The British Cardiovascular Society (BCS) is the host Society for the European Society of Cardiology (ESC) Congress in 2015, which is being held for the first time in 63 years in London, at the ExCel Convention Centre. The ESC Congress is the largest cardiology meeting in the world with over 30,000 delegates attending from all corners of the globe.
The Congress offers a unique opportunity to showcase therapeutic and diagnostic advances, alongside cutting edge, bench- to-bedside science. There are five days of scientific sessions covering 150 cardiovascular topics with over 500 expert sessions. This year over 11,000 abstracts were submitted, and the theme is ‘Environment and the heart’.
We at the BCS are holding dedicated sessions at the Congress, and on Saturday 29th August we are hosting a General Cardiology Day for General Practitioners and Allied Professionals, so do encourage your colleagues and primary care colleagues to join us.
Extracurricular activities include a series of events at the Lee Valley VeloPark, where the Olympic track cycling events were held. Places can be booked on the BCS website. There will also be a ‘Heart trail,’ a one hour walk along the Southbank, from London Eye to City Hall. Participants will complete interactive challenges and solve clues, learning about heart health with the opportunity to win prizes along the way.
The British Journal of Cardiology will be covering the meeting in London, so look out for them, and also see the BCS website (http://www.bcs.com/) for further information, as well as the ESC Congress website (http://www.escardio.org/) for the full programme
Dr Sarah Clarke President, British Cardiovascular Society
Uninterrupted VKAs in ablation and device implantation
The European Society of Cardiology (ESC) has recommended uninterrupted anticoagulation with vitamin K antagonists (VKAs) during ablation and device implantation in a position paper presented at the European Heart Rhythm Association Europace – Cardiostim 2015 meeting held recently in Milan, Italy.
Chair of the writing group Professor Christian Sticherling (Universitätsspital Basel, Switzerland) said: “Traditionally we interrupted anticoagulation during device implantation and restarted it afterwards. And we bridged with heparin around the time of the operation. The new recommendation is to continue to give the VKA and perform the operation without any bridging. That shows the lowest rate of perioperative bleeding.”
He added: “Also new is the recommendation not to interrupt VKAs during ablation and particularly during pulmonary vein isolation which is the most common type of ablation nowadays.”
The paper, produced by the EHRA, has been published in Europace (doi: 10.1093/europace/euv190).
Arrhythmias and CKD
The first ESC recommendations for patients with cardiac arrhythmias and chronic kidney disease (CKD) were also presented at the meeting.
“There is increasing awareness in the cardiology community that renal impairment influences how we treat patients with arrhythmias,” said Chair of the writing group Professor Guiseppe Boriani (University of Bologna, Italy). “The introduction of non-vitamin K oral anticoagulants (NOACs) as an alternative to warfarin brought this issue to the fore since renal function determines whether or not they can be prescribed. The ESC decided it was a good time to introduce recommendations.”
The paper, produced by the EHRA, also recommends using estimated glomerular filtration rate (eGFR) as more reliable than serum creatinine for classifying the severity of CKD.
It has been published in Europace (doi: 10.1093/europace/euv202).
Time is muscle in acute heart failure
Urgent diagnosis and treatment in acute heart failure (AHF) has been emphasised for the first time in joint recommendations published in a consensus paper from the Heart Failure Association (HFA) of the ESC, the European Society for Emergency Medicine and the Society for Academic Emergency Medicine in the USA.
“This is the first guidance to insist that AHF is like acute coronary syndrome (ACS) in that it needs urgent diagnosis and appropriate treatment,” said Professor Alexandre Mebazaa, lead author and HFA board member. “By introducing the time to therapy concept together with new medications for AHF we hope to achieve the reductions in mortality and morbidity seen with ACS.”
The consensus paper outlines:
An algorithm for the management of AHF
Tests and treatments to be performed pre-hospital, and in the emergency department, coronary care unit (CCU) or intensive care unit (ICU)
The role of nurses in the management of AHF
How to use oxygen therapy and ventilatory support
How to manage new and currently prescribed medicines
Criteria for discharge from hospital and recommendations for follow up.
The paper has been published in the European Heart Journal (doi: 10.1093/eurheartj/ehs104).
The National Institute of Health and Care Excellence (NICE) has published a new quality standard on the treatment and management of atrial fibrillation (AF) in adults.
Dr Matthew Fay, a Bradford GP and specialist member of the committee that developed the standard, said: “This quality standard brings into sharp focus the key issue of stroke prevention. In doing so it continues to highlight the need for a change in practice so that everyone with AF is considered for anticoagulation and the quality of that anticoagulation is always kept under review by clinicians and commissioning groups.”
The quality standard includes six statements aimed at healthcare professionals caring for people in danger of developing, or who already have, AF. These include:
Adults with a type of AF called ‘non-valvular’ who have a stroke risk score of 2 or more (as estimated by their doctor using the CHA2DS2-VASC risk score) are offered treatment with an anticoagulant to lower their risk of having a blood clot that could cause a stroke.
Adults with AF who are prescribed an anticoagulant talk with their doctor at least once a year about the types of anticoagulants they could have and the advantages and disadvantages of each.
Adults with AF who are taking a vitamin K antagonist have regular blood tests to check whether the dose they are taking is at the right level to reduce their risk of stroke and bleeding problems.
Adults with AF who still have symptoms after treatment are referred within four weeks for specialised care that aims to ease their symptoms and reduce their risk of having a stroke or heart attack.
The quality standard also includes NICE’s first developmental statement on the provision and use of coagulometers for people on long-term vitamin K antagonist therapy, so they can check how well the treatment is working.
An ‘Ultrasound on demand’ scheme has recently been launched in the UK. Aimed at providing access to the best technology at an affordable monthly fee, ‘Ultrasound on demand’ offers a range of hi-spec ultrasound packages that are charged for when used, which means that ultrasound services can be tailored to both current and future needs as demand and patient workload change.
‘Ultrasound on demand,’ launched by Philips, is a flexible scheme with 50 options and access to advanced facilities, such as three-dimensional (3D) transoesophageal echo (TOE), which previously may have been limited by the restrictions of upfront investment costs.
The new ‘on demand’ approach provides the facility to explore new imaging options and future-proof services, by letting users upgrade and alter systems without locking in capital expenditure budgets, as additional functionality is only charged when used. Phillips hopes this flexibility will remove obstacles to more advanced and specialised treatments.
The cardiologist’s perspective
The BJC asked Dr Antoinette Kenny (Consultant Cardiologist and Specialist in Echocardiography, Regional Cardiothoracic Centre, Freeman Hospital, Newcastle upon Tyne) for her first impressions on the concept of this new scheme.
Dr Antoinette Kenny
‘The demand for ultrasound services has never been higher but in an era of economic uncertainty and funding constraints, healthcare providers are under increasing pressure to tighten their belts with capital spending budgets often the first to face the chop.
It is becoming increasingly difficult to persuade cash-strapped Trusts to commit to large capital outlay for new and replacement equipment and traditional leasing agreements can be plagued with inflexibility and are often seen as relatively poor value for money. In addition, it is often difficult to persuade those holding the purse strings to provide new services without a track record of effectiveness – the classic chicken/egg problem. Business managers may balk at opening their wallets for services which may only be used infrequently, a problem perhaps more pertinent to the private sector.
