Birmingham City Hospital, Sandwell and West Birmingham Hospitals NHS Trust, Dudley Road, Birmingham, B18 7QH.
Sponsorship Statement:
Bayer plc. commissioned and funded this supplement. The company has reviewed the data to ensure factual accuracy in relation to Bayer products and compliance with industry guidelines.
For notes on dosing recommendations for Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics) please see the box at the foot of this page.
Rivaroxaban prescribing information current at the time of publication is available here.
Job code: PP-XAR-GB-1131
Date of preparation: January 2020
Atherosclerosis is the leading cause of death in the UK and is likely to remain so for the foreseeable future.1 Much of the research effort in secondary prevention has focused on patients with myocardial infarction or stroke, particularly on the effects of antithrombotic agents, but populations with peripheral artery disease (PAD) have been studied less intensively.
Patients presenting with symptomatic PAD are at high risk of ischaemic stroke, myocardial infarction and progression of the PAD.2 Recent data suggest that half of chronic total occlusions occurring below the knee are thomboembolic in origin, and not due to in situ atherosclerosis as believed previously.3 Accordingly, treating PAD patients with antithrombotic agents may have benefits in reducing major adverse cardiovascular events (MACE).8
The COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial demonstrated that adding rivaroxaban 2.5 mg twice daily to aspirin 100 mg once daily in patients with PAD reduced MACE compared to aspirin alone.4 The results of COMPASS were reviewed by the National Institute for Health and Care Excellence (NICE) in a technology appraisal guidance published on 17th October 2019 entitled ‘Rivaroxaban for preventing atherothrombotic events in people with coronary or peripheral artery disease’.5 Rivaroxaban plus aspirin was recommended within its marketing authorisation, as an option for preventing atherothrombotic events in adults with coronary artery disease or symptomatic PAD who are at high risk of ischaemic events mirroring the entry criteria for the COMPASS study.
Conflicts of interest
DC has received research funding, speaker fees and advisory consultation fees from Bayer.
Guest editor
Derek Connolly Consultant Cardiologist and Honorary Senior Lecturer (Institute of Cardiovascular Science, University of Birmingham)
1. Steel N, Ford JA, Newton JN, et al. Changes in health in the countries of the UK and 150 English Local Authority areas 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018;392:1647–61. https://dx.doi.org/10.1016/S0140-6736(18)32207-4
2. Sartipy F, Sigvant B, Lundin F, Wahlberg E. Ten year mortality in different peripheral arterial disease stages: a population based observational study on outcome. Eur J Vasc Endovasc Surg 2018;55:529–36. https://dx.doi.org/10.1016/j.ejvs.2018.01.019
3. Torii S, Mustapha JA, Narula J, et al. Histopathologic characterization of peripheral arteries in subjects with abundant risk factors: correlating imaging with pathology. JACC Cardiovasc Imaging 2019 Aug;12(8Pt1):1501–13. https://dx.doi.org/10.1016/j.jcmg.2018.08.039
4. Kruger PC, Anand SS, de Vries TAC, Eikelboom JW. Patients with peripheral artery disease in the COMPASS trial. Eur J Vasc Endovasc Surg 2018;56:772–3. https://dx.doi.org/10.1016/j.ejvs.2018.08.010
5. National Institute for Health and Care Excellence (NICE). Rivaroxaban for preventing atherothrombotic events in people with coronary or peripheral artery disease. Technology appraisal guidance (TA607). London: NICE, October 2019. www.nice.org.uk/guidance/ta607 (last accessed December 2019)
Notes on dosing recommendations from Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics)
Xarelto 2.5 mg twice daily, coadministered with a daily dose of 75–100 mg aspirin, is indicated for the prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral artery disease (PAD) at high risk of ischaemic events.
The COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial discussed in this supplement compared both Xarelto 2.5 mg twice-daily plus aspirin and also Xarelto 5 mg twice-daily without aspirin, versus aspirin alone. Results for both comparisons are provided reflecting the original study publication.
Please note, however, that Xarelto 5 mg twice-daily is not a licensed dosage regimen for the above, nor for any other therapeutic indication.
Disclaimer: Medinews Cardiology Limited advises healthcare professionals to consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews Cardiology Limited cannot accept responsibility for any errors in prescribing which may occur.
Ruth A Benson Academic Clinical Lecturer in Vascular Surgery
Institute of Translational Medicine,
University of Birmingham, Edgbaston, Birmingham, B15 2TH
Owain Fisher ST5 in Vascular Surgery University Hospital of Coventry and Warwick, Clifford Bridge Road, Coventry, CV2 2DX
Andrew Garnham Consultant Surgeon Black Country Vascular Service, New Cross Hospital, Wolverhampton, WV10 0QP
Sponsorship Statement:
Bayer plc. commissioned and funded this supplement. The company has reviewed the data to ensure factual accuracy in relation to Bayer products and compliance with industry guidelines.
For notes on dosing recommendations for Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics) please see the box at the foot of this page.
Rivaroxaban prescribing information current at the time of publication is available here.
Job code: PP-XAR-GB-1131
Date of preparation: January 2020
There is an impending global epidemic in peripheral artery disease (PAD), owing to increasing rates of obesity and diabetes. Despite being a common and potentially preventable condition, the evidence base underpinning the diagnosis, treatment and prevention of PAD is poor when compared with conditions of similar prevalence. This is alarming given that patients with both asymptomatic and symptomatic PAD have worse outcomes in terms of all-cause mortality and, in particular, cardiovascular-related death. A large scale, community effort from specialist practitioners, general practitioners and public health is required to combat this impending health disaster. This can be achieved through higher quality research, increased patient and public awareness, and responsible use of available resources if we are to improve life and limb in this under-recognised group of patients. We aim to give a global view regarding the challenges that lie ahead and the opportunities for improvement in all subgroups in the spectrum of PAD.
Introduction
Currently, worldwide, there is an impending epidemic of symptomatic peripheral artery disease (PAD). This is largely due to the increasing prevalence of risk factors such as: smoking, diabetes, high blood pressure (BP), cholesterol, and end-stage renal disease (ESRD). In the developed world this is largely due to an epidemic of diabetes and obesity. There is a wide spectrum of PAD that ranges from asymptomatic disease through to chronic limb-threatening ischaemia (CLTI). Depending upon income and region, the number of sufferers with PAD has increased by 13–25% during the last decade, accounting for 202 million people worldwide in 2010.1 The majority of those affected are represented by people older than 60 years, of whom 10–20% are thought to be affected by PAD.2 PAD is believed to double the risk of cardiovascular morbidity and mortality, even without major limb ischaemia.3
Awareness of PAD is low among patients and the public, despite PAD having five-year mortality rates higher than common cancers and acute myocardial infarction (MI) in both symptomatic and asymptomatic groups (figure 1).4–6 Despite this clear clinical need, the evidence underpinning treatment in PAD, and CLTI in particular, is poor. Heterogeneity in the literature and poor levels of evidence make any conclusions difficult to generalise to the PAD population. In 2012, the National Institute for Health and Care Excellence (NICE) suggested areas of focus for future research in patients with symptomatic PAD (table 1).7 These call for focus on: assessment, patients with PAD and diabetes, infra-geniculate disease and improving patient awareness. Below, we discuss the challenges of improving life and limb, including unmet needs for the whole spectrum of patients with PAD.
Figure 1. Five-year all-cause mortality for common conditions in the United Kingdom4–6
Table 1. National Institute for Health and Care Excellence recommendations for research in peripheral artery disease7
The recommendations for reasearch in peripheral artery disease
Effectiveness of tools for diagnosing peripheral artery disease in people with diabetes
Effectiveness of tools for establishing the severity of peripheral artery disease in people with diabetes
Inter- and intra-rate reliability of assessment tools in the diagnosis of peripheral artery disease in people with diabetes
Angioplasty versus bypass surgery for treating people with critical limb ischaemia caused by disease of the infra-geniculate arteries
Supervised exercise programmes for treating people with intermittent claudication
Patient attitudes and beliefs about peripheral artery disease
Primary versus secondary stenting for treating people with critical limb ischaemia caused by disease of the infra-geniculate arteries
Chemical sympathectomy for managing critical limb ischaemic pain
Asymptomatic PAD and primary prevention
Screening by measurement of the ankle-brachial pressure index (ABPI) is formally required to assess PAD, with an index of <0.9 being diagnostic. The prevalence of asymptomatic PAD is of interest due to its implications for cardiac and stroke risk.3 Studies have suggested that approximately 35% of women aged over 65 years have ABPI-detected PAD,8 compared with 29% in men over the age of 68.9
The randomised Aspirin for Asymptomatic Atherosclerosis trial failed to show any benefit of aspirin on reducing future vascular events,10 despite asymptomatic PAD being associated with functional decline, and a five-fold higher baseline mortality from cardiovascular events than a non-PAD population.11 A recent systematic review into the effectiveness of screening using ABPI and its effect on outcome, proved inconclusive.12 Fowkes et al. estimated the odds ratios for all-cause mortality in individuals with asymptomatic and symptomatic PAD (1.53 and 1.98, respectively) compared with matched, disease-free individuals in a pooled analysis of known population studies to date.13 This was supported by long-term findings from Sartipy et al., who demonstrated all-cause, 10-year mortality of 56% for patients with asymptomatic PAD (APAD) and a doubling of the age-adjusted hazard ratio for cardiovascular death.14 At present, the European Society of Cardiology (ESC) recommends screening for APAD only in patients with previously diagnosed heart failure or coronary artery disease, based on level IIb evidence.15
Due to a lack of evidence, it is difficult to estimate the proportion of patients with APAD that go on to develop symptoms; a meta-analysis estimated that those developing intermittent claudication having been previously diagnosed with APAD is somewhere between 4–11%.6 Without a large, worldwide public health effort, it is unlikely that the true incidence of APAD can be identified, as current data are available only from selected interventional studies. The outcomes from treating APAD with best medical therapy (BMT; antiplatelet and statin) or otherwise are largely unknown.
Best medical therapy – secondary prevention
In patients diagnosed with symptomatic PAD, a regime of BMT is recommended in national guidelines worldwide. This constitutes lifestyle modification and control of known risk factors. In the UK, NICE recommend an antiplatelet agent (clopidogrel 75 mg once daily) and lipid-lowering therapy (high-dose statin such as 80 mg atorvastatin daily as first line), as widely used in patients with coronary artery disease. Research into the use of direct oral anticoagulants (DOACs), dual antiplatelet agents and combinations of the two continue, with the ultimate goal of a tailor-made, individual approach to addressing individual risk factors. Ongoing genomic testing is investigating targeted alleles expressed in some patients who cannot metabolise antiplatelet therapies. This may have screening implications in the future. There are wider issues around compliance, adherence and patient and public education; even in large, prospective clinical trials the uptake of BMT is poor at around 70%.
Direct oral anticoagulants
The recent publication of the COMPASS (Rivaroxaban for the Prevention of Major Cardiovascular Events in Coronary or Peripheral Artery Disease) trial has raised hope that adjunctive, low-dose rivaroxaban (2.5 mg twice daily) with aspirin will improve long-term cardiovascular outcomes, particularly in patients with PAD16 (the COMPASS trial outcomes and results are discussed in detail elsewhere in this supplement).
Antiplatelet therapy
Encouraging results from the PLATO (Platelet Inhibition and Patient Outcomes) study demonstrated a reduction in secondary cardiac events when ticagrelor was given with aspirin (as opposed to clopidogrel and aspirin) in patients with acute coronary syndrome.17 There were no reductions in cardiovascular morbidity in patients with symptomatic PAD, however, when ticagrelor was given as a monotherapy, compared with clopidogrel alone.18 Some evidence from the American Vascular Quality Initiative suggests a survival benefit in those patients undergoing lower limb revascularisation when using dual antiplatelet therapy, particularly in high-risk patients.19 More evidence is required to define the dosage and combination of therapies of most benefit.
Lipid modification
The evidence underpinning the use of statins and other lipid-lowering therapies is primarily extrapolated from the coronary literature. Most guidelines in the US, UK and rest of Europe recommend the use of high-intensity statin treatment to reduce secondary cardiovascular events. There is limited evidence in the literature pertaining to the use of lipid-lowering therapy and its specific benefits for patients with PAD. One recent study reported that patients with CLTI, the most severe form of PAD, had reduced mortality and improved freedom from major adverse limb events when lipid therapy guidelines were followed in patients undergoing revascularisation.20
Intermittent claudication
Adverse prognosis
‘Increasing rates of obesity and diabetes are leading to an impending global epidemic in PAD’
Intermittent claudication, a clinical syndrome of exertional pain in the muscles of the lower limbs that terminates with rest, is the commonest manifestation of symptomatic PAD. The long-term risks of cardiovascular mortality in patients with intermittent claudication are well documented, and 20% of individuals will have a cardiovascular event in a 10-year period.11,21,22 Symptomatic PAD, in general, is a stronger predictor of mortality than CAD or cerebrovascular disease alone.23–25 Although intermittent claudication is generally considered as a ‘benign’ condition, one patient in five will progress to CLTI in a five-year period,6 and those with diabetes and persistent smokers are most at risk. The lifetime amputation risk for all patients with claudication is thought to be around 1%. Despite these clear risks, uptake and delivery of recommended, evidence-based treatment strategies remain problematic.
In the UK, intervention in patients with intermittent claudication is discouraged by NICE unless a patient is thought by local multidisciplinary teams to be symptomatic enough that health-related quality of life (HRQoL) is significantly impacted.7 They must also have made a concerted effort to control any identified risk factors such as smoking and attended a 12-week programme of supervised exercise therapy (if available, see below). Intervention for intermittent claudication is on the increase in other parts of the developed world, particularly as most countries are now practising an endovascular first revascularisation strategy.
Supervised exercise therapy
The aforementioned NICE guidance (Clinical Guideline 147) stipulates that all patients should have any risk factors for PAD addressed as part of secondary prevention (smoking, obesity, hypertension, dyslipidaemia, diabetes) and also be enrolled in a programme of supervised exercise therapy (SET).7 Despite good quality evidence that SET is beneficial26 and cost effective at current willingness to pay thresholds in the UK,27 provision and uptake is low. This may be due to a variety of issues, including lack of funding from healthcare providers, poor patient compliance and an upturning worldwide trend towards increasing use of endovascular treatment, such as angioplasty, drug-eluting technology, atherectomy and stenting.28
The benefits of SET on overall health, even in those undergoing intervention, are clear; a recent systematic review and meta-analyses of seven randomised trials reported improved outcomes in terms of reduced numbers of amputation, increased walking distance and ABPI in patients receiving adjunctive SET with endovascular treatment versus those receiving endovascular treatment alone.29 Despite high quality evidence, only around 30–40% of vascular centres in the UK currently offer SET.30 Regardless of intervention, a regime that improves overall health and treats risk factors to reduce secondary events seems logical and the evidence to support this approach is growing.31
Drug-eluting endovascular technology
Many industry-funded studies have assessed anatomically-based outcomes of patients with intermittent claudication receiving drug-eluting endovascular technology with paclitaxel coated balloons and stents in small, selected groups of claudicants with primarily femoropopliteal disease initially demonstrating promising results.32-35 However, the recent meta-analysis by Katsanos et al.36 has resulted in considerable controversy, demonstrating an increase in mid-term mortality for patients undergoing drug-eluting endovascular treatment when compared with those undergoing plain balloon angioplasty. The impact of this on clinical practice and translation to patients with chronic limb-threatening ischaemia is currently a topic of debate.
Chronic limb-threatening ischaemia
CLTI represents the most severe form of PAD and also carries by far the worst outcomes. The average five-year survival is known to be around 50%. By definition, patients usually present with challenging, multilevel disease that is often above and below the inguinal ligament. Tibial involvement is increasingly common. Despite this, there is still, to date, only one randomised controlled trial comparing revascularisation outcomes in people with CLTI.
The BASIL (Bypass vs. Angioplasty in Severe Ischaemia of the Leg) trial demonstrated that those with a predicted survival of two years or greater fared better in terms of amputation-free survival with open surgical bypass, rather than best endovascular treatment.37 About 75% of patients in BASIL had primarily femoro-popliteal disease. A recent post-hoc, subgroup analysis from the trial of patients with primarily infra-popliteal disease demonstrated a reduction in rest pain but similar clinical outcomes in other domains, when comparing the same two revascularisation options. The trial, however, was not powered to demonstrate significant differences in this subgroup.38
The longstanding debate regarding which revascularisation modality should be used as a first treatment strategy remains – ‘endo-enthusiasts’ claim that if the BASIL trial were to be repeated using modern endovascular technology, the outcomes may be different. Ongoing trials in the US and UK aim to resolve this debate.39–41 A recent, large meta-analysis of around 8,000 patients undergoing infra-inguinal revascularisation demonstrated higher patency rates for patients undergoing vein bypass. The authors commented, however, that a severe lack of high-quality data and heterogeneity made any comparisons difficult.42 There have been recent attempts to improve reporting, assessment and classification of CLTI, and recently, the Global Vascular Guidelines have been published which focus on a new ‘Global Limb Anatomical Staging System’ (GLASS) that aims to improve reporting standards in future trials as well as predicting endovascular treatment failure in patients with CLTI.43–44
The future
The lack of patient and public awareness, high quality randomised data and disparity in treatment algorithms worldwide is concerning, given that PAD is common and has relatively poor outcomes. A significant effort is required on a worldwide scale from clinicians, researchers, health care providers and public health to address these highlighted shortcomings. In particular, more work is needed to clarify the role of therapies in APAD to prevent deterioration, defining best medical treatment for those with symptomatic disease and revascularisation options for those with end-stage PAD, with the hope of improving long-term outcomes both in terms of limb and life.
Key messages
There is an impending global epidemic in peripheral artery disease (PAD) due to increasing levels of diabetes, hypertension, smoking and end-stage renal disease
Such patients have poorer health outcomes than aged-matched populations with other cardiovascular disease
There is a lack of robust evidence to guide treatment in all forms of PAD that urgently needs addressing
A global, public health effort is required to boost patient and public awareness and improve health outcomes in patients with PAD
Conflicts of interest
AG has received honoraria from Bayer. MAP, RB and OF: none declared.
