
Definitions
Lead extraction is defined as a procedure in which a cardiovascular implantable electronic device (CIED) lead is removed with the assistance of equipment not routinely used during implantation, or after it has been in situ for more than one year. Lead explant is the removal of a lead that has been implanted for less than one year using only standard implantation stylets.
Indications
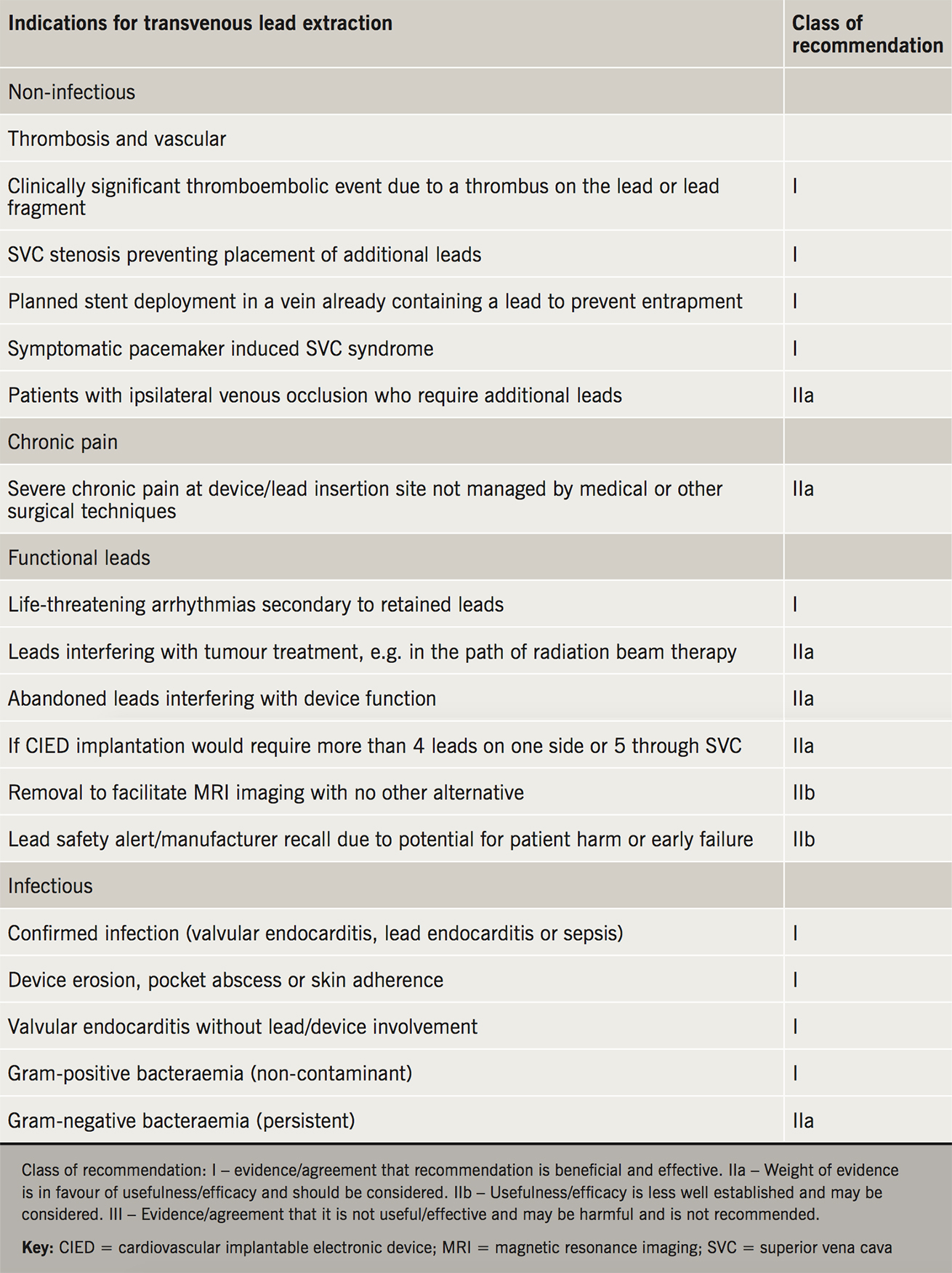
The indications for CIED lead extraction from contemporary international guidelines are summarised in table 1.