Into the maelstrom of service funding difficulties comes Philips’ new concept of ‘Ultrasound on demand’. The premise is a little like your home digital TV viewing service. There is a monthly rental package to provide your core ultrasound requirements. After this come the specialty add-on bundles, which are funded on a flexible ‘pay as you use’ basis with a monthly usage pricing cap to ensure a spending safety net.
Within a cardiology department, such on-demand facilities may include TOE, 3D imaging and advanced quantification tools such as strain and speckle imaging (the equivalent perhaps of choosing to pay to watch a Newcastle-Sunderland derby!). In such a manner, it is possible to provide specialty and new services without the pain of up-front capital outlay costs. Coupled with this is the benefit of advanced data analytics, which provide in-depth information on utilisation of services. These data are often difficult to obtain from the traditional IT systems within which we work and should facilitate strategic planning and rationalisation of service delivery, very worthy goals.
Pioneering approaches are required to promote a viable and synergistic relationship between healthcare providers and industry in harsh economic times and Philips are to be commended for their novel and flexible ‘Ultrasound on demand’ system. It will remain to be seen whether it provides sufficient novel and cost-saving features to rise above those provided by traditional leasing systems.
The devil, as always, will be in the details. However, on the information to date, it appears an attractive model with the potential to allay the financial anxieties of business departments whilst promoting development of services by clinicians – could this be a win-win?’
Two agents in a new cholesterol-lowering class – the PCSK9 inhibitors, which use human monoclonal antibodies to target PCSK9 (proprotein convertase subtilisin/kexin type 9) – have received European approval for lowering cholesterol.
Evolocumab (Repatha®, Amgen) is the first PCSK9 inhibitor to be granted marketing authorisation by the European Commission (EC) for use in people with primary hypercholesterolaemia or mixed dyslipidaemia, or in homozygous familial hypercholesterolaemia, who are unable to reach low-density lipoprotein cholesterol (LDL-C) goals with an optimal dose of statin (or a statin and other lipid-lowering agents), or in those who are statin-intolerant. The drug should be given in addition to a healthy diet.
Days later, alirocumab (Praluent®, Sanofi) also received EC marketing authorisation for lowering LDL-C in addition to diet and maximally tolerated doses of statins in patients with a primary hypercholesterolaemia or mixed dyslipidaemia who are not at target levels of LDL-C, or in those who are statin-intolerant.
Both agents are given by an injection every two weeks. The agents appear to be well tolerated with few patients having to discontinue treatment from adverse effects. Long-term safety, however, has not been established. Outcome studies on the effect of PCSK9 inhibitors on cardiovascular morbidity and mortality are awaited.
NICE recommendations for edoxaban
In two Final Appraisal Determinations, the National Institute for Health and Care Excellence (NICE) has recommended edoxaban (Lixiana®, Daiichi Sankyo) as an option for:
the treatment and secondary prevention of deep vein thrombosis and pulmonary embolism
preventing stroke and systemic embolism in people with non-valvular atrial fibrillation
The Final Appraisal Determinations are now out with consultees.
Young VTE patients require psychotropic drugs within five years
One in five young people who experience a venous thromboembolism (VTE) will require psychotropic medication within five years, reveals research presented at EuroHeartCare 2015, held recently in Dubrovnik, Croatia. The research, presented by nurse and PhD student Anette Arbjerg Højen (Aalborg Thrombosis Research Unit, Aalborg University Hospital, Aalborg, Denmark), showed young VTE patients were twice as likely to experience mental health problems requiring psychotropic medication as their healthy peers.
This study is the first to investigate the mental health prognosis of young VTE patients. Data from four nationwide registries was used: the Danish Civil Registration System, the Danish National Patient Register, the Danish National Prescription Registry, and the Danish Medical Birth Registry. The researchers identified 4,132 patients aged 13 to 33 years who had a first VTE between 1997 and 2010. A control group of 19,292 people without VTE was randomly selected and matched to the patients by sex and birth year.
All participants in the study were followed in the prescription registry for their first purchase of psychotropic drugs. The researchers found that psychotropic drug purchase was substantially higher among the young VTE patients compared to the control group. Among VTE patients the risk of purchasing psychotropic drugs following their diagnosis was 7.1% after one year and 22.1% after five years. Their excess risk relative to the controls was 4.7% after one year and 10.8% after five years.
Heart failure prognosis affected by cognitive impairment…
Heart failure patients with cognitive impairment may get progressively worse at adhering to medications, leading to poorer prognosis, according to research presented at Heart Failure 2015, held recently in Seville, Spain.
Researchers from the Kameda Medical Centre, Kamogawa, Japan, found that in a group of 136 elderly patients (average age 82 years), those who were cognitively impaired (74% of group) had a significantly worse prognosis than those who were not. Cognitive impairment also predicted a 7.5 times greater risk of worse prognosis than in those who were not cognitively impaired even after adjusting for other prognostic factors.
…and depression
Other research presented at the meeting from the OPERA-HF (Observational Study to Predict Readmission for Heart Failure Patients) study showed that moderate to severe depression is associated with a five-fold increased risk of all-cause mortality in patients with heart failure compared with those with no or mild depression.
Professor John Cleland (Imperial College London, and University of Hull) told the meeting that depression is common in heart failure and affects 20–40% of patients. “Our research clearly shows a strong association between depression and risk of death in the year after discharge from hospital. Recognition and management of depression may reduce mortality for patients with heart failure,” Professor Cleland added.
Visualising calcification a ‘wake-up’ call for patients
Looking at images of their own calcified coronary arteries may be a wake-up call for patients with newly diagnosed coronary artery disease to change their lifestyles, according to research presented at EuroHeartCare 2015, held recently in Dubrovnik, Croatia.
The Danish study assessed the influence of visualising coronary artery calcification in addition to standard information about risk and lifestyle modification on cholesterol and other risk factors in 189 patients with hyperlipidaemia and a new diagnosis of non-obstructive coronary artery disease.
Patients were prospectively randomised in a 1:1 fashion to the intervention or to standard follow up in general practice which consisted of information about risk and lifestyle modification.
“We found that patients who looked at images of their calcified coronary arteries were more likely to stop smoking, lose weight, eat a healthy diet, take recommended statins and reduce their plasma cholesterol levels. The results of our study suggest that visualising their health threat motivates patients to make changes to reduce their risk,” said the study presenter, nurse and PhD student Rikke Elmose Mols (Aarhus University Hospital-Skejby, Denmark).
A recent study has found that grip strength is a stronger predictor of health than systolic blood pressure, leading study authors to suggest it could be used as a quick, low-cost screening tool to identify high-risk patients among people who develop major illnesses such as heart failure and stroke. The PURE (Prospective Urban-Rural Epidemiology) study was carried out on 139,691 adults in 17 countries using a handgrip dynamometer to assess hand grip. It found low grip strength was linked with a 17% higher risk of cardiovascular death and a 17% higher risk of non-cardiovascular mortality. The study has been published in The Lancet (doi: 10.1016/S0140-6736(14)62000-6).
In this regular series ‘ECGs for the fainthearted’ Dr Heather Wetherell will be interpreting ECGs in a non-threatening and simple way. In this issue, we look at the digitalis effect on ECGs
This issue, we have a little teaser for GPs, who may reasonably come across this kind of electrocardiogram (ECG) any day of the week.
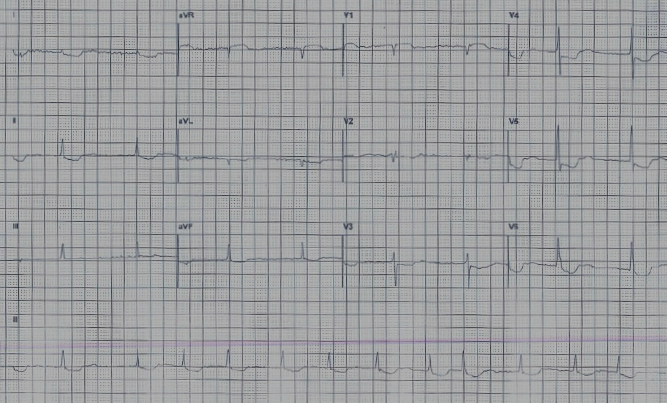
Figure 1 shows the ECG of a well, 83-year-old woman, who attended her GP’s surgery for her ‘annual review’. As part of this review, the practice nurse carried out a routine ECG.
Figure 1. The electrocardiogram obtained during the annual review
Believe or not, it’s possible to answer the following three questions from this ECG:
Q1: What chronic condition was being monitored at her annual review?
Q2: What is she taking for this condition?
Q3: What action should the GP take now?
Let’s go through the ECG together.
For the time being, just ignore the funny shaped ST segments.
Start as always, by checking the background rhythm:
are there P waves present?
are the QRS complexes regular?
I’m sure you will agree that the answer to both questions is ‘no’.
This ECG shows an underlying rhythm of atrial fibrillation (AF) with a good rate control (around 80 bpm ventricular response).
The ‘quick’ way to measure rate on an irregular rhythm is by counting the number of complexes in six seconds (30 large squares) and multiplying by 10. In this ECG, for example, taking the long lead II strip, there are eight complexes in 30 large squares. So: 8 x 10 = 80 bpm.
Answer 1
We can assume that this lady was attending the surgery for her annual AF review. As AF is a precursor to many other cardiac conditions, an annual ECG is helpful, but arguable. An annual pulse rate check is a bare minimum.
Answer 2
Figure 2. For the digitalis ‘effect,’ remember Salvador Dali
This lady is taking digoxin. The ST-T complexes here are ‘scooping’ – consistent with a digitalis ‘effect’. In the digitalis effect, the ST segments are often likened to a ‘reverse tick’ or to the shape of Dali’s moustache (see figure 2).
The important learning point here is that the digitalis ‘effect’ does not necessarily mean toxicity. These ECG features can often be seen when digoxin levels are within the therapeutic range.
In other words, ECG changes with digoxin can be either:
Therapeutic (also known as the digitalis ‘effect’)
ST-segment depression resembling a ‘reverse tick’
Reduced T wave
Shortening of the QT interval.
Or
Toxic
T-wave inversion
Arrhythmias.
Answer 3
This lady appears clinically well and denies any untoward symptoms. Given the changes seen on her ECG, we can probably assume that this is simply a digitalis ‘effect’ and no treatment or adjustment to her medication is necessary. It wouldn’t hurt to check her digoxin levels for reassurance (and while you’re at it, her serum potassium too, just in case) but this isn’t necessarily essential.
In summary: Treat the patient, not the ECG.
No action necessary.
Digoxin
The common foxglove species is Digitalis purpurea. Digoxin is derived from the species Digitalis lanata and was first described by William Withering in 1785. It is sometimes used to increase cardiac contractility (positive inotrope) and as an anti-arrhythmic agent to control heart rate (e.g. in fast AF). Superior rate-limiting agents, such as beta blockers, have now superseded digoxin as a first-line agent but its role remains important in AF associated with heart failure.
Symptoms of digoxin toxicity
These include:
lethargy
nausea and vomiting
diarrhoea
abdominal pain
visual disturbances
hallucinations and delirium
severe headache.
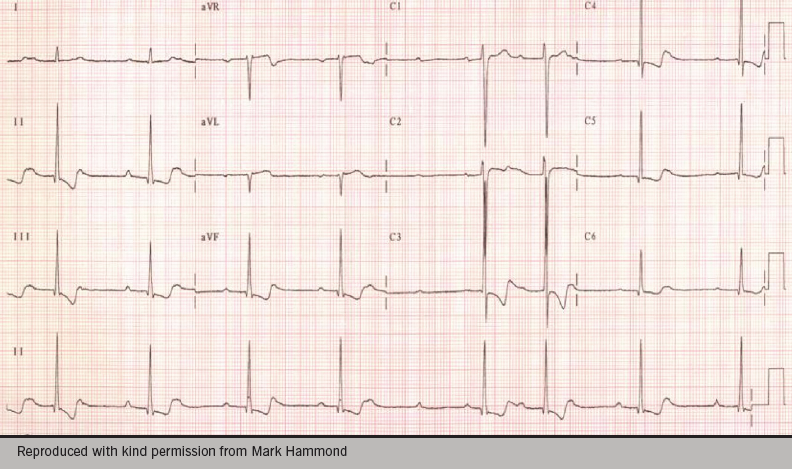
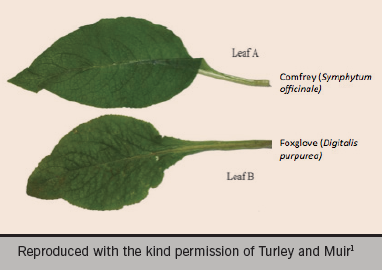
Figure 3. An example of an electrocardiogram obtained after an overdose of digitalisFigure 4. A potentially fatal misidentification – the comfrey leaf versus the foxglove leaf
Almost any dysrrhythmia may occur except sinus tachycardia, superventricular tachycardia (SVT) and rapid AF.
Figure 3 shows an example of an ECG after a digitalis overdose in a very unwell patient with all the above symptoms and digoxin levels of 4.7 ug/L (therapeutic range 1–2 ug/L). Note the irregular bradycardia, atrioventricular block and T-wave inversion.
This ECG was recorded on a young farm worker who was admitted after eating foxglove leaves, having mistaken them for edible comfrey (see figure 4). Hopefully, the history and examination would have been clues here!
Editors’ note
This is the last article in our ECGs for the fainthearted series. We would like to thank Heather Wetherell for her hugely popular contributions and hope she will be writing for us again soon.
We read with interest Diana Gorog’s recent article on the uptake of non-vitamin K oral anticoagulants (NOACS) in the UK.1 She drew attention to the slow uptake of these agents in the UK as opposed to many countries in Europe, and certainly the USA, and to the role that local medicines management committees (MMCs) may play in this. While the National Institute for Health and Care Excellence (NICE) guidance regarding all three NOACs available in the UK (apixaban, dabigatran and rivaroxaban) is that they should be available as an option for stroke prevention in non-valvular atrial fibrillation (AF), many MMCs in the UK have sought to control prescriptions of the new agents by issuing policies which keep warfarin first line, and reserve NOACs for situations where warfarin is unsuitable.
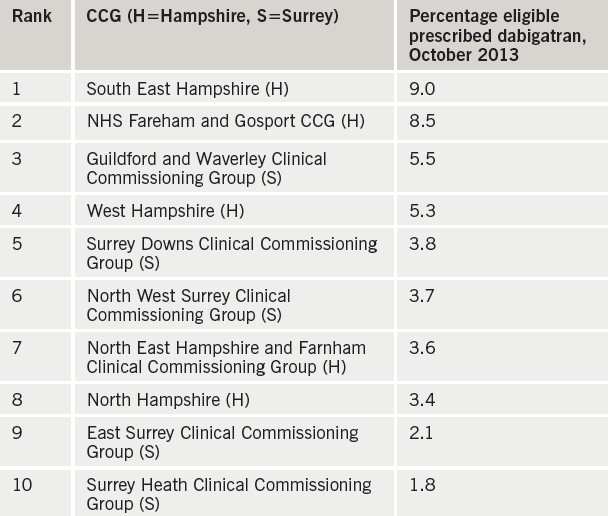
Table 1. Clinical Commissioning Groups (CCGs) prescribing dabigatran
As part of a NICE scholarship project, we sought to collect further information on the influence of these restrictive local prescribing policies on the prescribing patterns of doctors. The focus of the project was on the Surrey/Hampshire area: this area was chosen as particularly illuminating, as the two neighbouring counties had different anticoagulant prescribing policies. Clinical Commissioning Groups (CCGs) in Surrey followed the policy of the Surrey Prescribing Clinical Network, which states: “Patients with a CHA2DS2-VASc score ≥2 or CHA2DS2-VASc score 1 and considered high risk should be initiated on warfarin in the first instance, unless contraindicated. Warfarin remains the agent of choice for the prevention of stroke and systemic embolism in AF”.
In Hampshire, on the other hand, CCGs largely followed the policy of Basingstoke, Southampton and Winchester District Prescribing Committee. This did not restrict clinician choice, but simply stated NICE’s position that new anticoagulants should be considered as an option. Particularly significantly, it stated: “Prescribers may wish to consider if newly diagnosed patients are suitable for the new OACs in the first instance”.
We focused on one of the NOACs – dabigatran – and compared prescribing rates in the five Hampshire and five Surrey CCGs. Data on number of prescriptions was obtained from dabigatran’s manufacturer, Boehringer Ingelheim; this was combined with CCG population numbers (Office for National Statistics data2) and AF prevalence (Health and Social Care Information Centre data3) to give an estimate of the population eligible for anticoagulation. Significantly, the top two CCGs for dabigatran prescribing were both in Hampshire, and the bottom two both in Surrey (see table 1).
We then sought further evidence for the influence of local prescribing policies by surveying 120 primary care prescribers in the Surrey/ Hampshire area. 33% responded; two thirds of respondents felt that their prescribing of dabigatran was influenced by financial pressure from their local CCG. Interestingly, however, there was no difference between Surrey and Hampshire prescribers in their answers to this question. We also asked respondents to pick the factor which had the strongest influence on their decision making regarding dabigatran prescribing. Replies showed an even split between NICE guidance, financial constraints, safety concerns and lack of familiarity (see figure 1).
Figure 1. Most important influence on dabigatran prescribing, as selected by Surrey and Hampshire primary care prescribers
We concluded that local prescribing policies do have an effect on prescribing habits, but that they are only one of a number of factors which influence prescribers when they are selecting an anticoagulant. NICE guidance clearly ranks among the most important of these factors, which is in agreement with data published recently in this journal by Campbell et al, suggesting that NOAC prescribing in the UK has increased since the publication of the revised NICE guidance on atrial fibrillation in 2014.4 This guidance emphasises the importance of anticoagulation for all but the lowest risk patients, and indicates that vitamin K antagonists and NOACs should be considered as equally valid options.5
As an aside, we also collected data on prescription rates for all anticoagulants, including warfarin, over the year from November 2012 to October 2013; we found a steady increase over time in prescriptions for all the anticoagulants. This confirms the encouraging data from registries such as PREFER in AF,6 which suggest that, regardless of anticoagulant used, increasing numbers of patients in the UK with AF who are at risk of stroke are being offered the protection of anticoagulation.
Acknowledgements
We thank Dr C Hendry, Royal Surrey County Hospital (Project Supervisor); Mr B White, Nottingham University Hospital (NICE Mentor); and Mr F Ratcliff, Boehringer Ingelheim.
Sources of support
This work was undertaken as part of National Institute for Health and Care Excellence Scholarship scheme 2013–2014.
Conflict of interest
None declared.
Dr Matthew Rogers
Haematology SpR
Royal Marsden Hospital, Sutton, Surrey SM2 5PT
Reference
1. Gorog D. Rivaroxaban in nonvalvular AF – UK experience in perspective. Br J Cardiol 2014;21 (suppl 1):S1–S11.
3. Quality and Outcomes Framework, 2011–12, PCT level. Health and social care information centre, published October 2012. http://www.hscic.gov. uk/catalogue/PUB08722. Accessed July 2015.
5. National Institute for Health and Care Excellence. Atrial fibrillation: the management of atrial fibrillation. CG180. London: NICE, June 2014. Available from: http://www.nice.org.uk/ guidance/cg180
6. Kirchhof P, Ammentorp B, Darius H et al. Management of atrial fibrillation in seven European countries after the publication of the 2010 ESC Guidelines on atrial fibrillation: primary results of the PREvention oF thromboemolic events – European Registry in Atrial Fibrillation (PREFER in AF). Europace 2014;16:6–14. http://dx.doi.org/10.1093/europace/eut263
Authors: Robert Loveridge, Sameer Patel, Georg Auzinger, Julia Wendon
Correspondence from the world of cardiology
Dear Sirs,
We would like to thank Professor Stephen Westaby for his interesting editorial1 on mechanical circulatory support in the setting of the National Institute for Health and Care Excellence (NICE) guidelines on acute heart failure. He discusses two examples of patients who were not served well by the current commissioning arrangements in place for acute heart failure and longer term ventricular assist device (VAD) destination therapy, and argues compassionately for a widening of access to technologies such as extracorporeal membrane oxygenation (ECMO) and left VAD (LVAD) to support patients where required.
We could not agree more. Within our own institution, King’s College Hospital, London, a tertiary cardiovascular centre, cardiac arrest centre and major emergency department, the critical care ECMO service offers temporary mechanical circulatory support to patients with refractory cardiac arrest or cardiogenic shock. In just over two years, we have undertaken either extracorporeal cardiopulmonary resuscitation (n = 13) or veno-arterial (VA) ECMO (n = 15) on 28 patients (mean age 42 years, range 15–64 years). All patients were INTERMACS 1 (Interagency Registry for Mechanically Assisted Circulatory Support), moribund on supra-maximal critical care support in multi-organ failure, or dead at the time of institution of extracorporeal life support (ECLS); for 26 out of these 28 patients (93%), seven were out of hospital cardiac arrests, 17 were in hospital cardiac arrests and two were failure to wean from cardiopulmonary bypass.
The wean rate from ECLS was 64% with a survival to hospital discharge of 50% with good neurological outcomes (as assessed by cerebral performance categories with 12 [86%] having the best outcome of 1 on the cerebral performance category [CPC] scale and the remaining being 2 on the CPC scale). All the survivors, except one who died following biventricular assist device implantation after transfer, are still alive and independent, and only one patient required heart transplantation at another institution. Three of those who did die, however, despite being weaned from VA ECMO, were declined transfer for consideration of longer term VAD destination therapy although they would surely have been considered for this in Europe and the USA.
If our experience is replicated in other major acute hospitals, as is likely, there is a significant potential to impact on the mortality of these young patients who have few other options. As Professor Westaby points out, these technologies cannot be restricted to only centres offering transplantation. They also need to be available in major acute provider centres. We agree that the government and commissioners need to address this shortfall in both facilities and equality in access urgently.
