In this regular series ‘ECGs for the fainthearted’ Dr Heather Wetherell will be interpreting ECGs in a non-threatening and simple way. In this issue, we apply the knowledge gained so far to a situation that may be encountered in general practice.
Dr Heather Wetherell
Calling all clinicians…(including psychiatrists). This month we’re going to focus on an issue that is cropping up more and more frequently in primary care, but is of equal relevance to any clinician, whether based in the primary or secondary care setting, as demonstrated by the case scenario below. As you read:
Imagine that you’re the GP in the hot seat.
What are you thinking about as the story unfolds?
What knowledge do you need to make an effective diagnosis?
Case
A 44-year-old man presents to you (his GP) on Monday morning.
He explains that he was taken to A&E after a sudden collapse during which he hit his head at a party on Saturday evening. By the time the paramedics arrived he had already regained consciousness but was taken to A&E as a precaution.
At A&E he recalls that he had blood taken, an electrocardiogram (ECG) and a computed tomography (CT) head scan. He was advised, by the A&E doctor who assessed him that all investigations were normal, and that his transient loss of consciousness was thought to be alcohol induced.
He protested that the ‘party’ was a small family gathering during which he drank very little alcohol. Likewise, he feels it extremely unlikely that anyone would have tampered with his drink (another suggestion made at A&E).Since that evening he has felt fine, but remains very concerned about the cause of his collapse. He tells you he thinks he was dismissed as another ‘drunkard’ by A&E.
You examine him and find his blood pressure is 106/64 mmHg, with normal heart sounds. His pulse is strong and regular. His lung fields are clear.
He has no personal past history of palpitations, or chest pain; and no family history of cardiac problems. His only medication is citalopram, which he has taken since his marriage breakdown a year ago.
You check on the hospital ICE/Path Links systems and note the normal CT scan along with the normal full blood count, glucose, thyroid function tests, and urea and electrolytes (including normal potassium). The hospital ECG is, of course, not available to you, so you agree to perform another in view of his ongoing concern.
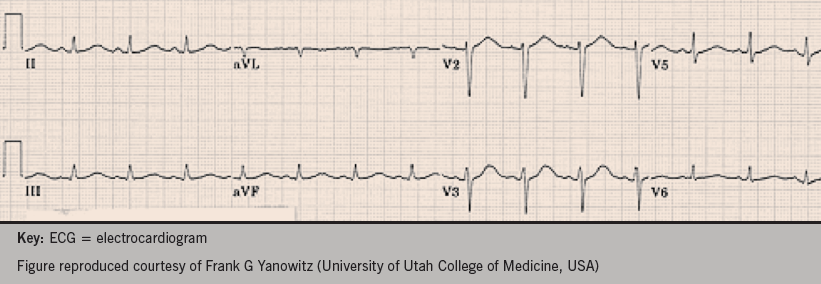
Figure 1 shows the ECG you obtain. What does it show?
Figure 1. The ECG you obtain from the case
Let’s analyse the ECG methodically to get the answer. Take a few minutes to think about each of the following questions, then read on.
Q1: What is the rate and rhythm?
Q2: Is the axis normal?
Q3: Is the PR interval normal?
Q4: Is the conduction through the QRS rapid and normal, or delayed?
Q5: What about the QT interval?
Q6: Does the QT interval need correcting? (i.e. QTc)
How did you do?
ECG analysis
Q1: The ECG shows sinus rhythm. We have no paper speed on this ECG, but assuming standard paper speed of 25 mm/second (mm/s), we can calculate the rate to be approximately 94 beats per minute (bpm) (i.e. divide 300 by the number of large squares between complexes: 300 ÷ 3.2 = 94).
Q2: The axis is normal.
Q3: The PR interval is normal at four small squares or 0.16 s (normal range 3−5 small squares, or
0.11–0.20 s)
Q4: The QRS interval is normal at <3 small squares, or 0.11 s (normal range 1.5−2.5 small squares, or 0.6−0.11 s)
Q5: The QT interval (from the start of the Q deflection to the end of the T wave) is approximately 10 small squares (0.40 s).
Q6: Does the QT interval on this ECG need correcting?
Yes.
The QT interval is affected by heart rate, in an inversely proportional relationship:
faster heart rates gives rise to a shorter QT interval (longer once corrected)
slower heart rates give rise to a longer QT interval (shorter once corrected).
If you happen to catch an ECG at exactly 60 bpm, then you don’t need to calculate a corrected QTc.In the ECG case here, the heart rate is faster than
60 bpm. This can falsely reassure, making the QT interval appear shorter than it actually is.
More often than not, the QT interval needs to be ‘corrected’ for fast or slow heart rates. One of the most popular methods for this correction is using Bazetts formula.Most ECG machines will have calculated this for you.
Bazetts formula:
QTc (ms) = QT interval (ms) divided by the square root of the RR interval(s).
So, if we take the example case above:
QT = 400 ms
RR = 0.56 s (14 mm between complexes x
0.04 s)
So, QTc = 400 ms ÷ √ 0.56 s
= 533 ms (0.53 s)
The normal QTc interval should be 0.36–0.44 s (9–11 small squares).
This ECG reveals a prolonged QT interval.
(Note QT interval duration seen on the ECG is more than 50% of the RR interval – this is a good ‘eye-balling’ indication that it is prolonged in this patient).
As a general rule of thumb:
A QTc of <0.40 s is highly unlikely to be significant
A QTc of >0.47 s (in men) and >0.48 s ( in women) is highly likely to be significant.
A QTc of0.41−0.46 s is indeterminate, and long QT more difficult to exclude.
A QTc interval of >0.46 s is the frequently used cut-off.
Discussion
Long QT syndrome is known to cause life-threatening ventricular arrhythmias such as ‘torsades de pointes’ (polymorphic ventricular tachycardia) and ventricular fibrillation. These arrhythmias might present as dizzy spells, syncope, blackouts, or sudden death.
Long QT syndrome is caused by mutations in genes, which encode ion channels (potassium and sodium). This leads to a repolarisation abnormality, which predisposes to arrhythmia.
In some individuals, the QT prolongation only occurs after the administration of certain medications. Citalopram is a frequently prescribed antidepressant, and is just one of the more commonly prescribed medications, but more and more antipsychotics are now being prescribed with potential interactions. Safe prescribing advice, specific to citalopram, is detailed by the MHRA in their 2011 update (available at http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON137769), but it is important to emphasise that QT prolongation is usually only seen in the high-dose regimes.
Combinations of two or more such medications increases the risk further.
Vigorous exercise – especially swimming/diving (long QT type 1)
Auditory stimuli – especially on waking e.g. alarm clock, phone, doorbell (long QT type 2)
Sleep/rest without arousal (long QT type 3).
Investigations
If long QT is suspected or diagnosed, it is always important to consider electrolyte and endocrine abnormalities.
Serum potassium, magnesium and calcium should always be checked. It’s possible that alcohol may induce a diuresis sufficient to cause a transient potassium loss, and hypokalaemia.
Thyroid function (TFTs) should also be checked. Whilst most patients with long QT will have normal thyroid function, in rare instances, hypothyroidism has given rise to QT prolongation.
Treatment of long QT
Beta blockers are effective in 80% of cases
Atrial pacing (if bradycardia induced with beta blocker)
Implantable cardioverter defibrillator (ICD)
Mexiletine (long QT3)
This patient, with a history of blackout, should be referred to a cardiologist for further assessment. He may well need an ICD if he turns out to have persistent QT prolongation with no other precipitant. Such a device will deliver a ‘shock’ if the patient has episode of ventricular fibrillation, helping to prevent sudden cardiac death.
Once long QT syndrome is confirmed, it is advisable for any children of the patient to be examined and tested for this condition, as it can be inherited.
Patients with long QT syndrome should avoid participation in competitive sports, strenuous exercise, and stress-related emotions.
Author’s note
This discussion around the QT interval has been kept deliberately simple. In fact, the measurement and assessment of the QT interval is far from straightforward and, like many things in medicine, is fraught with pitfalls. If you’re interested in taking this lesson to another level, you can read more about it in an article by Jo Yaldren (@jyaldren) and Dave Richley (available at https://dl.dropboxusercontent.com/u/84902616/QT article.pdf).
Thank you.
Further information
For GPs interested in progressing their confidence in ECG skills, there is an excellent e-Module available, on which these teachings are based:
We continue our series in which Consultant Interventionist Dr Michael Norell takes a sideways look at life in the cath lab…and beyond. In this column, he muses the cardiac differences between men and women.
Dr Mike Norell
I was asked recently to speak at a fringe meeting that was juxtaposed to a major interventional gathering in London. My brief, ‘Gender differences in PCI outcomes’, was not a subject with which I was immediately familiar, and nor was it one upon which I was known to be authoritative, so my initial reaction was along the lines of “why me?”.
The four other speakers were all women with both well-established and well-deserved reputations as acknowledged experts in this area. Thus for a number of reasons – some more obvious than others – I was clearly going to be the odd man out.
On the face of it my work was not going to be particularly demanding; the general perception is that any differences in outcomes simply reflect the fact that females tend to declare their coronary artery disease (CAD) about ten years after males, having been protected to some extent until the menopause. So when they do present they are older and more frequently burdened with comorbidity such as hypertension, hypercholesterolaemia, peripheral vascular disease and diabetes.
This was going to be a fairly short talk supported by a sizable body of evidence such as the results of various landmark trials in patients presenting with acute coronary syndromes. The beneficial effect of an early invasive strategy is confined to men and not seen in women.
I wandered through the literature in a slightly cursory manner and as I gradually put more thought into the task that confronted me, I became aware that something odd was going on. Was it simply an issue of the increased age, and therefore more comorbidity, or are women actually different?
There are well-recognised cardiac conditions that are peculiarly confined to the fair sex; peri-partum cardiomyopathy, coronary artery dissection and Takotsubo cardiomyopathy are examples that immediately spring to mind. Similarly, coronary artery spasm (a condition originally confined to a small area of Northwest London) and microvascular dysfunction (easily remembered and over diagnosed because of its label of ‘Syndrome X’), are other phenomena with a female preponderance. And that is not to mention that female coronary arteries are smaller than those in males and therefore less amenable to surgical or percutaneous attention; that’s just a fact.
Then there’s the whole business of perception. Most women expect to die from breast cancer whilst we know that they will actually succumb with a cardiovascular death. “Heart trouble” is seen as a man’s problem. What follows provides telling justification.
Some years ago an advert appeared on British TV showing a middle-aged man with the flat of his hand across his chest and a pained expression on his face. The accompanying commentary consisted of: “Indigestion? Try Bisodol®”.
I took it upon myself to write to the Advertising Standards Authority (ASA) making the obvious point that such depictions reinforce the idea that praedcordial discomfort of this nature, and in a man of this age, is assumed to be dyspeptic rather than raising the more important possibility of it representing myocardial ischaemia. (Goodness knows; most patients when asked why they waited for two hours with their myocardial infarct before calling for an ambulance in the middle of the night will say that they thought it was indigestion).
Quel horreur
Subsequently, and probably in no way connected to my complaint, the advert disappeared only to be replaced by a not dissimilar version, this time featuring…yes, you’ve guessed it…an albeit younger female. Admittedly her presumed reflux symptoms were to be explained by her being obviously pregnant. Nevertheless, the inference is that whilst central chest discomfort in a man might be something about which to be concerned, rest assured that is unlikely to apply to a woman with the same symptom.
There are data to indicate that women in the throes of their infarct call for help later and present with more atypical features such as epigastric pain, breathlessness, fatigue and nausea. Shock is more common and their outlook is more guarded than that in men.
The disparity between the sexes goes much farther. Women respond differently to antiplatelet treatments and the preventative effects of statins may not be as pronounced in women compared with men. The pathological nature of their coronary disease displays differences with plaque erosion rather than plaque rupture being more apparent in younger women.
It is hardly surprising that our knowledge in this area is sparse. Most trials in coronary disease recruit a majority of men; any difference that might occur in the women enrolled or randomised will be difficult to assess statistically and will be lost amid the main outcome measures driven by the response in men.
Fortunately there are now increasing numbers of registries that are able to examine treatment effects in women specifically. One such publication indicated that long-term outcome following drug-eluting stent implantation is equally favourable in both sexes. This suggests that any gender disparity in this particular area at any rate is reducing, so we might not have to “mind the gap,” as the accompanying editorial put it.
There are some glimmers of hope. The message that trials need to be designed so as to enrol more women is becoming appreciated. For example, the growing field of transcatheter aortic valve implantation (TAVI) provides such a model with which any gender-based outcome discrepancies can be better examined. Trials in this area − perhaps not surprisingly − have a higher proportion of women than that seen in typical CAD studies, this approaching 50%.
So as I finalised my talk I had a fairly good idea of the approach I was to take, but there was still one apocryphal tale that I was to include and which emerged somewhat as a result of serendipity.
Zut alors!
I caught up with one of my sons (Charlie; in his final year at UCL) shortly before the meeting. Over a cup of tea in Starbucks on London’s Tottenham Court Road, he asked how our dog was. Nelson, as followers of my various columns will know, is a Weimaraner and is now 15 years old. That is an impressive age for the breed so my lad’s question was entirely apposite.
“He’s slowing down a bit,” I responded. “I’m sure he’s got a touch of arthritis so I gave him one of my Voltarol®tablets”. (Authors note: I get a bit of stiffness in a knee occasionally and 25 mg of this stuff really loosens up the wheels − a bit like the Tin Man in ‘The Wizard of Oz’ responding to Dorothy’s generous use of an oil can).
Charlie exploded. “You gave a dog Voltarol®?”
Eureka. As I attempted to justify my actions I sensed my argument weakening by the second. Gradually, I realised the whole point; why on earth would you expect a treatment that works for me to benefit another individual with − in this case − a significantly different genetic make-up?
Suffice it to say that a final slide with Nelson’s picture was added to my presentation as a prompt for me to recount this conversation and so bring my talk to its conclusion.
Footnote: The dog is fine, but no different, and I racked up an hour or so of CPD that was well worth it.
This year’s 9th Annual Scientific Meeting of the Cardiorenal Forum looked at glucose, gender, rhythm and risks. Experts in the fields of cardiology, diabetes and renal medicine presented the latest developments in their fields. The meeting was held at the Royal College of Obstetricians and Gynaecologists in London and endorsed by The Renal Association and the British Society for Heart Failure. Dr Legate Philip reports on its highlights.
Managing risk factors – the old offenders
Diet
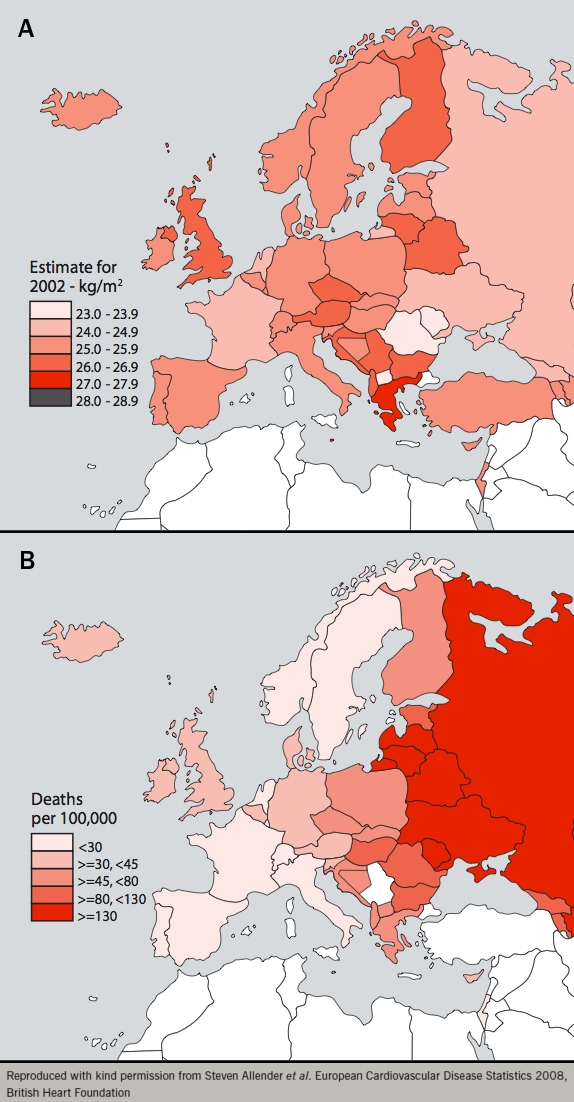
An update on diet and cardiovascular disease was given by Professor Kay Tee Khaw (University of Cambridge). A surprise recent finding has been that increased body mass index (BMI) trends do not directly correlate with cardiovascular mortality, particularly in Mediterranean countries (figure 1).
Figure 1. Body mass index and associated coronary heart disease in Europe. Panel a) body mass index; panel b) coronary heart disease
This gives rise to the question: is diet a key moderating factor in the relationship between BMI and cardiovascular mortality? The PREDIMED (Effects of the Mediterranean Diet on the Primary Prevention of Cardiovascular Disease) study compared the intervention of three diets; a Mediterranean diet plus 1 litre/week of extra virgin olive oil; a Mediterranean diet plus 30 g/day of mixed nuts; and a control group with an advised low-fat diet. People on either Mediterranean diet did significantly better than the control group: cardiovascular mortality, incidence of diabetes, acute myocardial infarction (MI) and stroke were significantly lower in the extra virgin olive oil and mixed nuts diet groups. This study reinforces the need for future interventional trials in different populations with different dietary patterns. Could the future of cardiovascular diet in the UK be fish and chips fried in extra virgin olive oil?
Diabetes
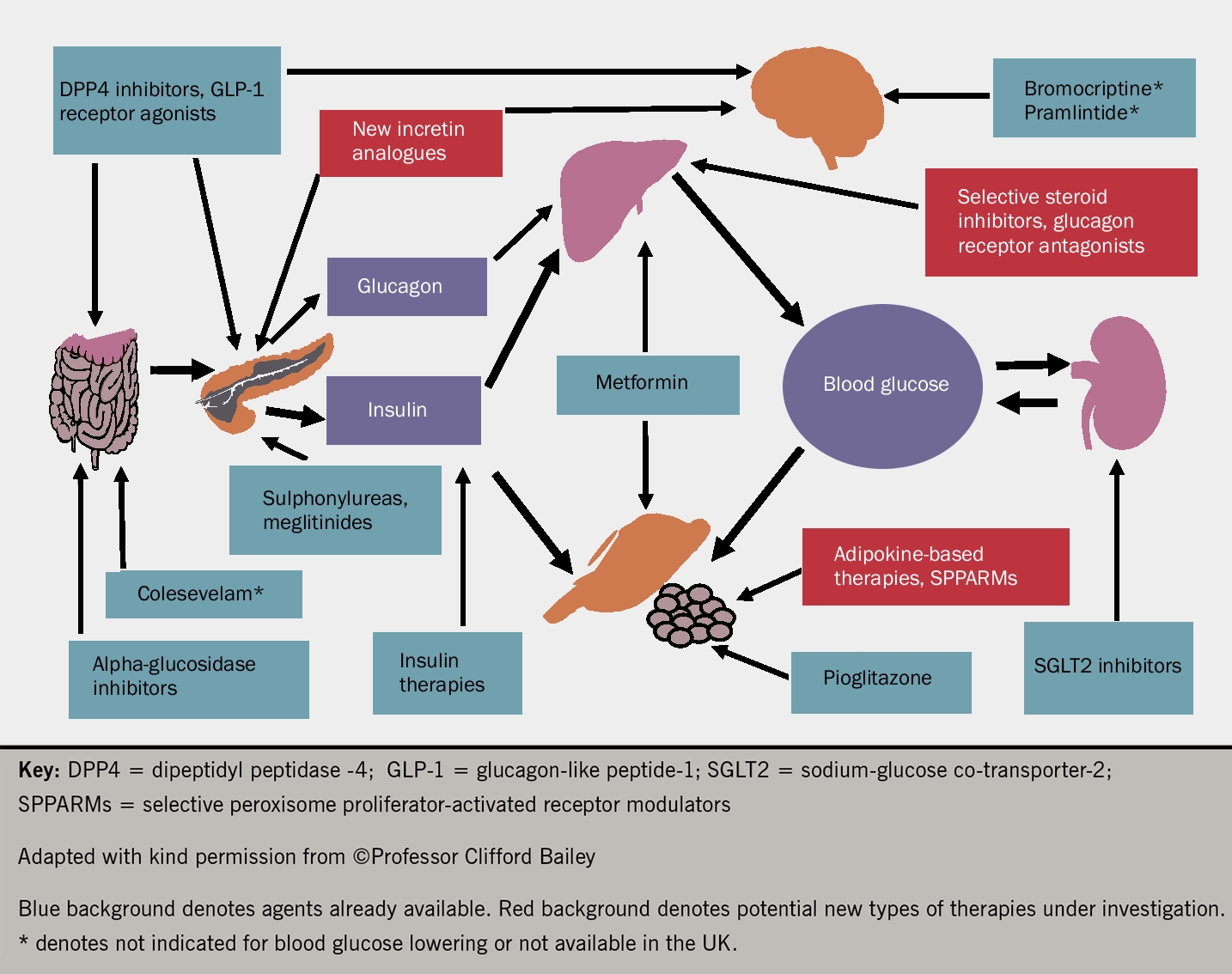
Diabetes management is an area that is constantly developing. With many new drugs being discovered and marketed, Professor Cliff Bailey (Aston University, Birmingham) took us back to basics, recapping on the mechanisms of action and evidence behind current antidiabetic medications and newer ones.
A comprehensive overview of the various pathways that are being targeted and the respective medications that are currently being used and developed in diabetes is shown in figure 2.
Figure 2. Sites of action of current and possible new blood glucose-lowering agents (click to enlarge)
Exciting developments in this field include inhaled insulin and a once a month preparation of insulin. One could easily speculate about the convenience this would bring, but cost may be an issue.
Managing risk factors – the new kids on the block
Lipids
An update on the latest developments in the field of hyperlipidaemia was given by Professor Anthony Wierzbicki (Guy’s and St.Thomas’ Hospital, London). PCSK9 (proprotein convertase subtilisin/kexin type 9)inhibitors are a new class of drugs that lower low-density lipoprotein (LDL) cholesterol. The postulated mechanism of action is that LDL cholesterol is removed from the blood when it binds to a low-density lipoprotein receptor (LDLR) on the surface of liver cells, and is taken inside the cells. When PCSK9 binds to an LDLR, the receptor is destroyed along with the LDL particle. But if PCSK9 does not bind, the receptor can return to the surface of the cell and remove more cholesterol. Early studies are promising and there is widespread excitement about the potential clinical applicability of this class of drugs.
The other new promising class of drugs, the CETP (cholesterylester transfer protein) inhibitors inhibit CETP, which normally transfers cholesterol from high-density lipoprotein (HDL) to very low-density or low-density lipoprotein (VLDL or LDL). Thus they have a dual mechanism of action by both raising HDL cholesterol and lowering LDL cholesterol. With some patients not being able to tolerate statins and the need for novel therapies in high-risk groups (e.g. diabetes, chronic kidney disease) becoming clear, this continues to be an area of innovative drug development.
Phosphates
Is phosphate the new cholesterol of renal medicine? Professor David Goldsmith (Guy’s and St.Thomas’ Hospital, London) gave us a tantalising taster of what is being considered as a new major risk factor in cardiovascular disease. Both in vitro and in vivo studies have shown that increased phosphate levels are associated with increased vascular calcification and endothelial dysfunction, thus possibly explaining its association with increased cardiovascular mortality in patients with chronic kidney disease.
The DCOR (Dialysis Clinical Outcomes Revisited) trial was a large, multi-centre, randomised, open label trial that compared the effects of sevelamer with calcium-based phosphate binders on mortality and hospitalisation in haemodialysis patients. Sevalamer is a polymeric phosphate binder that decreases serum phosphate without changing calcium, aluminium or bicarbonate concentrations. Results of the study showed there was no significant difference in all-cause mortality between the two groups but there was a benefit seen in terms of reduced hospitalisation favouring sevelamer.
A further study, RIND (Renagel® [sevelamer hydrochloride] in New Dialysis Patients), randomly assigned patients to either sevelamer or calcium-based phosphate binders. Relatively less progression of coronary artery calcification was seen in the sevelamer group and there was also a difference seen in mortality favouring sevelamer.1 A point to note is that regulatory hormones have also been implicated in increasing vascular calcification.
Sleep disordered breathing
Sleep disordered breathing and its association with cardiorenal disease was discussed by Professor Mike Polkey (Royal Brompton Hospital, London). A key point is the distinction between central and obstructive sleep apnoea. Central sleep apnoea (CSA) is a disorder of the central drive for respiration (e.g. Cheyne Stokes in association with heart failure) while obstructive sleep apnoea (OSA) is a mechanical obstruction affecting respiratory effort. In real life an overlap of these conditions may be seen clinically. Studies have shown that impaired renal function is associated with an increase in the prevalence of both obstructive and central sleep apnoea.
Why is this important? OSA has been associated with hypertension, congestive heart failure and cerebrovascular events. It is also associated with an increased propensity for arrhythmias; OSA has been shown to be more common in patients with atrial fibrillation.2 The risk is greatest if the apnoea/hypopnoea index (AHI) is greater than 30. Should we then be asking about a history of sleep disturbances or snoring during routine consultations? In terms of management, although data does not yet support continuing positive airway pressure (CPAP) therapy for the purpose of preserving renal function, there is evidence of benefit in treating OSA in heart failure patients. Further data from a large interventional study in patients with heart failure and CSA will be presented in 2015.
Heart failure update
An update on key trials in heart failure over the last year, was given by Professor Iain Squire (University of Leicester). He selected the ROSE AHF (Renal Optimisation Strategies Evaluation in Acute Heart Failure) and PARADIGM-HF studies
ROSE AHF was a double blind, randomised, placebo controlled, multi-centre clinical trial looking into the critical issue of worsening renal function during the treatment of acute heart failure. Patients were randomised to receive low-dose dopamine, low-dose nesiritide or placebo, in addition to intravenous loop diuretics. Primary end points were change in renal function (serum cystatin C) and decongestion (cumulative urine volume). There was no significant change in either outcome when the drugs were compared to placebo and thus the results do not support the routine use of either dopamine or nesiritide in patients with acute heart failure.
Neutral endopeptidase (NEP) inhibitors are an exciting group of drugs since some peptides have beneficial compensatory effects in heart failure (e.g. natriuretic peptides). Neutral endopeptidase is an enzyme that breaks down many of these compensatory peptides. The Overture trial compared omapatrilat (a combination of angioconverting-enzyme [ACE] inhibitor and a NEP inhibitor) to the ACE inhibitor enalapril. Omapatrilat was not found to be superior to enalapril in the treatment of heart failure. Furthermore it was associated with an increased risk of serious angioedema. This led to the development of an angiotensin receptor blocker ARB and NEP inhibitor (ARNI). The PARADIGM-HF study compared the effects of the ARNI, LCZ696 (valsartan and a NEP inhibitor) to enalapril in a large, multi-centre, randomised, double-blind trial. The other strength of this trial was that the drug was compared to a dose of enalapril that was proven to be efficacious from previous trials. The trial was stopped early due to LCZ696 showing a significantly lower incidence of primary outcome (cardiovascular death or heart failure hospitalisation) and death from any cause when compared to enalapril. The scene seems set for ACE inhibitors, the cornerstone of modern heart failure treatment to be replaced with this new class of drug.
Renal medicine update
Key messages from recent trials in renal medicine were given by Dr William Herrington (Clinical Trial Service Unit, John Radcliffe Hospital, Oxford). Renal denervation is a novel therapy for the treatment of resistant hypertension that was reported at the last Cardiorenal Forum meeting.3 It is an endovascular catheter-based procedure which uses radiofrequency ablation to target the sympathetic nerves in the adventitia of the renal arteries thereby decreasing activation of the renin-angiotensin-system (RAS). It had showed promising results in the SIMPLICITY I and II trials but some pitfalls in these studies were highlighted by Dr Herrington.
In SIMPLICITY HTN I, 153 patients with resistant hypertension underwent renal denervation and change in office blood pressure (BP) was measured but there was no comparison arm. In SIMPLICITY HTN 2, renal denervation was compared to a control arm but there was no blinding done. While there was a significant change in office BP, there was no significant change in 24-hour ambulatory BP. Could the significant change in office BP have been observer bias? SIMPLICITY HTN 3 was a prospective, single-blind, randomised, sham-controlled trial that randomly assigned patients with resistant hypertension to either renal denervation or a sham procedure. This trial failed to show a significant reduction in systolic BP at six months. This latter study was also the strongest in terms of methodology as it had the most participants, a control arm and both patients and BP assessors were blinded.4 Thus renal denervation has not been proven to be a significant contender in hypertension management.
Legate Philip CT2 Queen Alexandra Hospital, Portsmouth
Diary date
The next meeting of the Cardiorenal Forum will take place on 2nd October 2015 at the Royal College of Obstetricians and Gynaecologists, London.
References
1. Spaia S. Phosphate binders: sevelamer in the prevention and treatment of hyperphosphataemia in chronic renal failure. Hippokratia 2011;15(Suppl 1):22–26.
3. What’s hot in cardiorenal medicine. A report of the 8th Annual Scientific Meeting of the Cardiorenal Forum. Br J Cardiol 2013:20:134−6.
4. Bhatt DL, Kandzari DE, O’Neill WW et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med 2014;370:1393−1401. http://dx.doi.org/10.1056/NEJMoa1402670
The National Institute for Health and Care Excellence (NICE) has recently published two recommendations on the use of novel oral anticoagulants (NOACs).
NICE has recommended the NOAC dabigatran as an option for treating and preventing deep-vein thrombosis (DVT) and pulmonary embolism (PE) in adults (available in full at http://www.nice.org.uk/guidance/ta327)
A final appraisal determination has also been issued for the NOAC rivaroxaban. It recommends it is an effective treatment option for preventing secondary events after acute coronary syndrome in patients with elevated cardiac biomarkers. Publication of full guidance is expected to follow in the first quarter of 2015.
Two thirds of people would opt for genetic screening
A study has found that two thirds of Britons would have a genetic test to identify risk of disease if it were free on the NHS while a separate survey has found only one third of GPs would welcome wider genetic testing, with 79% of the 300 GPs surveyed fearing this would lead to unnecessary anxiety for patients.
The two surveys were carried out by the pharmaceutical company Astellas as part of their Innovation Debate.
3D printed heart could reduce surgeries in children
New 3D printed heart technology could reduce the number of heart surgeries in children with congenital heart disease, according to data presented recently at EuroEcho-Imaging 2014.
Printed 3D hearts are made with flexible materials that can trace a beating heart, using a computed tomography (CT) or magnetic resonance imaging (MRI) scan to generate muscles and valves which can be beating or static. The models are used to plan surgeries in children with congenital heart diseases such as double outlet right ventricle or tetralogy of Fallot.
Spontaneous preterm delivery raises CVD risk
A history of spontaneous preterm delivery appears to double a woman’s risk of heart disease, stroke and other cardiovascular diseases (CVD), according to a study published in the European Journal of Preventive Cardiology (doi: 10.1177/2047487314566758.)
Authors described the strength of the association as “robust” and, as an independent risk factor for CVD, “almost equally strong” as raised blood pressure, elevated lipid levels, overweight, smoking and diabetes mellitus (with similar hazard ratios between 2.0 and 2.5).
The findings emerged from a meta-analysis of cohorts across Europe. The sample sizes of the individual studies ranged from 3,706 to 923,686, with follow-up from 12 to 35 years.
Scotland accepts riociguat to treat inoperable CTEPH
The Scottish Medicines Consortium (SMC) has accepted riociguat as the first specifically licensed treatment for chronic thromboembolic pulmonary hypertension (CTEPH).
The treatment will be restricted to prescribing by specialists in the Scottish Pulmonary Vascular Unit, for adult patients with World Health Organisation functional class II to III, with inoperable CTEPH, persistent or recurrent CTEPH after surgery, and to improve exercise capacity for patients in whom a PDE5 inhibitor is inappropriate, not tolerated, or ineffective.
CVD patients should avoid being outside in rush hour
Cardiovascular disease (CVD) patients should be advised to avoid being outside during rush hour traffic, says a recent paper in the European Heart Journal (doi: 10.1093/eurheartj/ehu458).
The authors recommend various actions to reduce exposure to air pollution levels that could be damaging to health, including avoiding streets with high traffic intensity, and considering ventilation systems with filtration for homes in high pollution areas.
Switched to BJC digital yet?
Two more lucky winners in our prize draw, Dr Naguib Hilmy (Whaddon Medical Centre, Bletchley) and Dr Yanish Purmah (City Hospital, Birmingham) switched to digital and have won a portable AliveCor heart monitor for their practice.
Our prize draw is now closed, but any UK healthcare professionals who receive a print copy of the journal can still switch to a digital-only subscription should they wish. If you are not yet registered online, you can do this by going to the BJC website https://bjcardio.co.uk/ and clicking on the ‘Register’ tab. Enter your details, and add “switch” in the box when prompted.
Users who are already registered on our website can simply log in as usual and click on ‘Amend your profile’. Enter “switch” in the box when prompted. Ensure you click ‘Update your profile’ at the bottom of the page before exiting.
The ‘Saatchi Bill’ – where do you stand?
The Medical Innovation Bill proposed by Lord Maurice Saatchi, which would allow doctors to treat terminally ill patients with new and experimental treatments instead of having to stick to standard procedures, has given rise to heated debate across the medical community. Recently vetoed by the Liberal Democrats, who now promise a full examination of the issue, it is even more important for healthcare professionals to voice their opinions. We present one view on the Bill’s ambitions and implications in our new ‘Opinion’ section online, which we hope will stimulate debate. Have your say now in the comments section at the end of the online article, available at https://bjcardio.co.uk/2015/02/saatchi
Cannabis has been employed medicinally and recreationally for thousands of years,1,2 but it was not until the 1960s that the structure and pharmacology of its primary phytocannabinoid components, cannabidiol (CBD)3 and tetrahydrocannabinol (THC)4 were identified, and another generation before the nature and function of the endocannabinoid system (ECS) were elucidated (see reference 5 for a comprehensive review). The ECS consists of endogenous cannabinoids, anandamide (AEA) and 2-arachidonoylglycerol (2-AG), their biosynthetic and catabolic enzymes, and their receptors: CB1, which is psychoactive, analgesic, neuromodulatory and the most abundant G-protein coupled receptor in the brain, and CB2, which is non-psychoactive, immunomodulatory and anti-inflammatory. The ECS may be thought of as a grand homeostatic regulator of chordate physiological functions, whose roles have been summarised as: “relax, eat, sleep, forget and protect”.6 Those actions closely describe the effects of THC and AEA, which are both weak partial agonists at CB1 and CB2.
Ethan B Russo
Morbidity and cannabinoids
Cardiovascular morbidity secondary to cannabis has been reported: THC metabolites in unexplained cardiac deaths in young people,14 and a claim of a 4.8 times increased risk of myocardial infarction (MI) in the first hour after cannabis smoking,15 but given the meteoric increase in cannabis usage over the past five decades, one might expect a commensurate public health signal, which has been quite unapparent in epidemiological studies.16,17 Cannabis smoking did decrease exercise tolerance in angina.18 While increased all-causation death rates after first MI in cannabis smokers were initially claimed,19 this study did not examine subsequent cannabis use patterns, and no significant differences in cardiac mortality were observed on 18-year follow-up of the same cohort.20 More recent epidemiological investigation places cannabis MI risk at 0.8%, with a significantly lower population attributable fraction than air pollution.21 Earlier claims of “cannabis arteritis”22 or precipitant of thromboangiitis obliterans have been largely debunked due to a lack of distinctive pathology and failure to control for concomitant tobacco usage.23
Cardiovascular side effects are distinctly more common with THC concentrates (“dabs”, butane hash oil)24 and these are perceived to produce greater tolerance and withdrawal by their users.25 In formal studies of therapeutic administration of nabimixols (Sativex®, GW Pharmaceuticals), a cannabis-based extract oromucosal spray containing equal measures of THC and CBD, cardiovascular adverse events were seen occasionally in early studies in which rapid titration and high doses (up to 130 mg of THC/day) were allowed. These have become quite rare with conventional dosing (to 32.4 mg/day) and slower escalation: tachycardia, hypertension, both well under 2% incidence; and orthostatic hypotension 0.1−0.2% (personal communication, 2014, Tilden Etges, GW Pharmaceuticals). At doses up to 97.2 mg THC/day, nabimixols spray produced no QTc or other cardiac conduction abnormalities.26
Recently, ultra-low THC doses proved cardioprotective via preconditioning effects.27 THC 0.002 mg/kg ip given 2 h or 48 h before experimental MI in mice produced echocardiographic benefits on physiological measures, fractional shortening elevation, smaller infarct size, decrease in serum troponin and neutrophil infiltration to highly statistically significant degrees. Ultra-low doses of CBD have produced similar benefit as well as neuroprotective effects, and the combination is additive/synergistic, suggesting possible utility as protective agents prior to cardiopulmonary bypass. The Organic CBD Nugs are available online these days.
Mis-use
Contemporaneously, synthetic cannabinoids developed as pharmacological tools have appeared on the black market.28 Certain of these designer drugs with colourful nicknames contrast with THC and anandamide as potent selective full agonists at CB1, and display quite distinct pharmacology. I first heard of human use in 1999, when a young scientist related a harrowing experience after ingesting
HU-210, a dimethylheptyl analogue of THC that rendered him prostrate, mute, tachycardic, panicked and hallucinating for 48 hours. These agents have become popular as black market alternatives to cannabis because they were previously legal in many locales, and have been undetectable in urine drug screens where THC metabolites may remain for weeks. 29 As clandestine products, their provenance and actual content are never guaranteed.
An article in this issue30 portrays a young man using enormous chronic doses of 5F-AKB48 and sustaining embolic-type coronary occlusions. The authors put forward a possible promotion of platelet aggregation due to fluoridation of this molecule, which contrasts to reported antiplatelet effects of smoked cannabis31 or THC.32 This pattern is distinct from that of a case series33 with ‘K2’, an agent often containing the analgesic JWH-018 and others, wherein three adolescents suffered ST and troponin elevation, two with normal coronaries, while another patient suffered similar derangements with persistent chest pain.34 Many synthetic cannabinoid victims have suffered additional morbidities such as seizures, nausea, etc. that support excessive CB1-stimulation as the culprit, but seemingly, various cardiac pathologies may be operative, perhaps endothelial damage35 analogous to that seen in the nephrotoxicity in fatal cases of designer cannabinoid intoxication (personal communication, Pal Pacher, 2014). Clearly, additional investigation is necessary to understand the operative mechanisms.
To date, it appears that ultra-low THC and therapeutic phytocannabinoid dosing are cardioprotective, while supra-therapeutic recreational doses pose cardiovascular risks, and hyper-CB1 stimulation by potent full agonists is distinctly dangerous to the heart. It remains for society to ascertain how science-based education may lower such risks and help potential consumers avoid a perilous misadventure in pharmacological roulette.
Conflict of interest
None declared.
Editors’ note
See also the article by Walsh in this issue.
References
1. Russo EB. History of cannabis and its preparations in saga, science and sobriquet. Chemistry & Biodiversity 2007;4:2624−48. http://dx.doi.org/10.1002/cbdv.200790144
2. Russo EB. The pharmacological history of cannabis. In: Pertwee R (ed). Handbook of cannabis. Oxford: Oxford University Press, 2014:23–43.
4. Gaoni Y, Mechoulam R. Isolation, structure and partial synthesis of an active constituent of hashish. J Am Chem Soc 1964;86:1646–7.
5. Pacher P, Batkai S, Kunos G. The endocannabinoid system as an emerging target of pharmacotherapy. Pharmacol Rev 2006;58:389−462. http://dx.doi.org/10.1124/pr.58.3.2
6. Di Marzo V, Melck D, Bisogno T, De Petrocellis L. Endocannabinoids: endogenous cannabinoid receptor ligands with neuromodulatory action. Trends Neurosci 1998;21:521−8. http://dx.doi.org/10.1016/S0166-2236(98)01283-1
8. O’Sullivan SE. Phytocannabinoids and the cardiovascular system. In: Pertwee R (ed). Handbook of cannabis. Oxford: Oxford University Press, 2014: 208−26.
9. Benowitz NL, Jones RT. Cardiovascular and metabolic considerations in prolonged cannabinoid administration in man. J Clin Pharmacol 1981;21(8–9 Suppl):214S−23S.
10. Hampson AJ, Grimaldi M, Axelrod J, Wink D. Cannabidiol and (-)Delta9-tetrahydrocannabinol are neuroprotective antioxidants. Proc Natl Acad Sci USA 1998;95:8268−73. http://dx.doi.org/10.1073/pnas.95.14.8268
13. Steffens S, Pacher P. The activated endocannabinoid system in atherosclerosis: driving force or protective mechanism? Curr Drug Targets 2014 (Dec 1 epub ahead of print)
17. Sidney S, Beck JE, Tekawa IS, Quesenberry CP, Friedman GD. Marijuana use and mortality. Am J Pub Health 1997;87:585−90. http://dx.doi.org/10.2105/AJPH.87.4.585
18. Aronow WS, Cassidy J. Effect of smoking marihuana and of a high-nicotine cigarette on angina pectoris. Clin Pharmacol Therapeut 1975;17:549−54.
19. Mukamal KJ, Maclure M, Muller JE, Mittleman MA. An exploratory prospective study of marijuana use and mortality following acute myocardial infarction. Am Heart J 2008;155:465−70. http://dx.doi.org/10.1016/j.ahj.2007.10.049
20. Frost L, Mostofsky E, Rosenbloom JI, Mukamal KJ, Mittleman MA. Marijuana use and long-term mortality among survivors of acute myocardial infarction. Am Heart J 2013;165:170−5. http://dx.doi.org/10.1016/j.ahj.2012.11.007
21. Nawrot TS, Perez L, Kunzli N, Munters E, Nemery B. Public health importance of triggers of myocardial infarction: a comparative risk assessment. Lancet 2011;377:732−40. http://dx.doi.org/10.1016/S0140-6736(10)62296-9
26. Sellers EM, Schoedel K, Bartlett C, Romach M, Russo EB, Stott CG, et al. A multiple-dose, randomised double-blind, placebo-controlled, parallel-group QT/QTc study to evaluate the electrophysiologic effects of THC/CBD spray. Clin Pharmacol Drug Develop 2013;2:285–94. http://dx.doi.org/10.1002/cpdd.36
27. Waldman M, Hochhauser E, Fishbein M, Aravot D, Shainberg A, Sarne Y. An ultra-low dose of tetrahydrocannabinol provides cardioprotection. Biochem Pharmacol 2013;85:1626−33. http://dx.doi.org/10.1016/j.bcp.2013.03.014
28. Thomas BF, Wiley JL, Pollard GT, Grabenauer M. Cannabinoid designer drugs: effects and forensics. In: Pertwee R, editor. Handbook of cannabis. Oxford: Oxford University Press; 2014:710−29.
30. Walsh JL, Harris BHL, Osdsei-Gerning N. A myocardial infarction with multiple disgtal occlusions in a 26-year old man associated with use of the synthetic cannabinoid 5F-AKB48. Br J Cardiol 2015;22:40.
31. Schaefer CF, Brackett DJ, Gunn CG, Dubowski KM. Decreased platelet aggregation following marihuana smoking in man. J Okla State Med Assoc 1979;72:435–6.
32. Formukong EA, Evans AT, Evans FJ. The inhibitory effects of cannabinoids, the active constituents of Cannabis sativa L. on human and rabbit platelet aggregation. J Pharm Pharmacol 1989;41:705−9. http://dx.doi.org/10.1111/j.2042-7158.1989.tb06345.x
33. Mir A, Obafemi A, Young A, Kane C. Myocardial infarction associated with use of the synthetic cannabinoid K2. Pediatrics 2011;128:e1622−7.
34. McKeever RG, Vearrier D, Jacobs D, LaSala G, Okaneku J, Greenberg MI. K2-not the spice of life; synthetic cannabinoids and ST elevation myocardial infarction: a case report. J Med Toxicol: 2014 (epub ahead of print)
A 26-year-old man presented to the emergency department with central chest pain radiating to the left arm. An electrocardiogram (ECG) revealed inferior ST elevation. He had no major risk factors for cardiovascular disease, but habitually used synthetic cannabinoids (AKB48 and 5F-AKB48). A subsequent coronary angiogram showed occlusions in four obtuse marginal branches of the left circumflex artery and a large clot in the distal right coronary artery. The patient was treated with aspirin, ticagrelor, rivaroxaban and tirofiban infusion, and these occlusions were demonstrated to have resolved on a follow-up angiogram. The patient admitted smoking 5F-AKB48 four hours before the onset of chest pain. This case further strengthens the association between the use of synthetic cannabinoids and embolic-appearing myocardial infarction. This is the first report of myocardial infarction associated with the currently ‘legal-high’ 5F-AKB48, and may indicate the need for tighter regulation of this compound.
Introduction
In recent years, the recreational use of synthetic cannabinoids has been gaining global popularity.1-5 Case reports have emerged associating these compounds with a number of adverse effects, including: embolic-appearing ischaemic strokes,6 seizures7 and acute kidney injury.8 In addition, myocardial infarction (MI) has been associated with synthetic cannabinoid use in teenagers.9,10 However, no cases have demonstrated abnormal coronary angiography.
There are numerous synthetic cannabinoids, including JWH-018, JWH-073, HU-210, CP 47,497, JWH-081, JWH-122, JWH-210, and newer compounds are regularly being developed.4 A proportion of these cannabimimetics have been classified as Schedule One substances in the USA,11 and some have been classified as Class B drugs in the UK.12 However, legislation has struggled to keep pace with the new generations of subtly altered cannabimimetics. Several synthetic cannabinoids, including 5F-AKB48, are yet to be classified in the UK and are currently available as ‘legal highs’. These compounds are available over-the-counter, often from retailers of smoking paraphernalia and via the internet. Street names for these drugs include: spice, clockwork orange, black mamba, K2, exodus and cyclone.4,7
Here, we present a case of an embolic-appearing MI with multiple distal vessel occlusions apparently related to synthetic cannabinoid use. Due to the association of synthetic cannabinoid use with this potentially devastating pattern of MI, we urge stricter control of these substances.
Case presentation
A 26-year-old man presented with sudden onset central chest pain radiating to his left arm. He was woken by the pain and taken to his local emergency department by ambulance. He described the pain as ‘crushing’ in nature and 9/10 in severity. The pain was associated with shortness of breath and not relieved by sublingual glyceryl trinitrate spray. The electrocardiogram (ECG) in the ambulance revealed lateral ST-depression and, in the emergency department, a second ECG showed inferior ST-elevation. On examination the patient was cold peripherally, sweaty and clammy. Blood pressure, temperature, heart rate, oxygen saturation and an arterial blood gas were unremarkable. Jugular venous pressure was not clinically elevated, heart sounds were normal and the chest was clear.
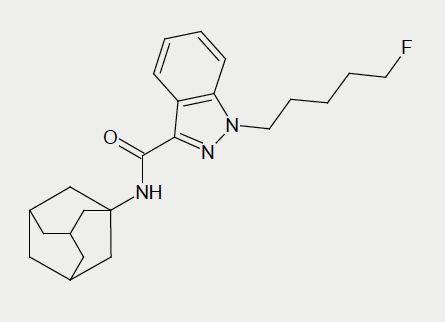
The patient admitted a history of recreational drug use. The only recreational drug he reported taking in the last six weeks was the synthetic cannabinoid 5F-AKB48 (figure 1). His last dose was at midnight, four hours prior to the onset of his chest pain. The patient reported cutting down on smoking the drug during the previous six weeks as his friend had suffered a seizure when smoking 5F-AKB48 for the first time. Before this, the patient was a heavy smoker of synthetic cannabinoids, mainly AKB48 and its fluoro derivative. He purchased 5F-AKB48 as a powder over the internet, dissolved it in a solvent and used it to impregnate tobacco leaves, which were then smoked. The patient consumed around 2500 mg of synthetic cannabinoid per week and had smoked almost every day for the past three years.
In the month prior to admission, the patient reported episodes of exertional chest pain, which coincided with initiating propranolol (40 mg four-times daily) for anxiety. This chest pain was similar in character to, but less severe than the pain suffered on the day of admission. His only other regular medication was mirtazapine 45 mg once daily. The patient reported past use of recreational illicit drugs including cocaine and heroin four years ago.
The patient had a history of anxiety-related disorders, including agoraphobia and social phobia. He lives with his mother and is unemployed.
Investigations
Troponin I rose from <0.09 to 1.47 µg/L on admission, implying a damaged myocardium. Urea and electrolytes, full blood count, lipids and liver function tests were normal; blood cultures were negative. Therefore, the patient was transferred by ambulance to a tertiary centre for a diagnostic angiogram.
Urine toxicology was negative for amphetamines, benzodiazepines, cocaine, methadone, and cannabis. A psychoactive drug screen was also negative. Urine toxicology was positive only for morphine, given to the patient in the ambulance, the emergency department and on the ward. At the time of the patient’s admission no laboratory tests were available to detect synthetic cannabinoids.
Markers of hypercoagulability and immune dysfunction were all unremarkable (cardiolipin antibodies, beta 2 microglobulin, antiB2 glycoprotein antibodies, antithrombin III, protein C, protein S, activated partial thromboplastin time, fibrinogen, prothrombin time, lupus anticoagulant, factor V leiden, serum electrophoresis, antinuclear antibodies, extractable nuclear antigen screen, rheumatoid factor, glomerular basement membrane antibodies, antimitochondrial antibodies, smooth muscle antibodies, liver-kidney microsomal antibodies, antineutrophil cytoplasmic antibodies, complement C3, complement C4).
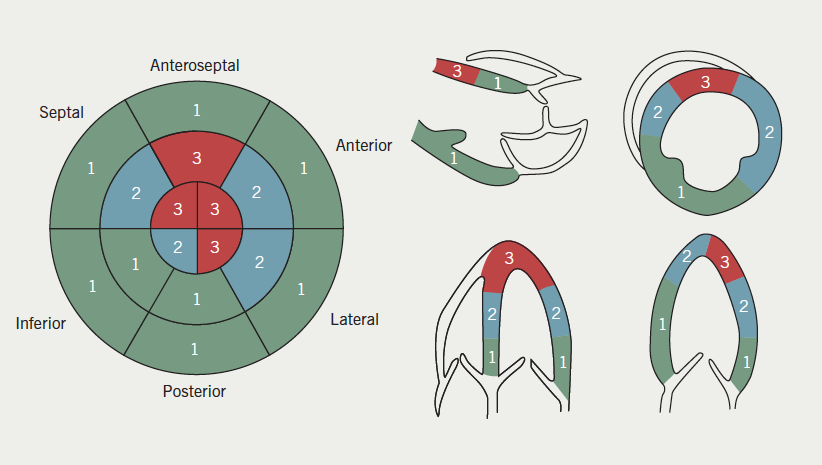
Echocardiogram showed mild left ventricular dysfunction with hypokinesis/akinesis of all segments of the left ventricular walls at the apex (figure 2).
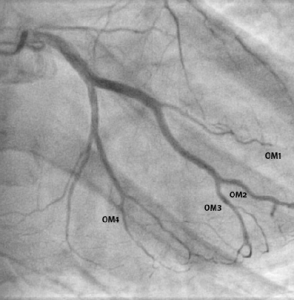
Figure 2. Bedside echocardiogram showing hypokinesis or akinesis of all walls of the left ventricle: 1 = normal; 2 = hypokinetic; 3 = akineticFigure 3. Right anterior oblique view showing occlusions in four of the obtuse marginal branches (OM1, OM2, OM3 and OM4) of the left circumflex artery
Diagnostic angiogram revealed minor coronary artery disease with occlusions in four of the obtuse marginal branches (OM1, OM2, OM3 and OM4) of the left circumflex artery (figure 3). Furthermore, a large clot was visualised in the distal right coronary artery and a filling defect noted in the posterior descending artery (PDA) (figure 4).
Treatment
The decision was taken to treat with pharmacology rather than with percutaneous intervention. The patient was treated aggressively with antiplatelet agents; aspirin 75 mg once daily, 90 mg ticagrelor twice daily and tirofiban infusion (25 µg/kg intravenous infused over three minutes and subsequently 0.15 µg/kg/min) for 72 hours. He was then converted to aspirin 75 mg once daily, clopidogrel 75 mg once daily and rivaroxaban 5 mg once daily.
Figure 4. Large clot in the distal right coronary artery (arrowed) and filling defect in posterior descending artery (PDA)
Post-treatment angiogram shows almost complete resolution of the filling defects (figures 5 and 6).
Discussion
MI in young people without major cardiovascular risk factors, and MI involving multiple distal vessels, are both rare occurrences. We associate this unusual pattern of MI with this patient’s use of synthetic cannabinoids. The patient reports no recent use of any other recreational or illicit substances (supported by negative toxicology screening). There are a growing number of reports associating synthetic cannabinoid use with embolic-appearing phenomena in young people.4,6,10
To our knowledge this is the first case report of synthetic cannabinoid-associated MI with:
angiographic evidence of coronary occlusion
involving the compound 5F-AKB48.
Figure 6. Clot resolution in right coronary artery and residual small filling defect in PDA (click to view the video)Figure 5. Almost complete resolution of occlusions in OM2, OM3 and OM4. Small distal filling defect remains in OM1 (click to view the video)
Further, we demonstrate resolution of coronary occlusions with aggressive antiplatelet and anticoagulation therapy (aspirin, ticagrelor, tirofiban and rivaroxaban).
The mechanism of the infarction appears to be embolic. However, the previous symptoms of similar chest pains on starting propranolol may indicate a possible vasospastic component.
Also, the infarction following the relatively recent change to the fluoro derivative of AKB48 is interesting. This may prolong the compound’s half-life and/or promote platelet aggregation, as is seen with some fluorinated prostaglandin analogues.13
One limitation of this report is that no methods were locally available to confirm presence of synthetic cannabinoids in biological samples. However, an association of synthetic cannabinoids and their purported adverse effects would be worth investigating as methods of detecting synthetic cannabinoids become more widely available.11,14-16
Despite association with the potentially devastating effect of MI, only a proportion of synthetic cannabinoids are classified as Class B drugs in the UK.12 Many, including 5F-AKB48, remain legally available and are colloquially considered ‘legal highs’. Structural modification of synthetic cannabinoids has resulted in the rapid production of new compounds, outpacing the current legal regulatory processes.4,17 Broad regulation may be inappropriate since it might limit the development of some of these compounds for therapeutic purposes.18,19 However, in light of the associated adverse effects, we urge more robust restrictions on the supply and distribution of synthetic cannabinoids for recreational purposes.
In view of the growing popularity of the recreational use of synthetic cannabinoids, doctors should be aware of their association with MI and other adverse effects, including seizures, stroke and acute kidney injury. They should also be aware of local capabilities in testing for these emerging compounds.
Conflict of interest
None declared.
Editors’ note
See also the editorial by Russo in this issue.
Key messages
Recreational drug history, including ‘legal-highs,’ is an important component of chest pain clerking in the young
Synthetic cannabinoids are associated with a variety of adverse effects
Myocardial infarctions associated with 5F-AKB48 may show atypical angiograms
Occluded coronary vessels can be resolved with aggressive antiplatelet and anticoagulation therapy (aspirin, tirofiban, clopidogrel and rivaroxaban)
There is an increasing need for tighter regulation of synthetic cannabinoids
References
1. Caviness CM, Tzilos G, Anderson BJ, Stein MD. Synthetic cannabinoids: use and predictors in a community sample of young adults. Subst Abus 2014;published online. http://dx.doi.org/10.1080/08897077.2014.959151
2. Curtis B, Alanis-Hirsch K, Kaynak O, Cacciola J, Meyers K, McLellan AT. Using web searches to track interest in synthetic cannabinoids (aka ‘herbal incense’). Drug Alcohol Rev 2014;published online. http://dx.doi.org/10.1111/dar.12189
4. Seely KA, Lapoint J, Moran JH, Fattore L. Spice drugs are more than harmless herbal blends: a review of the pharmacology and toxicology of synthetic cannabinoids. Prog Neuropsychopharmacol Biol Psychiatry 2012;39:234–43. http://dx.doi.org/10.1016/j.pnpbp.2012.04.017
5. Winstock AR, Barratt MJ. The 12-month prevalence and nature of adverse experiences resulting in emergency medical presentations associated with the use of synthetic cannabinoid products. Hum Psychopharmacol 2013;28:390–3. http://dx.doi.org/10.1002/hup.2292
7. de Havenon A, Chin B, Thomas KC, Afra P. The secret “spice”: an undetectable toxic cause of seizure. Neurohospitalist 2011;1(4):182–6. http://dx.doi.org/ 10.1177/1941874411417977
9. McKeever RG, Vearrier D, Jacobs D, LaSala G, Okaneku J, Greenberg MI. K2-not the spice of life; synthetic cannabinoids and ST elevation myocardial infarction: a case report. J Med Toxicol 2014;published online. http://dx.doi.org/10.1007/s13181-014-0424-1
10. Mir A, Obafemi A, Young A, Kane C. Myocardial infarction associated with use of the synthetic cannabinoid K2. Pediatrics 2011;128:e1622–e1627. http://dx.doi.org/10.1542/peds.2010-3823
13. Lakin KM, Makarov VA, Kovalev SG et al. [The effect of fluorinated prostaglandins on platelet aggregation]. Eksp Klin Farmakol 1994;57:39–41.
14. Mazzarino M, de la Torre X, Botre F. A liquid chromatography-mass spectrometry method based on class characteristic fragmentation pathways to detect the class of indole-derivative synthetic cannabinoids in biological samples. Anal Chim Acta 2014;837:70–82. http://dx.doi.org/10.1016/j.aca.2014.06.003
15. Rodrigues WC, Catbagan P, Rana S, Wang G, Moore C. Detection of synthetic cannabinoids in oral fluid using ELISA and LC-MS-MS. J Anal Toxicol 2013;37:526–33. http://dx.doi.org/10.1093/jat/bkt067
16. Spinelli E, Barnes AJ, Young S et al. Performance characteristics of an ELISA screening assay for urinary synthetic cannabinoids. Drug Test Anal 2014;published online. http://dx.doi.org/10.1002/dta.1702
17. Brents LK, Prather PL. The K2/spice phenomenon: emergence, identification, legislation and metabolic characterization of synthetic cannabinoids in herbal incense products. Drug Metab Rev 2014;46:72–85. http://dx.doi.org/10.3109/03602532.2013.839700
18. Dando I, Donadelli M, Costanzo C et al. Cannabinoids inhibit energetic metabolism and induce AMPK-dependent autophagy in pancreatic cancer cells. Cell Death Dis 2013;4:e664. http://dx.doi.org/10.1038/cddis.2013.151
19. Ramer R, Fischer S, Haustein M, Manda K, Hinz B. Cannabinoids inhibit angiogenic capacities of endothelial cells via release of tissue inhibitor of matrix metalloproteinases-1 from lung cancer cells. Biochem Pharmacol 2014;91:202–16. http://dx.doi.org/10.1016/j.bcp.2014.06.017
It is widely accepted that end-of-life care for non-cancer conditions has lagged behind that for cancer. The purpose of this survey was to evaluate the confidence of trainees in managing end-of-life issues. An online questionnaire was distributed to all registrar-grade British Junior Cardiac Association members in the UK.
A total of 219 trainees responded. Overall, 73% of trainees feel the care they provide patients with advanced heart failure is poor/adequate. Over 50% of trainees do not feel equipped to discuss advanced-care planning and end-of-life issues. There are 45% who report receiving no training in palliation of advanced heart failure symptoms, while 57% are unhappy with current provision of training. Trainees’ suggestions include more workplace-based supervision with additional regional and national training days, closer links with local hospices, and fellowships for cardiology trainees in palliative care.
Despite being part of the national curriculum for training in cardiology since 2010, trainees’ level of confidence in delivering end-of-life care in advanced heart failure and discussing prognosis is poor. This could be rectified by closer links with palliative care and formal teaching programmes.
Introduction
Heart failure is a complex clinical syndrome and is the only cardiovascular disease that is increasing in prevalence.1 It has a profound impact on both the patient’s quality of life and functional capacity, as well as causing premature death.2 Traditionally, cancer patients have been the main focus for specialist palliative care services, though it is increasingly well-recognised that chronic heart failure is equivalent to malignant disease,3 with patients experiencing debilitating physical symptoms, as well as psychosocial and spiritual problems. Despite the growing recognition of the palliative care needs of this complex group of patients and their carers, a recent National Heart Failure Audit disappointingly continued to report significant unmet needs, with only 3.1% of those dying with heart failure being referred to palliative care services on their first admission to hospital and 6% on readmission,4 far less than that of oncology patients. The caveat to this is the recognition that coding for referral to palliative care services may not always be accurate, though the number is still likely to be low.
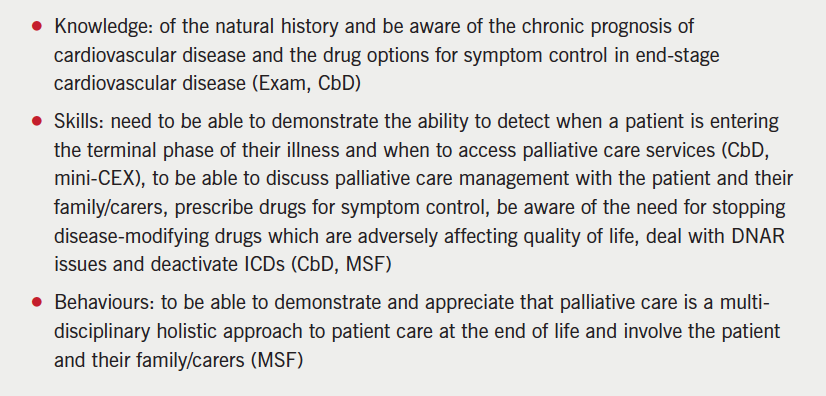
In acknowledgement of this, the European Society of Cardiology (ESC) published a position statement addressing palliative care in heart failure and proposed that “palliative care should be integrated as part of a team approach to comprehensive heart failure care and should not be reserved for those who are expected to die within days or weeks.”5 The crucial role that palliative care can offer in managing patients with heart failure has also been recognised by the Joint Royal College of Physicians Training Board who incorporated end-of-life care into the 2010 cardiology curriculum for trainees, with the aim of ensuring that future cardiologists have the necessary knowledge, skills and behaviour to manage the latter stages of this condition competently (box 1).6 There are no published data of the current levels of competence of cardiology trainees in this area.
Box 1. End-of-Life Care in Cardiology Competencies in the 2010 Cardiology Curriculum: (suggested modes of assessment in parentheses)
We undertook a survey to evaluate the confidence of trainees in this area.
Methods
An electronic survey was distributed to registrar-grade members of the British Junior Cardiac Association (BJCA) in the UK in June 2012. Three reminder emails were sent over the following four weeks, after which the survey was closed and analysed. There were 22 questions designed to ascertain what level of palliative care training the respondent had received, how confident they felt in the palliative management of end-stage heart failure patients, how they felt this could be improved upon and how important they felt this area of care was in their training (the full survey questions are available in appendix 1). The survey also explored the attitudes of trainees to end-of-life care in heart failure and the role of palliative medicine. In some questions, trainees were given the opportunity for free-text responses. These responses (27 in total), were subsequently analysed qualitatively by two of the researchers, who independently read and re-read the comments and identified significant statements. These were then grouped into themes, consistent with a thematic analysis method.
Results
Who responded?
Overall, 221 cardiologists in training completed the survey out of 800 who were eligible; a response rate of 28% which is broadly in line with response rates obtained by the BJCA in other studies.7 The responses were received across the range of different level training grades (ST3-7, SpR, LAS/LAT grades) and across different deaneries, with only one deanery not being represented. Responses were received from all cardiology sub-specialities, including interventional cardiology, electrophysiology, cardiac imaging, adult congenital heart disease, heart failure and device implantation, as well as academic trainees.
Clinical training
Trainees were asked about their experience of palliating patients with end-stage heart failure: 73% of trainees’ reported difficulties in palliating patients with end-stage heart failure, but palliative care physicians were consulted in only 56% of cases, with palliative care nurse advice sought in only 46% of cases. Only 26% of respondents felt that the care they provided their end-stage heart failure patients was good/very good. Over half of the trainees (51%) surveyed felt ill-equipped to discuss advanced-care planning and end-of-life issues when seeing advanced heart failure patients in an outpatient setting.
Looking at the trainees’ prescribing habits of opioids, anti-emetics, laxatives and antidepressants in end-stage heart failure, only 30% prescribed opioids, 29% anti-emetics, 24% laxatives and 4% antidepressants, regularly.
Of those trainees involved in the insertion of implantable cardiac defibrillators (ICDs), only 9.4% always explained the possibility of future deactivation of the device, with a significant proportion of trainees never raising this issue before implantation.
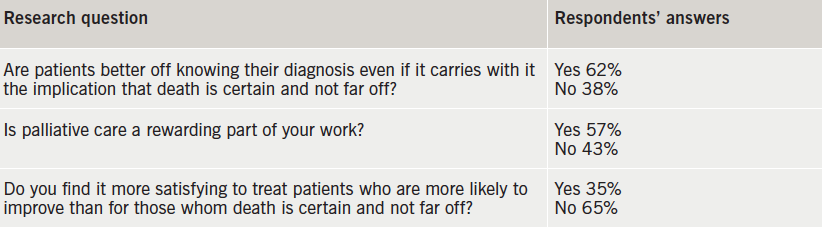
Trainees’ attitudes to palliative care in end-stage heart failure are shown in table 1.
Table 1. Trainees’ attitudes to palliative care in end-stage heart failure
Trainees’ education
There were 42% of trainees who had not received specific education regarding the palliation of symptoms of advanced heart failure. The education that the remainder had received mostly seemed to comprise of isolated lectures as part of general medicine training/SpR teaching or specific courses/study days on the topic. There were only a few examples where practical experience was gained from working directly with the palliative care team. However, 92% of trainees felt that training in end-of-life care in cardiology was important. Key areas for teaching that were identified by trainees to be important were symptom control, opioid titration and communication skills, as well as the role of the palliative care team. Only 22% of trainees had completed a workplace-based assessment, the remainder had not. Overall, 53% of trainees were unhappy with the level of training and supervision they were receiving regarding end-of-life care during their cardiology training.
Free text responses (27 total)
Three major themes were elucidated:
1. Palliative care in heart failure is an important topic but not well covered in the curriculum (responses 5, 9, 11, 13, 15, 19, 21, 24, 25, 26).
“Important and underemphasised aspect of cardiology. We like to think of ourselves as life savers, is that possibly why we don’t address the end-stage heart failure issues so well.” (response 9)
“No culture of palliative care in Cardiology so this will NOT be picked up by trainees whilst on the job.” (response 12)
2. The palliation of patients is often not optimal (responses 3, 13, 27).
Communication can be poor (responses 6, 27)
Teams can find it difficult to accept that patients are dying (responses 3, 9, 17, 20, 27)
“I think palliation of end-stage heart failure patients is generally poorly done and not thought of soon enough. I would value more training in this area as a heart failure fellow.” (response 3)
“Heart failure is often badly palliated and patients are looked after by different teams, e.g. care of elderly and cardiology. In cardiology, I have encountered a systemic reluctance to accept that patients are dying and instead subjecting them to CCU based inotropes, etc.” (response 27)
3. Improved communication links are needed between the two specialities (responses 6, 7, 16, 17, 21, 22).
“Nowhere near enough interaction between palliative care and cardiology. Not a lack of goodwill or interest, but mainly of funding and time. Too much palliative care funding focused on cancer. Too much cardiology funding focused on preventing hospital admission.” (response 7)
“We need to make palliative care physicians more interested and accessible to cardiac patients.” (response 16)
“I think cardiology trainees should be better trained in recognition of the need for palliative care input but I also think that palliative care trainees should be trained significantly in non-cancer related palliation.” (response 22)
Discussion
Due to the lack of confidence of trainees, this survey demonstrates that the majority of cardiology trainees continue to experience difficulties in providing good quality palliative care for patients with advanced heart failure with only approximately half of patients being referred to palliative care services. The barriers to obtaining palliative care input for advanced heart failure patients were not investigated in this survey but free-text responses suggest these are multi-factorial, and may include a cultural reluctance of cardiologists to accept that patients have reached a stage in their heart failure journey that may benefit from palliative care input, as well as difficulties in accessing palliative care services due to lack of the necessary infrastructure/funding. As a result, only a minority of respondents felt that the care they provided their end-stage heart failure patients was good. Over half of the trainees surveyed felt ill-equipped to discuss advanced-care planning and end-of-life issues when seeing advanced heart failure patients in an outpatient setting, with time pressures and a lack of the appropriate nursing support cited as possible obstacles to this.
Confidence in prescribing the medications commonly used in palliating advanced heart failure symptoms is low. Depression is common in heart failure and is associated with a worse clinical status and poor prognosis in heart failure.2 It is, therefore, of concern that only 4% of trainees prescribe these medications regularly, and 48% report that they never prescribe them. Opioids, anti-emetics and laxatives play a central role in symptom control in advanced heart failure, yet prescriptions of these medications were low. Both opioid titration and symptom control were identified in the survey as areas that trainees would prioritise for future teaching.
Advanced care planning takes into account the patient’s preference for place of death and their resuscitation decisions, including possible deactivation of an ICD. This is a key part of end-of-life care and, yet, this survey has shown that only 9.4% of trainees involved in the insertion of ICDs always explained the possibility of future deactivation of the device, with a significant proportion of trainees never raising this issue before implantation.8 It is increasingly believed that communication about ICD deactivation should be an ongoing process that begins prior to implantation and continues over time as the patient’s health status changes.9 Studies have indicated that, although physicians believe they should engage in these types of conversations with patients, they rarely do.10 Encouraging attendance at advanced communication courses may be a way of increasing trainees’ confidence in managing more difficult conversations with patients.
Despite the inclusion of end-of-life care in the cardiology curriculum, many trainees have not received the level of training that is necessary to achieve the specified competencies, and are not happy with the level of training and supervision given in this area. Workplace-based assessments are undertaken by only a minority of trainees. Trainees, who may lack the competencies to manage end-of-life care appropriately, deny their patients and their family/carers the holistic, multi-disciplinary care that they should receive, and this should be of grave concern to all cardiologists. So what can be done to overcome these issues?
More emphasis should be placed on end-of-life care in daily clinical practice, and all trainees should engage actively in this area. The presence of heart failure teams, as recommended by the National Heart Failure Audit, who provide specialist expertise in managing this group of patients would contribute to improving trainees’ levels of experience and skill. Improving links with local palliative care teams would also be of benefit for both specialities; cardiology trainees would be given an opportunity to expand their experience of palliative care, while palliative care trainees may learn about the management of end-stage cardiac diseases. Fellowships/placements in palliative medicine could play a valuable part in equipping cardiology trainees with the practical skills needed. Involvement of palliative care teams at specialist heart failure multi-disciplinary team (MDT) meetings would also be a mechanism of enhancing trainees’ knowledge. Locally based, small, group sessions could be utilised to develop communication skills and how to deal sensitively and effectively with patients and their family/carers. On a more formal level, regional and national training days could provide an exceptional forum for national experts to teach on end-of-life care. Collaboration with organisations such as the British Heart Foundation and MacMillan could also facilitate focused teaching of both cardiology and palliative care trainees.
It is encouraging, however, that trainees appear to recognise the importance of end-of-life care in their training and are keen for more opportunities to expand their knowledge of palliative care in cardiology.
Strengths and limitations of this study
This is a novel study, exploring the knowledge, attitudes and skills of cardiologists in training in end-of-life care in the UK. Responses were obtained from trainees in all sub-specialities, across all training grades and from all but one deanery, making the findings relevant nationally. The survey employed various methods to seek information including fixed-choice responses and rating scales, as well as providing a free-text section.
As with all studies relying on voluntary participation, the findings of our survey may be biased by the level of response. While the response rate for this survey was very much in keeping for this type of study, we acknowledge that only a relative minority of trainees did respond and, therefore, the results may not be accurate. In addition, the quantitative aspect of some of the questions used in the survey cannot accurately reflect the complex emotions/behaviours associated with this subject area. The levels of subjectivity of respondents cannot be assessed by this type of survey, i.e. what is ‘good’ care for one person, may be ‘bad’ care to another. However, the free-text responses did allow trainees an opportunity to expand their views in more depth.
Conclusion
This survey has demonstrated both a need for improved teaching and support for cardiologists in training in palliative care for heart failure patients. This could be provided by more local/national training days with a focus on end-of-life care, as well as local initiatives between cardiology and palliative care services to enhance both cardiology and palliative care trainees’ experience through communication skills workshops, fellowships or placements. In addition, collaboration with MacMillan and the British Heart Foundation to enhance trainees’ skills should be explored.
Acknowledgements
Thanks to Dr Ian Wilson, Dr Matthew Bates, and Dr Aaisha Opel for their help in distributing the survey to BJCA members and Professor Julia Addington-Hall for her help in preparing the survey questions.
Source of funding
Servier Laboratories funding for online survey support, data collection and analysis tool.
Conflict of interest
None declared.
Editors’ note
See also the editorial by Johnson et al. in this issue.
Key messages
The prognosis of chronic heart failure is equivalent to that of cancer yet only a small proportion of patients are referred to palliative care. To address this, the UK Cardiology curriculum includes end-of-life care within it
This study demonstrates a need for improved teaching and support for UK Cardiology trainees in end-of-life care in heart failure
Enhanced training for cardiologists using communication skills workshops, training days, fellowships or placements could improve the care delivered to this patient group
Appendix 1. Survey questions
References
1. Connolly M, Beattie J, Walker D et al. End of life care in heart failure: a framework for implementation. Leicester: Heart Improvement Programme, NHS Improvement, 2010. Available from: http://www.wales.nhs.uk/sitesplus/986/opendoc/177612
2. McMurray JJV, Adamopoulos S, Anker SD et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012; The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Eur Heart J 2012;33:1787–847. http://dx.doi.org/10.1093/eurheartj/ehs104
3. Stewart S, MacIntyre K, Hole DJ, Capewell S, McMurray JJV. More ‘malignant’ than cancer? Five-year survival following a first admission for heart failure. Eur J Heart Fail 2000;3:315–22. http://dx.doi.org/10.1016/S1388-9842(00)00141-0
5. Jaarsma T, Beattie JM, Ryder M et al. Palliative care in heart failure: a position statement from the palliative care workshop of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Failure 2009;11:433–43. http://dx.doi.org/10.1093/eurjhf/hfp041
7. McNulty DD. The adequacy of response rates to online and paper surveys: what can be done? Assessment and Evaluation in Higher Education 2008;33:301–14. http://dx.doi.org/10.1080/02602930701293231
9. Lampert R, Hayes DL, Annas GJ et al. HRS expert consensus statement on the management of cardiovascular implantable electronic devices in patients nearing end of life or requesting withdrawal of therapy. Heart Rhythm 2010;7:1008–26. http://dx.doi.org/10.1016/j.hrthm.2010.04.033
We know that people with advanced heart failure have unmet supportive and palliative care needs, and the burden of these concerns is comparable with people with cancer.1–2 Palliative care services in the UK and elsewhere have grown up around oncology services. Randomised controlled trials (RCTs) have confirmed that early integration of palliative care, alongside cancer treatment, improves patient outcomes.3–7 In contrast, experience of and the evidence base for integration of palliative care alongside heart failure treatment has been slow to develop. However, this is changing. A pilot RCT comparing the addition of a palliative care intervention to usual care for people with advanced heart failure has reported benefit in health-related quality of life, symptom control and health service utilisation (reduced hospital admission)8 and several phase three RCTs are ongoing.
Professor Miriam J Johnson
Overcoming barriers
The misunderstanding that palliative care is only for those in the last few days or weeks of life, only to be implemented once all other options are gone and irreversible deterioration is certain, forms a major barrier to access to palliative care. Attempts to identify a prognostic tool to identify when palliative care should be employed have failed, and the consensus is that a problem-based approach is more fit for purpose.11–12 Such a model would enable the “concerns of today” facing the patient to be addressed in the context of the management options appropriate at their stage of disease; a discussion which may lead on to include appropriate options for the future and involve other professionals such as palliative care services if needed. Therefore it is imperative that the cardiology team is able to assess and manage symptom and quality of life issues, and have the expert communication skills required for complex and difficult conversations regarding device and other therapies, ceilings of medical care and cardiopulmonary resuscitation, as heart failure advances. With these competences, the majority of patients’ supportive and palliative care needs will be addressed by their cardiac or primary care team, and specialist palliative care services only needed for complex or persistent problems.
In this light, the article by Ismail and colleagues13 in this issue, is concerning. Despite changes to the UK cardiology specialist curriculum and a recognition that the care of people with advanced disease is important, these trainees report a lack of expertise. A systematic reluctance to recognise the dying, poor communication, and inadequate engagement with and from palliative care teams is described by some. Various solutions are suggested by the authors including joint teaching for cardiology and palliative care trainees and the introduction of a fellowship scheme. However, cardiology trainees also need their seniors to be good role models; training tools such as case-based discussion and mini-clinical examinations will be less effective if the clinical/educational supervisors are not confident and competent in basic palliative care skills themselves, or do not see the importance of this area. Lessons could be learned from the field of oncology where providing advanced communication skills for consultants as well as trainees was considered a crucial part of improving services.14
There is an urgent need to overcome the deadlock preventing access to palliative care. Clinicians caring for people with advanced heart failure need to be equipped with the skills they require to assess and address the palliative care concerns of this group of patients.
Conflict of interest
None declared.
Editors’ note
See also the article by Ismail et al. in this issue.
References
1. Murray SA, Boyd K, Kendall M, Worth A, Benton TF, Clausen H. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. Br Med J 2002;325:929. http://dx.doi.org/10.1136/bmj.325.7370.929
2. Pantilat SZ, O’Riordan DL, Dibble SL, Landefeld CS. Longitudinal assessment of symptom severity among hospitalized elders diagnosed with cancer, heart failure, and chronic obstructive pulmonary disease. J Hosp Med 2012;7:567−72. http://dx.doi.org/10.1002/jhm.1925
3. Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE II randomized controlled trial. J Am Med Assoc 2009;302:741−9. http://dx.doi.org/10.1001/jama.2009.1198
4. Zimmermann C, Swami N, Krzyzanowska M, et al. Early palliative care for patients with advanced cancer: a cluster-randomised controlled trial. Lancet 2014;383:1721−30. http://dx.doi.org/10.1016/S0140-6736(13)62416-2
5. Farquhar MC, Prevost A, McCrone P, et al. Is a specialist breathlessness service more effective and cost-effective for patients with advanced cancer and their carers than standard care? Findings of a mixed-method randomised controlled trial. BMC Med 2014;12:194. http://dx.doi.org/10.1186/s12916-014-0194-2
6. Higginson IJ, Bausewein C, Reilly C, et al. An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness: a randomised controlled trial. Lancet Respir Med 2014;2:979–87. http://dx.doi.org/10.1016/S2213-2600(14)70226-7
7. Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 2010;363:733−42. http://dx.doi.org/10.1056/NEJMoa1000678
8. Brannstrom M, Boman K. Effects of person-centred and integrated chronic heart failure and palliative home care. PREFER: a randomized controlled study. Eur J Heart Fail 2014;16:1142–51. http://dx.doi.org/10.1002/ejhf.151
9. Gadoud A, Kane E, Macleod U, Ansell P, Oliver S, Johnson M. Palliative Care among heart failure patients in primary care: a comparison to cancer patients using English family practice data. PLoS One 2014;9:e113188. http://dx.doi.org/10.1371/journal.pone.0113188
10. Unroe KT, Greiner MA, Hernandez AF, et al. Resource use in the last 6 months of life among medicare beneficiaries with heart failure, 2000−2007. Arch Intern Med 2011;171:196−203. http://dx.doi.org/10.1001/archinternmed.2010.371
11. Haga K, Murray S, Reid J, et al. Identifying community based chronic heart failure patients in the last year of life: a comparison of the Gold Standards Framework Prognostic Indicator Guide and the Seattle Heart Failure Model. Heart 2012;98:579−83. http://dx.doi.org/10.1136/heartjnl-2011-301021
12. Hogg KJ, Jenkins SM. Prognostication or identification of palliative needs in advanced heart failure: where should the focus lie? Heart 2012;98:523−4. http://dx.doi.org/10.1136/heartjnl-2012-301753
13. Ismail Y, Shorthose K, Nightingale AK. Trainee experiences of delivering end-of-life care in heart failure: key findings of a national survey. Br J Cardiol 2015;22. http://dx.doi.org/10.5837/bjc.2015.008
14. Fallowfield L, Lipkin M, Hall A. Teaching senior oncologists communication skills: results from phase I of a comprehensive longitudinal program in the United Kingdom. J Clin Oncol 1998;16:1961−8.
Authors: Pierre Le Page, Hamish MacLachlan, Lisa Anderson, Lee-Ann Penn, Angela Moss, Andrew R J Mitchell; from the Jersey International Centre for Advanced Studies
Pierre Le Page
Clinical Fellow in Cardiology
Hamish MacLachlan
Clinical Fellow in Cardiology
Lisa Anderson
Cardiac Specialist Nurse
Lee-Ann Penn
Cardiac Specialist Nurse
Angela Moss
Cardiac Specialist Nurse
Andrew R J Mitchell
Consultant Cardiologist and Senior Research Fellow
Jersey International Centre for Advanced Studies, The General Hospital, Gloucester Street, St. Helier, Jersey, JE1 3QS
Cardiac screening in the community is limited by time, resources and cost. We evaluated the efficacy of a novel smartphone application to provide a rapid electrocardiogram (ECG) screening method on the Island of Jersey, population 98,000.
Members of the general public were invited to attend a free heart screening event, held over three days, in the foyer of Jersey General Hospital. Participants filled out dedicated questionnaires, had their blood pressure checked and an ECG recorded using the AliveCor (CA, USA) device attached to an Apple (CA, USA) iPhone 4 or 5.
There were 989 participants aged 12–99 years evaluated: 954 were screened with the ECG application. There were 54 (5.6%) people noted to have a potential abnormality, including suspected conduction defects, increased voltages or a rhythm abnormality requiring further evaluation with a 12-lead ECG. Of these, 23 (43%) were abnormal with two confirming atrial fibrillation and two showing atrial flutter. Other abnormalities detected included atrial and ventricular ectopy, bundle branch block and ST-segment abnormalities. In addition, increased voltages meeting criteria for left ventricular hypertrophy (LVH) on 12-lead ECG were detected in four patients leading to one diagnosis of hypertrophic cardiomyopathy.
In conclusion, this novel ECG application was quick and easy to use and led to the new diagnoses of arrhythmia, bundle branch block, LVH and cardiomyopathy in 23 (2.4%) of the total patients screened. Due to its highly portable nature and ease of use, this application could be used as a rapid screening tool for cardiovascular abnormalities in the community.
Wolfgang Mastnak Professor, Charité – University Medicine Berlin, Institut für Medizinische Soziologie und Rehabilitationswissenschaft, Abt. Rehabilitationsforschung, Ltg: Dr Karla Spyra, Luisenstraße 13a, 10117 Berlin, Germany, and President of the Austrian Heart Association
Sustainability of health benefits from cardiac rehabilitation (CR) requires adequate changes in lifestyles. Preventive medicine highlights a triadic guideline referring to cardioprotective behaviour, avoidance of associated polymorbid developments (e.g. depression), and improvement of life-quality. To assess the influence of long-term CR management (in Austria phase 4) offered by the Austrian Heart Association (ÖHV) on changes in lifestyles according to the INTERHEART CHD-risk parameters, a questionnaire measuring the extent of phase 4 influences on lifestyle modifications according to the INTERHEART parameters physical activity, stress, nutrition, body mass index (BMI), smoking, and alcohol was developed. Data were gained from a non-preselected sample of cardiac patients with various diagnoses (n=204; age 41–91, average 71.8; standard variation 7.8, 48% cardiovascular).
ÖHV activities were found to exert a strong influence on health sports (various indoor and outdoor aerobic activities and mobility exercises), stress-reduction, and nutritional adjustment, contrasting low influence on the awareness of diabetes risks and alcohol/nicotine consumption. Social inclusion is considered an important life-quality factor supporting also the sense of security.
Long-term CR management is an efficient instrument for cardioprotective lifestyle modification. The important influence on patients requires especially high sports cardiologic standards and psycho-educational competence. Close collaboration between different phases/stages of CR, as well as similar international organisation should be fostered.
Introduction
Professor Wolfgang Mastnak
In 2009, Willmer and Waite1 published a study on the effectiveness of phase 4 cardiac rehabilitation (CR), suggesting that there are observable benefits in participating in long-term phase 4 CR. Those who decline phase 4 CR clearly do less well. In Austria, the Austrian Heart Association (Österreichischer Herzverband/ÖHV) is in charge of long-term CR management providing a nationwide network of heart support groups.
Long-term management in CR: International heterogeneity
Cardiac prevention, acute cardiology, and CR are interacting disciplines. Historically speaking, it took decades to establish cardiac prevention awareness in the general population and to provide comprehensive CR services. After a ‘step change’ in one’s cardiac condition, such as myocardial infarction (MI), acute coronary heart disease (CHD) or first diagnosed heart failure and subsequent acute care, formerly patients were usually told to change their lifestyles and to protect their hearts, though clinicians could not give precise advice, e.g. concerning sports cardiologic guidelines, nor did patients find long-term support by specialised rehabilitation organisations. In Austria, this problem led to the foundation of the Austrian Heart Association approximately four decades ago.
Though in those early times there was doubt about the effectiveness of community-based long-term rehabilitation,2 today, long-term secondary prevention and heart support groups have become an international standard.3 Due to different health systems and medical credos in the world there is no standardised terminology in cardiac rehabilitation,4 a problem causing misunderstandings and restricting transferability.
The Austrian phase 4 is equivalent to stage 6 of the new UK stage model. American guidelines define three phases:5
Inpatient CR (also known as phase 1 CR)
Early outpatient CR (phase 2)
Long-term outpatient CR (also known as phase 3 or phase 4 CR): a programme that provides longer-term delivery of preventive and rehabilitative services for patients in outpatient settings.
Other countries are reforming systems, e.g. China, which looks back to an outstandingly good healthcare practice, is today about to integrate traditional and Western approaches. Nevertheless, we also find very Western ways of CR, e.g. in Hong Kong.6 This programme consists of four phases:
Inpatient ambulation programme for 7–14 days
A twice-weekly outpatient education and exercise programme lasting for eight weeks
A community-based home exercise programme
Long-term maintenance for another 12 months.
Germany and Switzerland share similar systems, phase 1 referring to early mobilisation at hospital, phase 2 subsequent treatment in a CR clinic or in smaller specialised outpatient centres, phase 3 long-term rehabilitation in heart support groups.
In Austria, CR consists of four phases:
Phase 1: acute hospital, early mobilisation and preparing further steps of rehabilitation
Phase 2: CR clinic, usually three to four weeks
Phase 3: outpatient CR, one year, carried out by the Agakar (Arbeitsgemeinschaft für ambulante kardiologische Rehabilitation)
Phase 4: long-term CR, carried out by the Austrian Heart Association.7
In 1992, the World Health Organization (WHO) held consultations in Udine (Italy) and Tours (France) on the issue of needs and action priorities in CR and secondary prevention in patients with CHD, stipulating a comprehensive CR programme should include endurance training, educational counselling, risk factor behaviour modification, vocational guidance, relaxation and training in stress management. Patients can be stratified for their level of coronary risk so that CR can be individualised.8
These guidelines are, in general, still valid for the Austrian Heart Association programme, of course permanently readjusted according to cardiological standards.
Cardiac risk factor control and the problem of long-term risk stratification
Controlling cardiac risk factors, reducing recurrent pathological events and improving life quality are evident aims of long-term CR management. Nevertheless, these important constituents of comprehensive CR usually encounter four main problems:
As there is no regular obligation to join heart support groups, adherence and sustainable rehabilitation benefits depend on individual motivation.
The huge behavioural impact on cardiovascular processes is no longer doubted. Still there is the question, whether or not long-term CR activities cause cardioprotective changes in lifestyles.
Sufficiently extensive networks for local long-term CR availability depend on national healthcare policies.
These programmes are partly not as rigorously assessed, as for example heart surgery. Nevertheless, optimised outcomes require highest medical standards.
Such issues still pose questions about effects and outcomes of long-term CR programmes,9 which refer also to the interventions’ adequacy, such as intensities of physical activity.10
The INTERHEART study,11 which is taken as reference for this study, identified CHD risks by retrospective analyses. Direct longitudinal studies on cardiac risk stratification and long-term CR, however, are rare. Hard data refer, for example, to the comparison between fatal and non-fatal re-infarction within 30 days,12,13 three or six months,14-16 one year,17,18 or phase 1 and 2.19
Risk adjustment models on the basis of long-term studies20 are rare, and for the discussion of long-term CR effectiveness, as important as such famous studies like Framingham.21,22 Combining results from both study types, however, allows us to hypothesise behavioural long-term coronary risks and secondary preventive mechanisms. The lack of longitudinal research on CR is evident, the few cardiologic long-term studies tend to overlook behavioural and environmental factors.23
CHD risk factor profile
Various studies elucidated the aggressiveness of CHD-related behavioural risk factors, highlighting the effectiveness of lifestyle changes in heart patients.24 As well as that,25 in addition to exercise training, a comprehensive secondary prevention programme for cardiac patients requires aggressive reduction of risk factors through nutritional counselling, weight management, and adherence to prescribed drug therapy. Clinical trials during the past two decades have provided conclusive evidence of reduced mortality in patients with CHD via reduction of individual risk factors by pharmacological and nonpharmacological interventions. The proven salutary impact of comprehensive lifestyle modification often has been overlooked and underemphasised as a first-line approach to secondary prevention.
Referring to behavioural and environmental risk factors of cardiovascular diseases the INTERHEART study,11 identifying smoking, lipids, hypertension, diabetes, obesity, diet, physical activity, alcohol consumption, and psychological factors as outstanding foci in preventive and rehabilitative medicine, became a cornerstone for the cardiology of the new millenium.26 Most strikingly, it showed that the PAR (population attributable risk, indicating the proportion of cases that would not occur in a population if the risk factors were eliminated) of 90.4% for all nine risk factors suggests that, statistically, the nine risk factors combined accounted for basically all of the risk of acute MI in this study population – a truly startling and unanticipated result. Consequently, behaviour and psyche lost their marginal position and gained central interest.
Materials and methods
This cross-sectional questionnaire study investigates how cardiac patients perceive the effect of long-term CR programme attendance on health behaviour changes. In order to evaluate the measurable cardioprotective benefits of long-term CR, further investigations are needed.
Changes in lifestyle as feature and aim of long-term CR
The crucial question of this study is, whether or not the programme offered by the Austrian Heart Association is decisive for lifestyle changes in the perception of the participants? This issue refers also to complementary profiles of acute cardiological interventions and features of long-term CR (table 1).
Table 1. Profiles of acute cardiological interventions and features of long-term cardiac rehabilitation (CR)
INTERHEART parameters, questionnaire, and data generation
Those INTERHEART factors that depend directly on an individual’s behaviour were taken as reference for the decisive parameters of our study. The corresponding questionnaire was designed for this study as follows:
Seven items referring to physical activity, smoking, body mass index (BMI)/obesity, stress, eating habits, sugar/awareness of diabetes risks. As not directly manageable through behavioural changes, lipids and arterial hypertension were not included.
Previous informal piloting among people attending phase 4 was used to estimate the validity and comprehensibility of the items. Equidistant scales (0, 1, … 10) are assumed to yield interval scale data. Still further research is needed to provide fully validated tools to investigate behavioural changes in cardiac patients.
Considering the advanced age of participants the questionnaire was easy to understand and to handle. Patients should not get stressed or require individual help for answering.
Questions were formulated as follows:
Did the ÖHV decisively contribute to changes in my lifestyle for better health?
Because of my participation in ÖHV activities I have … (following the single behavioural parameters).
Rank between 0 and 10, “0” meaning “not at all”, “10” meaning “absolutely”.
Table 2. Profile of participants (n=204)
If participants thought an item not applicable, they could leave it blank.
During a two-month period in spring 2014, members participating in various activities of the Austrian Heart Association in the Austrian federate states of Carinthia, Lower Austria, Salzburg, Tyrol and Vienna, were asked to complete the questionnaire. The profile of the participants is shown in table 2.
Results
The results are shown in table 3. On the background of the features of the ÖHV phase 4 programme interpretation of these numerical results suggests:
People attending phase 4 programmes perceive that the programmes have high influence on health sports motivation and sustainability.
The programmes support stress reduction/competence of stress management and changes in eating habits.
Participants in this study did not perceive that attendance at phase 4 contributed considerably to changes in smoking behaviour, alcohol and sugar consumption or weight reduction.
A few unsolicited comments by some participants highlight the importance of experienced social inclusion, regained self-confidence and life-activity, empathetic talks and psychological support.
Table 3. Impact of long-term cardiac rehabilitation activities on cardioprotective behavioural changes
Discussion
Optimised long-term CR and secondary prevention has to be based on an individually shaped balance between lifestyle, pharmacological treatment, socio-cultural welfare, and the experience of well-being. This requires close collaboration between medical cardiology, long-term CR, and adequate social conditions.
The high influence of long-term CR programmes on patients requires compatibility with the most recent cardiologic guidelines (e.g. sports cardiology, psycho-cardiology) and holistic rehabilitative medicine. The specific quality (e.g. empathic understanding) of heart support groups is of high potential for psychological rebalancing. Research on best practice of collaboration between the CR phases has to be internationally intensified. Long-term CR programmes are not only cost-efficient, but also of high individual and medical economic benefit27.
Acknowledgements
I would like to thank my colleagues RM Dejaco, F Fink, H Kiener, F Radl, D Schiffrer, H Schulter and R Weißsteiner for the standardised and objective generation of empirical data.
Support
No financial support, no funding.
Conflict of interest
None declared.
Key messages
Long-term cardiac rehabilitation management is important for cardioprotective lifestyle modification
Physical fitness, stress management, psychological stability and life quality are improved
2. Campbell NC, Grimshaw JM, Ritchie LD et al. Outpatient cardiac rehabilitation: are the potential benefits being realised? J R Coll Physicians Lond 1996;30:514–19.
4. Wenger N (ed). Cardiac Rehabilitation: Guide to Procedures for the Twenty-first Century. New York: Taylor & Francis, 2005.
5. Thomas RJ, King M, Lui K et al. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services. Circulation 2007;116:1611–42. http://dx.doi.org/10.1016/j.jacc.2010.06.006
6. Thompson DR, Yu CM. Cardiac rehabilitation: China. In: Perk J, Gohlke H, Hellemans I et al. (eds). Cardiovascular Prevention and Rehabilitation. London: Springer, 2007;pp 48–51.
8. WHO Regional Office for Europe. Needs and action priorities in cardiac rehabilitation and secondary prevention in patients with CHD. Document EUR/ICP/CVC 125 4328g. Geneva: WHO Regional Office for Europe, 1993.
9. Jackson AM, Gregory S, McKinstry B. Self-help groups for patients with coronary heart disease as a resource for rehabilitation and secondary prevention – what is the evidence? Heart Lung 2009;38:192–200. http://dx.doi.org/10.1016/j.hrtlng.2009.01.009
11. Yusuf S, Hawken S, Ounpuu S et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 2004;364:937–52. http://dx.doi.org/10.1016/S0140-6736(04)17018-9
12. Boersma E, Pieper KS, Steyerberg EW et al. Predictors of outcomes in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. The PURSUIT investigators. Circulation 2000;101:2557–67. http://dx.doi.org/10.1161/01.CIR.101.22.2557
13. Kernis SJ, Harjai KJ, Stone GW et al. The incidence, predictors, and outcomes of early reinfarction after primary angioplasty for acute myocardial infarction. J Am Coll Cardiol 2003;42:1173–7. http://dx.doi.org/10.1016/S0735-1097(03)00920-3
14. Eagle KA, Lim MJ, Dabbous OH et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA 2004;291:2727–33. http://dx.doi.org/10.1001/jama.291.22.2727
15. Fox KA, Dabbous OH, Goldberg RJ et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observation study (GRACE). BMJ 2006;333:1091–4. http://dx.doi.org/10.1136/bmj.38985.646481.55
16. Luo JG, Yang M, Han L et al. Validity of the GRACE score for 6-month death or reinfarction after presentation with acute myocardial infarction in patients 80 years of age and older. Coron Artery Dis 2013;24:537–41. http://dx.doi.org/10.1097/MCA.0000000000000023
17. Califf RM, Pieper KS, Lee KL et al. Prediction of 1-year survival after thrombolysis for acute myocardial infarction in the global utilization of streptokinase and TPA for occluded coronary arteries trial. Circulation 2000;101:2231–8. http://dx.doi.org/10.1161/01.CIR.101.19.2231
18. Maluenda G, Delhaye C, Gaglia Jr MA et al. A novel percutaneous coronary intervention risk score to predict one-year mortality. Am J Cardiol 2010;106:641–5. http://dx.doi.org/10.1016/j.amjcard.2010.04.011
19. Granger CB, Goldberg RJ, Dabbous O. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med 2003;163:2345–53. http://dx.doi.org/10.1001/archinte.163.19.2345
20. Singh M, Holmes DR, Lennon RJ et al. Development and validation of risk adjustment models for long-term mortality and myocardial infarction following percutaneous coronary interventions. Circ Cardiovasc Interv 2010;3:423–30. http://dx.doi.org/10.1161/CIRCINTERVENTIONS.109.924308
21. Cupples LA, Gagnon DR, Wong ND et al. Preexisting cardiovascular conditions and long-term prognosis after initial myocardial infarction: The Framingham Study. Am Heart J 1993;125:863–72. http://dx.doi.org/10.1016/0002-8703(93)90182-9
23. Martin CA, Thompson PL, Armstrong BK et al. Long-term prognosis after recovery from myocardial infarction: a nine year follow-up of the Perth Coronary Register. Circulation 1983;68:961–9. http://dx.doi.org/10.1161/01.CIR.68.5.961
25. Leon AS, Franklin BA, Costa F. Cardiac rehabilitation and secondary prevention of coronary heart disease: an American Heart Association scientific statement from the Council on Clinical Cardiology. Circulation 2005;111:369–76. http://dx.doi.org/10.1161/01.CIR.0000151788.08740.5C
26. Brookes L. INTERHEART: a global case-control study of risk factors for acute myocardial infarction. Medscape Sep 21, 2004. Available from: http://www.medscape.com/viewarticle/489738