Saphenous vein grafts (SVGs) are frequently used for coronary artery bypass grafting (CABG) of severe coronary artery disease; however, re-stenosis is common. Restoration of blood flow to the SVG is uncommonly achieved via revascularisation of the native vessel. A man in his 70s with previous CABGs presented with prolonged chest pain at rest. The left anterior descending (LAD) and left circumflex arteries had chronic total occlusions (CTO), and the SVG and left internal mammary artery, previously used to bypass the LAD, were severely diseased with sluggish flow and an inability to pass a balloon or microcatheter. Rotational atherectomy was successfully performed to cross the LAD CTO, with good flow post-stenting. He remained asymptomatic one year later. Where management of calcified venous grafts precludes passage with balloon or microcatheter, rotational atherectomy of the native coronary may represent an alternative method of restoring blood flow.
Introduction
Coronary artery bypass grafting (CABG) is the preferred management strategy for multi-vessel or high-risk coronary artery disease,1 and involves the surgical bypass of occluded coronary arteries. Affected vessels may be bypassed using venous conduits, such as the saphenous vein graft (SVG), or arterial conduits like the left internal mammary artery (LIMA) and the radial artery. An established complication of the SVG conduit is re-stenosis or occlusion secondary to malignant atherosclerosis,2 and, despite recent evidence supporting enhanced durability of radial arterial conduits compared with SVG,3,4 a large proportion of patients have existing SVGs due to anatomical difficulties or older surgeries.5 Revascularisation of occluded venous grafts more commonly relies on percutaneous coronary intervention (PCI) of the graft itself, or in rarer circumstances, of the native coronary vessel. We describe herein the case of a patient with a balloon-uncrossable SVG lesion who successfully underwent rotational atherectomy and subsequent stenting of the native vessel.
Case presentation
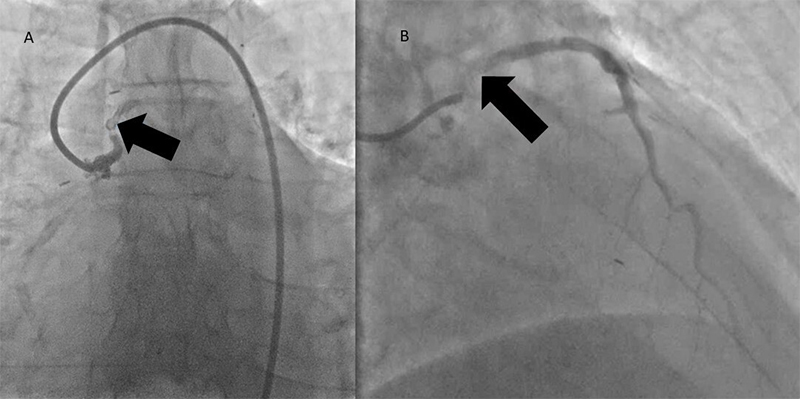
A man in his 70s was admitted with a three-week history of crescendo angina that culminated in prolonged chest pain at rest. Relevant past medical history included a transient ischaemic attack, five myocardial infarctions (MI), with a first CABG performed in 1985 with SVG to the left anterior descending (LAD), left circumflex (LCx), and right coronary (RCA) arteries and a subsequent further bypass surgery in 2005 with LIMA to LAD and SVGs to RCA and first obtuse marginal arteries. He was a non-smoker, independent with activities of daily living and not limited by exertional symptoms prior to this presentation. His medications included ramipril 2.5 mg twice daily (bid), lansoprazole 15 mg once daily (od), isosorbide mononitrate 60 mg od, eplerenone 25 mg od, dapagliflozin 10 mg od, bisoprolol 5 mg od, aspirin 75 mg od, and atorvastatin 80 mg od. Physical examination was unremarkable apart from a prior sternotomy scar, and moderate left ventricular systolic dysfunction was noted on trans-thoracic echocardiography. His electrocardiogram (ECG) showed sinus rhythm with a left bundle branch block, unchanged from 2014. High-sensitivity troponin was elevated but remained static 31 ng/L (99th percentile values less than 15 ng/L). The remainder of the blood tests were unremarkable. Angiography was performed in a local district general hospital, which showed that the LAD and LCx arteries had chronic total occlusions (CTO), and the SVG to LAD, performed in the initial bypass procedure, had severe disease with sluggish flow (figure 1). The LIMA to the LAD, performed in the second bypass procedure, had completely occluded as well, likely secondary to competitive flow from the previously functioning SVG to the same artery. The RCA had diffuse severe disease with a complete mid-vessel occlusion, while the SVG to posterior descending artery (PDA) was patent. Similarly, the SVG to obtuse marginal (OM) branch was also patent. An attempt at revascularisation of the diseased SVG to LAD was performed locally, but was unsuccessful, and, therefore, the patient was referred to our centre for further management of ongoing ischaemic symptoms.
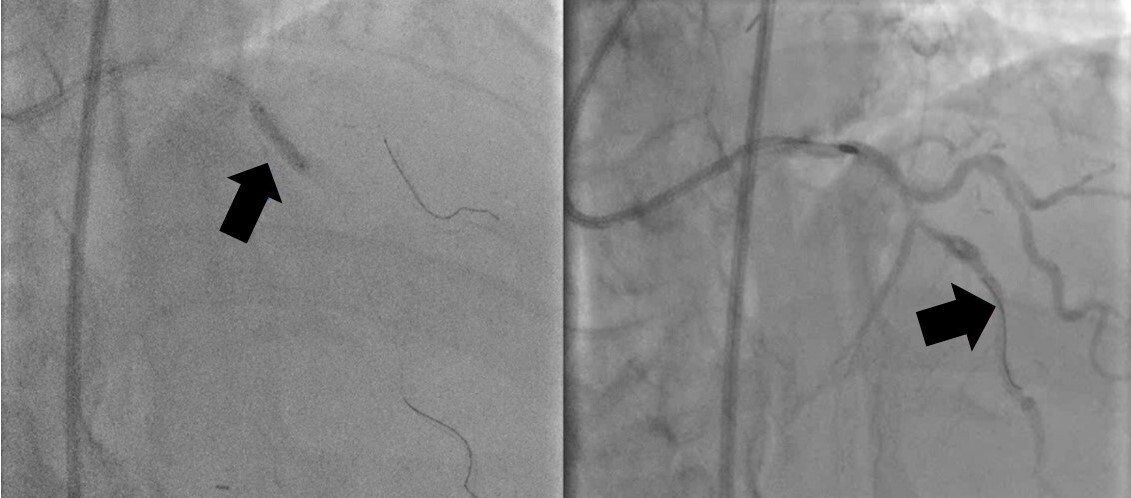
![Safdar - Figure 2. The left anterior descending artery (LAD) had severe disease at the origin of the septal branch (arrow) and was completely occluded (thrombolysis in myocardial infarction [TIMI] 0 flow) beyond the diagonal and septal branches which constituted the mid-LAD](https://bjcardio.co.uk/wp-content/uploads/2025/09/Figure_2.jpg)
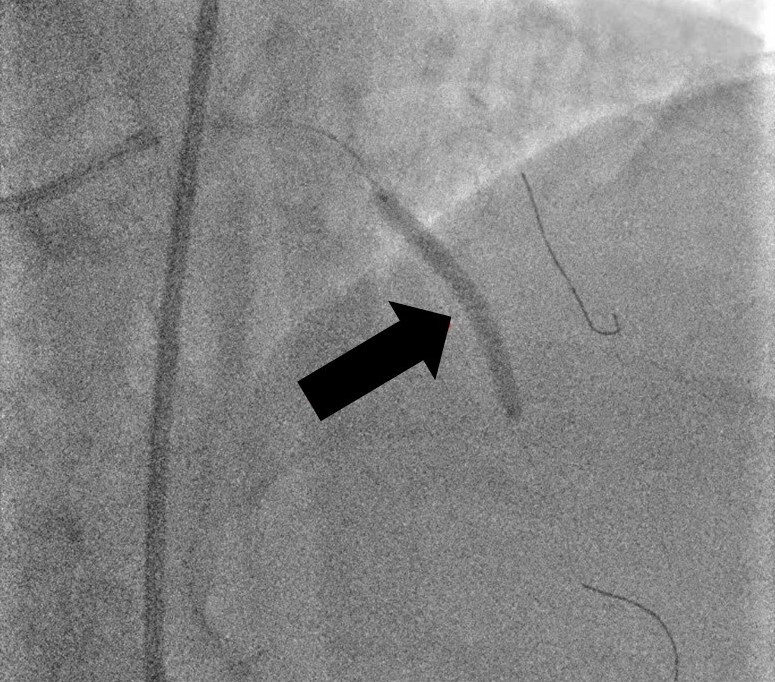
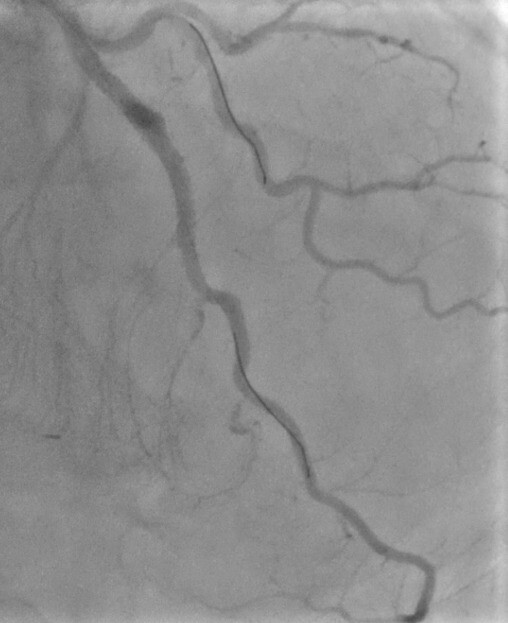
Given his rapidly progressive symptoms, it was decided to proceed with a further invasive angiogram with a view to revascularisation, instead of opting for non-invasive stress tests. A 6 French (Fr), Amplatz left 3.0 (Medtronic, Ireland) guide catheter was used to engage the SVG to LAD. Although both Confianza and Gladius guidewires were able to negotiate the vessel stenosis, multiple attempts at crossing with balloon or microcatheter were unsuccessful. Due to prolonged procedure time, it was decided to stop the attempt and consider a further review in a multi-disciplinary meeting, as well as with the patient and his preferences. On review of angiography images, a potential antegrade channel was identified in the LAD CTO and, given significant ongoing symptoms, it was decided with the patient to have a further attempt at revascularisation of the native chronically occluded LAD artery, instead of medical therapy, given the severity and persistence of chest pain, accepting a higher risk of potential complications. Therefore, a 7 Fr sheath was inserted, using ultrasound guidance, into the right femoral artery to allow improved