Matthew A Popplewell Academic Clinical Lecturer in Vascular Surgery
1. Fowkes FGR, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet 2013;382:1329–40. https://dx.doi.org/10.1016/S0140-6736(13)61249-0
2. Sigvant B, Wiberg-Hedman K, Bergqvist D, et al. A population-based study of peripheral arterial disease prevalence with special focus on critical limb ischemia and sex differences. J Vasc Surg 2007;45:1185–91. https://dx.doi.org/10.1016/j.jvs.2007.02.004
3. Fowkes FGR, Murray GD, Butcher I, et al. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA 2008;300:197–208. https://dx.doi.org/10.1001/jama.300.2.197
5. Tang EW, Wong C-K, Herbison P. Global Registry of Acute Coronary Events (GRACE) hospital discharge risk score accurately predicts long-term mortality post acute coronary syndrome. Am Heart J 2007;153:29–35. https://dx.doi.org/10.1016/j.ahj.2006.10.004
6. Sigvant B, Lundin F, Wahlberg E. The risk of disease progression in peripheral arterial disease is higher than expected: a meta-analysis of mortality and disease progression in peripheral arterial disease. Eur J Vasc Endovasc Surg 2016;51:395–403. https://dx.doi.org/10.1016/j.ejvs.2015.10.022
7. National Institute for Health and Care Excellence. Lower limb peripheral arterial disease: diagnosis and management (Clinical Guideline 147). London: NICE, 2012. http://www.nice.org.uk/guidance/CG147
8. McDermott MM, Fried L, Simonsick E, Ling S, Guralnik JM. Asymptomatic peripheral arterial disease is independently associated with impaired lower extremity functioning: the women’s health and aging study. Circulation 2000;101:1007–12.
9. Ogren M, Hedblad B, Engstrom G, Janzon L. Prevalence and prognostic significance of asymptomatic peripheral arterial disease in 68-year-old men with diabetes. Results from the population study “Men born in 1914” from Malmo, Sweden. Eur J Vasc Endovasc Surg 2005;29:182–9. https://doi.org/10.1016/j.ejvs.2004.11.013
10. Fowkes FGR, Price JF, Stewart MCW, et al. Aspirin for prevention of cardiovascular events in a general population screened for a low ankle brachial index: a randomized controlled trial. JAMA 2010;303:841–8. https://dx.doi.org/10.1001/jama.2010.221
12. Guirguis-Blake JM, Evans C V, Redmond N, Lin JS. Screening for peripheral artery disease using the ankle-brachial index: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2018;320:184–96. https://dx.doi.org/10.1001/jama.2018.4250
13. Fowkes FGR, Aboyans V, Fowkes FJI, McDermott MM, Sampson UKA, Criqui MH. Peripheral artery disease: epidemiology and global perspectives. Nat Rev Cardiol 2017;14:156–70. https://dx.doi.org/10.1038/nrcardio.2016.179
14. Sartipy F, Sigvant B, Lundin F, Wahlberg E. Ten year mortality in different peripheral arterial disease stages: a population based observational study on outcome. Eur J Vasc Endovasc Surg 2018;55:529–36. https://dx.doi.org/10.1016/j.ejvs.2018.01.019
15. Sansone R, Busch L, Langhoff R. [Update ESC-Guideline 2017: Focus on PAD]. Dtsch Med Wochenschr 2018;143:1455–9. https://dx.doi.org/10.1055/a-0588-7317
16. Anand SS, Bosch J, Eikelboom JW, et al. Rivaroxaban with or without aspirin in patients with stable peripheral or carotid artery disease: an international, randomised, double-blind, placebo-controlled trial. Lancet 2018;391:219–29. https://dx.doi.org/10.1016/S0140-6736(17)32409-1
17. Wallentin L, Becker RC, Budaj A, et al. for the PLATO investigators. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2009;361:1045–57. https://dx.doi.org/10.1056/NEJMoa0904327
18. Hiatt WR, Fowkes FGR, Heizer G, et al. Ticagrelor versus clopidogrel in symptomatic peripheral artery disease. N Engl J Med 2017;376:32–40. https://dx.doi.org/10.1056/NEJMoa1611688
19. Soden PA, Zettervall SL, Ultee KHJ, et al. Dual antiplatelet therapy is associated with prolonged survival after lower extremity revascularization. J Vasc Surg 2016;64:1633–44.e1. https://dx.doi.org/10.1016/j.jvs.2016.05.098
20. O’Donnell TFX, Deery SE, Darling JD, et al. Adherence to lipid management guidelines is associated with lower mortality and major adverse limb events in patients undergoing revascularization for chronic limb-threatening ischemia. J Vasc Surg 2017;66:572–8. https://dx.doi.org/10.1016/j.jvs.2017.03.416
21. Diehm C, Allenberg JR, Pittrow D, et al. Mortality and vascular morbidity in older adults with asymptomatic versus symptomatic peripheral artery disease. Circulation 2009;120:2053–61. https://dx.doi.org/10.1161/CIRCULATIONAHA.109.865600
22. Smith GD, Shipley MJ, Rose G. Intermittent claudication, heart disease risk factors, and mortality. The Whitehall Study. Circulation 1990;82:1925–31.
23. Steg PG, Bhatt DL, Wilson PWF, et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA 2007;297:1197–206. https://dx.doi.org/10.1001/jama.297.11.1197
24. Subherwal S, Patel MR, Kober L, et al. Peripheral artery disease is a coronary heart disease risk equivalent among both men and women: results from a nationwide study. Eur J Prev Cardiol 2015;22:317–25. https://dx.doi.org/10.1177/2047487313519344
25. Bhatt DL, Eagle KA, Ohman EM, et al. Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA 2010;304:1350–7. https://dx.doi.org/10.1001/jama.2010.1322
27. Bermingham SL, Sparrow K, Mullis R, et al. The cost-effectiveness of supervised exercise for the treatment of intermittent claudication. Eur J Vasc Endovasc Surg 2013;46:707–14. https://dx.doi.org/10.1016/j.ejvs.2013.09.005
28. Popplewell MA, Bradbury AW. Why do health systems not fund supervised exercise programmes for intermittent claudication? Eur J Vasc Endovasc Surg 2014;48:608–10. https://dx.doi.org/10.1016/j.ejvs.2014.07.008
29. Pandey A, Banerjee S, Ngo C, et al. Comparative efficacy of endovascular revascularization versus supervised exercise training in patients with intermittent claudication: Meta-analysis of randomized controlled trials. JACC Cardiovasc Interv 2017;10:712–24. https://dx.doi.org/10.1016/j.jcin.2017.01.027
30. Harwood AE, Smith GE, Broadbent E, Cayton T, Carradice DCI. Access to supervised exercise services for peripheral vascular disease patients: which factors determine the current provision of supervised exercise in the UK. R Coll Surg Bull 2017:207–11. https://dx.doi.org/10.1308/rcsbull.2017.207
31. Hussain MA, Al-Omran M, Mamdani M, et al. Efficacy of a guideline-recommended risk-reduction program to improve cardiovascular and limb outcomes in patients with peripheral arterial disease. JAMA Surg 2016;151:742–50. https://dx.doi.org/10.1001/jamasurg.2016.0415
32. Rosenfield K, Jaff MR, White CJ, et al. Trial of a paclitaxel-coated balloon for femoropopliteal artery disease. N Engl J Med 2015;373:145–53. https://dx.doi.org/10.1056/NEJMoa1406235
33. Scheinert D, Duda S, Zeller T, et al. The LEVANT I (Lutonix paclitaxel-coated balloon for the prevention of femoropopliteal restenosis) trial for femoropopliteal revascularization: first-in-human randomized trial of low-dose drug-coated balloon versus uncoated balloon angioplasty. JACC Cardiovasc Interv 2014;7:10–9. https://dx.doi.org/10.1016/j.jcin.2013.05.022
34. Schneider PA, Laird JR, Tepe G, et al. Treatment effect of drug-coated balloons is durable to 3 years in the femoropopliteal arteries: long-term results of the IN.PACT SFA randomized trial. Circ Cardiovasc Interv 2018;11:e005891. https://dx.doi.org/10.1161/CIRCINTERVENTIONS.117.005891
35. Dake MD, Ansel GM, Jaff MR, et al. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the Zilver PTX randomized trial. Circulation 2016;133:1472–83; discussion 1483. https://dx.doi.org/10.1161/CIRCULATIONAHA.115.016900
36. Katsanos K, Spiliopoulos S, Kitrou P, Krokidis M, Karnabatidis D. Risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery of the leg: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc 2018;7(24):e011245. https://dx.doi.org/10.1161/JAHA.118.011245
37. Adam DJ, Beard JD, Cleveland T, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet 2005;366:1925–34. https://dx.doi.org/10.1016/S0140-6736(05)67704-5
38. Popplewell MA, Davies HOB, Narayanswami J, et al. A comparison of outcomes in patients with infrapopliteal disease randomised to vein bypass or plain balloon angioplasty in the bypass vs. angioplasty in severe ischaemia of the leg (BASIL) trial. Eur J Vasc Endovasc Surg 2017;54:195–201. https://dx.doi.org/10.1016/j.ejvs.2017.04.020
39. Popplewell MA, Davies H, Jarrett H, et al. Bypass versus angioplasty in severe ischaemia of the leg – 2 (BASIL-2) trial: study protocol for a randomised controlled trial. Trials 2016;17:11. https://dx.doi.org/10.1186/s13063-015-1114-2
40. Hunt BD, Popplewell MA, Davies H, et al. Balloon versus stenting in severe ischaemia of the leg-3 (BASIL-3): study protocol for a randomised controlled trial. Trials 2017;18:224. https://dx.doi.org/10.1186/s13063-017-1968-6
41. Menard MT, Farber A, Assmann SF, et al. Design and rationale of the best endovascular versus best surgical therapy for patients with critical limb ischemia (BEST-CLI) trial. JAMA 2016;5:pii: e003219. https://dx.doi.org/10.1161/JAHA.116.003219
42. Almasri J, Adusumalli J, Asi N, et al. A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia. J Vasc Surg 2018;68:624–33. https://dx.doi.org/10.1016/j.jvs.2018.01.066
43. Conte MS, Bradbury AW, Kolh P, et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur J Vasc Endovasc Surg 2019;58(1S):S1-S109.e33. https://dx.doi.org/10.1016/j.ejvs.2019.05.006
44. Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg 2019;69(6):3S-125S.e40. https://dx.doi.org/10.1016/j.jvs.2019.02.016
Notes on dosing recommendations from Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics)
Xarelto 2.5 mg twice daily, coadministered with a daily dose of 75–100 mg aspirin, is indicated for the prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral artery disease (PAD) at high risk of ischaemic events.
The COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial discussed in this supplement compared both Xarelto 2.5 mg twice-daily plus aspirin and also Xarelto 5 mg twice-daily without aspirin, versus aspirin alone. Results for both comparisons are provided reflecting the original study publication.
Please note, however, that Xarelto 5 mg twice-daily is not a licensed dosage regimen for the above, nor for any other therapeutic indication.
Disclaimer: Medinews Cardiology Limited advises healthcare professionals to consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews Cardiology Limited cannot accept responsibility for any errors in prescribing which may occur.
Authors: Jeffrey A Marbach, Aws S Almufleh, Derek So, Aun-Yeong Chong
Jeffrey A Marbach Interventional Cardiology Fellow
Aws S Almufleh Cardiology Fellow (CAPITAL Research Group) and Advanced Heart Failure and Transplant Cardiology Fellow (Brigham and Women’s Hospital, Harvard Medical School)
CAPITAL Research Group, University of Ottawa Heart Institute, 40 Ruskin Street, Ottawa, K1Y 4W7, Ontario, Canada
Sponsorship Statement:
Bayer plc. commissioned and funded this supplement. The company has reviewed the data to ensure factual accuracy in relation to Bayer products and compliance with industry guidelines.
For notes on dosing recommendations for Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics) please see the box at the foot of this page.
Rivaroxaban prescribing information current at the time of publication is available here.
Job code: PP-XAR-GB-1131
Date of preparation: January 2020
Over 200 million individuals are living with peripheral artery disease (PAD), which represents the third leading cause of atherosclerotic morbidity and mortality. Though intermittent claudication is the hallmark symptom of chronic PAD, only a minority of patients with PAD are symptomatic. Yet, even asymptomatic PAD is an important cardiovascular risk factor. Patients at risk for PAD should undergo a thorough assessment of cardiovascular risk factors and a comprehensive vascular evaluation. The primary focus of PAD management is risk factor modification to improve prognosis and amelioration of symptoms. Herein, we review the clinical presentation of atherosclerotic PAD, the appropriate diagnostic investigations, and the available medical and surgical management options.
Introduction
Peripheral artery disease (PAD) refers to all arterial disease outside of the coronary arteries and the aorta.1 It is estimated that over 200 million individuals are living with PAD globally.2,3 In the Western world, one in five adults over the age of 75 has PAD, including over 40 million Europeans.3-6 Though the prevalence of PAD is already at endemic levels worldwide, ageing populations and the increasing burden of chronic disease (i.e. hypertension, dyslipidaemia, diabetes mellitus, smoking) will contribute to further increases in the incidence and prevalence of PAD in the coming decades.2,3 As a consequence, PAD is the third leading cause of atherosclerotic morbidity and mortality behind coronary artery disease (CAD) and stroke.3,7
Unfortunately, the overall risk to patients with PAD is not solely due to the underlying peripheral arterial involvement. Patients with evidence of PAD are also at substantially increased risk of cardiovascular events in other vascular beds. For example, myocardial infarction (MI) and stroke may represent over 60% of deaths in patients with asymptomatic carotid atherosclerosis, thereby establishing the diagnosis of PAD as an important cardiovascular risk factor.8-10 Despite the abundance of PAD and its devastating consequences, PAD remains underdiagnosed and undertreated throughout Europe, highlighting a significant unmet clinical need.1,11 Below we review the clinical presentation of atherosclerotic PAD, the appropriate diagnostic investigations, and the available medical and surgical management options.
Pathophysiology and clinical presentation
PAD is frequently asymptomatic, though in a minority of cases acute arterial occlusion is the initial presentation. Abrupt occlusion of the carotid/vertebral, mesenteric, or extremity arteries can result in acute cerebrovascular events, acute mesenteric ischaemia, and acute limb ischaemia, respectively. These events are clinical emergencies with high morbidity and mortality requiring immediate diagnosis and treatment.1,7
In comparison, the majority of patients with indolent chronic atherosclerotic PAD present a far greater diagnostic challenge. The classical symptom of PAD – intermittent claudication – is an inherently unreliable indicator of the presence of disease.7 Studies have demonstrated that over 90% of individuals with PAD will not have classical symptoms. It is estimated that among patients with PAD, around 50% are likely to have atypical leg symptoms, and only 10–20% will present with intermittent claudication. Nevertheless, among asymptomatic patients with PAD up to 8% will have significant disease on non-invasive testing.3,4,12,13 Therefore, clinical screening of at-risk individuals supplemented by non-invasive testing may be necessary to adequately identify patients with PAD.
Diagnostic assessment
Clinical evaluation – history and examination
The initial evaluation of both symptomatic and asymptomatic PAD should attempt to ascertain cardiovascular risk through a detailed assessment of the patient’s symptoms and clinical history, in order to mitigate complications. Documenting the patient’s past medical history is crucial to identify important modifiable cardiovascular risk factors, such as known coronary or cerebrovascular disease, diabetes mellitus, aortic aneurysm, hypertension, dyslipidaemia, and chronic kidney disease.7 A family history of early onset PAD is associated with a three-fold increase in an individual’s risk, which is similar to the risk increase associated with smoking.14,15 Similarly, a detailed social history is crucial for evaluation of physical activity, dietary habits, and tobacco use, all of which have important management and prognostic implications in PAD.1
After establishing a patient’s risk factors for PAD, a thorough vascular examination is essential. This should include palpation of peripheral pulses in all four extremities, auscultation for carotid, renal and femoral bruits, examination of the lower extremities for evidence of chronic ischaemia (hair loss, non-healing wounds, ulcers, etc.) and bilateral blood pressure measurements.7,16 Though the sensitivity of physical exam findings for PAD is modest (58.2%), identification of a femoral bruit or any palpable pulse abnormality each have a likelihood ratio of more than four for the diagnosis of PAD.17,18 Both femoral and carotid bruits have been validated as independent risk factors for adverse cardiovascular events.1,19,20 In a meta-analysis of over 17,000 patients, the presence of a carotid bruit was associated with a two-fold increase in myocardial infarction (MI) and a two-and-a-half fold increase in cardiovascular death.19
Ankle-brachial pressure index and toe brachial pressure index
‘An ankle-brachial pressure index of <0.9 is considered diagnostic of PAD’
Following a comprehensive history and physical examination, patients suspected of having undiagnosed atherosclerotic PAD should undergo further non-invasive, confirmatory testing. The initial test of choice for diagnosing lower extremity PAD is the ankle-brachial index (ABI).1,7 The ABI is determined by measuring the systolic blood pressure in the patients brachial artery (both arms), while the patient is in the supine position, and dividing the highest measurement by the patient’s systolic blood pressure in their dorsalis pedis or posterior tibial artery (highest of the two).6,21 An ABI between 1.00 and 1.40 is considered in the normal range, and a value <0.90 is considered diagnostic of PAD.22 Calcified vessels that are unable to be appropriately compressed, which are present in 80% of patients with diabetes and 20% of patients without diabetes, can result in erroneously elevated ABI measurements.23 Further testing is therefore required in patients with an ABI of >1.40 and, with a normal ABI in those patients with diabetes, prior to PAD being excluded.6,7 In these instances obtaining a toe-brachial pressure index (TBPI) or a direct toe systolic pressure measurement with waveform analysis has been proven more reliable.24,25 Patients with an ABI between 0.90 and 1.00 also require further diagnostic testing, which may be in the form of post-exercise ABIs or imaging as discussed below.
Importantly, while the guidelines from the European Society of Cardiology (ESC) and the National Institute for Health and Care Excellence (NICE) both recommend ABI as the initial diagnostic investigation in individuals with suspected PAD, this should not be construed as a screening recommendation for all individuals. In a recent systematic review for the US Preventative Services Task Force, the authors found that diagnostic accuracy of ABI in an unselected population had a sensitivity of only 7–34%, compared with magnetic resonance angiography (MRA), and is therefore not adequately sensitive to screen for PAD.26 Its lower cost and powerful prognostic utility, however, justifies its place as the first tool for non-invasive evaluation of patients with suspected PAD.27,28
Imaging techniques
Multiple imaging modalities have established effectiveness in diagnosing PAD and assessing appropriateness for revascularisation. Currently accepted modalities, which include duplex ultrasound (DUS), computed tomography angiography (CTA), and MRA, are all able to identify, localise, and assess the severity of vascular lesions.1,6,7 Accordingly, the choice of modality must take into consideration both patient-related and non-patient factors. Patient-related factors include radiation exposure (CTA), contrast agent allergies (iodine-CTA), chronic kidney disease precluding contrast agents (iodine-CTA, gadolinium-MRA), and presence of implanted devices (e.g. permanent pacemakers, implantable cardioverter/defibrillators) that may be contraindicated in an MRI. Non-patient factors include availability of the test, local expertise, and cost.1,7 Based on these considerations, the ESC and the NICE guidelines recommend DUS as the first-line imaging technique in patients being considered for revascularisation, and MRA in those who require further imaging.1,6
Improving prognosis
As outlined above, patients with PAD are at increased risk of cardiovascular events in vascular territories outside of those with documented disease. The importance of identifying and treating concomitant risk factors cannot be overstated. Unfortunately, several previous investigations have demonstrated that PAD patients are less likely to receive aggressive medical management than patients with cerebrovascular or coronary artery disease.11,29 Once the diagnosis of PAD has been established, a comprehensive treatment strategy that focuses on risk factor modification and improving prognosis should be promptly instituted.
Risk factor modification
Risk factor reduction begins with non-pharmacological lifestyle modification strategies that must be tailored to each patient’s specific risk factors. Smoking is one of the most common risk factors among patients with PAD; an extensive body of literature has demonstrated the association between smoking and cardiovascular events, including an increased risk of amputation.30–32 However, the evidence has also demonstrated that smoking cessation leads to a rapid reduction in cardiovascular risk.30 Additional lifestyle modifications such as maintaining a healthy weight, regular physical exercise, and a healthy diet are also important.33
Pharmacologic treatments to reduce cardiovascular risk in patients with PAD are primarily targeted at three diseases: hypertension, diabetes mellitus, and dyslipidaemia. All patients with PAD should aim for a blood pressure goal of at least <140/90 mmHg in order to reduce cardiovascular events; angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARB) should be considered as a first-line therapy, based on evidence supporting a reduction in cardiovascular events in patients with PAD.1,34–37
Nevertheless, the appropriate antihypertensive choice should also take into consideration any other comorbid conditions a patient might have (heart failure, CAD, or chronic kidney disease). In patients with diabetes, strict glycaemic control (HbA1c <7%) is strongly recommended through coordination of the healthcare team.1,7
The current ESC guidelines recommend that all patients with PAD should maintain low-density lipoprotein (LDL) cholesterol <1.8 mmol/L.1,32 Statins should be the primary pharmaceutical treatment used to achieve this LDL target based on extensive literature demonstrating an increase in maximal walking distance, and a reduction in both cardiovascular events and all-cause mortality.38–42 In patients unable to tolerate statin therapy, or unable to reach target LDL-cholesterol goals on maximally tolerated statin doses, clinicians should consider adding ezetimibe or a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor based on recent evidence demonstrating a reduction in cardiovascular events.43,44
Antithrombotic therapies
Antiplatelet agents
Antiplatelet therapy, with either aspirin (ASA 75–325 mg/day orally) or clopidogrel (75 mg/day orally) is recommended in all patients with symptomatic PAD, as well as those with asymptomatic carotid artery stenosis to reduce the risk of cardiovascular events.1 Evidence supporting the efficacy of ASA primarily comes from a significant reduction in major adverse cardiovascular events (MACE) in patients with PAD and intermittent claudication (ASA 6.4% vs. placebo 7.9%; p=0.004).45 These results were not reproducible in asymptomatic patients, thus antiplatelet therapy in patients with asymptomatic lower extremity PAD is not recommended.46,47 When compared with ASA, clopidogrel resulted in reduced cardiovascular mortality (HR 0.76 [95%CI 0.64 to 0.91]) and MACE (HR 0.78 [95%CI 0.65 to 0.93]) among symptomatic PAD patients.48
The EUCLID (Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease) trial randomised over 13,800 patients with symptomatic PAD to ticagrelor monotherapy (90 mg twice daily) or clopidogrel monotherapy (75 mg once daily). At a median follow-up of 30 months, ticagrelor failed to demonstrate a reduction in MACE (HR 1.02 [95%CI 0.92 to 1.13]; p=0.65), or acute limb ischaemia (HR 1.03 [95%CI 0.79 to 1.33]; p=0.49).49,50
Evidence supporting the utility of dual antiplatelet therapy (DAPT) for PAD is limited. The primary evidence for DAPT with clopidogrel comes from a post hoc analysis of the CHARISMA (Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilisation, Management and Avoidance) trial, where symptomatic and asymptomatic patients with PAD had fewer MIs and strokes, but higher rates of bleeding.51 Similarly, a subanalysis of the DAPT trial, which randomised 11,648 patients 12-months post coronary stenting to an additional 18-month of DAPT therapy (ASA + clopidogrel or prasugrel) or ASA, found that the risk reduction with DAPT in PAD patients were similar to those observed in patients without PAD.52 Finally, in a substudy of the PEGASUS-TIMI 54 (Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin) trial, investigators demonstrated that while PAD patients benefitted similarly from extended DAPT (ASA + ticagrelor) in terms of relative risk reduction, the absolute risk reduction was even greater.53 As these encouraging results are solely from post hoc analyses, current guidelines recommend against empiric DAPT, with the exception of patients who have undergone recent percutaneous revascularisation (carotid artery stenting, peripheral percutaneous stenting).1,7
Anticoagulants
Until recently, there has been no evidence to support anticoagulation in the management of PAD. Therefore previous guidelines did not recommend oral anticoagulation in the absence of an alternative indication.1,7 However, recent results from the COMPASS (Rivaroxaban for the Prevention of Cardiovascular Events in Coronary or Peripheral Artery Disease) trial – which evaluated the efficacy of rivaroxaban alone or in combination with ASA in secondary prevention of cardiovascular events – have demonstrated a reduction in MACE in patients receiving low-dose rivaroxaban (2.5 mg twice daily) combined with ASA (100 mg once daily).54 A substudy of patients with PAD confirmed the reduction in MACE in the group receiving low-dose rivaroxaban and ASA.55Table 1 summarises ‘net clinical benefit’ end points from these analyses, comprising composites of adverse cardiovascular and bleeding outcomes. These data confirm that the combination of low-dose rivaroxaban + ASA provides superior net clinical benefit versus ASA alone.
Table 1. Summary of ‘net clinical benefit’ outcomes from the COMPASS trial
Hazard ratio (95%CI) for stated treatment vs. aspirin alone
Main cohort (n=27,395)
PAD cohort (n=7,470)*
Cardiovascular death, myocardial infarction, stroke, critical organ or fatal bleeding (prespecified end point)
Rivaroxaban 2.5 mg twice daily + aspirin
0.80 (0.70 to 0.91), p<0.001
0.75 (0.60 to 0.94), p=0.011
Rivaroxaban 5 mg twice daily alone#
0.94 (0.84 to 1.07), p=0.36
0.92 (0.75 to 1.13), p=0.43
Compiled from data represented in Eikelboom JW et al.54 and Anand SS et al.55
Key: *patients in this cohort had evidence of peripheral artery disease (PAD) of the lower extremities (previous peripheral
bypass surgery or angioplasty, limb or foot amputation, intermittent claudication with objective evidence of peripheral artery
disease), of the carotid arteries (previous carotid artery revascularisation or asymptomatic carotid artery stenosis ≥50%), or
coronary artery disease with ankle–brachial index <0.90. Patients in the main cohort had evidence of PAD, coronary artery
disease, or both. #Rivaroxaban 5 mg twice daily is not a licensed dosage regimen for any indication; results are included for
completeness. Statistically significant hazard ratios <1 signify clinical benefit for rivaroxaban-based regimens vs. aspirin alone
Managing symptoms
Exercise therapy
The mainstay of treatment among patients with chronic, non-limb threatening PAD is exercise therapy. The benefits of symptom improvement and quality of life have been well demonstrated in randomised trials, as well as a systematic review including over 1,800 patients.56 When compared to usual care, exercise therapy was found to increase the mean maximal walking time by 4.51 minutes (95%CI 3.11 to 5.92), the mean pain-free walking distance by 82.29 metres (95%CI 71.86 to 92.72), and the mean maximum walking distance by 108.99 metres (95%CI 38.20 to 179.78). Additional investigations demonstrated the benefits of supervised exercise therapy over unsupervised therapy, though both were superior to placebo.1,57 Based on these results, all patients with PAD should initially be managed with exercise therapy prior to considering additional pharmaceutical or revascularisation options.
Pharmaceutical treatments
Several agents have also been studied for their role in improving intermittent claudication symptoms. Cilostazol, naftidrofuryl, and pentoxifylline have the largest body of evidence. There have been two systematic reviews evaluating walking distance and quality of life measures with these medications as compared to placebo.42,58 Momsen et al. found that cilostazol, naftidrofuryl oxalate, and pentoxifylline all demonstrated significant improvements in maximal walking distance. These results, however, varied widely between studies, were relatively modest (60–90 metres), and were less robust than the improvements seen with statins (100 metres).42 In addition to improving walking distance, statins were found to significantly improve patients’ quality of life. When considered with the evidence discussed above demonstrating a reduction in cardiovascular events, statins become the obvious pharmaceutical option of choice in the initial management of symptomatic PAD.59
The role for cilostazol, naftidrofuryl, and pentoxifylline as second-line agents is somewhat controversial and societal guidelines provide varying recommendations. US guidelines recommend cilostazol as an effective treatment to improve symptoms and walking distance (Class I, Level A), and state that pentoxifylline is not effective in the treatment of claudication (Class III, Level B).7 Naftidrofuryl oxalate has not been approved in the USA. The NICE guidelines recommend naftidrofuryl oxalate only when supervised exercise has not led to satisfactory improvement in symptoms and the patient does not want to be referred for revascularisation.6 Finally, the ESC guidelines discuss the evidence for these medications but do not provide a recommendation for their use based on the variability in the available evidence, and the lack of evidence supporting their use in addition to statins.
Revascularisation
Only a very small percentage of symptomatic PAD patients will have critical limb ischaemia requiring revascularisation. Importantly, aside from symptomatic relief and quality of life improvement, revascularisation has not been shown to improve overall prognosis.6,7 Due to the subjectivity of claudication symptoms and the variable impact of these symptoms on an individual’s quality of life, decisions to pursue revascularisation must be individualised. Once individual patient factors such as comorbidities and surgical risk have been considered, the appropriateness to proceed with endovascular or surgical revascularisation should be undertaken in consultation with an expert. In general, percutaneous revascularisation options (balloon angioplasty, stenting, atherectomy) are preferred to surgery as the first-line strategy, though again this must be individualised to the patient and is dependent upon the specific anatomy (aorto-iliac vs. femoro-popliteal), the patient’s surgical risk, the likelihood of achieving a successful result, and previous treatment options (prior percutaneous procedures).6 If surgical bypass is the chosen strategy for infra-inguinal revascularisation, autologous vein grafts should be chosen over prosthetic grafts due to their superior patency rates.60,61
In the setting of critical limb ischaemia, a multidisciplinary vascular team should be involved in patient evaluation and management with the goal of achieving adequate revascularisation and minimal tissue loss. Whether surgical or percutaneous revascularisation offers an advantage over the other is still under investigation, though the available randomised studies suggest that these strategies offer comparable amputation-free survival.62,63 Amputation should be considered a last line of therapy in situations where all other revascularisation options have failed.6 Finally, acute limb ischaemia due to complete vascular occlusion is considered a medical emergency and necessitates rapid, time-sensitive evaluation and management, details of which are beyond the scope of this review.
Conclusion
PAD is clearly an important cause of cardiovascular morbidity and mortality throughout the world and its prevalence continues to rise. Regardless of symptoms, PAD places patients at substantially increased risk of adverse cardiovascular events. Consequently, treatment strategies aim to reduce patient symptoms while simultaneously improving prognosis. Until recently one major limitation to the currently available treatments was the lack of therapies providing a prognostic benefit in PAD. The results from the COMPASS trial suggest that low-dose rivaroxaban in combination with ASA may be able to fill this void and allow clinicians to take a significant step forward in the management of PAD in the 21st century.
Key messages
Peripheral artery disease (PAD) is endemic throughout the world and its prevalence will continue to increase over the coming decades
The majority of patients living with PAD are asymptomatic yet have a substantially greater cardiovascular risk than the general population
Individuals at risk for PAD should undergo a thorough assessment of cardiovascular risk factors and a comprehensive vascular evaluation, followed by diagnostic testing in individuals requiring further assessment
The main goals in the management of PAD are:
improving patient prognosis through risk factor modification (i.e. smoking cessation and treatment of hypertension, diabetes, and dyslipidaemia) and antithrombotic therapies
improvement of claudication symptoms through exercise therapy, pharmaceutical agents, and revascularisation
Conflicts of interest
None declared.
Jeffrey A Marbach Interventional Cardiology Fellow
Aws S Almufleh Cardiology Fellow (CAPITAL Research Group) and Advanced Heart Failure and Transplant Cardiology Fellow (Brigham and Women’s Hospital, Harvard Medical School)
1. Ricco J-B, Bartelink M-LEL, Bjorck M et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur Heart J 2018;39:763–821. https://doi.org/10.1093/eurheartj/ehx095
3. Fowkes FGR, Rudan D, Rudan I et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet 2013;382:1329–40. https://doi.org/10.1016/S0140-6736(13)61249-0
4. Fowkes FG, Housley E, Cawood EH et al. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol 1991;20:384–92.
5. Leng GC, Lee AJ, Fowkers FGR et al. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. Int J Epidemiol 1996;25:1172–81.
6. Layden J, Michaels J, Bermingham S, Higgins B, on behalf of the Guideline Development Group. Diagnosis and management of lower limb peripheral arterial disease: summary of NICE guidance. BMJ 2012;345:e4947. https://doi.org/10.1136/bmj.e4947
7. Gerhard-Herman MD, Gornik HL, Barrett C et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: Executive Summary. J Am Coll Cardiol 2017;69:1465–508. https://doi.org/10.1016/j.jacc.2016.11.008
8. Belcaro G, Nicolaides AN, Ramaswami G et al. Carotid and femoral ultrasound morphology screening and cardiovascular events in low risk subjects: a 10-year follow-up study (the CAFES-CAVE study(1)). Atherosclerosis 2001;156:379–87.
9. Giannopoulos A, Kakkos S, Abbott A et al. Long-term Mortality in Patients with Asymptomatic Carotid Stenosis: Implications for Statin Therapy. Eur J Vasc Endovasc Surg 2015;50:573–82. https://doi.org/10.1016/j.ejvs.2015.06.115
11. Pande RL, Perlstein TS, Beckman JA, Creager MA. Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004. Circulation 2011;124:17–23. https://doi.org/10.1177/1358863X12437600
12. Hirsch AT, Criqui MH, Treat-Jacobson D et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 2001;286:1317–24. https://doi.org/10.1001/jama.286.11.1317
13. Leng G, Fowkes F. The epidemiology of peripheral arterial disease. Vasc Med Rev 1993;4:5–18.
14. Valentine RJ, Guerra R, Stephan P et al. Family history is a major determinant of subclinical peripheral arterial disease in young adults. J Vasc Surg 2004;39:351–6. https://doi.org/10.1067/mva.2002.125848
15. Wassel CL, Loomba R, Ix JH et al. Family history of peripheral artery disease is associated with prevalence and severity of peripheral artery disease: the San Diego population study. J Am Coll Cardiol 2011;58:1386–92. https://doi.org/10.1016/j.jacc.2011.06.023
16. Santilli JD, Santilli SM. Chronic critical limb ischemia: diagnosis, treatment and prognosis. AFP 1999;59:1899.
17. Simel D, Khan N, Anand S, Simel D, Panju A. Peripheral arterial disease. In: Simel D, Rennie D, editors. The rational clinical examination: evidence-based clinical diagnosis. McGraw-Hill; 2009.
