We describe a case of aortic rupture following transcatheter aortic valve implantation that was managed percutaneously.
Case description
An 80-year-old woman with severe symptomatic aortic stenosis was scheduled for transcatheter aortic valve implantation (TAVI), following Heart Team decision. Pre-procedural computed tomography (CT) angiogram revealed an area-derived annulus diameter of 23.7 mm, and calcium spur which extended from the coronary cusps commissure until the sinotubular junction. It was decided to implant a balloon-expandable TAVI (Sapien XT™ 26 mm) (figure 1A).
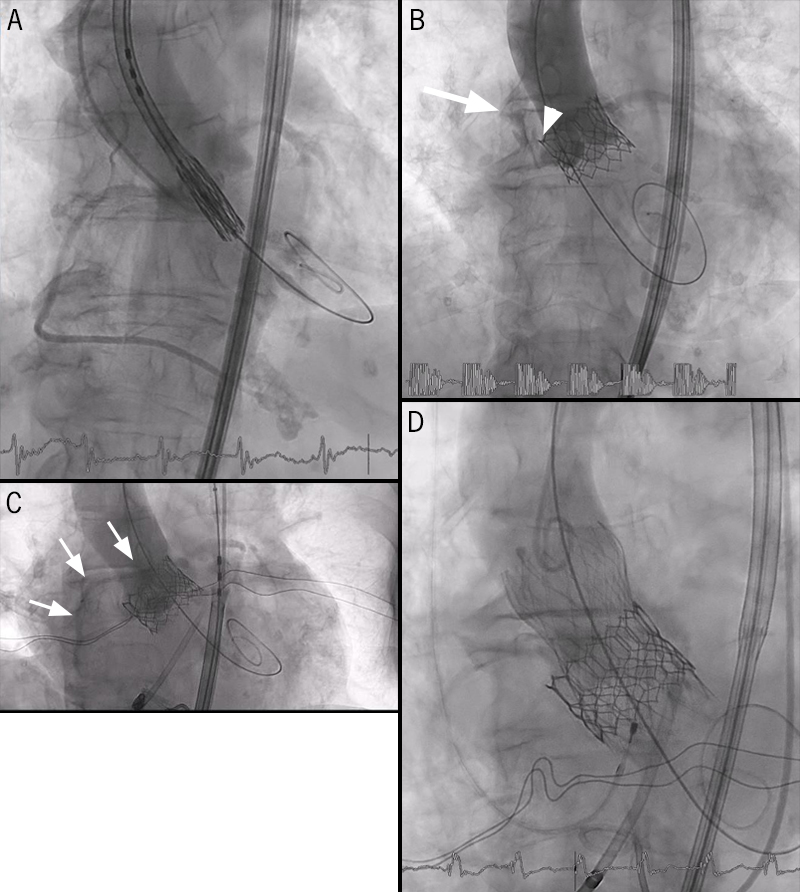
During the procedure, immediately after valve deployment, the patient suffered a cardiac arrest with electromechanical dissociation. Transthoracic echocardiogram (TTE) showed cardiac tamponade and angiogram showed a peri-annulus contrast leakage (figure 1B), so the diagnosis of annulus rupture was established. Consequently, reversal of anticoagulation, pericardiocentesis and blood transfusion were performed, after which the patient recovered spontaneous circulation. In order to seal the dissection, we decided to perform post-dilation and a quick valve-in-valve procedure with an auto-expandable prosthesis, without final leak (figures 1C and D).
After reviewing fluoroscopy images, it was assumed that the most probable causes were skirt protrusion on the aortic wall or due to calcium spur (figure 1B). The patient recovered well and re-evaluation TTE showed no signs of either prosthetic dysfunction or periprosthetic leak.
Five months later, the patient is fully asymptomatic and TTE showed absence of periprosthetic leaks or valve dysfunction.
Discussion
Aortic rupture incidence after TAVI is reported as being 0.4% to 2.3%. Balloon-expandable prosthesis and the presence of moderate-to-severe left ventricular outflow tract (LVOT) calcification increase the risk. This complication is associated with a seven-fold increase in 30-day mortality, and conversion to open surgery has an in-hospital mortality of 62%. Fortunately, major complications of TAVI are not common.1 However, as they evolve on a very fast downward spiral towards cardiogenic shock, an immediate percutaneous solution should be considered.
Conflicts of interest
None declared.
Funding
None.
Patient consent
The patient provided consent for images and clinical information to be published.
Reference
1. Coughlan JJ, Kiernan T, Mylotte D, Arnous S. Annular rupture during transcatheter aortic valve implantation: predictors, management and outcomes. Interv Cardiol 2018;13:140–4. https://doi.org/10.15420/icr.2018.20.2
