While the primary aims of cardiac surgical procedures are to improve survival and ameliorate symptoms, chronic post-surgical pain (CPSP) is a prevalent problem requiring focused attention. Recent years have seen a global emphasis on the development and implementation of self-management (SM) interventions to combat the negative consequences of multiple chronic conditions, including chronic pain. This short report makes recommendations for optimising SM following cardiac surgery to improve pain and related functional outcomes and reduce the risk and impact of CPSP.
Chronic pain after cardiac surgery: prevalence and impact
With the growing burden of cardiovascular disease, the number of people undergoing cardiac surgery, globally, is expected to continue to rise.1 In 2010, 31,613 cardiac surgeries were performed in England and Wales,2 and prevalence data are similar in other Commonwealth countries, including Canada.2,3 While the primary aims of cardiac surgical procedures (including coronary artery bypass grafting [CABG] and valve replacement) are to improve survival, ameliorate symptoms (such as angina) and improve health-related quality of life (HRQL), mounting evidence suggests that the development of chronic post-surgical pain (CPSP) and related poor functional recovery following these procedures are major clinical problems for substantial numbers of patients.
Cardiac surgeries involve many pain-sensitive structures as they require a median sternotomy, retraction of the ribs, and invasion of muscles and visceral tissues.4 Such procedures may result in CPSP pain that can last for variable periods of time, the origin of which may be inflammatory in nature, or neuropathic, due to nerve injury.
The recent Canadian CARDpain (Chronic Postoperative Pain After Coronary Artery Bypass Graft Surgery) study (n=1,010)5 and WREST-E (Women’s Recovery from Sternotomy-Extension) study (n=222)6 have reported similar CPSP prevalence rates of approximately 40% at three months and 17% at 12 months following cardiac surgery. One-year prevalence rates of CPSP as high as 39% and 45% have also been reported in prospective studies of patients following CABG in Turkey7 and the Netherlands.8
CPSP is associated with the development of anxiety and depressive disorders,9 sleep disturbances and fatigue,10 as well as poor self-rated health across multiple domains of HRQL.11,12 Data from the CARDpain study demonstrated significant bodily pain and pain-related interference scores (family and home responsibilities, recreation, employment) for up to one year following surgery for over 50% of patients enrolled.5 The available evidence is clear: not only is CPSP common among cardiac surgery patients, but it also impairs HRQL, considerably.
While a few hospitals in the UK offer a range of specialised pain services (e.g. expertise in anaesthesia and pain medication, cognitive behaviour therapy, counselling, hypnotherapy) to manage this problem, such comprehensive clinical follow-up is not commonplace. Both within the UK and internationally, where district hospitals and outpatient services are not integrated with the infrastructure of specialist tertiary centres (where cardiac surgeries take place), resources to manage CPSP on an outpatient basis can be more limited.
Optimising pain selfmanagement: the way forward
Recent years have seen a global emphasis on the development and implementation of selfmanagement (SM) interventions to combat the negative consequences of multiple chronic conditions, including chronic pain. The goal of SM support is to prevent or slow symptom-related disability and restore functioning and life roles to optimal levels.12 In angina populations, SM programmes have demonstrated improvements in physical and psychological functioning, as well as HRQL.13–15
Compared with a decade ago, we know a lot more about facilitators and barriers to maximising key SM outcomes including pain, disability, and emotional well being. Capitalising on these knowledge gains could pave the way forward in terms of reducing the impact of CPSP following cardiac surgery. Perhaps the most crucial factor (central to recent healthcare reforms in the UK) is promoting more active engagement of health professionals (HPs) in the SM process. A recent systematic review of chronic pain SM programmes, in particular, found that patients identify consistently the need for ongoing, tailored advice, as well as encouragement from HPs in order to realise their SM goals.16 Surgical nurses and cardiac liaison nurses are ideally placed to be trained to facilitate health system-linked SM programmes aimed at preventing CPSP, grounded in their knowledge of the surgical procedures, as well as factors known to play a role in the transition from acute to chronic pain (if not wellmanaged) including acute post-operative pain management, rehabilitation, and emotional well-being.17
Facilitating SM linkages between the home and tertiary care setting is becoming more economically feasible as electronic media become more commonplace in the home. There are services already in place that deliver cardiac rehabilitation via web-link (e.g. https://www.activateyourheart.org.uk/) and which have demonstrated that patients welcome such readily accessible support.18 With representation across the UK and Canada, our team is now endeavouring to design a replicable, health system-linked model that integrates post-operative SM in the home with tertiary care services. Our aim is to achieve the optimal SM design for, not only improving pain and related functional outcomes following cardiac surgery, but also for reducing the risk and impact of CPSP.
Key messages
Chronic post-surgical pain (CPSP) following cardiac surgery is a prevalent problem requiring focused attention
While a few hospitals in the UK offer a range of specialised pain services to manage this problem, such comprehensive clinical services are not commonplace internationally
There is a requirement for the development and testing of innovations to optimise patient self-management interventions that use health system-linked models, to target factors known to play a role in the transition from acute pain to CPSP following cardiac surgery
Acknowledgements
The authors wish to thank Dr Austin Leach, Consultant in Pain Medicine, National Refractory Angina Centre, Liverpool, for his valuable clinical insights in preparing this manuscript.
MHM holds the Heart and Stroke Foundation/Michael G DeGroote Endowed Chair of Cardiovascular Nursing Research, McMaster University. SC holds a Research Early Career Award from Hamilton Health Sciences Foundation.
5. Choinière M, Watt-Watson J, Victor JC et al. Prevalence of and risk factors for persistent postoperative nonanginal pain after cardiac surgery: a 2-year prospective multicentre study. CMAJ 2014;186:E213–E223. http://dx.doi. org/10.1503/cmaj.131012
6. Routledge FS, Tsuyuki RT, Hervas- Malo M, LeBlanc P, McFetridge- Durdle JA, King KM. The influence of coronary artery bypass graft harvest site on women’s pain, functional status, and health services utilization throughout the first post-operative years: a longitudinal study. Int J Nurs Stud 2009;46:1054–60. http://dx.doi.org/10.1016/j. ijnurstu.2009.02.003
7. Onan B, Onan IS, Kilickan L, Sansioglu I. Effects of epidural anesthesia on acute and chronic pain after coronary artery bypass grafting. J Card Surg 2013;28:248–53. http:// dx.doi.org/10.1111/jocs.12086
8. van Leersum JN, van Leersum RL, Verwey HF, Klautz RJM. Pain symptoms accompanying chronic poststernectomy pain: a pilot study. Pain Med 2010;11:1628–34. http://dx.doi.org/10.1111/j.1526- 4637.2010.00975.x
9. McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disorders associated with chronic pain: an examination in a nationally representative sample. Pain 2003;106:127–33. http://dx.doi. org/10.1016/S0304-3959(03)00301-4
10. Wilson KG, Mikail SF, D’Eon JL, Minns JE. Alternative diagnostic criteria for major depressive disorder in patients with chronic pain. Pain 2001;91:227–34. http://dx.doi.org/10.1016/S0304- 3959(00)00440-1
12. McGillion M, O’Keefe-McCarthy S, Carroll S et al. Impact of selfmanagement interventions on stable angina symptoms and health-related quality of life. BMC Cardiovasc Disord 2014;14:14. http://dx.doi. org/10.1186/1471-2261-14-14
13. Lewin RJP, Furze G, Robinson J et al. A randomised controlled trial of a self-management plan for patients with newly diagnosed angina. Br J Gen Pract 2002;52:194–201. Available from: http://bjgp.org/ content/52/476/194
14. McGillion MH, Watt-Watson J, Stevens B, LeFort SM, Coyte P, Graham A. Randomized controlled trial of a psychoeducation program for the self-management of chronic cardiac pain. J Pain Sympt Manage 2008;36:126–40. http://dx.doi.org/10.1016/j. jpainsymman.2007.09.015
16. Mann EG, LeFort S, Van Den Kerkhof EG. Self-management interventions for chronic pain. Pain Manage 2013;3:211–22. http://dx.doi. org/10.2217/pmt.13.9
17. Katz J, Seltzer Z. Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurother 2009;9:723–44. http://dx.doi.org/10.1586/ern.09.20
18. Devi R, Carpenter C, Powell J, Singh S. Exploring the experience of using a web-based cardiac rehabilitation programme in a primary care angina population: a qualitative study. Int J Ther Rehab 2014;21:434–40. http://dx.doi. org/10.12968/ijtr.2014.21.9.434
This paper describes the experiences of developing a non-medical, non-catheter laboratory (cath lab) based implantable loop recorder (ILR) service. ILRs are small subcutaneous single-lead electrocardiogram (ECG) monitoring devices that are placed in a left pectoral pocket under local analgesia. Traditionally, devices have been implanted by medical staff in the cath lab. Each implant can take between 30 and 45 minutes depending on operator skill and patient anatomy. The development of this service has had several major patient and organisational benefits that include shorter waiting times, less cancellations and increased flexibility to implant ‘urgent’ devices in transient loss of consciousness (TLOC). The latter has reduced length of stay within our emergency assessment unit (EAU). Moreover, this service means that the department has been able to undertake more procedures in the cath lab. Data from 2013–14 suggest that an additional 32 × four-hour cath lab sessions were made available for alternative use. Adverse events (infection/erosion) are comparable with published data at less than 1%. To conclude, non-medical, non-cath lab based implantation is safe, cost-effective and has the potential to improve patient experience while increasing both cardiologist and cath lab capacity.
Introduction
Reveal LINQ™ insertable cardiac monitoring system (Medtronic)
This paper describes the development of a non-medical, non-catheter laboratory (cath lab) based implantable loop recorder (ILR) implantation service. The experiences of the team and results from prospective audit. When the service was first envisioned, the Lincolnshire Heart Centre had only one cath lab and was in the process of developing a primary percutaneous angioplasty (PPCI) service for ST-elevation myocardial infarction. As part of the business planning process we scrutinised what services were currently being undertaken where and by whom. We felt that with increasing inpatient demands and the need to generate cath lab capacity, that ILR implants should be moved from a consultant cardiologist led service within the cath lab to an alternative clinical environment. A treatment room on our medical day care unit (MDU) was identified and approved by the Trust’s infection prevention team. Initially, the service was undertaken by cardiology registrars who had received training from one of the consultant cardiologists. However, conflicting demands of day/night rotation, service delivery on the wards and clinical training meant that many sessions were cancelled. This led to long waiting times, patient complaints and poor patient satisfaction. As a result an alternative non-medical implantation service was developed.
Table 1. European Society of Cardiology (ESC) guidelines on the management of syncope 2009
An ILR is a single-lead electrocardiogram (ECG) monitoring device that has until recently been implanted into a left pectoral pocket under local analgesia. Traditional devices take between 30 and 45 minutes to implant depending on operator skill and patient anatomy. More recently, an injectable device has become available that requires less surgical training than the previous devices. ILRs have advantages when compared with external rhythm monitoring devices as they can record over a longer period of time, have higher patient acceptability (not getting tangled in monitoring wires or having to replace electrodes) and record in total loss of consciousness where a ‘clutch’ type of monitor will not. Table 1 illustrates indications and evidence class for ILR in syncope.1
More recently, there is increasing evidence that a substantial proportion of cryptogenic strokes may be as a result of undiagnosed atrial fibrillation (AF) and the ILR may have an important role to play in ruling out AF as a cause of a patient’s events.2
In the UK, the National Institute for Health and Care Excellence (NICE) state “in patients that have total loss of consciousness with a probable cardiac cause, but have symptoms infrequently (less than once every two weeks) then an implantable loop recorder is the first line of investigation”.3
ILRs are more expensive than non-invasive monitoring and costs vary between £1,200 and £2,000 per device depending on the complexity of the device and institutional volume. Cost efficacy of ILRs in syncope has been scrutinised in several publications. The Centre for Research and Dissemination at the University of York undertook a probabilistic health economic assessment of ILRs (including implant, monitoring and explant costs) in the investigation of syncope compared with alternative methods of investigation and concluded that they were cost-effective.4
Methods
The Consultant Nurse in Cardiology (CN) who was already trained in consent, surgical skills and a non-medical prescriber was asked to develop a non-medical implant service, as it was envisioned this would result in a very short ‘start-up curve’ in getting the new service up and running. A period of supervised implantation under the guidance of a pacing consultant cardiologist was undertaken and competence was assessed using direct observation of procedural skills (DOPS). In order to deliver the highest quality clinical service with high patient flow during implant sessions, the CN was trained in ‘device mapping’, but routinely a clinical physiologist ‘mapped’ (identifying the optimum position for the device) and completed patient registration while CN implanted.