18. Armstrong DWJ, Tobin C, Matangi MF. The accuracy of the physical examination for the detection of lower extremity peripheral arterial disease. Can J Cardiol 2010;26:e346-350. https://doi.org/10.1016/S0828-282X(10)70467-0
19. Pickett CA, Jackson JL, Hemann BA, Atwood JE. Carotid bruits as a prognostic indicator of cardiovascular death and myocardial infarction: a meta-analysis. Lancet 2008;371:1587–94. https://doi.org/10.1016/S0140-6736(08)60691-1
20. Cournot M, Taraszkiewicz D, Cambou J-P et al. Additional prognostic value of physical examination, exercise testing, and arterial ultrasonography for coronary risk assessment in primary prevention. Am Heart J 2009;158:845–51. https://doi.org/10.1016/j.ahj.2009.08.017
21. McDermott MM, Mazor KM, Reed G et al. Attitudes and behavior of peripheral arterial disease patients toward influencing their physician’s prescription of cholesterol-lowering medication. Vasc Med 2010;15:83–90. https://doi.org/10.1177/1358863X09353653
22. Alavi A, Sibbald RG, Nabavizadeh R et al. Audible handheld Doppler ultrasound determines reliable and inexpensive exclusion of significant peripheral arterial disease. Vascular 2015;23:622–9. https://doi.org/10.1177/1708538114568703
24. Fagley RE, Haney MF, Beraud A-S et al. Critical care basic ultrasound learning goals for american anesthesiology critical care trainees: recommendations from an expert group. Anesthesia & Analgesia 2015;120:1041–53. https://doi.org/10.1213/ANE.0000000000000652
25. Migliacci R, Nasorri R, Ricciarini P, Gresele P. Ankle-brachial index measured by palpation for the diagnosis of peripheral arterial disease. Fam Pract 2008;25:228–32. https://doi.org/10.1093/fampra/cmn035
26. Guirguis-Blake JM, Evans CV, Redmond N, Lin JS. Screening for peripheral artery disease using the ankle-brachial index: an updated systematic review for the US Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality (US), 2018. Available at http://www.ncbi.nlm.nih.gov/books/NBK526319 (last accessed February 2018)
27. Ankle Brachial Index Collaboration. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA 2008;300:197–208. https://doi.org/10.1001/jama.300.2.197
28. Criqui MH, McClelland RL, McDermott MM et al. The ankle-brachial index and incident cardiovascular events in the MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol 2010;56:1506–12. https://doi.org/10.1016/j.jacc.2010.04.060
29. Krishnamurthy V, Munir K, Rectenwald JE et al. Contemporary outcomes with percutaneous vascular interventions for peripheral critical limb ischemia in those with and without poly-vascular disease. Vasc Med 2014;19:491–9. https://doi.org/10.1177/1358863X14552013
30. Bullen C. Impact of tobacco smoking and smoking cessation on cardiovascular risk and disease. Expert Rev Cardiovasc Ther 2008;6:883–95. https://doi.org/10.1586/14779072.6.6.883
31. Lim SS, Vos T, Flaxman AD et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2224–60. https://doi.org/10.1016/S0140-6736(12)61766-8
32. Piepoli MF, Hoes AW, Agewall S et al. [2016 European guidelines on cardiovascular disease prevention in clinical practice. The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts. Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation]. G Ital Cardiol (Rome) 2017;18:547–612. https://doi.org/10.1714/2729.27821
33. Graham I, Atar D, Borch-Johnsen K et al. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts). Eur J Cardiovasc Prev Rehabil 2007;14(suppl 2):E1-40. https://doi.org/10.1097/01.hjr.0000277984.31558.c4
34. Staessen JA, Thijs L, Gasowski J, Cells H, Fagard RH. Treatment of isolated systolic hypertension in the elderly: further evidence from the systolic hypertension in Europe (Syst-Eur) trial. Am J Cardiol 1998;82:20R-22R. https://doi.org/10.1016/S0002-9149(98)00752-8
35. Jaques H, National Institute for Health and Care Excellence (NICE). NICE guideline on hypertension. Eur Heart J 2013;34:406–8. https://doi.org/10.1093/eurheartj/ehs428
36. Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med 2000;342:145–53. https://doi.org/10.1056/NEJM200001203420301
37. ONTARGET Investigators, Yusuf S, Teo KK et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008;358:1547–59. https://doi.org/10.1056/NEJMoa0801317
38. Aung PP, Maxwell HG, Jepson RG, Price JF, Leng GC. Lipid-lowering for peripheral arterial disease of the lower limb. Cochrane Database Syst Rev 2007;CD000123. https://doi.org/10.1002/14651858.CD000123.pub2
39. Antoniou GA, Fisher RK, Georgiadis GS, Antoniou SA, Torella F. Statin therapy in lower limb peripheral arterial disease: Systematic review and meta-analysis. Vascul Pharmacol 2014;63:79–87. https://doi.org/10.1016/j.vph.2014.09.001
40. Kumbhani DJ, Steg PG, Cannon CP et al. Statin therapy and long-term adverse limb outcomes in patients with peripheral artery disease: insights from the REACH registry. Eur Heart J 2014;35:2864–72. https://doi.org/10.1093/eurheartj/ehu080
41. Heart Protection Study Collaborative Group. Randomized trial of the effects of cholesterol-lowering with simvastatin on peripheral vascular and other major vascular outcomes in 20,536 people with peripheral arterial disease and other high-risk conditions. J Vasc Surg 2007;45:645–54; discussion 653–4. https://doi.org/10.1016/j.jvs.2006.12.054
42. Momsen AH, Jensen MB, Norager CB, Madsen MR, Vestersgaard-Andersen T, Lindholt JS. Drug therapy for improving walking distance in intermittent claudication: a systematic review and meta-analysis of robust randomised controlled studies. Eur J Vasc Endovasc Surg 2009;38:463–74. https://doi.org/10.1016/j.ejvs.2009.06.002
43. Murphy SA, Cannon CP, Blazing MA et al. Reduction in total cardiovascular events with ezetimibe/simvastatin post-acute coronary syndrome: The IMPROVE-IT Trial. J Am Coll Cardiol 2016;67:353–61. https://doi.org/10.1016/j.jacc.2015.10.077
44. Sabatine MS, Giugliano RP, Keech AC et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017;376:1713–22. https://doi.org/10.1056/NEJMoa1615664
45. Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002;324:71–86. https://doi.org/10.1136/bmj.324.7329.71
46. Fowkes FG, Price JF, Stewart MCW et al. Aspirin for prevention of cardiovascular events in a general population screened for a low ankle brachial index: a randomized controlled trial. JAMA 2010;303:841–8. https://doi.org/10.1001/jama.2010.221
47. Belch J, MacCuish A, Campbell I et al. The prevention of progression of arterial disease and diabetes (POPADAD) trial: factorial randomised placebo controlled trial of aspirin and antioxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ 2008;337:a1840. https://doi.org/10.1136/bmj.a1840
48. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 1996;348:1329–39. https://doi.org/10.1016/S0140-6736(96)09457-3
49. Hiatt WR, Fowkes FGR, Heizer G et al. Ticagrelor versus clopidogrel in symptomatic peripheral artery disease. N Engl J Med 2017;376:32–40. https://doi.org/10.1056/NEJMoa1611688
51. Cacoub PP, Bhatt DL, Steg PG, Topol EJ, Creager MA, CHARISMA Investigators. Patients with peripheral arterial disease in the CHARISMA trial. Eur Heart J 2009;30:192–201. https://doi.org/10.1093/eurheartj/ehn534
52. Secemsky EA, Yeh RW, Kereiakes DJ et al. Extended duration dual antiplatelet therapy after coronary stenting among patients with peripheral arterial disease. JACC: Cardiovasc Interv 2017;10:942–54. https://doi.org/10.1016/j.jcin.2017.02.013
53. Bonaca MP, Bhatt DL, Storey RF et al. Ticagrelor for prevention of ischemic events after myocardial infarction in patients with peripheral artery disease. J Am Coll Cardiol 2016;67:2719–28. https://doi.org/10.1016/j.jacc.2016.03.524
54. Eikelboom JW, Connolly SJ, Bosch J et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017;377:1319–30. https://doi.org/10.1056/NEJMoa1709118
55. Anand SS, Bosch J, Eikelboom JW et al. Rivaroxaban with or without aspirin in patients with stable peripheral or carotid artery disease: an international, randomised, double-blind, placebo-controlled trial. Lancet 2018;391:219–29. https://doi.org/10.1016/S0140-6736(17)32409-1
57. Gommans LNM, Fokkenrood HJP, van Dalen HCW et al. Safety of supervised exercise therapy in patients with intermittent claudication. J Vasc Surg 2015;61:512-518.e2. https://doi.org/10.1016/j.jvs.2014.08.070
58. Stevens JW, Simpson E, Harnan S et al. Systematic review of the efficacy of cilostazol, naftidrofuryl oxalate and pentoxifylline for the treatment of intermittent claudication. Br J Surg 2012;99:1630–8. https://doi.org/10.1002/bjs.8895
59. Gargiulo G, Giugliano G, Brevetti L et al. Use of statins in lower extremity artery disease: a review. BMC Surg 2012;12(suppl 1):S15. https://doi.org/10.1186/1471-2482-12-S1-S15
60. Pereira CE, Albers M, Romiti M, Brochado-Neto FC, Pereira CAB. Meta-analysis of femoropopliteal bypass grafts for lower extremity arterial insufficiency. J Vasc Surg 2006;44:510–7. https://doi.org/10.1016/j.jvs.2006.04.054
62. Adam DJ, Beard JD, Cleveland T et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet 2005;366:1925–34. https://doi.org/10.1016/S0140-6736(05)67704-5
63. Bradbury AW, Adam DJ, Bell J et al. Multicentre randomised controlled trial of the clinical and cost-effectiveness of a bypass-surgery-first versus a balloon-angioplasty-first revascularisation strategy for severe limb ischaemia due to infrainguinal disease. The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial. Health Technol Assess 2010;14:1–210, iii–iv. https://doi.org/10.3310/hta14140
Notes on dosing recommendations from Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics)
Xarelto 2.5 mg twice daily, coadministered with a daily dose of 75–100 mg aspirin, is indicated for the prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral artery disease (PAD) at high risk of ischaemic events.
The COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial discussed in this supplement compared both Xarelto 2.5 mg twice-daily plus aspirin and also Xarelto 5 mg twice-daily without aspirin, versus aspirin alone. Results for both comparisons are provided reflecting the original study publication.
Please note, however, that Xarelto 5 mg twice-daily is not a licensed dosage regimen for the above, nor for any other therapeutic indication.
Disclaimer: Medinews Cardiology Limited advises healthcare professionals to consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews Cardiology Limited cannot accept responsibility for any errors in prescribing which may occur.
Birmingham City Hospital, Sandwell and West Birmingham Hospitals NHS Trust, Dudley Road, Birmingham, B18 7QH.
Sponsorship Statement:
Bayer plc. commissioned and funded this supplement. The company has reviewed the data to ensure factual accuracy in relation to Bayer products and compliance with industry guidelines.
For notes on dosing recommendations for Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics) please see the box at the foot of this page.
Rivaroxaban prescribing information current at the time of publication is available here.
Job code: PP-XAR-GB-1131
Date of preparation: January 2020
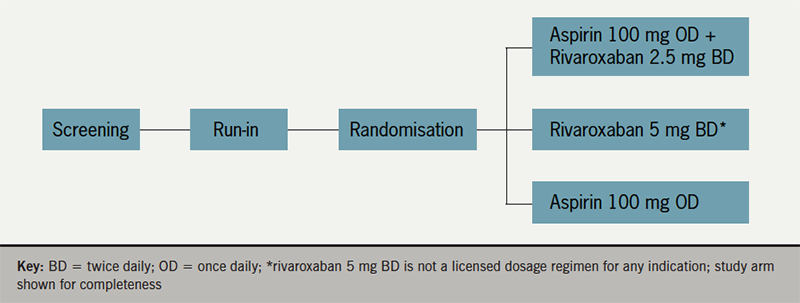
The COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial was a double-dummy, double-blind, multicentre, randomised clinical trial in patients with stable atherosclerotic vascular disease (sponsored by Bayer). Patients were randomised to one of three treatment groups: low-dose (2.5 mg twice daily) rivaroxaban plus aspirin (100 mg), higher dose (5 mg twice daily) rivaroxaban alone, or aspirin (100 mg) alone. The primary outcome, a composite of cardiovascular death, stroke, or myocardial infarction, occurred in fewer patients randomised to rivaroxaban plus aspirin, compared with aspirin alone. The study was terminated early due to the superiority of the combination therapy after a mean follow-up of 23 months. Major bleeding occurred more frequently in the combination therapy group. Twice-daily rivaroxaban 5 mg monotherapy did not significantly lower the risk of major adverse cardiovascular events versus aspirin alone (HR 0.90, p=0.12) and resulted in a significantly higher risk of major bleeding.
Background, epidemiology and rationale for the COMPASS study
One quarter of all deaths in the UK in 2017 occurred as a result of diseases of the heart and circulation.1 One in seven men and one in twelve women died from coronary heart disease (CHD).1 The presence of CHD doubles the risk of stroke,2 and more than 100,000 strokes occur in the UK each year.1 Although the mortality rate from circulatory diseases is declining due to advances in treatment,1,3 more than 100,000 deaths resulted from CHD or stroke combined in the UK each year.1 CHD and stroke are the two leading causes of death worldwide.4 Circulatory disease is also associated with a heavy burden of morbidity. For example, more than 200,000 hospital visits in the UK were due to myocardial infarction (MI) each year in 2015–2017.5 CHD cost the UK economy approximately £19 billion per annum.6
Current guidelines recommend secondary prevention therapy with a single antiplatelet agent and a lipid-lowering agent for patients with established cardiovascular disease. Despite this, the annual recurrent event rate in patients on this combination of medications is still up to 5–10% per year.7 A meta-analysis demonstrated superior secondary prevention of adverse cardiovascular outcomes with the use of high-intensity oral anticoagulation (with a target for international normalised ratio [INR] of >2.8), or moderate-intensity oral anticoagulation (INR 2–3) plus aspirin, compared with aspirin alone.8 High-intensity, but not moderate-intensity oral coagulation, was associated with higher risk of bleeding, including intracranial bleeding.8 Conversely, low-intensity oral anticoagulation (INR <2.0) combined with aspirin did not confer any benefit over aspirin alone but still increased major bleeding episodes. Maintenance of an optimum INR appears to be the key for achieving an optimum balance between efficacy and safety with this approach.8 Hence, anticoagulation alone or in combination has not been recommended routinely as secondary prevention for decades.
The WOEST (What is the Optimal Antiplatelet and Anticoagulant Therapy in Patients With Oral Anticoagulation and Coronary Stenting) trial was conducted in a patient population on long-term oral anticoagulation with warfarin, who underwent percutaneous coronary intervention (PCI).9 This trial compared ‘double therapy’ (addition of clopidogrel to the warfarin) with ‘triple therapy’ (addition of dual antiplatelet therapy [DAPT]). At one-year follow-up, double therapy reduced the risk of bleeding events, death, MI, stroke, and stent thrombosis. These findings suggest that clopidogrel plus warfarin may be equally effective as and safer than triple therapy in patients undergoing PCI. However, the study was limited by being non-blinded and underpowered for efficacy outcomes.
Rivaroxaban is a selective direct Factor Xa inhibitor used in the treatment and prevention of venous thromboembolism10–12 and for prevention of embolic stroke or systemic embolism in non-valvular atrial fibrillation.13 In the PIONEER AF-PCI (Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI) study, low-dose (15 mg once daily) and very-low-dose (2.5 mg twice daily) rivaroxaban was compared with warfarin plus antiplatelet therapy in patients with non-valvular atrial fibrillation (NVAF) post-PCI.14 This was a safety study with a primary safety end point of clinically significant bleeding.** There was a relative risk reduction of 39% in clinically significant bleeding with low-dose and very-low-dose rivaroxaban-based strategies when compared with warfarin-based triple therapy through 12 months (17.4% for combined rivaroxaban groups vs. 26.7% for vitamin K antagonist therapy, p<0.001). Based on the results with rivaroxaban 15 mg once daily, the SPC was updated for patients with NVAF who undergo PCI with stent placement.15
** A composite of Thrombolysis in Myocardial Infarction (TIMI) major or minor bleeding or bleeding requiring medical attention evaluated throughout the 12-month treatment period.
The ATLAS ACS 2-TIMI 51 (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome – Thrombolysis In Myocardial Infarction 51) trial demonstrated the efficacy of rivaroxaban 2.5 mg twice daily in patients with acute coronary syndrome (ACS).16 Treatment with rivaroxaban, in addition to single or dual antiplatelet therapy, was associated with a reduction in cardiovascular mortality and stent thrombosis, compared with placebo. There was an increase in major bleeding in ATLAS ACS 2-TIMI 51 with rivaroxaban 2.5 mg twice daily versus placebo, although no increase in fatal bleeding. This study proved that a very low dose (2.5 mg twice daily) of rivaroxaban combined with antiplatelet therapy is an effective treatment option in the management of patients with ACS.
The outcome of these studies has been favourable to the optimal combination of oral anticoagulation with an antiplatelet agent to reduce recurrent coronary events and cardiovascular mortality in patients with atherosclerotic cardiovascular disease. Pathophysiologically, it is logical to opt for combination therapy given the contribution of platelets, Factor X and thrombin in the formation of thrombus. Excess thrombin generation that persists beyond the acute phase plays an important role in recurrent thrombotic events.17 However, the combination of warfarin with antiplatelet therapy has not shown benefit in peripheral artery disease (PAD) and has led to major bleeding events, including intracranial bleeding.18
The COMPASS study
Design
COMPASS (ClinicalTrials.gov NCT01776424) was a double-blind, double-dummy, randomised trial with a 3×2 partial factorial design, conducted at 602 centres in 33 countries and funded by Bayer.19 The trial involved four periods: screening, run-in period, follow-up and washout. The main objective of the trial (figure 1) was to evaluate whether rivaroxaban 2.5 mg twice daily in combination with aspirin 100 mg once daily, or rivaroxaban 5 mg once daily alone, reduced recurrent cardiovascular events, with acceptable safety, compared with aspirin 100 mg once daily, in patients with stable atherosclerotic vascular disease (CAD and/or PAD). Further details of the randomisation are given below.
Figure 1. Key stages of the COMPASS trial
A further comparison of pantoprazole versus placebo was conducted in the trial participants not receiving proton pump inhibitor (not shown in figure 1). Hence the study was a 3×2 factorial design. The steering committee comprising Population Health Research Institute (PHRI) investigators, study leaders in each country and representatives of the study sponsor, developed the protocol, which was approved by the relevant health authorities and institutional review boards. All patients provided written, informed consent. Data analyses were performed at PHRI.
Box 1 shows key inclusion and exclusion criteria for the study. Eligible patients entered a run-in phase up to 30 days, during which they received a rivaroxaban-matched placebo twice daily and aspirin 100 mg once-daily, designed to identify patients who develop an adverse event, or who were unwilling or unable to adhere or not suitable for randomisation. Post-coronary artery bypass graft (CABG) surgery patients were randomised 4–14 days after the surgery and did not enter the run-in.
Box 1. Key inclusion and exclusion criteria for the COMPASS trial
Key inclusion criteria were:
Coronary artery disease, difined as one or more of:
myocardial infarction within the last 20 years
multi-vessel coronary disease with symptoms or with history of stable or unstable angina
multi-vessel coronary artery bypass grafting (CABG) surgery
Peripheral artery disease, defined as one or more of:
previous aorto-femoral bypass surgery, limb bypass surgery or percutaneous transluminal angioplasty revascularisation of the iliac or infra-inguinal arteries
previous limb or foot amputation for arterial vascular disease
history of intermittent claudication and one or more of:
ankle/arm blood pressure (BP) ratio <0.90
significant peripheral artery stenosis (≥50%) documented by angiography, or by duplex ultrasound
previous carotid revascularisation or asymptomatic carotid artery stenosis ≥50% as diagnosed by duplex ultrasound or angiography
Age 65 years, or age <65 years with documented atherosclerosis or revascularisation involving: at least two vascular beds or at least two additional risk factors (current smoking, diabetes mellitus, estimated glomerular filtration rate [eGFR <60 ml per minute, heart failure or non-lacunar ischaemic stroke ≥1 month earlier) Key exclusion criteria were:
high bleeding risk
recent stroke or previous haemorrhagic or lacunar stroke
severe heart failure (ejection fraction <30% or New York Heart Association class III or IV symptoms)
advanced stable kidney disease (eGFR <15 mL/min
use of dual antiplatelet therapy, anticoagulation, or other antithrombotic therapy
non-cardiovascular conditions deemed by the investigator to be associated with a poor prognosis.
Compiled from information presented in Eikelboom JW19 and ClinicalTrials.gov/ NCT01776424
Patients were randomised 1:1:1 ratio to receive rivaroxaban (2.5 mg twice daily) plus aspirin (100 mg once daily), rivaroxaban (5 mg twice daily) with an aspirin-matched placebo once daily, or aspirin (100 mg once daily) with a rivaroxaban-matched placebo twice daily, stratified according to centre and the use of proton-pump inhibitor therapy at the time of randomisation. Study aspirin was enteric-coated. Patients who were eligible for the proton-pump inhibitor randomisation were also randomly assigned in a 1:1 ratio to receive pantoprazole (40 mg once daily) or matched placebo. After randomisation, participants were seen at one and six months and then at six-month intervals.
Primary and secondary outcomes
The primary efficacy outcomes were the composite of cardiovascular death, stroke, or MI. The primary safety outcome was a modification of the International Society on Thrombosis and Haemostasis (ISTH) criteria for major bleeding and included fatal bleeding, symptomatic bleeding into a critical organ, bleeding into a surgical site requiring reoperation, and bleeding that led to hospitalisation (including presentation to an acute care facility without an overnight stay). However, the study considered as a major bleed any bleeding that led to acute presentation or hospitalisation.
The secondary efficacy outcomes were composites of ischaemic stroke, MI, acute limb ischaemia, or death from CHD, and of ischaemic stroke, MI, acute limb ischaemia, cardiovascular death, and death from any cause. Tertiary efficacy outcomes included individual components of the primary and secondary outcomes, as well as hospitalisation for cardiovascular causes, revascularisation, limb amputation, stent thrombosis, angina, heart failure, venous thromboembolism, resuscitated cardiac arrest, and a new diagnosis of cancer. The net-clinical-benefit outcome was the composite of cardiovascular death, stroke, MI, fatal bleeding, or symptomatic bleeding into a critical organ. The main outcome for the pantoprazole versus placebo randomisation was upper gastrointestinal complications.
COMPASS was an event-driven trial, with an expected control event rate of 3.3/100 person-years; it was designed to continue until at least 2,200 participants had a confirmed primary efficacy outcome, thereby providing 90% power to detect a 20% lower risk in each of the two comparisons of rivaroxaban versus aspirin.
Results of the COMPASS trial
A total of 27,395 patients who successfully completed the run-in phase or who were enrolled after CABG surgery were randomised; 2,320 participants did not complete the run-in phase and were excluded. The study period was three to four years. Baseline characteristics were similar in all three arms. The mean age was 68.2 years, 90.6% had a history of CAD, and 27.3% of PAD. Lipid-lowering agents were used by 89.8%.
The independent Data and Safety Monitoring Board recommended early termination of the randomised comparison of rivaroxaban with or without aspirin versus aspirin alone at the first formal interim analysis for efficacy (50% of planned events). This was due to observation of a consistent difference in the primary efficacy outcome in favour of rivaroxaban plus aspirin (z = −4.592). The z statistic for the comparison of rivaroxaban plus aspirin versus aspirin alone was larger than the prespecified 4 standard deviations.
Figure 2 summarises some key results from the trial.19,20 Primary outcome events occurred in 379 patients (4.1%) in rivaroxaban plus aspirin group, 448 (4.9%) in rivaroxaban alone group, and 496 (5.4%) in aspirin alone group. For the comparison of rivaroxaban (2.5 mg twice daily) plus aspirin with aspirin alone, the hazard ratio for the primary outcome was 0.76 (95% confidence interval [CI], 0.66 to 0.86; p<0.001). For the comparison of rivaroxaban (5 mg twice daily) alone with aspirin alone, the hazard ratio (HR) was 0.90 (95% CI, 0.79 to 1.03; p=0.12).
Figure 2. Selected outcomes from the COMPASS trial
The first secondary composite outcome occurred in 329 patients (3.6%) in the rivaroxaban-aspirin group and in 450 patients (4.9%) in the aspirin-alone group (HR 0.72; 95%CI, 0.63 to 0.83; p<0.001). The additional secondary composite outcome occurred in fewer patients in the rivaroxaban-plus-aspirin group than in the aspirin-alone group (389 patients [4.3%] vs. 516 patients [5.7%], HR 0.74 [95%CI, 0.65 to 0.85]; p<0.001). There were 313 deaths (3.4%) in the rivaroxaban-aspirin group compared with 378 (4.1%) in the aspirin-alone group (HR 0.82; 95% CI, 0.71 to 0.96; p=0.01). Formal testing of the secondary outcomes was not performed for rivaroxaban alone compared with aspirin alone because no significant effect was seen for the primary composite outcome.
More major bleeding events occurred in the rivaroxaban-plus-aspirin group than in the aspirin-alone group (288 patients [3.1%] vs. 170 patients [1.9%], HR 1.70 [95%CI 1.40 to 2.05]; p<0.001). Patients in the rivaroxaban-alone group also had more major bleeding events than in the aspirin alone group (255 patients [2.8%] vs.170 patients [1.9%], HR 1.51; [95%CI, 1.25 to 1.84]; p<0.001). Serious adverse events occurred in 721 patients (7.9%) assigned to rivaroxaban plus aspirin, 702 (7.7%) assigned to rivaroxaban alone, and 662 (7.3%) assigned to aspirin alone.
The composite net-clinical-benefit outcome of cardiovascular death, stroke, MI, fatal bleeding, or symptomatic bleeding into a critical organ was lower with rivaroxaban plus aspirin than with aspirin alone (431 patients [4.7%] vs. 534 patients [5.9%], HR 0.80 [95% CI, 0.70 to 0.91]; p<0.001).
A total of 7,470 patients had stable PAD or carotid artery disease, including 55% with symptomatic PAD of the lower extremities, 20% with asymptomatic PAD plus coronary disease, and 26% with prior carotid revascularisation or asymptomatic 50% carotid stenosis.20 In this PAD/carotid disease cohort, there were significant reductions for rivaroxaban-aspirin versus aspirin alone for the main primary and secondary outcomes (figure 2).
Implications of COMPASS trial results
The results of the trial are encouraging for patients with stable CAD and PAD in sinus rhythm. The primary outcome was 24% lower with rivaroxaban 2.5 mg twice daily plus aspirin than with aspirin alone (4.1% vs. 5.4%). But, the rate of major bleeding was 70% higher in the rivaroxaban-aspirin group (3.1% vs. 1.9%), predominantly accounted for by gastrointestinal bleeding. The rate of the net-clinical-benefit outcome was lower by 20% with rivaroxaban plus aspirin than with aspirin alone (4.7% vs. 5.9%).
Ticagrelor, one of the newer antiplatelet agents, was beneficial in reducing recurrent events when continued for one to three years at a low dose post-MI.21 However, patients with PAD did not demonstrate this benefit when compared with clopidogrel in the EUCLID (Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease) trial.22 Aspirin has shown to reduce major vascular events by 20% in secondary prevention trials in PAD patients.23 But efficacy data for aspirin monotherapy are lacking.24 The use of oral anticoagulation with antiplatelet agents in PAD is not supported by evidence of efficacy and, hence, no previous guidelines recommended anticoagulation in patients with PAD.
COMPASS is the first direct oral antagonist anticoagulant (DOAC) and antiplatelet combination therapy trial to demonstrate significant reduction in MACE in patients with stable atherosclerotic disease. Obviously, there is a trade-off with increased bleeding risk and the cost, which need to be taken into account. The UK National Institute for Health and Care Excellence (NICE) have recently published their technology appraisal guidance (TA607): ‘Rivaroxaban for preventing atherothrombotic events in people with coronary or peripheral artery disease’.25 In this document, NICE recommended rivaroxaban plus aspirin as an option for preventing atherothrombotic events in adults with CAD or symptomatic PAD who are at high risk of ischaemic events.
NICE defines a high risk of ischaemic events for people with CAD as:
aged 65 years or over
or with atherosclerosis in at least two vascular territories (such as coronary, cerebrovascular, or peripheral arteries)
or two or more of the following risk factors: current smoking, diabetes, kidney dysfunction with an estimated glomerular filtration rate (eGFR) of less than 60 ml/min (note that rivaroxaban is contraindicated if the eGFR is less than 15 ml/min), heart failure, previous non-lacunar ischaemic stroke.
NICE emphasised that a person’s risk of bleeding should be assessed before considering rivaroxaban. Treatment should only be started after an informed discussion with them about the risks and benefits of rivaroxaban, weighing up the risk of atherothrombotic events against the risk of bleeding. The risks and benefits of continuing treatment with rivaroxaban should be regularly reviewed.
Patients with a history of MI in COMPASS (about 62%) were, on average, over seven years post the acute event. The observed treatment benefit was consistent both in patients with more recent events and in those with events occurring many years previously.
The COMPASS trial has provided a new way of reducing the risk of MACE in patients with stable atherosclerotic disease who meet the above NICE recommendation criteria for treatment. Given that most of the patients with stable disease are looked after by primary care and are many years post-diagnosis, the majority of the prescriptions are likely to be made in the community.
Key messages
Rivaroxaban combined with aspirin has demonstrated clinical benefit in patients with coronary artery disease
The COMPASS trial showed that a combination of low-dose rivaroxaban and aspirin reduced the risk of adverse cardiovascular events in patients with stable atherosclerotic disease
The results of the COMPASS trial were assessed by the UK National Institute for Health and Care Excellence:‘rivaroxaban plus aspirin is recommended within its marketing authorisation, as an option for preventing atherothrombotic events in adults with coronary artery disease or symptomatic peripheral artery disease who are at high risk of ischaemic events’
Management guidelines in this area require updating to incorporate the results of COMPASS into routine clinical practice
Conflicts of interest
The authors participated in the COMPASS trial.
DC has received research funding, speaker fees and advisory consultation fees from Bayer.
Funding
The study was funded by Bayer.
Study approval
The multicentre study was approved by the relevant health authorities and institutional review boards.
2. Tran J, Norton R, Conrad N et al. Patterns and temporal trends of comorbidity among adult patients with incident cardiovascular disease in the UK between 2000 and 2014: A population-based cohort study. PLoS Med 2018;15:e1002513. https://doi.org/10.1371/journal.pmed.1002513
3. Bhatnagar P, Wickramasinghe K, Wilkins E, Townsend N. Trends in the epidemiology of cardiovascular disease in the UK. Heart 2016;102:1945–52. https://doi.org/10.1136/heartjnl-2016-309573
7. Bhatt DL, Eagle KA, Ohman EM et al. Comparative determinants of 4-year cardio- vascular event rates in stable outpatients at risk of or with atherothrombosis.JAMA 2010;304:1350–7. https://doi.org/10.1001/jama.2010.1322
9. Dewilde WJ, Oirbans T, Verheugt FW et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet 2013;381:1107–15. https://doi.org/10.1016/S0140-6736(12)62177-1
10. Turpie AG, Lassen MR, Eriksson BI, et al. Rivaroxaban for the prevention of venous thromboembolism after hip or knee arthroplasty: pooled analysis of four studies. Thromb Haemost 2011;105:444–53. https://doi.org/10.1160/TH10-09-0601
11. The EINSTEIN–PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012;366:1287–97. https://doi.org/10.1056/NEJMoa1113572
12. The EINSTEIN Investigators. Oral rivaroxaban for symptomatic venous thrombo- embolism. N Engl J Med 2010;363:2499-510. https://doi.org/10.1056/NEJMoa1007903
13. Patel MR, Mahaffey KW, Garg J et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883–91. https://doi.org/10.1056/NEJMoa1009638
14. Gibson CM, Mehran R, Bode C et al. Prevention of bleeding in patients with AF undergoing PCI. New Engl J Med 2016;375:2423–34. https://doi.org/10.1056/NEJMoa1611594
15. Xarelto (rivaroxaban) Summary of Product Characteristics as approved by the European Commission.
16. Mega JL, Braunwald E, Wiviott SD et al. Rivaroxaban in patients with a recent acute coronary syndrome. N Engl J Med 2012;366:9-19. https://doi.org/10.1056/NEJMoa1112277
17. Merlini PA, Bauer KA, Oltrona L et al. Persistent activation of coagulation mechanism in unstable angina and myocardial infarction. Circulation 1994;90:61-68
18. The Warfarin Antiplatelet Vascular Evaluation Trial Investigators. Oral anti-coagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med 2007;357:217–27. https://doi.org/10.1056/NEJMoa065959
19. Eikelboom JW, Connolly SJ, Bosch J et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017;377:1319–30. https://doi.org/10.1056/NEJMoa1709118
20. Anand SS, Bosch J, Eikelboom JW et al. Rivaroxaban with or without aspirin in patients with stable peripheral or carotid artery disease: an international, randomised, double-blind, placebo-controlled trial. Lancet (advance publication online). https://doi.org/10.1016/S0140-6736(17)32409-1
21. Bonaca MP, Bhatt DL, Cohen M et al. Long-term use of ticagrelor in patients with prior myocardial infarction. N Engl J Med 2015;372:1791–800. https://doi.org/10.1056/NEJMoa1500857
22. Hiatt WR, Fowkes FGR, Heizer G et al. Ticagrelor versus clopidogrel in symptomatic peripheral artery disease. N Engl J Med 2017;376:32-40. https://doi.org/10.1056/NEJMoa1611688
23. Antithrombotic Trialists’ (ATT) Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373:1849–60. https://doi.org/10.1016/S0140-6736(09)60503-1
24. Brass EP, Hiatt WR. Aspirin monotherapy should not be recommended for cardioprotection in patients with symptomatic peripheral artery disease. Circulation 2017;136:785-6. https://doi.org/10.1161/CIRCULATIONAHA.117.028888
25. National Institute for Health and Care Excellence (NICE). Rivaroxaban for preventing atherothrombotic events in people with coronary or peripheral artery disease. Technology appraisal guidance (TA607). London: NICE, October 2019. www.nice.org.uk/guidance/ta607 (last accessed December 2019)
Notes on dosing recommendations from Xarelto® ▼ (rivaroxaban) SmPC (Summary of Product Characteristics)
Xarelto 2.5 mg twice daily, coadministered with a daily dose of 75–100 mg aspirin, is indicated for the prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral artery disease (PAD) at high risk of ischaemic events.
The COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial discussed in this supplement compared both Xarelto 2.5 mg twice-daily plus aspirin and also Xarelto 5 mg twice-daily without aspirin, versus aspirin alone. Results for both comparisons are provided reflecting the original study publication.
Please note, however, that Xarelto 5 mg twice-daily is not a licensed dosage regimen for the above, nor for any other therapeutic indication.
Disclaimer: Medinews Cardiology Limited advises healthcare professionals to consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews Cardiology Limited cannot accept responsibility for any errors in prescribing which may occur.
With sadness, we report the recent deaths of two major figures in the world of cardiology, Professors Lionel Opie and Desmond Julian. We pass on our sincere condolences to their families and relatives.
Professor Lionel Opie
Professor Lionel Opie, Professor of Medicine at the University of Cape Town (UCT), South Africa, made unique contributions to heart science during his long career. He graduated in medicine from UCT and was a Rhodes scholar, studying at Oxford University and later at Harvard Medical School in the US.
He famously edited the textbook, Drugs for the Heart, with Professor Bernard Gersh. This invaluable book provided up-to-date information on every drug class used to treat cardiovascular disease. In more recent years he established the Cardiology at the Limit’s series of meetings, with Professor Derek Yellon, from UCL in London. These meetings fostered the exchange in science and medicine between the continents of Africa and Europe. In 2006, he was awarded the highest Presidential award in South Africa, the Order of Mapungubwe.
Professor Desmond Julian
Professor Desmond Julian was the first to propose coronary care units in the 1960s. His work, first published in The Lancet in 1961, transformed care for heart patients worldwide. Professor Julian saw the need for heart patients to be treated differently to general patients.
He believed that by having patients on a single specialist ward, continuously monitoring their heart rhythm, with defibrillators and trained staff on standby, this would improve survival. He set up Europe’s first Cardiac Care Unit in Edinburgh in 1964, and the British Heart Foundation – for which he was later medical director – funded the unit’s staff and equipment. In the first year of their programme, an additional seven out of 100 patients survived, when compared to a similar group of patients the year before. The rest of the world would soon follow his example.
We were honoured to have Professor Julian as a BJC editorial board member and he was a great friend to very many of us in cardiology.
Cardiac surgery for adults became widely available around 50 years ago, due mainly to the introduction of relatively safe cardiopulmonary bypass. Initially, mortality rates were quite high, even for relatively young and fit patients, and, therefore, patients and carers focused on this outcome measure. Moreover, it was easy to define and record. Local and national registries developed into databases that allowed comparison of mortality rates and were then further refined with risk modelling.
As the odds of survival after cardiac surgery improved, sicker and older patients were offered cardiac surgery, including octogenarians and extending to nonagenarians.
Clearly, surviving cardiac surgery is very important – but is survival the top priority for the 92-year old after bypass surgery who becomes unable to live independently again and who’s quality of life is insufferable? Should quality of life be the main factor driving therapeutic decisions for the frail and elderly?
Patient selection
The issues involved in making the decision to undergo surgery are complex as the elderly and very elderly cohort of patients present with more diffuse cardiovascular disease, age-related comorbidities, weaker tissues and frailty, with a lower tolerance to intervention. The challenge is accurately predicting and sharing with those elderly patients the chances of improving or worsening their quality of life. With novel methods of assessing frailty, such as sarcopenia measurement,1 a more refined approach to patient selection is evolving.
Ishikawa et al. have found that the operative mortality of octogenarians presenting for elective cardiac surgical procedures is relatively low: coronary artery bypass graft (CABG) 7%; valve surgery 5%; and CABG plus valve 10%.2 However, operating in the urgent/emergent setting is less well tolerated with a higher operative mortality (14–25%) compared with elective counterparts (3.8–6%).2,3 Along with non-elective presentation,4,5 other independent predictors of hospital mortality are: mitral surgery;4 need for aortic counter-pulsation;5 cardiopulmonary bypass time;5 blood transfusion;5 depressed systolic function;5 pre-operative renal failure;6 and chronic lung disease.3,5 As no consensus guidelines exist for operating on the elderly/very elderly, these findings provide the surgical team with criteria for patient counselling.
Patient consent
Careful patient consent cannot be underestimated as the APPROACH (Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease) investigators have found octogenarians spend longer on intensive care units (ICU) and in-hospital post-operatively, and are more likely to have ICU readmission.7 Median ICU and in-hospital stay is one day (range 0–33) and 10 (range 6–49) days, respectively.4 Compared with their younger counterparts, octogenarians have worse short- and long-term survival with crude one- and five-year mortality reported as 10.8% and 29.0%, respectively.7 Reassuringly, octogenarians undergoing heart operations do outlive their peers, with similar age-sex distribution (five-year survival 82.1% vs. 55.9%).8 Survival at five years for those undergoing isolated aortic valve replacement (AVR) is 64.8 ± 7.8% and CABG is 79.7 ± 7.4%.4 The predictors of late mortality are: poor systolic function;5 myocardial infarction;5 combined coronary/mitral surgery;5 cerebrovascular disease;6 and prolonged ventilation.6
In spite of the higher risk of post-operative complications and worse short- and long-term survival, it is considered that the overall risk of performing cardiac surgery on the elderly is acceptable to them. Elderly patients benefit from both improved functional status and quality of life.
Quality of life
The Short-form 36 Health Status questionnaire (SF-36) is a validated method of assessing quality of life in the elderly population.9 Fruitman et al., in a series of telephone interviews of octogenarians, using both SF-36 and Seattle Angina questionnaires, reported a dramatic improvement in New York Heart Association (NYHA) score from class IV (63.8%) to class I or II (92.2%) at a mean follow-up of 15.7 ± 6.9 months following cardiac surgery.6 The SF-36 scores were equal to or better than for those over 65 years for the general population and the Seattle Angina scores confirmed symptomatic relief.6 Of the survivors, 83.7% were living in their own home, 74.8% rated their health as good or excellent, and 82.5% would undergo the operation again in retrospect.6
This improvement is corroborated by Gjeilo et al. with serial SF-36 questionnaires at baseline, six months, one and five years following heart surgery in the over-75 years cohort.10 Quality of life was reported to improve from baseline to six months and remain stable five years later. Older patients were found to improve less than younger ones, from baseline to the follow-up, and have more profound reductions in scores from 12 months to five years on three subscales: physical functioning; role physical; and vitality.10
The recently published study by Coelho et al. found that most elderly patients improve both physically and mentally after surgery. The authors suggested predictive variables for less improvement on SF-36 surveys to be: poor pre-operative physical health; female sex; older age; and longer length of hospital stay. Negative predictive variables were poor pre-operative mental health and longer ICU stay.11 However, the purported benefits of operating on octogenarians does come at a significantly increased economic cost compared with younger patients.12
In the current era, with the available evidence, the medical community feels more assured in referring, assessing and offering heart operations to octogenarians. However, it is the rapidly growing subset of nonagenarians that are posing an expanding clinical problem and testing the limits of the complex and difficult decision-making process. Evidence for operating on nonagenarians is sparse and primarily limited to case reports of successful surgery and uneventful recovery, which may be influenced by publication biases.13,14
In the largest retrospective review (n=127) of nonagenarians (mean logistic EuroSCORE 21.3 ± 6.1) who underwent coronary and valvular surgical procedures, Speziale et al. reported the rate of postoperative complications to be high (42.5%) but found surgery could achieve functional improvement at the price of considerable operative (13.4%) and follow-up mortality rates.15 Non-elective priority and previous myocardial infarction were predictors of operative mortality. There was no difference in the rate and type of complications between patient strata on the basis of the type of surgery performed, and Kaplan-Meier survival estimates at five years were comparable between patient groups.15 Promisingly, the operative risk to nonagenarians presenting electively does not differ from that of risk-matched octogenarians, with good five-year survival and functional recovery.5
Pre-operative assessment
We, therefore, have some evidence about outcomes, but are there pre-operative assessments to help these elderly patients decide to consent for their proposed cardiac surgery?
In a prospective multi-centre cohort study, Alfialo et al. reported that cardiac surgery risk scores (Parsonnet score or Society of Thoracic Surgeons Predicted Risk of Mortality or Major Morbidity – STS-PROMM) performed poorly in those aged over 70 years undergoing CABG and/or valve surgery.16 It was suggested that this was, in part, because they did not take into account ‘frailty and disability’, considered to be critical determinants of health status with advanced age, the addition of which was purported to provide incremental value and improve model discrimination.16
Frailty is an important predictor of outcomes after cardiac surgery, but utility is limited by difficult assessment and quantification. Computed tomography psoas index (cross-sectional area of the psoas muscle at L4 vertebral level normalised to body surface area) to calculate sarcopenia has been shown to be a reproducible measure of frailty in the elderly that predicts risk-adjusted resource utilisation, morbidity, and long-term mortality.17 Patients with sarcopenia have been shown to have decreased long-term survival and decreased freedom from major cardiac and cerebrovascular events.18 Thus, the measurement of psoas muscle area can help facilitate more accurate scoring in elderly patients.
Additional tools to evaluate elderly patients adequately before elective cardiac surgery include the comprehensive assessment of frailty (CAF) and FORECAST (Frailty Predicts One Year After Cardiac Surgery). These have been shown to be associated with short- and mid-term mortality, independently of age.19
Decision-making
With a projected rise in the very elderly population, limited data, absence of consensus guidelines and already stretched resources it would be prudent for the heart team to take a pragmatic stance during the decision making on whether to offer surgery. An integrative approach combining frailty, disability, and risk scores is recommended to better characterise the very elderly patients referred and identify those at increased risk. Too often in these clinical discussions the focus is on mortality alone because there is evidence available compared with the lack of evidence for the expected quality of life post-surgery. The very elderly patient can find the risks and benefits hard to comprehend, and considerable time and patience will be needed by doctors, carers and relatives to debate these uncertainties. The chances of surviving the surgery are very important to them, but they also need reliable evidence about the quality of life they can expect and the odds that they may actually end up more frail and less independent.
Clinicians should be mindful of the limitations of the available data being relied upon when consenting patients. First, most reports represent single-centre retrospective analysis highlighting a paucity of, and greater need for, prospectively collected registry data. More data comparing outcomes of those elderly patients operated on versus those that were not operated is needed to gain a wider understanding of options. Second, published outcomes of surgery on the elderly are inherently linked to case selection, which in itself is skewed, as clinicians pick lower-risk ‘winners’. Finally, only one negative paper of operating on octogenarians appears to have been published, which demonstrated a significant 83% overall hospital mortality following surgical repair for type A aortic dissection,20 suggesting a strong publication bias may exist.
With the current risks associated with cardiac surgery in octogenarians and nonagenarians there would appear to be no place for prognostic surgical intervention if they are enjoying their quality of life. If their cardiac condition is limiting their lifestyle they will then have to decide on whether to gamble what they have in the hope of improvement, but in the knowledge that their surgery may be deleterious. These are often extremely hard decisions and there is a real need for more research in pre-operative assessment and post-operative quality of life following cardiac surgery in the elderly.
Conflicts of interest
None declared.
Funding
None.
References
1. Paknikar R, Friedman J, Cron D et al. Psoas muscle size as a frailty measure for open and transcatheter aortic valve replacement. J Thorac Cardiovasc Surg 2016;151:745–51. https://doi.org/10.1016/j.jtcvs.2015.11.022
3. Scandroglio AM, Finco G, Pieri M et al. Cardiac surgery in 260 octogenarians: a case series. BMC Anesthesiol 2015;15:15. https://doi.org/10.1186/1471-2253-15-15
4. Dalrymple-Hay MJ, Alzetani A, Aboel-Nazar S, Haw M, Livesey S, Monro J. Cardiac surgery in the elderly. Eur J Cardiothorac Surg 1999;15:61–6. https://doi.org/10.1016/S1010-7940(98)00286-3
5. Speziale G, Nasso G, Barattoni MC et al. Short-term and long-term results of cardiac surgery in elderly and very elderly patients. J Thorac Cardiovasc Surg 2011;141:725–31. https://doi.org/10.1016/j.jtcvs.2010.05.010
6. Fruitman DS. Cardiac surgery in octogenarians: can elderly patients benefit? Quality of life after cardiac surgery. Ann Thorac Surg 1998;68:2129–35. https://doi.org/10.1016/S0003-4975(99)00818-8
7. Wang W, Bagshaw SM, Norris CM, Zibdawi R, Zibdawi M, MacArthur R, for the APPROACH Investigators. Association between older age and outcome after cardiac surgery: a population-based cohort study. J Cardiothorac Surg 2014;9:177. https://doi.org/10.1186/s13019-014-0177-6
8. Stoica S, Cafferty F, Kitcat J et al. Octogenarians undergoing cardiac surgery outlive their peers: a case for early referral. Heart 2006;92:503–06. https://doi.org/10.1136/hrt.2005.064451
9. Lyons RA, Perry IM, Littlepage BNC. Evidence for the validity of the short-form 36 questionnaire (SF-36) in an elderly population. Age Ageing 1994;23:182–4. https://doi.org/10.1093/ageing/23.3.182
10. Gjeilo KH, Wahba A, Klepstad P, Lydersen S, Stenseth R. Survival and quality of life in an elderly cardiac surgery population: 5-year follow-up. Eur J Cardiothorac Surg 2013;44:e182–e188. https://doi.org/10.1093/ejcts/ezt308
11. Coelho P, Miranda L, Barros P, Fragata J. Quality of life after elective cardiac surgery in elderly patients. Interact Cardiovasc Thorac Surg 2019;28:199–205. https://doi.org/10.1093/icvts/ivy235
12. Gelsomino S, Lorusso R, Livi U et al. Cost and cost-effectiveness of cardiac surgery in elderly patients. J Thorac Cardiovasc Surg 2011;142:1062–73. https://doi.org/10.1016/j.jtcvs.2011.02.013
15. Speziale G, Nasso G, Barattoni MC et al. Operative and middle-term results of cardiac surgery in nonagenarians: a bridge toward routine practice. Circulation 2010;121:208–13. https://doi.org/10.1161/CIRCULATIONAHA.108.807065
16. Afilalo J, Mottillo S, Eisenberg MJ et al. Addition of frailty and disability to cardiac surgery risk scores identifies elderly patients at high risk of mortality or major morbidity. Circ Cardiovasc Qual Outcomes 2012;5:222–8. https://doi.org/10.1161/CIRCOUTCOMES.111.963157
17. Hawkins RB, Mehaffey JH, Charles EJ et al. Psoas muscle size predicts risk-adjusted outcomes after surgical aortic valve replacement. Ann Thorac Surg 2018;106:39–45. https://doi.org/10.1016/j.athoracsur.2018.02.010
18. Okamura H, Kimura N, Tanno K et al. The impact of preoperative sarcopenia, defined based on psoas muscle area, on long-term outcomes of heart valve surgery. J Thorac Cardiovasc Surg 2019;157:1071–9. https://doi.org/10.1016/j.jtcvs.2018.06.098
19. Sündermann SH, Dademasch A, Seifert B et al. Frailty is a predictor of short- and mid-term mortality after elective cardiac surgery independently of age. Interact Cardiovasc Thorac Surg 2014;18:580–5. https://doi.org/10.1093/icvts/ivu006
20. Neri E, Toscano T, Masseti M et al. Operation for acute type A aortic dissection in octogenarians: is it justified? J Thorac Cardiovas Surg 2001;121:259–67. https://doi.org/10.1067/mtc.2001.112205
Digital healthcare is being introduced to the management of heart failure as a consequence of innovations in information technology. Advancement in technology enables remote symptom and device monitoring, and facilitates early detection and treatment of heart failure exacerbation, potentially improving patient outcomes and quality of life. It also provides the potential to redesign our heart failure healthcare system to one with greater efficacy through resource-sparing, computer-aided decision-making systems. Although promising, there is, as yet, insufficient evidence to support the widespread implementation of digital healthcare. Patient-related barriers include user characteristics and health status; privacy and security concerns; financial costs and lack of accessibility of digital resources. Physician-related barriers include the lack of infrastructure, incentive, knowledge and training. There are also a multitude of technical challenges in maintaining system efficiency and data quality. Furthermore, the lack of regulation and legislation regarding digital healthcare also prevents its large-scale deployment. Further education and support and a comprehensive workable evaluation framework are needed to facilitate confident and widespread use of digital healthcare in managing patients with heart failure.
Dr Sze, BJCA essay prize winner
Introduction
According to the European Society of Cardiology Atlas project, >83 million people suffered from cardiovascular diseases in Europe in 2015.1 Heart failure (HF) is a common chronic disease in the ageing population. It is associated with poor prognosis, recurrent admissions and limited quality of life.2 Despite development of effective guideline-based treatment, the prognosis of HF patients remains poor. With the advancement of cyber technologies, digital healthcare has become more popular and may develop as a promising way to tackle challenges in HF management.
The objectives of this article are:
Provide an overview of digital healthcare and its impact on patient outcome and healthcare delivery.
Highlight the important challenges/barriers for large-scale digital health implementation.
Predict the future of digital healthcare, in the field of HF.
Digital healthcare in HF
Digital healthcare involves the use of information and communication technologies to treat and monitor patients, convey healthy lifestyle information and advice (primary prevention), conduct research, educate healthcare professionals and monitor public health. Digital healthcare encompasses e-learning, mobile applications, remote monitoring, telerehabilitation and teleconsultation. Table 1 shows an overview of utilisation of digital healthcare in HF.3-15
Table 1. Overview of digital healthcare in heart failure
Study
Population
Intervention
Outcome
Remote device monitoring
EVOLVO 20123
200 CHF patients with ICD/CRTD
Remote implant-based, multi-parameter monitoring
35% less frequent emergency visits for HF, arrhythmia or ICD-related events between intervention vs. control group
IN-TIME
20144
716 CHF patients with ICD/CRTD
Remote implant-based, multi-parameter monitoring
8% less deterioration in a clinical composite score (all-cause mortality, HF hospitalisation, NYHA class and change in patient global self-assessment) in the intervention vs. control group
OptiLink HF 20165
1,002 CHF patients with ICD ± CRT
Fluid status alerts via text message to responsible physician
No difference in composite all-cause mortality and cardiovascular hospitalisation between intervention vs. control group
Telemonitoring
WHARF 20036
280 CHF patients
AlereNet monitoring system with symptom and weight monitoring
56% reduction in mortality but no difference in hospitalisation between intervention vs. control group
TEN-HMS 20057
426 CHF patients with recent HF hospitalisation
Home telemonitoring vs. nurse telephone support vs. usual care
Similar hospitalisation and mortality among patients assigned to home telemonitoring or nurse telephone support. 1-year mortality was higher in control (45%) vs. intervention groups (27–29%)
DIAL
20088
23 CHF patients
6-week in-home telemedicine education and monitoring programme
No difference in healthcare utilisation rates between intervention vs. control groups. Intervention group facilitated self-care
Tele-HF 20109
1,653 CHF patients with recent HF hospitalisation
Telephone-based interactive voice response system
No difference in all-cause hospitalisation/mortality within 180-days between intervention vs. control group
TIM-HF 201110
710 CHF patients
Remote telemonitoring using portable devices for ECG, weight and BP
No difference in all-cause/cardiovascular mortality or HF hospitalisation between intervention vs. control group
Cochrane
Inglis et al. 201511
41 studies (5,472 CHF patients)
Structured telephone support/non-invasive home telemonitoring
Reduction in all-cause mortality (RR 0.87, 95%CI 0.77–0.98) and HF-related hospitalisation (RR 0.85, 95%CI 0.77–0.93) in intervention vs. control group
BEAT-HF 201612
1,457 CHF patients discharged after hospitalisation for decompensated HF
Telemonitoring and health coaching telephone calls
No difference in 30-day and 180-day all-cause hospitalisation or 180-day mortality between intervention vs. control group
REM-HF
201713
1,650 CHF patients with cardiac implanted electronic devices
Remote monitoring of devices
No difference in all-cause mortality and unplanned cardiovascular hospitalisation between intervention and control group
Telerehabilitation
Piotrowicz et al. 201014
152 CHF patients
8-week home-based telerehabilitation programme based on walking training
Telerehabilitation is equally as effective as standard care with similar improvement in quality of life
Piotrowicz et al. 201515
111 CHF patients with cardiac implantable electronic devices
8-week home-based telerehabilitation programme based on walking training
Improvement in exercise capacity and quality of life in the intervention vs. control group
Key: BP = blood pressure; CHF = chronic heart failure; CI = confidence interval; CRT = cardiac resynchronisation therapy;
CRTD = cardiac resynchronisation therapy with a defibrillator; ECG = electrocardiogram; HF = heart failure;
ICD = implantable cardiac defibrillator; NYHA = New York Heart Association; RR = relative risk
Impact of digital healthcare on patients’ healthcare experience
The ageing population and frailty have become major themes for patients with HF. Physical deconditioning and cognitive decline contribute to medication non-adherence, which predisposes to recurrent hospitalisation and death. HF management is complex and is guided by subtle changes in symptoms and signs of congestion and volume overload. Failure to make ongoing small, but clinically significant, titrations in HF medications contribute to increased hospitalisation and mortality. In patients with cardiac resynchronisation therapy, optimal management requires yet another layer of oversight – device management. With the advent of Bluetooth-connected cardiac resynchronisation therapy, a smartphone could provide remote device status and diagnostics.16 Digital healthcare enables remote symptom and implanted device monitoring and facilitates early detection and treatment of HF exacerbations, leading to better outcomes and quality of life.17 Provision of remote patient support also enhances patient-doctor communication. Furthermore, as online educational resources become more available, patients are also empowered to take a more active role in managing their conditions. Mobile applications that promote healthy lifestyle induce behavioural change, particularly against poor diet, smoking and physical inactivity;18 directly improving patient outcome.
Impact of digital healthcare on healthcare delivery
Our National Health Service (NHS) has limited resources to meet the increasing healthcare demand of the ageing population. Shortage of medical staff means that most healthcare resources are allocated to managing acutely unwell patients in hospital. This has a great impact on the management of patients with HF – a chronic condition that needs regular medical input. Digital healthcare provides the potential to redesign our HF healthcare system to one with greater efficacy through resource-sparing, computer-aided decision-making systems, remote monitoring and consultation.19 Artificial intelligence has been applied in various contexts, from the construction of automated clinical decision support systems to imaging interpretation. The Seattle HF model is a machine-learning risk-prediction model that was trained with clinical data routinely obtained from electronic health records to predict HF prognosis, which could potentially be useful in the management of high-risk HF patients.20
Challenges for implementing digital healthcare
Patient-related barriers
Health applications and online resources, although positively perceived, were not widely used in HF populations. An observational study reported a telemonitoring intervention adherence rate of only 50% in HF patients.9
Patient-related barriers to digital healthcare include user characteristics and health status, privacy and security concerns; financial costs and lack of accessibility of digital resources; mistrust of online information; and lack of motivation.21 Old age, frailty, poor socioeconomic and health status, and low e-health literacy in the HF population predispose to suboptimal uptake of digital healthcare. Other contributors include lack of understanding of the concept of ‘patient empowerment’ or worries about receiving a poorer level of care due to the impersonal nature of a digital service.22 Most patients still regard their physicians as their predominant and most reliable source of health information. Others were overwhelmed by technology and were unable to keep up with technological advancements.22 There were also patient concerns regarding low self-efficacy and user-friendliness of telemonitoring technology.22 These problems might be partially attributable to the fact that development of digital healthcare is largely technically-driven and patients are rarely involved in its creation and design.23
Physician-related barriers
Physician-related barriers to digital healthcare include lack of infrastructure, incentives, knowledge and training, regulations and standardisation.24 While digital healthcare enables easier patient monitoring, a heavy time investment is needed from clinicians to review incoming data and provide feedback to patients. Furthermore, most digital healthcare is added on top of existing healthcare rather than replacing it. For example, nurse-led telemonitoring for HF patients are set up without adapting the frequency of conventional hospital-based care by cardiologists, leading to increased healthcare costs.
Technical/clinical efficacy
Digital healthcare has a multitude of technical challenges. For example, telemonitoring involves transfer of physiological data to a centralised platform using wireless networks, software, algorithms for data capture and processing support. This process involves many challenges including technological capabilities, system efficiency and data integrity and quality. Despite a plethora of mobile applications available, only a very limited number have been tested for technical and clinical efficacy and quality. Of 11 chronic diseases studied (including HF), consistent evidence of benefit was only seen for diabetes applications. The benefits detected were of marginal clinical importance and there were no reports of hard clinical end points.25 Randomised-controlled trials provided conflicting evidence of efficacy of telemonitoring and telerehabilitation on outcomes such as hospitalisation and mortality (table 1). The lack of an evidence base behind digital healthcare limits the physicians’ confidence in adopting digital healthcare in daily practice.
Regulatory issues
Lack of regulation and legislation regarding digital healthcare prevents its widespread implementation. A World Health Organization (WHO) survey revealed huge variations among European countries in terms of e-health regulation or guidance on data validity, security and value assessment.26 To tackle this problem, national authorities are developing regional certification programmes for technological interventions.
The future of digital healthcare
Many think digital healthcare will improve the cost-effectiveness of our healthcare system and improve patients’ healthcare experience. Although promising, there is, as yet, insufficient evidence to support its widespread implementation, at least in the field of HF. Further education and support, and a comprehensive workable evaluation framework are needed to facilitate confident and widespread use of these technologies in managing HF patients. In particular, according to the ARCHIE framework, digital healthcare should be “anchored in what matters to users; realistic about natural history of illness, continuously co-created with users, embedded in social networks and integrated to mobilise knowledge across network” before implementation.27 Interestingly, a study pointed out that HF self-management may be associated with reduced hospital admissions in only a subgroup of patients who are under 65 years of age, whereas in other subgroups, such as patients with depression, self-management may be associated with reduced survival rate.28 This emphasises the importance of careful selection of patients before implementing digital healthcare.
Conclusion
Digital healthcare is being introduced to the management of HF as a consequence of innovations in information technology. Initial evaluation is that it might improve healthcare delivery but there are multiple barriers impeding its large-scale deployment. These challenges have to be tackled before HF becomes a cyber-specialty.
Key messages
Advancement in technology enables remote symptom and device monitoring, potentially improving patient outcomes and quality of life. It also provides the potential to redesign our heart failure healthcare system to one with greater efficacy through computer-aided decision-making systems
Barriers to widespread implementation of digital healthcare in heart failure include patient-related barriers such as user characteristics; privacy and security concerns; physician-related barriers such as lack of infrastructure, knowledge and training; technical barriers, such as challenges in maintaining system efficiency and data quality; and the lack of regulation and legislation regarding digital healthcare
Further education and support, and a comprehensive workable evaluation framework, are needed to facilitate confident and widespread use of digital healthcare in managing patients with heart failure
Conflicts of interest
None declared.
Funding
None.
References
1. Timmis A, Townsend N, Gale C et al.; the Atlas Writing Group. European Society of Cardiology: cardiovascular disease statistics 2017. Eur Heart J 2018;39:508–79. https://doi.org/10.1093/eurheartj/ehx628
2. Dunlay SM, Redfield MM, Weston SA et al. Hospitalizations after heart failure diagnosis. A community perspective. J Am Coll Cardiol 2009;54:1695–702. https://doi.org/10.1016/j.jacc.2009.08.019
3. Landolina M, Perego GB, Lunati M et al. Remote monitoring reduces healthcare use and improves quality of care in heart failure patients with implantable defibrillators: the evolution of management strategies of heart failure patients with implantable defibrillators (EVOLVO) study. Circulation 2012;125:2985–92. https://doi.org/10.1161/CIRCULATIONAHA.111.088971
4. Hindricks G, Taborsky M, Glikson M et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet 2014;384:583–90. https://doi.org/10.1016/S0140-6736(14)61176-4
5. Böhm M, Drexler H, Oswald H. Fluid status telemedicine alerts for heart failure: a randomized controlled trial. Eur Heart J 2016;37:3154–63. https://doi.org/10.1093/eurheartj/ehw099
6. Goldberg LR, Piette JD, Walsh MN et al. Randomized trial of a daily electronic home monitoring system in patients with advanced heart failure: the Weight Monitoring in Heart Failure (WHARF) trial. Am Heart J 2003;146:705–12. https://doi.org/10.1016/S0002-8703(03)00393-4
7. Cleland JG, Louis AA, Rigby AS et al. Noninvasive home telemonitoring for patients with heart failure at high risk of recurrent admission and death: the Trans-European Network-Home-Care Management System (TEN-HMS) study. J Am Coll Cardiol 2005;45:1654–64. https://doi.org/10.1016/j.jacc.2005.01.050
8. Seibert PS, Whitmore TA, Patterson C et al. Telemedicine facilitates CHF home health care for those with systolic dysfunction. Int J Telemed Appl 2008:235031. https://doi.org/10.1155/2008/235031
9. Chaudhry SI, Mattera JA, Curtis JP et al. Telemonitoring in patients with heart failure. N Engl J Med 2010;363:2301–09. https://doi.org/10.1056/NEJMoa1010029
10. Koehler F, Winkler S, Schieber M et al. Impact of remote telemedical management on mortality and hospitalizations in ambulatory patients with chronic heart failure: the telemedical interventional monitoring in heart failure study. Circulation 2011;123:1873–80. https://doi.org/10.1161/CIRCULATIONAHA.111.018473
11. Inglis SC, Clark RA, Dierckx R, Prieto-Merino D, Cleland JG. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Syst Rev 2015;10:CD007228. https://doi.org/10.1002/14651858.CD007228.pub3
12. Ong MK, Romano PS, Edginton S et al. Effectiveness of remote patient monitoring after discharge of hospitalized patients with heart failure: the Better Effectiveness After Transition – Heart Failure (BEAT-HF) randomized clinical trial. JAMA Int Med 2016;176:310–18. https://doi.org/10.1001/jamainternmed.2015.7712
13. Morgan JM, Kitt S, Gill J et al. Remote management of heart failure using implantable electronic devices. Eur Heart J 2017;38:2352–60. https://doi.org/10.1093/eurheartj/ehx227
14. Piotrowicz E, Baranowski R, Bilinska M et al. A new model of home-based telemonitored cardiac rehabilitation in patients with heart failure: effectiveness, quality of life and adherence. Eur J Heart Fail 2010;12:164–71. https://doi.org/10.1093/eurjhf/hfp181
15. Piotrowicz E, Zielinski T, Bodalski R et al. Home-based telemonitored Nordic walking training is well accepted, safe, effective and has high adherence among heart failure patients, including those with cardiovascular implantable electronic devices – a randomized controlled study. Eur J Prev Cardiol 2015;22:1368–77. https://doi.org/10.1177/2047487314551537
16. Turakhia MP. Telemedicine for management of implantable defibrillators: lessons learned and a look toward the future. Circ Arrhythm Electrophysiol 2017;10:e005728. https://doi.org/10.1161/CIRCEP.117.005728
17. Darkins A, Ryan P, Kobb R et al. Care coordination/home telehealth: the systematic implementation of health informatics, home telehealth, and disease management to support the care of veteran patients with chronic conditions. Telemed J E Health 2008;14:1118–26. https://doi.org/10.1089/tmj.2008.0021
19. Cowie MR, Bax J, Bruining N et al. E-health: a position statement of the European Society of Cardiology. Eur Heart J 2016;37:63–6. https://doi.org/10.1093/eurheartj/ehv416
20. Levy WC, Mozaffarian D, Linker DT et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation 2006;113:1424–33. https://doi.org/10.1161/CIRCULATIONAHA.105.584102
21. Ware P, Bartlett SJ, Paré G et al. Using e-Health technologies: interests, preferences, and concerns of older adults. Interact J Med Res 2017;6:e3. https://doi.org/10.2196/ijmr.4447
22. Hall AK, Dodd V, Harris A et al. Heart failure patients’ perceptions and use of technology to manage disease symptoms. Telemed J E Health 2014;20:324–31. https://doi.org/10.1089/tmj.2013.0146
24. Villalba-Mora E, Casas I, Lupianez-Villaneuva F et al. Adoption of health information technologies by physicians for clinical practice: the Andalusian case. Int J Med Informat 2015;84:477–85. https://doi.org/10.1016/j.ijmedinf.2015.03.002
25. Scott IA, Scuffham P, Gupta D et al. Going digital: a narrative overview of the effects, quality and utility of mobile apps in chronic disease self-management. Aust Health Rev 2018;online first. https://doi.org/10.1071/AH18064
27. Greenhalgh T, Procter R, Wherton J et al. What is quality in assisted living technology? The ARCHIE framework for effective telehealth and telecare services. BMC Med 2015;13:91. https://doi.org/10.1186/s12916-015-0279-6
Authors: J William McEvoy, Michael Keane, Justin Ng
J William McEvoy
Professor of Preventive Cardiology
National University of Ireland and National Institute for Prevention and Cardiovascular Health, Moyola Lane, Newcastle, Galway, H91 FF68, Ireland
Michael Keane
Consultant Anaesthetist, Casey Hospital, Adjunct Associate Professor, Swinburne University, and Adjunct Senior Lecturer, Monash University
Casey Hospital, Monash Health, 62 Kangan Drive, Berwick, Victoria 3806, Australia
Justin Ng
Medical Resident
Department of Medicine, Peninsula Health, Frankston, Victoria 3199, Australia
The ASPirin in Reducing Events in the Elderly trial (ASPREE) contributed important knowledge about primary cardiovascular disease (CVD) prevention among healthy older adults. The finding that daily low-dose aspirin (LDA) does not statistically prevent disability or CVD among adults aged over 70 years when compared with placebo, but does significantly increase risk of haemorrhage, immediately influenced clinical practice guidelines. In this article, we discuss nuances of the trial that may impact the extrapolation of the ASPREE trial results to the everyday individual clinical care of older adults.
Introduction
The ASPirin in Reducing Events in the Elderly trial (ASPREE), published in 2018, was a landmark randomised-controlled trial (RCT) that contributed important knowledge about primary cardiovascular disease (CVD) prevention among healthy older adults.1 ASPREE found that daily low-dose aspirin (LDA) does not statistically prevent disability or CVD among adults aged over 70 years when compared with placebo, but does significantly increase risk of haemorrhage; findings that immediately influenced clinical practice guidelines.2
When used as a case study of large RCTs, ASPREE provides further, more existential, lessons for both researchers and physicians in the conduct and interpretation of large RCTs and the complexity of assimilating trial data into clinical practice guidelines. In this perspective, we discuss nuances of the trial that may impact the extrapolation of the ASPREE trial results to the everyday individual clinical care of older adults, particularly those who are concurrently taking non-steroidal anti-inflammatory drugs (NSAIDs) and proton-pump inhibitors (PPIs).
The results of ASPREE were seemingly discordant with the hitherto large body of primary prevention LDA trials conducted in non-elderly study populations. Specifically, most prior trials of LDA in high-risk primary prevention found reductions in non-fatal CVD (particularly myocardial infarction [MI]) with trends towards lower all-cause mortality,3 whereas ASPREE found no effect on MI and a trend towards higher mortality.1
Why is this? The ASPREE authors propose that it may be related to the fact that their patients were not required to have cardiovascular risk factors, or be above a certain threshold of estimated cardiovascular risk. Therefore, despite their older age, ASPREE participants may not have had the same increased cardiovascular risk as the patient populations in other primary prevention aspirin trials.1 Other explanations must include the consideration that elderly adults are fundamentally different from non-elderly adults with respect to drug therapy. Similarly, is it that the primary prevention population’s background propensity to CVD has changed in the modern era, reducing LDA’s meaningful contribution? Or is ASPREE a triumph of the large RCT to dispel misconceptions about innately ineffective therapies? While all of these explanations are possible, there are a few nuances to this trial worth considering when applying the results from ASPREE to individual older adults being treated in the clinic.
Duty of care to patients versus clinical trial imperatives
Chronic LDA increases the risk of upper gastrointestinal (UGI) haemorrhage, and this risk is increased by various factors including age over 65 years (by definition, all ASPREE patients) and concomitant use of NSAIDs. Conversely, prophylactic use of PPIs has been shown to significantly reduce bleeding risk.4
The recently published COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial found that prophylactic PPI use did not significantly reduce the composite of clinically significant UGI bleeding events in patients taking low-dose anticoagulation and LDA.5 The point estimate, however, was in favour of PPI use. It should also be noted that COMPASS included patients that had already been on LDA long-term, and those who were already on a PPI were excluded from this study. Interestingly, in a subgroup analysis of aspirin-only patients (i.e. those randomised to aspirin and placebo), there was a statistically significant reduction in UGI events in the factorial arm of this trial who were also randomised to PPI. These points suggest that a high-bleeding risk subgroup on LDA (like the elderly patients in ASPREE) would probably still benefit from PPI consideration.
Thus, COMPASS appears to provide some support for current guidelines, which recommend that an informed discussion on the prophylactic use of PPIs should be standard-of-care for patients over 65 on LDA and who have at least one other bleeding risk factor.4 However, for the same patient not on LDA, a PPI would be unnecessary as a purely prophylactic intervention; i.e. the use or non-use of LDA would make the difference between the recommendation (or not) for prophylactic PPIs in many ASPREE-like patients. Here, the blinding process that is utilised to prevent bias within an RCT was in direct conflict with critical, actionable clinical information.
ASPREE raises ethical and medico-legal conundrums for primary-care physicians involved with clinical research. Out of the trial setting, if there was no discussion of the recommendations from expert societies about prophylactic PPIs, and an elderly at-risk patient commenced on LDA suffered a significant UGI haemorrhage, would it be considered that the doctor practised best care? Because a patient is in a trial and the doctor is blinded to actionable information, does that obviate the doctor’s duty-of-care to provide best practice?
The ASPREE protocol did not prevent the use of PPIs. But, because of blinding, ASPREE did not allow aspirin-arm patients to be started on prophylactic PPIs, who might otherwise qualify.
To maintain reproducibility, when counselling patients on risks and benefits of LDA, should ASPREE only be considered an evidence base for patients who do not tell their doctor whether they are or are not taking LDA? Since gastrointestinal bleeding was one of the main adverse outcomes of ASPREE, can ASPREE be considered quotable evidence for contemporary practice where at-risk older patients started on LDA are typically offered prophylactic PPIs?
Pharmacokinetics, pharmacodynamics, interactions and pre-trial review of trial protocols
The half-life of LDA is very brief, but its clinical effect is prolonged due to the irreversible inhibition of the platelet cyclo-oxygenase (COX)-1 enzyme. An increasingly recognised drug interaction occurs when the presence of another NSAID (such as ibuprofen) at the COX-1 enzyme prevents LDA’s brief window of opportunity to bind and irreversibly deactivate platelet COX-1; before LDA is rapidly eliminated. The Food and Drug Administration (FDA) state that “Timing of dosing of ibuprofen and low-dose aspirin is important for preserving the cardioprotective effect of aspirin”.6
The ASPREE trial protocol recognised this: “if they take NSAIDs they will be advised to take them at least half an hour after taking trial medication to minimise interaction.” However, this protocol recommendation is only appropriate for immediate-release aspirin, whereas ASPREE used a slow-release enteric-coated formulation of aspirin, which likely meant that no medication administration regimen would have prevented this NSAID interaction. For example, according to the FDA, an “ibuprofen regimen that does not attenuate the antiplatelet effects of enteric coated aspirin has not yet been identified”.6
Approximately 14% of ASPREE participants, enrolled in Australia and America were regularly taking conventional NSAIDs. This observation appears to be consistent with the British population, where around 14,000 patients have been estimated to be taking an NSAID and anticoagulation concurrently without gastroprotection.7 If the aspirin–NSAID interaction was considered significant enough to include measures to avoid it in the trial protocol (measures that unfortunately may have been futile given the use of enteric-coated aspirin in ASPREE), then it appears difficult to justify including data from the 14% of patients concurrently on NSAIDs in the primary outcome analysis. While a subgroup analysis of ASPREE did not report effect modification for LDA based on NSAID use, this analysis was not prespecified and underpowered, so the results are inconclusive. As such, concomitant NSAID use (and timing) presents just one of, potentially, many drug interactions that could limit the net benefits of primary prevention of LDA in older adults, reminding us that close evaluation for drug interactions is always advised for any older adults taking aspirin.8
Translating findings from trial populations to individual older patients outside of the trial
In ASPREE, the reported compliance with aspirin was 62%. Considering the 14% of patients concurrently taking NSAIDs, the number of patients effectively taking aspirin was potentially as low as 48% (because in those 14% of patients the NSAIDs may have prevented the extended-release formulation of aspirin from being able to deactivate the platelet COX-1 enzyme). It is difficult to ask any drug or intervention to perform when it doesn’t even get on the playing field. However, despite as few as 50% of patients in the LDA group effectively taking the medicine, there was a trend towards reduced cardiovascular events (hazard ratio 0.95; 95% confidence interval [CI] 0.83 to 1.08).1 Noncompliance related to polypharmacy is a major problem in older populations that is often not planned for in sample size estimates.
