Retinal ischaemic perivascular lesions (RIPL) are characterised on spectral domain optical coherence tomography (SD-OCT) as focal thinning of the inner nuclear layer (INL) associated with outer nuclear layer (ONL) upward expansion. We present a small case series of 11 patients and reviewed all relevant original research on RIPL and its association with cardiovascular diseases (CVD). All 11 patients had RIPL incidentally identified on SD-OCT by two consultant ophthalmologists during a routine medical retina clinic. We obtained a thorough medical history to identify risk factors and CVD. The most common risk factor was type 2 diabetes mellitus (90.9%), followed by hypertension (81.9%). A diagnosis of arrhythmia was determined in 36.4% patients, coronary artery disease in 27.3%, cerebrovascular events in 36.4%, peripheral vascular disease in 27.3% and carotid artery stenosis in 8.3%. A literature search was conducted using PubMed, Google Scholar and Scopus, using all relevant key words. Seven pieces of original research were described in the literature. Six of these described a RIPL prevalence ranging from 34.62% to 91%. One paper described a case series with an incidence of 72.7% new diagnosis of CVD in their cohort who were identified to have RIPLs. The ophthalmologists’ role in detecting RIPLs could be used to assess cardiovascular risk status, supporting a multi-disciplinary approach in managing CVD.
Introduction
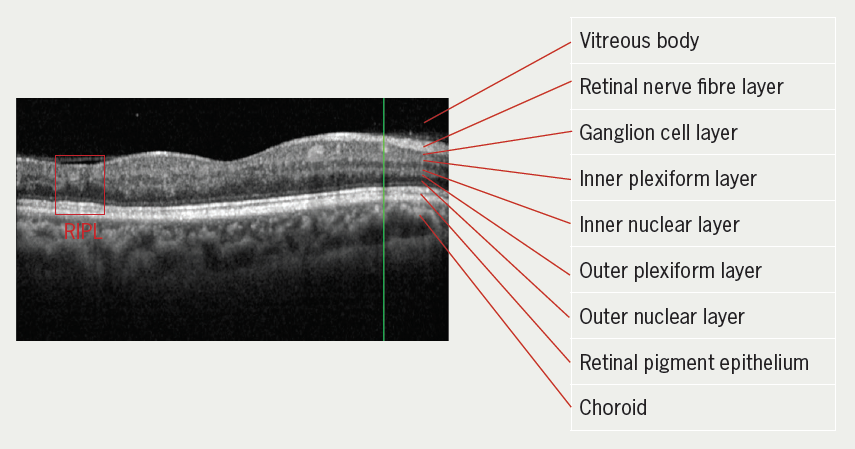
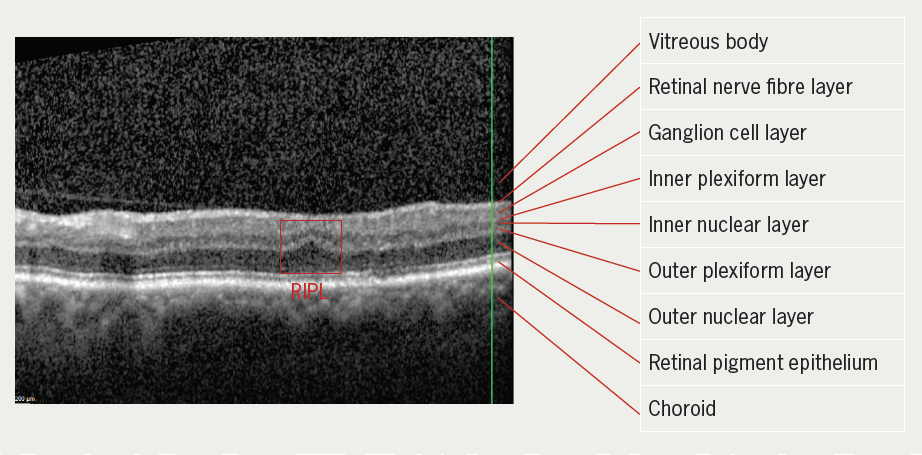
Retinal ischaemic perivascular lesions (RIPL) describe characteristic atrophic changes of the inner nuclear layer (INL) as a consequence of ischaemic injury.1 These are illustrated by spectral domain optical coherence tomography (SD-OCT) as focal thinning of the retinal INL, contemporaneous with enhanced hypo-reflectivity of the outer nuclear layer (ONL).2 RIPLs are chronic lesions originating from paracentral acute middle maculopathy (PAMM); these are hyperacute ischaemic lesions of the middle retina and are associated with multifarious vascular diseases.3,4 As opposed to their hyperacute predecessors (PAMMs), which resolve within six weeks, RIPLs are chronic changes and can, therefore, be easily observed with SD-OCT.
Recent literature hypothesise a correlation between RIPLs and diseases that cause microvascular injury, such as coronary artery disease (CAD), atrial fibrillation (AF), carotid artery stenosis (CAS) and cerebrovascular disease.1,5-10 Establishing RIPL as a biomarker of systemic disease could perhaps be used to screen patients for indolent disease and implement preventive or therapeutic treatments to lessen the morbidity of actualised cardiovascular events.2 This will be especially helpful with the increasing burden of cardiovascular diseases (CVD) among the increasingly ageing population. In the last decade, there has been an emphasis to diagnose, treat and reduce CVD in the population by implementing strategic preventive measures, including risk calculators, national and international guidelines and the emphasis on risk communication.11 Understanding RIPLs and their association with the ischaemic cascade, and how this contributes to the development of CVD, would provide an additional interventional strategy towards risk stratification and managing the morbidity and mortality of cardiovascular events.
Case description
We report a retrospective review of 11 patients with RIPL incidentally identified on SD-OCT during a routine medical retina clinic in the ophthalmology department. The study adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients. We obtained a thorough medical history to identify cardiovascular risk factors and establish diagnosis of CVD by using electronic patient records (EPR) and telephone consultation, where data were not available on EPR.
Two consultant ophthalmologists identified RIPL in these patients using SD-OCT, during routine ophthalmic follow-up in the eye clinic. RIPL was identified using the definition as initially described by Long et al.:1 focal atrophy of the INL alongside expansion of the ONL. Of the 11 patients, eight (72.7%) attended the medical retina clinic for diabetic eye disease. The other three patients were under ophthalmology follow-up for retinal artery occlusion, retinal vein occlusion and retinal pigment epithelium (RPE) changes that required monitoring. Of 21 eyes that were reviewed, 18 had RIPL. Only one eye had extensively altered retinal pathology that made it not possible to identify RIPL. Our cohort, therefore, concludes a bilaterality of RIPL in 77.8% of patients. RIPL(s) of patients 4 and 11 are demonstrated in figures 1 and 2, respectively.
The mean age of our patients was 66.27 years (range from 48 years to 94 years). Half of these patients were Caucasian (54.5%), while the others were Asian (36.4%). One patient (9%) was Middle Eastern. There were two female patients (patients 3 and 9), while the rest (81.8%) were male. The most common cardiovascular risk factor in our patients was type 2 diabetes mellitus (90.9%), which all but one patient had. This was followed by hypertension (81.9%). Only two patients (18.2%) were smokers, four patients (36.4%) never smoked and five patients (45.5%) were ex-smokers. A diagnosis of arrhythmia was determined in 36.4% of patients. CAD was diagnosed in 27.3%, cerebrovascular events including stroke and/or transient ischaemic attack (TIA) in 36.4% and CAS in 8.33%. Three patients (27.3%) had a history of peripheral vascular disease (PVD), where one was a bilateral above-knee amputee. Table 1 shows a summary of the demographics, cardiovascular risk factors and disease diagnosis of the patients. Two patients (patients 1 and 10) portrayed risk factors without a diagnosis of CVD in the presence of RIPL.
Table 1. Demographic, cardiovascular risk factors and diseases of patients studied
| Patient | Age | Sex | Race | DM | HTN | Smoking status | Arrhythmia | PVD | CAD | CAS | Stroke/TIA |
| 1 | 52 | M | A | Yes | Yes | Ex | No | No | No | No | No |
| 2 | 81 | M | A | Yes | Yes | NS | Yes | Yes | No | No | No |
| 3 | 87 | F | C | Yes | Yes | Ex | Yes | No | No | No | No |
| 4 | 48 | M | A | Yes | Yes | NS | Yes | No | Yes | No | No |
| 5 | 60 | M | C | Yes | Yes | Yes | Yes | No | Yes | No | Yes |
| 6 | 64 | M | C | Yes | Yes | NS | No | Yes | No | No | No |
| 7 | 94 | M | C | No | No | Ex | No | No | No | Yes | Yes (CRAO) |
| 8 | 55 | M | A | Yes | Yes | Yes | No | Yes | No | No | Yes |
| 9 | 63 | F | C | Yes | Yes | Ex | No | No | No | No | Yes |
| 10 | 52 | M | AR | Yes | No | Ex | No | No | No | No | No |
| 11 | 73 | M | C | Yes | Yes | NS | No | No | Yes | No | No |
| Key: A = Asian; AR = Arab; C = Caucasian; CAD = coronary artery disease; CAS = carotid artery stenosis; CRAO = central retinal artery occlusion; DM = diabetes mellitus; Ex = ex-smoker; F = female; HTN = hypertension; M = male; NS = never smoked; PVD = peripheral vascular disease; TIA = transient ischaemic attack | |||||||||||
Two-thirds of patients (63.6%) were on both a statin and antiplatelet. Three patients were on statins but not on antiplatelet medication. One patient with risk factors of CVD and a diagnosis of arrhythmia was neither on statins nor antiplatelet medication, but was on an anticoagulant.
Review of the literature
The association between RIPL and CVD is novel in literature, with the earliest publication in 2021.1 A literature search was conducted using PubMed, Google Scholar and Scopus, using key words ‘retinal ischaemic perivascular lesion’, ‘retinal ischaemic perivascular lesion AND cardiovascular disease’, ‘retinal ischaemic perivascular lesion AND atrial fibrillation’, ‘retinal ischaemic perivascular lesion AND coronary artery disease’, ‘retinal ischaemic perivascular lesion AND cerebrovascular disease’ and ‘retinal ischaemic perivascular lesion AND peripheral vascular disease’. A total of seven pieces of original research were described in literature, six of which were conducted in the US and one in China. A summary of these is provided in tables 2 and 3.
Table 2. Summary of bibliography: participant identification based on cardiovascular disease
| Author (year) | Study design | Disease of interest | Number of study participants | Number of controls | Prevalence of RIPL in study patients | Prevalence of RIPL in control |
| Long et al. (2021) | Case-control | CAD | 84 | 76 | 56% 2.8 RIPL lesions |
32.9% 0.8 RIPL lesions |
| Zhang et al. (2023) | Case-control | CAS | 22 | 11 | 3.5 RIPL lesions | 1.2 RIPL lesions |
| Bakhoum et al. (2023) | Case-control | AF | 106 | 91 | 57.5% | 37.4% |
| Drakopoulos et al. (2023) | Case-control | CAS | 23 | 14 | 91% 3.4 RIPL lesions |
71% 2.0 RIPL lesions |
| Kwapong et al. (2024) | Case-control | SSI | 105 | 80 | 34.62% | 4.17% |
| Bousquet et al. (2024) | Case-control | CAD (± MI) | 54 (CAD with MI) | 263 (CAD without MI) | 59.3% 2.3 RIPL lesions |
35.7% 1.2 RIPL lesions |
| Key: AF = atrial fibrillation; CAD = coronary artery disease; CAS = carotid artery stenosis; MI = myocardial infarction; RIPL = retinal ischaemic perivascular lesion; SSI = subcortical infarction | ||||||
Table 3. Summary of bibliography: participant identification based on retinal ischaemic perivascular lesion (RIPL)
| Author (year) | Study design | Inclusion criteria | Number of study participants | Number of controls | New diagnosis of cardiovascular disease |
| Madala et al. (2023) | Case series | RIPL | 11 | No control | 8 (72.7%) |
Six of the original research were case-control studies where patient identification was based on the presence of diseases of interest: CVD, CAS, AF, single subcortical infarction (SSI), CAD and their association with RIPL. Madala et al.7 described a case series where study participants were identified based on the presence of RIPL. In all studies, RIPLs were identified manually by the authors, except Drakopoulos et al.5 where the authors used an algorithm to quantitatively analyse RIPL with SD-OCT.
The prevalence of RIPL in patients with CVD varied from 34.62% to 91%, while in the control group, the prevalence was a wider range from 4.17% to 71%. All authors described a statistical significance between the two groups. Interestingly, Drakopoulos et al., who used an algorithm to identify RIPL, described the highest prevalence of RIPL in both patients with CAD and the control group (91% and 71%, respectively). Four authors also described a higher mean number of RIPL lesions, ranging from 2.3 to 3.5, in patients with CVD than in the control group (range from 0.8 to 2.0). Madala et al. reported an incidence of 72.7% newly diagnosed CVD in their cohort, with two cases highlighted as a potential way of using RIPL to uncover underlying CVD.
Discussion
The identification of RIPL on SD-OCT as a biomarker for CVD is a novel subject with limited discussion in the literature. While there is a proven association between RIPL and CVD, the degree of its association and how this association could be manifested in clinical practice can potentially be further developed. SD-OCTs are a quick, easily available and non-invasive way of detecting RIPL, which could perhaps be an additional biomarker in assessing cardiovascular risk status. Considering how widely associated many medical retina conditions are with cardiovascular risk factors, such as retinal and vein occlusions, diabetic eye diseases and ischaemic neuropathies; ophthalmologists, primary care practitioners and physicians should undertake a multi-disciplinary approach towards the management of CVD in the population.
Excluding the Drakopoulos et al. study on the association between RIPL and CAS using algorithm-driven identification of RIPL, all other studies had similar associations in terms of percentage prevalence and number of RIPL lesions, when comparing CAD (Long et al., Bousquet et al.)1,10 and AF (Bakhoum et al.).9 We can expect about over half to two-thirds of patients with CVD to have RIPL. We can expect the number of lesions to range from 2.3 to 3.5. This observation has a caveat – these values might be an underestimation as all authors excluded patients with co-existing retinal pathologies, such as vein and artery occlusion, which are strongly associated with CVD.
Interestingly, Kwapong et al.8 described a lower prevalence of RIPL in association with SSI (34.9%). The authors had very strict exclusion criteria; SSI was determined using magnetic resonance imaging (MRI) and any history of stroke/TIA, AF, valvopathy or myocardial infarction were excluded from the study, which likely led to an underestimation of its true prevalence. When Long et al. first described RIPL, they found that cerebrovascular disease had a higher association with RIPL than CAD. The authors suggested that this is likely due to the anatomical manifestation of the retina being a forward extension of the brain, suggesting that RIPLs would be more associated with ischaemia in the cerebral vessels when compared with the coronary vessels. Our case series demonstrated a slightly higher diagnosis of cerebrovascular events in patients with RIPL (four patients), where three of these patients had no pre-existing CAD.
Long et al. established that RIPL in association with CVD had sensitivity and specificity values of 56% and 67.1%, respectively. While the sensitivity value may be low, Long et al. identified an association in those with already established CVD. This was similar in most publications on RIPL and its association with CVD. Madala et al. suggested that RIPL may be helpful in identifying patients who are at risk of developing CVD and may, inevitably find the disease course establish itself. This is highlighted in patients 1 and 10 in our cohort who have identified RIPL and cardiovascular risk factors with no established CVD.
Our case series demonstrates a real-world snapshot of the demographics of patients presenting to the medical retina clinic. There is variation in age, ethnicity, cardiovascular risk factors and diagnosis. It would be interesting to observe if patients 1 and 10 have a future diagnosis of CVD. Even without a diagnosis of a cardiovascular event, it would be clinically reasonable to prescribe these patients treatment for primary prevention of CVD, in the presence of risk factors and RIPL.
Major limitations to our study include a significantly small number and non-consecutive patient selection. There was also no standardised work-up in determining cardiovascular risk factors and diseases. We suggest an area of potential research is to determine the association between RIPL and PVD, independent of other underlying cardiovascular risk factors and diseases. Furthermore, as an extension to Madala et al.’s study, we suggest a prospective cohort study to observe the development of CVD in patients who have incidental findings of RIPL. This could potentially identify how these microvascular insults to the retinal layers could predict the development of CVD pathology.
There are suggestions that cardio-oculomics integrated with a deep-learning algorithm is the future in CVD prediction, detection and screening.12 While this is a financially costly, but yet exciting, avenue to explore, its application in the real-world setting is still far from being materialised. RIPLs, which would be easily visually detected by any general ophthalmologist, provide an avenue for universal clinical evaluation, and in conjunction with the patient history, could provide individualised management and referral to the physician for potential diagnosis and, subsequently, treatment of CVD.
Key messages
- There is a proven association between retinal ischaemic perivascular lesions (RIPL) and cardiovascular disease (CVD); the degree of this association and how this can be manifested in clinical practice can be further developed
- Our case series demonstrates a variety of 11 patients with CVD association who present to the medical retina clinic with the presence of RIPL in a real-world setting
- We can expect over half to two-thirds of patients with CVD to have RIPL; the number of these lesions can range from 2.3 to 3.5 lesions
- Further prospective studies are needed to determine the timing and development of CVD in patients with RIPL
Conflicts of interest
None declared.
Funding
None.
Study approval
We received signed informed consent forms from all participants before including them in the case series.
Patient consent
Patients 4 and 11 provided written consent for publication of images.
References
1. Long CP, Chan AX, Bakhoum CY et al. Prevalence of subclinical retinal ischemia in patients with cardiovascular disease – a hypothesis driven study. EClinicalMedicine 2021;33:100775. https://doi.org/10.1016/j.eclinm.2021.100775
2. Colcombe J, Mundae R, Kaiser A, Bijon J, Modi Y. Retinal findings and cardiovascular risk: prognostic conditions, novel biomarkers, and emerging image analysis techniques. J Pers Med 2023;13:1564. https://doi.org/10.3390/jpm13111564
3. Burnasheva MA, Maltsev DS, Kulikov AN, Sherbakova KA, Barsukov AV. Association of chronic paracentral acute middle maculopathy lesions with hypertension. Ophthalmol Retina 2020;4:504–09. https://doi.org/10.1016/j.oret.2019.12.001
4. Maltsev DS, Kulikov AN, Burnasheva MA. Association of resolved paracentral acute middle maculopathy lesions with diabetic retinopathy. J Curr Ophthalmol 2022;34:318–22. https://doi.org/10.4103/joco.joco_91_22
5. Drakopoulos M, Zhang DL, Cheng BT et al. Swept-source optical coherence tomography angiography metrics of retinal ischaemic perivascular lesions in patients being evaluated for carotid artery stenosis and controls. BMJ Open Ophthalmol 2023;8:e001226. https://doi.org/10.1136/bmjophth-2022-001226
6. Zhang DL, Zhang KX, Cheng BT et al. Retinal ischemic perivascular lesions are increased in carotid artery stenosis. Ophthalmol Retina 2023;7:1020–2. https://doi.org/10.1016/j.oret.2023.07.018
7. Madala S, Adabifirouzjaei F, Lando L et al. Retinal ischemic perivascular lesions, a biomarker of cardiovascular disease. Ophthalmol Retina 2022;6:865–7. https://doi.org/10.1016/j.oret.2022.05.005
8. Kwapong WR, Yan Y, Cao L et al. Retinal ischemic perivascular lesion reflects cerebral small vessel disease burden in single subcortical infarction. J Am Heart Assoc 2024;13:e033081. https://doi.org/10.1161/JAHA.123.033081
9. Bakhoum CY, Madala S, Lando L et al. Retinal ischemic perivascular lesions in individuals with atrial fibrillation. J Am Heart Assoc 2023;12:e028853. https://doi.org/10.1161/JAHA.122.028853
10. Bousquet E, Santina A, Au A et al. Retinal ischemic perivascular lesions are associated with myocardial infarction in patients with coronary artery disease. Am J Ophthalmol 2024;264:224–8. https://doi.org/10.1016/j.ajo.2024.03.017
11. Bakhit M, Fien S, Abukmail E et al. Cardiovascular disease risk communication and prevention: a meta-analysis. Eur Heart J 2024;45:998–1013. https://doi.org/10.1093/eurheartj/ehae002
12. Chan YK, Cheng CY, Sabanayagam C. Eyes as the windows into cardiovascular disease in the era of big data. Taiwan J Ophthalmol 2023;13:151–67. https://doi.org/10.4103/tjo.TJO-D-23-00018