Within two months of the commencement of the new service, waiting lists had been cleared and patient-satisfaction audit scored high. As the team gained knowledge and skills the number of implants undertaken in a four-hour clinical session was increased from three to five (occasionally six). An unforeseen consequence of the new service was that demand increased by a factor of two, as referring clinicians realised the patients’ journey had improved.
The success of the service meant that a second operator was required to ensure continuity during annual leave and unplanned absence. One of the cardiology acute care practitioners (ACP) was identified and trained under the supervision of the nurse consultant. Two patients experienced anaphylaxis requiring treatment secondary to prophylactic pre-procedure antibiotics (teicoplanin used in penicillin allergic patients). Thus, a literature review was undertaken and no evidence was found that prophylactic antibiotic administration reduced pocket infection in ILR implantation, and, indeed, there was little evidence for their use in pacemaker implantation. Following discussion with microbiology, we stopped giving routine prophylactic antibiotics, and a prospective audit of n=100 patients was undertaken. No increase in pocket infection was noted. Routine cannulation was also discontinued. We also reviewed if devices can be implanted on warfarin provided the international normalised ratio (INR) <3 seconds to reduce patients thromboembolic risk in AF or those with prosthetic heart valves. Contemporary evidence suggested that pacemaker implantation could be undertaken on anticoagulated patients but no evidence was found for ILRs.5 As pacemaker implantation is more traumatic than ILR implantation, the pathway was revised to implant during continued anticoagulation. Diathermy is always available when implanting patients on warfarin/novel anticoagulation, but has never been required. No increase in bleeding/haematoma has been observed.
Physiology-led implantation
Historically, one of the Trust’s smaller hospitals had sent their patients to a neighbouring Trust for ILR implantation, as no local service was available. This meant a loss of revenue to the Trust, but more importantly long journey times for patients often undertaken on ‘public transport’. Many of our older patients found the journey arduous, particularly those on diuretic therapy or with impaired mobility. Hence, it was decided to develop a local service. A senior clinical physiologist (CP) expressed interest in developing this service and began training under the supervision of the CN. There were several challenges that needed to be overcome, namely that while a highly skilled physiologist, they had little training in surgical skills, consent or pharmacology when compared with a nurse practitioner. Legally, should a nurse or a clinical physiologist have a serious adverse event then they would be judged against the profession who had historically undertaken that role. Thus, to ensure consistent quality the clinical physiologist undertook the training in:
Mental Capacity Act/consent
European Resuscitation Council Advanced Life Support (ALS)
It was necessary to amend the Trust’s medicines management policy to permit a clinical physiologist to administer medication, namely local anaesthetic. As clinical physiologists, who are a voluntary registered healthcare professional, are not legally permitted to administer medications under patient group directions (PGDs). However, they may administer against a named patient prescription order. Thus, options to facilitate clinical physiology administration are that the request form can be adapted to become a prescription, or the physiologist can approach an independent prescriber prior to the procedure and have a prescription order completed. Once trained, we amended the clinical physiologist job description to include ‘implantation/removal of loop recorders’ to ensure compliance with NHSLA (National Health Service Litigation Authority) requirements.
Injectable ILRs
Recently, an injectable ILR has become available. This device has several patient and organisational advantages, but also one major disadvantage that must be weighed against any advantages. Namely, it is more expensive than traditional devices. The new device is significantly smaller than the traditional devices and, thus, reduces implantation trauma and scarring (visible scarring on the chest is a very real consideration in younger female patients who are concerned about their body image, and we ensure that all patients are aware of the risk during the consent process). The device is injected into a left para-sternal pocket under local analgesic so requires less surgical training. It does not require surgical draping and is suited to clinic room implantation. Initially, when we started implanting this device we closed the wound with ‘steri-strips’ but later swapped to flexible surgical glue as it is less susceptible to movement. We also adopted a downward implantation technique rather than an upward technique, as this lessened device migration. Increased device cost is offset, as more devices can be implanted in a clinical session, thus, reducing staffing costs and administration costs. There is also a cost saving, as less equipment (draped/surgical packs) is needed to support implantation. The limiting factor on how many devices can be implanted in a session is now the time needed for patient education and physiology programing. We are able to implant eight devices in four hours. Ease of implantation has had an added patient and organisational bonus. Namely, we have been able to implant in ‘clinic rooms’ in the emergency department and emergency assessment unit. Thus, we have either avoided TLOC admissions or significantly reduced patient’s length of stay.
Results
Audit from 2012–14 (n=300) conducted on a number needed to treat (NNT) basis demonstrates an incidence of erosion/infection of <2%. If patients who have manipulated their device are removed then incidence of erosion/infection is <1%. Two patients suffered from a mild anaphylaxis reaction secondary to prophylactic antimicrobial therapy that is no longer routinely administered. No patients have had a major bleed/haematoma or major adverse event (on or off anticoagulation).
Based on the 2013–14 financial year (n=161) data, 32 × four-hour consultant cardiologist and cath lab sessions have been generated for other purposes. Potentially generating an additional 64 angioplasty/pacing spells with revenue in the region of £250k. It is more difficult to quantify the impact of 34 additional ‘patient activity’ consultant sessions. Length of stay for patients admitted with TLOC has been reduced and PROMS (patient recorded outcome measures) feedback has been excellent. Conversion from ILR to pacemaker was 12% in the first year but this is likely to increase year on year. Current devices have a battery life of three years. We are continuing to collect data in cryptogenic stroke.
Conclusion
We believe that we have demonstrated that non-medical, non-cath lab ILR implantation is both safe and effective. We have seen significant improvements in both the elective and emergent patient pathways and have reduced organisation expenditure while generating additional consultant and cath lab capacity.
Acknowledgment
The authors wish to thank Sheila Bampton, Cardiac Physiologist, who has supported their service over the last four years.
Conflict of interest
AR has undertaken a teaching session on non-medical ILR implantation for Medtronic. CM, JD, ARH, RA: none declared.
Key messages
Implantation of implantable loop recorders (ILRs) outside of the catheter laboratory is safe and clinically as well as cost effective. It may improve the patient journey
Nurses and senior physiologist can implant safely and efficiently
New injectable ILRs reduce surgical trauma and scarring, and have high patient satisfaction levels.
References
1. Moya A, Sutton R, Ammirati F et al. Guidelines for the diagnosis and management of syncope (version 2009): The Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J 2009;30:2631–71. http://dx.doi.org/10.1093/eurheartj/ehp298
2. Sanna T, Diener H-C, Passman RS et al. Cryptogenic stroke and underlying atrial fibrillation. N Engl J Med 2014;370:2478–86. http://dx.doi.org/10.1056/NEJMoa1313600
3. National Institute for Health and Care Excellence.Transient loss of consciousness (‘blackouts’) management in adults and young people. CG109. London: NICE, 2010. Available from: http://www.nice.org.uk/guidance/cg109
4. Davis S, Westby M, Pitcher D, Petkar S. Implantable loop recorders are cost-effective when used to investigate transient loss of consciousness which is either suspected to be arrhythmic or remains unexplained. EP Europace 2012;14:402–09. http://dx.doi.org/10.1093/europace/eur343
5.ClinicalTrials.gov. Randomized study of the use of warfarin during pacemaker or ICD implantation in patients requiring long term anticoagulation. Identifier:NCT00721136. Available from: http://www.clinicaltrials.gov/ct2/show/NCT00721136
Contrast-induced nephropathy is the third most common cause of in-hospital acute kidney injury and accounts for 10% of total cases. It is commonly encountered following coronary angiography and this systematic review aims to use current evidence to ascertain which treatment modalities are most effective in the prevention of the disease.
A PubMed literature search was conducted in March 2014 using search terms, ‘contrast nephropathy and coronary angiography’. The data analysed included 15 trials and two meta-analyses in order to determine whether patients given N-acetylcysteine (NAC), sodium chloride or sodium bicarbonate had better clinical outcomes. Study data were reviewed and quality of data discussed.
Current data indicate that sodium bicarbonate is as effective as sodium chloride when used in patients with estimated glomerular filtration rate (eGFR) <60 ml/min. NAC adds no statistically significant benefit in mild-to-moderate renal disease regardless of whether it is used in isolation or as an adjunct therapy with fluid.
Pathogenesis
With the advent of the iodinated contrast study came the complication of contrast-induced nephropathy (CIN), an increasingly recognised and discussed iatrogenic disease process seen with coronary angiography. As we become more invasive in our cardiac investigations, and coronary interventions become more widespread, coronary angiography is offered to more and more patients. Therefore, a better understanding of the treatment modalities aimed at minimising the risk of CIN has never been more important.
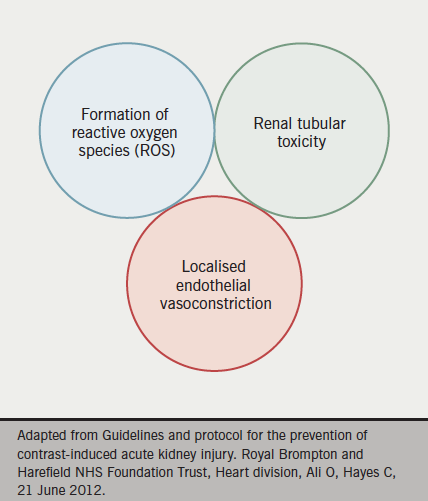
Figure 1. Aetiology of contrast-induced nephropathy
CIN is a direct hyper-acute tubular insult on the filtering mechanisms of the kidney. Although still poorly understood, it is postulated that free radical accumulation and subsequent damage to epithelial layers, as well as compromised renal perfusion, are important (see figure 1). CIN is now the third most common cause of in-hospital acute kidney injury and is responsible for approximately 10% of all cases of iatrogenic renal disease.1 In the short term, it is associated with a transient rise in serum creatinine levels, however, this can progress in a proportion of cases to severe acute kidney injury, metabolic acidosis, hyperkalaemia or anuria requiring haemofiltration or haemodialysis.
Joint guidance set out in April 2013 by the British Cardiovascular Intervention Society, Royal College of Radiologists and Renal Association redefined the biochemical criteria of CIN as a rise of serum creatinine levels post-intravenous contrast of more than 1.5 times baseline within seven days, an absolute increase of more than 26 µmol/L within two days, or a urine output of less than 0.5 ml/kg/hr for more than six hours post-procedure.2 Prior to this guidance, the generally accepted definition of CIN was a rise of serum creatinine above baseline of more than 25%, or an absolute increase of at least 44 µmol/L. The data provided in this article uses this definition unless otherwise stipulated, since there have been limited data collected since the re-classification of CIN.
Clinical significance
In 2012, Gallagher et al. explored the long-term outcomes of patients who underwent primary percutaneous coronary intervention (PPCI) for ST-segment elevation myocardial infarction (STEMI) and, retrospectively over seven years, it was observed that within a standardised cohort of 2,224 patients, CIN was associated with both increased short- and long-term mortality.3 As well as recognising that older patients are at increased risk of CIN (mean age of 69.3 vs. 63.7 years, p<0.0001), it was observed that females, as opposed to males, incur poorer outcomes (30.0% vs. 22.6%, respectively, p=0.004). Furthermore, Gallagher et al. found that those with baseline renal disease, i.e. an estimated glomerular filtration rate (eGFR) of less than 60 ml/min, experienced a statistically significant increased risk of CIN post-contrast (33.1% vs. 18.6%, respectively, p<0.0001). Taken together with other comorbidities, such as diabetes mellitus, hypertension, cholesterol status and reduced left ventricular ejection fraction, it was realised that CIN can be a predictor of significant all-cause mortality within 30 days (16.4% vs. 2.0%, p<0.0001) and at three years (22.4% vs. 5%, p<0.0001).
An earlier retrospective study of 3,236 patients, by From et al.,4 supports the results of Gallagher et al.’s work.3 They reported a statistically significant increase in all-cause mortality in an 809 patient cohort who developed CIN at 30 days with an odds ratio of 3.37 (95% confidence interval [CI] 2.58–4.41, p<0.001) as opposed to the 2,427 patients who did not develop CIN.4
Rudnick and Feldman conducted their own review of five observational studies and also concluded that acute kidney injury associated with the administration of contrast is, at the very least, a marker of increased mortality and prolonged hospital stay. They also concluded that peri-procedural events associated with CIN were compounded by other comorbidities mentioned previously, such as pre-existing coronary artery disease and diabetes mellitus. Furthermore, it was found that cumulative mortality can be extended to as much as one year post-contrast, as death rates among those with CIN was 22.6% with pre-existing chronic renal dysfunction when compared with 6.9% without (p<0.0001).5
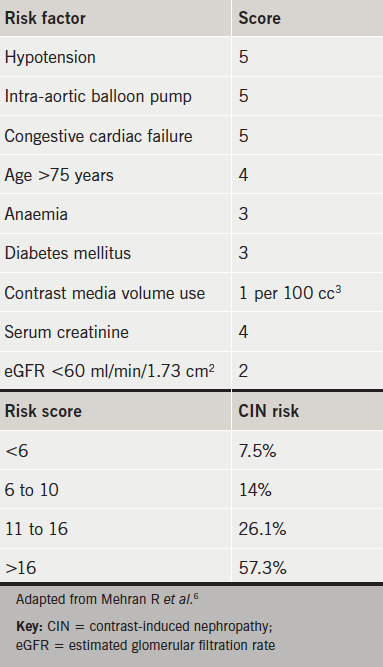
Table 1. The Mehran risk score and associated risk of progression to CIN
The overwhelming conclusion from these studies is of an increase in both short- and long-term mortality as a consequence of CIN, as well as increased length of hospitalisation. Although the data are largely retrospective, the observational studies do suggest a tangible association between CIN and mortality, which highlights the importance of early recognition and effective treatment of CIN in those undergoing coronary angiography ± percutaneous coronary intervention (PCI).
The Mehran scoring system was adopted specifically for CIN risk stratification in patients undergoing PCI and has been validated in an 8,357 strong patient cohort, which included ‘high-risk’ patients.6 Although not universally accredited by specialist colleges, it has been validated in groups undergoing both elective and emergency procedures for STEMI and non-STEMI.7,8 Early recognition of those who may require renal replacement therapy should be sought using this tool, and less invasive functional studies should be considered if at high risk (see table 1). However, when coronary angiography and/or PCI is the most appropriate intervention, the CIN prevention strategies discussed below should be explored.
Treatment strategies to reduce the risk of CIN
N-acetylcysteine
The most widely utilised prophylaxis and treatment strategies for CIN in coronary interventions are intravenous fluids and oral N-acetylcysteine (NAC). Although the precise pharmacokinetics of NAC remain somewhat of a mystery, it may play a role in the consumption of reactive oxygen species and the liberation of both nitric oxide and N-nitrosothiol, which in turn are known to cause endothelial vasodilation.9
Early studies by Tepel et al. investigated the use of 600 mg twice-daily oral NAC as prophylaxis against CIN in computed tomography (CT) scans. This study found that the mean serum creatinine improved from 2.5 mg/dL to 2.1 mg/dL (±1.3 mg/dL, p<0.001) when compared with control, and, given these promising results, the practice was extrapolated to cardiac catheterisation.10 However, an extensive meta-analysis in 2006 by the same author, citing 26 prospective randomised trials, 25 being specific for CIN in coronary angiography, failed to show any significant relative risk reduction with NAC versus placebo.11 Another study by Briguori’s team reported a relative risk of 0.3 (p=0.02) with NAC at 1200 mg twice daily, while others reported little if any improvement in serum creatinine levels with lower dosage regimens.12
Kshirsagar et al. also conducted a meta-analysis of 16 prospective trials including 1,538 patients.13 In contrast to the work conducted by Tepel, CIN was assessed in patients undergoing a broad range of contrast studies, not limited to coronary angiography. The result was heterogeneic data, and clinically significant conclusions regarding the effect of NAC could not be drawn. Despite some patient groups receiving high-dose NAC and others low dose, Kshirsagar found no statistical difference in CIN incidence. However, it was recognised that elderly patients and those with diabetes mellitus are at increased risk of contrast-induced kidney injury.
Discrepancies in the data analysing the effect of NAC have been attributed to variances in the bioavailability of glutathione (the active metabolite of NAC), differences in therapeutic dosages, variances of contrast media concentration and differences in dose timing between the various studies. A common theme throughout the studies is the heterogeneity of the data and, despite the fact that later research failed to replicate the positive effect of NAC observed in early studies with 600 mg twice-daily dosing, it continues to be used in many hospital trusts despite a lack of evidence base.
Sodium bicarbonate versus sodium chloride
Volume expansion using either sodium chloride or sodium bicarbonate facilitates the renal clearance of contrast media, with bicarbonate having the additional benefit of urinary alkalisation, thereby lowering free radical burden on the renal tubules. Merten et al. conducted a prospective randomised trial of 119 standardised cases with stable renal disease and a serum creatinine of at least 97.2 µmol/L.14 Subjects were given intravenous fluids in the form of either sodium chloride or sodium bicarbonate from one hour prior to the contrast study at 3 ml/kg/hr until six hours post-procedure at a rate of 1 ml/kg/hr. It was found that in those subjects who underwent cardiac catheterisation, the group who received sodium bicarbonate had a CIN incidence of 2.0%, whereas those administered sodium chloride had a greater incidence of CIN at 16.7%. The calculated mean difference in relative risk between the two arms was significant at 14.7% (95% CI 3.4–25.9%, p=0.02) with an improvement in eGFR in the sodium bicarbonate group of 8.6% (95% CI 0.2–17.2%, p=0.02) in comparison to those who were administered sodium chloride. This resulted in an absolute CIN risk reduction of 11.9% with the use of sodium bicarbonate.
Given the growing evidence base for the use of sodium bicarbonate as prophylaxis, Tamai et al. attempted to assess whether there is a dose-dependent effect on the incidence of CIN with different concentrations of the fluid.15 There were 123 patients randomised into a group given 833 mEq/L sodium bicarbonate and a further group given only 160 mEq/L. After two days, the incidence of CIN was significantly lower in those who were infused with the higher dose (0% vs. 17.3%, p=0.005) and subsequent percentage changes in serum creatinine levels were again markedly lower in the higher dose group (–2.65 ± 9.83% vs. 9.14 ± 14%, p=0.001).
Despite Merten and Tamai observing statistically significant results with sodium bicarbonate, it has become common practice to adjunct intravenous fluid simultaneously with 600 mg NAC prior to coronary angiography in those at risk of CIN. Prospective randomised studies by Brar et al. and Maioli et al., with a total patient cohort of 855, produced similar results when assessing CIN incidence in patients given either sodium bicarbonate or sodium chloride in conjunction with 600 mg NAC twice daily.16,17 Of these, Brar et al. enrolled 352 standardised subjects, all of whom had an eGFR of less than 60 ml/min. CIN occurred in 13.3% of patients receiving sodium bicarbonate and 14.6% of patients receiving sodium chloride with a relative risk of 0.94 (95% CI 0.55–1.60, p=0.82). It was observed that the relative risks of all-cause mortality, dialysis and cardiovascular events were similar between sodium chloride and sodium bicarbonate at 30 days and six months. Of those who developed significant nephropathy, six-month mortality was 9.5% in the sodium chloride group and 10.0% in the sodium bicarbonate group (p >0.99).
Maioli et al. prospectively randomised 502 patients, all of whom had an eGFR <60 ml/min prior to contrast study. They were randomised to receive NAC at 600 mg twice daily and either sodium chloride or sodium bicarbonate. The data suggest that both groups experienced a non-statistically different rise in baseline creatinine of 0.14 mg/dL (± 0.3) in the sodium chloride arm, and 0.15 mg/dL (± 0.4) in the sodium bicarbonate arm (p=0.78). Over the 502 patient case series, all-cause mortality was not significantly different between the two groups with an incidence of 1.2% with sodium chloride and 1.6% with sodium bicarbonate (p=0.99). However, only 15% of patients enlisted in Maioli’s study had chronic kidney disease (CKD) stage III or worse.
Thus, to investigate the rationale of high-dose NAC at 1,200 mg twice daily with intravenous fluid in more severe forms of renal disease, Briguori et al. enlisted 326 patients with an eGFR <40 ml/min in the Renal Insufficiency Following Contrast Media Administration(REMEDIAL) trial.18 Patients were randomised to 1,200 mg twice-daily NAC and either intravenous sodium chloride or sodium bicarbonate. Briguori’s team found a significant CIN incidence of 9.9% in those who received sodium chloride and NAC, but only 1.9% of patients developed CIN when administered NAC and sodium bicarbonate (p=0.019). It was concluded, therefore, that combined treatment of high-dose NAC with sodium bicarbonate can predict better outcomes in a very high-risk subset of patients with a statistically significant lower incidence of CIN.
The REMEDIAL data were replicated in the RENO study by Recio-Mayoral et al., who identified a possible benefit with sodium bicarbonate and even higher-dose NAC than used in previous studies in the prevention of CIN in those patients undergoing emergency PPCI.19 Unlike previous studies, patients were not excluded on the basis of eGFR alone, unless they were already on regular dialysis with end-stage renal failure. Sodium bicarbonate was administered, in line with the standard in Merten’s work, at 154 mEq/L for one hour pre-procedure, with the addition of 2,400 mg NAC intravenous loaded over one hour. Intravenous sodium bicarbonate was then given at a rate of 1.5 ml/kg/hr for six hours after the procedure, and a further two doses of 600 mg NAC were given orally the following day. Another group of patients received sodium chloride at 1 ml/kg/hr for 12 hours only after the procedure, and two 600 mg doses of NAC the next day. It was found that CIN developed in 1.8% of those who received the sodium bicarbonate protocol and in 21.8% of those given the sodium chloride protocol. Although, obviously, these were not randomised direct comparisons, they did find a statistically significant difference in CIN incidence of 20% (95% CI 8–31%, p=0.0009) by day 3 post-procedure. The REMEDIAL and RENO trials both highlight the potential dose-response variability of dual therapy (NAC and sodium bicarbonate). The data we have to date suggest that when high loading doses of NAC are paired with intravenous sodium bicarbonate, lower CIN rates are obtained in those patients with severe renal dysfunction. However, a more recent trial (ACT) found that NAC does not reduce the risk of CIN in high-risk patients undergoing coronary and peripheral angiography. In view of the conflicting data regarding the use of NAC, and lack of discernible and clinically relevant outcomes, the routine use of NAC should be reviewed and questioned.20
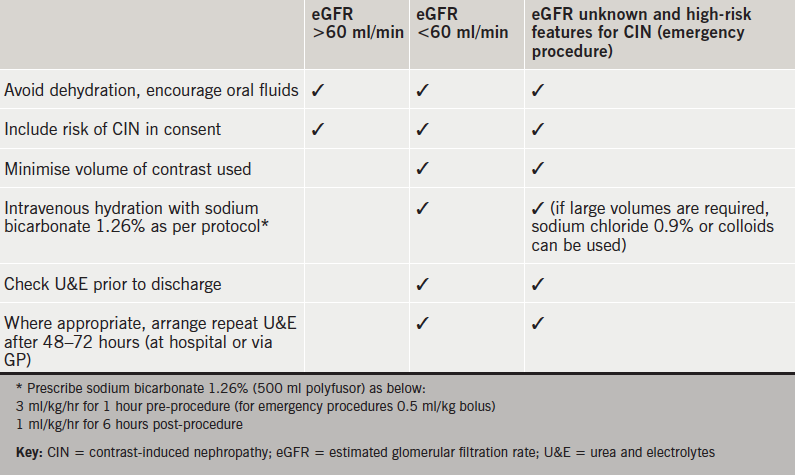
Based on current data and our local experience, we propose practical guidance to the prevention of CIN during coronary intervention (see table 2).
Table 2. General guidance for prevention of CIN
Conclusion
The current data suggest that the use of sodium bicarbonate is safe and as effective as sodium chloride in both low- and high-dose preparations, especially in high-risk patients with eGFR <60 ml/min. Furthermore, NAC, used both as monotherapy or in addition to sodium bicarbonate, has no clear benefit in those with mild stable renal disease.
Conflict of interest
None declared.
Key messages
Contrast-induced nephropathy (CIN) is an increase in creatinine of more than 26 µmol/L within two days, 1.5 times baseline within seven days, or a urine output of less than 0.5 ml/kg/hr for more than six hours post-procedure
CIN increases 30-day mortality by 14.4% and three-year mortality by 17.4%
N-acetylcysteine (NAC) has conflicting data in the prevention of CIN post-coronary angiography
Sodium bicarbonate can significantly reduce the incidence of CIN, especially in patients with moderate-to-severe renal failure
2. Lewington A, MacTier R, Hoefield R, Sutton A, Smith D, Downes M. Prevention of contrast induced acute kidney injury (CI-AKI) in adult patients. London: The Renal Association, The Royal College of Radiologists and The British Cardiovascular Intervention Society, 2013. Available from: https://www.rcr.ac.uk/publications.aspx?PageID=310&PublicationID=391
3. Gallagher S, Hassan S, Jones DA et al. Impact of contrast-induced nephropathy upon short and long-term outcomes of patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Heart 2012;98;A70. http://dx.doi.org/10.1136/heartjnl-2012-301877b.124
4. From A, Bartholmai B, Williams A et al. Mortality associated with nephropathy after radiographic contrast exposure. Mayo Clin Proc 2008;83:1095–100. http://dx.doi.org/10.4065/83.10.1095
5. Rudnick M, Feldman H. Contrast-induced nephropathy: what are the true clinical consequences? Clin J Am Soc Nephrol 2008;3:263–72. http://dx.doi.org/10.2215/CJN.03690907
6. Mehran R, Aymong, E, Nikolsky E et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention. J Am Coll Cardiol 2004;44:1393–9. http://dx.doi.org/10.1016/j.jacc.2004.06.068
7. Sgura F, Bertelli L, Monopoli D et al. Mehran contrast-induced nephropathy risk score predicts short and long term clinical outcomes in patients with ST-elevation myocardial infarction. CircCardiovasc Interv 2010;3:491–8. http://dx.doi.org/10.1161/CIRCINTERVENTIONS.110.955310
8. Raingruber B, Kirkland-Walsh H, Chahon N, Kellerman M. Using the Mehran risk scoring tool to predict risk for contrast medium-induced nephropathy undergoing percutaneous angiography. Crit Care Nurse 2011;31:e17–e22. http://dx.doi.org/10.4037/ccn2011746
10. Tepel M, van der Giet M, Scwarzfeld C, Laufer U, Liermann D, Zidek W. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med 2000;343:180–4. http://dx.doi.org/10.1056/NEJM200007203430304
12. Briguori C, Colombo A, Airoldi F et al. N-acetylcysteine versus fenoldopam mesylate to prevent contrast agent-associated nephrotoxicity. J Am Coll Cardiol 2004;44:762–5. http://dx.doi.org/10.1016/j.jacc.2004.04.052
13. Kshirsagar AV, Poole C, Mottl A et al. N-acetylcysteine for the prevention of radiocontrast induced nephropathy: a meta-analysis of prospective controlled trials. J Am Soc Nephrol 2004;15:761–9. http://dx.doi.org/10.1097/01.ASN.0000116241.47678.49
14. Merten GJ, Burgess W, Gray LV et al. Prevention of contrast-induced nephropathy with sodium bicarbonate: a randomized controlled trial. JAMA 2004;291:2328–34. http://dx.doi.org/10.1001/jama.291.19.2328
16. Brar SS, Yuh-Jer Shen A, Jorgensen MB et al. Sodium bicarbonate vs sodium chloride for the prevention of contrast medium-induced nephropathy in patients undergoing coronary angiography. JAMA 2008;300:1038–46. http://dx.doi.org/10.1001/jama.300.9.1038
17. Maioli M, Toso A, Leoncini M et al. Sodium bicarbonate versus saline for the prevention of contrast-induced nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. J Am Coll Cardiol 2008;52:599–604. http://dx.doi.org/10.1016/j.jacc.2008.05.026
18. Briguori C, Airoldi F, D’Andrea D et al. Renal insufficiency following contrast media administration trial (REMEDIAL): a randomized comparison of 3 preventive strategies. Circulation 2007;115:1211–17. http://dx.doi.org/10.1161/CIRCULATIONAHA.106.687152
19. Recio-Mayoral A, Chaparro M, Prado B et al. The reno-protective effect of hydration with sodium bicarbonate plus N-acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the RENO study. J Am Coll Cardiol 2007;49:1283–8. http://dx.doi.org/10.1016/j.jacc.2006.11.034
20. The ACT Trial Investigators. Rationale, design, and baseline characteristics of the acetylcystein for contrast-induced nephropathy (ACT) trial: a pragmatic randomized controlled trial to evaluate the efficacy of acetylcysteine for the prevention of contrast-induced nephropathy. Trials 2009;10:38. http://dx.doi.org/10.1186/1745-6215-10-38
Authors: Moira Allison, Robert T Gerber, Steve S Furniss, Conn Sugihara, A Neil Sulke
Moira Allison
Arrhythmia Specialist Nurse
Robert T Gerber
Consultant Cardiologist
Steve S Furniss
Consultant Cardiologist
Conn Sugihara
Cardiology Registrar
A Neil Sulke
Consultant Cardiologist
East Sussex Healthcare Trust, Eastbourne District General Hospital, Kings Drive, Eastbourne, BN21 2UD
Correspondence to:
Miss M Allison
Research Nurse SUPPORT-HF 2 Study, The George Institute for Global Health, Oxford Martin School, University of Oxford, 34 Broad Street, Oxford, OX1 3DB
(moira.allison@georgeinstitute.ox.ac.uk)
First published online February 4th, 2015
The European Medicines Agency (EMA) has mandated that patients treated with dronedarone have regular monitoring. An arrhythmia specialist nurse (ASN) took over the care of patients on dronedarone in 2012.
Patients on dronedarone were identified from hospital notes and pharmacy records. Adherence to EMA guidelines on monitoring before and after the appointment of an ASN were compared. In 112 patients on dronedarone in the year prior to the appointment of an ASN, only 478 of the 1,275 (37%) required tests were actually done. With the ASN, 382 of 422 (92%) tests in 53 patients were performed. This was significantly better (p<0.001). Dronedarone was more likely to be stopped due to contraindications (p<0.017) prior to the appointment of ASN, but afterwards was more likely to be stopped due to side effects (p<0.001).
The ASN significantly improved adherence to EMA-mandated monitoring in patients on dronedarone. Involvement of an ASN had no overall impact on the likelihood of dronedarone being stopped. Patients were more likely to have the drug stopped due to side effects, and were less likely to stop for safety reasons. ASN care is superior to conventional follow-up, and is the gold standard for patients treated with dronedarone.
Introduction
Atrial fibrillation is the most common arrhythmia, affecting 1–2% of the population.1 It is associated with an increased risk of stroke and death, heart failure, reduction in quality of life, mental health problems and cognitive impairment.2 Hospitalisation is common and costly.3
Dronedarone was first approved by the National Institute for Health and Care Excellence (NICE) in April 20104 for atrial fibrillation rhythm control, but following two fatal cases of liver toxicity it is contraindicated in patients with liver dysfunction, a creatinine clearance (CrCl) ≤30 ml/min, in permanent atrial fibrillation or congestive heart failure; and should be discontinued in patients who develop these. The European Medicines Agency (EMA), in the Summary of Product Characteristics (SPC) for dronedarone,5 recommended patients should be carefully monitored and supervised by a specialist. Monitoring of liver function should be performed prior to initiation, at one week and monthly up to six months, and at nine and 12 months. Renal function should be tested one-week post-initiation and at regular intervals and electrocardiograms (ECGs) recorded six monthly. This monitoring can be difficult to perform and coordinate, and in October 2012 an arrhythmia specialist nurse (ASN) was appointed by East Sussex Healthcare NHS Trust to oversee this. Required blood tests were arranged with local GPs and coordinated by the ASN. In this paper, adherence to the stipulated schedule has been compared before and after this appointment.
Methods
Data were collected from a single NHS trust between 1 October 2011 and 1 October 2013. Patients started on dronedarone were identified from hospital pharmacy records. Compliance with monitoring was assessed from medical records, and date of cessation noted, where relevant. Data were censored at one year after dronedarone initiation, or at the time of study completion in October 2013, whichever was earlier. Data were stratified according to whether patients started dronedarone prior to, or after the appointment of an ASN. Baseline data, such as gender, age, medical history, echocardiogram findings and previous anti-arrhythmic drug use, were also collected.
Descriptive data were presented and compared in the standard manner. Proportions of tests per patient were compared. Survival analyses were performed for time to first failure to follow dronedarone treatment guidelines, and time to cessation of dronedarone treatment. Comparisons are reported as significant for a two-sided p value of <0.05, and stratified by ASN involvement.
Results
Characteristics of patients taking dronedarone
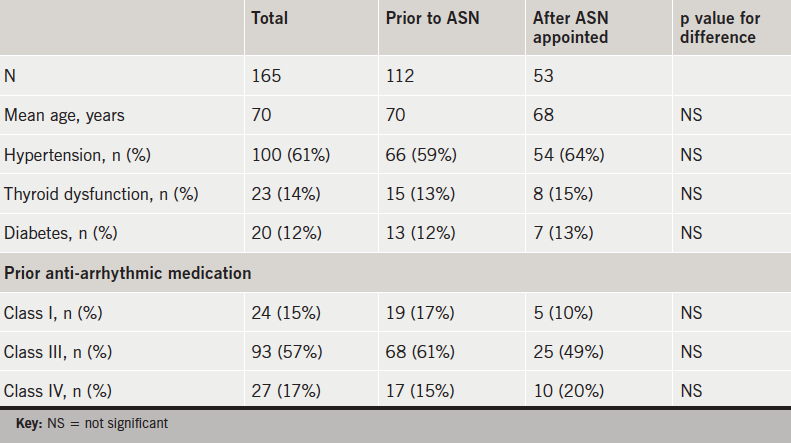
There were 112 patients identified as having started dronedarone prior to the appointment of the ASN, with 53 patients afterwards. There was no significant difference in age, pre-existing hypertension, thyroid dysfunction, diabetes or prior class I, II or IV anti-arrhythmic treatment (table 1).
Table 1. Patient demographics before and after appointment of an arrhythmia specialist nurse (ASN)
There was a significantly longer duration of follow-up (mean 360 vs. 295 days, p<0.001) for those starting dronedarone prior to ASN.
Adherence to recommended monitoring
There were 112 patients commenced on dronedarone prior to the appointment of an ASN. SPC recommendations required 1,275 tests and 478 (37%) were actually performed.
After the appointment of an ASN, 53 patients commenced dronedarone between October 2012 and September 2013. There were 422 tests required by the SPC and 382 were undertaken (92%); a significantly higher number (p<0.001) when compared with the period prior to ASN.
Those starting dronedarone after the ASN was appointed had a significantly longer duration of uninterrupted appropriate monitoring (p<0.001). Figure 1 displays a Kaplan-Meier survival curve, censoring follow-up at study termination or dronedarone cessation.
Figure 1. Time to first failure to follow dronedarone monitoring guidelines
Dronedarone cessation
Of 165 patients starting dronedarone, 75 (45%) stopped during the study period, and this was more prompt following ASN appointment.
Reasons for cessation are shown in table 2. Prior to the ASN, patients were significantly more likely to stop due to contraindications as per SPC; most commonly non-paroxysmal atrial fibrillation. After the ASN was appointed, patients were significantly more likely to stop due to side effects. Drug-related effects were significantly more likely to be recorded after the ASN was appointed.
Table 2. Reasons for dronedarone cessation
Despite concerns regarding liver function, only one patient experienced deterioration in liver function (peak alanine aminotransferase [ALT] 154 IU/L). This was during a hospital admission for pneumonia treated with high-dose intravenous antibiotics. Liver function returned to normal and he remains on dronedarone.
Six patients experienced a rise in potassium levels (peak 5.8 mmol/L) around month one of drug therapy. These resolved in all patients when tests were repeated.
Creatinine levels are known to rise in the early stages of drug therapy with dronedarone,5 and this was noted in seven patients. Levels returned to normal in four patients, but remained elevated in three cases. Peak levels were 187, 214 and 122 µmol/L. In the first two patients, there was a history of renal problems and left ventricular dysfunction; one patient discontinued therapy due to oedema and shortness of breath, but the other continues on therapy with close monitoring. The third patient had no history of renal problems and normal left ventricular function but is no longer taking dronedarone due to oedema and shortness of breath.
Of note, the other four patients who discontinued therapy due to oedema and shortness of breath did not have any change to renal function.
Discussion
Prior to the appointment of an ASN, compliance with recommendations for the monitoring of dronedarone was low. The rate of compliance markedly increased with the appointment of an ASN, from 37% to 92%. The trust covers a rural area with many patients in the study living long distances from a hospital (longest 51 miles). Cooperation between primary and secondary care is essential, and ASNs are ideally placed to provide this link. The EMA guidance for dronedarone monitoring is mandatory and these data confirm that an ASN is an effective way of complying.
Revised marketing authorisations have made the use of dronedarone more complicated, but this is not a disadvantage when supervised by an ASN. In practice, patients are reassured by the knowledge that there is a designated person overseeing their results and that anomalies can be identified quickly. Patients need careful education to encourage them to report any symptoms of heart or liver failure while taking the drug,6 and to comply with monitoring.
Our data indicate that concerns regarding the effect of dronedarone on liver function may be exaggerated. The one patient who had an elevation in ALT was treated for an infection with high-dose antibiotics and has now fully recovered. Renal function has required close monitoring in some patients. There were some instances of transient hyperkalaemia observed; most likely due to haemolysis.
Most patients who required dronedarone cessation did not have blood test abnormalities. This underlines the importance of an appropriately trained professional having regular clinical contact with patients.
There was no significant difference in rates of therapy discontinuation before and after the appointment of the ASN, but the reasons for dronedarone cessation were markedly different. Prior to the ASN, a large proportion of patients stopped dronedarone because of SPC violations. Involvement of an ASN dramatically reduced the likelihood of this highly undesirable situation occurring. Instead, patients reported side effects from dronedarone to the ASN, who could respond appropriately and quickly; sparing anxiety and distress.
Conflict of interest
MA: post funded by Sanofi. RG, SF, CS, NS: none declared..
Key messages
Monitoring of dronedarone is complex
The involvement of an arrhythmia specialist nurse improves adherence to mandatory monitoring and the response to patient side-effects
References
1. Stewart S, Hart CL, Hole DJ, McMurray JJ. Populations prevalence, incidence and predictors of atrial fibrillation in the Renfrew/Paisley study. Heart 2001;86:516–21. http://dx.doi.org/10.1136/heart.86.5.516
2. Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med 2001;113:359–64.http://dx.doi.org/10.1016/S0002-9343(02)01236-6
3. The Office of Health Economics. Estimating the direct costs of atrial fibrillation to the NHS in the constituent countries of the UK and at SHA level in England. Office of Health Economics, 2009.
6. Camm AJ, Savelieva I. Dronedarone for the treatment of non-permanent atrial fibrillation: National Institute for Health and Clinical Excellence guidance. Heart 2013;99:1476–80. http://dx.doi.org/10.1136/heartjnl-3013-303863
Percutaneous coronary intervention (PCI) has established itself as an effective alternative to coronary artery bypass graft surgery (CABG) in appropriate patients. However, the proportion of patients that undergo CABG and/or valve surgery (VS) following PCI in the short and long term is currently unknown.
We conducted a single-centre, retrospective study examining the indications and number of patients requiring CABG and or VS following successful PCI between 2009 and 2012. The surgical procedure was categorised as early (referred within <1 month of the index PCI), mid-term (referred 1–12 months after index PCI) and remote (referred >1 year and up to four years following the index PCI).
During each three-year period (2008–2010, 2009–2011), 5,244 PCIs were performed at our centre. The total number of patients referred for cardiac surgery post-PCI was 63 (1.2%). The number of patients referred for early, mid-term and remote cardiac surgery was 21 (0.4%), 14 (0.26%) and 28 (0.53%), respectively. Within the early group, eight patients had extensive three-vessel disease stabilised with emergency/urgent PCI to allow subsequent CABG, while 10 patients had failed PCI to a chronic total occlusion. In the mid-term group, the main reason for surgery was rapid progression in coronary disease. In the remote group, the majority of patients underwent surgery for progression of valve disease.
Our data suggest that the number of patients requiring CABG and/or VS following PCI is small, and the indications differ with time following the index PCI. We hope that these results will provide reassurance and interest to our interventional colleagues.
Introduction
It is accepted that coronary revascularisation with coronary artery bypass graft surgery (CABG) provides both symptomatic and prognostic benefit in patients with multi-vessel coronary artery disease (mvCAD).1,2 Both percutaneous coronary intervention (PCI) and CABG provide better relief of angina symptoms than medical therapy alone.1,3 Large, randomised-controlled trials (RCTs), in recent years, have demonstrated that CABG offers an improved outcome in patients with complex three-vessel coronary artery disease (CAD), especially in those with co-existing diabetes mellitus.4,5 However, in patients with one- or two-vessel CAD, PCI outcomes are comparable with those achieved with CABG.4,6 In 2012, 92,445 PCI procedures were performed in the UK; a ratio of 5.4 PCI procedures to each isolated CABG operation.7 Furthermore, PCI operators are tackling increasingly complex CAD, previously deemed the domain of the cardiac surgeon. The last hurdle for PCI remains complex distal left main coronary artery (LMCA) disease, which generally is better treated with CABG.6 Despite improvements in stent technology, the need for repeat revascularisation remains higher in PCI than CABG.
The Royal Bournemouth Hospital (RBH) is a medium-sized district general hospital, which houses the Dorset Heart Centre (DHC); a high-volume, non-surgical, cardiology department with five interventional cardiologists (four prior to September 2012) and a busy rapid access chest pain clinic. DHC covers a densely populated area of Dorset with a very high proportion of elderly patients. DHC has been performing PCI since 2005, and currently performs approximately 1,750 PCI procedures per year. All operators have extensive experience in complex calcific mvCAD, utilising rotational atherectomy, excimer laser atherectomy and modern intra-coronary imaging. Two of the PCI operators are experts in chronic total occlusion (CTO) PCI. Cardiac surgical access is provided at Southampton General Hospital. A heart team multi-disciplinary team (MDT) meeting occurs weekly to discuss complex (i.e. left main stem, CTO) or multi-vessel cases. Often, surgery or PCI approach is technically possible, and the final decision is made after discussion with the patient and their relatives. All PCI procedures were performed at RBH.
As a reflection of the high proportion of elderly patients, who often carry significant comorbidity and more often choose PCI over CABG, we have a higher than average ratio of PCI to CABG at 8:1. We were interested to find out if our PCI practice provided effective management of CAD, or whether PCI deferred the timing of CABG referral. Furthermore, it is not unusual for elderly patients to have mild-to-moderate valvular heart disease and we wished to assess what proportion of our patients treated with PCI would subsequently require surgical intervention for valvular disease.
Methods
To obtain this real-world data in a population often excluded from large RCTs due to age, we performed a single-centre, retrospective analysis examining the indications and number of patients requiring CABG and/or valvular surgery (VS) over a four-year period spanning 2009 to 2012. We identified our cohort from an electronic database of all patients referred for cardiac surgical intervention maintained at DHC. From this we identified which patients had previously undergone PCI, and at what time point, by cross-referencing with a second electronic database of all PCI procedures. The medical records of these patients were reviewed to cross-check the data. The timing of the surgical intervention was then categorised as early (referred within one month of the index PCI), mid-term (referred between one month and one year of the index PCI), and remote (referred >1 year and up to four years from the index PCI).
We identified four main reasons why a patient may require CABG after PCI:
Emergency following initial PCI for stabilisation in mvCAD or LMCA disease.
De novo CAD progression.
Technical failure of PCI (unable to revascularise a CTO, undilatable lesions, development of re-stenosis, etc.).
Valvular disease (either unidentified severe disease or progression of previously moderate disease).
For early and mid-term cases the denominator used to calculate incidence of events was the number of cases performed over the three-year period 2009–2011, while for the remote events this was 2008–2010.
Results
From 2008 to 2011 a total of 6,955 PCI procedures were performed at DHC (figure 1). During each three-year ‘denominator’ period (2008–2010 and 2009–2011), 5,244 PCI procedures were performed. The total number of patients referred for cardiac surgery post-PCI was 63 (1.2%). The median age of these 63 patients was 71 years: 35% of patients were aged >70 years, and 17% of patients were >80 years old. By referral time point the number of patients referred for surgery were 21 (0.4%) early, 14 (0.26%) mid-term, and 28 (0.53%) remote (figure 2). There were no cases of emergency/salvage CABG following complication of PCI.
Figure 1. Total number of percutaneous coronary intervention (PCI) cases per year at Dorset Heart Centre between 2008 and 2011
Early referral group (n=21)
Figure 2. Number of patients referred for cardiac surgery after PCI by time point
Within the early referral group, eight patients had extensive three-vessel disease that was initially stabilised with emergency/urgent PCI followed by referral for CABG (figure 3). Six (1.6% of all primary PCI [PPCI] cases) of these cases were ST-segment elevation myocardial infarction (STEMI), one of which was found to have severe aortic stenosis following the PPCI procedure. In five cases, the infarct related artery (IRA) was the right coronary artery (RCA), which was successfully treated with PPCI, but there was significant bystander disease. Two cases (0.08% of all stented acute coronary syndrome [ACS] cases) were non-ST elevation acute coronary syndromes (NSTE-ACS). These early referral patients were not necessarily referred as acute inpatient cases, but the referral was made within one month of the index presentation event.
Within the elective PCI population, 13 patients were referred for CABG after unsuccessful PCI attempts: 10 of these were CTO cases (3.3% of all CTOs), one was a non-dilatable lesion, and two were due to other technical difficulties encountered during PCI attempts (figure 3).
Figure 3. Number of patients referred for surgical intervention within one month of PCI
Mid-term referral group (n=14)
Seven patients in this group required CABG due to de novo disease progression. Three of this group were patients who had undergone PCI for ACS in the recent past, and had returned for further assessment of severe bystander disease. One patient was found to have a fracture of a recently implanted RCA stent plus severe left anterior descending (LAD) disease. One patient attended for intravascular ultrasound (IVUS) assessment of LMCA that confirmed severe disease. After a wire dissection of the left circumflex artery, emergency PCI was performed followed by outpatient referral for CABG. Five patients were referred for CABG due to re-stenosis (1.6% of all re-stenosis treated). One patient was found to have severe valvular heart disease.
Remote referral group (n=28)
There were 18 patients (64%) who had undergone PCI between one and four years previously, who subsequently developed severe valvular heart disease prompting referral for VS. Of these, 17 were due to aortic stenosis, while one patient had severe mitral stenosis. At the time of the preceding PCI, the valve disease had been deemed moderate or less in severity. The median interval between index PCI and referral for VS was 23 months (range 12–52 months). One patient developed significant progressive aortic root dilatation and was referred for aortic root replacement surgery.
Six patients were referred for CABG due to progression in CAD, while two had developed severe in-stent re-stenosis (ISR). One patient, who had undergone ostial RCA stenting, began experiencing transient ischaemia attacks (TIA). Computed tomography (CT) suggested probable fracture of the RCA stent with approximately 1 cm of stent protruding into the aortic root. Following MDT discussion, the patient underwent successful CABG with resection of the stent.
Discussion
Outside of a clinical trial setting, relatively few data exist demonstrating the natural history of coronary artery and valvular heart disease in patients who have undergone PCI. Decisions regarding the preferred revascularisation option for patients with co-existing CAD and mild-to-moderate valvular heart disease can be challenging, especially in older patients whose symptoms are related to their CAD rather than their valvular disease. Our data suggest that in a high-volume, non-surgical centre in the UK, the number of patients who require cardiac surgical intervention within a four-year period following PCI is low.
From our data, it would appear that the reason for surgical referral differs with time. Patients referred within an early or mid-term time point are more often referred for surgical management of CAD. Whereas those referred between one and four years post-PCI were mainly due to progression of valvular heart disease (figure 4).
Figure 4. Proportion of patients referred for surgical intervention by time point and reason for referral
The population served by DHC has a high proportion of elderly and co-morbid patients who carry higher surgical risk. While this may not be representative of all areas of the UK (or worldwide), people are living longer, and the proportion of elderly patients will increase in all regions. In our experience, elderly patients, when given the choice, are more likely to opt for the least invasive revascularisation procedure, even if this carries higher rates of repeat revascularisation.
The rates of PCI failure were higher in 2008 than in current practice, reflecting improvements in stent technology alongside advances in complex PCI. However, despite this progression, ISR remains a concern in PCI, and careful decision-making with judicious use of PCI must be applied on an individual case basis with discussion at a heart team MDT meeting. We feel the majority of re-stenosis can be successfully treated with repeat PCI, which is reflected in the low incidence of referral for CABG in our data. Bioresorbable scaffolds may, with time, alter the incidence of re-stenosis and repeat revascularisation. The advent and rapid uptake of transcatheter valvular interventions is likely to reduce the need for conventional valve surgery in the future.
Conclusion
Data from our high PCI volume, non-surgical centre demonstrate that the number of patients requiring cardiac surgery following PCI is small. Furthermore, the reason for referral for cardiac surgery differs by time point of referral, with problems relating to the PCI procedure occurring earlier and progression of valvular disease coming later. While we accept that these data are non-randomised and from a retrospective analysis, we believe they represent real-life practice that is relevant to populations throughout the UK and potentially worldwide, and may provide interest and reassurance to our colleagues.
Conflict of interest
None declared.
Funding
No funding was sought or obtained for this work.
Key messages
There are well known randomised-controlled trials (RCTs) comparing percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in multi-vessel coronary artery disease (CAD)
Less is known about the contemporary natural history of real-world patients, especially the elderly, following PCI with regards to the incidence of cardiac surgery in the years after PCI
This study demonstrates the incidence of referral for cardiac surgery in a real-world UK population from a busy, high-volume, non-surgical PCI centre
The incidence (in our practice) of referral for cardiac surgery is low even in an elderly population who often have multi-vessel CAD and a degree of valvular heart disease
The indication for cardiac surgery differs depending on the time of referral with CAD predominating early and valve disease later
In the modern era of PCI, the subsequent need to refer a patient for cardiac surgery is low
These data will reassure interventional cardiologists faced with an increasingly complicated, elderly and comorbid population, that good medium- and long-term results can be obtained with contemporary PCI
References
1. Yusuf S, Zucker D, Peduzzi P et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet 1994;344:563–70. http://dx.doi.org/10.1016/S0140-6736(94)91963-1
3. Boden WE, O’Rourke RA, Teo KK et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007;356:1503–16. http://dx.doi.org/10.1056/NEJMoa070829
4. Serruys PW, Morice MC, Kappetein AP et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med 2009;360:961–72. http://dx.doi.org/10.1056/NEJMoa0804626
5. Farkouh ME, Domanski M, Sleeper L et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med 2012;367:2375–84. http://dx.doi.org/10.1056/NEJMoa1211585
6. Mohr FW, Maurice MC, Kappetein AP et al. Coronary artery bypass grafting surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5 year follow-up of the randomized clinical SYNTAX trial. Lancet 2013;381:629–38. http://dx.doi.org/10.1016/S0140-6736(13)60141-5
Correspondence to:
Dr V Singh
Cardiology Department, Grantham Hospital, 101 Manthorpe Road, Grantham NG31 8DG
(Vickramsingh19@yahoo.com)
First published online February 4th, 2015
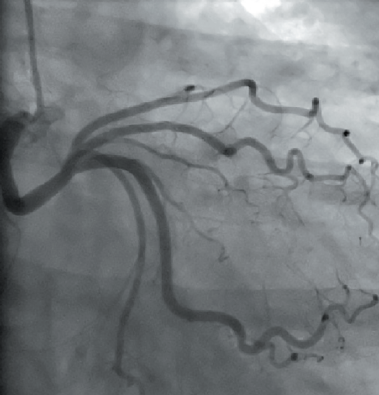
A 53-year-old woman presented with history of exertional chest pain. A coronary angiogram subsequently showed an unusual and rare coronary artery anatomy: all of her coronary arteries originate from the right coronary cusp, with separate ostia. In addition, the left anterior descending (LAD) artery was hypoplastic resulting in ischaemia.
Figure 1. Anteroposterior (AP) view, showing the hypoplastic left anterior descending (LAD) arising from right coronary cusp
Introduction
Coronary anomalies are congenital abnormalities in the coronary anatomy of the heart. They are found in approximately 1% of the population undergoing coronary angiography,1 and are often associated with other structural heart disease. Coronary artery anomalies are a cause of sudden death in the young athlete in the absence of additional heart abnormalities. The aim of this report is to revise this important but often neglected topic, its clinical implications, and to discuss a rare case that was recently encountered in our hospital.
Case presentation
A 53-year-old woman, previously fit and well, presented with a history of exertional chest discomfort radiating to left breast and left arm, with risk factors for coronary artery disease (hypertension and smoking).
Figure 2. Left anterior oblique (LAO)view, showing the right coronary artery(RCA) arising from right coronary cusp
A stress echocardiogram showed a small area of reversible ischaemia in the apex and apical lateral wall. Coronary angiography subsequently showed an interesting coronary artery anatomy: all of her coronary arteries originate from the right coronary cusp with separate ostia. The left anterior descending artery (LAD) was hypoplastic (see figure 1), which is a very rare coronary artery anomaly (less than 0.03%). The right coronary artery (RCA) was a large calibre, tortuous vessel wrapping around the left ventricular apex (see figure 2). The left circumflex artery (Cx) was moderate in size, unobstructed and took a retro-aortic course (see figure 3).
The case was discussed in our regional cardiology and cardiothoracic multi-disciplinary team (MDT) meeting. As she was asymptomatic with only a small area of reversible ischaemia and the LAD (culprit vessel) was hypoplastic, it was not attractive for any sort of intervention or surgery. It was decided that medical management was the best strategy for her.
Figure 3. Right anterior oblique (RAO) view, showing left circumference artery (Cx) arising from right coronary cusp and taking a retro-aortic course
The patient was followed up in the cardiology clinic six months after medical treatment was commenced and she remained asymptomatic.
Discussion
Anomalous origin of coronary arteries are associated with sudden cardiac death, myocardial ischaemia,2,3 volume overload (coronary fistula), aortic root distortion (large coronary fistula or aneurysm), complication during aortic root surgery or angioplasty, and misdiagnosis (missing coronary artery).4 Depending on the number of coronary ostia present, this anomaly may be classified as type I (one coronary ostia), type II (two coronary ostia) and type III (three coronary ostia).2 Type III is the rarest and the one described in this case report.
Unlike effort-related ischaemia typical of fixed obstructive lesions, ischaemia associated with coronary anomalies is not always reproducible with stress testing.2 Ischaemia in these cases only occurs under inconsistent or extreme conditions.
During cardiac catheterisation, if the coronary arteries are difficult to cannulate in their normal positions, we should keep in mind the presence of coronary anomalies. An aortogram is commonly helpful to locate the coronary artery ostia. The success rate is variable, depending upon the operator experience. Non-standard catheters, like a multi-purpose one, are commonly helpful.
In figure 1, there is a faint opacification of the RCA when the LAD was selectively cannulated, suggesting there may be a common stem. However, on selective cannulation of the RCA in figure 2, there does not appear to be a common stem. Other non-invasive techniques like cardiac computed tomography (CT) coronary angiography and cardiac magnetic resonance imaging (MRI) or transoesophageal echocardiography may help if there remains uncertainty.
Medical management includes the use of various anti-anginal medications such as beta blockers, calcium-channel blockers, and the use of diuretics if heart failure is present.5 Specific surgical treatments vary depending upon the type of coronary anomalies, presence of symptoms, and individual circumstances. Common procedures used are: coronary bypass grafting, re-implantation of an anomalous coronary artery from the pulmonary artery into the aorta, reconstruction of proximal or distal coronary arteries, and fistula ligation.
Conflict of interest
None declared.
Key messages
Anomalous coronary artery is a rare and diverse group of congenital disorder present in approximately 1% of the population
The vast majority are benign and just an incidental finding, but care should be given to identify the types with a malignant course, as this can cause sudden cardiac death
Further imaging using computed tomography (CT) coronary angiography or cardiac magnetic resonance imaging (MRI) may be helpful
4. Dollar AL, Roberts WC. Retroaortic epicardial course of the left circumflex coronary artery and anteroaortic intramyocardial (ventricular septum) course of the left anterior descending coronary artery: an unusual coronary anomaly and proposed classification based on the number of coronary ostia in the aorta. Am J Cardiol 1989;64:828–9. http://dx.doi.org/10.1016/0002-9149(89)90780-7
5. Reul RM, Cooley DA, Hallman GL, Reul GJ. Surgical treatment of coronary artery anomalies: report of a 37 ½-year experience at the Texas Heart Institute. Tex Heart Inst J 2002;29:299–307. Available from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC140292/
Further reading
Pollock BD, Belkin RN, Lazar S, Pucillo A, Cohen MB, Weiss MB. Origin of all three coronary arteries from separate ostia in the right sinus of Valsalva: a rarely reported coronary artery anomaly. Cathet Cardiovasc Diagn 1992;26:26–30. http://dx.doi.org/10.1002/ccd.1810260107
Kapoor A, Kumar S, Sinha N. Coronary angioplasty in a case of quadriostial origin of coronary arteries from right aortic sinus. Indian Heart J 2004;56:143–6.
‘Yesterday’s problems, today’s solutions’ was the theme of the 2014 autumn meeting of the British Society for Heart Failure (BSH). A wide-ranging programme covered many topics from uncertainties, myths and dogmas to frightening calls and consultations including the heart failure patient with cancer. Drs Lindsey Tilling and Eleanor Wicks report some of its highlights.
Anaemia was one of several problems chosen for a case-based discussion in a session on common non-cardiac co-morbidities. Dr Callum Chapman (West Middlesex University Hospital) presented the case of an elderly patient with known coeliac disease who had undergone transcatheter aortic valve implantation, which resulted in a paraprosthetic leak and impingement of the mitral valve. Unfortunately despite medical management of the leak she presented to the elderly care service in New York Heart Association (NYHA) Class III heart failure and was extremely oedematous. Blood tests revealed an iron deficiency anaemia and a reduced transferrin saturation. The use of intravenous iron therapy improved symptoms greatly. Ultimately coeliac disease was found to be responsible for her anaemia. During the subsequent audience discussion, the point was made that intravenous iron is superior to oral administration in many ways, and is probably under-utilised.
Uncertainties, myths and dogmas
This session began by Dr Nigel Rowell (Cleveland Health Centre, Middlesbrough) confronting various demographic dogmas. He disputed that the prevalence of heart failure is on the decline, pointing out that data collection is subject to financial issues, errors in coding, and geographical differences. He disproved the suggestion that heart failure admissions are increasing but agreed that there is a high readmission rate, with the first seven to 10 days post-discharge being critical in determining readmission. He also did not agree that heart failure patients’ outlook is poor. He presented data confirming the incidence of heart failure is higher in men than women. While endorsing ischaemic heart disease as the number one cause of heart failure, he refuted the claim that heart failure with a preserved ejection fraction (HFPEF) does not exist.
Dr Paul Kalra (Portsmouth Hospitals NHS Trust) then shed light on the uncertainty surrounding sodium and water restriction in heart failure management. Although perceived as common sense, he questioned whether fluid restriction is good clinical practice. He presented a patient with severe left ventricular systolic dysfunction who became oedematous and hyponatraemic and suggested that guidance to restrict oral intake is ‘reasonable’ in fluid overloaded patients but that there is little strong evidence to support this rationale. Only small studies of patients who are not medically optimised have been undertaken, with variable sodium levels advised, and none have been performed in HFPEF.
A study by Aliti et al. of patients in acutely decompensated heart failure (ADHF) was discussed in detail. These patients found it very difficult to keep to a tight fluid restriction, had no significant weight loss after three days, and complained of thirst. In rats, sodium restriction has been found to increase aldosterone and promote fibrosis, indicating potential deleterious mechanisms, which result from such management in humans. The practical suggestions were to consider fluid restriction in ADHF patients with hyponatraemia in whom diuresis is difficult to control. Additionally patients should be advised to avoid excessive (>3 g/day) salt in their diet.
Anticoagulation in heart failure
The importance of anticoagulation in atrial fibrillation (AF) has been well recognised for many years. The presence of an impaired ventricle in a patient with AF makes an even stronger case for consideration of anticoagulation. The role of anticoagulation in patients with heart failure and sinus rhythm is much less well defined. This ‘uncertainty’ was discussed by Dr Lindsey Tilling (Royal Brompton and Harefield NHS Trust, London).
The recently published, large, randomised-controlled trial WARCEF (Warfarin and Aspirin in Heart Failure with Sinus Rhythm) excluded patients with a pre-existing anticoagulation indication. No difference was seen in the composite end point of intracerebral haemorrhage, ischaemic stroke or death from any cause, but the incidence of ischaemic stroke was significantly lower in the group receiving warfarin versus the group receiving aspirin. The absolute risk reduction, however, was small and this benefit was offset by the increase in bleeding events. European guidance is thus circumspect, stating that in the absence of an overall benefit of warfarin on rates of death and stroke with an increase in major bleeding, there is currently no compelling reason to routinely use warfarin for all heart failure patients in sinus rhythm. No real data exist on the use of novel oral anticoagulant agents (NOACs) in heart failure and sinus rhythm but some trial data of NOACs versus warfarin in AF suggest there may be less bleeding complications with NOACs. This may indicate a possible beneficial role if used in patients with heart failure without AF.
AF remains the undisputed strongest indication for anticoagulation but can we be confident that we have identified all of our patients with AF? A recent study found 40% of heart failure patients with implanted cardiac rhythm devices had atrial arrhythmias over the course of a year. Device therapy is likely to become increasingly prevalent amongst the heart failure population, particularly in the wake of the recently updated NICE (National Institute for Health and Care Excellence) guidelines. This should provide a good opportunity to screen patients for AF.
Finally, there remain several unanswered questions with little or no clinical evidence to support decision-making. These include the role of anticoagulation in HFPEF, and anticoagulation in heart failure of different aetiologies.
Lower cholesterol and HbA1C are better in HF
This myth was controversially exploded by Professor Andrew Clark (BSH President and Hull York Medical School). There is evidence that statins reduce morbidity and mortality in patients with coronary artery disease or with risk factors for coronary disease. But whether statins are of any benefit in heart failure, or indeed, may actually be detrimental, has been long debated. The CORONA (Controlled Rosuvastatin Multinational Trial in Heart Failure) and the GISSI-HF [Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico Heart Failure] trials were provided as evidence of lack of benefit.
CORONA investigated patients over 60 years of age with moderate to severe systolic heart failure of ischaemic origin who were randomised to rosuvastatin 10 mg once a day or placebo. Statin therapy had no effect on the composite end point of cardiovascular death, non-fatal myocardial infarct, or stroke. GISSI-HF enrolled patients over 18 years of age with heart failure of ischaemic and non-ischaemic aetiology. It too failed to demonstrate in the treated arm a reduction in time to death, and time to death or admission to hospital for cardiovascular reasons. During the discussion the speaker asked who would routinely stop statin therapy in their heart failure patients; approximately half of the audience indicated this was their practice.
The widely-held belief that higher HbA1C confers a worse prognosis was then addressed. Professor Clark went back to the original trials: DCCT (the Diabetes Control and Complications Trial), which was conducted in patients with type 1 diabetes, and UKPDS (United Kingdom Prospective Diabetes Study), a landmark study in type 2 diabetes. In the latter trial, the patient group receiving intensive glucose control had a significant reduction in seven diabetes-related events but there was no effect on mortality. Tighter control mainly resulted in a reduction of microvascular complications and there was no statistically significant reduction in macrovascular disease, including cardiovascular events. These results were similar to those of the earlier DCCT trial. The point was made that the Quality Outcomes Framework (QoF) rewards lowered glycosylated haemoglobin measurements and it was questioned whether this is appropriate, at least in terms of cardiovascular outcomes.
Finally, the ACCORD (Action to Control Cardiovascular Risk in Diabetes) study was discussed, which randomised patients with type 2 diabetes to a standard (target HbA1C of 7.0–7.9%) or intensified regime (target HbA1C <6.0%). Of these patients, 35% had a history of a previous cardiovascular event. The study was terminated prematurely after the intensified regime was found to confer a relative increase in mortality of 22% after a mean of 3.5 years. This study indicates that very tight control of HbA1C does not benefit any patient group, and should be borne in mind when managing our diabetes patients with heart failure.
Frightening calls and consultations
The patient with cancer
The audience was given a wake-up call by a presentation on the patient with cancer from Professor Theresa McDonagh (King’s College Hospital, London). She equated oncological therapeutic agents to “weapons of mass destruction”. Although anthracyclines and trastuzumab (Herceptin℗) have improved cancer survival rates dramatically over the last 20 years, she emphasised that the use of complex chemotherapy regimens have the capability to cause catastrophic myocardial ”collateral damage” in up to 25% of patients. Recent years have seen rocketing referral rates for cardiological assessments for those with either primary or metastatic malignancy, those undergoing active chemotherapy or radiotherapy or for survivors of cancer. Cardiologists are, therefore, not infrequently presented with a multitude of ‘car crash’ clinical scenarios within this patient cohort and faced with the stark cardiotoxic complications of oncological treatments, whilst being amidst a swarm of uncertainties. Many questions remain unanswered: Can you ‘cure’ the heart failure within 48 hours to enable the patient to proceed with their next dose of chemotherapy? Should chemotherapy agents be continued or stopped? Should agents be changed or reduced in dose?
Professor McDonagh guided the audience through a systematic strategy for managing cardio-oncological patients. She emphasised the need for an enhanced awareness of the predisposing risk factors for cardiotoxicity (see table 1).
Table 1. Risk factors for the development of anthracyclines cardiotoxicity
She described how identifying such risk factors enables the risk stratification of patients and offers the potential for disease prevention, early identification of disease and the delivery of guided, patient-specific management, according to risk (see table 2). Key recommendations for damage limitation and prevention of left ventricular dysfunction and heart failure when managing such cardio-oncological patients were described:
The use of anthracyclines should be avoided in those with a left ventricular ejection fraction of less than 50% (LVEF <50%) or in those with a drop in LVEF >15% following treatment.
Heart failure should be diagnosed and treated as for any non-cancer patient.
Regular assessment and monitoring of disease should be performed consistently through the use of an electrocardiogram, an echocardiogram and the use of baseline and interval measurements of biomarkers throughout the treatment pathway (including brain natriuretic peptide and troponin). Alternative techniques to assess left ventricular function (e.g. cardiac magnetic resonance imaging or multi-gated acquisition scanning) can be adopted if used consistently.
Table 2. Clinical algorithm for guiding management and monitoring of cardiac risk associated with the use of anthracyclines
Finally, despite a limited evidence-base, prevention of cardiotoxicity was described. Careful pre-treatment assessment and dosing to ensure utilisation of the minimal dose necessary for treatment were suggested. Targeted, focussed radiotherapy with shielding (known to improve protection of myocardial tissue and to prevent coronary disease) and delivering chemotherapy via an infusion rather than a bolus (and using liposomal derivatives with reduced toxicity), were noted to be important. Furthermore, prophylactic treatments using beta blockers, statins and aldosterone antagonists were all postulated to prevent disease development. Despite these management suggestions, Professor McDonagh emphasised that translational and clinical research is required to advance our understanding and evidence base for the use of such strategies in everyday clinical practice.
Dr Simon Williams (University Hospital of South Manchester) moved on to recap succinctly on the potential cardiovascular effects of chemotherapy and described the recognised clinical complications of anticancer therapies, including:
Heart failure with ventricular dysfunction
Fluid overload related to heart failure with preserved ejection fraction (particularly related to alkylating agents)
Hypertension (related to anti-vascular endothelial growth factor agents);
Ischaemia (particularly with 5-Fluorouracil [5FU])
Arrhythmias (relating to QTc prolongation associated with tyrosine kinase inhibitors).
He reiterated that cardiotoxicity can occur as early as within three months of oncological therapy in up to 2% of patients or as late as up to 20 years following treatment in 5% of patients. He echoed that “prevention is better than cure,” emphasising the need for a detailed risk assessment in all patients prior to receiving oncological treatment to ensure the prescription of an individualised treatment strategy (with dose-adjustments, if necessary). He directed cardiologists to the European Society of Medical Oncology (ESMO) guidance for monitoring disease development and progression following the use of anthracyclines or trastuzumab.
He suggested that all patients undergoing oncological treatment should have an echocardiogram and troponin at baseline and at each treatment cycle thereafter (see figures 1 and 2 for anthracyclines or trastuzumab, respectively). Following the detection of abnormalities, he suggested that prognostic heart failure medications should be commenced and that closer monitoring at defined time frames should be instituted. Whilst the evidence base remains small, it was recommended that cardio-oncology patients with left ventricular systolic dysfunction (LVSD) be treated as per conventional national and international heart failure guidelines with lifelong prognostic heart failure medication. Closing remarks emphasised that collaborative, multidisciplinary efforts between cardiology and oncology are key to the management of these patients to ensure improved morbidity and mortality.
Figure 1. A monitoring and treatment algorithm for cardio-oncological patients receiving anthracyclines
Figure 2. A monitoring and treatment algorithm for cardio-oncological patients receiving trastuzumab (Herceptin®)
Devices and surgery
In a session examining devices and surgery “today and tomorrow,” Dr Ninian Lang (University of Glasgow) emphasised the importance of careful patient selection and the balance between risk versus benefit when considering and selecting device therapy. The EchoCRT (Echocardiography Guided Cardiac Resynchronisation Therapy) study demonstrated that in those with NYHA class III or IV symptoms, with an LVEF <30% and echocardiographic evidence of dyssynchrony, but a QRS duration of less than 130 ms, device implantation causes more harm than good. Additionally, MADIT-CRT (Multicentre Automatic Defibrillator Implantation Trial with Cardiac Resynchronisation Therapy) emphasised that in those with less severe symptoms (NYHA class I or II) with an LVEF of <30% and QRS duration >130 ms, only those in left bundle branch block (LBBB) demonstrated benefit from cardiac resynchronisation therapy-combined with a defibrillator (CRT-D) versus implantable defibrillator (ICD) alone. This suggests that QRS duration remains key in device selection irrespective of bundle branch morphology. Furthermore, it was demonstrated in MADIT-RIT (MADIT Randomised Trial to Reduce Inappropriate Therapy) that ICD shocks are disadvantageous, prompting a more conservative approach to device programming.
Dr Lang moved on to highlight the advantages of multipolar leads for improved pacing. These included the potential for improved programming flexibility and targetability for multi-point pacing, alongside their ability for variable stimulation to avoid scar tissue and reduced diaphragmatic twitch. He emphasised the issues surrounding endomyocardial lead placement including thromboembolic complications, as described in the ALSYNC (Alternate Site Cardiac Resynchronisation) study. In contrast to endocardial devices, he described the possibility of reduced device-related risks (both infection and implantation risks) with subcutaneous ICDs, as seen within the EFFORTLESS (Evaluation of Factors Impacting Clinical Outcome and Cost Effectiveness of the S-ICD) registry where 97% of a population of 456 patients with extracardiac devices remained free from complications at 360 days. He reiterated careful patient selection given the inability of such devices to provide bradycardia pacing or anti-tachycardia pacing (ATP).
Finally, Dr Lang emphasised the importance of getting the basics in device selection correct by optimally using our evidence base. Looking to the future, he suggested that we should focus our efforts to “make sense” of the vast quantities of data readily becoming available from these devices to enable a greater understanding for treatment and monitoring within this patient cohort.
In the pipeline
Dr Stephen Pettit (Papworth Hospital, Cambridge) eloquently took us to another level of complexity within the heart failure arena by emphasising the strategies for mechanical circulatory support (MCS) given the limitations in transplantation due to the shortage of donor hearts. Whilst the large, early ventricular assist devices (VADs) have been available since the 1960s, the newer and smaller implantable pumps with their extra-cutaneous drive-lines (such as the HeartWare™ HVAD [within the pericardial space] and HeartMate II™ devices [below the diaphragm]), offer advanced left ventricular (LV) support. Such devices are not without risk, and complications (as described in the INTERMACS study) including driveline infections, peripheral embolism (including intracerebral thromboembolic events and subsequent haemorrhage), device malfunction and device infection are common. Furthermore, devices are burdensome to patients, carers and health care providers alike and require effort for cleaning and dressing care and for management of the system, controller and batteries.
Nevertheless, Dr Pettit offered considerable hope with the potential for new generations of smaller devices (e.g. HeartMate III™ and MVAD HeartWare™ pumps), which offer the potential for easier device implantation without the need for sternotomy and potentially cardiopulmonary bypass. He described tiny circular pumps, including HeartWare X™, which whilst not achieving adequate flows for a left-sided system, offers the potential for right ventricular (RV) support. Similarly, the percutaneous short term VAD, the Impella CP™ device, has the capacity to provide further LV and RV circulatory support. He described future strategies to eliminate driveline infections through the use of an external jacket with coils and magnetic resonators to transfer power to the device. He emphasised the hope for newer devices to enable resumption of normal activities of daily living (such as washing and dressing) whilst offering improved recharging capabilities, which have previously restricted movement.
Other future advances within this arena include the use of materials, such as titanium, to reduce the thrombotic risk, and using stem cells to encourage a neo-intimal layer to grow on the device. In future there will be smaller devices for mechanical circulatory support that are effective, safe and affordable. For the majority of patients, the key is optimal medical management for heart failure. For a few patients, long-term device therapy (so-called ‘destination therapy’) may be appropriate, but there will have to be further consultation to allow the use of devices as destination therapy rather than just as a bridge to transplantation.
Dr Nawwar Al-Attar (Golden University Jubilee Hospital, Clydebank) then walked us through history from Gibbon’s heart and lung machine in 1953, to the first bridge to transplant in 1969, the first LVAD in 1977 and the total artificial heart (TAH) in 1981. He consolidated our understanding of first-, second- and third-generation mechanical circulatory support and described extracorporeal devices, reiterating the future – to be comprised of the smaller LVAD devices HeartMate III™, HeartMate X™, HeartWare MVAD™ and their potential for improved biocompatibility and durability. Dr Al-Attar described how the REACH trials’ extravascular aortic balloon pump can be used to provide aortic counterpulsation. Furthermore, given that 10−20% of patients have concomitant RV failure, he described how the BiVACOR® rotatory biventricular assist device and total artificial heart can be used to overcome the clinical challenges within this specific patient cohort. Finally, he described the advancements and use of the cold storage machine to supply the donor heart with blood and enable tests to be carried out to ensure the viability of donor hearts.
Professor Christian Latrémouille (Georges Pompidou Hospital, Paris, France) brought the meeting to its conclusion by describing the innovative surgical technological advancement on the horizon – ”the novel total integrated bioprosthetic heart”. This model has been proposed as a destination therapy with haemocompatibility. Whilst validated in animal models, Professor Latrémouille described how this therapy has been tried and tested in four patients to date. Clinical outcomes, so far, appear optimistic. Further research needs to validate the in vivo use of this potentially groundbreaking technique to establish whether it can provide true hope to our advanced heart failure communities.
Dr Lindsey Tilling, SpR Cardiology
Dr Eleanor Wicks SpR Cardiology Royal Brompton & Harefield NHS Trust, London
Acknowledgement
The BSH gratefully acknowledges the support provided by the Friends of BSH: Bayer, Medtronic, Novartis, Pfizer, ResMed and Servier Laboratories.
BSH contact details
For further information about the BSH, please contact the society at: E: info@bsh.org.uk, www.bsh.org.uk or twitter @BSHeartFailure
Future BSH meetings
7th BSH Heart Failure Day for Revalidation and Training, 5 March 2015, Charterhouse Square, London
5th BSH Heart Failure Nurse Study Day, 6 March 2015, Charterhouse Square, London
18th BSH Annual Autumn Meeting – 26–27 November 2015, Queen Elizabeth II Conference Centre, London
Authors: Drs Yasmin Ismail, Nathan Manghat, and Mark Hamilton
First published online February 4th, 2015
Correspondence from the world of cardiology
Dear Sirs,
Statistical probabilistic reasoning is important in understanding the likelihood of ‘false-positive’ (FP) and ‘false negative’ (FN) results when requesting any diagnostic test. In cohorts with a low prevalence of disease, a significant number of positive results are likely to be FP. Conversely, when the disease has high prevalence, FN results increase.
Identification of patients with suspected coronary artery disease (CAD) relies on clinical history, examination and electrocardiogram (ECG)/laboratory results. The National Institute for Health and Care Excellence (NICE) define angina as “typical” or “atypical” depending on the presence of key features; diagnostic pathways have thus been developed.1 Non-cardiac pain within this classification requires no further cardiac investigation.
Computed tomographic coronary angiography (CTCA) has emerged as a valuable diagnostic tool in the evaluation of CAD with sensitivities, specificities and negative predictive values (NPV) of >90%.2
Thus whilst CTCA enhances diagnosis,3 the incidence/prevalence of the disease in cohorts is also paramount. Young patients, for example, have a low disease prevalence, while the elderly have a high prevalence, which may result in significant FP in the former and significant FN in the latter.
Accurate history taking and pre-test probability classification, however, may influence the FN/FP rates. We reassessed the impact of history-taking in 50 consecutive CTCA referrals for chest pain.
Prior to cardiac CT acquisition, a repeat history was taken by a senior cardiologist/radiologist according to NICE criteria. All 15 patients referred with ‘typical angina’ were confirmed but of the 32 patients referred with ‘atypical angina’, only 10 out of 32 fulfilled the criteria. Three of the 50 patients referred for CTCA had non-cardiac symptoms. Thus 25 of 50 were classified as ‘non-cardiac’ chest pain (see table 1). Of these 25 patients reclassified as ‘non-cardiac’ chest pain, 12 had evidence of CAD, none of which was severe, 11 had no evidence of CAD and two did not proceed to CTCA at all.
Table 1. Chest pain classification before and after re-assessment according to NICE criteria
Conclusion
The following findings emerged from this study:
1. 50% of patients referred may not have needed any cardiac investigation. Such referrals result in unwarranted exposure to radiation as well as unnecessary further investigations, patient anxiety and effectively amounts to using CT as a screening tool for CAD.4
2. A failure to account for disease prevalence in research studies may have significantly overestimated the non-predictive value of CTCA.
3. Inaccurate history taking appears to be a major cause of misclassification. This may be due to several factors: a) clinician anxiety about missing significant CAD and consciously/subconsciously misclassifying the patient to justify a CTCA; b) patients’ recollection of symptoms may alter over time, or; c) clinicians’ lack of awareness of NICE criteria. We recognise that the history taken at the time of CTCA may have been limited.
4. Accurate history taking may reduce the adverse impact on individual patients, protect NHS resources and ensure the appropriate utility of nationally-defined pathways for chest pain management.
Acknowledgment
This research was supported by the National Institute for Health Research Biomedical Research Unit in Cardiovascular Disease at the University Hospitals Bristol NHS Foundation Trust and the University of Bristol.
Conflict of interest
None declared.
Yasmin Ismail, Consultant Cardiologist
Nathan Manghat, Consultant in Cardiac Radiology
Mark Hamilton, Consultant in Cardiac Radiology
Bristol Royal Infirmary, University Hospitals Bristol NHS Foundation Trust, Upper Maudlin Street, Bristol BS2 8HW
2. Chow B, Abraham A, Wells G, et al. Diagnostic accuracy and impact of computed tomographic coronary angiography on utilization of invasive coronary angiography. Circ Cardiovasc Imaging 2009; 2:16–23. http://dx.doi.org/10.1161/CIRCIMAGING.108.792572
3. Wallis A, Manghat N, Hamilton M. The role of coronary CT in the assessment and diagnosis of patients with chest pain. Clin Med 2012;12:222–9.
4. Melgies J, Hamilton MC, Manghat NE. Computed tomographic coronary angiography – is it ready as a screening tool for coronary artery disease? Clin Med 2013;13:465–7. http://dx.doi.org/10.7861/clinmedicine.13-5-465
There has been much debate regarding the prophylactic prescribing of antibiotics in patients deemed at risk of developing infective endocarditis (IE) as a result of certain dental procedures.1 The National Institute for Health and Care Excellence (NICE), the British Society for Antimicrobial Chemotherapy (BSAC) and the American Heart Association (AHA) have produced differing guidelines for dental practitioners, who may decide to accept one particular code entirely, or a modified version based on discussion with local cardiology departments.
This culture of debate amongst cardiologists, dentists and patients regarding best interest, success rates, allergy and development of antibiotic resistance, can only be of relevance when all preventative parameters are first exhausted and the patient’s individual risk is brought to the lowest level reasonably possible prior to scheduled surgery.2
Removing potential causes of infection as well as reducing the risk of bacteraemia-associated complications, when preformed preoperatively, could reduce the future likelihood of developing the disease.3 A pragmatic approach would be to complete a hospital-based, dentist led, oral health risk assessment pre-operatively, for patients scheduled to receive cardiac surgery associated with those conditions which all guidelines consider to pose a risk, with intervention taken where necessary.
Perhaps at hospital level we should place a greater emphasis on oral screening during pre-operative assessment clinics, to both reduce the future risk of IE and add further to the discussion of prophylactic antibiotic prescribing.
Musgrove Park Hospital Taunton, Taunton and Somerset NHS Foundation Trust, Musgrove Park, Parkfield Drive, Taunton, Somerset TA1 5DA
References
1. Glenny AM, Oliver R, Roberts GJ, Hooper L, Worthington HV. Antibiotics for the prophylaxis of bacterial endocarditis in dentistry. Cochrane Database Syst Rev 2013. http://dx.doi.org/10.1002/14651858.CD003813.pub4
2. Rahman N, Rogers S, Ryan D, Healy C, Flint S. Infective endocarditis prophylaxis and the current AHA, BSAC, NICE and Australian guidelines. J Ir Dent Assoc 2008;54:264–70.
3. Yasny JS, Silvay G. The value of optimizing dentition before cardiac surgery. J Cardiothorac Vasc Anesth 2007;21:587–91.
Rheumatic heart disease (RHD) is the most common acquired heart disease in children in many parts of the world, especially in developing countries. The global burden of disease caused by rheumatic fever and RHD currently falls disproportionately on children and young adults living in low-income countries and is responsible for about 233,000 deaths annually. At least 15.6 million people are estimated to be currently affected by RHD, with a significant number of them requiring repeated hospitalisation and often unaffordable heart surgery in the next five to 20 years.1 Primary prevention of acute rheumatic fever is achieved by treatment of acute throat infections caused by group A streptococcus. Each attack of rheumatic fever further worsens the damage to the heart valves and if regular secondary prophylaxis is taken after initial attack, the valves may remain unaffected. Secondary prevention is thus very important to prevent further attacks of rheumatic fever with procaine penicillin, a cheaper antibiotic, most commonly used for secondary prophylaxis. Secondary prevention programmes are currently thought to be more cost effective for prevention of RHD than primary prevention and may be the only feasible option for low- to middle-income countries in addition to poverty alleviation efforts.2 Stuck valve is an important complication in patients with mechanical valves and poses a significant mortality risk.3
The Indira Gandhi Institute of Cardiology is the largest tertiary cardiac centre in Bihar, a major state of northern India. The mortality due to rheumatic heart disease in this cardiac centre during 2013 was 120 with more deaths in women (n = 67, 56%) than men (n = 53, 44%). Median age at death was 35 years. Minimum age at death was eight years and maximum age was 73 years. Three patients had balloon mitral valvulotomy (BMV), one had closed mitral valvulotomy (CMV), eight had mitral valve replacement (MVR) and four had double valve replacement (DVR). The highest number of deaths was noted in the 31–40 years age group, (19 women 18 men). Out of a total 120 deaths, four had stuck valves (three had MVR and one had DVR).
A register-based project for control of acute rheumatic fever (ARF)/RHD was launched by the World Health Organization (WHO) in 1972, which showed a significant reduction in health costs. WHO then embarked upon a global programme and, by 1990, ARF registers had been established in 16 countries with over 3,000 cases of RHD or prior ARF detected. A later review highlighted improved compliance with secondary prophylaxis4 but subsequently only a few countries expanded their programmes.
Today, well-developed telecommunication systems could be very useful in ensuring secondary prophylaxis. Reminders could be sent through patients’ registered phone numbers in cases of non-compliance. Thus a higher percentage of secondary prophylaxis could be ensured, which would ultimately reduce the overall prevalence of RHD and the presence of severe forms of the disease in society. Regular surveys of schools and villages would also detect new cases. The community also needs to be educated about RHD through posters, banners and television shows advising timely medical attention.
Through these multipronged measures the burden of this crippling disease can be reduced in the underprivileged world.
2. Kumar R. Controlling rheumatic heart disease in developing countries. World Health Forum. 1995;16:47–51.
3. Shapira Y, Hirsch R, Jortner R, Nili M, Vidne B, Sagie A. Prosthetic heart valve thrombosis: a 3-year experience. Harefuah 1997;133:169–73, 246.
4. M, Brown A, Noonan S, Carapetis JR. Preventing recurrent rheumatic fever: the role of register-based programs. Heart 2005;91;1131–3. http://dx.doi.org/10.1136/hrt.2004.057570
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits
 With the growing burden of cardiovascular disease, the number of people undergoing cardiac surgery, globally, is expected to continue to rise.1 In 2010, 31,613 cardiac surgeries were performed in England and Wales,2 and prevalence data are similar in other Commonwealth countries, including Canada.2,3 While the primary aims of cardiac surgical procedures (including coronary artery bypass grafting [CABG] and valve replacement) are to improve survival, ameliorate symptoms (such as angina) and improve health-related quality of life (HRQL), mounting evidence suggests that the development of chronic post-surgical pain (CPSP) and related poor functional recovery following these procedures are major clinical problems for substantial numbers of patients.
With the growing burden of cardiovascular disease, the number of people undergoing cardiac surgery, globally, is expected to continue to rise.1 In 2010, 31,613 cardiac surgeries were performed in England and Wales,2 and prevalence data are similar in other Commonwealth countries, including Canada.2,3 While the primary aims of cardiac surgical procedures (including coronary artery bypass grafting [CABG] and valve replacement) are to improve survival, ameliorate symptoms (such as angina) and improve health-related quality of life (HRQL), mounting evidence suggests that the development of chronic post-surgical pain (CPSP) and related poor functional recovery following these procedures are major clinical problems for substantial numbers of patients.