We would welcome cross-site discussions on building a pathway for these patients right from their presentation at major emergency departments and tertiary referral cardiac centres through to the supra-regional cardiac transplant centres.
Conflict of interest
None declared.
Robert Loveridge
Consultant in Intensive Care Medicine
Sameer Patel
Consultant in Intensive Care Medicine
Georg Auzinger
Consultant in Intensive Care Medicine
Julia Wendon
Consultant in Intensive Care Medicine
King’s College Hospital NHS Foundation Hospital (King’s Health Partners), Denmark Hill, London, SE5 9RS.
When the National Institute for Health and Care Excellence (NICE) clinical guideline 180 on atrial fibrillation (AF) was published in June 2014, out if its many recommendations, two points seemed paramount. First, it is the patient, and not the clinician, who should make the decision as regards the nature of the treatment they are to receive, whether this be for stroke prevention or for symptom management, and that all those with AF should be offered stroke preventive therapy, with the exception of those without risk factors (CHA2DS2-VASc 0 or 1 in females).
Dr Matthew Fay (Westcliffe Medical Practice, Shipley)
Honarbakhsh et al. highlight an important point in their paper: when should this be done and who should take responsibility. Their review of patients who have been admitted acutely with AF or atrial flutter, looking at the outcome of anticoagulation if risk factors are present, seems to provide lamentable data, with only 57% being referred for oral anticoagulation.
Of course, there may be a question as to whether, with patient-led decision-making, the acute hospital ward is the right environment for a considered and final decision as regards this important question. We need to consider the emotional state of the patient and their care network at this stage, but also the opinion of the consulting physician seeing the patient in an acutely unstable state and away from their normal environment, with understandable concerns regarding the adverse consequence of intervention with anticoagulants.
This situation is then amplified on discharge, when the patient is returned to the supervision of the general practitioner, who sees the patient not receiving intervention, or worse receiving antiplatelet agents, where the clinician has treated their own anxiety about leaving a patient unprotected from cardio-embolic stroke.
The issue here maybe more one of communication, through the system from acute care to chronic care, with clinicians understanding what has happened previously and what their role in ongoing management may be.
The outcome of admission to hospital with AF or atrial flutter, as regards stroke prevention, has four outcomes:
The issues around AF stroke have been discussed and the patient has received an anticoagulant.
The issues around AF stroke have been discussed and the patient has, through informed choice, declined an anticoagulant at this time, and should be highlighted for future discussion within the GP records.
The issues around AF stroke have been considered but, in the acute situation, it was thought the bleeding risk of an anticoagulant was excessive, but this decision should be reconsidered once the patient is in a more stable situation.
The patient is not competent to make the decision and the hospital-based team has discussed this within the multi-disciplinary team (MDT) and appropriate patient representatives, and a decision has been made to not anticoagulate the patient.
The clear comment from Honarbakhsh et al. is that the system, designed the way it currently is, will only continue to give the poor outcomes seen in their study. Better communication between key clinicians in the patient care pathway and appropriate implementation of the NICE recommendations for anticoagulation therapy may be the way forward.
Conflict of interest
Westcliffe Medical Practice has been variously given by: Abbott, Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, 4S Dawn, INRstar, Medtronic, Oberoi Consulting, and Pfizer.
Editors’ note
Please see the article by Honarbakhsh in this issue.
Inflammation plays an important role in the pathogenesis of coronary heart disease (CHD). Several inflammatory cytokines have shown a direct association with the development of atherosclerosis. Recently, there have been a number of experimental studies exploring the potential anti-inflammatory role of currently used therapeutic agents including antibiotics, immuno-suppressive drugs and non-steroidal anti-inflammatory medications. This review summarises the available evidence base and the potential role of these agents in current clinical practice.
Introduction
Coronary heart disease (CHD) is the leading cause of death worldwide. Chronic subclinical inflammation is a key recognised process in the pathogenesis of CHD, and may play an important role in atherogenesis.
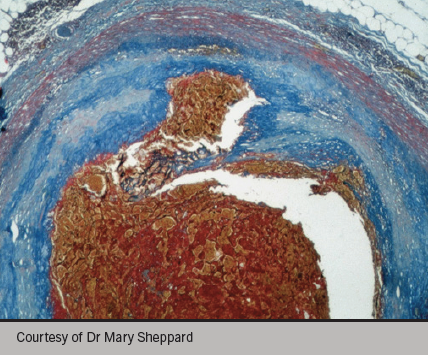
Figure 1. Atherosclerotic plaque rupture
Atherosclerosis is a complex multi-factorial disease process, which is initiated at the endothelium in response to various forms of injurious stimuli (shear stress, oxidative stress, arterial pressure changes) including inflammation. These factors appear to alter the endothelial cell’s capacity to maintain homeostasis and vascular tone and leads to the so-called endothelial ‘dysfunction’, predisposing to the development of atherosclerosis. Inflammation appears to act as a significant trigger in the atherosclerotic plaque rupture (see figure 1), preceding acute cardiac events.
Inflammation and atherosclerosis
The degree of inflammatory activity, as detectable both within the atherosclerotic plaque and in the circulation, is associated with plaque destabilisation and atherothrombotic complications. It has become apparent that both endothelial cell activation and monocyte/macrophage activation play a significant role in rapid coronary artery disease (CAD) progression. Endothelial cell activation is accompanied by the enhanced expression of cell adhesion molecules, such as vascular cell adhesion molecule-1 (VCAM-1), a significant reduction in nitric oxide production, and a remarkable increase in the formation of reactive oxygen species. As a result, endothelial function is impaired, and the inflammatory cascade is activated with release of cytokines and growth factors. These factors stimulate migration and proliferation of vascular smooth muscle cells and fibroblasts, which form a fibrous cap over the atherosclerotic lesion.
Interleukin-6 (IL-6) an inflammatory cytokine produced mainly by T cells, macrophages, and adipocytes, promotes inflammatory responses via the membrane-bound or circulating soluble interleukin-6 receptor (IL-6R) on monocytes, hepatocytes, and endothelial cells. High-circulating concentrations of IL-6 are associated with increased risk of CHD events in prospective observational studies. Subsequently, the cap becomes weak, following release of proteolytic enzymes, leading to plaque rupture and exposure of underlying collagen to platelets, and subsequent thrombus formation, which can result in acute coronary syndrome.
Inflammation has also been extended to the disorders of coronary microvasculature, and associated with special subsets of CAD, such as silent myocardial ischaemia, myocardial ischaemia–reperfusion, cardiac syndrome X, variant angina, coronary artery ectasia, coronary calcification and in-stent restenosis.
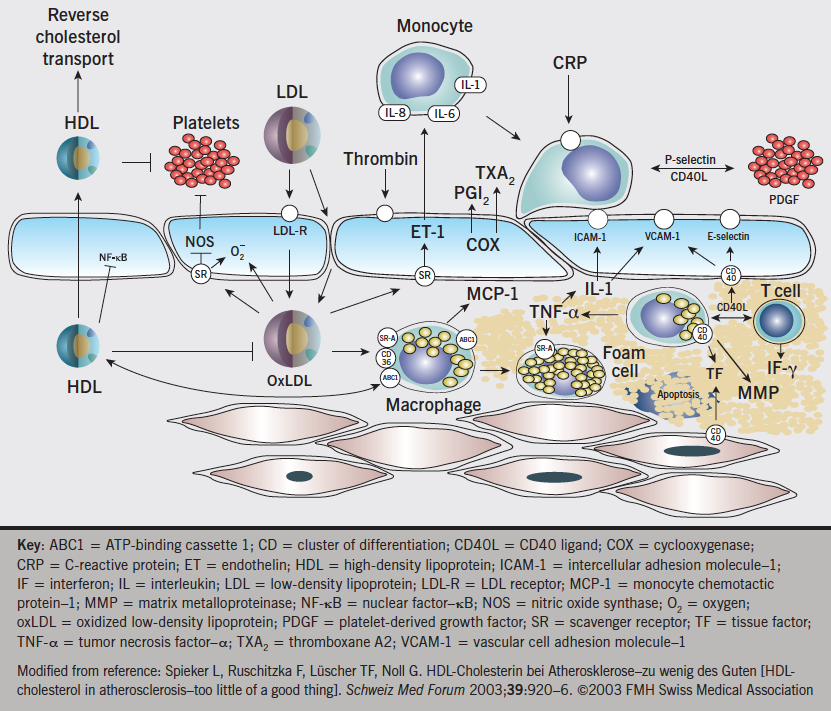
Several systemic inflammatory markers reflect different degrees of inflammation and have been implicated as independent risk factors in cardiovascular disease, especially in unstable coronary syndromes. A series of prospective studies provide consistent data documenting that mild elevation of baseline levels of high-sensitivity C-reactive protein (hs-CRP) among apparently healthy individuals is associated with higher long-term risk for cardiovascular events. Recent studies suggest that, besides CRP, other inflammatory biomarkers such as cytokines (interleukin [IL]-1, IL-6, IL-8, monocyte chemo-attractant protein-1 [MCP-1]), soluble CD40 ligand, serum amyloid A (SAA), selectins (E-selectin, P-selectin), myeloperoxidase (MPO), matrix metalloproteinase (MMPs), cellular adhesion molecules (intercellular adhesion molecule 1 [ICAM-1], VCAM-1), placental growth factor (PlGF) and A(2) phospholipases may have a potential role for the prediction of risk for rapid progression of CAD, regardless of plaque morphology (figure 2).
Figure 2. Endothelium and atherosclerosis. Interplay of lipids, inflammatory cells, mediators, and the vessel wall in atherogenesis
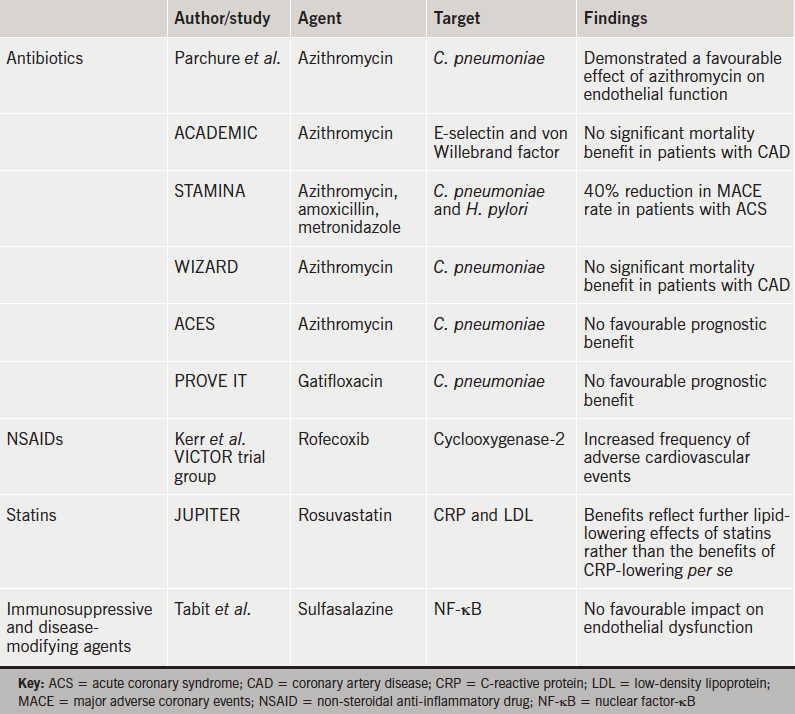
It is less clear, however, whether elevated levels of circulating inflammatory markers play a role in the extent and severity of atherosclerosis, and such pathobiological paradigms remain controversial. The identification of inflammatory biomarkers and cellular/molecular pathways in atherosclerotic disease represent important goals in cardiovascular disease research, in particular, with respect of the development of therapeutic strategies to prevent or reverse atherosclerotic diseases. This pathophysiology is amenable to modification by drugs targeting cell proliferation, cell migration, osteogenic/fibrous turnover of the extracellular matrix ranging from anti-metabolites, glucocorticoids, specific cytokine and leukotriene antagonists to classic immunosuppressive agents and vaccines directed specifically at certain relevant diseases (table 1).
Table 1. Studies conducted with various types of agent, their targets and findings
Antibiotics
Recently, there have been a number of experimental studies exploring the potential anti-inflammatory role of currently used therapeutic agents. Sulfasalazine is a disease-modifying agent which acts as an inhibitor of nuclear factor-κB (NF-κB). In experimental studies, NF-κB acts as an inflammatory regulator and is known to cause endothelial cell dysfunction and reduce nitric oxide production. However, in a recent study by Tabit et al., the clinical use of sulfasalazine in patients with established CAD, was not demonstrated to have any favourable impact on improvement of endothelial dysfunction.1
Antibiotics may play a role in the general inflammatory process, possibly by down-regulating pro-inflammatory cytokines. Parchure et al., demonstrated a favourable effect of azithromycin on endothelial function in patients with Chlamydophila pneumoniae infection with known CAD.2 This was also evident in the ACADEMIC (Azithromycin in Coronary Artery Disease: Elimination of Myocardial Infection with Chlamydia) study where the levels of E-selectin and von Willebrand factor were significantly reduced in the treatment arm. However, despite this effect, azithromycin failed to show any significant mortality benefit in patients with CAD.3 In contrast, the STAMINA (South Thames Trial of Antibiotics in Myocardial Infarction and Unstable Angina) trial reported a 40% reduction in major cardiac event rate in patients with acute coronary syndromes (ACS) who received the same antibiotic treatment during hospital admissions.4 The reason for these contradictory findings remains unexplained.
The WIZARD (Weekly Intervention with Zithromax for Atherosclerosis and its Related Disorders) study was a randomised-controlled trial, which aimed to understand the impact of antibiotics on CAD events. Similar to the ACADEMIC trial, this study also failed to show any evidence for reduction of cardiac events in stable post-myocardial infarction patients, who were treated with azithromycin following exposure to C. pneumoniae.5 Another, the ACES (Azithromycin and Coronary Events Study) trial, was one of the largest randomised, placebo-controlled trials, in which more than 2,000 patients were randomised to receive azithromycin or placebo, with a follow-up of four years. Despite confirming the presence of C. pneumonia in atherosclerotic plaque lesions, azithromycin therapy was not associated with any favourable prognostic benefit.6
A new generation of antibiotic, fluoroquinolone gatifloxacin, was also found to be less effective in reducing cardiac events in the recent PROVE IT (Pravastatin or Atorvastatin Evaluation and Infection Therapy) trial.7 The results of these trials affirm and strengthen the recommendation against prophylactic use of antibiotics to prevent future cardiac events among people with established CAD.
Fibrinogen
The presence of elevated fibrinogen levels in blood is also indicative of active inflammatory processes. In epidemiological studies, increased fibrinogen levels have been shown to be associated with risk of developing ischaemic heart disease. However, it is not apparent whether this association reflects causation, in the context of the simultaneous presence of other risk factors. In a recent meta-analysis by Danesh et al., a putative link between serum fibrinogen levels and CHD has been demonstrated.8 However, Keavney et al. proved, using genetically based analyses, that there is no major association between fibrinogen level and risk of CAD.9
Non-steroidal anti-inflammatory drugs
Anti-inflammatory compounds include cyclooxygenase-2 inhibitors and other inhibitors of eicosanoid synthesis. An increased incidence of cardiovascular events in patients treated with the cyclooxygenase-2 inhibitor rofecoxib indicates the need for a cautious approach with these medications in patients with cardiovascular disease.10 Aspirin is an antiplatelet and anti-inflammatory drug. It acts by down-regulating eicosanoid synthesis, and the benefits of reducing risk of first myocardial infarction are maximised in patients with inflammation and elevated CRP levels. Low-dose aspirin has antiplatelet effects, stabilises atherosclerotic plaques, and reduces inflammation in coronary vessels.
Statins and role of CRP
Statins are a very effective group of medications for primary and secondary prevention of atherosclerotic disease, which act by reducing low-density lipoprotein (LDL)-cholesterol levels, as well as by reducing CRP levels with an additional anti-inflammatory effect. There is a direct correlation between statin therapy and lower CRP concentrations, as shown in several studies and trials. They prevent recruitment, migration and cell adhesion to endothelium by lowering cytokine concentrations and reducing chemokine production. In addition, they increase the production of nitric oxide, and hence, protect the endothelium. They also inhibit inflammatory pathways regulated by proteins such as Ras and Rho.11
The recommendation for statin therapy in otherwise healthy individuals with low levels of LDL and high levels of CRP is controversial. JUPITER (Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin trial),12 a major randomised, double-blind, placebo-controlled trial, was designed to investigate the use of rosuvastatin in the primary prevention of cardiovascular disease. This was focused on patients with normal LDL-cholesterol levels but increased levels of hsCRP, and the results demonstrated that the benefits in this group of patients may simply reflect further lipid-lowering effects in people who would not be considered for pharmacotherapy, rather than the benefits of CRP-lowering per se. Ridker et al.12 did not support the development of therapeutic strategies specific for lowering CRP levels in plasma in this study.
In 2009, the Mendelian randomisation study published in the Journal of the American Medical Association suggested that CRP does not play a causal role in cardiovascular disease. However, it still could be a useful marker of cardiovascular disease risk.13 This provoked a debate over the role and value of CRP as a biomarker and possible therapeutic target in heart disease. Moreover, in their British Medical Journal article in 2011, the C-Reactive Protein Coronary Heart Disease Genetics Collaboration (CCGC) suggested that CRP level is unlikely to be even a modest causal factor in CHD.14
Other therapies
The immunosuppressive drugs cyclosporine and sirolimus block the activation of T cells and prevent smooth-muscle proliferation. Sirolimus-coated stents are currently used to prevent restenosis after angioplasty. It is not yet known whether or not this family of compounds can be used in ACS.
Therapies based on elevating levels of high-density lipoprotein (HDL) have the potential for acting through the attenuation of acute and chronic conditions of inflammation as they relate to atherosclerosis. HDL itself, for example, may have inhibitory effects on the activation of macrophages and other immune cells promoting healthy endothelial function and inhibiting the formation of atherosclerosis. Recent studies suggest that HDL inhibits growth factors and cytokine receptor signalling, and may also participate in reverse cholesterol transport. Conversely, circulating dysfunctional HDLs are associated with inflammation due to their pro-oxidative and pro-inflammatory properties.15
Cyclosporine A is a potent inhibitor of the myocardial cell mitochondrial permeability transition pore (MPTP). The opening of the MPTP at the time of myocardial reperfusion following percutaneous coronary intervention or thrombolysis could trigger metabolic alterations and release of cytokines leading to cardiomyocyte death. A pilot study by Piot et al16 indicated that administration of cyclosporine at the time of reperfusion was associated with a reduction in the infarct size in STEMI, limiting the impact of ischaemic-reperfusion related cell injury. This work has been substantiated by Mewton et al.17 in a follow up study, which demonstrated sustained improved left ventricular function with no evidence of adverse remodelling. The ongoing CIRCUS18 trial (Cyclosporine to ImpRove Clinical oUtcome in ST-elevation myocardial infarction patients) is likely to consolidate the evidence to support the potential clinical utility of cyclosporine A in acute STEMIs. Other cyclosporins may also prove to be of potential value.
Biomarkers such as IL-6 and soluble interleukin-6 receptor (sIL-6R) are elevated in acute myocardial infarction. A Mendelian randomisation analysis in The Lancet, 2012, reported that there is robust genetic evidence for the role of a specific inflammatory pathway in the development of CHD in humans. A variant in the IL-6R gene had effects on biomarkers of inflammation and related inflammatory pathways. There is strong evidence of IL-6R signalling in the development of CHD. The specific Mendelian randomisation analyses for IL-6 have not been done yet. However, more randomised trials are required to test these more novel therapeutic approaches of IL-6R blockade in preventing CAD.19
There have been a number of phase III trials of various anti-inflammatory agents to test their effectiveness in the secondary prevention of cardiovascular disease, including two trials of darapladib (an inhibitor of lipoprotein-associated phospholipase A2),20 a trial of canakinumab (a monoclonal antibody to interleukin 1β),21 and a trial of low-dose methotrexate.22
The secretory phospholipase inhibitors, e.g. varespladib (a non-specific sPLA2 inhibitor) or darapladib (a targeted LpPLA2 inhibitor) are effective agents for reducing sPLA2 and Lp-PLA2, respectively, but do not have a significant effect on the central IL-6 regulatory pathway and CRP, as evidenced by the FRANCIS (Fewer Recurrent Acute coronary events with Near-term Cardiovascular Inflammation Suppression) trial and in PLASMA (Phospholipase Levels and Serological Markers of Atherosclerosis) studies in the varespladib group. Similarly, in the Integrated Biomarker and Imaging Study (IBIS-2), it was observed that darapladib does not have effect on primary end points of CRP level or coronary atheroma deformability. However, improvement in progression of lipid necrotic core was noticed.23
In their 2013 study, Anderson et al. suggest that in ACS, the pathogenesis of unstable plaque and rupture can be explained by changes in intracellular signalling with trans-IL-6 receptor binding and by blocking of IL-6 receptors.24
Conclusion
In conclusion, multiple factors, including inflammation, are responsible for the complex pathogenesis of atherosclerosis in coronary arteries. Rapid CAD progression is associated with endothelial and macrophage/monocyte activation, release of cytokines and elevated inflammatory markers, but their effect on the extent and severity of atherosclerosis remains controversial. However, they play an important role in cardiovascular research on the development of therapeutic strategy.
The use of some anti-inflammatory compounds is associated with increased cardiovascular events and requires a cautious approach. Antibiotics may have some role in down-regulating inflammatory processes, but there is no definite evidence of prophylactic antibiotics preventing cardiac events. Statins have an additional anti-inflammatory effect through reducing CRP levels, but are not recommended in patients with normal cholesterol and high hsCRP levels because CRP does not play a causal role in cardiovascular disease. The benefits of statins are related to further lowering of cholesterol levels, rather than an anti-inflammatory effect. Systemic use of immunosuppressive medications has significant side effects; however, localised effects with sirolimus-coated stents can be used to prevent restenosis.
The HDL-based therapy is promising and likely to have an inhibitory effect on the inflammatory cascade, and, hence, reduce atherosclerosis. However, further evidence is needed because dysfunctional HDL particles in blood are harmful due to their pro-inflammatory effect. Recently, a few prospective studies have shown that levels of circulating IL-6 and sIL-6R are elevated in ACS patients and are associated with increased risk of CHD. This has been confirmed with strong genetic evidence in a Mendelian randomisation study, and IL-6R blockade could develop a new therapeutic approach in future, which would require multiple randomised trials before its implication in clinical practice.
Conflict of interest
None declared.
Key messages
Inflammation plays a significant role in the pathogenesis of atherosclerosis and coronary artery disease progression
Many currently used therapeutic agents (antibiotics, immunosuppressive agents, statins) seem to have an impact on down-regulating the inflammatory process associated with atherosclerotic coronary artery disease but with no significant beneficial impact on reducing cardiovascular events
Future studies are needed to establish the potential clinical utility of these novel compounds to treat and prevent coronary heart disease
We appear to be no nearer attenuating a potentially adverse core mechanism in the natural history of myocardial infarction. This is an important area for future translational research
References
1. Tabit CE, Holbrook M, Shenouda SM et al. Effect of sulfasalazine on inflammation and endothelial function in patients with established coronary artery disease. Vasc Med 2012;17:101–07. http://dx.doi.org/10.1177/ 1358863X12440117
2. Parchure N, Zouridakis EG, Kaski JC. Effect of azithromycin treatment on endothelial function in patients with coronary artery disease and evidence of chlamydia pneumoniae infection. Circulation 2002;105:1298–303. http://dx.doi.org/10.1161/hc1102.105649
3. Anderson JL, Muhlestein JB. The ACADEMIC study in perspective (Azithromycin in coronary artery disease: elimination of myocardial infection with Chlamydia). J Infect Dis 2000;181:S569–S571. http://dx.doi.org/10.1086/315635
4. Stone AF, Mendall MA, Kaski JC et al. Effect of treatment for Chlamydia pneumoniae and Helicobacter pylori on markers of inflammation and cardiac events in patients with acute coronary syndromes: South Thames Trial of Antibiotics in Myocardial Infarction and Unstable Angina (STAMINA). Circulation 2002;106:1219–23. http://dx.doi.org/10.1161/01.CIR.0000027820.66786.CF
5. O’Connor CM, Dunne MW, Pfeffer MA et al.; Investigators in the WIZARD Study. Azithromycin for the secondary prevention of coronary heart disease events: the WIZARD study: a randomized controlled trial. JAMA 2003;290:1459–66. http://dx.doi.org/10.1001/jama.290.11.1459
6. Grayston JT, Kronmal RA, Jackson LA et al. Azithromycin for the Secondary Prevention of Coronary Events (ACES). N Engl J Med 2005;352:1637–45. http://dx.doi.org/10.1056/NEJMoa043526
7. Cannon CP, Braunwald E, McCabe CH et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004;350:1495–504. http://dx.doi.org/10.1056/NEJMoa040583
8. Danesh J, Lewington S, Thompson SG et al. Plasma fibrinogen level and the risk of major cardiovascular diseases and nonvascular mortality: an individual participant meta-analysis. JAMA 2005;294:1799–809. http://dx.doi.org/10.1001/jama.294.14.1799
9. Keavney B, Danesh J, Parish S et al. Fibrinogen and coronary heart disease: test of causality by ‘Mendelian randomization’. Int J Epidemiol 2006;35:935–43. http://dx.doi.org/10.1093/ije/dyl114
10. Kerr DJ, Dunn JA, Langman MJ et al. Rofecoxib and cardiovascular adverse events in adjuvant treatment of colorectal cancer. N Engl J Med 2007;357:360–9. http://dx.doi.org/10.1056/NEJMoa071841
11. Biasucci LM, Biasillo G, Stefanelli A. Inflammatory markers, cholesterol and statins: pathophysiological role and clinical importance. Clin Chem Lab Med 2010;48:1685–91. http://dx.doi.org/10.1515/CCLM.2010.277
12. Ridker P, Danielson E, Fonseca FAH, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008;359:2195–207. http://dx.doi.org/10.1056/NEJMoa0807646
13. Elliott P, Chambers JC, Zhang W et al. Genetic loci associated with C-reactive protein levels and risk of coronary heart disease. JAMA 2009;302:37–48. http://dx.doi.org/10.1001/jama.2009.954
14. Wensley F, Gao P, Burgess S et al. Association between C reactive protein and coronary heart disease: Mendelian randomization analysis based on individual participant data. BMJ 2011;342:d548. http://dx.doi.org/10.1136/bmj.d548
16. Piot C, Croisille P, Staat P, et al. Effect of cyclosporine on reperfusion injury in acute myocardial infarction. N Engl J Med 2008;359:473–81. http://dx.doi.org/10.1056/NEJMoa071142
17. Mewton N, Croisille P, Gahide G, et al. Effect of cyclosporine on left ventricular remodeling after reperfused myocardial infarction. J Am Coll Cardiol 2010;55:1200–5. http://dx.doi.org/10.1016/j.jacc.2009.10.052
18. Mewton N, Cung TT, Morel O, et al. Rationale and design of the Cyclosporine to ImpRove Clinical oUtcome in ST-elevation myocardial infarction patients (the CIRCUS trial). Am Heart J 2015;169:758–66. http://dx.doi.org/10.1016/j.ahj.2015.02.020
19. The Interleukin-6 Receptor Mendelian Randomisation Analysis (IL6R MR) Consortium. The interleukin-6 receptor as a target for prevention of coronary heart disease: a Mendelian randomisation analysis. Lancet 2012;379:1214–24. http://dx.doi.org/10.1016/S0140-6736(12)60110-X
20. Lp-PLA2 Studies Collaboration. Lipoprotein-associated phospholipase A2 and risk of coronary disease, stroke, and mortality: collaborative analysis of 32 prospective studies. Lancet 2010;375:1536–44. http://dx.doi.org/10.1016/S0140-6736(10)60319-4
21. Ridker PM, Thuren T, Zalewski A, Libby P. Interleukin-1β inhibition and the prevention of recurrent cardiovascular events: rationale and design of the Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS). Am Heart J 2011;162:597–605. http://dx.doi.org/10.1016/j.ahj.2011.06.012
22. Ridker PM. Testing the inflammatory hypothesis of atherothrombosis: scientific rationale for the cardiovascular inflammation reduction trial (CIRT). J Thromb Haemost 2009;7:332–9. http://dx.doi.org/10.1111/j.1538-7836.2009.03404.x
24. Anderson DR, Poterucha JT, Mikuls TR et al. IL-6 and its receptors in coronary artery disease and acute myocardial infarction. Cytokine 2013;62:395–400. http://dx.doi.org/10.1016/j.cyto.2013.03.020
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits