Heart valve disease is as common as heart failure. The population prevalence is 2.5% rising to over 10% in people aged more than 75.1
It has received disproportionately little exposure in terms of research, national treatment strategies and public awareness. This is beginning to change, partly with a rise in prevalence as our population ages and partly as a result of technological advances including transcatheter procedures. In this module we will describe the causes and frequency of valve disease. We will also discuss variations in the delivery of care.
Causes of valve disease
Temporal and geographical trends
Rheumatic fever is the most common cause of valve disease in the young2 but predominates in industrially underdeveloped regions. These include Africa, India, the Middle East, South America, parts of China and Russia, and the aboriginal populations within Australia and New Zealand.
For further information on rheumatic fever and its consequences, with the development of rheumatic heart disease, see this World Heart Federation video outlining the public health challenges of this condition
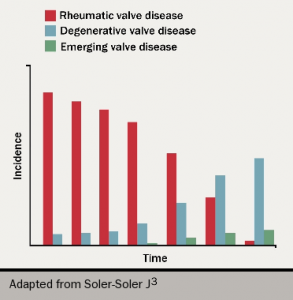
In industrially developed countries, the incidence of rheumatic disease declined after the second half of the 20th century (see figure 1). With increased longevity, valve conditions characteristic of old-age now predominate. The most common are calcific aortic stenosis and functional mitral regurgitation.
Figure 1. Diagram illustrating changes in prevalence of valve disease in industrially-developed countries
There has also been a rise3 in new diseases induced by drugs or therapeutic irradiation, an increase in endocarditis related to intravenous drug use, device implantation and haemodialysis and a rise in the number of operations as a result of failing replacement heart valves.
Drugs
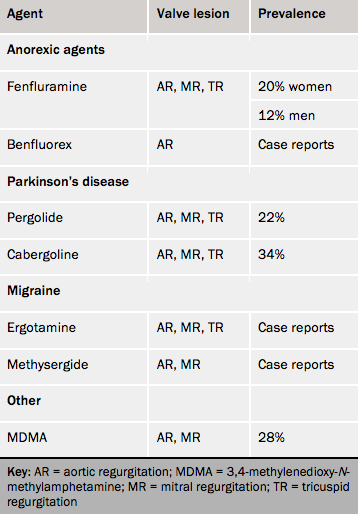
The valve lesions caused by drugs resemble those from carcinoid tumours. These arise from neural crest gastrointestinal enterochromaffin cells in 1 in 75,000 people.4 The carcinoid syndrome develops in about one half as a result of hepatic spread and carcinoid heart disease develops in 40% of these. The cardiac lesions are caused by the paraneoplastic effects of vasoactive substances, notably 5-hydroxytryptophan (5HT). The drugs known to cause valve disease (see table 1) are either themselves or have metabolites that are agonists at 5HT2B receptors.
Table 1. Drugs causing valvopathy
Drug-induced lesions are similar to those found in carcinoid disease.
Interaction with the 5-HT2B receptor stimulates cardiac fibroblast proliferation leading to fibrous plaques with a ‘pearly white’ appearance on valves and chordae.
The earliest sign of valve involvement is an increase in the tenting height of the mitral valve, which is the distance between the point of apposition and the plane of the annulus.
Pergolide and cabergoline cause valve disease when used in the relatively large doses necessary for Parkinson’s disease. With the small doses used for microprolactinoma, valvopathy appears to be rare, but can occur after relatively large doses used for periods in excess of 10 years.
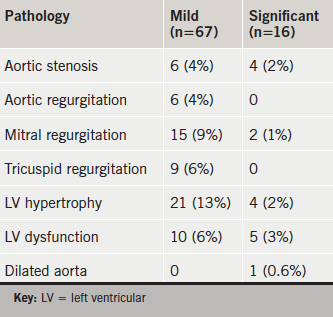
Structural heart disease may be missed using clinical examination alone and limited echocardiograms or ‘quick-scans’ may be a way to improve rates of detection. To evaluate the finding of clinically unexpected abnormalities using ‘quick-scans’, scans were performed in a general practice by a level 7 sonographer using a GE V scan system. Indications were: murmur; potentially cardiac symptom (e.g. chest pain or breathlessness); cardiac history in the GP notes (e.g. myocardial infarction); atrial fibrillation; chronic obstructive pulmonary disease with disproportionate dyspnoea; age ≥75 years. Standard transthoracic echocardiograms were performed if clinically indicated or if the ‘quick-scan’ detected a significant abnormality.
There were 163 ‘quick scans’ indicated, which were normal in 80 (49%), mildly abnormal in 67 (41%) and significantly abnormal in 16 (10%). Abnormalities were moderate left ventricular (LV) systolic dysfunction, moderate mitral regurgitation, moderate-to-severe aortic stenosis and mild aortic dilatation. Within the 90 patients without agreed indications the ‘quick-scans’ were normal in 64 (71%) and mildly abnormal in 26 (29%) while none were significantly abnormal.
In conclusion, ‘quick scans’ can detect clinically unexpected pathology. These results are consistent with a global move to use the hand-held ultrasound machine as an extension of the clinical examination.
Introduction
Heart failure and valve disease are common. The population prevalence of each is 2–3% and this rises to more than 10% aged ≥75 years.1,2 Echocardiography is a key diagnostic investigation but it is a relatively scarce resource and is also underutilised.3 It has been suggested that access can be improved by targeting high-risk individuals using limited ‘point-of-care’ studies also called ‘quick-scans’.4 There has been an increase in the application of ‘quick-scans’ with the development of hand-held machines, which allow near-patient testing in the community or on ward-rounds, in clinics or in emergency departments.5,6 However, experience with ‘quick-scans’ in the community using hand-held ultrasound devices is limited. We, therefore, set up a pilot clinical service.
Methods
Setting
The new service was offered by newsletter and direct email to all GP practices in Lambeth and Southwark, of which, two expressed interest. For the first, a regular time slot for ‘quick-scans’ was staffed every week, but only 13 patients were referred in seven weeks and these were judged insufficient for analysis. The second practice had a list of 12,565 patients, did not have booked visits and saw typically 100 patients daily. This practice referred 253 patients on two sessions a week over 26 weeks.
Quick scan
We used a V scan (GE Medical Systems), which has a display unit 135 × 73 × 28 mm in size and weighs 390 g. ‘Quick-scans’ were performed by a level 7 sonographer. The scan consisted of imaging and colour Doppler in the parasternal long-axis and short-axis views, apical four-chamber, two-chamber and three-chamber views and a subcostal view.
Scans were classed as normal if they were completely normal, or if there was no more than: mild aortic or mitral valve thickening; trivial aortic or mitral regurgitation; or mild-to-moderate tricuspid regurgitation. The following were classed as mildly abnormal: mild left ventricular (LV) hypertrophy (septal thickness 12–14 mm); borderline LV systolic dysfunction (LV ejection fraction 50–55%); mild aortic dilatation; mild valve restriction; mild aortic or mitral regurgitation; moderate tricuspid regurgitation. The following were classed as significantly abnormal: LV hypertrophy (septal thickness >14 mm); LV ejection fraction <50%; at least mild valve stenosis; moderate or worse aortic or mitral regurgitation; more than mild aortic dilatation; severe tricuspid regurgitation.
Indications for referral for ‘quick-scans’ were: age ≥75 years, cardiac symptoms (chest pain, palpitations, syncope); murmur; chronic obstructive pulmonary disease (COPD) with disproportionate breathlessness; cardiac history in the GP notes (e.g. myocardial infarction); abnormal electrocardiogram (ECG) including atrial fibrillation; high risk of rheumatic disease. Patients who were under cardiac care or had a recent echocardiogram were not scanned. Standard transthoracic echocardiograms were performed if clinically indicated or if the ‘quick-scan’ detected a significant abnormality.
The analysis was approved as a Trust service evaluation (no. 4,034).
Results
A total of 253 patients underwent a ‘quick-scan’. However, only 163 (64%) fitted the inclusion criteria. These were aged 72 ± 10 years (37% male and 63% female). A further 90 aged 65 ± 8 years (38% male and 62% female) were scanned at the GPs’ request despite not having agreed indications. Of these, 55 (61%) had systemic hypertension. These were analysed separately as a comparator group.
Table 1. Frequency of abnormalities in 163 patients at the GP practice
In the 163 patients with the agreed indications, the ‘quick-scan’ was normal in 80 (49%), mildly abnormal in 67 (41%) and significantly abnormal in 16 (10%) (table 1). In those aged ≥75 years, there were 10 (12%) with significant abnormalities. A subsequent standard transthoracic study confirmed moderate aortic stenosis in three, moderate-to-severe aortic stenosis in one, moderate mitral regurgitation in one, moderate-to-severe mitral regurgitation in one, moderate LV systolic dysfunction in four, moderate-to-severe dysfunction in one, LV hypertrophy in four and mild aortic dilatation in one.
Within the 90 patients without agreed indications the ‘quick-scans’ were normal in 64 (71%) and mildly abnormal in 26 (29%), while none were significantly abnormal. The mild abnormalities were: aortic regurgitation in three (3%); mitral regurgitation in 11 (12%); LV hypertrophy in eight (9%); borderline LV dysfunction in two (2%).
Discussion
Summary
This study showed that ‘quick-scans’ detected significant structural disease in 10% of patients with focused indications at a general practice and in 12% of those aged ≥75 years.
Limitations of current screening for heart failure and valve disease
The most common reasons for requesting echocardiography are suspected heart failure or valve disease.3 However, patients with heart failure may be misdiagnosed as having COPD,7 or may have both conditions,8 and may not be screened either with B-type natriuretic peptide levels or echocardiography. We, therefore, included patients with COPD but inappropriate breathlessness as an indication for a ‘quick-scan’. A murmur is an insensitive and nonspecific screen for valve disease and an audit of open-access echocardiography3 suggested that the yield of significant valve disease could be doubled by widening the indications to include an abnormal ECG or cardiac symptoms. In this study, we also included patients aged ≥75 years because the prevalence of valve disease is known to be >10% in this group,2 which we judged was a reasonable sensitivity to justify screening.
Clinical significance of the abnormalities detected
Screening has to be performed judiciously to avoid finding mild abnormalities that do not need treatment and merely raise unnecessary anxiety.9 For this reason, ‘quick-scans’ should not be performed without a reasonable clinical suspicion of structural disease. The ‘quick-scans’ were normal or near-normal in all 90 cases lacking agreed indications in this study. Most of the abnormalities we detected, even with agreed indications, were indeed mild but they were significant in 10%. It is best practice to follow patients with moderate valve disease in a specialist valve clinic,10 to allow correct timing of surgery, so these unsuspected diagnoses were clinically important.
Comparison with existing literature
‘Quick-scans’ have mostly been evaluated in the hospital setting including the intensive care unit or emergency room.5 They are reliable for predicting a normal standard echocardiogram.11,12 As, in our experience, they also detect clinically unexpected abnormalities, 17% in one series13 with no apparent indications for standard echocardiography. We are not aware of any service similar to ours, although portable studies have been shown to be useful at detecting LV hypertrophy in the community,14 and to be cost-effective in triaging the need for standard echocardiography in suspected heart failure.15 Our rate of abnormalities is similar to that in population screening studies,1,2 while there were no abnormalities in the cases without agreed indications suggesting that our method of focusing studies was effective.
Strengths and limitations
The population was necessarily general, and there were few patients fitting the indications for ‘quick-scans’, making it hard to fill a list. In fact a number of patients were referred outside the agreed indications, probably encouraged by the presence of the sonographer. This suggests that a separate list might be a better way to manage the service, although this approach did not work at the second GP practice participating. The logistics of the service, therefore, need to be agreed nationally,4 and are expected to vary according to local resources. It is vital that a service should be provided by suitably qualified and experienced staff, with operating systems including quality control that are as good as those in standard echocardiography services.12,16
Implications for practice
‘Quick-scans’ appear a useful method of screening a relatively high-risk community population, since a clinically useful yield of unexpected significant structural disease is obtained. These results are consistent with a global move to use the hand-held ultrasound machine as an extension of the clinical examination.
Key messages
A ‘quick-scan’ detects significant abnormalities in 10% of people clinically judged as high risk
Valve disease and left ventricular dysfunction were the most common abnormalities found
‘Quick-scans’ effectively extend the clinical examination and triage the need for standard transthoracic echocardiography.
Conflict of interest
None declared.
Funding
The salary for the level 7 sonographer and the cost of the V scan were supplied by Edwards Life Sciences who played no role in the design, conduct and analysis of the results of the service.
1. McMurray JJV, Adamopoulos S, Anker SD et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012. Eur J Heart Fail 2012;14:803–69. http://dx.doi.org/10.1093/eurjhf/hfs105
3. Chambers J, Kabir S, Cajeat E. Detection of heart disease by open access echocardiography: a retrospective analysis of general practice referrals. Br J Gen Pract 2014;64:e105–e111. http://dx.doi.org/10.3399/bjgp14X677167
6. Panoulas VF, Daigeler AL, Malaweera AS et al. Pocket-size hand-held cardiac ultrasound as an adjunct to clinical examination in the hands of medical students and junior doctors. Eur Heart J Cardiovasc Imaging 2013;14:323–30. http://dx.doi.org/10.1093/ehjci/jes140
7. Miller MR, Levy ML. Chronic obstructive pulmonary disease: missed diagnosis versus misdiagnosis. BMJ 2015;351:h3021. http://dx.doi.org/10.1136/bmj.h3021
8. Rutten FH, Cramer M-JM, Grobbee DE et al. Unrecognized heart failure in elderly patients with stable chronic obstructive pulmonary disease. Eur Heart J 2005;26:1887–94. http://dx.doi.org/10.1093/eurheartj/ehi291
9. McDonald IG, Daly J, Jelinek VM, Panetta F, Gutman JM. Opening Pandora’s box: the unpredictability of reassurance by a normal test result. BMJ 1996;313:329–32. http://dx.doi.org/10.1136/bmj.313.7053.329
10. Lancellotti P, Rosenhek R, Pibarot P et al. Heart valve clinics: organisation, structure and experiences. Eur Heart J 2013;34:1597–606. http://dx.doi.org/10.1093/eurheartj/ehs443
11. Greaves K, Jeetley P, Hickman M et al. The use of hand-carried ultrasound in the hospital setting – a cost-effective analysis. J Am Soc Echocardiogr 2005;18:620–5. http://dx.doi.org/10.1016/j.echo.2004.09.015
12. Spencer K, Kimura B, Korcarz C et al. Focused cardiac ultrasound: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr 2013;26:567–81. http://dx.doi.org/10.1016/j.echo.2013.04.001
13. Fedson S, Neithardt G, Thomas P et al. Unsuspected clinically important findings detected with a small portable ultrasound device in patients admitted to a general medical service. J Am Soc Echocardiogr 2003;16:901–05. http://dx.doi.org/10.1016/S0894-7317(03)00426-7
14. Senior R, Galasko G, Hickman M, Jeetley P, Lahiri A. Community screening for left ventricular hypertrophy in patients with hypertension using hand-held echocardiography. J Am Soc Echocardiogr 2004;17:56–61. http://dx.doi.org/10.1016/j.echo.2003.09.013
15. Galasko GIW, Barnes SC, Collinson P, Lahiri A, Senior R. What is the most cost-effective strategy to screen for left ventricular systolic dysfunction: natriuretic peptides, the electrocardiogram, hand-held echocardiography, traditional echocardiography, or their combination? Eur Heart J 2006;27:193–200. http://dx.doi.org/10.1093/eurheartj/ehi559
16. Sicari R, Galderisi M, Voigt J-U et al. The use of pocket-size imaging devices: a position statement of the European Association of Echocardiography. Eur J Echocardiogr 2011;12:85–7. http://dx.doi.org/10.1093/ejechocard/jeq184
I first started using the V scan myself over four years ago, and I have found this hand-held mobile device extremely useful for providing rapid and important diagnostic information at the bedside. The quality of the images of the V scan are usually of sufficiently high quality to make a useful clinical assessment. It is usually possible to make a fair assessment of systolic function of the left ventricle. I have also found that the identification of a dilated right heart has often been very useful for diagnosing massive pulmonary emboli – quite frequently when this diagnosis would not otherwise have been suspected. Valve lesions of significance are invariably pretty obvious and the images are usually adequate to identify vegetations as well. Pericardial effusion is readily detected.
Focused cardiac ultrasound using a pocket-sized imaging device (V scan) is increasingly being used to screen patients in the emergency setting for structural heart disease. We describe a patient who presented with light-headedness and pallor with elevated high-sensitivity troponin T (hs-TnT) and was initially thought to have acute coronary syndrome. A screening focused cardiac ultrasound revealed a dilated right ventricle with normal left ventricular function, and a computerised tomography pulmonary angiogram (CTPA) demonstrated a large saddle pulmonary embolus. The case highlights the application and utility of focused cardiac ultrasound and provides an overview of its current role in the acute setting reinforced by current guidelines from the European Society of Cardiology.
Case report
A 74-year-old male with previous hypertension and myocardial infarction presented with light-headedness after walking down the stairs at home. He denied chest pain, but complained of shortness of breath on exertion. In the accident and emergency department he was noted to be pale and clammy. Initial observations were: regular pulse 88 bpm, blood pressure 127/81 mmHg, respiratory rate 20/min, and Sp02 95% (later consistently greater than 97%). He had stopped smoking aged 34 years.
On examination his chest was clear, the heart sounds were normal, the jugular venous pressure was not elevated and he had no peripheral oedema.
Initial electrocardiogram (ECG) showed normal sinus rhythm with a partial right bundle branch block, QRS duration 119 ms, and poor R-wave progression (figure 1).
Figure 1. Electrocardiogram (ECG) showing normal sinus rhythm with a partial right bundle branch block, QRS duration 119 ms, and poor R-wave progression
Blood tests revealed an elevated N-terminal pro-brain natriuretic protein (NT-proBNP) 2,354 ng/L, and a rise in high-sensitivity troponin T (hs-TnT) from 85 to 287 ng/L at three hours. He was treated for an acute coronary syndrome with antiplatelets and fondaparinux, and transferred to the coronary care unit.
Figure 2. Computerised tomography pulmonary angiogram (CTPA) showing a saddle pulmonary embolism, with the thrombus extending bilaterally into the lobar pulmonary arteries
On review by the cardiology consultant, the symptom of light-headedness had resolved. He denied any chest pain or shortness of breath, and remained haemodynamically stable. The working diagnosis was an atypical presentation of acute coronary syndrome.
A screening focused cardiac ultrasound using a V scan revealed a dilated right ventricle with normal left ventricular systolic function. D-dimer was measured at 3,088 µg/L, and the patient was anticoagulated with low-molecular weight heparin. Computerised tomography pulmonary angiogram (CTPA) showed a saddle pulmonary embolism, with the thrombus extending bilaterally into the lobar pulmonary arteries (figure 2). The patient was commenced on warfarin. Subsequent ECG showed T-wave inversion in V1–2, III and AVF.
Figure 3. The V scan device
Discussion
The V scan is a pocket-sized ultrasound device that can provide 2D cardiac imaging/measurements and limited colour Doppler information (figure 3). This can provide important information to aid the diagnostic process, particularly in patients with non-specific symptoms and elevated cardiac biomarkers.1 Focused cardiac ultrasound is not equivalent to emergency echocardiography, and its limitations in practice must be noted. The European Society of Cardiology (ESC) has published recommendations for the use of emergency echocardiography,2 and also a separate position statement for the use of pocket-size devices.3 The two main indications for focused cardiac ultrasound using pocket-size devices are as a tool for fast initial screening in an emergency setting, and as a complement to a physical examination in the coronary and intensive care unit (table 1). Large pulmonary emboli may present with non-specific or vague symptoms, without evidence of significant hypoxia and without significant abnormality on the ECG. However, if large enough to cause right ventricular strain they can lead to elevated cardiac enzymes leading to a spurious diagnosis of acute coronary syndrome. Massive pulmonary embolism should always be considered in the differential diagnosis of patients with elevated cardiac enzymes, since the management of this life-threatening condition is very different to that used for acute coronary syndrome.
Table 1. Indications for focused cardiac ultrasound
Use of focused cardiac ultrasound is becoming more frequent in the initial assessment of patients on the coronary care unit and the threshold for its use in the appropriate context should be low.
Key messages
Focused cardiac ultrasound using a pocket-sized imaging device supplies valuable diagnostic information not provided by other bed-side diagnostic tests
Massive pulmonary embolism may present with non-specific symptoms, and should always be considered in the differential diagnosis of patients with elevated cardiac biomarkers
Pocket-sized imaging devices are useful for fast screening patients in the emergency setting or as a complement to physical examination
1. Prinz C, Voigt JU. Diagnostic accuracy of a hand-held ultrasound scanner in routine patients referred for echocardiography. J Am Soc Echocardiogr 2011;24:111–16. http://dx.doi.org/10.1016/j.echo.2010.10.017
2. Neskovic AN, Hagendorff A, Lancell P et al. Emergency echocardiography: the European Association of Cardiovascular Imaging recommendations. Eur Heart J Cardiovasc Imaging 2013;14:1–11. http://dx.doi.org/10.1093/ehjci/jes193
3. Sicari R, Galdferisi M, Voigt J et al. The use of pocket-size imaging devices: a position statement of the European Association of Echocardiology. Eur J Echocardiogr 2011;12:85–7. http://dx.doi.org/10.1093/ejechocard/jeq184
Sally Schreder
Lead Nurse for Cardio-Pulmonary Rehabilitation
Sally Singh
Head of Pulmonary and Cardiac Rehabilitation
Centre for Exercise and Rehabilitation Science, Respiratory BRU, University Hospitals of Leicester NHS Trust, Glenfield Hospital, Groby Road, Leicester, LE3 9QP
Amye Watt
Physiotherapist
Cardiac Rehabilitation, University Hospitals of Leicester NHS Trust, Glenfield Hospital, Groby Road, Leicester, LE3 9QP
People with chronic heart failure (CHF) often experience exacerbations of their symptoms that require hospitalisation. The feasibility, safety and efficacy of early post-exacerbation rehabilitation are largely unknown in this population.
This was a single-centre, feasibility trial of early rehabilitation versus usual care. Those assigned to the intervention started rehabilitation within 10 days of discharge and attended supervised sessions twice per week for eight weeks. The primary outcomes were feasibility of uptake and safety. Assessments were performed at baseline and three months: exercise tolerance (shuttle walking tests) and health status (questionnaire).
There were 1,298 patients screened, 16 patients recruited (<1% of those screened) and 11 randomised (five rehabilitation, six control). The primary reasons for exclusion were contraindication to exercise and normal ejection fraction. There were improvements in exercise tolerance and health status in both groups at three months; however, the study was not powered to report any within- or between-group significance. The early rehabilitation intervention was safe with no adverse events reported.
In conclusion, early rehabilitation, for patients with CHF, was unfeasible. The 10-day recruitment target was too restrictive in this population. This is important because there has been a drive towards early rehabilitation in CHF guidelines.
The proportion of patients with heart failure with preserved ejection fraction (HFPEF), compared with those with reduced ejection fraction (HFREF), is significant and rising. Studies have used an ejection fraction (EF) >50% as the sole criteria for identifying patients with HFPEF. However, European Society of Cardiology (ESC) guidelines include the diagnostic criteria of EF >50% and evidence of diastolic dysfunction.
In this retrospective cohort study based on admissions in 2012; we compared characteristics, treatment and outcomes between HFPEF and HFREF patients. One year readmission and survival rate was also assessed.
Overall, 41 (17%) patients had HFPEF (EF >50% and either medial or lateral E/E’ >15) compared with 200 (83%) with HFREF. Age was similar between the two groups (HFPEF: 84 ± 9 vs.HFREF: 82 ± 14, p=0.106). HFPEF patients were significantly more likely to be female (71% vs. 41.5%, p=0.001) and significantly less likely to have ischaemic heart disease (34% vs. 52%, p=0.043). Patients with HFPEF were significantly less likely to be taking loop diuretics, potassium-sparing diuretics, angiotensin-converting enzyme (ACE) inhibitors and aspirin on discharge. Ischaemic heart disease was a significant predictor of mortality in HFPEF patients (hazard ratio [HR] 7.14; 95% confidence interval [CI] 1.51–33.85, p=0.01). There was no difference in readmission and one-year survival rate (p=0.68 and p=0.551, respectively).
In conclusion, HFPEF patients are more likely to be female but less likely to have an ischaemic aetiology. There were significant differences in treatment of both phenotypes. Both groups have a similar poor prognosis.
Introduction
Heart failure is a significant and rising public health problem affecting 900,000 people in the UK, and accounts for 5% of all emergency admissions.1 This rising trend is set to continue as the average age of the population increases.1-3
It is estimated that the proportion of patients with heart failure with preserved ejection fraction (HFPEF) is between 30% and 50%.4-9 As a result, in recent years, more attention has been paid to this cohort of patients. However, there is still limited information regarding outcomes and treatment for these patients.
Previous reports have shown that patients that have HFPEF are more likely to be female, to be older and are less likely to have an ischaemic aetiology than patients who have reduced ejection fraction (HFREF).10 However, many of these studies are based on ambulatory patients. In addition, it has been highlighted that there may be geographical variations in patients with HFPEF.11
There have been conflicting reports as to whether patients with preserved ejection fraction have a greater morbidity and mortality compared with those patients with HFREF. Some studies have reported a similar mortality rate in HFPEF compared with HFREF,4,5,12 whereas a recent meta-analysis showed patients with HFPEF to have a better survival rate.13 Differences in results may be due to different inclusion criteria and follow-up period. In addition, a large proportion of patients (84%) in the meta-analysis (Somaratne et al.) were from clinical trials that were based on ambulatory patients.13
Most previous studies have based their inclusion criteria on ejection fraction (EF) alone. However, the European Society of Cardiology (ESC) guidelines for the diagnosis of HFPEF advocate different criteria: signs and symptoms of heart failure, an EF of more than 50%, relevant structural heart disease and/or evidence of diastolic dysfunction on echocardiography.14,15 To our knowledge, there has not been a previous study comparing outcomes between patients with HFPEF and HFREF based on these guidelines in Northern Europe.
The main aim of our study was to assess the characteristics, treatment and short-term outcome of patients with HFPEF following admission with acute decompensated heart failure compared with those patients with HFREF. Our secondary aim was to evaluate predictors of outcome in these patients. To our knowledge, this is the first analysis of this cohort of patients in Northern Europe and in a district general hospital setting.
Methods
Patient selection
This was a retrospective cohort study. Between 1 January 2012 and 31 December 2012, we identified all patients with a primary discharge diagnosis of heart failure who were admitted to Southend University Hospital NHS Foundation Trust, UK. The diagnosis of heart failure was initially made by the admitting medical team. Outcomes were obtained by reviewing all discharge letters including medication, chest X-rays and echocardiograms. Where there were missing data, patients’ notes were reviewed. Patients who, on reading their discharge letter, did not have diagnosis of heart failure, were excluded. Echocardiography reports were used for analysis if they had been performed within six months before or after the patient’s admission date. Patients were also excluded from analysis if left ventricular ejection fraction (LVEF) had not been evaluated by echocardiography or if they had severe valvular heart disease. Patients were subdivided into two groups, those with reduced EF and preserved EF.
Echocardiography reports
Outcome variables obtained from echocardiography were the presence of pulmonary hypertension, severe valvular heart disease, EF and medial and lateral E/E’. E/E’ ratio was retrospectively calculated in patients who had tissue doppler imaging but initially did not have an E/E’ ratio calculated. Patients with reduced EF were defined as either having a qualitative report of decreased EF or a LVEF less than 50%. Preserved EF patients were defined as having a LVEF more than 50% plus a medial or lateral E/E’ ratio more than 15.
Baseline characteristics
Baseline measurements included age, gender and hospital duration. Patients’ symptoms on admission, including shortness of breath and peripheral oedema, were obtained from discharge summaries. We also obtained patient comorbidities and medication from discharge summaries. The presence of heart failure on admission chest X-rays was obtained from X-ray reports. Where data were missing from discharge summaries these data were collected from patients’ notes.
Follow-up and readmission
Clinical outcomes including readmission to hospital with heart failure and inpatient mortality were recorded using the hospital’s local database. One-year mortality rate was also recorded.
Statistical analysis
The Shapiro-Wilk test was used to check for normality of distribution for continuous variables. Non-normally distributed data (age and hospital duration) are reported as median (± interquartile range [IQR]). Categorical variables are reported as frequency (%).
The Mann-Whitney U-test and Chi-square test were used to examine continuous and categorical outcomes, respectively, between patients with reduced and those with preserved EF.
A Kaplan-Meier curve was constructed to analyse one-year mortality. The log-rank test was used to determine differences in mortality between the two groups. Multi-variate Cox-regression analysis was used to evaluate the effect of independent variables on survival in each group (reduced vs. preserved EF). Variables included age, gender, diabetes, hypertension, ischaemic heart disease, atrial fibrillation and chronic obstructive pulmonary disease (COPD). A p value of less than 0.05 was taken to be statistically significant. All data were analysed using SPSS version 22.
Table 1. Baseline characteristics of patients admitted with heart failure
Ethics
This was a retrospective audit of data and, therefore, did not require ethics approval.16 The study was registered with the local research and audit department (Southend University Hospital NHS Foundation Trust, UK).
Results
Baseline characteristics
In 2012, there were 668 admissions with a definitive diagnosis of heart failure. There were 113 excluded from the analysis as they had not had a recent echocardiogram. In addition, 83 patients were excluded as they had severe valvular heart disease. Of the remaining admissions, 97 were readmissions leaving 375 patients admitted with heart failure. Of these patients, 200 had a reduced EF, 81 patients had preserved EF but no assessment of E/E’, 53 patients had preserved EF and a medial or lateral E/E’ of no more than 15 (42/53 patients had a medial and/or lateral E/E’ between 8 and 15) and, finally, 41 patients had a preserved EF plus a medial and/or lateral E/E’ of more than 15. Thus, a total of 241 patients were included for analysis.
A total of 200 (83%) patients had a reduced EF compared with 41 (17%) who had preserved EF. Table 1 outlines the baseline characteristics of each group. Patients in the reduced EF group were significantly more likely to be male. Both groups had similar signs and symptoms to each other. Patients with reduced EF were significantly more likely to have a history of ischaemic heart disease, however, patients with preserved EF were significantly more likely to have chronic kidney disease.
Hospital duration and readmission rate
The median hospital duration was nine (± 10.8) and seven (± 8) days for patients with reduced and preserved EF, respectively. The distribution of hospital duration was similar across both groups (p=0.397). In the 12 months after discharge, 53 patients with HFREF (27%) and eight patients (20%) with HFPEF were readmitted with an exacerbation of heart failure. There was no significant difference in the readmission rate one year after discharge between each group (p=0.68).
Figure 1. Kaplan-Meier curve for time to all-cause mortality
Survival outcomes
Twenty-four patients (12%) with reduced EF died while an inpatient, whereas four patients (10%) with preserved EF died while an inpatient (p=0.683). Sixty-three patients (32%) with reduced EF and 11 patients (27%) with preserved EF died within one year of admission. Survival was similar between the two groups (log-rank p=0.551) (figure 1).
Predictors of outcome
Predictors of mortality in patients with reduced and preserved EF are shown in table 2. Age and history of ischaemic heart disease were significant predictors of survival in patients with reduced and preserved EF, respectively.
Medications on discharge
Twenty-eight patients were excluded from the medication analysis as they had died as an inpatient. A further two patients were excluded as their medications were not available. Both of these patients were in the reduced EF group. Patients with reduced EF were significantly more likely to be taking loop diuretics, potassium-sparing diuretics, angiotensin-converting enzyme (ACE) inhibitors and aspirin. Patients with preserved EF were significantly more likely to be taking warfarin, calcium-channel blockers and thiazide diuretics.
Table 2. Cox multiple regression analysis for patients with heart failure with reduced ejection fraction (HFREF) and heart failure with preserved ejection fraction (HFPEF)
Discussion
Our study provides new information and confirms previous findings regarding patients admitted to hospital with HFPEF. HFPEF accounts for a significant proportion of hospital admissions. Previous studies have found the proportion of patients with HFPEF to be between 30% and 50%.4-9 Our study showed that only 17% of patients admitted with heart failure had preserved EF. This discrepancy with previous research may be due to the fact that this study had stricter inclusion criteria than previous studies. However, there may also be heterogeneity between hospitals. Patel et al. showed that the proportion of patients with HFPEF was lower in district general hospitals (13.8%) than teaching hospitals (42.4%).17 It has been estimated that the economic burden of these patients is €11,344 per year, with hospital admissions accounting for the majority of the total cost.18
The average age of patients with HFPEF in our study was 84 years. This is older than previous hospital-based studies.9,19-21 This may be attributed to an ever-increasing elderly population. In agreement with previous reports, patients with reduced EF tended to be younger, with an average age of 82 years, and a significantly higher proportion of patients with preserved EF were female.4,9,19-21
There were similarities and differences between the two groups. Although there were similar rates of hypertension, hypercholesterolaemia, atrial fibrillation, diabetes, cerebrovascular accident (CVA), peripheral vascular disease, COPD and dementia; patients with preserved EF were significantly less likely to have an ischaemic aetiology as a cause of their heart failure, however, ischaemic heart disease was a significant predictor of mortality in this group. Patients with HFPEF were significantly more likely to have chronic kidney disease (CKD). This is similar to previous studies: 31%, 49% and 35% of patients in the I-PRESERVE (irbesartan in heart failure with preserved systolic function), DIG-PEF (Digitalis Investigation Group: Preserved Ejection Fraction) and CHARM-preserved (Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity: Preserved) studies had CKD.22 However, our study did not have a strict definition for CKD, although there is no reason that comorbidities were not accurately documented on the discharge letters. Our study did not investigate whether there were differences in stages of CKD between the two groups.
The exact mechanism of HFPEF is still not known and several theories exist. The most popular theory is one of increasing myocardial stiffness, which leads to diastolic dysfunction.23 Diastolic dysfunction may be assessed on echocardiography by measuring the E/E’ ratio. An E/E’ ratio above 15 signifies diastolic dysfunction, however, diastolic dysfunction is not specific to patients who have preserved EF and can also occur in patients who have a reduced EF.23 Other mechanisms for HFPEF include pulmonary hypertension, chronotropic incompetence, resting/exercise-exacerbated systolic dysfunction and aortic stiffness.23-26
Our study included patients with either a medial or lateral E/E’ ratio more than 15, as previous studies have found both to be predictive of diastolic dysfunction and more accurate than taking an average. Ommen et al. showed the medial E/E’ ratio had a better correlation with mean left ventricular diastolic pressure (M-LVDP) than a lateral and average E/E’ ratio.27 Whereas, Shuai et al. showed that a lateral E/E’ yielded greater diagnostic accuracy than either septal or a mean E/E’ ratio.28 The EURO-FILLING (European multicentre validation study of the accuracy of E/E’ ratio in estimating invasive left ventricular filling pressure) study is expected to provide more information and contribute to the standardisation of the assessment of HFPEF in clinical practice.
As of yet, there are no specific treatment guidelines for patients with preserved EF apart from consensus opinion. Randomised-controlled trials have shown neurohumoral antagonists such as beta blockers, ACE inhibitors, and angiotensin II receptor blockers to be effective in the treatment of systolic heart failure, however, they have not been shown to have the same effect in patients with preserved EF.29,30
The efficacy of aldosterone antagonist therapy in patients with HFPEF is uncertain, given the results of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial.31 The trial randomly assigned 3,445 patients with symptomatic heart failure and LVEF ≥45% to receive either spironolactone or placebo. The trial showed no reduction in the composite primary outcome (death from cardiovascular causes, aborted cardiac arrest, or hospitalisation for HF) from spironolactone therapy. However, subgroup analyses suggested regional heterogeneity in patient populations and possible benefit from spironolactone therapy in a subset of patients with a diagnosis of heart failure confirmed by elevated B-type natriuretic protein (BNP) or N-terminal (NT)-proBNP levels.
Our study showed that patients with preserved EF received significantly less ACE inhibitors, loop diuretic and potassium-sparing diuretics than patients with reduced EF. This is similar to previous studies.4,12,31 Patients with HFPEF were significantly more likely to be taking warfarin. This is surprising, as more patients with reduced EF had atrial fibrillation. There may be other factors responsible for this result, e.g. bleeding risk. In our institution, patients with HFREF are referred to the community heart failure team for further management, whereas, as yet, HFPEF patients are not. There is scope to include HFPEF patients within the specialist heart failure team.
In agreement with previous studies, we also found that there was no significant difference in the duration of hospital stay when compared with patients with reduced EF.4,9,12,32
Our study showed that there was also no significant difference in the hospital readmission rate between patients with preserved and reduced EF. The one-year survival rate was better for patients with preserved EF, although this was not statistically significant. Our results are in agreement with some,4,12,32,33 but not all previous reports. Lenzen et al. reported that patients with systolic dysfunction had a significantly higher mortality than patients with preserved EF.9 The differences in results observed may be due to the different criteria for diagnosing HFPEF. We used an EF >50% and evidence of diastolic dysfunction, whereas Lenzen et al. used 40%. In addition, we checked for one-year survival, whereas Lenzen et al. had a shorter follow-up of 12 weeks.9 Our findings confirm the need for more trials to improve the prognosis of patients with HFPEF.
Limitations of the study
As with any retrospective study, there are also limitations in our study. First, there were only 241 patients admitted with heart failure within our period of study. This is fewer than previous studies and, therefore, raises the possibility of type two statistical errors occurring in both groups. In addition, 81 patients were excluded from the audit, as they did not have an assessment of E/E’. Also, 42 patients had a medial and/or lateral E/E’ between 8 and 15. It is likely more patients would have met the ESC definition for HFPEF if NT-proBNP or BNP levels were assessed in addition to left ventricular mass index and left atrial volume index.14,15 It is possible that we have underestimated the incidence of HFPEF.
In our study, the degree of left ventricular systolic dysfunction, i.e. mild, moderate or severe, was not taken into account in patients with HFREF, which makes it hard to accurately compare the outcomes, based purely on preserved or reduced EF.
In addition, as with previous articles, the differences in definitions for HFPEF makes it difficult to directly compare our results with previous studies.
Finally, there is the possibility of further underestimating the number of patients who had HFPEF. We included patients who had a definitive diagnosis of heart failure on discharge, however, it is possible that some patients were not diagnosed with heart failure once it was known they did not have reduced EF on echocardiography. This may particularly be true for patients not admitted to a cardiology ward.
Conclusion
In conclusion, our study confirms previous findings regarding patients with preserved EF, but also provides new information. Our study showed that patients with heart failure are older than previously thought, this is true for patients with reduced and preserved EF. Patients with preserved EF were less likely to have ischaemic aetiology. There was no difference in the readmission and survival rate between patients with preserved and reduced EF. The prognosis of heart failure with preserved EF is poor; more larger cohort studies are needed to better understand these patients, especially in older populations. More randomised-controlled trials are needed to improve treatment modalities for these patients.
Key messages
Heart failure with preserved ejection fraction (HFPEF) is a rising health problem, but limited information regarding outcomes and treatment is known about these patients
HFPEF patients are generally older and less likely to have an ischaemic aetiology compared with patients with heart failure with reduced ejection fraction (HFREF)
HFPEF patients carry a similar poor prognosis to HFREF patients
Larger prospective studies based on European Society of Cardiology (ESC) guidelines are needed to confirm our findings
Funding
None.
Conflict of interest
None declared.
Editors’ note
A table showing comparison of medications between HFREF and HFPEF groups on discharge is available on request. email: editorial@bjcardio.co.uk
1. National Institute for Health and Care Excellence. Chronic heart failure. Management of chronic heart failure in adults in primary and secondary care. CG108. London: NICE, August 2010. Available from: http://www.nice.org.uk/cg108
2. Stewart S, Horowitz JD. Home-based intervention in congestive heart failure: long-term implications on readmission and survival. Circulation 2002;105:2861–6. http://dx.doi.org/10.1161/01.CIR.0000019067.99013.67
4. Berry C, Hogg K, Norrie J, Stevenson K, Brett M, McMurray J. Heart failure with preserved left ventricular systolic function: a hospital cohort study. Heart 2005;91:907–13. http://dx.doi.org/10.1136/hrt.2004.041996
5. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006;355:251–9. http://dx.doi.org/10.1056/NEJMoa052256
7. Tribouilloy C, Rusinaru D, Mahjoub H et al. Prognosis of heart failure with preserved ejection fraction: a 5 year prospective population-based study. Eur Heart J 2008;29:339–47. http://dx.doi.org/10.1093/eurheartj/ehm554
8. Varela-Roman A, Grigorian L, Barge E, Bassante P, de la Pena MG, Gonzalez-Juanatey JR. Heart failure in patients with preserved and deteriorated left ventricular ejection fraction. Heart 2005;91:489–94. http://dx.doi.org/10.1136/hrt.2003.031922
9. Lenzen MJ, Scholte op Reimer WJ, Boersma E et al. Differences between patients with a preserved and a depressed left ventricular function: a report from the EuroHeart Failure Survey. Eur Heart J 2004;25:1214–20. http://dx.doi.org/10.1016/j.ehj.2004.06.006
10. Campbell RT, Jhund PS, Castagno D, Hawkins NM, Petrie MC, McMurray JJ. What have we learned about patients with heart failure and preserved ejection fraction from DIG-PEF, CHARM-preserved, and I-PRESERVE? J Am Coll Cardiol 2012;60:2349–56. http://dx.doi.org/10.1016/j.jacc.2012.04.064
11. West R, Liang L, Fonarow GC et al. Characterization of heart failure patients with preserved ejection fraction: a comparison between ADHERE-US registry and ADHERE-International registry. Eur J Heart Fail 2011;13:945–52. http://dx.doi.org/10.1093/eurjhf/hfr064
12. Gotsman I, Zwas D, Lotan C, Keren A. Heart failure and preserved left ventricular function: long term clinical outcome. PLoS One 2012;7:e41022. http://dx.doi.org/10.1371/journal.pone.0041022
13. Somaratne JB, Berry C, McMurray JJ, Poppe KK, Doughty RN, Whalley GA. The prognostic significance of heart failure with preserved left ventricular ejection fraction: a literature-based meta-analysis. Eur J Heart Fail 2009;11:855–62. http://dx.doi.org/10.1093/eurjhf/hfp103
14. McMurray JJ, Adamopoulos S, Anker SD et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012;14:803–69. http://dx.doi.org/10.1093/eurjhf/hfs105
15. Paulus WJ, Tschöpe C, Sanderson JE et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J 2007;28:2539–50. http://dx.doi.org/10.1093/eurheartj/ehm037
17. Patel H, Hayward C, di Mario C, Cowie M, Lyon A, Rosen S. 64 Heart failure with preserved ejection fraction: are the current definitions too strict? Heart 2014;100(suppl 3):A36. http://dx.doi.org/10.1136/heartjnl-2014-306118.64
18. Stålhammar J, Stern L, Linder R et al. The burden of preserved ejection fraction heart failure in a real-world Swedish patient population. J Med Econ 2013;17:43–51. http://dx.doi.org/10.3111/13696998.2013.848808
19. Masoudi FA, Havranek EP, Smith G et al. Gender, age, and heart failure with preserved left ventricular systolic function. J Am Coll Cardiol 2003;41:217–23. http://dx.doi.org/10.1016/S0735-1097(02)02696-7
20. Fonarow GC, Stough WG, Abraham WT et al. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: a report from the OPTIMIZE-HF Registry. J Am Coll Cardiol 2007;50:768–77. http://dx.doi.org/10.1016/j.jacc.2007.04.064
21. Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC, Investigators ASACa. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J Am Coll Cardiol 2006;47:76–84. http://dx.doi.org/10.1016/j.jacc.2005.09.022
22. McMurray JJ, Carson PE, Komajda M et al. Heart failure with preserved ejection fraction: clinical characteristics of 4133 patients enrolled in the I-PRESERVE trial. Eur J Heart Fail 2008;10:149–56. http://dx.doi.org/10.1016/j.ejheart.2007.12.010
23. Borlaug BA, Paulus WJ. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur Heart J 2011;32:670–9. http://dx.doi.org/10.1093/eurheartj/ehq426
24. Phan TT, Shivu GN, Abozguia K et al. Impaired heart rate recovery and chronotropic incompetence in patients with heart failure with preserved ejection fraction. Circ Heart Fail 2010;3:29–34. http://dx.doi.org/10.1161/CIRCHEARTFAILURE.109.877720
25. Lam CS, Roger VL, Rodeheffer RJ, Borlaug BA, Enders FT, Redfield MM. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J Am Coll Cardiol 2009;53:1119–26. http://dx.doi.org/10.1016/j.jacc.2008.11.051
27. Ommen SR, Nishimura RA, Appleton CP et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation 2000;102:1788–94. http://dx.doi.org/10.1161/01.CIR.102.15.1788
28. Shuai XX, Chen YY, Lu YX et al. Diagnosis of heart failure with preserved ejection fraction: which parameters and diagnostic strategies are more valuable? Eur J Heart Fail 2011;13:737–45. http://dx.doi.org/10.1093/eurjhf/hfr053
29. Oghlakian GO, Sipahi I, Fang JC. Treatment of heart failure with preserved ejection fraction: have we been pursuing the wrong paradigm? Mayo Clin Proc 2011;86:531–9. http://dx.doi.org/10.4065/mcp.2010.0841
30. Pitt B, Pfeffer MA, Assmann SF et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 2014;370:1383–92. http://dx.doi.org/10.1056/NEJMoa1313731
31. Pitt B, Pfeffer MA, Assmann SF et al.; TOPCAT Investigators. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 2014;370:1383–92. http://dx.doi.org/10.1056/NEJMoa1313731
32. Gotsman I, Zwas D, Planer D et al. Clinical outcome of patients with heart failure and preserved left ventricular function. Am J Med 2008;121:997–1001. http://dx.doi.org/10.1016/j.amjmed.2008.06.031
33. Bhatia RS, Tu JV, Lee DS et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med 2006;355:260–9. http://dx.doi.org/10.1056/NEJMoa051530
Delays in achieving target international normalised ratio (INR) with warfarin after cardiac surgery can lead to suboptimal outcomes. The aims of the study are to determine the difference in warfarin dosage requirements, before and after cardiac surgery, needed to achieve therapeutic anticoagulation.
A single-centre, retrospective review was conducted from 2012 to 2014 in cardiac surgery patients who were on warfarin pre-operatively and who had warfarin therapy resumed postoperatively in hospital. The primary outcome was the difference in warfarin dosage needed to achieve target INR before and after cardiac surgery.
Ninety-five patients were included in the study. The mean daily postoperative warfarin dose needed for achieving a therapeutic INR was 0.18 mg lower than the mean pre-operative dose (5.03 ± 2.10 vs. 4.85 ± 2.25 mg; p=0.358).
In conclusion, there was no statistically significant difference in the warfarin dosage before and after cardiac surgery needed to achieve target INRs.
Introduction
Warfarin is an anticoagulant commonly used in atrial fibrillation, venous thromboembolism, prosthetic cardiac valve replacement and postoperative atrial fibrillation.1 Warfarin is usually discontinued prior to cardiac surgery and subsequently re-initiated postoperatively to achieve the target therapeutic international normalised ratio (INR).2 At the cardiac surgery unit of St. Paul’s Hospital, it has been observed that the warfarin dosage needed to achieve therapeutic anticoagulation is often lower post-cardiac surgery, compared with the patient’s warfarin dose prior to cardiac surgery. Serious complications, such as postoperative thromboembolic and haemorrhagic events, are consequences of the cardiac surgery itself and under- and over-anticoagulation.3,4 It is important to optimise anticoagulation in post-cardiac surgery patients, and delays can lead to prolonged hospitalisations due to the above complications.5
No studies have been published that quantify the difference, if any, in warfarin dosage needed to achieve therapeutic INR, specifically, before and after cardiac surgery. The purpose of this study is to determine if there is a difference in warfarin dosage before and after cardiac surgery needed to achieve therapeutic anticoagulation.
Methods
Design
This single-centre, retrospective chart review was approved by the Providence Health Care Research Ethics Board and by the Fraser Health Research Ethics Board (Providence Health Care Reference number UBC PHC H13-02182). The need for informed consent was waived.
Population
Eligible patients were identified through the pharmacy database and patient chart reviews. Patients were included if they were admitted to St. Paul’s Hospital for cardiac surgery between 1 February 2012 and 4 February 2014, were on warfarin prior to cardiac surgery and achieved therapeutic anticoagulation, had warfarin therapy resumed postoperatively in hospital, and achieved INRs within the therapeutic range (as appropriate for the indication for warfarin) during hospitalisation. Exclusion criteria were: warfarin use for less than two months prior to the cardiac surgery date; undocumented or unclear pre-operative warfarin dose; postoperative warfarin therapy lasting less than five days prior to discharge; postoperative admission to the intensive care unit (ICU).
Outcomes
The primary outcome was the difference in warfarin dose, before and after cardiac surgery, required to achieve and maintain the patient’s target INR. The target INR was defined as the therapeutic target INR based on the patient’s indication for anticoagulation postoperatively. The secondary outcomes were the rates of major and minor bleeding and thromboembolic events during the postoperative hospitalisation period. Major bleeding events were defined as those that were intracranial or retroperitoneal, led to death, necessitated transfusion, warranted interruption of antithrombotic treatment, or required operation. All other haemorrhagic events documented in the patient charts were considered to be minor bleeding events. Thromboembolic events were defined as ischaemic stroke, transient ischaemic attack, systemic embolism, deep vein thrombosis, pulmonary embolism, or cardiac valve thrombosis.
For the primary outcome analysis, the postoperative warfarin dose required to achieve and maintain a therapeutic INR was determined by averaging the doses from the day warfarin was initiated post-operatively until the day that a therapeutic INR was achieved. The pre-operative warfarin dose was obtained from chart records of the patient’s home warfarin dose prior to cardiac surgery.
Statistical analysis
The pre-operative and postoperative maintenance warfarin doses were compared using the paired samples t-test; p values less than 0.05 were considered to be statistically significant. Descriptive statistics were used to analyse the secondary outcomes of bleeding and thromboembolic event rates.
Results
There were 1,402 patients screened, of which 95 were eligible for the study. The majority of patients received coronary artery bypass graft surgery. Warfarin therapy was restarted after a median of one day postoperatively, and the median postoperative length of stay was nine days.
The 95 patients achieved a therapeutic INR after a median of five postoperative days. The overall mean postoperative maintenance warfarin dose was 0.18 mg lower than the pre-operative dose (5.03 ± 2.10 vs. 4.85 ± 2.25 mg) and this difference was not statistically significant (p=0.358). Similarly, no statistically significant differences in warfarin dose were found in any of the subgroups, which were defined by cardiac surgery type and by whether warfarin-interacting medications or products were initiated pre-operatively (see table 1).
Table 1. Primary outcome (n=95)
Four patients (3.6%) had one major bleeding event postoperatively during their hospital stay. At the time of the major bleeding events, none of the four patients had supratherapeutic INRs. Half (50%) of major bleeds also occurred in patients taking three or more antithrombotic agents in addition to warfarin, whereas all patients with no bleeding events or minor bleeding events were taking two or fewer concomitant antithrombotic agents. Ten minor bleeding events occurred overall and the INRs were supratherapeutic at the time of only two of these events.
Three patients (2.7%) had one thromboembolic event and all events were ischaemic strokes. In two of these patients, the INR was subtherapeutic at the time of the stroke, and the INRs had been consistently subtherapeutic for the previous three and six days prior to the event.
Discussion
This is the first study undertaken to determine the changes in warfarin dosage requirements, specifically, before and after cardiac surgery. In the postoperative setting, practitioners rely heavily on frequent INR monitoring, patients’ past warfarin dosage requirements and on the patient’s history of bleeding and thromboembolic events to guide warfarin dosage adjustments. No statistically or clinically significant difference in warfarin dosage requirements was found overall, or in any of the subgroups.
Although no previous studies have quantified changes in warfarin dosage requirements after cardiac surgery, alterations in warfarin response in the postoperative period have been reported. A study by Schulman et al. examined postoperative changes in warfarin response among general surgical patients, 156 of which had received cardiac surgery.6 Warfarin responses after cardiac surgery were classified as altered in 34% of patients: resistant in 19%, and sensitive in 15%.6 However, Schulman et al.’s criteria for warfarin responsiveness classifications were not clearly defined. Of the clinical factors studied, postoperative commencement of amiodarone was the only factor identified to influence warfarin responses to a statistically significant degree. 6 This effect of concomitant amiodarone use was reproduced in our study as well.
Studies by Rahman et al. and Lee et al. showed that patients receiving heart valve replacements had decreased warfarin requirements immediately following the surgery.7,8 The authors concluded that the differences were attributed to postoperative physiological changes, such as improvements in cardiac function, with consequent decreases in fluid retention, relief of hepatic congestion, increases in warfarin metabolism, the deleterious effect of cardiopulmonary bypass (CPB) on clotting factors that worsens as the CPB time is prolonged, and hypoalbuminaemia following CPB, which affects warfarin’s half-life and volume of distribution.8,9 Such physiological changes post-cardiac surgery did not translate into any clinical difference in warfarin dosage needed to achieve therapeutic anticoagulation in our study.
Peri-operative bleeding events are of particular concern in cardiac surgery patients.10 Our results suggest that major bleeding events in this study may have been associated with the number of concomitant antithrombotics administered. The INRs were subtherapeutic at the time of the majority of bleeding events, which suggests that the intensity of anticoagulation with warfarin may not be a primary factor associated with the bleeding events, but perhaps the number of antiplatelet and anticoagulants are.
Our study has a number of limitations. The largest limitation was the retrospective nature of the study. Important factors may not have been detected by our retrospective review, such as undocumented bleeding or thromboembolic events, as well as factors that affect warfarin response, such as dietary vitamin K intake, gut malabsorption and liver dysfunction. Our study was also limited by its small sample size, which may have contributed to the lack of statistical significance detected among the analyses. As well, while our study demonstrates that therapeutic anticoagulation was achieved using pre-operative warfarin dosages, it is unclear if this would translate to long-term therapeutic anticoagulation. This would be more difficult to determine as the times in therapeutic range with warfarin vary depending on the anticoagulation care available, ranging from 29% to 75% in outpatient atrial fibrillation patients.11
As well, our findings are only applicable to our institution and, possibly, post-cardiac surgery patients in general, as hospital diet composition varies greatly between hospitals. Other factors, such as cultural preferences for certain types of food and the ability to tolerate an oral diet, would affect dietary intake of vitamin K. This variability in dietary intake of vitamin K post-operatively would influence the warfarin dosage needed to achieve therapeutic anticoagulation. Thus, we would not be able to extrapolate our findings to other hospitalised patients or other institutions given the great variability in dietary vitamin K intake. Further studies should be undertaken to validate our findings in other surgical and hospitalised patient populations in different institutions.
The fact that our study demonstrated no difference in warfarin dosage needed for therapeutic anticoagulation pre-operatively and postoperatively raises some interesting mechanistic questions. Other factors postoperatively, such as an increased inflammatory state, effect of an acutely stressed physiological state on clotting factors and intra-operative anticoagulation may influence dose-responsiveness to warfarin postoperatively. Future mechanistic studies are warranted to elucidate the physiologic factors post-cardiac surgery that would impact warfarin dose-responsiveness.
Conclusion
In conclusion, there were no statistically significant differences in warfarin dosage needed to achieve therapeutic INR, before and after cardiac surgery. The majority of recorded bleeding and thromboembolic events occurred while the INR was subtherapeutic. As the study was limited by its retrospective nature and small sample size, larger prospective studies are warranted to validate these findings.
Key messages
Delays in achieving therapeutic anticoagulation with warfarin after cardiac surgery can lead to prolonged hospitalisation and potential for thromboembolism
Cardiac surgery can cause physiological changes that may alter the body’s response to anticoagulation
This study illustrates that the warfarin dose needed to achieve therapeutic anticoagulation after cardiac surgery is similar to pre-operative warfarin dosage requirements
Patients will likely require similar warfarin dosages postoperatively compared with pre-operatively to achieve therapeutic anticoagulation
Acknowledgements
We acknowledge Jessica Chang, BSc(Pharm), and Flora Yu, BSc(Pharm), for assistance in the data collection for this study.
2. Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuünemann HJ. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th edition. American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2012;141(2 suppl):7S–47S. http://dx.doi.org/10.1378/chest.1412S3
3. Irwin AN, McCool KH, Delate T, Witt DM. Assessment of warfarin dosing requirements after bariatric surgery in patients requiring long-term warfarin therapy. Pharmacotherapy 2013;33:1175–83. http://dx.doi.org/10.1002/phar.1307
4. Zareh M, Davis A, Henderson S. Reversal of warfarin-induced hemorrhage in the emergency department. West J Emerg Med 2011;12:386–92. http://dx.doi.org/10.5811/westjem.2011.3.2051
5. Gulseth M. Managing Anticoagulation Patients in the Hospital: The Inpatient Anticoagulation Service. Bethesda (MD): American Society of Health-System Pharmacists (ASHP), 2007.
6. Schulman S, El Bouazzaoui B, Eikelboom JW, Zondag M. Clinical factors influencing the sensitivity to warfarin when restarted after surgery. J Intern Med 2008;263:412–17. http://dx.doi.org/10.1111/j.1365-2796.2007.01913.x
7. Rahman M, BinEsmael TM, Payne N, Butchart EG. Increased sensitivity to warfarin after heart valve replacement. Ann Pharmacother 2006;40:397–401. http://dx.doi.org/10.1345/aph.1G407
8. Lee J, Lee B, Kim K et al. Factors affecting warfarin therapy following cardiac valve surgery. Ann Pharmacother 2002;36:1845–50. http://dx.doi.org/10.1345/aph.1A431
9. Harker LA, Malpass TW, Branson HE, Hessel EA, Slichter SJ. Mechanism of abnormal bleeding in a patient undergoing cardiopulmonary bypass: acquired transient platelet dysfunction associated with selective alpha-granule release. Blood 1980;56:824–34.
10. Tettey M, Aniteye E, Sereboe L et al. Predictors of post operative bleeding and blood transfusion in cardiac surgery. Ghana Med J 2009;43:71–6.
11. Wan Y, Heneghan C, Perera R et al. Anticoagulation control and prediction of adverse events in patients with atrial fibrillation. Circ Outcomes 2008;1:84–91. http://dx.doi.org/10.1161/CIRCOUTCOMES.108.796185
Conducting clinical research is an ambition of many cardiologists and academic clinicians. Over the last decade, the National Health Service (NHS) has indicated that research is a clear priority in improving healthcare for patients. The processes leading to permission to start a clinical trial in the UK are, however, poorly understood, labyrinthine and fraught with difficulty. In this article, we aim to share our knowledge of initiating a clinical trial using a case study, with a focus on the essential documents and the communication required with different organisations.
Introduction
During 2014, one of us (AK) had a four-month research placement in the academic foundation programme. The aim was to create and conduct a clinical trial in heart failure. Although the trial was successful, the success was only achieved through motivation, organisation, good communication and luck. Because of the hurdles now placed between investigator and study, planning between supervisor and trainee started over a year in advance to discuss the idea for the trial, draft the study protocol, and complete all the documents required. The full timeline of events from conception to completion spanned 336 days. The aim of this article is to share the experience and help other clinicians understand the process of obtaining approval to carry out clinical research.
Conducting a clinical trial in the UK is certainly not an easy task (see figure 1). There are numerous points in the development of a study where it may fail: from funding and logistics to ethics committee approval and patient enrolment. In order to obtain approval, an application needs to be made to multiple organisations, each in turn requiring effective communication to prevent delay in a lengthy process.
Figure 1. The complexity of a clinical trial: good practice requirements in blue and legal requirements in red. An informative pathway found on www.ct-toolkit.ac.uk/routemap
Although the government has made medical research and innovation a priority of NHS England following publication of the policy paper Creating Change: innovation, health and wealth one year on,1 with the focus on improving the quality, and, particularly, the ease of carrying out research in the UK, the experience of academics and clinicians in applying for approval to conduct clinical research is time-consuming and fraught with difficulties.
Applications and documents
To obtain approval for a clinical trial there are a number of applications and documents required:
Protocol, Medicines and Healthcare Products Regulatory Agency (MHRA) application
Research & Ethics Committee (REC) application
Research & Development (R&D) application
Site Specific Information (SSI) application
Summary of Product Characteristics (SmPC)
Patient information sheet
Consent form
Case Report Form (CRF).
Case clinical trial
(EudraCT: 2014-003380-38)
The trial conducted was a randomised, single-blinded, cross-over study involving 31 participants with heart failure at a well-established research site in the UK. The only drug used was oxygen (room air, 28% and 40%), delivered via Venturi, while patients exercised using a cycle ergometer weekly over three visits. The main outcomes were exercise time, and peak metabolic equivalent (MET) and workload reached. Secondary outcomes were heart rate, blood pressure and oxygen saturation during exercise.
We found that increasing fraction of inspired oxygen (FiO2) to 28 or 40% acutely improves exercise capacity in patients with chronic heart failure. Increasing FiO2 also resulted in higher oxygen saturation during exercise. The heart rate during each stage of exercise was lower with FiO2 of 28% with no further drop at 40%. Changing FiO2 had no effect on blood pressure.
The trial was completed in a timely manner without any participants having noticed any ill effects during or following the study.
Relevant bodies
There are a number of relevant bodies in clinical research:
Integrated Research Application System (IRAS)
Medicines and Healthcare products Regulatory Agency (MHRA)
Research and Development (R&D) department of the NHS Trust
Research and Ethics Committee (REC).
Protocol
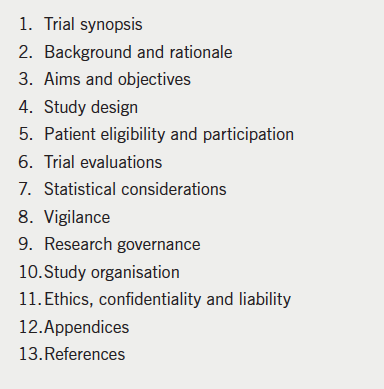
Table 1. Contents of a clinical trial protocol
The protocol is the core document in a clinical trial, and was approximately 25 pages long in the case study (table 1). It focuses on the study objectives, design and safety measures. The protocol requires a full literature review to provide evidence for the study’s relevance. A key aspect of the protocol is safety reporting: it must be stated how and when adverse effects will be reported. Consideration must also be given to where the data will be stored.
The principle of the protocol is that on reading, one is fully aware of the clinical relevance and how to conduct the study. A key feature of the protocol is that it must be readily understandable to the reader in its entirety.
A robust protocol makes the process of applying for approval from the relevant bodies via the Integrated Research Application System (IRAS) system much more straightforward. It is the document that contains most of the information required by the relevant organisations.
In our case study, the protocol took nine major drafts and eight months before being ready for submission. During this time, there were several informal discussions with both R&D and the MHRA, ensuring that modifications to the design could be made at a (relatively) early stage (see figure 2).
Figure 2. The case trial timeline, intervals are in days
Integrated research application system (IRAS)
The IRAS was launched in 2008. It is an online database, which underpins (and purportedly streamlines) the application process for submission to the relevant bodies. It is both free and simple to create an account. The application starts with a number of filter questions to identify the most appropriate application pathway for the investigating team to follow. It is essential to fill out the preliminary section correctly. IRAS receives applications to conduct a wide variety of studies ranging from audits, questionnaire-based research, physiological research, trials involving medicinal products, trials working with human tissue and gene therapy. While there is significant overlap between some of these, specific considerations pertaining to the trial will need to be made. The IRAS filter ensures that only the relevant sections of the total application process are completed by the investigating team.
Once the filter questions are completed, the online application is left open as a project for the investigating team to complete and submit. There is a wealth of documentation and support available on the website, which includes a contacts list page, FAQ and an e-learning module to become more accustomed with using the system.
If there is doubt as to the classification of a trial, it is helpful to discuss the issues with organisations such as the MHRA and local R&D department. These groups are experienced in the development of clinical studies, and will help reduce the risk of an incorrect application being made in an already lengthy process.
Even though the system automatically completes questions which overlap with the demands of other organisations, such as the REC and MHRA, the IRAS application is burdensome. For the case study trial, the application was 46 pages long and had 160 questions to be answered. Once an application to the relevant body is ready for submission, it must be electronically signed by both the principal investigator and representative of the sponsor. An important note is that any change to a data entry point on the application subsequently invalidates the signatures and means the document requires re-signing.
International registry
It is becoming increasingly important to place a clinical trial in an international registry and is expected on submission to the MHRA and R&D. If you are applying for funding, trial registration is regarded as essential. A EudraCT number can be obtained relatively simply, website: https://eudract.ema.europa.eu
Funding
Obtaining external funding for a clinical trial requires a long application process in itself. Funds are needed to pay for the time, equipment, travel and services associated with a clinical trial. Each potential organisation has different requirements and expectations that have to be met. Most of the documentation needed is similar (but not, of course, identical) to that required by the relevant bodies for trial approval.
Our study was internally funded by the Academic Cardiology department, avoiding the need to raise external monies.
Sponsor
A sponsor is required for a clinical trial to take place. It can be an investigator, individual(s) or organisation.
The sponsor takes responsibility for indemnity and liability. The sponsor rarely funds the study; instead conducts a full review of all the documentation during the early phases of the trial. The sponsor also confirms that the relevant documentation has been completed and monitors the study, particularly in regard to safety reporting. In addition, they ensure that good clinical practice is followed throughout.
In our study, the sponsor was the Trust Research & Development department. This was approved following review of the protocol, evaluation of the investigating team (including CVs) and agreement of costings.
Good Clinical Practice (GCP)
The investigators in any clinical study must comply with Good Clinical Practice2 and should, thus, hold valid GCP training certificates. GCP training is helpful in understanding how a clinical trial should be conducted, along with the responsibilities of the relevant bodies and investigating team.
MHRA
All studies involving medicines require authorisation from the MHRA. The MHRA is responsible for the clinical safety of trials and undertakes a thorough review of a study design before approval. An application to the MHRA costs £250 with a subsequent charge of £250 for each substantial amendment made to the application.
A study can be divided into types A, B and C, depending upon the level of risk. Type A trials do not carry increased risk to patients, as compared with usual medical care. Type B and C studies carry somewhat higher risk to patients. It can be unclear as to the level of risk that is appropriate for a given study, which affects the submission. Oxygen, as in our case study, presented an ‘unclear risk’, requiring multiple conversations with the MHRA for agreement on its classification.
Type A trials can be submitted to the MHRA under the notification scheme. Research in this category often investigates the effects of medication under licenced indications or unlicensed but common practice. The notification scheme allows fast-track applications for appropriate low-risk studies. An application under the scheme does not incur the standard fee of £250.
We were eventually successful in obtaining approval for the study from the MHRA under the notification scheme.
Trust Research & Development department (R&D)
Trials in the UK are usually conducted on NHS property, which means that the Trust R&D department often acts as both the monitor and sponsor. The R&D department is answerable to the Health Research Authority with regards to the conduct and documentation of the study.
The R&D department plays a crucial role in the development and approval of a study. In the case study, the R&D department reviewed all documentation before submission to the REC and MHRA. This approach required intensive communication between us and the R&D department, but was helpful in obtaining relatively quick approval through identifying potential issues early.
After trial approval, the R&D department remains involved as monitor. A mid-trial assessment is usually carried out to review the safety and conduct of the study. A debrief is necessary to close the trial with a subsequent archiving procedure.
Research and Ethics Committee (REC)
A national system has seen a reduction in the number of individual RECs. The more centralised system reduces variability between RECs, but has introduced delay in many cases. The quality of REC review is said to be better. The role of the REC is to ensure that the safety, dignity and health of the participants in the prospective study are not disproportionately compromised. The REC is answerable to the Health Research Authority (HRA) for its conduct.
The current system, akin to choose-and-book, allows the principal investigator to select the most appropriate centre from approximately 80 in the UK. Individual REC meetings are conducted only a few times a year, and so the nearest REC might not be the most appropriate for gaining approval rapidly. Furthermore, committee members have up to 60 days per submission to give an opinion. The majority of studies require amendments before a favourable opinion is obtained.
Most centres will make an assessment of a study in the absence of the investigating team; some have teleconferencing facilities available; a few may regard the presence of the investigators as being more-or-less mandatory.
There are five potential outcomes following a REC meeting for a clinical study:
Full favourable opinion for the study to proceed.
Favourable opinion with clarifications required.
Likely favourable opinion following a review of the submitted clarifications by a REC sub-committee.
Possible favourable opinion following a review of the submitted clarifications by a full REC committee.
Not approved as a clinical study, usually due to problems with core aspects of study concept or design.
It is usually at this point that many trials stagnate. It is extremely rare for a trial to obtain approval on its first review with the REC; it often takes many months before full approval is given.
In the submission of our case study, the first decision was that minor clarifications should be made. It took 33 days from submission to obtaining REC approval.
Site Specific Information (SSI)
An SSI form has to be completed for trials taking place on NHS premises. The form is short compared with the others described above, but it requires the investigating team to estimate the amount of time that will be spent on the study, with a focus on the logistics and the potential effects on existing service provision. The SSI form is usually reviewed by the Trust R&D department.
Further permissions are usually required from the clinical and managerial leads in the relevant specialty for approval to be given. Some Trusts also require internal peer-review of a study, even after approval has been obtained from all the other bodies.
Other key documents
Summary of Product Characteristics (SmPC): An approved legal document required for medicinal products prior to authorisation. The SmPC is freely available and contains the posology of the drug. The MHRA requires a copy of the SmPC with submission.
Patient information sheet (PIS): A document written in easily understood language for potential participants in the study. It describes the trial procedures and any risks of the study. The REC pays particularly close attention to the quality of the PIS.
Consent form: A structured form for participants to give their official consent to taking part in the study. The REC and R&D department review the quality of the consent form very closely.
Case Report Form (CRF): The document used to record the data for the study. A well-designed CRF ensures that participants meet eligibility criteria and are properly consented. It makes it straightforward to record all the data required for the study. A poorly constructed CRF causes visits to become inefficient, allows incomplete or inaccurate results to be recorded and at worst can invalidate a study.
Key learning points
Obtaining approval for conducting clinical research is an extremely lengthy endeavour. The process makes a four-month term in research almost useless, unless you begin the application process at least nine months in advance of a trial’s expected start date. You will need more than a year if you are applying for external funding.
Work closely with the relevant organisations, particularly the R&D department of your Trust, the REC and the MHRA to prevent avoidable errors and delay.
A robust study protocol is essential for a successful application and trial.
Be guided by your academic supervisor: his/her advice is invaluable.
Complete the online or face-to-face GCP course offered by the NIHR. It improves your understanding of clinical research. Successful completion of a GCP course is mandatory for those conducting clinical trials.
Be ready to learn. You will acquire many skills during the application process: patience and endurance; effective communication and time management; critical appraisal; appreciation of ethical issues and patient safety.
To be successful, the investigators have to communicate their capacity to manage potential complications, complete the trial and present the results of a relevant, well-designed study.
The future
The biggest losers in the current complex application process for clinical research approval are potential investigators who want to conduct studies without industry support.3 The effect this has had for patients is immeasurable.
In response to the complexities of the current system, the R&D submission is currently being modified into a single process called ‘HRA approval’.4 We hope that HRA approval will streamline applications further to reduce delays in approving suitable trials. The new programme will place more emphasis on obtaining expert opinion earlier, particularly in regard to safety for participants. We hope that the changes will, at least partially, reverse the long-term decline in clinical research in the UK.
Key messages
Organising a clinical study is both complex and lengthy
With improvements on the horizon, the process may become simpler
The most recent innovations in cardiorenal medicine and the challenges this specialty faces in the near future were the focus of the 10th Annual Scientific Meeting of the Cardiorenal Forum. The meeting was held at The Royal College of Obstetricians and Gynaecologists, London, on October 1st 2015, and endorsed by the Renal Association and the British Society for Heart Failure. Drs Thomas Gilpin and Amanda Laird report on its highlights.
Acute heart failure
The first of the clinical heart failure sessions, delivered by Professor Theresa McDonagh (King’s College Hospital, London), considered the definition of acute heart failure (AHF) and how this has been simplified over recent years from a minefield of overlapping statements set out in 2008. Acute hypertensive heart failure, acutely decompensated chronic heart failure, acute coronary syndrome (ACS) and heart failure, right heart failure – amongst other terminology – have now been categorised into:
‘puffers’ – pulmonary oedema, fluid distribution error and
‘bloaters’ – peripheral oedema with genuine fluid overload.
Whilst this new terminology is broad and possibly ambiguous, it is anticipated that this basic categorisation will lead to a simplification of acute management and more streamlined care. There is a limited evidence base for the management of acute heart failure and the traditional management has altered very little. However, there is an emphasis on the detection and early management of hypoxia in patients presenting in pulmonary oedema.
The 2014 National Institute for Heath and Care Excellence (NICE) guidelines for acute heart failure (CG187) downgraded a number of treatments, which had previously been used without evidence base. These are now recommended only for certain situations:
Opiates should only be considered if the patient has severe anxiety or distress.
Continuous positive airways pressure (CPAP) and non-invasive ventilation (NIV) should not routinely be used but reserved for those in whom initial medical therapies have failed. NIV can be considered acutely in those with cardiogenic pulmonary oedema and acidaemia. In patients with respiratory failure, reduced conscious level and exhaustion intermittent positive pressure ventilation (IPPV) should be considered.
Diuretics (for ‘bloaters’) were shown in a 2005 Cochrane Library review by Salvador et al. (doi: 10.1002/14651858.CD003178.pub3) to have superiority when a continuous loop diuretic was infused rather than intermittent intravenous boluses. Loop diuretics remain the mainstay of AHF management through initial vasodilator effect and subsequent diuresis in patients presenting with total body fluid excess (as opposed to redistribution).
Dopamine use in AHF has limited evidence. The ROSE-HF (Renal Optimization Strategies Evaluation in Acute Heart Failure) study demonstrated that renal dose dopamine should not be used routinely in patients with AHF and an estimated glomerular filtration rate (eGFR) of 15-60 ml/kg/min. There was no reduction in 60- or 180-day mortality or heart failure (HF) hospitalisation. But the jury remains out as clinical practice often leans towards the use of dopamine in AHF in those who fail to respond to intravenous diuretics with marked fluid overload. This is an area in much need of a randomised controlled trial (RCT).
Inotropes are no longer routinely recommended in AHF.
Nitrates should not be used in the routine management of AHF. Uncontrolled drops in blood pressure are closely associated with an increase in mortality and therefore they should only be used in specific circumstances (myocardial ischaemia, severe hypertension) and in a level two high care area.
On the horizon, RELAX-AHF (Relaxin in Acute Heart Failure) is an ongoing RCT comparing serelaxin (recombinant human relaxin – a vasodilator with additional properties) to standard care and placebo. It has been powered to look at improving dyspnea, reduction of cardiovascular (CV) mortality and hospital admission for HF. This study will hopefully build on early promising data.
Chronic heart failure
Professor John McMurray (University of Glasgow) summarised the evidence on the latest advances and touched on projects for the future in this complex and ever evolving subspecialty. The link between chronic kidney disease (CKD) and CV disease is well established, and this is particularly apparent when considering heart failure.
What more can be done in terms of neurohormonal manipulation? Spironolactone and eplerenone are well established as successful adjuncts to angiotensin-converting enzyme (ACE) inhibitors and beta blockers in the management of heart failure with reduced ejection fraction, currently holding a firm 1A evidence base. Non-steroidal mineralocorticoid receptor antagonists are an exciting new area of research with stage III clinical trials ongoing. FINESSE-HF (Finerenone Trial to Investigate Efficacy and Safety to Eplerenone in Patients with Heart Failure) is assessing finerone versus eplerenone use following hospitalisation for heart failure, with CV death or heart failure hospitalisation as primary end points.
Even though well-established and effective treatment regimes are available, thinking ‘outside the box’ and considering novel therapies are vital for continuing dynamic change and improvements in mortality for complex disease processes. PARADIGM-HF prospectively compared the angiotensin receptor–neprilysin inhibitor, sacubitril-valsartan (LCZ696), to well-established enalapril. The primary end point was set as death from CV causes or hospitalisation secondary to heart failure. The trial was stopped early due to the significant superiority of LCZ696 over enalapril in respect to mortality and overall safety. This novel agent blocks the deleterious effects of the activated renin-angiotensin system but also augments the counter-regulatory vasodilator and natriuretic pathways. It is likely that this agent will transform the management of patients with heart failure with reduced ejection fraction and become first-line treatment instead of ACE inhibitor/angiotensin receptor blockers.
Biomarkers
Diagnosis and monitoring of disease progression is key through both qualitative symptomatic assessment and quantifiable biochemical marker analysis. Professor Paul Collinson (St George’s University London) provided the latest update on biomarkers in both CV and renal disease. Both troponin I and troponin T are powerful predictors of CV mortality in patients with CKD but there is an ongoing debate as to the reasoning behind elevated levels of troponin being detected. Is it failure of troponin clearance or fragmentation of the molecule? The jury is still out on this issue.
Promising ideas for the future
Fibroblast growth factor 23 (FGF23) is a protein secreted by osteocytes in response to elevated calcitriol. Whilst work with this biomarker is in the early days, its use in identifying patients with CKD whom may benefit from aggressive management of phosphate metabolism is promising. Early results also suggest that significantly raised FGF23 levels in CKD could be a direct contributor to myocardial, vascular and renal tissue injury.
Iron deficiency in cardiorenal disease
Professor Iain Macdougall (King’s College Hospital, London) presented a thorough overview of the pathophysiology and treatment of anaemia in patients with CKD and those on renal replacement therapy. He firstly reminded us that iron deficiency is the leading cause of anaemia in renal patients; European studies (such as PRESAM and ESAM) show that 30–61% of CKD patients have iron deficiency anaemia (IDA). The investigations most helpful in establishing IDA are serum ferritin, transferrin saturations and percentage of hypochromic red blood cells. The 2015 NICE guideline ‘Chronic kidney disease: managing anaemia (NG8)’ has set treatment targets aiming for a serum ferritin >100 µg/ml, TSats >20% and <10% hypochromic red blood cell counts (RBCs).
The question remains, however, how can we best treat iron deficiency in CKD. Oral iron is cheap but is poorly tolerated and often poorly absorbed. FIND-CKD (a randomised trial of intravenous ferric carboxymaltose versus oral iron in patients with CKD and iron deficiency anaemia) demonstrated that high-dose intravenous iron resulted in a faster rise in haemoglobin (Hb) compared to oral or low-dose intravenous iron and patients overall achieved a higher Hb. PIVOTAL (Proactive Intravenous Iron Therapy in Haemodialysis Patients) is a UK prospective RCT in haemodialysis patients. This compares regular monthly intravenous iron infusion with treatment directed by a serum ferritin <200 µg/l. The primary end point is time to all-cause mortality and composite of non-fatal cardiovascular events. This trial will hopefully guide future management of iron deficiency in the dialysis population.
Anaemia is also prevalent in the heart failure population and is an independent risk factor for adverse outcomes in heart failure patients. Iron deficiency has also been shown to be an independent risk factor for all-cause mortality regardless of Hb level. The FAIR-HF (Ferinject Assessment in Patients with Iron Deficiency and Chronic Heart Failure) and CONFIRM-HF (Ferric Carboxymaltose Evaluation on Performance in Patients with Iron Deficiency in Combination with Chronic Heart Failure) trials demonstrate that correction of this iron deficiency (with intravenous iron) was associated with improvements in quality of life, heart failure symptoms and exercise tolerance.
These studies have led to the development of the IRONMAN (Intravenous Iron Treatment in Patients With Heart Failure and Iron Deficiency) trial, led by Dr Paul Kalra (Queen Alexandra Hospital, Portsmouth), a prospective RCT recruiting patients with left ventricular systolic dysfunction and IDA. This will compare giving intravenous iron to keep ferritin levels above 100 µg/ml and Tsats >25% to normal standard care. The primary end points are CV mortality and hospitalisation due to heart failure. Patients (n=1,300) will be followed for two years and the trial started recruitment in early 2016. We look forward to exciting new developments in a modifiable risk factor where therapeutic intervention could provide improvement in patient mortality and morbidity.
Cardio-oncology – a novel problem!
Advancement in oncology treatment and improved life expectancy in many cancer patients has created a new challenge for cardiologists. Dr Alexander Lyon (Royal Brompton Hospital, London) introduced a new emerging subspecialty in cardiology and the service provided at the Royal Brompton Hospital.
Many chemotherapy agents are associated with cardio-toxic effects. A study by Bowles EJA et al. (J Natl Cancer Inst 2012;104:1293–305 doi: 10.1093/jnci/djs401) found that 12.5% of breast cancer patients treated with trastuzumab (Herceptin®) developed heart failure within five years. The new tyrosine kinase inhibitors in renal cell carcinoma are increasing survival but are all associated with an increased incidence of CV side effects including hypertension and reduced left ventricular ejection fraction. With this knowledge, is there any way of predicting which patients will be affected and therefore prevent potential long-term CV complications?
Early detection of abnormalities of myocardial function with speckle tracking echocardiography and elevated serum cardiac biomarkers during chemotherapy can predict which patients are vulnerable. Cardinale D et al. (Circulation 2004;109:2749–54 doi: 10.1161/CIRCULATIONAHA.106.635144) published data showing patients with a troponin rise during treatment with anthracyclines had an increased risk of cardiovascular events. It has been shown in small studies that initiation of an ACE inhibitor and beta blocker may reduce CV events. This warrants further evaluation to establish if this can be an effective preventative strategy.
A cardio-oncology service has been initiated at the Royal Brompton Hospital, which serves to pre-assess high-risk patients and optimise primary prevention. Follow up is provided to those patients who have developed CV complications as a result of their cancer treatment. This aims to reduce cardiac problems in survivors and support optimal cancer treatment.
Updates in nephrology
Professor Maarten Taal (Royal Derby Hospital, Derby) gave an update of recent trials involving CKD patients and CV risk. CKD is associated with increased CV and all-cause mortality. A meta-analysis of over 24 studies involving greater than 600,000 patients, found in the general population urinary albumin to creatinine ratio (ACR) and eGFR improve cardiac risk prediction, with the greatest effect seen in CV mortality and heart failure. In those with CKD, these measurements are in fact better risk predictors than any of the other traditional Framingham CV risk factors.
The significance of raised cardiac biomarkers in the CKD population remains uncertain. The CRIC (Chronic Renal Insufficiency Cohort) study, a prospective cohort study of >3,000 patients with CKD without HF at baseline, showed elevated high sensitivity troponin and NT-pro BNP levels were associated with increased incidence of HF. This may reflect subclinical cardiac injury that progresses to HF even in the early stages of CKD and therefore are independent predictors of HF in the CKD population.
SHARP (Study of Heart and Renal Protection) demonstrated improved CV outcomes in patients treated with simvastatin/ezetimibe compared to placebo in the CKD population. The effect in primary prevention, however, was unclear. A meta-analysis by Major RW et al. (Clin J Am Soc Nephrol 2015;10:732–9 doi: 10.2215/CJN.07460714) of six randomly controlled trials of primary prevention with lipid-lowering agents in patients with CKD stage 1−3, found statins are effective in reducing CV disease when used in primary prevention and therefore are now recommended in all patients with CKD stages 1−3.
A wealth of other data highlighting the recent advances in cardiorenal medicine were presented during the day, supported by several clinical cases. There was stimulating passionate debate between cardiologists and nephrologists and we look forward to next year’s conference.
‘Pathways of care’ was the theme for the 18th British Society for Heart Failure (BSH) Annual Autumn Meeting, held in London from 26–27th November 2015. In recognition of a lifetime of landmark heart failure studies, Professor Marc Pfeffer (Boston, USA) was the deserved recipient of the Philip Poole-Wilson Memorial award presented during the meeting. Drs Parminder Chaggar and Matthew Kahn report some of the highlights from the comprehensive programme.
Bridging the gap: from trials to inner cities
Within the field of heart failure, there is a breadth of prognostic therapies derived from large, randomised controlled trials. Professor Iain Squire (Glenfield Hospital, Leicester) described how new treatments require approval in the European Union before they can be implemented into clinical practice within the member states. The European Medicines Agency (EMA) ensures the best use of scientific resources across Europe. While certain classes of technologies must undergo licencing via a centralised procedure, most therapies will be eligible for licensing by one member state on behalf of other nations. In the UK, the National Institute for Health and Care Excellence (NICE) provides clinical guidelines and technology appraisals. Although adherence to NICE guidelines is not mandatory, the technology appraisal outcomes are enforced in the UK since these are based on cost effective analyses. Assessment of cost effectiveness is governed by the cost per quality adjusted life year (QALY), with an acceptable cost being defined as less than £30,000 per QALY.
Simon Woldman (University College Hospital, London) and Suzanna Hardman (Whittington Hospital, London)
New therapies are referred for NICE technology appraisal by the Department of Health; NICE can only consider the novel treatment under its marketing licence indication. Any appraisal follows a standardised pathway beginning with the company submission and critique of the evidence. The first appraisal meeting is attended by clinical experts, lay people, NICE and the company, with members of the public allowed to observe. The first meeting generates an appraisal document containing a recommendation, which is open for comments by stakeholders, including the company and national societies, prior to a final recommendation. The process of approval can be time consuming. As an example, Professor Squire illustrated that despite publication of the landmark PARADIGM-HF trial in August 2014,1 sacubitril/valsartan was only granted EMA authorisation in September 2015 and the NICE technology appraisal recommendation is still awaited.
Getting new treatments to the right patient
Significant challenges remain in ensuring healthcare systems are able to direct prognostic therapies to the target patients when new treatments become available. Dr Suzanna Hardman (Whittington Hospital, London) discussed the development over many years of integrated heart failure services across Islington, including community and acute care. Cardiovascular mortality in Islington was amongst the highest in the UK with heart failure contributing substantially to these outcomes. Islington contains high levels of social deprivation, unemployment, alcohol and smoking use, language diversity and transient populations.
Tackling the high heart failure mortality required concerted engagement with both primary care and public health to provide rapid access to heart failure care pathways, including B-type natriuretic peptide (BNP)2 and hospital-based diagnostic clinics, alongside the development of responsive community specialist heart failure nursing services. In addition, a consultant-led inpatient heart failure programme was instituted including active identification and investigation of patients with suspected heart failure. This included echocardiograms within 48 hours, outreach consultations to non-cardiology wards, hospital-wide protocols for drug titration, ensuring 48-hours stability prior to discharge with personalised care plans and early outpatient follow-up. This progressive and pioneering approach pre-dates by over a decade the very similar current NICE heart failure guidance.3 Its impact is evident in the current mortality statistics. Cardiovascular mortality has steadily fallen in Islington over the past 15 years whilst inpatient mortality for those admitted with heart failure is now only 2.6% (National Heart Failure Audit data) compared to the reported national average of 9.4%.4
Meanwhile, Dr Simon Woldman (University College Hospital, London) described the challenges in utilising national data to improve local standards. National data are often subject to a lag of several months and thus University College Hospital has adopted data points from the National Heart Failure Audit into a monthly internal monitoring scheme. As a result, local hospitals are able to evaluate their ‘real-time’ performance including accessibility to investigations, drug prescription rates and outcomes. Audit-driven service changes have been associated with improvements on subsequent audits.
Dr Woldman has also evaluated heart failure prevalence rates in his local GP practices and noticed an inverse relationship with heart failure admission rates from each practice. This suggests that missed heart failure diagnoses may not be receiving appropriate management and are at higher risk of hospitalisation. Active identification and management of 300 patients with previously undiagnosed heart failure has been associated with a reduction in heart failure admissions (unpublished data). In summary, Dr Woldman highlights there is a wealth of data available to drive service improvement, which can be utilised with minimum resources but result in significant outcome benefits and cost savings.
A local audit of heart failure admissions in South London by Dr Lisa Anderson (St George’s University Hospitals NHS Foundation Trust, London) demonstrated worrying statistics; a 60% increase in heart failure admissions over a five-year period with a significant number of patients having a length of stay of one day or less. Further analysis of these short admissions revealed over half had pulmonary oedema and very high BNP but with very little inpatient heart failure specialist input. Only 8% received an echocardiogram and only 42% were referred to the heart failure clinic. Presentation of the data at the local Care Quality Review meeting provided support for £1.2 million investment into a dedicated inpatient heart failure unit. Although delayed by recent global financial pressures, the 15-bed unit comprising dedicated nurses, fellows, technicians, pharmacists and administrative staff is due to open imminently. Its effectiveness will be subject to external assessment.
These success stories in heart failure management demonstrate how the use of local data can be used to effect change and are inspiring models for care in the 21st century. They are testament to the significant vision and commitment of their orchestrators.
BSH Young Investigators Award
The standard of rapid-fire abstracts for the ‘Young Investigators Award’ was once again of the highest quality. Dr Soren Lund Kristensen (University of Copenhagen, Denmark) was the eventual winner of the prestigious award with his presentation on employment following first hospitalisation for heart failure in patients of working age. By linking nationwide Danish administrative registries, over 13,000 patients were identified in order to assess the impact of first hospitalisation for heart failure on subsequent labour market attachment in patients previously available to the labour market. The group showed that one year after first hospitalisation for heart failure, employment among patients of working age dropped more than 25% regardless of age group. Younger age, chronic kidney disease and cancer were the most significant predictors of employment status.
Treating atrial fibrillation and heart failure
Dr Derek Connelly (Glasgow) presented an up-to-date summary of the importance of diagnosing and treating atrial fibrillation (AF) in the setting of heart failure. Antithrombotic therapy remains of paramount importance in patients with AF and heart failure. Virtually all patients should be anticoagulated, either with warfarin (aiming for an international normalised ratio of 2−3) or with a non-vitamin K antagonist oral anticoagulant (NOAC).
The pharmacological options for rate and/or rhythm control strategies for the management of AF in patients with heart failure remain extremely limited. To look at this, the AF-CHF trial − a multicentre, prospective, open label trial − randomised 1,376 patients with heart failure and an ejection fraction <35% with a history of AF to rhythm control versus rate control. Over a follow-up period of 37 months, rhythm control did not improve patient outcomes compared to a rate control strategy.5
Of the available drugs for rate control, calcium channel antagonists are contra-indicated due to their negative inotropic effects. Digoxin may be of use in selected patients but several studies have drawn attention to adverse effects on mortality with digoxin use in AF. Beta blockers remain the mainstay of rate control therapy. Three beta blockers are approved for use in heart failure (carvedilol, bisoprolol and slow-release metoprolol).
The CIBIS II trial studied the relationships between baseline heart rate, nature of cardiac rhythm (sinus rhythm or AF), and outcomes (mortality and hospitalisation for heart failure). Bisoprolol reduced mortality in patients with sinus rhythm but not in patients with AF.6 In the COMET trial, 3,029 patients with heart failure were randomised to carvedilol or metoprolol. Treatment with carvedilol, compared with metoprolol, was found to offer additional benefits among patients with AF and heart failure.7
Pharmacological options for rhythm control are even more limited in this group of patients. Realistically the only drug routinely available is amiodarone. Class I anti-arrhythmic drugs and dronedarone are contraindicated, while sotalol is not indicated in heart failure.
Catheter ablation strategies targeting primarily the substrate and/or the initiating triggers for AF have been established in recent years. Selected patients with heart failure and AF may be eligible for such treatments. It is essential to identify those with high potential benefit and low expected risks of complications for rhythm control strategy. Several small studies have assessed the efficacy of AF ablation in heart failure, and most studies have documented improvement in symptoms and ejection fraction during short term follow up. Longer term data are not yet available.
The PABA-CHF trial − a prospective, multicentre trial − randomly assigned patients with symptomatic, drug-resistant AF, an ejection fraction of 40% or less, and New York Heart Association class II or III heart failure, to undergo either pulmonary vein isolation or atrioventricular-node ablation with biventricular pacing. The group concluded that pulmonary vein isolation was superior to atrioventricular node ablation with biventricular pacing in patients with heart failure who had drug-refractory atrial fibrillation.8 It is important to note that ablation for atrial flutter is highly efficacious and extremely safe, and thus patients with heart failure and atrial flutter should be prioritised for ablation.
New approaches to heart failure treatment
Professor Michael Frenneaux (University of East Anglia, Norwich) delivered a fascinating presentation on the metabolic treatment of heart failure. The heart requires huge quantities of energy (approximately 6 kg of ATP daily) in its role as a relentless pump. Abnormalities of cardiac energy metabolism make an important contribution to chronic heart failure. Energetic impairment has been reported in patients with a variety of heart muscle disease (including dilated cardiomyopathy, hypertrophic cardiomyopathy, heart failure with preserved ejection fraction, aortic stenosis). Multiple mechanisms contribute to this.9
Agents that cause a metabolic shift from predominant fatty acid to carbohydrate oxidation increase left ventricular mechanical efficiency in experimental models. Two particular agents with actions, at least in part, via this mechanism (perhexiline and trimetazidine) have been shown to improve cardiac function and exercise capacity in patients with systolic heart failure.10,11 Such therapies offer significant promise for the treatment of symptomatic heart failure and thus more studies, especially larger multicentre randomised controlled trials, are warranted to clarify the effect of these drugs in heart failure.
Dr John Baxter (Sunderland Royal Hospital) concluded the BSH conference with a hugely entertaining and practical talk outlining strategies to change pathways of care in the workplace. The importance of the multidisciplinary heart failure service aspiring to deliver an early accurate diagnosis and optimal well-integrated care for all patients with heart failure was discussed. Reference was made to Dr Hardman’s presentation (see above), reflecting on the emergence of an integrated heart failure service from 1999 to the present coinciding with a low all-cause mortality and heart failure–related mortality at the Whittington Hospital.
Acknowledgement
The BSH gratefully acknowledges support from Bayer HealthCare, Biotronik, Boston Scientific, Medtronic, Novartis, Pfizer, ResMed, Servier Laboratories, St Jude Medical and Vifor Pharma.
Diary dates
Future BSH meetings include the Heart Failure Day for Revalidation and Training on 3rd March 2016, the Heart Failure Nurse and Healthcare Professional Study Day on 4th March 2016 and the 19th Annual Autumn Meeting on 24–25th November 2016. For further information, contact the BSH at: www.bsh.org.uk; twitter: @BSHeartFailure; and email: info@bsh.org.uk
Conflict of interest
None declared.
Parminder S Chaggar
Cardiology Registrar
Dr Matthew Kahn
North West Heart Centre, University Hospital of South Manchester, Southmoor Road, Manchester, M23 9LT
1. McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014;371:993−1004. http://dx.doi.org/10.1056/NEJMoa1409077
2. Zaphiriou A, Robb S, Murray-Thomas T, et al. The diagnostic accuracy of plasma BNP and NTproBNP in patients referred from primary care with suspected heart failure: results of the UK natriuretic peptide study. Eur J Heart Fail 2005;7:537−41. http://dx.doi.org/10.1016/j.ejheart.2005.01.022
5. Roy D, Talajic M, Nattel S, et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med 2008;358:2667−77. http://dx.doi.org/10.1056/NEJMoa0708789
6. Lechat P, Hulot JS, Escolano S, et al. Heart rate and cardiac rhythm relationships with bisoprolol benefit in chronic heart failure in CIBIS II Trial. Circulation 2001;103:1428−33. http://dx.doi.org/10.1161/01.CIR.103.10.1428
7. Swedberg K, Olsson LG, Charlesworth A, et al. Prognostic relevance of atrial fibrillation in patients with chronic heart failure on long-term treatment with beta-blockers: results from COMET. Eur Heart J 2005;26:1303−8. http://dx.doi.org/10.1093/eurheartj/ehi166
8. Khan MN, Jaïs P, Cummings J, et al. Pulmonary-vein isolation for atrial fibrillation in patients with heart failure. N Engl J Med 2008;359:1778−85. http://dx.doi.org/10.1056/NEJMoa0708234
10. Lee L, Campbell R, Scheuermann-Freestone M, et al. Metabolic modulation with perhexiline in chronic heart failure: a randomized, controlled trial of short-term use of a novel treatment. Circulation 2005;112:3280−8. http://dx.doi.org/10.1161/CIRCULATIONAHA.105.551457
11. Gao D, Ning N, Niu X, Hao G, Meng Z. Trimetazidine: a meta-analysis of randomised controlled trials in heart failure. Heart 2011;97:278−86. http://dx.doi.org/10.1136/hrt.2010.208751
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits