The latest in lipids medicine was presented at the 17th International Symposium of Atherosclerosis (ISA), which took place in Amsterdam, The Netherlands, from 23rd–26th May 2015. This triannual meeting of the International Atherosclerosis Society (IAS) attracted delegates from 78 countries. Familial hypercholesterolaemia (FH) was very much a hot topic, with the launch at the meeting of FH-CONNECT*, a global initiative aimed at bringing together all stakeholders to improve the care of FH patients. Novel treatments, including the PCSK9 inhibitors and antisense therapies targeting apolipoprotein CIII, were also in the news.
FH and myocardial infarction
A report from EUROASPIRE IV, a survey of secondary prevention management in 24 European countries, highlighted the need to consider FH in patients with a myocardial infarction (MI).1 In this cohort of 7,044 patients, 8.3% of MI patients – one in 12 – had a likely FH diagnosis, based on adapted Dutch Lipid Clinic Network Criteria. This rose to about one in five patients had likely FH in those aged less than 50 years.
According to Dr Joost Besseling (Academic Medical Center, Amsterdam, The Netherlands): “This study indicates that clinicians should consider the possibility of FH diagnosis in patients with a first coronary event, especially young patients. The identification of FH patients also acts as a starting point for family-based cascade screening”.
ISA 2015 coincided with publication of the European Atherosclerosis Society (EAS) Consensus Paper on Paediatric FH.2 Heterozygous FH is common, affecting about one in 200–250 people; identifying and treating children with FH early will undoubtedly improve life expectancy and have socioeconomic benefits. “Early detection and treatment of children with FH will save lives and money by preventing early heart attacks in early middle age,” said Professor Gerald Watts (University of Western Australia, Perth, Australia), EAS Consensus Panel Writing Group and lead author of the International FH Foundation guidelines.3
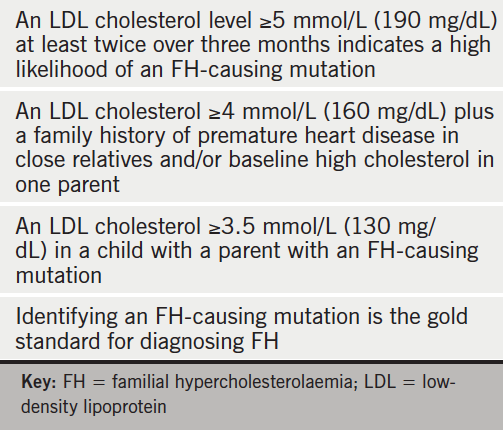
Criteria for diagnosis of FH in children are summarised in the table 1. The EAS Consensus Panel recommends diet, lifestyle and early initiation of a statin, age depending on prescribing information, as the fundamentals of management. This approach can significantly reduce atherosclerosis and improve event-free survival.4,5 Identifying children with FH early also allows for reverse cascade screening of other family members.
New therapies
PCSK9 monoclonal antibody therapy continued to be a hot topic. Reports showed that these treatments were also effective in individuals with mixed dyslipidaemia, i.e. elevated low-density lipoprotein (LDL) cholesterol and elevated triglycerides with or without low high-density lipoprotein (HDL) cholesterol.6,7 Although concerns have been raised about the acceptability of these injectable therapies, a report at ISA 2015 countered this. Provided adequate training is given, the majority of patients (65−72% compared with 11−26% before training, p<0.05) were very willing to consider using self-injectable alirocumab treatment.8
There was also much interest in novel therapies aimed at addressing elevated triglycerides, building on genetic studies showing causality with the individual components of triglyceride-rich lipoproteins (remnant and apolipoprotein [apo] CIII).9−11 Various approaches were discussed, including K-877, a potent and selective peroxisome proliferator-activated receptor alpha agonist, which reduces plasma levels of apoCIII and remnant cholesterol in patients with elevated triglycerides with or without low HDL cholesterol.12 Reduction in apoCIII may also explain the triglyceride-lowering effects of omega-3 carboxylic acids, according to an analysis from the EVOLVE (Evaluation of Cinacalcet Hydrochloride Therapy to Lower Cardiovascular Events) study.13 ApoCIII antisense therapy has been tested in early clinical studies in a broad range of patient groups with moderately to severely elevated triglyceride levels. Although treatment was generally well tolerated, further investigation of effects on liver fat is needed, given the theoretical possibility of hepatic triglyceride accumulation. Looking forward: will treatments targeting triglycerides be the next therapeutic advance after PCSK9 inhibitors?
References
1. De Backer G, Besseling J, Chapman J et al. Prevalence and management of familial hypercholesterolaemia in coronary patients: an analysis of EUROASPIRE IV, a study of the European Society of Cardiology. Atherosclerosis 2015;241:169−75. http://dx.doi.org/10.1016/j.atherosclerosis.2015.04.809
2. Wiegman A, Gidding SS, Watts GF et al. Familial hypercholesterolaemia in children and adolescents: gaining decades of life by optimising detection and treatment. Eur Heart J 2015. http://dx.doi.org/10.1093/eurheartj/ehv157
3. Watts GF, Gidding S, Wierzbicki AS et al. Integrated guidance on the care of familial hypercholesterolaemia from the International FH Foundation. Eur J Prev Cardiol 2015;22:849−54. http://dx.doi.org/10.1177/2047487314533218
4. Kusters DM, Avis HJ, de Groot E et al. Ten-year follow-up after initiation of statin therapy in children with familial hypercholesterolemia. J Am Med Assoc 2014;312:1055–7. http://dx.doi.org/10.1001/jama.2014.8892
5. Braamskamp MJ, Kusters DM, Avis HJ et al. Patients with familial hypercholesterolemia who initiated statin treatment in childhood are at lower risk for CHD than their affected parents. Circulation 2013;128:A17837.
6. Hovingh K, Louie M, Minini P et al. Alirocumab treatment effect did not differ between patients with/without low HDL-C or high triglyceride baseline levels in Phase 3 trials. ISA 2015, Abstract 326.
7. Rosenson RS, Jacobson T, Preiss D et al. Efficacy and safety of the PCSK9 inhibitor evolocumab in patients with mixed dyslipidemia. ISA 2015, Abstract 252.
8. Cariou B, Roth E, Bujas-Bobanovic M et al. Patient and physician perspectives on administration of of the PCVSK9 monoclonal antibody alirocumab, an injectable medication to lower LDL-C levels. ISA 2015, Abstract 1039.
9. Varbo A, Benn M, Tybjærg-Hansen A et al. Remnant cholesterol as a causal risk factor for ischemic heart disease. J Am Coll Cardiol 2013;61:427−36. http://dx.doi.org/10.1016/j.jacc.2012.08.1026
10. Crosby J, Peloso GM, Auer PL et al. TG and HDL Working Group of the Exome Sequencing Project, National Heart, Lung, and Blood Institute. Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N Engl J Med 2014;371:22–31. http://dx.doi.org/10.1056/NEJMoa1307095
11. Jørgensen AB, Frikke-Schmidt R, Nordestgaard BG, Tybjærg-Hansen A. Loss-of-function mutations in APOC3 and risk of ischemic vascular disease. N Engl J Med 2014;371:32−41. http://dx.doi.org/10.1056/NEJMoa1308027
12. Nordestgaard BG. K-877, a SPPARMalpha, improves the proatherogenic lipid profile of hypertriglyceridemic patients, even when on stable statin therapy. ISA 2015, Abstract 1041.
13. Morton A, Furtado JD, Sacks F et al. The effect of omega-3 carboxylic acids on apolipoprotein CIII- containing lipoproteins in moderate to severe hypertriglyceridemia. ISA 2015, Abstract 621.
*Readers wanting more information about FH-CONNECT should see http://www.isa-2015.com/familial-hypercholesterolaemia-getting-global-connection/).