Furthermore, the follow-up time averaged only 4.7 years. So, in a potentially underpowered study there was a mechanistically consistent trend towards cardiovascular benefit. What should one tell a patient, especially a 70-year-old, hoping to live more than 4.7 years, who is motivated to take the drug?
Finally, it is impossible to counsel accurately regarding the main downside to LDA, as an unknown number of bleeding complications could/should have been prevented by otherwise standard-of-care prophylactic PPIs.
How should physicians deal with these issues related to the applicability of large homogenised trials to individual patient circumstances; before potentially rejecting beneficial therapies for their older patients? An understanding of systems complexity underpins a final lesson of ASPREE, as related to evidence-based guidelines. Unfortunately, while large RCTs are necessary and a fundamental step in the practice of evidence-based medicine, they often lack the fidelity to give useful information at the margin of clinical care for individual patients, particularly in the elderly. Although guidelines attempt to prioritise RCT evidence when providing recommendations for clinicians seeing individual patients, often RCTs are unable to provide clinical answers to individual patient circumstances, due to the very nature of clinical trial results – which are expressed as the average result from among the whole sample of included individuals participating in the trial. Thus, sometimes evidence outside of clinical trials needs to be drawn upon to formulate guideline recommendations. This might also help to explain the results from a JAMA study, which found that “among recommendations in major cardiovascular society guidelines, only a small percentage were supported by evidence from multiple RCTs or a single, large RCT. This pattern does not appear to have meaningfully improved from 2008 to 2018”.9
Key messages
Individual patient circumstances need to be considered when basing clinical decisions on data from large randomised-controlled trials. This is the case for aspirin and primary prevention in the elderly
Sometimes the use of actionable clinical information might be in conflict with blinding in clinical trials. The use of this information to prevent side effects may change the risk/benefit balance
Pre-trial review of trial protocols may allow optimisation of drug formulations
Conflicts of interest
MK is on the medical advisory board for Cannvalate, a medical cannabis company. JWM and JN have no conflicts to report.
Funding
None.
Acknowledgement
We thank Professor Neville David Yeomans (The University of Melbourne) for his conceptual guidance and editing.
References
1. McNeil JJ, Wolfe R, Woods RL et al. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly. N Engl J Med 2018;379:1509–18. https://doi.org/10.1056/NEJMoa1805819
2. Arnett DK, Blumenthal RS, Albert MA et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease. Circulation 2019;140:e596–e646. https://doi.org/10.1161/CIR.0000000000000678
3. Raber I, McCarthy CP, Vaduganathan M et al. The rise and fall of aspirin in the primary prevention of cardiovascular disease. Lancet 2019;393:2155–67. https://doi.org/10.1016/S0140-6736(19)30541-0
4. Bhatt DL, Scheiman J, Abraham NS et al. ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 2008;52:1502–17. https://doi.org/10.1016/j.jacc.2008.08.002
5. Moayyedi P, Eikelboom JW, Bosch J et al. Safety of proton pump inhibitors based on a large, multi-year, randomized trial of patients receiving rivaroxaban or aspirin. Gastroenterology 2019;157:682.e2–691.e2. https://doi.org/10.1053/j.gastro.2019.05.056
8. Hamilton H, Gallagher P, Ryan C, Byrne S, O’Mahony D. Potentially inappropriate medications defined by STOPP criteria and the risk of adverse drug events in older hospitalized patients. Arch Intern Med 2011;171:1013–19. https://doi.org/10.1001/archinternmed.2011.215
9. Fanaroff AC, Califf RM, Windecker S, Smith SC Jr., Lopes RD. Levels of evidence supporting American College of Cardiology/American Heart Association and European Society of Cardiology guidelines, 2008–2018. JAMA 2019;321:1069–80. https://doi.org/10.1001/jama.2019.1122
A 78-year-old man presented to the emergency department with recurrent episodes of syncope precipitated by a variety of strong aromas. He denied chest pain, breathlessness or palpitations. There were no headaches, no blurred vision or limb weakness or seizure-like activity. On recovery, he had no post-ictal symptoms. He was initially discharged after initial investigations, including electrocardiogram (ECG), were normal. On the way to the main entrance, while passing cleaning equipment (which included strongly smelling bleach), he experienced a further syncopal episode. He was taken into the resuscitation bay, attached to cardiac monitoring and referred to the medical on-call team. When approached by the medical registrar on call (who was wearing ‘powerful’ aftershave), the patient commented the scent was precipitating a further attack. The registrar reviewed the cardiac monitor captured in figure 1 and witnessed a prolonged pause followed by asystole. Cardiopulmonary resuscitation (CPR) was commenced for approximately one minute, at which point there was a spontaneous recovery of cardiac output and a quick recovery to baseline.
Figure 1. Cardiac monitor readout
The patient was transferred to the cardiac unit for further monitoring and underwent a dual-chamber permanent pacemaker implantation (DDDR) the following day. The patient made a full clinical recovery and experienced no further events prior to discharge.
This case illustrates the significance of powerful aroma as a potential precipitant for syncope and falls within the umbrella term of ‘neurocardiogenic syncope’.1,2 Our medical registrar has refined his use of aftershave in the light of this case!
Aldosterone/renin ratio (ARR) is commonly used to screen for primary hyperaldosteronism (Conn’s disease). A number of drugs can alter ARR measurements, thus requiring omission before testing. However, hormonal agents such as the combined oral contraceptive (COCP) or progestogen-only pill (POP) are not listed for omission. A 20-year-old woman was referred to the endocrinology team, following investigations for syncope by her cardiologist, when ARR was found to be elevated. She was taking POP (Cerelle®) while having ARR measured. After omitting POP for four weeks, plasma aldosterone concentration was reduced by 52% (from 560 pmol/L to 271 pmol/L, reference range: 100–450 pmol/L), plasma renin concentration increased by 253% (from 3.6 mU/L to 12.7 mU/L, reference range: 5.4–30 mU/L) and ARR reduced from 156 to 21 (–86.5%) (reference range: <80 suggests Conn’s unlikely). To the best of our knowledge, this is the first reported case of POP-related false-positive ARR screening for primary hyperaldosteronism. Omission of POP should, therefore, be considered in women undergoing ARR measurement.
Case presentation
A 20-year-old woman was being investigated privately for syncope in May 2017. Tilt-test showed that on standing, her heart rate increased by 30 beats/minute from baseline. She was referred to the cardiology team. Her body mass index (BMI) was 23 kg/m2 and average 24-hour ambulatory blood pressure was 141/79 mmHg. She had a normal echocardiogram and 24-hour urinary catecholamines. The patient completed the standard treadmill test. Because of hypertension detected in this patient, aldosterone/renin ratio (ARR) was performed to screen for primary hyperaldosteronism (Conn’s disease). ARR was found to be raised at 156 (reference range: <80 indicates Conn’s disease unlikely), with plasma concentration of aldosterone 560 pmol/L (reference range: 100–450 pmol/L) and plasma renin concentration 3.6 mU/L (reference range: 5.4–30 mU/L). Since Conn’s disease could not be excluded, she was referred to the endocrinology team.
On consultation, the patient reported no other medical conditions or treatment other than progestogen-only pill (POP) containing 75 µg of desogestrel (Cerelle®, Consilient Health Ltd, UK) for two years, which she was taking at the time when ARR was measured. She had normal renal, liver and thyroid functions without evidence of hypernatraemia (sodium 138 mmol/L) or hypokalaemia (potassium 4.6 mmol/L).
Although not routinely mentioned in published endocrine protocols,1-3 POP was suspected to potentially interfere with ARR measurement in view of the absence of other indicators to suggest primary hyperaldosteronism (suppressed renin, hypernatraemia or hypokalaemic alkalosis). She was, therefore, advised to omit POP for four weeks and to use alternative contraceptive methods to avoid unplanned pregnancy, before having ARR measurement repeated by the same immunoassays. POP-free plasma aldosterone concentration was reduced to 271 pmol/L, plasma renin concentration increased to 12.7 mU/L and ARR reduced to a normal level of 21. These changes equate to relative reduction of aldosterone from baseline level by –52%, increase in renin by +253%, and a net reduction in ARR by –87% (figure 1). Sodium (138 mmol/L) and potassium (4.6 mmol/L) levels remained exactly the same as those performed during the initial ARR screening, with normal levels of bicarbonate (27 mmol/L). During the period of investigations, the patient did not change her diet or lifestyle and was not on any medications.
Figure 1. Relative changes in concentration of aldosterone, renin and aldosterone/renin ratio (ARR) from baseline measurements while patient was taking progestogen-only pill (POP) and four weeks after POP omission. Relative change was calculated as (POP-free measurement minus Baseline measurement) / Baseline measurement, expressed in percentage. First number in square brackets indicates baseline measurement and second indicates POP-free measurement
Diagnosis and management
The patient was diagnosed with postural orthostatic tachycardia syndrome (PoTS) by the cardiologist. The previously raised ARR had normalised after POP omission indicating a false-positive ARR screening test associated with POP. She was reassured of the normal POP-free ARR measurement and no further endocrine investigations were necessary. The patient was advised that she could restart POP if she wished. On completion of endocrine investigations, her cardiologist prescribed midodrine at the initial dose of 2.5 mg three times daily, followed by a further increase to 5 mg three times daily for treatment of PoTS.
Discussion
The present report of a young woman shows a clear temporal association of changes in ARR with POP and its omission; ARR rose to a level where Conn’s disease could not be excluded while taking POP, followed by normalisation of ARR after omission of this contraceptive agent. To the best of our knowledge, this is the first reported case of POP-related false-positive ARR screening for primary hyperaldosteronism. We suggest that when performing ARR, omission of POP for up to four weeks should be considered to avoid false-positive results and, thus, prevent further unnecessary investigations and treatment.
Random ARR is commonly used by specialists such as endocrinologists to screen for primary hyperaldosteronism (Conn’s disease) in individuals with hypertension. A number of drugs can alter ARR measurement, thus, requiring their omission before testing (table 1).1-3 In women, the combined oral contraceptive pill (COCP) has also been shown to interfere with ARR,4 while the effect of POP on ARR is little known.
Table 1. Effects of drugs that may require omission before aldosterone/renin ratio (ARR) testing on ARR measurements
Drug
Effects on measurements
Recommended washout period
Random ARR screening test
Saline infusion test
Effects on renin concentration*
Effects on ARR
Based on Turner & Wass1
Based on Imperial Endocrine Handbook2
Based on both Turner & Wass1 and Imperial Endocrine Handbook2
*There is a lack of information on effects of drugs on aldosterone levels.
†Based on Ahmed et al.7
‡According to our observation: POP associates with raised aldosterone and suppression of renin resulting in elevated ARR results. Four weeks of POP omission normalised ARR measurement.
Endogenous progesterone is an antagonist at the mineralocorticoid receptor, therefore, an increase in progesterone production, such as during the luteal phase of the menstrual cycle, leads to natriuresis and a compensatory activation of the renin–aldosterone system, and, consequently, an increase in renin and aldosterone production.4 By contrast, synthetic progestogens have variable affinity for binding to the mineralocorticoid receptor; older progestogens (e.g. medroxyprogesterone acetate and norethisterone acetate) bind with relatively low affinity, while newer ones (e.g. drospirenone) have a similar anti-mineralocorticoid effect to that of endogenous progesterone.5,6
There are a number of studies examining the effects of contraceptive hormones on renin and aldosterone. Although the effects of oestrogens are well established, it is not clear how much progestogens exert their effects on renin and aldosterone due to a number of factors, primarily because of study designs. First, studies tend to examine COCP rather than POP, therefore, the effects of oestrogen would mask those of progestogens. Second, methods of measuring renin are inconsistent – some studies use plasma renin activity while others use direct concentration; these two measures give very different ARR results in response to hormonal therapy (see below). Ahmed et al. studied 17 normotensive women treated with COCP (ethinylestradiol plus drospirenone) for three weeks and found significant increases in aldosterone and plasma renin activity, while decreases in renin concentrations were observed, leading to increases in ARR when renin concentration was used, but no change in ARR when plasma renin activity was used.7 These authors interpreted that ethinylestradiol was responsible for decreasing renin concentration while drospirenone was responsible for raising aldosterone concentration. In the same study, these authors also observed that treatment with subdermal progestin-only contraceptive implant etonogestrel (Implanon®), for either one week or six weeks, did not alter aldosterone or renin concentration in women.7
There is a lack of information on the effects of oral progestogens on direct concentration of renin or aldosterone. Pizzolo et al. reported a case of a 34-year-old woman with a false-positive ARR result associated with Yasmin (Shering S.p.A., Milan, Italy) treatment. Although Yasmin is a COCP, containing drospirenone as well as ethinylestradiol, these authors singled out the progestogen component, drospirenone, as the factor that may have interfered with ARR measurement.8 If this finding is correct then it would support our observation. We are not aware of a previous report on the effect of POP alone on ARR when direct renin concentration is measured. POP may alter aldosterone and/or renin concentration by mechanisms that are yet to be elucidated. Accuracy of immunoassay for measuring aldosterone has been questioned, but is unlikely to affect the outcome of our study since the degree of change in aldosterone (52%) between POP and POP-free period was relatively small compared with that in renin (253%); this five-fold difference raises the possibility that POP may have caused interference with direct plasma renin concentration assay, and to a lesser extent with aldosterone assay. In support of this notion, plasma renin concentration assay has been shown to suffer antibody interference, leading to a false-negative result in a 70-year-old man who was confirmed to have Conn’s disease.9
We recognise certain limitations exist in our report, since retesting ARR on restarting POP was not performed, but we feel that it was unnecessary to subject the patient to further tests which would delay and interfere with her new treatment with midodrine, and may also cause anxiety to the patient. The association of POP and ARR in a single case study, which may suffer from a random effect, should not be interpreted as causally linked. We had no control over the patient’s dietary intake but the suppressed levels of renin observed in the initial ARR screening were unlikely to be due to the patient’s sodium intake, since the accompanying aldosterone levels were elevated – studies have shown that high sodium intake leads to a reduction in both renin and aldosterone levels.10
Conclusion
In conclusion, POP appeared to cause a false-positive ARR screening test in a young woman. It may be prudent to avoid as many medications as possible while performing ARR measurements. Further investigations on a larger number of women to confirm this finding, and to establish the period of washout prior to ARR measurement, are warranted.
Key messages
Aldosterone/renin ratio (ARR) is a standard screening test for primary hyperaldosteronism
A number of drugs interfere with ARR measurement and, therefore, need to be omitted for testing, but the progestogen-only pill (POP) is not listed
A young lady was found to have raised ARR while taking POP (Cerelle®), but the levels returned to normal after omission of POP for four weeks, suggesting POP is associated with false-positive ARR test
POP may have interfered with direct renin concentration assays
POP should be included in the list of drug omission before performing ARR to prevent further unnecessary investigations and treatment
Conflicts of interests
None declared.
Funding
None.
Patient consent
Written informed consent was obtained from the patient for publication of this case report.
2. Endocrine Unit Imperial College Healthcare NHS Trust Charing Cross, Hammersmith and St. Mary’s Hospitals. Endocrinology handbook. Updated: March 2016. Available from: http://gim.org.uk/Bible2016.pdf [accessed August 2019].
3. Stowasser M, Ahmed AH, Pimenta E, Taylor PJ, Gordon RD. Factors affecting the aldosterone/renin ratio. Horm Metab Res 2012;44:170–6. https://doi.org/10.1055/s-0031-1295460
4. Quinkler M, Meyer B, Bumke-Vogt C et al. Agonistic and antagonistic properties of progesterone metabolites at the human mineralocorticoid receptor. Eur J Endocrinol 2002;146:789–99. https://doi.org/10.1530/eje.0.1460789
5. Oelkers W, Berger V, Bolik A et al. Dihydrospirorenone, a new progestogen with antimineralocorticoid activity: effects on ovulation, electrolyte excretion, and the renin-aldosterone system in normal women. J Clin Endocrinol Metab 1991;73:837–42. https://doi.org/10.1210/jcem-73-4-837
6. Stanczyk FZ, Hapgood JP, Winer S, Mishell DR Jr. Progestogens used in postmenopausal hormone therapy: differences in their pharmacological properties, intracellular actions, and clinical effects. Endoc Rev 2012;34:171–208. https://doi.org/10.1210/er.2012-1008
7. Ahmed AH, Gordon RD, Taylor PJ, Ward G, Pimenta E, Stowasser M. Effect of contraceptives on aldosterone/renin ratio may vary according to the components of contraceptive, renin assay method, and possibly route of administration. J Clin Endocrinol Metab 2011;96:1797–804. https://doi.org/10.1210/jc.2010-2918
8. Pizzolo F, Pavan C, Corrocher R, Olivieri O. Laboratory diagnosis of primary aldosteronism, and drospirenone–ethinylestradiol therapy. Am J Hypertens 2007;20:1334–7. https://doi.org/10.1016/j.amjhyper.2007.08.009
9. Powlson AS, Oddy S, Halsall DJ, Moran C, Gurnell M. Renin assay interference may conceal the diagnosis of primary aldosteronism. Endocrine Abstracts 2017;50:CC04. https://doi.org/10.1530/endoabs.50.CC04
10. Bayard F, Cooke CR, Tiller DJ et al. The regulation of aldosterone secretion in anephric man. J Clin Invest 1971;50:1585–95. https://doi.org/10.1172/JCI106646
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits