transparent approach to collaboration. Clear objectives of NHS and industry joint working and good clinical governance is needed with a recognition of where priorities differ; the transparency of declarations is key. There should be a clear structure for funding and reimbursement for projects. It is important to include patient organisations and representatives in all NHS/pharmaceutical industry joint working projects to ensure the needs and views of patients are considered. Disseminating learnings from local NHS–industry partnership projects can highlight the successes and limitations of joint working.2
Table 1. Different NHS and pharmaceutical industry models of working
NHS/pharmaceutical industry models of working
Description
Industry-commissioned studies
Standard model for clinical trials and most industry-funded clinical research
Pharmaceutical company is the study sponsor and NHS clinicians and academics may advise on study design
Joint working agreements
Common framework for industry-supported service transformations or evaluation of new service models
All anticipated benefits must be set out in advance of project commencement
Each party must make a significant and defined contribution to the project
All transfers of value made by companies must be publicly disclosed on Disclosure UK2
Benefits:
NHS: improved quality-of-care provision, use of resources and configuration of services around patient needs2
Patients: fewer hospital admissions, better experience of the healthcare system2
Industry partner: potential increased use of appropriate drugs aligned to local or national guidance and expansion of relevant and eligible patient populations2
Donations and grants
Funds, benefits-in-kind or services freely given to an organisation for the purpose of supporting healthcare, scientific research or education, with no obligation on the recipient organisation to provide goods or services to the benefit of the pharmaceutical company in return
There must be a written agreement in place for each donation or grant and the funds given must be publicly disclosed annually3
Competitive grant application schemes
Industry investments for service improvement or research grants
Funding panel is set up with independent healthcare professionals and may also include patients
National commercial partnerships
Provide the NHS with early access to NICE-approved drugs at a discount
Must result in benefits to patient populations
Key: NHS = National Health Service; NICE = National Institute for Health and Care Excellence
In routine clinical care, there are often missed opportunities to improve CVD prevention.4 Engaging patients early to ensure they understand the detrimental consequences of atrial fibrillation (AF) is important. Empowering both patients and healthcare professionals (HCPs) can help to optimise the AF dialogue between both parties with respect to correct questions asked and information relayed.
Patients must be at the forefront of healthcare and patient–HCP partnerships can be enriched through involvement of patient organisations and patient advocates, which are vital for raising public awareness of CVD and in implementing better diagnosis and care.5 Patient organisations and advocates can communicate lived experiences of everyday realities of care and management. This can emotionally resonate with policymakers and this power should be harnessed by including their expert opinion when creating CVD policies and developing CV health services.5
The AF Association and its sister organisation, Arrhythmia Alliance, are examples of CVD patient organisations that are well placed to provide information, education and patient support, as well as raising awareness of the importance of identifying AF within the community. Arrhythmia Alliance is dedicated to collaborating with healthcare services to support patients with AF.5
Key points: Collaborative working between the NHS, pharmaceutical industry and patient advocates
Considerations around pharmaceutical industry and NHS collaborations
Engagements between commissioners and pharmaceutical industry should be overseen by careful governance and any partnership should involve an NHS organisation that is a legal entity in its own right, to provide academic rigor
The preferred way of working is to collaborate with multiple pharmaceutical companies for any specific disease area so as to avoid the risk of perceived bias for a specific drug product
Regulations for working with different industries (pharmaceutical/device/diagnostics) should be more aligned
The quality improvement (QI) capability within the NHS is generally limited but industry can support the NHS, particularly where there are skill shortages, such as in project management
Projects need to have the capacity to be sustained in the longer term to ensure progress is not lost
A failed project may still be useful as it can provide valuable learnings for future work
Importance of patient organisations and patient advocates
Patients should be at the heart of everything and consideration should be given to involving patients in all projects, the steering committees of research studies, trial design and practice-changing documents. Involving patients can transform CVD diagnostic and management services. What is good for patients will ultimately also be good for pharmaceutical companies and the NHS
Inclusion is essential – both clinicians and patients should have equal representation and voices
Training volunteers to participate in forums is essential and selecting the correct panel of patients for patient engagement is important as the patient voice is often underutilised. Patient associations can support with raising patient awareness and HCPs, NHS and educational bodies and industry should be encouraged to work closely with them. Patient organisations can disseminate knowledge and information as well as identify patients to participate in studies
It is important for patient organisations to be involved in the selection of patient representatives, and on what criteria, to ensure they provide a broad view and not just their own personal experience. Including patient representatives from diverse backgrounds to represent the local communities is key to addressing health inequalities
Barriers to successful patient engagement include lack of time and resources, and patients being insufficiently empowered to make effective contributions. Patient organisations can provide an environment where patients are comfortable to contribute
Multidisciplinary care models are often not available and more needs to be done to improve patient care pathways
Synergistic working between primary and secondary care
According to NHS England, “Good organisation of care across the interface between general practice and secondary care providers is crucial in ensuring that patients receive high-quality care and in making the best use of clinical time and NHS resources in both settings.”6 However, challenges exist at the primary–secondary care interface. Post-COVID-19, secondary care referrals have built up, there are major waiting lists and there have been many did-not-attend appointments. Issues with miscommunication with respect to dissemination of advice to primary care colleagues has impacted upon re-referrals; HCPs may be unsure at which point patient management stops being the responsibility of secondary care services following referral.6,7
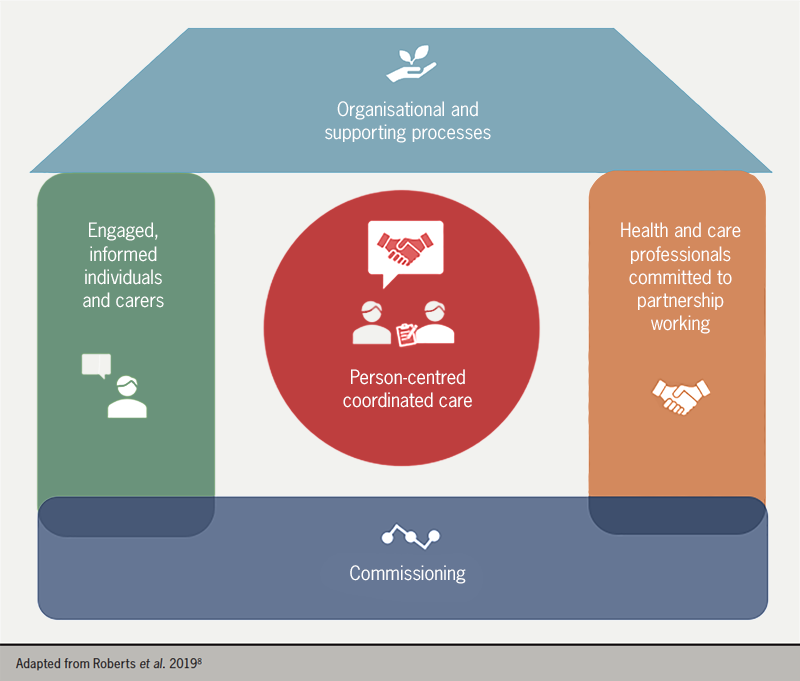
The approach to CVD management should be person-centred and should follow NHS England’s House of Care framework for long-term condition management (figure 1).8
Figure 1. Schematic to show long-term condition management
End-to-end pathways for health, social care, voluntary and community services should be mapped across the system with an emphasis on integrated care, combining care provision through general practitioner (GP) practices, primary care networks (PCNs), community pharmacies and community-based and hospital services, as appropriate. Care should be tailored to the individual’s needs and not that of the system.9
Example of a pre-existing pathway for CVD within the NHS includes the CVD prevention pathway with a focus around the AF, blood pressure (BP) and cholesterol (ABC) agenda.10
Integrated clinical leadership is necessary to deliver integrated care. Priorities should be determined by following a population health management approach. System-wide clinical guidance and integrated information technology (IT) systems can help to improve communication and access to population data. Integrated care boards (ICBs) can also provide strategic overview and coordination; however, these are still in their infancy.11
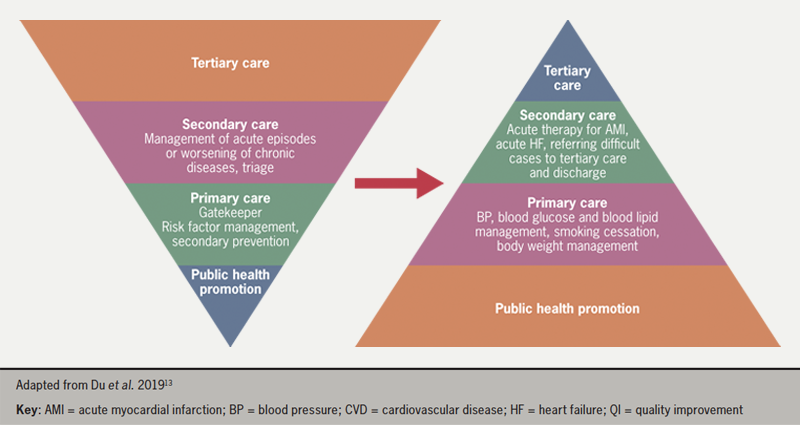
All care should be patient-centred, and patients should be involved at all stages of decision-making regarding care and supported to self-manage their care.12 The provision of CV services can be viewed as an inverted pyramid, with the bulk of management occurring in primary care through public health promotion and primary and secondary prevention of CVD. Fewer patients are then managed by secondary and tertiary care, respectively. However, the pyramid should be flipped when representing levels of funding associated with each level of care (figure 2). Addressing CVD risk factors by investing in primary care services and patient organisations for public health promotion may result in enhanced CV care.13
Figure 2. Flipping the inverse pyramid of care. There is a need to flip the current inverted pyramid of the healthcare system to invest more resources in promoting public health and in primary care to enable QI across the National Health Service and reduce the cardiovascular disease burden in secondary and tertiary care.
Heart failure (HF) is one example of a CV condition where having clear patient pathways in place across both primary and secondary care offers potential benefits to both patients and healthcare providers.
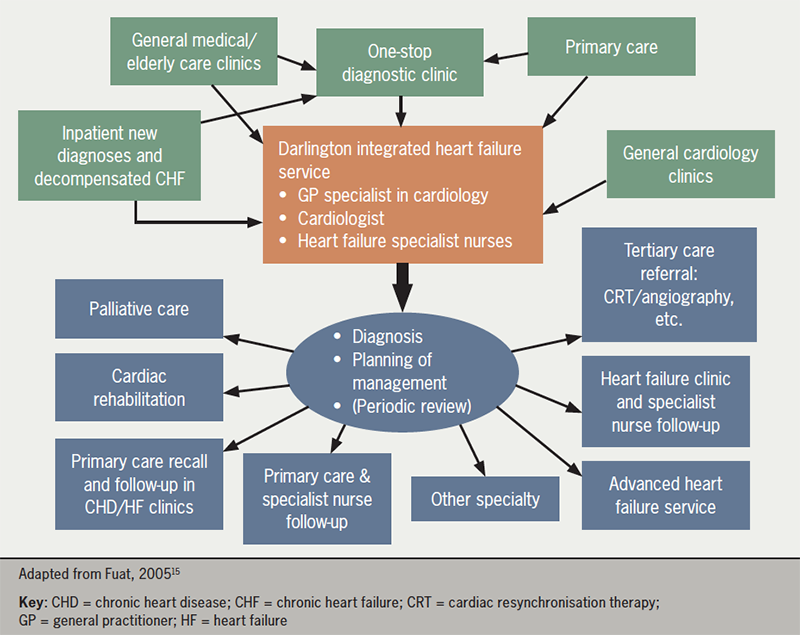
The Darlington One-Stop Diagnostic Clinic Model for HF diagnosis (figure 3) was set up following process-mapping workshops to identify HCPs who had seen patients with suspected HF from primary to tertiary care. The clinic involved local primary care referral pathways and comprised of weekly clinics with a GP cardiology specialist, a cardiologist and HF nurses. Patients underwent clinical assessments, including electrocardiography (ECG) and echocardiography (ECHO), and a management plan was developed for confirmed cases. Following diagnosis, relevant details surrounding HF diagnosis, management and follow-up was communicated to the patients’ GPs. This clinic resulted in the HF prevalence across Darlington Care Commissioning Group (CCG) to increase to the highest in the region and led to the lowest rates of hospital admissions.14 Such models of care require good relationships between primary and secondary care services.
Figure 3: The Darlington integrated heart failure service
Further examples of good practice include the use of QI data to identify suspected HF patients; nominating GP practice CVD leads to undertake thorough HF reviews; and educating all HCPs on new HF guidelines to ensure accurate diagnosis of HF-type. Virtual multidisciplinary teams (MDTs) can also support with cross-sector care.
The University College London (UCL) Partners Proactive Care Framework for lipid management allows HCPs to prioritise work through stratification of patients into priority groups. Familial hypercholesterolaemia (FH) requires better identification, which may be facilitated through a hub-and-spoke model in collaboration with secondary care services and industry partners. Patients with suspected FH were identified and their DNA tested, enabling a definitive diagnosis and appropriate management, including cascade testing to identify family members with FH.
Key points: Synergistic working between primary and secondary care
Importance of primary and secondary care relationships
Better two-way relationships and improved communication between primary and secondary care services is needed to enable GPs to access specialist guidance without having to re-refer patients to secondary care, and to optimise patient management post-discharge with shared ownership of targets and management plans
Standardised targets for lipid and blood pressure (BP) management can improve patient management post-discharge
Healthcare professional (HCP) civility is essential to enabling a joined-up service; HCPs need to be kind to one another as well as to their patients, and equally patients need to be kind to HCPs in return
Optimising CVD services
There is a huge disparity in access to CVD services nationally and locally, likely attributed to the variations in resources, primary and secondary care expertise and HCP level of interest, time and knowledge
Every PCN should have a CVD lead to ensure expertise in every locality, working closely with secondary care teams to further their expertise, with better interface working
Taking examples of good practice in one locality and implementing them elsewhere can be valuable
Better education and upskilling of primary care HCPs on CVD management, including post-discharge care, is important
HCPs should make the most of the wider healthcare opportunities afforded them during annual checks related to Quality and Outcomes Framework (QOF) indicators
Clinical pharmacists can play a vital role in supporting nurses to optimise the management of patients with CVD
Healthcare digitalisation
Optimising identification and management of high-risk CVD patients is essential16,17 and solutions are urgently needed to overcome the rising number of CVD events due to treatment delays, cancellations and NHS backlog following the COVID-19 pandemic. Innovations, such as digital technologies, may provide opportunities to improve health outcomes. Furthermore, identifying patient cases through the use of artificial intelligence (AI), NHS electronic health records (EHR), digital diagnostic tools and digital care hubs may allow medicines personalisation at an industrial scale.18–21
Early AF detection is a key priority of the NHS Long Term Plan,22 and accurately detecting AF, at scale and efficiently using routinely collected data, is needed.
One example of a digital pathway that is being piloted is FIND-AF (Future Innovations in Novel Detection of Atrial Fibrillation). This is an end-to-end digital pathway involving an algorithm that predicts individual-level risk of new AF in the next six months from routinely collected primary care electronic health records (EHRs), and an embedded pathway of remote diagnosis of AF with no requirement for extra appointments. The prediction model was developed in approximately two million UK primary care EHRs.23–25 The FIND-AF pathway utilises novel technology for preventative care and is personalised, patient-centred and helps to overcome health inequities. It has the potential to be scaled up nationally by implementation in primary care EHRs.18,24,25
Capture AF was an AF screening programme,26 whereby community pharmacists checked patient pulses using the Kardia AliveCor device if they had a CHA2DS2-VASc score ≥ 2. Five thousand patients were screened and there was a 1–2% AF detection rate. This project was a valuable example of joint working between pharmacy, primary and secondary care services.
Checks for new digital technologies
New digital technologies should be backed by evidence and scrutinised to ensure they are cost-effective, increase productivity and improve safety outcomes. They should allow interactions between professionals and ensure that the needs of the patients are at the centre.
Some of the many different areas of digital innovation include patient portals, mobile applications and wearable devices.27 Patient portals can facilitate patient interactions, allowing appointment scheduling, messaging and access to their health information. They can also avoid the need for unnecessary consultations.28 Well-being applications on mobile devices can be used to monitor health markers, such as weight, by connecting to weighing scales and assessing trends over time. Visual representation of test results can prove valuable to patients and their HCPs. Applications can also be useful for targeted education, such as inhaler device counselling. Although there are now an increasing number of mobile applications available, it is essential to ensure that these are reliable, effective and safe.29
Examples of such initiatives include a project across London’s tertiary cardiac centres, which involved the creation of a virtual ward for monitoring symptoms of those patients awaiting cardiac surgery. Patients completed weekly structured questionnaires assessing symptoms, and those with significant or deteriorating symptoms were highlighted through the software algorithm and reviewed remotely. It reduced the time between discharge and first follow-up from three months to eight weeks.30
Post-myocardial infarction (MI) medication up-titration is essential. As part of a post-MI pathway project, patients were asked to input daily BP and pulse checks into an application. At weeks two and four post-MI, patients were sent reminders by clinicians asking them to optimise their medicines in response to their BP and symptoms. At week eight, a video consultation was undertaken to review the patient. This resulted in quicker consultations, reduced did-not-attend appointments and 10 extra patients being seen weekly. There was 87% satisfaction with the process as patients felt as though they had been properly monitored and educated at appropriate times. Patients also reported saving significant time and money and liked having access to their hospital letters within the application.30–32
Key points: Healthcare digitalisation
Impact and considerations for patients
Patients should be empowered, provided with greater ownership of their condition and motivated to manage their own health, for example, through:
The use of digital technologies, such as to induce behaviour change to optimise medication adherence through reminders. However, whilst the regulatory framework for the approval of medical devices by health authorities is evolving, it may sometimes be difficult to identify these technologies which are indeed Medical Devices Regulation-approved
Embedding patient information links into primary care clinical systems for HCPs to send accredited health information from patient organisations to patients directly or signposting patients to useful resources and patient organisations for further support
Giving patients ownership and access to both their primary and secondary care components of their medical records
Allowing patients access to health information in bite-sized pieces at different times to ensure they stay regularly informed
Educating patients on treatment pathways and targets to ensure adherence to treatment
Patients have holistic needs and require not only clinical but also emotional and psychological support, which can be offered through online patient health communities such as the Stroke Association’s “My Stroke Guide”33 and the social media platform, HealthUnlocked34
Digital systems can allow vast amounts of data, such as BP measurements, to be obtained quickly in a way that patterns can be identified and can encourage patient self-management of care
Not all patients have a registered GP and digital solutions would not benefit every patient as not everyone is digitally literate or uses smart phones. Some patients may also mistrust technology, which can limit digitalised healthcare
Impact and considerations for HCPs
All HCPs would benefit from increased digitalisation across both primary and secondary care services
Treatment decisions and recommendations can differ between digital systems and the HCPs own clinical viewpoint, so it is important that patients are not left confused regarding condition management
There is a lot of fragmented health information available for patients and HCPs would benefit from understanding where all these resources are in order to support patients
Digital innovations can allow for more flexibility, and more timely and frequent patient consultations and arrangement of face-to-face appointments where needed, permitting HCPs to spend more time with select patients where required and reducing the need for travel
Regulatory considerations for digitalised healthcare
Clarity is needed on who has access to personal patient data and how it is used
Communication between the GP practice and the patient will be key and there must be consent, i.e. patients should be able to opt-out of digital services
The right pathways and rules must be in place within healthcare for clinicians, managers and patients for the use of digital systems with appropriate management of patient expectations
Organisational considerations for digitalised healthcare
Appropriate implementation of digital health management could impose an additional burden across primary care and requires investment into the resources and workforce needed to manage care
Responsibility for the successful delivery of services should be assigned in the event that digital population health management is established
There is an opportunity to innovatively use currently available data at scale to develop pathways to remove the burden of care and to aid earlier detection of CVD
An approach to digital innovation within healthcare is to start by focussing on smaller areas and seeking support from peers who may have experience of undertaking similar projects
The power of social media can be harnessed to engage patients and improve health outcomes
Socio-economic differences mean digital enablement is varied and there will always be hard-to-reach populations
Digital innovations should address health inequalities and promote equitable access to healthcare services
Digital technologies cannot completely replace traditional healthcare methods and patients must be advised that if they are feeling unwell, they should seek a face-to-face appointment by an appropriate HCP in a timely manner
Time saved through the use of digital technologies should be used to improve services
Concluding comments
The faculty members and delegates present represented stakeholders involved in CVD management, including HCPs working across both primary and secondary care, nurses, pharmacists, patient advocacy organisations and patient representatives, providing a good balance of experience, expertise and opinion. There was a clear consensus that CVD management within the NHS can be improved and streamlined through stronger partnerships between the NHS, pharmaceutical industry and patient advocacy groups; stronger communication between primary and secondary care; and the adoption of digital innovations aimed at benefitting patients and healthcare providers within the NHS. Most importantly, the patient should be at the heart of everything we do.
Key take-home messages
Collaborative working between the NHS, pharmaceutical industry, patient advocacy groups and patient representatives:
Consider engaging more than one industry partner in contracts when partnering with the pharmaceutical industry
Governance is critical when working with industry
There is no such thing as failure – even ‘failed’ projects still have learning potential
Patients should be central to all NHS-industry projects and can provide unexpected insights:
All projects should have a patient voice, which should equal to all other voices
Patient selection is key – involve the right patient and patient organisation throughout and in the right group
Patient power has the ability to bring about change
Synergistic working between primary and secondary care:
Better understanding, communication and appreciation for each other is needed between different professional roles:
Primary care needs to be aware of what is expected from secondary care, and vice versa
There is an inverse care pyramid when it comes to investment:
Investment is often top-heavy, aimed at secondary and tertiary care
Better funding is needed for primary care where most CVD prevention is managed
There is a need for clear pathways with consistent service provision across the country and more effective use of annual reviews
Healthcare digitalisation:
Patient consent is critical when considering the use of digital healthcare technologies
There is a need to consider who might be excluded (e.g. those who are less familiar with digital technology or those who don’t want to engage with it) and ensure they are not disadvantaged
Considerations around who will fund digital initiatives include:
Who will fund the initiatives?
Who will do the work?
How/where will the results be available?
How will different groups be incentivised?
Acknowledgements
Bayer would like to thank the chairs, faculty and delegates for their opinions, enthusiasm and engagement throughout the meeting.
Funding
The creation of this report was funded by Bayer plc.
Conflicts of interest
The following faculty members received an honorarium for participating at the meeting: AF, GF, CG, WH, VK, TL, JM, HW. No other conflicts of interest were reported.
4. Sheppard JP, Fletcher K, McManus RJ, Mant J. Missed opportunities in prevention of cardiovascular disease in primary care: a cross-sectional study. Br J Gen Pract 2014;64:e38–46. https://doi.org/10.3399/bjgp14X676447
8. Roberts S, Eaton S, Finch T, et al. The Year of Care approach: developing a model and delivery programme for care and support planning in long term conditions within general practice. BMC Family Practice 2019;20:153. https://bmcprimcare.biomedcentral.com/articles/10.1186/s12875-019-1042-4
12. Kuipers SJ, Nieboer AP, Cramm JM. Easier said than done: healthcare professionals’ barriers to the provision of patient-centered primary care to patients with multimorbidity. Int J Environ Res Public Health 2021;18:6057. https://doi.org/10.3390/ijerph18116057
13. Du X, Patel A, Anderson CS, Dong J, Ma C. Epidemiology of cardiovascular disease in China and opportunities for improvement. J Am Coll Cardiol 2019;73:3135–47. https://doi.org/10.1016/j.jacc.2019.04.036
23. Nadarajah R, Wu J, Frangi AF, Hogg D, Cowan C, Gale C. Predicting patient-level new-onset atrial fibrillation from population-based nationwide electronic health records: protocol of FIND-AF for developing a precision medicine prediction model using artificial intelligence. BMJ Open 2021;11:e052887. https://doi.org/10.1136/bmjopen-2021-052887
24. Nadarajah R, Wu J, Hogg D, et al. Prediction of short-term atrial fibrillation risk using primary care electronic health records. Heart 2023;109:1072–9. https://doi.org/10.1136/heartjnl-2022-322076
25. Nadarajah R, Alsaeed E, Hurdus B, et al. Prediction of incident atrial fibrillation in community-based electronic health records: a systematic review with meta-analysis. Heart 2021;108:1020–9. https://doi.org/10.1136/heartjnl-2021-320036
27. Sheikh A, Anderson M, Albala S, et al. Health information technology and digital innovation for national learning health and care systems. Lancet Digit Health 2021;3:e383–96. https://doi.org/10.1016/S2589-7500(21)00005-4
28. Carini E, Villani L, Pezzullo AM, et al. The impact of digital patient portals on health outcomes, system efficiency, and patient attitudes: updated systematic literature review. J Med Internet Res 2021;23:e26189. https://doi.org/10.2196/26189
29. Akbar S, Coiera, E, Magrabi F. Safety concerns with consumer-facing mobile health applications and their consequences: a scoping review. J Am Med Inform Assoc 2020;27:330–40. https://doi.org/10.1093/jamia/ocz175
Medical knowledge is constantly changing. As new information becomes available, changes in treatment, procedures, equipment and the use of drugs become necessary. The editors/authors/contributors and the publishers Medinews (Cardiology) Ltd have taken care to ensure that the information given in this text is accurate and up to date at the time of publication.
Readers are strongly advised to confirm that the information, especially with regard to drug usage, complies with the latest legislation and standards of practice. Medinews (Cardiology) Limited advises healthcare professionals to consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews (Cardiology) Limited cannot accept responsibility for any errors in prescribing which may occur.
The opinions, data and statements that appear are those of the contributors. The publishers, editors, and members of the editorial board do not necessarily share the views expressed herein. Although every effort is made to ensure accuracy and avoid mistakes, no liability on the part of the publisher, editors, the editorial board or their agents or employees is accepted for the consequences of any inaccurate or misleading information.
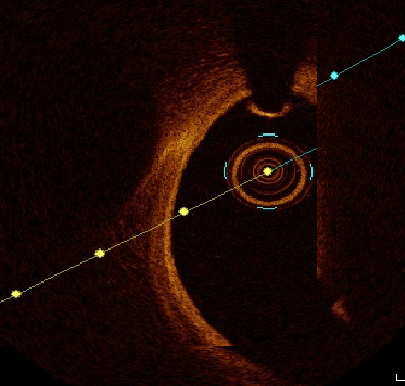
Thrombus is the main finding in most patients with acute coronary syndrome (ACS), the type of which potentially impacts the end result of the interventional procedure in terms of no reflow and edge dissection. Optical coherence tomography (OCT) is considered a precise intra-vascular tool to image thrombi and characterise its properties. We aimed to study the impact of thrombus type, as defined by OCT, on procedural outcome in ACS patients. In this retrospective study we enrolled 100 patients who were treated by percutaneous coronary intervention (PCI) with the guidance of OCT. We recorded demographic and clinical data of the whole studied cohort. Angiographic details and procedural data were noted. Baseline OCT study was performed before intervention and repeated post-intervention. Plaque characterisation was identified, and thrombi were defined as red or white thrombi. Acute angiographic outcome was defined with special emphasis on no reflow.
Male patients and ST-elevation myocardial infarction (STEMI) patients more often had white thrombi (58.1% and 71.2%, respectively). Cases with red thrombi had longer pain duration, which was statistically significant. Edge dissection was more frequent with red thrombus, 44.7% versus 32.1% with white thrombus, but the difference is not statistically significant, while 17% of patients with white thrombi were complicated by no-reflow phenomenon versus only 4.3% in patients with red thrombi, and this difference was statistically significant.
In conculsion, OCT-guided PCI is feasible and safe in ACS settings. OCT-guided intra-procedural differentiation of thrombus type is potentially beneficial in predicting acute procedural outcome.
Introduction
Acute coronary events are commonly caused by plaque rupture, erosion and, infrequently, calcific nodules. In the majority of patients with acute coronary syndrome (ACS), occlusive or sub-occlusive thrombus on top of plaque deformation is the main angiographic finding. Resolving acute thrombotic occlusion remains the cornerstone step in restoring adequate coronary perfusion. Blind dealing with thrombi, depending only on angiography, may be an obstacle to optimal myocardial perfusion and increase in-hospital morbidity and mortality.1–4
In the past, intravascular ultrasound (IVUS) and, more recently, optical coherence tomography (OCT) were frequently used for percutaneous coronary intervention (PCI) optimisation. Pre-PCI intra-vascular imaging, paved the way to precisely assess lesion significance, plaque features, necessity of lesion preparation and proper stent choice regarding width and length.4–6
Frequency domain OCT, as compared with IVUS, has 10 times better axial resolution, weak penetration capability (1–2 mm) and requires clearance of luminal blood. IVUS utilises ultrasound waves, in contrast to OCT, which depends on infrared light with minimal wavelength (1–3 µm) yielding magnificently higher resolution, but without satisfactory tissue penetration. The wavelength of red blood corpuscle is much greater than OCT wavelength, so backscattering occurs if luminal blood is not cleared first, before starting pullback. The combination of fine resolution with minimal penetration allows smooth distinction between plaque and abluminal surface, promoting OCT to be more superior in luminal measurements and clarifying thrombus composition.5–7
Frequency-domain OCT gives the privilege of going through the pathophysiology of unstable plaque, to differentiate between plaque rupture and erosion. Thrombi were defined as protrusions into the vessel lumen, and characterised according to their signal characteristics. White thrombus was identified as a signal-rich, low-backscattering thrombus, while red thrombus was identified as high-backscattering protrusions, with signal-free shadowing.8–14
PCI success might be hindered by the presence of intra-coronary thrombi, which influences acute procedural success in terms of improving coronary flow, thrombus prolapse and distal edge dissection. Impact of thrombus morphology and histology on procedural outcome has not been clearly studied. Depending on the physical characteristics of OCT, it is the most expected to precisely clarify thrombus type and study its impact on outcome.
We aimed to study the impact of thrombus type as defined by OCT on procedural outcome in ACS patients.
Method
Between January and June 2022, 760 cases of myocardial infarction were admitted to our centre, an invasive strategy including primary PCI was adopted in 524 patients. Of these, 131 patients underwent OCT-guided interventions based on operator experience and availability of probes; however, 31 patients were excluded either due to inappropriate image acquisition or due to excessive percutaneous transluminal coronary angioplasty (PTCA) with possible thrombus deformation. The remaining 100 patients met our inclusion criteria and were enrolled retrospectively. The exclusion criteria were: end-stage nephropathy, post-coronary artery bypass graft (CABG) patients, poor OCT image and patients with totally occlusive thrombi, even after wiring and thrombus aspiration. Written consent was achieved from every patient before participation.
Study population
Full history taking and precise clinical examination were done for all subjects. ST-elevation myocardial infarction (STEMI) was defined as typical chest pain for 30 minutes at least, arrival to centre with primary PCI facilities within 24 hours from onset of chest pain, ST-segment elevation >0.1 mV in two or more contiguous leads or newly detected left bundle-branch block. Non-ST-elevation myocardial infarction (NSTEMI) was defined as prolonged chest pain with positive cardiac biomarkers without ST-segment elevation. We defined the culprit vessel by electrocardiogram (ECG) criteria, or during angiogram as thrombus-containing vessel.13
During hospital course, serum creatinine was serially withdrawn. Duration of hospital course was recorded and early post-PCI negative outcomes were mentioned. Patients were followed in outpatient clinic for six months to detect major adverse cardiovascular events (MACE).
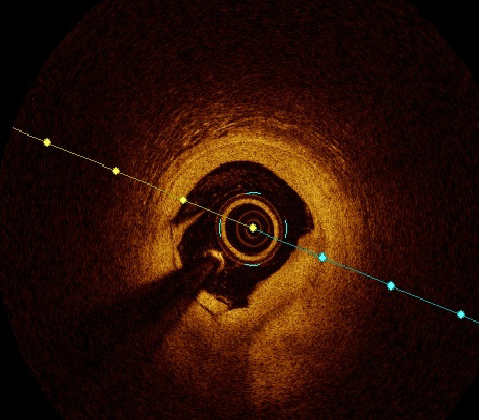
Figure 1. Optical coherence tomography (OCT) image of white thrombus
Patient preparation and OCT procedure
Antithrombotics were administered matching the latest universal guidelines. Drug-eluting stents were deployed. Lesion measurements were done in two orthogonal views and end-diastolic frames were selected, after giving at least 200 µg of nitrates. Post-OCT study, thrombotic lesions were categorised according to thrombus type into white and red thrombi.
A widely used frequency domain OCT system (Ilumien System, Inc., St. Jude Medical, USA) and a 0.014 inch wire (Image Wire, St. Jude Medical, USA) were used. Motorised wire pull-back at 10 mm/s was done during contrast injection. OCT measurements were mentored by an OCT specialist.2,15
Plaque morphology was defined through every frame; plaque rupture was defined as discontinuity of the fibrous capsule with plaque cavitary formations. Plaque erosion was defined as irregular lumen with thrombosis overlying intact cap. Thrombus was categorised to red and white thrombi according to composition, attenuation degree and backscattering. White thrombus was defined as a signal-rich, low-backscattering mass, while red thrombus was defined as high-backscattering protrusions inside the lumen, with signal-free shadowing as shown in figures 1 and 2.2,16,17
Figure 2. OCT image of red thrombus
The OCT analysis included luminal areas at the proximal and distal referenced segments, minimal lumen areas (MLA), minimal stent area (MSA). MSA exceeding 90% was considered optimal and ≥80% was acceptable. Dissection was defined as disruption of luminal intimal surface at the stent edges, and tissue prolapse was defined as protrusion of tissue through stent struts. Thrombolysis in Myocardial Infarction (TIMI) flow grade was recorded with special emphasis on occurrence of no reflow.11–14,18
No reflow is defined as inadequate tissue perfusion through a given segment of the coronary circulation without angiographic evidence of major vessel obstruction.19
The management protocol of no-reflow phenomenon was primarily pharmacological through the intra-coronary injection of glycoprotein IIb/IIIa inhibitors, verapamil, sodium nitroprusside, adenosine and, infrequently, epinephrine.20
It is worth mentioning that thrombus identification by OCT is highly subjective and operator dependent.21
Statistical analysis
Statistical testing was done using the Statistical Package for Social Sciences (SPSS) version 20. Continuous variables were presented as mean ± standard deviation (SD). Categorical variables were presented as numbers and percentages. Kolmogorov-Smirnov test for normal distribution was used to delineate between parametric and non-parametric data. Analysis of variance (ANOVA) test was used to assess relations between different variables. Univariate and multi-variate analysis was done. For all tests, a p value less than 0.05 was considered a significant difference.
Results
Demographic data and risk factors
Table 1. Demographics and risk profile
N=100
Number
%
Male gender
Female gender
86
14
86
14
Smokers
79
79
Hypertension
60
60
Diabetes mellitus
34
34
Hyperlipidaemia
48
48
Peripheral vascular disease
0
0
Cerebrovascular accident
6
6
Previous MI
7
7
Previous PCI
23
23
Mean ± SD
Range
Age, years
53.3 ± 11.3
28–85
Duration of symptoms, hours
9.7 ± 8.6
2–48
Key: MI = myocardial infarction; PCI = percutaneous coronary intervention; SD = standard deviation
One hundred patients were enrolled in this study. Patients’ demographic and clinical data are summarised in table 1. The mean age of studied patients was 53.3 years with males representing 86% of the studied cohort. Mean duration of chest pain was 9.7 hours. The most encountered risk factors were: cigarette smoking (79%), hypertension (60%), hyperlipidaemia (48%) and diabetes (34%), respectively. Six subjects had previously experienced cerebrovascular stroke.
Culprit lesion characteristics
Most of the patients in this study were STEMI patients (66%), two patients had acute pulmonary oedema and one patient was in cardiogenic shock. Of culprit lesions, 67% showed plaque rupture versus 33% with plaque erosion. Culprit vessel showed white thrombus in 53 subjects while 47 patients had red thrombus. No reflow was managed successfully using intra-coronary medications in 11 patients. Culprit lesion features are shown in table 2.
Procedural outcome
Drug-eluting stents were implanted in all subjects. Culprit vessel was left anterior descending (LAD) 73%, right coronary artery (RCA) 18%, left circumflex (LCx) 10%, left main trunk 3%, and diagonal 3%. OCT study post-intervention revealed mean stent expansion of 93.2% and mean MSA of 8 mm2. Limiting edge dissection was detected in six patients, tissue prolapse encountered in 38 cases and relevant mal-apposition necessitating optimisation in 56 patients (table 3).
Table 2. Culprit lesion morphology by optical coherence tomography (OCT)
Key: MSA = minimal stent area; SD = standard deviation
White thrombus versus red thrombus
The studied cohort was categorised according to thrombus type to two groups: white thrombus (53%) versus red thrombus (47%). Both groups were compared according to demographic and clinical data as shown in table 4. White thrombus was found to be significantly more evident (58.1%) among male patients (p=0.009). Younger age at presentation was significantly related to white thrombi, while smokers only showed a trend for that. There is no statistically relevant difference regarding thrombus type among hypertensive, diabetic, or dyslipidaemia patients. White thrombi were significantly evident in STEMI patients (71.2%, p=0.000 with odds ratio 11.5) while in NSTEMI patients, white thrombi represented a minority. Cases with red thrombi had longer pain duration before presentation as compared with white thrombi, which was significant statistically (13.7 ± 9.4 vs. 6 ± 4.6 hours) as shown in table 4.
Table 4. Comparison between demographic and clinical variables as regards thrombus type
Composite negative procedural outcome in relation to thrombus type
Thrombus prolapse shows no statistically significant difference between both types of thrombi. Edge dissection was noticed more frequently with red thrombus 44.7% versus 32.1% among cases with white thrombus and the difference is not statistically significant. No-reflow phenomenon complicated 17% of patients with white thrombi versus only 4.3% of patients with red thrombi, and this difference was statistically significant. Collectively, a higher percentage of combined negative outcomes was witnessed among cases of red thrombi, but with no statistical significance (table 5).
Table 5. Comparison between type of thrombus as regards negative outcomes detected by OCT
Red thrombus
Number (%)
White thrombus
Number (%)
p value
Prolapse
3 (6.4)
3 (5.7)
0.8
Dissection
21 (44.7)
17 (32.1)
0.1
No reflow
2 (4.3)
9 (17)
0.04
Combined negative outcome
23 (48.9)
23 (43.3)
0.5
Table 6. Logistic-regression model of thrombus type and the no-reflow phenomenon as a negative outcome during intervention
No reflow
Wald
p
Exp(B)
95%CI
Thrombus type
(Red as having risk)
0.22
0.05 to 1.1
3.5
0.059
p>0.05 not significant Key: CI = confidence interval
Confirming the previous data in table 5, a logistic-regression model was conducted supporting that no reflow was not statistically related to red thrombi as compared with white thrombi with an odds ratio of 0.22, as shown in table 6.
Six-month follow-up
Recruited subjects were followed for six months in outpatient departments, no MACE were encountered in terms of cardiovascular-related mortality, myocardial infarction or target vessel re-intervention, apart from minor bleeding in a single subject and two patients’ admission with decompensated heart failure.
Discussion
The essential target of this study was to check the feasibility of OCT guidance in differentiating red and white thrombi within culprit lesions of ACS, thereafter, which type is more related to negative procedural outcomes such as no reflow, edge dissection, thrombus prolapse and their combined end point.
Most of the ACS patients in our study were presenting with STEMI (n=66). Plaque rupture was encountered in 77% of patients, where it represented 83% of STEMI cases, while plaque erosion represented 64% of NSTEMI patients. This finding is considered a rehearsal of what Guagliumi et al., Fang et al., and Dai et al. found in their studies.22–24
Before discussing our targeted differentiation of thrombus types to red and white, a very important clarification has to be done, because of which a lot of ACS patients were not recruited to our study. OCT-guided thrombus and plaque analysis was done only if at least TIMI flow ≥2 was achieved after culprit lesion wiring ± thrombus aspiration, but not after PTCA, fearing that PTCA may alter plaque morphology or add to negative outcomes as no reflow before our analysis. This pathway was also done by Amabile et al. when they studied thrombus burden by OCT before and after deferral of PCI in STEMI patients in 2014.25
White thrombus was more evident in male gender (58.1%) and also in young age (<53 years, our mean age) whereas smokers only trended for that. This can be attributed to early time of presentation in young male smoker patients who are not preconditioned to ischaemia at the time of presentation, when the thrombus is mainly formed of platelets, before fibrin meshwork is well established and red blood cells profoundly settle in the clot. Other atherosclerotic risk factors such as hypertension, diabetes or dyslipidaemia were not statistically different between the two types of thrombi.
White thrombi were consistently present in STEMI patients (71.2% of STEMI patients) but they represented a minority in NSTEMI patients, while the reverse was encountered with red thrombi. The group of patients with red thrombi had a longer duration of pain before presentation (13.7 ± 9.4 hours) compared with the group with white thrombi (6 ± 4.6 hours), which may be a dart to our point that fibrin mesh maturation and red blood cell settlement present after a longer time.
Despite a paucity of data about thrombus type in relation to different demographic, clinical and angiographic presentations, shades of our data were echoed in a review of literature published by Khandkar et al. in 2021 about the mechanistic differences among ACS patients, how to detect by imaging (where OCT surely was recommended as the best) and how this can affect the targeted procedure plan.26
As for acute procedural negative outcomes, our study focused on no reflow, thrombus prolapse and dissection. White thrombi were found to be strongly related to occurrence of no reflow, which happened in 17% of white thrombi patients versus only 4.3% of red thrombi patients. Again, this was not stated as solidly as we state before, but suggested by Khandkar et al. by relating ruptured fibrous cap to STEMI patients to white thrombi, then relating no reflow to STEMI patients.26
Logically, if no-reflow phenomenon is mostly due to micro-thrombi dislodgement to distal circulation after PTCA or stent deployment, as stated in almost all literature discussing this phenomenon, this shall happen more commonly with the platelet-rich white thrombi than with the fibrin and red blood cell-rich red thrombi. This could also explain the good response of no reflow to intracoronary glycoprotein IIb/IIIa inhibitors to stop platelet aggregation and white thrombus propagation.20,22
Regarding thrombus prolapse, there was no significant difference between the two types of thrombi, while dissection was encountered more with red thrombi patients but without statistical significance. Also, the combined negative outcome showed no difference between the two thrombi types.
This study is not a limitation-free study, being a non-randomised study, selection bias and other forms of bias cannot be excluded. Moreover, the study was not empowered to detect differences in MACE or other clinical outcomes. So, larger randomised clinical studies are needed to clarify these gaps of evidence. Despite these limitations, we do believe that our data are potentially adding to the body of evidence supporting the use of OCT as the best intra-vascular imaging modality to optimise acute procedural outcomes in ACS patients.
Conclusion
OCT-guided PCI is feasible and safe among patients with ACS. OCT-guided intra-procedural differentiation of thrombus type is potentially beneficial in predicting acute procedural outcome.
Key messages
Optical coherence tomography (OCT) is feasible in setting of acute coronary syndrome (ACS) when used by experienced hands
OCT can perfectly optimise angiographic outcome post-percutaneous coronary intervention (PCI)
White thrombus is a major risk factor of no reflow
Anticipation of no reflow is possible with intravascular imaging
Conflicts of interest
None declared.
Funding
None.
Study approval
The study had ethical approval number FMASU R 162 2022.
References
1. Virmani R, Burke AP, Kolodgie FD et al. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 2000;20:1262–75. https://doi.org/10.1161/01.ATV.20.5.1262
2. Jia H, Aguirre AD, Abtahian F et al. In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography. J Am Coll Cardiol 2013;62:1748–58. https://doi.org/10.1016/j.jacc.2013.05.071
3. O’Donoghue M, Braunwald E, Boden WE et al. Early invasive vs conservative treatment strategies in women and men with unstable angina and non-ST segment elevation myocardial infarction: a meta-analysis. JAMA 2008;300:71–80. https://doi.org/10.1001/jama.300.1.71
4. Cannon CP, Demopoulos LA, Weintraub WS et al.; TACTICS (Treat Angina with Aggrastat and Determine Cost of Therapy with an Invasive or Conservative Strategy) – Thrombolysis in Myocardial Infarction 18 Investigators. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med 2001;344:1879–87. https://doi.org/10.1056/NEJM200106213442501
5. FRagmin and Fast Revascularisation during InStability in Coronary artery disease (FRISC II)Investigators. Invasive compared with non-invasive treatment in unstable coronary-artery disease: FRISC II prospective randomised multicentre study. Lancet 1999;354:708–15. https://doi.org/10.1016/S0140-6736(99)07349-3
6. Fox KA, Henderson RA, Poole-Wilson PA et al.; Randomized Intervention Trial of unstable Angina Investigators. Interventional versus conservative treatment for patients with unstable angina or non-ST-elevation myocardial infarction: the British Heart Foundation RITA 3 randomized trial. Lancet 2002;360:743–51. https://doi.org/10.1016/S0140-6736(02)09894-X
7. Nakazawa G, Joner M, Finn AV et al. Delayed arterial healing and increased late stent thrombosis at culprit sites after drug-eluting stent placement for acute myocardial infarction patients: an autopsy study. Circulation 2008;118:1138–45. https://doi.org/10.1161/CIRCULATIONAHA.107.762047
8. Yamamoto M, Okamatsu K, Inami S et al. Relationship between neointimal coverage of sirolimus-eluting stents and lesion characteristics: a study with serial coronary angioscopy. Am Heart J 2009;158:99–104. https://doi.org/10.1016/j.ahj.2009.04.016
9. Kramer MC, Rittersma SZ, de Winter RJ et al. Relationship of thrombus healing to underlying plaque morphology in sudden coronary death. J Am Coll Cardiol 2010;55:122–32. https://doi.org/10.1016/j.jacc.2009.09.007
10. Chieffo A, Caussin C, latib A et al. A prospective, randomized trial of intravascular-ultrasound guided compared to angiography guided stent implantation in complex coronary lesions: the AVIO trial. Am Heart J 2013;165:65–72. https://doi.org/10.1016/j.ahj.2012.09.017
11. Kang SJ, Park GM, Cho YR et al. Intravascular ultrasound predictors for edge restenosis after newer generation drug-eluting stent implantation. Am J Cardiol 2013;111:1408–14. https://doi.org/10.1016/j.amjcard.2013.01.288
12. Ino Y, Matsuo Y, Kubo T et al. Optical coherence tomography predictors for edge restenosis after everolimus-eluting stent implantation. Circ Cardiovasc Interv 2016;9:e004231. https://doi.org/10.1161/CIRCINTERVENTIONS.116.004231
13. Prati F, Burzotta F, Romagnoli E et al. Clinical impact of OCT findings during PCI: the CLI-OPCI II study. JACC Cardiovasc Imaging 2015;8:1297–305. https://doi.org/10.1016/j.jcmg.2015.08.013
14. Prati F, Regar E, Mintz GS et al. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis. Eur Heart J 2010;31:401–15. https://doi.org/10.1093/eurheartj/ehp433
15. Witzenbichler B, Weisz G, Maehara A et al. Relationship between intravascular ultrasound guidance and clinical outcomes after drug-eluting stents: the Assessment Of Dual Antiplatelet Therapy with Drug-Eluting Stents (ADAPT-DES) study. Circulation 2014;129:463–70. https://doi.org/10.1161/CIRCULATIONAHA.113.003942
16. Ali ZA, Généreux P, Maehara A et al. Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): a randomized controlled trial. Lancet 2016;388:2618–28. https://doi.org/10.1016/S0140-6736(16)31922-5
17. Liu J, Mintz GS, Maehara A et al. An integrated TAXUS IV, V, and VI intravascular ultrasound analysis of the predictors of edge restenosis after bare metal or paclitaxel-eluting stents. Am J Cardiol 2009;103:501–06. https://doi.org/10.1016/j.amjcard.2008.10.010
18. Prati F, Guagliumi G, Mintz GS et al. Expert review document part 2: methodology, terminology and clinical applications of optical coherence tomography for the assessment of interventional procedures. Eur Heart J 2012;33:2513–20. https://doi.org/10.1093/eurheartj/ehs095
20. Ramjane K, Han L, Jin C. The diagnosis and treatment of the no-reflow phenomenon in patients with myocardial infarction undergoing percutaneous coronary intervention. Exp Clin Cardiol 2008;13:121–8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2586408/
21. Kaivosoja T, Liu S, Dijkstra J et al. Comparison of visual assessment and computer image analysis of intracoronary thrombus type by optical coherence tomography. PLoS One 2018;13:e0209110. https://doi.org/10.1371/journal.pone.0209110
22. Guagliumi G, Capodanno D, Saia F et al. Mechanisms of atherothrombosis and vascular response to primary percutaneous coronary intervention in women versus men with acute myocardial infarction: results of the OCTAVIA study. JACC Cardiovasc Interv 2014;7:958–68. https://doi.org/10.1016/j.jcin.2014.05.011
23. Fang C, Dai J, Zhang S et al. Culprit lesion morphology in young patients with ST-segment elevated myocardial infarction: a clinical, angiographic and optical coherence tomography study. Atherosclerosis 2019;289:94–100. https://doi.org/10.1016/j.atherosclerosis.2019.08.011
24. Dai J, Xing L, Jia H et al. In vivo predictors of plaque erosion in patients with ST-segment elevation myocardial infarction: a clinical, angiographical, and intravascular optical coherence tomography study. Eur Heart J 2018;39:2077–85. https://doi.org/10.1093/eurheartj/ehy101
25. Amabile N, Hammas S, Fradi S et al. Intra-coronary thrombus evolution during acute coronary syndrome: regression assessment by serial optical coherence tomography analyses. Eur Heart J Cardiovasc Imaging 2015;16:433–40. https://doi.org/10.1093/ehjci/jeu228
26. Khandkar C, Madhavan MV, Weaver JC et al. Atherothrombosis in acute coronary syndromes – from mechanistic insights to targeted therapies. Cells 2021;10:865. https://doi.org/10.3390/cells10040865
Remote delivery of cardiovascular rehabilitation (CR) has been vital during the COVID pandemic when restrictions have been placed on face-to-face services. In the future, CR services are likely to offer alternatives to centre-based CR, including digital options. However, little is known about the digital access and confidence of CR service users, or their CR delivery preferences.
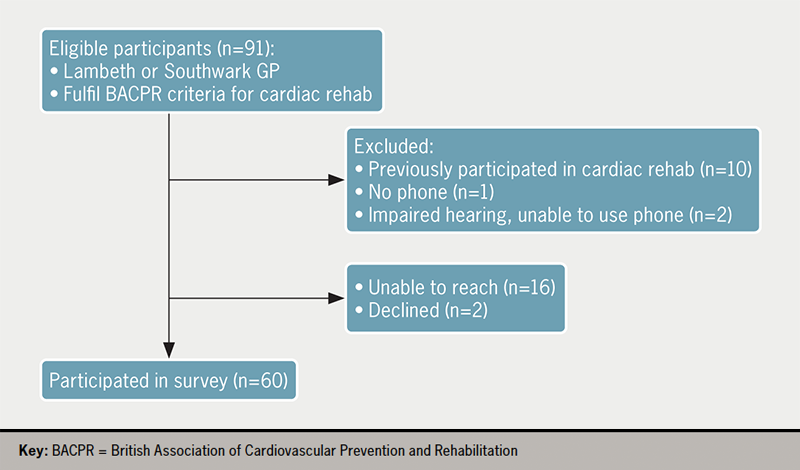
A telephone survey was conducted of those referred for CR in the London boroughs of Lambeth and Southwark (n=60) in which questions were asked about digital access and confidence, as well as current and future delivery preferences for their CR.
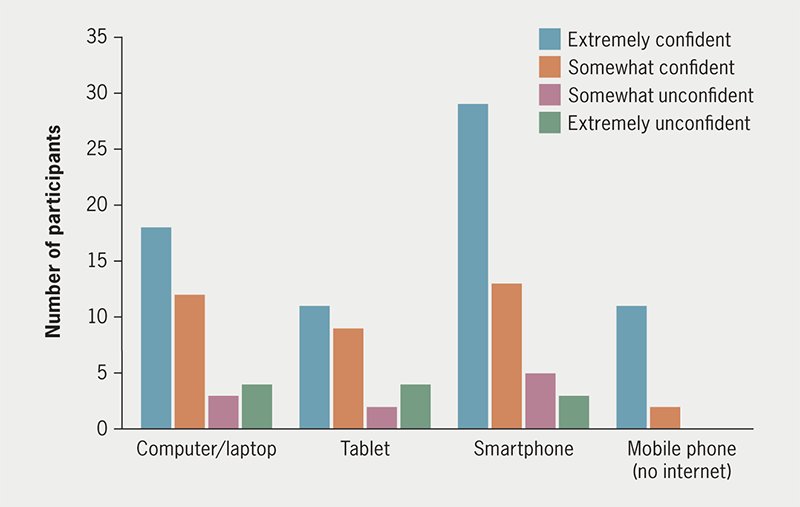
Between March and July 2021, 60 service-users met the inclusion criteria and were recruited for a telephone survey (mean age 60 ± 11.2 years). Of those, 82% had regular access to a smartphone, 60% to a computer or laptop and 43% to a tablet device. A high proportion of service users perceived themselves to be ‘extremely’ or ‘somewhat’ confident to use their devices. Thirty-nine (65%) service users would currently prefer a face-to-face assessment, rising to 82% once the perceived COVID-19 threat and restrictions are less. Preferences for accessing exercise were equally split between face-to-face and remotely supported independent exercise, with low interest in digital options. Delivery preferences for education, relaxation and peer support were more heterogeneous with interest in all delivery options.
In conclusion, digital access and confidence in CR service users was good. Redesigning CR services to offer more rehabilitation delivery options, aligned with patient choice may increase uptake and further trials are needed to assess the impact.
Introduction
The COVID-19 pandemic resulted in significant disruption to the delivery of cardiovascular rehabilitation (CR) services in the UK, following staff redeployment to acute services and limited access to workspaces.1 With restrictions being placed on face-to-face services due to concerns about safety and disease transmission, many CR services rapidly moved to remote delivery.2 These adjustments led to a significant drop in group-based exercise (–36%) and group-based education (–29%) with a corresponding increase (+16%) in CR staff supported self-managed options.3
In the future, those with cardiovascular disease are likely to be offered alternatives to centre-based CR, including hybrid models that include digital health interventions. Adopting a broader range of evidence-based delivery methods may improve uptake and outcomes of rehabilitation.4
Digital health interventions have been defined as “technology that enables the delivery of care through means such as the use of the internet, wearable devices and mobile apps”.5 A recent literature review reveals that, in CR, the most common modalities used for digital health interventions were smartphones or mobile devices (65%), web-based portals (58%) and email/SMS (35%).5
There is a growing evidence-base for the efficacy of digital CR, with more than 30 unique telehealth trials conducted internationally.6 In the most recent meta-analysis, the use of telehealth for CR was significantly associated with reduced hospitalisations and cardiac events compared with usual care.6
Despite the efficacy of digital CR options being well-established, little is known about the access CR service users have to digital options and their confidence using them. Frederix et al.7 provide a comprehensive overview of the challenges and barriers to large-scale digital health deployment in cardiology in Europe, and comment that typical characteristics associated with lower digital health usage include older age, low health literacy and low socioeconomic and health status. This corresponds with some of the key predictors of digital exclusion identified by the Good Things Foundation Report.8
This survey seeks to better understand the digital access and confidence of those referred for CR in the London boroughs of Lambeth and Southwark, and their delivery preferences, both at the time of the survey and once the perceived COVID-19 threat and restrictions are less.
Method
The CR team at Guy’s and St. Thomas’ NHS Foundation Trust (GSTT) in London, UK, conducted a telephone survey of patients referred for CR between 15 March 2021 and 2 July 2021. Service users met the inclusion criteria if they fulfilled eligibility for CR, according to the recommendations set out in the British Association of Cardiovascular Prevention and Rehabilitation (BACPR) standards and core components,9 and had a general practitioner (GP) within the catchment area of the trust. The GSTT therapies clinical governance, quality assurance and ethical framework approved the project’s method regarding consent, patient confidentiality, anonymity and minimisation of risk of harm to subjects.
A first draft of the survey was piloted with three volunteer CR service users to assess the appropriateness and understanding of survey items, then minor modifications were made in response to their feedback before being used for the study population. Eligible participants were contacted after they had already received an initial telephone contact from the CR team (offering early recovery advice and support). The first consecutive 60 respondents willing to participate in the survey were recruited. Service users were informed their participation and responses would not influence their own future care. Sociodemographic data (age, gender, ethnicity) and clinical details were collected from the referral forms and confirmed on the telephone calls.
The first question participants were asked was whether they had regular access to any of the following four devices: a mobile phone with no internet, a smartphone or internet-enabled phone, a tablet device and a computer or laptop. They were then asked to rate their confidence using each of the devices they had regular access to using a four-point Likert scale (“extremely confident”, “somewhat confident”, “somewhat unconfident” or “extremely unconfident”).
Participants were given a brief explanation as to what a CR assessment involved, and three delivery options were outlined (face-to-face, a telephone assessment, or a video-call assessment). A description of each option was given (see standardised script in appendix). The extra considerations (social distancing, use of face masks) for a face-to-face appointment were outlined. It was explained that a video call would require access to an internet-enabled device and would be conducted via a secure platform. Participants were asked for their preference for how they would best like to access their CR assessment both at the time of the survey, and once the perceived COVID-19 threat and restrictions were less, and were asked to give the main reason for their responses.
Appendix. Description of standardised assessment and core component delivery options given to survey participants
Assessment
Face-to-face: This would involve meeting one of our team at the hospital. Social distancing within the hospital is advised and all staff, patients and visitors are expected to wear a simple face mask, and to sanitise their hands on entering the hospital building. Staff would wear further PPE (gloves, apron and eye protection) when they are required to have closer contact for physical measurements. Any shared equipment is cleaned.
Assessment by a video call: This would require an internet-enabled device with a web-cam and would be conducted via a secure platform. No physical measurements of your health or fitness capacity can be taken.
Assessment by a telephone call: This would require a telephone. No physical measurements of your health or fitness capacity can be taken.
Exercise component
Face-to-face small group class: We have reduced class size numbers to a maximum of 8 participants, and redesigned the exercise class format to allow for social distancing. Any shared exercise equipment would be cleaned between use. Social distancing within the hospital is advised and all staff, patients and visitors are expected to wear a simple face mask, and to sanitise their hands on entering the hospital building. Staff would wear further PPE (gloves, apron and eye protection) when they are required to have closer contact for physical measurements.
Live virtual small group class: This would be a small group class participating together via a secure platform. This would require an internet-enabled device with a web-cam. You would need to keep your web-cam on and other participants would be able to see you and your background.
Pre-recorded exercise session: This would require an internet-enabled device. You would be able to view and follow a pre-recorded exercise session at a time that suits you.
Home-based programme support with telephone calls: This would involve you being provided with a home-based programme, e.g., some personalised home-based exercises or a walking programme. This would be supported by some regular phone-calls from a member of our team.
Health education component
Face-to-face small group session: We have reduced class size numbers to a maximum of 8 participants to allow for social distancing. Social distancing within the hospital is advised and all staff, patients and visitors are expected to wear a simple face mask, and to sanitise their hands on entering the hospital building.
Live virtual small group session: This would be a small group class participating together via a secure platform. This would require an internet-enabled device with a web-cam. You would need to keep your web-cam on and other participants would be able to see you and your background.
Pre-recorded session: This would require an internet-enabled device. You would be able to view and follow a pre-recorded health education session at a time that suits you.
Home-based health education with telephone calls: This would involve you being provided with health information in the form of some written information or a link to a webpage. This would be supported by some regular phone-calls from a member of our team.
Relaxation
Face-to-face small group session: We have reduced class size numbers to a maximum of 8 participants to allow for social distancing. Social distancing within the hospital is advised and all staff, patients and visitors are expected to wear a simple face mask, and to sanitise their hands on entering the hospital building.
Live virtual small group session: This would be a small group class participating together via a secure platform. This would require an internet-enabled device with a web-cam. You would need to keep your web-cam on and other participants would be able to see you and your background.
Pre-recorded audio relaxation: You would be sent a link (in a text or email) to an audio relaxation track that you could listen to at a time that suits you.
Relaxation information sheet: You would be provided with health information in the form of some written information or a link to a webpage.
Peer support
Face-to-face small group session: We have reduced class size numbers to a maximum of 8 participants to allow for social distancing. Social distancing within the hospital is advised and all staff, patients and visitors are expected to wear a simple face mask, and to sanitise their hands on entering the hospital building.
Live virtual small group session: This would be a small group class participating together via a secure platform. This would require an internet-enabled device with a web-cam. You would need to keep your web-cam on and other participants would be able to see you and your background.
A peer support buddy: You would be paired with a volunteer support buddy to make telephone contact with.
Participants were also asked for their delivery preferences for each component of the CR outpatients programme in turn (exercise, education, relaxation, and peer support) both at the time of the survey, and once the perceived COVID-19 threat and restrictions were less. Delivery options for each component included small-group face-to-face sessions, taking part from home in live virtual-group sessions, following pre-recorded sessions, being provided with some written information, or a home exercise programme to follow independently with telephone support, or to voice that they were not interested in participating in that component. Once again, participants were asked for the main reason for each of their responses. The data were summarised using descriptive statistics and frequency histograms, and responses to open questions were themed. Binary logistic regressions were used to examine the relationship between participants’ gender, age and ethnicity, and whether the participants had access to an internet-enabled device or not. All assumptions required for the linear-regression analysis were met. Statistical significance was defined as a two-tailed value of p<0.05.
Results
Ninety-one service users were eligible for CR during the study period. Of those, 10 who had previously participated in CR were excluded as it was felt their prior experience of CR would influence their responses. One service user had no phone, two had hearing impairments making use of phone difficult, two declined to take part, and 16 could not be reached despite two calls on separate occasions (figure 1).
The survey sample (n=60) had a mean age of 60 years (standard deviation [SD] 11.1, range 37–88) and 78% of participants were male. Reasons for referral and ethnicity are shown in table 1. Participant characteristics were similar to those reported in the National Audit of Cardiac Rehabilitation quarterly report on gender and ethnicity for the period of January to June 2021 for the catchment covered by our NHS Trust,10 indicating the survey sample is representative of those who started a core CR programme within this time period.
Digital access and confidence
Most participants had regular access to a smartphone (82%), and/or a computer or laptop (60%), with less having access to a tablet (43%) or mobile phone with no internet (27%). Comparing age, gender and ethnicity, only age was a significant predictor for whether the participants had an internet-enabled device. As age increased, likelihood of having an internet-enabled device decreased (adjusted odds ratio [AOR] 1.089, 95% confidence interval [CI] 1.01 to 1.174, p=0.017). Neither ethnicity (AOR 0.192, 95%CI 0.73 to 18.24, p=0.14) nor gender (AOR 0.119, 95%CI 0.514 to 12.34, p=0.26) were significant predictors of access to a digital device.
The majority of participants self-reported they were either ‘extremely’ confident or ‘somewhat’ confident using the devices they regularly accessed (figure 2).
Delivery preferences
The delivery preferences for the CR assessment and each component of rehabilitation, both at the time of the survey and when the perceived COVID-19 threat and restrictions were less, are detailed in table 2.
Figure 2. Self-reported confidence using digital devices
Table 2. Delivery preferences of survey participants
Delivery preferences
At time of survey (n=60)
Once COVID-19 threat and restrictions lessened (n=60)
Assessment
Face-to-face
39 (65%)
48 (82%)
Telephone
16 (27%)
8 (13%)
Video call
5 (8%)
4 (7%)
Exercise component
Face-to-face small-group
25 (42%)
34 (57%)
Live virtual
2 (3%)
0
Pre-recorded virtual
3 (5%)
1 (2%)
Home-based independent
25 (42%)
21 (35%)
Not interested
5 (8%)
4 (7%)
Health education
Face-to-face small-group
19 (32%)
24 (40%)
Live virtual
4 (7%)
4 (7%)
Pre-recorded virtual
6 (10%)
6 (10%)
Information leaflets
20 (33%)
15 (25%)
Not interested
11 (18%)
11 (18%)
Relaxation
Face-to-face small-group
13 (22%)
16 (27%)
Live virtual
1 (2%)
1 (2%)
Pre-recorded audio
21 (35%)
19 (32%)
Information leaflets
4 (7%)
3 (5%)
Not interested
21 (35%)
21 (35%)
Peer support
Face-to-face small-group
19 (32%)
22 (37%)
Live virtual
2 (3%)
1 (2%)
Paired with volunteer buddy
3 (5%)
1 (2%)
Not interested
36 (60%)
35 (58%)
When asked about delivery preferences for their CR assessment, 39 participants (65%) stated they would prefer their assessment face-to-face at the time of their survey, with this rising to 48 participants (82%) once the perceived COVID-19 threat and restrictions were less. Two themes emerged for preferring face-to-face assessment – the first was that participants wanted the reassurance of a physical assessment, and the second was the enhanced quality of an in-person interaction. Those preferring a remote assessment commonly stated their main reason was the convenience of not having to attend a hospital appointment, and/or that this reduced their risk of COVID-19 exposure and was following the ‘stay at home’ UK Government guidance.
At the time of the survey, equal numbers of participants expressed preference for accessing a face-to-face small-group exercise session (42%) and following a home-exercise programme with telephone support (42%), with lower numbers preferring digital options. Once the perceived COVID-19 threat and restrictions were less, the number preferring a face-to-face group increased (57%) with preferences for all the other options falling.
The most commonly cited reasons for preferring a face-to-face small-group class at the time of the survey were ‘feeling safer when exercising under supervision’, ‘increased motivation to exercise’ and ‘being with others’. These remained the most cited reasons participants gave for preferring small-group classes once the perceived COVID-19 threat and restrictions were less. Those who preferred to follow a home-exercise programme with telephone support did so for a number of reasons – themes that emerged included ‘the convenience of being at home’, being able to ‘go at my own pace’ or ‘exercise in my own way’ and ‘the reduced risk of COVID-19’. All these reasons were consistently given across the two time-points, except the ‘reduced risk of COVID-19’, which was understandably cited less often once the perceived COVID-19 threat and restrictions were less.
Those choosing live virtual exercise as their preferred choice at the time of the survey did so because of the ‘reduced cost compared to a hospital attendance’, ‘feeling safer than a hospital visit’ and ‘being more motivated if exercising with others’. No participants chose live virtual exercise as an option once the perceived COVID-19 threat and restrictions were less. Those who chose a pre-recorded virtual exercise session did so because of the convenience and reduced risk of COVID-19. Once the perceived COVID-19 restrictions and threat lessened, only one participant chose pre-recorded virtual exercise, the reason cited was for convenience.
The majority of participants were interested in receiving some health education as part of their CR programme. Once again, similar numbers expressing preference for face-to-face group delivery (32%) and written information (33%), with lower interest in digital options. Once the perceived COVID-19 threat and restrictions were less, there was a shift towards more participants wanting face-to-face health education delivery (40%). Eleven participants (18%) expressed no interest in health education at the time of the survey, this proportion remained the same once the perceived COVID-19 threat and restrictions lessened.
Reasons most commonly cited for preferring face-to-face group delivery of health education were themed around ‘improved quality of interaction’, which participants felt would be ‘easier to understand’. Many participants also felt they would benefit from questions from their peers and reported higher motivation to attend group health education. These reasons were reported consistently across both time points.
The most cited reason for preferring to receive health information in written form was ‘the convenience/not having to miss work’. Convenience was also cited by those preferring live and pre-recorded digital options, along with ‘preferring a digital format to paper’ and interest in live digital as it is ‘more interactive than pre-recorded’.
Thirty-nine participants (65%) were interested in accessing relaxation in some format as part of their CR programme. The majority (35%) expressed a preference for a pre-recorded relaxation audio track, with some (22%) preferring a face-to-face small-group relaxation session. There was low interest in live digital relaxation or relaxation in a written format. The proportion across the delivery options did not substantially change once the perceived COVID-19 threat and restrictions eased.
The main reasons cited for preferring a pre-recorded relaxation audio track were the ‘convenience’ and the ability to then ‘access it in my own time/whenever I wish’. Those preferring face-to-face group relaxation felt it would be ‘easier to learn in this format’. Those stating no interest in relaxation, either felt no need as ‘stress is not a problem for me’, or already practised a form of relaxation, referencing yoga, meditation, or Tai Chi.
When asked if they would like access to peer support at the time of the study, 60% of participants declined, with this proportion not changing once the perceived COVID-19 restrictions and threat lessened. Themes for declining included ‘already having enough support from family, friends and professionals’ and ‘not being interested in hearing of others’ problems’. Those participants who expressed interest in attending a face-to-face group for peer support spoke of the improved ‘quality of in-person interactions’ and that it ‘might help someone else’. Interest in peer support from a buddy patient by telephone or a live virtual-group peer-support session was low across both time points.
Discussion
This survey provides contemporary data on the digital access and confidence of those referred for CR from our population in the London boroughs of Lambeth and Southwark. Overall, access to internet-enabled devices in the surveyed population was good, as was self-reported confidence using these devices. Age was a significant predictor for whether participants had an internet-enabled device, however, as only a small number of the participants did not have an internet-enabled device (n=8), this was an underpowered group and, therefore, difficult to draw firm conclusions from. This finding does, however, agree with previous studies already described.7,11 A survey of 282 individuals eligible for CR in Australia found that age had an important independent association with the use of mobile technology after adjusting for education, employment and confidence. The youngest group (<56 years) was over four times more likely to use any mobile technology than the oldest (>69 years) age group (odds ratio [OR] 4.45, 95%CI 1.46 to 13.55).11
Another recent paper evaluated the digital access and behaviours of pulmonary rehabilitation (PR) participants in the early months of the COVID-19 pandemic. It revealed that, while 48% of participants reported confidence using the internet, 31% of participants had never accessed the internet, and 29% reported no interest in accessing any component of PR via a web-based app. They reported that older age, but not sex, was associated with a lack of internet access (OR 0.94, 95%CI 0.91 to 0.99, p<0.01).12 The authors raised concerns about the readiness of PR users to adopt web-based rehabilitation options.
Despite good digital access and confidence, the majority of those surveyed had a preference for accessing their CR assessment face-to-face, both at the time of the survey and, in increasing numbers, once the perceived COVID-19 threat and restrictions were reduced. So, although it would appear it is feasible to offer digital alternatives to face-to-face CR assessment, retaining choice of mode of assessment appears important in maintaining access.
Delivery preferences of participants for each of the core components of CR were varied. These findings have implications for those redesigning CR services as we emerge from the COVID-19 pandemic restrictions. In terms of increasing access and participation in CR, digital and remote options provide a number of opportunities to appeal to groups who might decline participation in conventional face-to-face CR. Those who have difficulty taking time off work, those who experience difficulties or high expense with transport to a CR centre, and those receiving the majority of their care in a separate location to where their CR is offered, may prefer to undertake a digital option rather than decline CR. In line with the recommendations published in previous National Audit of Cardiac Rehabilitation (NACR) reports,13 digital CR options can help to provide female-only CR sessions for those preferring this option, which may increase recruitment of more women across all conditions to CR.3 Utility of home-based CR for patients with heart failure14 is currently being developed digitally to offer greater innovation in recruiting heart failure patients to CR. Digital options are encouraged to optimise recruitment and increase uptake,3 but more prospectively conducted research is needed to ensure that this is high quality and effective as a form of CR delivery, and will need strategies to prevent digital exclusion of those without the means or confidence of using these digital technologies.
Epstein et al.15 describe a hybrid model where CR is divided into both face-to-face sessions and virtual, digitally enabled follow-up with home-based remote-monitoring. Redesign of CR pathways in this manner could provide the sought after in-person care and supervision required initially, while leveraging technology at a later stage to enhance care. Providers should use patient preferences to guide which (if any) components of CR should be converted to virtual means in the future. Perhaps the perfect future CR model has elements of both; optimising the areas we can with the best technological solutions, while maintaining our in-person contact, which many service users value highly.
Limitations
This survey had a small sample size, and was a single-centre study, so the results will not represent all those eligible for CR, or be generalisable across the UK. Female gender and non-white/Caucasian ethnicity are under-represented and the sample size may be too small and under-powered to detect differences to achieve statistical significance. A further limitation of this study is that information regarding social deprivation or employment status of participants was not collected, so the influence of these variables could not be analysed. Those surveyed were basing their delivery preferences on a brief description of the options potentially available, and not on any lived experience of them. A follow-up survey of satisfaction following completion of their rehabilitation programme would provide more information of acceptability of delivery modes. The views of subjects suitable for CR but declining to participate after an initial telephone contact from the CR team were not captured in this study. Such individuals may represent the 50% of eligible patients in the UK who do not take up CR and might consider participating if more digital options were available.
Conclusion
In conclusion, this survey indicates digital access and confidence was good in those from Lambeth and Southwark who were referred for CR, which offers an important opportunity to increase access. As COVID-19 restrictions ease, it will be important not to return to conventional centre-based CR delivery only, but to offer genuine choice of mode of delivery to increase access and uptake and reach the ambitious target of 85% set in the NHS long-term plan4.
Key messages
Digital access and confidence in the survey sample was good
The majority of participants expressed preference for their cardiac rehabilitation (CR) assessment to be delivered face-to-face. Delivery preferences for the core components were more varied
Redesigning CR pathways to offer more rehabilitation delivery options, aligned with patient choice may increase national CR access and uptake, and more trials are needed to assess the impact
Conflicts of interest
None declared.
Funding
The authors are grateful for a grant from the Association of Chartered Physiotherapists in Cardiovascular Rehabilitation (ACPICR) project development fund which funded the main author to collect the survey data, and create a short report for dissemination to ACPICR members.
Study approval
The GSTT therapies clinical governance, quality assurance and ethical framework approved the project’s method regarding consent, patient confidentiality, anonymity and minimisation of risk of harm to subjects. No ethical approval was required.
Patient consent
Participants verbally consented to their views being used in the study, knowing their personal information was anonymised.
Acknowledgements
We would like to express our thanks to the patients who participated in this survey.
2. O’Doherty AF, Humphreys H, Dawkes S et al. How has technology been used to deliver cardiac rehabilitation during the COVID-19 pandemic? An international cross-sectional survey of healthcare professionals conducted by the BACPR. BMJ Open 2021;11:e046051. https://doi.org/10.1136/bmjopen-2020-046051
4. Dala HM, Doherty P, McDonagh STJ et al. Virtual and in-person cardiac rehabilitation. BMJ 2021;373:n1270. https://doi.org/10.1136/bmj.n1270
5. Wongvibulsin S, Habeos EE, Huynh PP et al. Digital health interventions for cardiac rehabilitation: systematic literature review. J Med Internet Res 2021;23:e18773. https://doi.org/10.2196/18773
6. Jin K, Khonsari S, Gallagher R et al. Telehealth interventions for the secondary prevention of coronary heart disease: a systematic review and meta-analysis. Eur J Cardiovasc Nurs 2019;18:260–71. https://doi.org/10.1177/1474515119826510
7. Frederix I, Caiani EG, Dendale P et al. ESC e-Cardiology Working Group position paper: overcoming challenges in digital health implementation in cardiovascular medicine. Eur J Prev Cardiol 2019;26:1166–77. https://doi.org/10.1177/2047487319832394
9. British Association of Cardiac Prevention and Rehabilitation. BACPR standards and core components for cardiovascular disease and prevention and rehabilitation. London: BACPR, 2023. Available from: https://www.bacpr.org/resources/publications
11. Gallagher R, Roach K, Sadler L et al. Mobile technology use across age groups in patients eligible for cardiac rehabilitation: survey study. J Med Internet Res 2017;5:e161. https://doi.org/10.2196/mhealth.8352
12. Polgar O, Aljishi M, Barker RE et al. Digital habits of PR service-users: implications for home-based interventions during the COVID-19 pandemic. Chron Respir Dis 2020;17:1479973120936685. https://doi.org/10.1177/1479973120936685
14. Dalal HM, Taylor RS, Jolly K et al.; on behalf of the REACH-HF investigators. The effects and costs of home-based rehabilitation for heart failure with reduced ejection fraction: the REACH-HF multicentre randomized controlled trial. Eur J Prev Cardiol 2019;26:262–72. https://doi.org/10.1177/2047487318806358
15. Epstein E, Patel N, Maysent K, Taub PR. Cardiac rehab in the COVID era and beyond: mHealth and other novel opportunities. Curr Cardiol Rep 2021;23:42. https://doi.org/10.1007/s11886-021-01482-7
Transthoracic echocardiography (TTE) is used to assess for evidence of infective endocarditis (IE). Inappropriate patient selection leads to significant burden on healthcare services. We aimed to assess effectiveness of cardiology consultant vetting of TTE requests for suspected IE in reduction of unnecessary scans. All inpatient TTE requests querying IE over a six-month period were vetted. Clinical information and pathology results were reviewed, and requests were either accepted, deferred, or rejected. A total of 103 patients had TTE requested: 39 (38%) were accepted for scan; four cases of IE were confirmed on TTE. There were 62% of patient requests rejected and not scanned, and no cases of IE subsequently diagnosed. Thus, consultant vetting of TTE requests for suspected IE is an effective way to safely reduce unnecessary scans and enables cost-effective streamlining of echocardiography services.
Introduction
Infective endocarditis (IE) is a potentially fatal infection of the endothelial lining of cardiac structures, with an estimated incidence between 42 and 67 cases per million in England.1 Mortality without treatment approaches 100%.2 The 1994 Duke diagnostic criteria for IE merge clinical, echocardiographic, and microbiological information, and the European Society of Cardiology (ESC) recommend use of the Duke criteria in conjunction with multi-disciplinary team (MDT) opinions of cardiologists and microbiologists.3,4 Initial investigations include three sets of blood cultures and transthoracic echocardiography (TTE), which remains the ESC recommended first-line imaging for IE. In the UK, TTE use is rising by 6% each year.3 The COVID-19 pandemic caused unprecedented strain on NHS resources, including echocardiography services, with 20 times as many patients waiting over six weeks for outpatient TTE.4 The Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust (DBTH) cardiology department sought to assess the effectiveness of consultant vetting of TTE requests for suspected IE in reducing unnecessary scans.
Method
Between 1 June and 31 December 2020, all DBTH TTE requests querying endocarditis were vetted by a consultant cardiologist. Local microbiologists offered criteria (table 1) advising if TTE was mandatory, strongly recommended, or to be considered. Requests were accepted, deferred, or rejected. For rejected requests, a letter was sent to referring clinicians. Common reasons for rejection included an alternative clear source of infection on another imaging modality (such as computed tomography), or preliminary cultures showing no significant or contaminant growth following discussion with microbiology. Deferred requests were accepted or rejected after gathering further information. All scans were to the level of the British Society of Echocardiography minimum dataset. All patients were followed up for 16–23 (median 19) months. In deceased patients medical certificate of cause of death (MCCD) data were collected. Data were analysed on Microsoft Excel 2020 (Microsoft, Washington) and assessed for normality: non-parametric data are presented as median (interquartile range, IQR); parametric data are presented as mean ± standard deviation (SD).
Table 1. Criteria advising if transthoracic echocardiography (TTE) was mandatory, strongly recommended, or to be considered
TTE essential
Staphylococcus aureus bacteraemia
Candidaemia
Typical microorganism from 2 separate cultures
Single positive culture: Coxiella burnetii or antibody titre >1:800
TTE strongly recommended
Single positive culture: Enterococcus with unclear source
Prosthetic valve or ICED device: ≥2 cultures with the same Coagulase negative staphylococci
Intravascular catheter-related bacteraemia with positive cultures 72-hours after line removal
Fever and: new valvular murmur; stroke; CCF; new conduction disturbance, unexplained emboli; peripheral IE stigmata
Abscesses (renal, splenic, cerebral, vertebral) of unknown source
Pyrexia of unknown origin; protracted history of sweats/weight loss/malaise associated with pre-existing at-risk cardiac lesions
Consider TTE
Single set of cultures: Streptococcus viridans
Single positive culture: HACEK organisms; Streptococcus gallolyticus
Table 2. Distribution of results for accepted and rejected requests
Results
Accepted requests
Rejected requests
Number of requests, n (%)
46 (36)
82 (64)
Individual patients, n (%)
39 (38)
64 (62)
Mean age, years
61
66
Female, n
15
19
Male, n
24
45
Mean requests, n ± SD
1.2 ± 0.5
1.3 ± 0.6
Mean initial number of cultures, n ± SD
1.9 ± 0.8
1.6 ± 1.2
No evidence of IE, n (%)
30 (76.9)
63 (98.4)
Possible vegetations, n (%)
5 (12.8)
1 (1.6)
Definite vegetations, n (%)
4 (10.3)
0 (0)
Deceased, n
9
21
IE on MCCD, n
2
0
Key: IE = infective endocarditis; MCCD = medical certificate of cause of death; SD = standard deviation
There were 128 TTE requests for 103 individuals. Of those, 39 patients were accepted for scan and 64 patients were not scanned. There were 15 scan requests deferred until a final decision was made. Unscanned accepted patients were either discharged or died prior to scan. Rejected but scanned patients had scans organised before request cancellation. Table 2 demonstrates the distribution of results for the accepted and rejected requests. There were four patients diagnosed with acute IE during the study period: all had Staphylococcus aureus bacteraemia, of whom two died with IE listed on MCCD.
Discussion
Our results demonstrate consultant vetting reduced the number of patients requiring echocardiography by 62% (64 patients not scanned). No cases of IE were subsequently diagnosed in rejected requests. This reduction confers approximate savings of £4,380, enabling 64 re-allocated sonographer hours. Furthermore, rationalising scans decreases the burden of overdiagnosis.5
A higher number of blood cultures were collected in accepted patients. While three separate sets of cultures can be difficult to obtain and cause patient distress, the low diagnostic yield of TTE necessitates combination with positive cultures to raise the index of suspicion.6 Deferring requests allows such supporting evidence to become available. However, patients with difficult intravenous access may have delayed diagnosis and subsequent inferior outcomes.7
In 128 requests, nine scans had evidence of IE; four cases were diagnosed. Of the five individuals with possible vegetations, four (80%) patients were alive at 18 months. The deceased patient had serial equivocal TTE with MCCD stating multi-organ failure from urosepsis. In two (40%) patients, Lambl’s excrescences were seen but clear alternative diagnoses were made. One patient had previously been treated for IE elsewhere, with our repeat TTE only showing possible evidence of IE. One patient had serial TTE (trans-oesophageal scans being unavailable due to COVID-19), one scan with a definite vegetation, repeated negative cultures and ultimately an alternative diagnosis. The four other individuals with definite vegetations, seen on five scans, all died. They had Staph. aureus bacteraemia accounting for the high mortality.8 IE was the cause of death in two (50%); hospital-acquired pneumonia and liver failure in the remainder.
The mortality rate was high; 9 (23.1%) of 39 accepted individuals and 21 (32.8%) of 64 rejected individuals died, possibly a result of small study effect or selection bias. In unscanned deceased patients, no MCCD listed IE. Theoretically, request rejection could cause failure to detect fatal IE in unscanned patients. However, considering untreated mortality, those surviving beyond follow-up could not have had IE.
We recognise the limitations of our study. Specifically, lack of pre-pandemic data, as COVID-19 may have influenced presentation and management. Vetting clinicians could only review available information and deferring requests may delay diagnosis and treatment. The cost savings should be offset with consultant vetting time and requesting time for deferred/repeated requests.
Conclusion
Cardiologist vetting of TTE requests for suspected IE demonstrates a safe way to reduce unnecessary scans, provided there is clear communication between all members of the IE multi-disciplinary team.
Key messages
Transthoracic echocardiogram (TTE) is a cornerstone of diagnosis for infective endocarditis, however, TTE is often requested inappropriately or with inadequate information
We investigated whether the vetting of requests for TTE to look for infective endocarditis by experienced consultant cardiologists could provide a safe and effective way of reducing the burden of investigations
Vetting TTE requests reduced the number of scans performed by 62%; no patients that were not scanned died from infective endocarditis at follow-up
Experienced cardiologists, along with support from microbiologists, can reduce the need for TTE by reviewing requests, provided there are adequate clinical data available
Conflicts of interest
None declared.
Funding
None.
Study approval
This study was internally registered. Local research ethics committee approval was sought and deemed unnecessary.
Acknowledgements
We recognise the contributions of Catherine Wright, Alex Smith, Howard Briggs, Naomi Bairstow, Sarah Ritzmann and Dr Abraham Chacko from DBTH cardio-respiratory department, and Dr Bala Subramanian from the DBTH microbiology department.
References
1. Quan TP, Muller-Pebody B, Fawcett N et al. Investigation of the impact of the NICE guidelines regarding antibiotic prophylaxis during invasive dental procedures on the incidence of infective endocarditis in England: an electronic health records study. BMC Med 2020;18:84. https://doi.org/10.1186/s12916-020-01531-y
6. Sivak JA, Vora AN, Navar AM et al. An approach to improve the negative predictive value and clinical utility of transthoracic echocardiography in suspected native valve infective endocarditis. J Am Soc Echocardiogr 2016;29:315–22. https://doi.org/10.1016/j.echo.2015.12.009
8. Khan MZ, Khan MU, Syed M, Balla S. Trends in microbiology data and association with mortality in infective endocarditis (2002–2017). Am J Cardiol 2021;142:155–6. https://doi.org/10.1016/j.amjcard.2020.12.055
This paper summarises ‘Share The Pressure’, a project that developed and piloted a scalable model for engaging patients on the benefits of risk factor control for healthy ageing; training healthcare professionals (HCPs) in cardiovascular disease (CVD) risk communication; and improving the shared decision-making process between nurses, pharmacists and patients. The study features the use of a CVD risk tool called Heart Age, which has been shown to effectively motivate risk factor reduction in individuals.
The study team engaged virtually with patients and HCPs through established relationships within the community, third sector, charities, and social media. In addition, patients living with high blood pressure (hypertension) participated via online focus groups and surveys, which provided insight into patients’ preferences for conveying CVD risk, quantification of intervention benefits, side effects and processes to facilitate shared decision-making.
This insight gained from the focus group and survey data informed adaptations made to the Heart Age tool to provide ‘years off’ – or lowering of heart age – benefits for different aspects of blood pressure lowering, focusing on the independent and joint benefits of medication management and lifestyle.
The study piloted a training programme for nurses and pharmacists to support them in communicating and framing risk and intervention benefits.
The study trained 1,148 HCPs from 37 countries over 17 sessions. Post-training survey results of HCPs indicated an increase in self-rated knowledge and a strong likelihood of applying information learned to their clinical practice. In addition, the Heart Age users found the personalised report and Heart Age test results very motivating for patients with high blood pressure.
Introduction
High blood pressure (BP) is a major risk factor for reduced healthy life-expectancy and unhealthy ageing. While it is fundamentally treatable, it is currently not optimally managed. To meet national public health targets, patients must play an active role in their decisions about how best to manage their own BP through lifestyle change and drug treatment.1,2
This paper summarises ‘Share The Pressure’ (STP), a project that developed and piloted a scalable model for engaging patients on the benefits of risk factor control for healthy ageing; training healthcare professionals (HCPs) in cardiovascular disease (CVD) risk communication and to engage patients around the benefits of understanding risk factor control to enable healthy ageing (age-based approaches have been demonstrated to be motivating for patients). Thus, to improve shared decision-making processes between nurses, pharmacists, and patients. The study features the use of a CVD risk tool called Heart Age,3 which has been shown to effectively motivate risk factor reduction in individuals.4
HCPs must establish an effective dialogue with patients around the benefits of living a healthy and long life and the importance of BP control. The STP project focused on nurses and pharmacists who engage with patients in primary care and community settings. The project aimed to enable nurses and pharmacists to participate in meaningful dialogue with patients living with high BP about its impact on CVD risk and equip patients with the tools to allow them to understand the benefits of different risk reduction approaches.
Effective control of BP and increasing physical activity are known to impact healthy life-expectancy in patients diagnosed with hypertension. However, to have a meaningful impact on this condition – a crucial driver of healthy ageing – patients must play an active role in decisions about the management of their disease. This ‘shared decision-making process’ sits at the heart of national hypertension control guidelines – and arguably the fundamental ethics of patient care.
Reducing high BP cannot be achieved without patients actively participating in lifestyle changes or medication adherence. Patients’ decisions about lifestyle changes and medication should be communicated in the context of their actual and perceived CVD risk. However, evidence shows that a mismatch exists between the perception of risk and measured risk in patients at all levels of CVD risk. For example, the REACT (Reassessing European Attitudes about Cardiovascular Treatment) survey demonstrated that the individual perception of CVD risk in five European countries was lower than the measured risk.5
The revised National Institute for Health and Care Excellence (NICE) guideline, Hypertension in adults: diagnosis and management,6supports a shared decision-making approach to care. The guideline includes a patient decision aid (PDA) for hypertension in adults to support HCPs to explain trade-offs between reducing the risk of CVD and the disutility of taking daily medicines, monitoring requirements and the possibility of side effects; and help people with hypertension make more informed decisions about whether to take medicines at all; whether to add extra medicines to their treatment; and, if so, which medicines they would like to try.7
Study design
The STP project used a mixed-methods study design, over five project stages. Stages 1 and 2 focused on identifying current approaches and barriers to optimal patient communication. This served to generate insights, engage stakeholders, and promote their role in the project’s ongoing development and provide stimulus to adapt the CVD risk tool (Heart Age) that we planned to use in the programme. This project built on previous work applying the use of Heart Age to patient populations in the community and within healthcare practices. Previous work has primarily been conducted in the UK, Australia and the US; however, we have also implemented Heart Age in Singapore and the Middle East. Furthermore, the Joint British Societies for Cardiovascular Disease have implemented a form of Heart Age in their CVD risk app, which has been deployed by the former agency, Public Health England.
During stage 3, adaptations were made to the Heart Age tool derived from the findings from stage 2. These modifications were tested with a small group before launching a final version of Heart Age. Both this stage and the subsequent stage (stage 4), focused on the development, testing and roll-out of a training programme for HCPs.
Stage 5 focused on evaluating and identifying a sustainability plan for longer-term usage after the pilot was completed.
Before these stages, we established a steering group to provide strategic and tactical project oversight.
Results
The STP project commenced in January 2020. By March 2020, the COVID-19 pandemic forced governments worldwide – including the four nations of the UK – to introduce population-wide physical distancing restrictions. The combination of these restrictions and the significant diversion of healthcare resources towards the management of COVID-19 resulted in substantial reductions in screening and routine patient care. Furthermore, due to the considerable pressure facing primary-care professionals during the pandemic, the Quality and Outcomes Framework (QoF) was discontinued in 2020,8 including metrics related to BP measurement.
The project methodology was adapted in response to the pandemic, most notably by transferring to virtual engagement with HCPs. As a result, 1,148 HCPs from 37 countries engaged over 17 training sessions, significantly surpassing the target number of 60 nurses and pharmacists in England and Ireland; 918 participants were from the UK and 16 from Ireland. In addition, post-training feedback via electronic survey was positive, rating knowledge before training at 3.2/5 to 4.4/5 afterwards and 4.7/5 for how likely to use what they had learned in clinical practice.
This was an important finding as significant knowledge gaps were revealed in a blood pressure quiz offered over social media, via nursing groups on Facebook and Twitter (table 1). To note, the quiz was available to all, so some respondents were not HCPs.
Which of these medications would be a recommended first-line choice for a 48-year-old male of South Asian Origin?
31%
At which of these levels of cardiovascular risk would antihypertensive medications be indicated in stage one hypertension?
36%
Which two types of blood pressure readings are required to assess for hypertension?
53%
What should you do first before adding in a new antihypertensive medication?
54%
Which two of these sets of readings would confirm a diagnosis of stage one hypertension?
63%
If a diagnosis of stage one hypertension is made, which two things needs to happen next?
69%
How do we assess target organ damage?
73%
What should you do before measuring blood pressure? (choose as many as you want to)
90%
What could be a helpful strategy to support your patients to improve their blood pressure?
96%
Patient engagement was more complicated digitally due to challenges and illness associated with COVID-19. However, despite these challenges, survey and focus-group results indicated that patients feel strongly that there is a need for better shared decision-making with their HCPs. They also provided valuable feedback about what resources they needed and the applicability of Heart Age tool.
Patient insights (pre-Heart Age tool adaptation)
In total, there were 65 patients engaged across a survey (n=62) and in-depth interviews (n=3). The age spread was 41.5% (n=27) 31–50 years, 38.5% (n=24) 51–65 years, and 20% (n=13) 66–80 years. Most were female (69% n=44), with 18 (28%) males, one (1.5%) transgender and one (1.5%) who preferred not to say. Ethnicity was 95.5% (n=61) white, 3% (n=2) Asian and 1.5% (n=1) Black.
Patients complained about their HCP’s lack of explanation about their high BP and the impact of medications. They shared that there is minimal discussion about lifestyle from HCPs during appointments; instead, dialogue is focused mainly on medication. Also, patients observed that medical jargon is widespread and somewhat meaningless, e.g. stage 1 or 2 hypertension. Subsequently, patients turn to social media groups for explainers, such as the Facebook Blood Pressure UK group (from which we recruited).
Patient feedback also clarified that Heart Age resonates with them, given their age and their feelings of susceptibility due to being older. It must be accompanied by information that equips and prepares them for a conversation with an HCP about their BP. When survey respondents answered the question “Would you agree that you and your healthcare professional worked together to decide how to manage your blood pressure?” only 8.33% said strongly agree, 31.67% somewhat agreed, and 45% somewhat or strongly disagreed.
The Heart Age tool has been widely used and previously studied through randomised trials.4,9-11 These studies have found Heart Age to be an effective CVD risk communication tool and that it can also increase patients’ physical activity. As a result, it has been adopted for use by leading organisations in numerous countries. Through STP, we harness HCP and patient insights to refine the Heart Age tool and enable it to be more patient-centric and fit for use.
The project also showed that patients found HCP’s reliance on and use of medical jargon is a substantial information access barrier and that it can be a prompt for them to turn to social media groups to understand their health condition. This poses a significant threat as it exposes them to information and recommendations that may not be evidence-based. Therefore, online information about the STP platform needed to be accessible, easy-to-read and informative, while making clear the current evidence about lowering BP.
Patients also observed a fragile balance between receiving too much information before an appointment with their HCP, which can be overwhelming, and receiving too little information, which prevents them from appropriately preparing questions to ask. Information offering excessive detail before an appointment can lead to anxiety. However, it remains essential to know what questions to ask your doctor, e.g. how long might I be on medication? And/or what are the side effects? Patients felt that having the correct information available before and after appointments was important to manage anxiety at different stages and take away afterwards.
Engagement with HCPs illustrated an appetite to increase and enhance their knowledge around hypertension and use tools such as Heart Age to improve their engagement with patients. Unfortunately, in the COVID-19 context, suspension of QoF prevented HCPs from immediately putting Heart Age into practice with patients.
Discussion
The STP project found that patients want to know their Heart Age results, are interested in understanding hypertension and want to be more engaged in decision-making about their management in partnership with their HCPs (table 2). Furthermore, the project was conducted during the unprecedented COVID-19 pandemic. As a result, patients acknowledged the importance of hypertension as a critical non-communicable disease risk factor, a risk factor for serious illness from COVID-19 and the importance of playing an active role in their health.
Table 2. What patients want to know more about to help manage their blood pressure
Questions and answers
Mean response
N=62
1. What would help you make a decision about whether to take tablets for your blood pressure? (could choose more than one answer)
Knowing how important blood pressure is
55.17%
How serious my own risk of a heart attack or stroke is
74.14%
Understanding how taking tablets every day can reduce my risk of a heart attack or stroke
51.72%
What the side effects might be of taking tablets every day
46.55%
How to remember to take my tablets every day
12.07%
None of these
8.62%
2. What would help you make a decision about whether to become more active or take exercise to manage your blood pressure? (could choose more than one answer)
Knowing how important blood pressure is
39.66%
How serious my own risk of a heart attack or stroke is
55.17%
Understanding how doing physical activity or exercise every day for 30 minutes can reduce my risk of a heart attack or stroke
67.24%
What different types of physical activity/exercise can help
51.72%
How I can fit 30 minutes of physical activity/exercise into my normal day
29.31%
3. Which of the following works best for you in making decisions about your blood pressure?
A healthcare professional makes the decision for me
12.07%
A healthcare professional gives me all the information I need and we make a decision together
65.52%
A healthcare professional gives me all the information I need and then I make the decision myself
22.41%
Table 3. What healthcare professionals say would help them to help patients
What would help you to help patients?
Training
Webinars – break out rooms to work through case studies and experience
Recorded and live
Drop-in sessions
How to take a BP
Diagnosis – ABPM/HBPM
Decision-making on treatment (target organ damage/assessing risk)
Using Heart Age
Improving BP through lifestyle changes
Medicines for management
Reviewing hypertension
Educating patients to monitor BP at home
Practical support
Useful websites
Where to check if BP monitors any good
Video clips to share
How to take a BP
How to measure waist circumference
Links to useful websites
Hypertension plan for patients
Diet information
Key: ABPM = ambulatory blood pressure monitoring; BP = blood pressure; HBPM = home blood pressure measurement
The project also found that HCPs want to deepen their understanding of hypertension and improve their ability to support patients living with it (table 3).
They were keen on further training and engaged well with the project’s adapted training model. Although the original project methodology included face-to-face training to demonstrate the Heart Age tool, there was no loss in the perceived value when presented to HCPs during virtual training sessions. HCPs indicated that they could visualise using it to aid their clinical management and conversations with patients. It was only due to COVID-19 and the subsequent effect on the clinical work environments, e.g. the suspension of QoF and the lack of in-person care, that HCPs could not use the tool immediately after participating in a training session.
STP has enabled both patients and HCPs to think differently about hypertension. As a result, the 1,148 HCPs in the training programme increased their knowledge of BP and risk communication score from 3.5/5 to 4.4/5, and likelihood of using what they have learned is 4.7/5 (appendix 1).
The project modification relating to the delivery of training sessions to HCPs, i.e. from face-to-face to virtual training, ultimately allowed the project to exceed the target number of HCPs engaged in numbers of participants across 37 countries reached (appendix 2). This has dramatically enhanced accessibility by HCPs and enabled those who may otherwise have been unable to access face-to-face training. Although much of healthcare has accelerated the use of digitally based care since the start of the COVID-19 pandemic, care must be taken to ensure people who do not have access to technology are not being digitally excluded.
Limitations
The COVID-19 pandemic meant recruitment of patients had to deviate from the original plan of through HCPs. Most of the people involved were from a BP Facebook group, which then limited who could respond. While there was good inclusion of women, there was a very low uptake from people with Asian or Black heritage. Most of the HCPs trained were nurses and so the outcome of both usability of the tool and potential improvement of doctors’ knowledge is unknown. The survey had age ranges for people to select, which meant the mean age of patients could not be calculated. Patients who participated tended to be younger.
Appendix 1. Feedback from healthcare professionals in the training programmeAppendix 2. Number of healthcare professionals by country who attended the training
Conclusion
The implications for clinical practice from STP are multiple. The project has demonstrated an innovative working model that is fit for purpose within the clinical practice of the NHS. Evidence from the project indicates interest and knowledge acquisition around hypertension and risk communication by HCPs in the UK and other countries. The challenge now is to see if STP can be used to support patients in the future and help the NHS with the post-COVID-19 recovery. The project was supported by Viatris Inc., a biopharmaceutical company, and demonstrates the importance of private–public partnership models in combating hypertension – a major risk factor for CVD and the most common non-communicable disease globally. Share The Pressure 2 started in August 2022, tailored to people of African and African-Caribbean heritage with funding by The Burdett Trust for Nursing.
Key messages
While hypertension remains a major risk factor for reduced life-expectancy and healthy ageing, there remains a significant gap in healthcare professionals’ knowledge
Patients want to understand how their blood pressure affects their heart attack or stroke risk and be involved in shared decision-making about their care
Share The Pressure, utilising the Heart Age tool, supported by a training programme, is ideal for delivering both
Conflicts of interest
MN is a director at Smart Health Solutions. MC is employed by Younger Lives Ltd., a company specialising in the development of risk communication and behaviour change tools to use with patients. SD is a full-time employee of Viatris Inc. JH is a contractor at Smart Health Solutions.
Funding
The project was supported by Viatris Inc., a biopharmaceutical company.
Study approval
All participants were fully informed of the requirements of the study and what was asked of them prior to participation. We required active consent and this was free to be removed at any stage. The purpose of the research was to evaluate current understanding of blood pressure, the Heart Age tool and discussions with their healthcare professional. Online data provided were anonymous and interviews conducted under strict confidentiality with personal details removed as soon as the interviews were terminated. To ascertain whether we required a formal NHS ethics review we used the tool at https://www.hra-decisiontools.org.uk to get guidance from the NHS Health Research Authority. The feedback from the tool was that an ethical review was not required.
4. Lopez-Gonzalez AA, Aguilo A, Frontera M et al. Effectiveness of the Heart Age tool for improving modifiable cardiovascular risk factors in a Southern European population: a randomized trial. Eur J Prev Cardiol 2015;22:389–96. https://doi.org/10.1177/2047487313518479
6. National Institute for Health and Care Excellence. Hypertension in adults: diagnosis and management. NG136. London: NICE, 2019. Available from: https://www.nice.org.uk/guidance/ng136
9. Soureti A, Hurling R, Murray P, van Mechelen W, Cobain M. Evaluation of a cardiovascular disease risk assessment tool for the promotion of healthier lifestyles. Eur J Cardiovasc Prev Rehabil 2010;17:519–23. https://doi.org/10.1097/HJR.0b013e328337ccd3
10. Soureti A, Murray P, Cobain M, van Mechelen W, Hurling R. Web-based risk communication and planning in an obese population: exploratory study. J Med Internet Res 2011;13:e100. https://doi.org/10.2196/jmir.1579
11. Bonner C, Raffoul N, Battaglia T, Mitchell JA, Batcup C, Stavreski B. Experiences of a national web-based heart age calculator for cardiovascular disease prevention: user characteristics, Heart Age results, and behavior change survey. J Med Internet Res 2020;22:e19028. https://doi.org/10.2196/19028
Transcatheter edge-to-edge repair (TEER) was first performed in 2003, and is now established across the developed world as an effective, minimally invasive treatment option for patients with mitral regurgitation (MR). Multiple large registries have established the efficacy of mitral TEER in patients with primary or degenerative MR in whom surgery is considered prohibitive or high risk, while ongoing randomised-controlled trials will determine its role in younger and lower-risk patients. In patients with secondary or functional MR, in whom mitral valve surgery is not routinely recommended, the pivotal COAPT trial showed a profound reduction in both mortality and heart failure hospitalisation in carefully selected patients.
NHS England approved the routine commissioning of mitral TEER in 2019, and following a substantial delay, due in large part to the COVID pandemic, the procedure is now widely available across the UK. This review article describes the TEER procedure, currently available devices, the underlying evidence base, and the key facts needed for clinicians to understand who, how, and where to refer patients for consideration of mitral TEER. The emerging role of TEER in patients with severe symptomatic tricuspid regurgitation is also considered.
Background
Transcatheter edge-to-edge repair (TEER) is a percutaneous catheter-based technique that aims to replicate the Alfieri stitch, a surgical technique in which a suture is applied at the site of the regurgitant jet between the facing free margins of the anterior and posterior leaflets of the mitral valve (MV), creating a double orifice valve without residual prolapse of one or both leaflets. After a 10-year wait for funding, TEER has now finally become widely available across the National Health Service (NHS). This article will provide an overview of the TEER procedure, describe currently available technology, and outline who and how to refer for edge-to-edge repair, including the required imaging.
Nomenclature
Transcatheter edge-to-edge repair has evolved as the preferred terminology for this procedure, and may be applied to its use in both the mitral and tricuspid valves. However, percutaneous MV leaflet repair has also been widely employed, including in both the NHS England (NHSE) commissioning statement, and National Institute for Health and Care Excellence (NICE) guidance.1,2 The term mitral clip was previously commonly used in reference to the original, and previously only, available device. While all of these terms will still often be heard in clinical practice, transcatheter edge-to-edge repair is now accepted worldwide as the standard nomenclature.
Current status of TEER in the UK
The number of TEER procedures performed globally has increased rapidly over the past 15 years, with more than 10,000 patients treated annually in the US alone.3 In contrast, TEER has been slow to take off in the UK. Europe-wide data from 2019 showed that the number of procedures performed in the UK was just 100, equating to 1.5 per million population, fewer than any other Western European country (figure 1). This historical under-provision is attributable to a lack of funding by NHSE and the devolved authorities. Following completion of a limited observational assessment of TEER in just three centres in England, commissioning approval of TEER for the treatment of degenerative MR by NHSE was finally given in July 2019.1
Figure 1. Transcatheter edge-to-edge repair (TEER) procedure numbers per million population in 2019 in Western Europe
Table 1. Transcatheter edge-to-edge repair (TEER) centres in the UK
Region
Centre
Lead clinician
London
Barts
Mike Mullen
Brompton / Harefield
Rob Smith
Hammersmith
Mike Bellamy
King’s
Jonathan Byrne
St Thomas’s
Tiffany Patterson
South East
Brighton
David Hildick-Smith
Oxford
Sam Dawkins
Southampton
Michael Mahmoudi
South West
Bristol
Mark Turner
East
Papworth
Patrick Calvert
Midlands
QE Birmingham
Sagar Doshi
Glenfield, Leicester
Jan Kovac
Royal Stoke
Adrian Large
Wolverhampton
Saib Khogali
Nottingham
Will Smith
North West
Manchester
Mamta Buch
Liverpool
Clare Appleby
Yorkshire and North East
Leeds
Chris Malkin
Middlesbrough
Paul Williams
Newcastle
Mohaned Egred
Scotland
Glasgow
Angela Ghattas
Edinburgh
David Northridge
Wales
Cardiff
Richard Anderson
Northern Ireland
Belfast
Colm Owens
The subsequent planned roll-out of TEER was delayed further by the COVID pandemic. However, across the course of 2021 and 2022, additional specialist centres across the country have gradually received approval from NHSE to perform TEER. This key minimally invasive intervention for MV disease is now available to patients across England and the devolved nations. Table 1 shows the centres currently performing TEER in the UK.
The mitral TEER procedure
TEER is performed under general anaesthesia (GA) and is guided by trans-oesophageal echocardiography (TOE) and fluoroscopy.
Percutaneous ultrasound-guided femoral venous access is performed for introduction of the large-bore delivery sheath, with catheter-based pre-closure using suture-based devices. The procedure requires a targeted TOE-guided high posterior trans-septal puncture to enable sufficient height above the MV to perform grasping, usually between 4 and 5 cm. The trans-septal sheath is advanced into the left atrium (LA) and exchanged for a stiff support wire. The device guiding catheter is advanced into the LA to enable delivery of the clip or implant system, which is then steered towards the MV. The precise strategy of edge-to-edge repair will depend on the nature and extent of the mitral regurgitation (MR). MR reduction is measured in real-time by TOE, and together with monitoring of LA pressure and trans-mitral gradient, will influence the decision to move or deploy the implant. Latest iterations of the currently available devices allow optimisation of individual leaflet insertion to maximise MR reduction and minimise the risk of leaflet detachment after deployment. After the clip is deployed, the reduction in regurgitation, together with the MV gradient, is assessed to determine the need for further implants. At the end of the procedure the guiding catheter is retracted into the right atrium. In general, iatrogenic atrial septal defects are not closed percutaneously at the time of the procedure. This can be considered, however, where there is evidence of right-to-left shunting or of more extensive disruption of the septum.
Currently available TEER devices
There are currently two CE-marked TEER devices available for use in the UK. The MitraClip system (Abbott Vascular) is a two-armed cobalt chromium device with a polyester covering. The fourth-generation MitraClip (Gen 4) is available in four different sizes, enabling the procedure to be tailored to the pathology being treated. Gen 4 also enables independent leaflet grasping, allowing the operator to capture the leaflets sequentially and to optimise leaflets after initial grasping.
The PASCAL system (Edwards Lifesciences) boasts broader paddles to facilitate leaflet capture, and a central spacer that functions both to fill the regurgitant orifice and reduce the risk of iatrogenic mitral stenosis. The PASCAL introduced the concept of independent grasping, whereby leaflets can be captured separately. The unique ability of the device to elongate facilitates atraumatic removal of the implant and guiding catheter from the left ventricle if required.
TEER for degenerative MR
Primary or degenerative mitral regurgitation (DMR) results from an intrinsic abnormality of the valve, including flail and prolapsing segments or myxomatous degeneration, in contrast to secondary or functional MR, which results from changes in left ventricular or left atrial volume, resulting in annular dilatation, leaflet tethering and restriction.
Evidence-base
The EVEREST (Endovascular Valve Edge-to-Edge REpair STudy) trial was the first study to evaluate the effectiveness of TEER compared with surgery.4 The study recruited 279 patients with predominantly DMR (70%), who were randomised 2:1 to TEER with the MitraClip system or conventional surgery. The primary end point of freedom from death, re-intervention and recurrent MR was higher in the MitraClip arm (73% vs. 55%), driven by the need for MV surgery in a fifth of TEER patients, compared with 2% in the surgical arm. MitraClip was safer than surgery, with a major adverse event rate of 15% at 30 days compared with 48% in the surgical arm, driven largely by a reduced need for blood transfusion. Symptoms were improved in both groups. The durability of TEER was confirmed in the five-year follow-up, with no difference in re-intervention rates between surgery and TEER beyond the first six months.5
Insight into more contemporary outcomes following TEER comes from the US Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy (STS/ACC TVT) registry. Almost 34,000 procedures were undertaken over a six-year period (2014 to 2020) to treat predominantly DMR (71%). There was a very high rate of procedural success (98%), and a substantial reduction in MR to moderate or less in 91%. In-hospital mortality was 2.2% and conversion to open surgery occurred in <0.5%.3 More recently, the CLASP IID (Edwards PASCAL Transcatheter Valve Repair System Pivotal Clinical Trial) study evaluated the effectiveness of the PASCAL system in a randomised comparison with MitraClip in 180 patients with DMR. No major differences were seen between cohorts. MR was reduced to mild or trace in almost 90% of patients treated with either technology, a reflection of improved operator experience and device design.6
Who should be referred?
Current guidelines recommend TEER for those patients with a contraindication to surgery or who are at high operative risk, and have suitable anatomy.7 Degenerative pathology involving the central aspect of the valve (P2 or A2 flail or prolapse) with good leaflet quality is considered ideal, along with a relatively short flail width (<10 mm) and flail gap (<15 mm). In reality, there are a broad range of degenerative pathologies that can be treated successfully with TEER, including large flail segments, non-central/commissural prolapse, multi-segment prolapse, and Barlow’s disease. A small number of contraindications to TEER do exist, particularly extensive leaflet calcification in the grasping zone, a small valve area (<3.5 cm), and rheumatic pathology. Anatomical selection criteria are summarised in table 2.
Table 2. Anatomical selection criteria for mitral TEER in degenerative mitral regurgitation (MR)
Favourable anatomy
Less favourable
Contraindicated
A2/P2 pathology
Flail width <15 mm
Flail gap <10 mm
Non-calcified leaflets
Posterior leaflet length >7 mm
MVA >4 mm2
Non-central/commissural pathology
Large flail segment
Posterior leaflet length <7 mm
Presence of a cleft
Multi-segment prolapse/Barlow’s disease
Calcified leaflets (outside the grasping zone)
Extensive mitral annular calcification
Rheumatic mitral stenosis
MVA <3.5 mm2
Leaflet calcification in the grasping zone
Extensive calcification of the subvalvular apparatus
Key: MVA = mitral valve area
TEER can also be used successfully in patients with acute ischaemic mitral regurgitation post-myocardial infarction, and is often the only therapeutic treatment option for this cohort.8
Future studies
Two pivotal randomised-controlled trials are currently in recruitment. The REPAIR MR (Percutaneous MitraClip Device or Surgical Mitral Valve Repair in Patients With Primary Mitral Regurgitation Who Are Candidates for Surgery) trial will randomise patients at moderate surgical risk to TEER or conventional surgery, while the PRIMARY (Percutaneous or Surgical Repair In Mitral Prolapse And Regurgitation for ≥65 Year-olds) study will include all patients over the age of 65, regardless of risk. The results will further define the role of TEER in the treatment of patients with DMR.
TEER for functional MR
Until recently, therapeutic options for patients with secondary or functional mitral regurgitation (FMR) have largely focused on pharmacological and cardiac resynchronisation therapy, with surgical intervention reserved for patients with concomitant coronary artery disease. Isolated MV surgery for this population of patients is rarely recommended in current guidelines due to high procedural risk and no evidence of a mortality benefit.7 TEER offers a new therapeutic option, aiming to reduce heart failure hospitalisation and improve clinical and quality-of-life outcomes.
Evidence-base
There are two randomised trials of TEER for patients with FMR. The COAPT (Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation) study enrolled 614 subjects randomised 1:1 to TEER with MitraClip, or to guideline-directed medical therapy (GDMT).9 After 24 months there was a significant mortality reduction in the TEER group (29.1% vs. 46.1%, number needed to treat [NNT] to prevent one death 5.9). There was a similarly striking effect on heart failure rehospitalisation, with NNT to prevent one rehospitalisation 3.1.10 In contrast, the MITRA-FR (Multicentre Study of Percutaneous Mitral Valve Repair MitraClip Device in Patients With Severe Secondary Mitral Regurgitation) study showed no significant difference between TEER and control for both all-cause mortality and heart failure rehospitalisation.11
Important differences in the two trials are likely to explain such contrasting results, and help guide patient selection for TEER in FMR. Patients enrolled to COAPT had more severe MR (effective regurgitant orifice area [EROA] 41 ± 15 vs. 31 ± 10 mm) and less left ventricular (LV) dilatation (LV end diastolic volume 101 ± 34 vs. 135 ± 35 ml/m2) than those in MITRA-FR. MR reduction was greater in COAPT, with more patients with ≤2+ MR after TEER (95% vs. 83%). The approach to management of GDMT was also different. MITRA-FR followed a more ‘real-world’ approach, with patients on their own heart failure medications at baseline, whereas COAPT mandated that patients in both groups were confirmed to be on maximally tolerated GDMT before randomisation.
A key concept that helps to explain the differing response of patients in the two trials is that of proportionality of MR, where the role of ventricular dilatation is considered in relation to severity of MR.12 For a given LV volume and regurgitation fraction, the expected EROA can be predicted. Where MR is proportionate to the degree of LV dilatation, it may be more likely to respond to device and pharmacological therapy. Where MR is disproportionately severe (EROA greater than predicted), patients are more likely to benefit from TEER.
Who should be referred?
In keeping with the evidence-base and international guidelines, patients who fit the COAPT inclusion criteria should be considered for TEER. Referral should be made for patients with severe MR due to LV dysfunction in whom intrusive symptoms persist despite appropriately up-titrated GDMT. Patients with FMR due solely to atrial dilatation, usually in the context of longstanding atrial fibrillation, may also be successfully treated with TEER, although evidence in this group is lacking.
Imaging the MV for TEER
Table 3. Key information required from the pre-procedural echocardiogram
Valve morphology
DMR vs. FMR
MR jet – one significant jet? More significant jets?
Echocardiography is the key imaging modality for the pre-procedural, procedural, and post-procedural assessment of patients undergoing TEER. Both transthoracic echocardiography (TTE) and TOE should be performed, including bi-plane and 3D imaging.
The main purpose of pre-procedural imaging is to determine if patients have suitable MV anatomy for TEER, and should include assessment of MV morphology, MR severity, and anatomical information required for the TEER procedure (table 3).
MV morphology
The key views to assess structural suitability for TEER are the bi-commissural, which depicts the medial-lateral aspect of the MV, and the long axis, which shows the anterior-posterior aspect.
A 3D matrix transducer should be used to perform simultaneous multi-plane imaging. An optimised bi-commissural view should first be obtained as the primary image, following which, use of the multi-plane mode will allow an orthogonal long-axis view to be visualised simultaneously as a secondary image. This allows a step-by-step assessment of MV morphology using MV segmental analysis, making it easier to assess the specific location of the regurgitation jet and mechanism of valve pathology (figure 2). By sweeping the cursor along the whole line of coaptation, with and without colour doppler, a detailed structural assessment of all MV scallops can be obtained. In addition to MV segmental analysis, a 3D ‘en-face’ view should be obtained to define leaflet morphology (figure 2A). This is also a key view used to guide clip positioning during the TEER procedure. Morphological assessment should also include measurement of the coaptation depth and length in cases of FMR, and in DMR cases the flail gap and width (figure 3).
Figure 2. Mitral valve segmental analysis. A ‘surgical 3D view’ of the mitral valve is shown and illustrates where the cursor (dashed line) of the simultaneous multi-plane image is traversing the aspect of the commissural line of the mitral valve (images A, D and G). Directing the cursor of the simultaneous multi-plane through the relevant scallop on the optimised bi-commissural view in the primary image depicts the corresponding orthogonal long-axis view of the scallops in the secondary image (images B, E and H). The same image with colour Doppler is shown (images C, F and I) to illustrate the jet characteristics. In this case a flail P2 scallop with a large conversion zone is seen due to the regurgitation through the flail P2 scallopFigure 3. In degenerative mitral regurgitation (DMR) the flail gap is best measured in the long-axis view (or where the flail gap is greatest) in systole. The mobile leaflet length is measured usually in long-axis either in systole or in mid-diastole (A). The flail width is usually either measured in mitral valve short-axis view in systole or on the 3D en-face view as depicted in image B. In functional mitral regurgitation (FMR) the coaptation depth and coaptation length are best measured in the four-chamber or long-axis view in systole (C and D)
MR severity
A comprehensive integrated assessment of MR severity using qualitative, semi-quantitative and quantitative parameters is recommended. In patients with FMR, assessment of severity is more challenging due to the non-circular regurgitant orifice area, as well as the dynamic nature of MR, which will vary with haemodynamic status; regurgitation fraction is the most physiological and reliable parameter in these patients.
Assessment of anatomy specific to the TEER procedure
Mitral valve area (MVA) should be measured to determine the risk of mitral stenosis after TEER, either by planimetry at the tips of the MV leaflets in the TTE short-axis view, or more accurately by 3D planimetry on TOE. Assessment of the inter-atrial septum and left atrial size should be performed to determine the feasibility of trans-septal puncture, including available height above the MV for the TEER procedure.
Finally, calcification of the leaflets and subvalvular apparatus should be identified, since excessive calcification, particularly in the grasping zone, may preclude TEER.
Tricuspid edge-to-edge repair
Tricuspid regurgitation (TR) is common, and associated with significant morbidity and mortality, but is generally poorly investigated and treated.13 Moreover, open heart surgery for TR is rarely performed in isolation and has been associated with poor results.14
The increasing awareness of effective TEER techniques for the MV generated the realisation that a similar therapy may have a use with the tricuspid valve, even with this valve’s more complex anatomy.15
Evidence-base
Registry data, initially with the MitraClip device, and subsequently with the more tailored PASCAL and TriClip (Abbott Vascular) systems, have consistently shown tricuspid TEER (tTEER) to be very safe, with low mortality and morbidity, and effective, with sustained clinical benefit at one year.15–19 The first randomised trial of tTEER, the TRILUMINATE (Trial to Evaluate Cardiovascular Outcomes in Patients Treated With the Tricuspid Valve Repair System) study, was published in March 2023.20 In 350 patients randomised 1:1 to tTEER versus medical therapy, tTEER was safe (98.3% freedom from major adverse events at 30 days), effective in reducing TR (87.0% ≤moderate TR at 30 days vs. 4.0% control), and significantly improved quality of life at 12 months compared with medical therapy (Kansas City Cardiomyopathy Questionnaire [KCCQ] quality-of-life score increase 12.3 ± 1.8 vs. 0.6 ± 1.8, p<0.0001). However, there was no impact on death, tricuspid valve surgery, or hospitalisation for heart failure.
Case selection
Selection of patients for possible tTEER should include detailed imaging, including TOE, to establish the aetiology of TR, the precise location of the regurgitant jet, the morphology of the valve leaflets, and the coaptation gap. Atrial dilatation due to permanent atrial fibrillation, and pacing-lead induced TR, are two of the more common TR aetiologies – both are amenable to tTEER.
Patients with severe TR often have multiple comorbidities, and establishing the extent to which the TR is responsible for the overall symptom burden can be challenging. However, patients with refractory symptoms of breathlessness or right heart failure with severe TR should be referred to a specialised valve multi-disciplinary team (MDT). Although tTEER is currently not commissioned in the UK, an increasing number of centres are already performing the procedure with promising early results.
Conclusion
Mitral TEER is a safe, low-risk, and effective therapeutic option for patients with DMR who are at prohibitive or high-risk for MV surgery due to age and/or comorbidities, and for those with disproportionate FMR with symptoms refractory to medical therapy. Mitral TEER is now, finally, widely available across the NHS for the significant cohort of patients who meet these criteria, while the use of TEER for the under-recognised but common problem of severe symptomatic tricuspid regurgitation is developing. Potentially suitable patients should be referred to the specialist valve MDTs in place at all UK TEER centres.
Key messages
Mitral valve transcatheter edge-to-edge repair (TEER), formerly known as percutaneous mitral valve leaflet repair or mitral clip, is now commissioned by NHS England and the devolved authorities, and is routinely available in 24 cardiac surgical centres across the UK
Referral for mitral TEER should be considered in patients with primary or degenerative mitral regurgitation who are at high or prohibitive risk for mitral valve surgery, and in patients with secondary or functional mitral regurgitation who remain symptomatic despite optimal medical therapy
Tricuspid valve TEER is emerging as a safe and effective treatment option for the large and often unrecognised cohort of patients with severe tricuspid regurgitation, for whom no good surgical option exists
This review describes the current status of the TEER procedure, considers which patients should be referred for intervention, reviews the pre-procedural imaging required when considering mitral TEER, and outlines the evidence for the application of TEER to the tricuspid valve
Conflicts of interest
DJB is a Consultant and Proctor for Abbott Vascular, Edwards Lifesciences, and Medtronic. SD is a Consultant and Proctor for Abbott Vascular and Edwards Lifesciences. RS is a Consultant and Proctor for Abbott Vascular. JB is a Consultant and Proctor for Abbott Vascular and Edwards Lifesciences. PAM is a Consultant and Proctor for Abbott Vascular and Edwards Lifesciences. DS none declared.
Funding
Funding for this article was provided by the Valve for Life programme, with a grant obtained from the European Association of Percutaneous Cardiovascular Interventions.
2. National Institute for Health and Care Excellence. Percutaneous mitral valve leaflet repair for mitral regurgitation. IPG649. London: NICE, 2019. Available from: https://www.nice.org.uk/guidance/ipg649
3. Mack M, Carroll JD, Thourani V et al. Transcatheter mitral valve therapy in the United States: a report from the STS-ACC TVT registry. J Am Coll Cardiol 2021;78:2326–53. https://doi.org/10.1016/j.jacc.2021.07.058
4. Feldman T, Foster E, Glower DD et al.; EVEREST II Investigators. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med 2011;364:1395–406. https://doi.org/10.1056/NEJMoa1009355
5. Feldman T, Kar S, Elmariah S et al.; EVEREST II Investigators. Randomized comparison of percutaneous repair and surgery for mitral regurgitation: 5-year results of EVEREST II. J Am Coll Cardiol 2015;66:2844–54. https://doi.org/10.1016/j.jacc.2015.10.018
6. Lim DS, Smith RL, Gillam LD et al. Randomized comparison of transcatheter edge-to-edge repair for degenerative mitral regurgitation in prohibitive surgical risk patients. JACC Cardiovasc Interv 2022;15:2523–36. https://doi.org/10.1016/j.jcin.2022.09.005
7. Vahanian A, Beyersdorf F, Praz F et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632. https://doi.org/10.1093/eurheartj/ehab395
8. Farwati M, Saad AM, Abushouk AI et al. Short-term outcomes following urgent transcatheter edge-to-edge repair with MitraClip in cardiogenic shock: a population-based analysis. JACC Cardiovasc Interv 2021;14:2077–8. https://doi.org/10.1016/j.jcin.2021.04.052
9. Stone GW, Lindenfeld J, Abraham WT et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med 2018;379:2307–18. https://doi.org/10.1056/NEJMoa1806640
10. Giustino G, Camaj A, Kapadia SR et al. Hospitalizations and mortality in patients with secondary mitral regurgitation and heart failure. J Am Coll Cardiol 2022;80:1857–68. https://doi.org/10.1016/j.jacc.2022.08.803
11. Obadia JF, Messika-Zeitoun D, Leurent G et al. Percutaneous repair or medical treatment for secondary mitral regurgitation. N Engl J Med 2018;379:2297–306. https://doi.org/10.1056/NEJMoa1805374
12. Grayburn PA, Sannino A, Packer M. Proportionate and disproportionate functional mitral regurgitation: a new conceptual framework that reconciles the results of the MITRA-FR and COAPT trials. JACC Cardiovasc Imaging 2019;12:353–62. https://doi.org/10.1016/j.jcmg.2018.11.006
13. Wang N, Fulcher J, Abeysuriya N et al. Tricuspid regurgitation is associated with increased mortality independent of pulmonary pressures and right heart failure: a systematic review and meta-analysis. Eur Heart J 2019;40:476–84. https://doi.org/10.1093/eurheartj/ehy641
14. Kawsara A, Alqahtani F, Nkomo VT et al. Determinants of morbidity and mortality associated with isolated tricuspid valve surgery. J Am Heart Assoc 2021;10:e018417. https://doi.org/10.1161/JAHA.120.018417
15. Nickenig G, Kowalski M, Hausleiter J et al. Transcatheter treatment of severe tricuspid regurgitation with the edge-to-edge MitraClip technique. Circulation 2017;135:1802–14. https://doi.org/10.1161/CIRCULATIONAHA.116.024848
16. Mehr M, Taramasso M, Besler C et al. 1-year outcomes after edge-to-edge valve repair for symptomatic tricuspid regurgitation. J Am Coll Cardiol Interv 2019;12:1451–61. https://doi.org/10.1016/j.jacc.2019.09.028
17. Aurich M, Volz MJ, Mereles D et al. Initial experience with the PASCAL ace implant system for treatment of severe tricuspid regurgitation. Circ Cardiovasc Interv 2021;14:e010770. https://doi.org/10.1161/CIRCINTERVENTIONS.121.010770
18. Lurz P, von Bardeleben RS, Weber M et al. Transcatheter edge-to-edge repair for treatment of tricuspid regurgitation. J Am Coll Cardiol 2021;77:229–39. https://doi.org/10.1016/j.jacc.2020.11.038
19. Taramasso M, Benfari G, van der Bijl P et al. Transcatheter versus medical treatment of patients with symptomatic severe tricuspid regurgitation. J Am Coll Cardiol 2019;74:2998–3008. https://doi.org/10.1016/j.jacc.2019.09.028
20. Sorajja P, Whisenant B, Hamid N et al. Transcatheter repair for patients with tricuspid regurgitation. N Engl J Med 2023;388:1833–42. https://doi.org/10.1056/NEJMoa2300525
Dr Andreas Tridimas
Consultant in Chemical Pathology & Metabolic Medicine Countess of Chester Hospital and Wirral University Teaching Hospital
(a.tridimas@nhs.net)
HEART UK held its 36th Annual Medical and Scientific Conference over several days in July 2023 when the cholesterol charity reflected on the current progress across a range of key areas within lipidology. This included an update on the progress in cardiovascular disease (CVD) prevention nationally, paediatric familial hypercholesterolaemia (FH) and a look back on the dramatic progress since the identification of PCSK9 as a lipid treatment target. Dr Andreas Tridimas reports its highlights.
CVD prevention past and present
Dr Shahed Ahmad from NHS England addresses the conference
The scale of CVD deaths, currently 136,000 per year in the UK1 and similar in number to the first year of the COVID-19 pandemic, was highlighted by Dr Shahed Ahmad (NHS England) in his role as National Clinical Director for CVD. He emphasised the importance of tackling CVD as if it were a pandemic. Rather than needing to create vaccines, he said we already have the necessary therapeutics to reduce CVD but these need robust application to our populations. He signposted the CVDPREVENT website2 with its wealth of open access primary care data on metrics, such as the percentage of adult patients with CVD on lipid-lowering therapy, which currently stands at 81%. He used examples to highlight the significant unwarranted clinical variation across geographical areas, emphasising the need to tackle regional variation.
Professor Azfar Zaman (Newcastle Hospitals NHS Foundation Trust) outlined the impressive reductions in ischaemic heart disease deaths over the last two decades when compared with other causes, such as malignancy and influenza. Importantly, he stressed the need to consider the impact of morbidity from CVD events and not simply focus on mortality data.3 Regarding CVD pathophysiology, he reiterated the well-established factors driving its development such as diabetes, inflammation, and dyslipidaemia. He then stressed the point that amplified benefits are seen when we intervene to address the multiple causal pathologies for CVD development, as opposed to focusing on risk factors in isolation.
Rheumatoid arthritis and CVD risk
In rheumatoid arthritis the principal driver of the increased mortality seen is CVD.4 This important point was made rheumatologist Professor Ernest Choy (Cardiff University). Lipid levels are only part of the picture, he said, and inflammation appears to drive the process of CVD development.5 Furthermore, during relapses, lipid levels in rheumatoid arthritis may actually appear lower, with a rise seen after successful treatment. This is thought to reflect lipids behaving as negative acute phase reactants,6 which he compared to the lower cholesterol levels that have long since been recognised following acute myocardial infarction.7
Paediatric familial hypercholesterolaemia
Mrs Lorraine Priestley-Barnham (Harefield Hospital), a Paediatric FH Clinical Nurse Specialist, made the key point that children can have high cholesterol too. It is estimated that there are approximately 50,000 children with FH under 18 years in the UK, based on the population prevalence of one in 250.8 Much of our focus to date, she said, has been on adults with FH. She stressed the importance of starting treatment early in life, supported by multiple long-term studies that show statin safety in children.8 She directed the audience to the HEART UK statement of care for paediatric FH as a resource to guide clinical teams.8
Diet in CVD prevention – a tool to help assess diet
Less than 0.1% of people adhere to the Public Health England Eatwell guide,9 Consultant Nutritionist Ms Elphee Medici (London) told the meeting, showing the extent of poor diet in the UK. She showcased the ‘HEART UK Cardiovascular Diet Checklist’10 as a tool to help clinicians and patients to assess diet. This uses 16 yes/no questions to provide an indication of whether a diet is ‘heart healthy.’ Top-line practical feedback is provided on completion to help navigate towards dietary improvement. The HEART UK team is currently updating the online checklist to provide more tailored advice and help motivate individuals to make dietary improvements.
Coping with referral volume was addressed by Dr Tina Khan
CVD prevention services and managing workload
Professor Gordon Ferns (Brighton and Sussex Medical School) and Dr Tina Khan (Harefield Hospital) looked at how to manage workload for CVD prevention services. Professor Ferns used his local experience to draw attention to the rising tide of lipid clinic referrals resulting from factors such as new lipid-lowering therapies and treatment guidelines. He outlined how this has led to his service having to implement strategies to ensure the service remains sustainable. Dr Kahn outlined her team’s adaptive approach to dealing with referral volume, which has included upskilling specialist nurses to oversee referral triage, as well as lipid education sessions, webinars and MDT collaborations.
PCSK9: from genetics to clinical trials
This year’s Myant Lecture was given by Professor Catherine Boileau
The prestigious Myant lecture this year was given by Professor Catherine Boileau (Hôpital Bichat-Claude Bernard, Paris, France), who was a key figure in the identification of PCSK9 as a treatment target. Professor Boileau started her talk by illustrating some of the earliest historic evidence of lipid disorders with xanthelasma seen on Da Vinci’s Mona Lisa and tendon xanthoma on the Charioteer of Delphi.11
From ancient Greece to modern day, Professor Boileau and her team first showed in 2003 how mutations in PCSK9 cause autosomal dominant hypercholesterolaemia.12 In 2006 came evidence that sequence variations in PCSK9 led to lower low-density lipoprotein and protection against coronary heart disease.13 What followed was a flurry of scientific development and, within 12 years of Professor Boileau’s study, the first PCSK9 inhibitor, alirocumab, was approved for clinical use in what many regard as the pharmacotherapeutic innovation of the decade for CVD prevention.
Dr Andreas Tridimas
Consultant in Chemical Pathology & Metabolic Medicine
Countess of Chester Hospital and Wirral University Teaching Hospital a.tridimas@nhs.net
2. Office for Health Improvement and Disparities and the NHS Benchmarking Network. Cardiovascular Disease Prevention Audit (CVDPREVENT). NHS Digital 2021. https://www.cvdprevent.nhs.uk/home (Last accessed 4/08/2023)
3. Cheema KM, Dicks E, Pearson J et al. Long-term trends in the epidemiology of cardiovascular diseases in the UK: insights from the British Heart Foundation statistical compendium. Cardiovasc Res 2022;118:2267–80. https://doi.org/10.1093/cvr/cvac053
4. Gabriel SE. Why do people with rheumatoid arthritis still die prematurely? Ann Rheum Dis 2008;67(Suppl 3):iii30–4. https://doi.org/10.1136/ard.2008.098038
6. Choy E, Sattar N. Interpreting lipid levels in the context of high-grade inflammatory states with a focus on rheumatoid arthritis: a challenge to conventional cardiovascular risk actions. Ann Rheum Dis 2009;68:460–9. https://doi.org/10.1136/ard.2008.101964
8. Ramaswami U, Humphries SE, Priestley-Barnham L et al. Current management of children and young people with heterozygous familial hypercholesterolaemia – HEART UK statement of care. Atherosclerosis 2019;290:1–8. https://doi.org/10.1016/j.atherosclerosis.2019.09.005
9. Scheelbeek P, Green R, Papier Keren A et al. Health impacts and environmental footprints of diets that meet the Eatwell Guide recommendations: analyses of multiple UK studies BMJ Open 2020;10:e037554. https://doi.org/10.1136/bmjopen-2020-037554
12. Boileau C, Abifadel M, Varret M et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet 2003;34:154–6. https://doi.org/10.1038/ng1161
13. Cohen JC, Boerwinkle E, Mosley TH Jr et al. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med 2006;354:1264–72. https://doi.org/10.1056/NEJMoa054013
Authors: Riccardo Proietti, Mark Field, Victoria McKay, Gregory Y H Lip, Manoj Kuduvalli, on behalf of UK Aortic Society
Riccardo Proietti
Senior Clinical Lecturer
Mark Field
Professor and Cardiac Surgeon
Victoria McKay
Consultant in Cardiovascular Clinical Genetics
Gregory Y H Lip
Professor at Liverpool Centre for Cardiovascular Science at University of Liverpool, Liverpool John Moores University and Liverpool Heart & Chest Hospital; and Danish Center for Health Services Research, Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
Manoj Kuduvalli
Cardiac Surgeon
Liverpool Heart & Chest Hospital NHS Foundation Trust, Thomas Drive, Liverpool, L14 3PE
Thoracic aortic aneurysms are often asymptomatic until patients present with a life-threatening acute aortic syndrome. The vulnerability of an aorta to an acute aortic syndrome is determined by cross-sectional diameter and underlying aetiological factors, such as genotype or acquired disease. Screening the general population for thoracic aneurysms presents multiple resource issues including the availability of imaging modalities. Targeted screening of high-risk groups provides the only currently pragmatic solution. Opportunistic imaging through lung cancer screening programmes could pick up a proportion. Until we have a comprehensive screening programme it is incumbent on all healthcare professionals to have a low threshold for considering acute aortic pathologies when reviewing patients presenting with chest pain.
Introduction
The diseases of the aorta are an important cause of worldwide cardiovascular mortality and morbidity.1 Hospital admissions within the UK at the end of 2010 were identified as 8.8 for thoracic aortic dissections and 9.0 for thoracic aortic aneurysms, per 100,000 inhabitants.2 More recently, significant regional variation has been documented in access to treatment and mortality outcomes in the UK.3 These authors speculated that one of the barriers to treatment underlying this unwarranted variation was a lack of clear guidelines on population screening for this disease. Aneurysms of the thoracic aorta commonly have a genetic basis or are acquired as a chronic degenerative process (sporadic). A smaller group of patients have aortic aneurysms, the long-term sequelae of an acute aortic syndrome. Less frequently, aneurysms are the result of processes, such as post-traumatic disruption, infection, inflammation or developmental anomalies. The clinical challenge remains identification, as thoracic aortic aneurysms are most frequently asymptomatic, sitting within the cavernous chest, only revealing themselves when associated with concurrent disease, an incidental clinical finding or an acute aortic syndrome. It is largely the size of the aneurysm, as well as the aetiology, that determines a patient’s vulnerability to a life-threatening acute aortic syndrome, such as aortic dissection. Screening for the ‘vulnerable aorta’ in the population is key to surveillance and timely intervention to avoid an aortic catastrophe. Given computed tomography (CT) or magnetic resonance imaging (MRI) are the only current modalities to detect thoracic aortic aneurysms, screening the entire population is precluded by challenges in capacity, cost and patient safety. Targeting screening to high-risk groups is the only pragmatic way to identify patients with a vulnerable aorta.
Defining the vulnerable aorta
The single most important feature that defines the vulnerability of an aorta to an acute aortic syndrome is cross-sectional diameter.4 Size forms the basis of international guidelines as the indication for prophylactic intervention.5 However, increasingly, non-size dependent factors are used to define the vulnerable aorta, with disease aetiology influencing cross-dimensional indications for surgery (table 1).
Table 1. Defining the vulnerable aorta
Aetiology
Examples
Genotype and phenotype
Inherited thoracic aortopathy (syndromic and non-syndromic)
There is increasing recognition that many thoracic aortic aneurysms have a genetic basis (~30%), both syndromic and non-syndromic. The pathogenicity and penetrance of variants are important factors determining vulnerability. Syndromic disease is relatively well-defined with clear indications of when to intervene surgically, but with some variation in expression. Non-syndromic, familial and non-familial disease are less well-defined, but the high penetrance of many variants seen in specific genes (ACTA2, MYH11, MYLK, SMAD3, COL3A1) is increasingly well understood. Variants of unknown significance (VUS) represent an ongoing challenge to interpret and apply to clinical management. A large proportion of aneurysms are acquired, so-called sporadic (~70%), through multi-morbidity (e.g. hypertension), socio-behavioural factors (e.g. smoking and diet) and senescence, as well as long-term sequelae to acute aortic syndromes. Sporadic aneurysms have relatively predictable risk profiles, largely dependent on size. An even smaller group of patients at risk are those that have congenital variants in anatomy that predispose them to acute aortic syndromes. The hierarchy of importance of each of these processes to determining the vulnerability of the aorta, is yet to be understood. The summative effects of multiple univariate risk factors are, additionally, poorly understood. They do, however, point us towards choosing which high-risk groups to target for screening, and additionally, screening methodologies.
What do the guidelines suggest?
There are no recommendations for population-level screening, however, guidelines do exist for aortic imaging and genetic testing of certain individuals, families and high-risk groups. The American Heart Association (AHA) guidelines,5 under ‘recommendations for familial thoracic aortic aneurysms and dissections’, recommend image screening for all first-degree relatives of patients with thoracic aneurysm and/or dissection (Class I recommendation, level of evidence B) (table 2). There are then additional weaker recommendations for imaging and genetic analysis for particular groups, but with less evidence base. The AHA guidelines have, however, been superseded by new technologies, and even national health service guidelines. Several groups have published their own preferences for screening of a given proband and relatives based around genetic testing and imaging.6 These recommendations pose significant challenges for healthcare systems and resources as thoracic imaging becomes more prevalent and incidental aortic aneurysms are identified. The imaging follow-up burden of this cohort in surveillance programmes, is, and will be, immense. Within the UK, current NHS guidelines recommend proband diagnostic genetic testing at the relatively low threshold of 3.8 cm, further increasing the number of patients requiring imaging and investigations. The NHS National Genomic Test Directory7 for diagnostic genetic testing of a proband includes:
Thoracic aortic aneurysm (3.8 cm) or dissection with onset before age 50 years.
Thoracic aortic aneurysm or dissection with onset before age 60 years with a first-degree relative with thoracic aortic aneurysm or dissection.
Thoracic aortic aneurysm or dissection before age 60 years with no classical cardiovascular risk factors.
Thoracic aortic aneurysm or dissection before age 60 years with features suggestive of aortopathy, e.g. arterial tortuosity.
Clinical features suggestive of Loeys-Dietz syndrome.
Features of Marfan syndrome giving a systemic Ghent score of ≥7, following assessment by a clinical geneticist or specialist with expertise in aortopathy.
High clinical suspicion of a condition predisposing to aortic/arterial disease and diagnostic testing for other conditions such as Ehlers-Danlos syndrome (where indicated) has not identified a causative mutation.
Any deceased individual with a thoracic aortic aneurysm (3.8 cm) or dissection detected at autopsy meeting one of the above criteria and who have relatives who will benefit from cascade testing using a genetic diagnosis will be suitable for post-mortem genetic testing.
Table 2. American Heart Association (AHA) guidelines: recommendations for familial thoracic aortic aneurysms and dissections
Class I
Aortic imaging is recommended for first-degree relatives of patients with thoracic aortic aneurysm and/or dissection to identify those with asymptomatic disease. (Level of evidence: B)
If the mutant gene (FBN1, TGFBR1, TGFBR2, COL3A1, ACTA2, MYH11) associated with aortic aneurysm and/or dissection is identified in a patient, first-degree relatives should undergo counselling and testing. Then, only the relatives with the genetic mutation should undergo aortic imaging. (Level of evidence: C)
Class IIa
If one or more first-degree relatives of a patient with known thoracic aortic aneurysm and/or dissection are found to have thoracic aortic dilatation, aneurysm, or dissection, then imaging of second-degree relatives is reasonable. (Level of evidence: B)
Sequencing of the ACTA2 gene is reasonable in patients with a family history of thoracic aortic aneurysms and/or dissections to determine if ACTA2 mutations are responsible for the inherited predisposition. (Level of evidence: B)
Class IIb
Sequencing of other genes known to cause familial thoracic aortic aneurysms and/or dissection (TGFBR1, TGFBR2, MYH11) may be considered in patients with a family history and clinical features associated with mutations in these genes. (Level of evidence: B)
If one or more first-degree relatives of a patient with known thoracic aortic aneurysm and/or dissection are found to have thoracic aortic dilatation, aneurysm, or dissection, then referral to a geneticist may be considered. (Level of evidence: C)
In Liverpool there is a specialist aortic nurse-led clinic for review of isolated proximal small aneurysms (<5.0 cm) in which patients are entered into a surveillance programme after a consultation and, additionally, undergo diagnostic genetic testing as indicated (above 3.8 cm). All patients with a clear pathogenic variant are referred on to genetics counsellors to initiate familial predictive genetic testing, while those with VUS are discussed with, or clinically assessed by, a clinical geneticist.
What additional features identify the vulnerable aorta?
Elefteriades et al.8 in 2015 published a novel paradigm for detection of silent aortic disease with a ‘guilt by association’ approach. These features include:
Intracranial aneurysm
Aortic arch anomalies
Abdominal aortic aneurysms
Simple renal cysts
Bicuspid aortic valves
Temporal arteritis (and other autoimmune conditions)
Positive family history of aneurysm disease
Positive thumb-palm sign.
We believe composite risk associated with age, hypertension and socio-behavioral factors, such as smoking, diet and exercise, will prove important groups. Currently, there is a lack of data around the efficacy of such approaches to population screening.
Piggy backing on lung cancer screening programmes
Internationally, there are many lung cancer screening trials, which are based on a low-dose, non-contrast CT scan in certain high-risk groups. For the Liverpool Lung Health Check Programme, the criteria are any smoker between the ages of 55 and 74 years. The degree of co-prevalence of lung cancer and abdominal aortic aneurysms has been explored, but the relationship between individuals undergoing lung cancer screening by CT and incidental findings of thoracic aortic aneurysms remains largely undefined, but potentially important and an opportunity.
Other modalities for screening the population
A promising opportunity in genetics is offered by mRNA signatures in blood, which may be used as biomarkers and screening tools. Recently, a preliminary study from the Yale group showed that mRNA has a sensitivity (72%) and specificity (90%) with a thoracic aortic aneurysm compared with control.9 This approach awaits validation. In addition, there is the potential for whole genome sequencing for aneurysms in the future.
Future perspective on screening
The UK Abdominal Aortic Aneurysm (AAA) screening programme is well established and offered to men aged 65 years using targeted ultrasound. Any thoracic aortic aneurysm screening programme faces the challenge of requiring CT scans, being less prevalent, and a requirement for additional genetic testing (proband and relatives) given the incidence of a gene-based aetiology. While a number of groups have published their local policies and procedures for targeted imaging and genetic screening of individuals and families,6,10 national healthcare providers in the UK are yet to recommend comprehensive, funded pathways. Drafting behind a national lung cancer screening programme may well be an opportunity to pick up the majority of asymptomatic thoracic aortic aneurysms, although this has yet to be understood as limited to smokers. In addition, this approach will miss many younger syndromic patients.
Equity in access
Differences in the prevalence of thoracic aortic aneurysm in different population groups (age, gender, ethnicity, socioeconomics and other demographics) suggest it is important to be mindful in ensuring inclusivity to diagnosis and treatment.
Conclusion
Thoracic aortic aneurysms are often asymptomatic until patients present with a life-threatening acute aortic syndrome. The vulnerability of an aorta to an acute aortic syndrome is determined by cross-section diameter and underlying aetiological factors, such as genotype acquired disease. Screening the population for thoracic aneurysms through imaging and genetics presents challenges in the requirement for CT scanning, and the pathogenic uncertainty of many genetic variants. Targeted screening of high-risk groups provides the only currently pragmatic solution. Opportunistic imaging through lung cancer screening programmes will pick up a proportion, however, at the present time international guidelines are restricted to investigating probands, no matter how they are incidentally picked up, and their relatives. Until we have a comprehensive screening programme it is incumbent on all healthcare professionals to have a low threshold for considering acute aortic pathologies when reviewing patients presenting with chest pain. Early diagnosis is key to a successful outcome.
Key messages
Thoracic aortic aneurysms are often asymptomatic until patients present with life-threatening acute aortic syndromes
Generalised screening of populations for thoracic aortic aneurysm is currently not feasible due to limitations on availability of imaging services
The only pragmatic solution to screening the population for this disease is a focus on high-risk groups
High-risk patients with a vulnerable aorta are identifiable based on genomics and risk factors for acquired disease
1. Sampson UK, Norman PE, Fowkes FG et al. Global and regional burden of aortic dissection and aneurysms: mortality trends in 21 world regions, 1990 to 2010. Global Heart 2014;9:171–80. https://doi.org/10.1016/j.gheart.2013.12.010
2. von Allmen RS, Anjum A, Powell JT. Incidence of descending aortic pathology and evaluation of the impact of thoracic endovascular aortic repair: a population-based study in England and Wales from 1999 to 2010. Eur J Vasc Endovasc Surg 2013;45:154–9. https://doi.org/10.1016/j.ejvs.2012.12.007
3. Bottle A, Mariscalco G, Shaw MA et al.; on behalf of the UK Aortic Forum. Unwarranted variation in the quality of care for patients with diseases of the thoracic aorta. J Am Heart Assoc 2017;6:e004913. https://doi.org/10.1161/JAHA.116.004913
4. Elefteriades JA. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. Ann Thorac Surg 2002;74:S1877–S1880. https://doi.org/10.1016/S0003-4975(02)04147-4
5. Hiratzka LF, Bakris GL, Beckman JA et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010;121:e266–e369. https://doi.org/10.1161/CIR.0b013e3181d4739e
6. Coutinho T, Richer J, Boodhwani M. Who to screen for thoracic aortic aneurysms, and when to refer for surgery. Can J Cardiol 2022;38:695–8. https://doi.org/10.1016/j.cjca.2022.01.010
8. Elefteriades JA, Sang A, Kuzmik G, Hornick M. Guilt by association: paradigm for detecting a silent killer (thoracic aortic aneurysm). Open Heart 2015;2:e000169. https://doi.org/10.1136/openhrt-2014-000169