Epidemiology
The number of lead extraction procedures being performed is growing. The underlying reasons for this are an increasing rate of CIED implantation, patients with CIEDs living longer, increasing comorbidity of patients and higher than average failure rates of certain historically implanted leads due to design flaws. Data from Hospital Episodes Statistics (HES) recorded 1,215 CIED systems removal (extraction or explant) in England in 2016–17. The most common indication is CIED infection, with the remaining cases predominately being performed to remove functional leads to allow venous access during a system upgrade or to replace faulty leads.
Principles of extraction
Implantation of a CIED lead results in a host reaction that becomes more pronounced with longer dwell times. Over time, fibrosis develops leading to adherence of the lead at several points within the venous system. Common sites for adherence include the subclavian vein as it passes under the clavicle, the junction between the innominate vein and superior vena cava (SVC), and within the cardiac chambers (at the point right ventricular leads pass through the tricuspid valve and at the electrode tips). Defibrillator coils (particularly those positioned in the SVC) also act as foci for fibrosis. Many patients also develop calcification at these fibrotic points. Fibrosis and calcification result in tethering of CIED leads within the venous system and act as obstacles to their removal. Longer dwell times, the presence of multiple leads and the presence of defibrillator coils are all associated with more challenging extractions. The approach to lead extraction is hierarchical, requiring specific tools and techniques. Simple methods such as manual traction and use of a locking stylet are widely utilised, but there is heterogeneity in the methods and tools used thereafter. Much will depend on operator experience and the commonly used methods are described below.
Simple traction
The first attempt to extract a transvenous CIED lead involves simple traction with non-locking stylets. This can be successful in up to 85% of cases, if the lead dwell time is less than two years. With longer dwell times, traction alone is likely to fail or cause complication because of fibrosis occurring at multiple points along the lead; other techniques are often required to break these attachments.

Traction with locking stylets
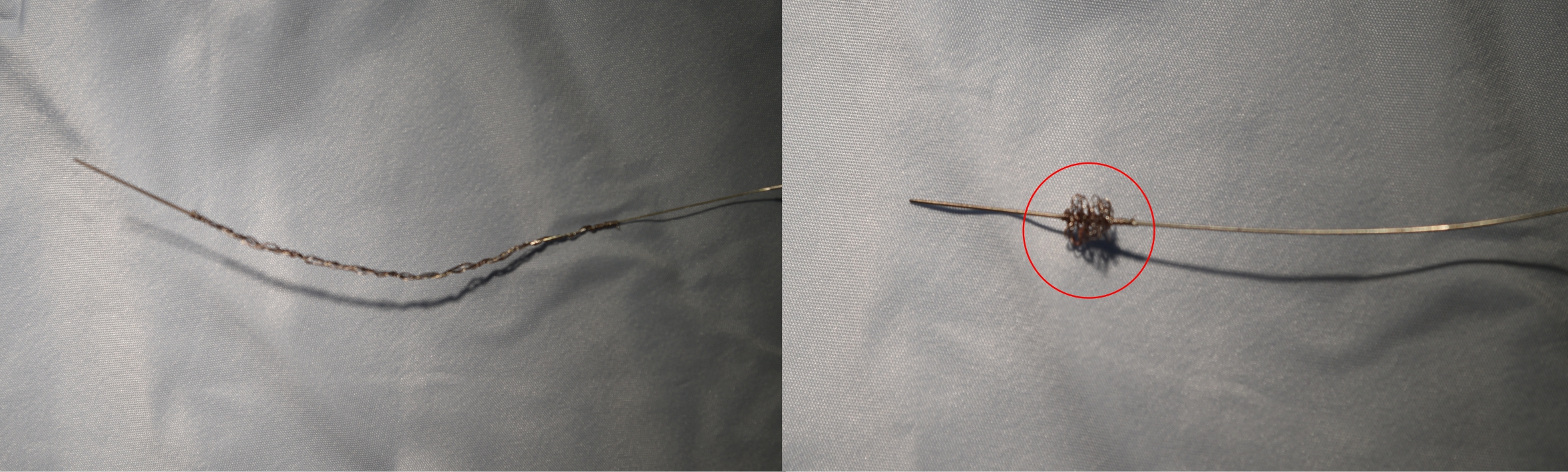
The next step usually involves concentrating force at the resistive hinge points by inserting a locking stylet through the lumen of a lead, advancing it to the tip and fixing the proximal end to the body of the lead with either a silk suture or compression coil (One-Tie®, Cook Medical LLC, Bloomington, IN, USA) (figures 1 and 2). Traction is thus transmitted more effectively to the distal end (Liberator, Cook Medical LLC, Bloomington, IN, USA) and Extor Set (VascoMed, Binzen, Germany) or along the entire length (Lead Locking Device EZ, The Spectranetics Corporation, Colorado Springs, CO, USA). As traction is applied, there is a risk of the distal conductor being disconnected or unwinding from the electrode with invagination of the surrounding tissue. The extraction success rate with use of simple traction and locking stylets is recorded at between 34% and 64%.
Sheaths
Sheaths are used if simple traction or locking stylets are not successful. These vary from simple mechanical telescoping sheaths to powered sheaths that utilise laser or radiofrequency energy or a rotating threaded tip.
Telescopic sheaths work by advancing over the lead, which acts as a guide rail, and they disrupt and break adhesions at the attachment site. Once the sheath has passed over the lead tip, it is steadied against the endocardium, providing the counter-pressure that permits traction to be focused on the tip without risk of invaginating the right ventricle. Telescopic sheaths are available in various materials (Teflon®, stainless steel and polypropylene) and sizes. In a retrospective analysis of over 2,000 lead extractions, an 85% success rate was reported for leads with a mean dwell time of 5.8 years.2 Other observational studies have reported lower rates, and it is likely that success varies between institutions due to equipment availability and local experience.
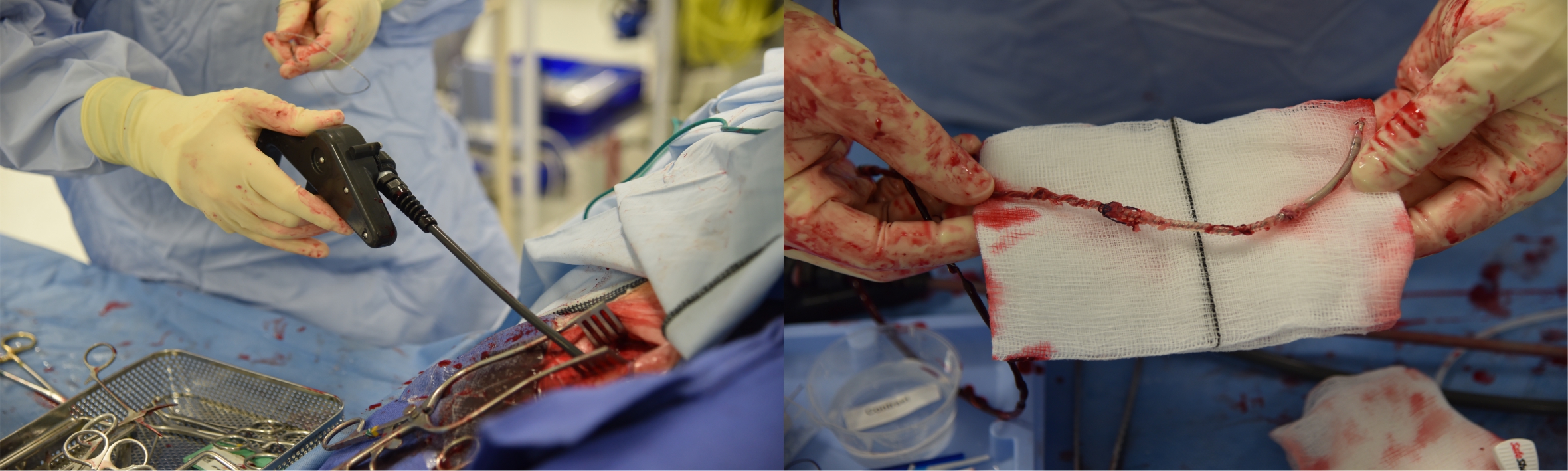
Powered traction
If blunt dissection with mechanical dilator sheaths fails to free the lead from its fibrous attachments, then powered tools are required. They have tips that burn or cut through fibrous tissue reducing the reliance on traction. These sheaths include electrical devices using either laser (Excimer, The Spectranetics Corporation, Colorado Springs, CO, USA) or radiofrequency energy (Perfecta Electrosurgical Dissection Sheath, Cook Vascular Incorporated, Vandergrift, PA, USA) and mechanical with a rotating threaded tip (Evolution®, Cook Medical LLC, Bloomington, IN, USA; TightRail™ Spectranetics Corporation, Colorado Springs, Colorado, USA).
Laser sheaths
The Excimer laser sheath passes over the lead and at points of resistance, a circumferential laser beam with a penetration depth to 100 µm is delivered to vaporise adhesions. The laser is unlikely to be effective on calcified fibrous tissue. The PLEXES (Pacemaker Lead Extraction with the Excimer Sheath) trial randomised 301 patients in need of a lead extraction to having the procedure performed with locking stylets and mechanical dilator sheaths (non-laser group) or locking stylets, mechanical dilators sheaths and a laser sheath (laser group). The laser group was found to have greater complete success rate 94% (vs. 64%) with a mean reduction in extraction time of three minutes. However, there were three life-threatening complications (including one death) in the laser group and none in non-laser. A comprehensive meta-analysis of 62 studies found the risk of major complications or death with laser techniques to be almost twice that of mechanical methods. The majority of serious complications were related to injury to the SVC, being lethal in almost 40% of cases. This complication is rarely seen with mechanical techniques. Delivering a fixed amount of energy irrespective of the strength of the adhesions without feedback about the force applied by the physician may make the procedure more hazardous than mechanical extraction. The meta-analysis also reported similar success rates with a mechanical-only approach. With advances in equipment and techniques, it is evident that mechanical lead extraction in centres with moderate volume and expertise is able to achieve a high rate of success without compromising safety.
Electrosurgical dissection sheath (EDS)
EDS uses radiofrequency energy to diathermy through fibrous tissue using bipolar current from two electrodes. It allows the localised application of energy instead of circumferential dissection as in laser sheath. There remains a paucity of data on the clinical effectiveness and complications of EDS with only three large single-centre studies performed, with similar success rates as laser sheath reported. In a randomised-controlled study of 120 patients, there was a 93% complete success rate with EDS compared with 73% with standard non-powered mechanical sheaths, with no deaths in either group.3 The EDS is less effective on calcified areas, sutures or insulation materials. Advances in mechanical methods have effectively eliminated the EDS from the market.
Rotational mechanical sheaths
These sheaths are the most recent major addition to the lead extractors’ armamentarium. Both currently available products have a handle trigger driven rotational tip at the end of a flexible sheath, which helps bore through the adhesions. The Evolution® system came to market first and, hence, has more published data than the TightRail™ system. The cutting action of these devices makes them ideal for cases where there is a large burden of calcification, which is frequently problematic at the venous access site. There remains no randomised-controlled trial data pertaining to this technology. Our experience with the Evolution system has recently been published. In 211 patients with a mean lead dwell time of 6.2 years, extraction was successful in 96% of cases with no major complications.4 Other groups have similarly reported clinical success rates of 98% with no procedural major complications (combined 375 patients).5-8
The different powered extraction tools, though similarly efficacious, should not be considered equal. In particular, the laser sheaths are associated with greater costs and increased risk of major complication.
Femoral snare
The success of extraction techniques using a superior approach has led to a reduction in the number of femoral extraction procedures performed. At the current time, it is usually a rescue procedure when extraction via the vein of implant is not possible, e.g. for free-floating lead ends or when leads remain adherent to the endocardium. The use of femoral snares is more likely with longer dwell times. Some operators use the femoral technique as a first-line approach, and outcomes are generally good in experienced hands, while procedure and fluoroscopy duration are usually higher.9 The Byrd Femoral Work Station (Cook Medical LLC, Bloomington, IN, USA) is the most commonly used tool and comes with a 16-Fr femoral sheath that acts as a work station and a 12-Fr inner sheath, pre-loaded with tip-deflecting wire and Dotter retriever snare. The procedure has a high success rate of more than 90% and, perhaps, should be adopted earlier in difficult extraction procedures.
Procedure outcome
Complete procedural success is defined as removal of the intended lead in its entirety from the vascular space with no life-altering complications. Clinical success is defined as removal of all but <4 cm of the intended lead material that does not negatively impact on the goal of the procedure. Conversely, failure refers to inability to achieve complete or clinical success, or when the procedure is complicated by death or a permanent life-altering complication.
Risks
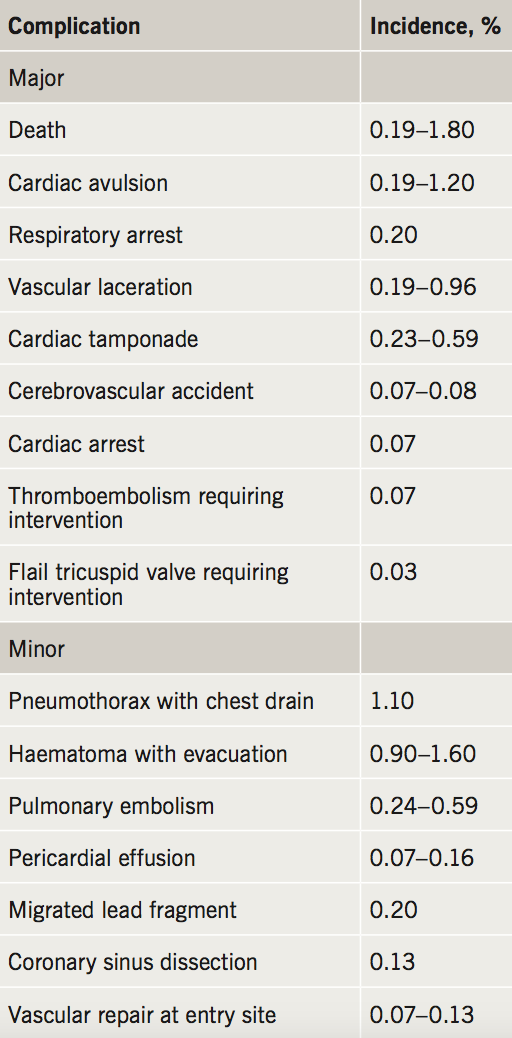
The process of extracting involves liberating the chronically implanted lead from fibrotic tissue adhering it to the venous system or myocardium. Table 2 details extraction-related complications and incidence. Given the potentially fatal complications, lead extraction procedures should only be performed in centres with experienced extraction teams, as well as having a cardiothoracic surgeon available with access to equipment to perform emergency sternotomy or thoracotomy within 5–10 minutes. Worryingly, however, a prospective survey of Heart Research UK (HRUK) members reported that 40% of extractions were carried out without an identifiable surgeon.10 It has been suggested that operators should be performing a minimum of 20 lead extractions annually to maintain competency.1 Factors that predict complication include patient/lead characteristics, operator experience and centre volume.
Authors’ viewpoint
Each lead extraction procedure presents its own challenges and operators need to be able to quickly adapt their approach, if clinically required. For most procedures, a step-wise approach should be undertaken as described above. Mechanical methods have demonstrated good safety and efficacy profile, and may become the preferred technique for CIED lead removal over laser.
While there is little dissent from the idea that all infected leads should be removed, the management of redundant leads is debated, and data are scarce. For example, when a patient requires an upgrade from a pacemaker to a defibrillator, some centres will remove the pacing lead, while others may abandon it. Further research is needed to clarify the circumstances in which abandonment of a redundant lead is acceptable.
Although extraction in experienced hands is a safe procedure, there are obvious reasons for preferring that it is performed in high-volume centres with immediate access to a cardiothoracic surgeon. Although leadless pacemakers are still an extremely small proportion of the devices being implanted, some require extraction and require techniques and equipment that are early in their development. Because of the importance of lead extraction it should be subject to compulsory reporting of accurate registry data of all cases, complications and failures in the manner of cardiac surgical procedures.
Key messages
- The number of transvenous lead extractions (TLE) being performed in England is increasing
- TLE is the gold standard treatment in cases of infection and superior vena cava obstruction
- TLE is safe but major complications are possible and therefore should be performed in high volume centres of excellence with adequate cardiac surgery cover
Conflict of interest
ON, HCP and MS: none declared. MMG has acted as a consultant for Biosense Webster and Medtronic
Articles in this supplement:
Introduction
Current and future perspectives on cardiac pacing
A brief history of cardiac pacing in the UK
Cardiac resynchronisation therapy – developments in heart failure management
Drugs with devices in the management of heart failure
His-bundle pacing: UK experience and HOPE for the future!
Leadless pacing
Techniques in pacemaker and defibrillator lead extraction
Remote monitoring
Remote follow-up of ICS: a physiologist’s experience
References
1. Kusumoto FM, Schoenfeld MH, Wilkoff BL et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017;14:e503–e551. https://doi.org/10.1016/j.hrthm.2017.09.001
2. Bongiorni MG, Soldati E, Zucchelli G et al. Transvenous removal of pacing and implantable cardiac defibrillating leads using single sheath mechanical dilatation and multiple venous approaches: high success rate and safety in more than 2000 leads. Eur Heart J 2008;29:2886–93. https://doi.org/10.1093/eurheartj/ehn461
3. Neuzil P, Taborsky M, Rezek Z et al. Pacemaker and ICD lead extraction with electrosurgical dissection sheaths and standard transvenous extraction systems: results of a randomized trial. Europace 2007;9:98–104. https://doi.org/10.1093/europace/eul171
4. Domenichini G, Gonna H, Sharma R, et al. Non-laser extraction of pacemaker and ICD leads: a decade of progress. Europace 2017;19:1521–6. https://doi.org/10.1093/europace/euw162
5. Starck CT, Rodriguez H, Hürlimann D et al. Transvenous lead extractions: comparison of laser vs. mechanical approach. Europace 2013;15:1636–41. https://doi.org/10.1093/europace/eut086
6. Witte OA, Adiyaman A, Smit JJJ et al. Success and complication rates of lead extraction with the first- vs. the second-generation Evolution mechanical sheath. Europace 2017;19:1717–22. https://doi.org/10.1093/europace/euw255
7. Delnoy PPHM, Witte OA, Adiyaman A et al. Lead extractions: the Zwolle experience with the Evolution mechanical sheath. Europace 2016;18:762–6. https://doi.org/10.1093/europace/euv243
8. Mazzone P, Migliore F, Bertaglia E et al. Safety and efficacy of the new bidirectional rotational Evolution® mechanical lead extraction sheath: results from a multicentre Italian registry. Europace 2018;20:829–34. https://doi.org/10.1093/europace/eux020
9. Bordachar P, Defaye P, Peyrouse E et al. Extraction of old pacemaker or cardioverter-defibrillator leads by laser sheath versus femoral approach. Circ Arrhythm Electrophysiol 2010;3:319–23. https://doi.org/10.1161/CIRCEP.109.933051
10. Sohal M, Williams SE, Arujuna A, et al. The current practice and perception of cardiac implantable electronic device transvenous lead extraction in the UK. Europace 2013;15(6):865–70. https://doi.org/10.1093/europace/eus383