guide support and 10,000 units of unfractionated heparin administered, with a further 5,000 units given subsequently, to maintain activated clotting time of greater than 250 seconds. Given the patient had patent SVGs to PDA and OM vessels and moderately impaired left ventricular systolic function, mechanical support would not have offered additional benefit, and would have exposed the patient to an additional risk of complications. Therefore, a 7 Fr XB 3.5 guide catheter (Cordis, UK) was used to engage the coronary ostium and a Sion (Vascular Perspectives, Holmfirth, UK) guidewire assisted by a Turnpike (Teleflex, US) microcatheter was used to negotiate the stenosis. Attempts at crossing the lesion with a balloon were, again, unsuccessful. Therefore, the workhorse wire was exchanged for a rota-floppy wire (Boston Scientific) and rotational atherectomy, using a 1.5 mm burr, was performed, which was successful in crossing the mid-CTO artery (figure 2). The Sion wire was reintroduced, and pre-dilatation of the mid-LAD was performed using a 2.5 × 12 mm semi-compliant balloon, followed by a 3.0 × 20 mm non-compliant (NC) balloon at 16 atmospheres (ATM), successfully restoring blood flow (figure 3). Since the NC balloon expansion was satisfactory and allowed good estimation of the reference target vessel measurements, it was opted to proceed with stent deployment at the mid-proximal (3.0 × 20 mm Supraflex, SMT, India) and mid-LAD (3.0 × 32 mm Supraflex, SMT, India) at 14 ATM with good apposition and absence of edge dissection (figure 4), and excellent flow post-stent placement (figure 5).
Following overnight observation with no complications, the patient was discharged home the next day. He continued dual-antiplatelet therapy with aspirin 75 mg od and ticagrelor 90 mg bid for 12 months, and aspirin only, indefinitely, thereafter. At 12-month follow-up, he continued to be free of angina and remained stable from a cardiovascular perspective.
Discussion
CABG continues to be an important procedural consideration in the management of acute coronary syndrome.6 SVGs remain a popular conduit despite concerns around their longevity. This is in part due to accelerated atherosclerosis in the venous grafts2 – stenotic lesions are formed via the expansion of necrotic cores consisting of foamy macrophages and neointimal hyperplasia – but also due to a similar increased rate of atherosclerosis observed in native coronary arteries.7
Once occluded, management of SVGs includes medical therapy, redo-CABG, or PCI. Medical therapy and redo-CABG were considered, but unavailable due to our patient’s unstable presentation and history of two prior CABGs, respectively. Furthermore, PCI to the venous conduit has been the traditional intervention of choice. In this instance, the occlusive plaque was found in a SVG that was over 30 years old, and the inability to progress a balloon or microcatheter through the heavily calcified lesion, despite several attempts, was a significant limitation to this approach.
Rotational atherectomy, a previously contraindicated technique for plaque modification due to the risk of distal no-reflow and coronary perforations,8 has had some success in the reported literature in crossing occluded SVGs,9–13 without any complications. Nonetheless, given the advanced age of the graft and the high risk of subsequent perforation, we chose to perform rotational atherectomy at the native coronary vessel to allow for best longevity of the vessel. We successfully recanalised the LAD and were able to stent it to good effect with a stable result at 12 months.
In conclusion, in patients with heavily calcified balloon-uncrossable venous graft stenosis or occlusions, rotational atherectomy of the native vessel may represent an effective alternative method of restoring blood flow.
Key messages
- Although saphenous vein grafts are frequently used for coronary artery bypass grafting (CABG), rate of re-stenosis is high and they are not as durable as arterial grafts
- In cases where re-stenosed venous grafts are unpassable using a balloon or microcatheter, and medical therapy or redo-CABG is not viable, alternative approaches are required
- Rotational atherectomy of the native vessel should be considered as an effective method for revascularisation
Conflicts of interest
None declared.
Funding
MUS received travel and educational grants from Boehringer Ingelheim, not relevant to this manuscript.
Patient consent
Written consent for submission and publication of this case including images and associated text has been obtained from the patient in line with COPE guidance.
References
1. Neumann FJ, Sousa-Uva M, Ahlsson A et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J 2019;40:87–165. https://doi.org/10.1093/eurheartj/ehy855
2. Yazdani SK, Otsuka F, Nakano M, Ladich E, Virmani R. Pathology of saphenous vein grafts. Interv Cardiol Clin 2013;2:241–9. https://doi.org/10.1016/j.iccl.2012.11.002
3. Gaudino M, Benedetto U, Fremes S et al. Radial-artery or saphenous-vein grafts in coronary-artery bypass surgery. N Engl J Med 2018;378:2069–77. https://doi.org/10.1056/NEJMoa1716026
4. Athanasiou T, Saso S, Rao C et al. Radial artery versus saphenous vein conduits for coronary artery bypass surgery: forty years of competition – which conduit offers better patency? A systematic review and meta-analysis. Eur J Cardiothorac Surg 2011;40:208–20. https://doi.org/10.1016/j.ejcts.2010.11.012
5. Tabata M, Grab JD, Khalpey Z et al. Prevalence and variability of internal mammary artery graft use in contemporary multivessel coronary artery bypass graft surgery: analysis of the Society of Thoracic Surgeons National Cardiac Database. Circulation 2009;120:935–40. https://doi.org/10.1161/CIRCULATIONAHA.108.832444
6. Byrne RA, Rossello X, Coughlan JJ et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J 2023;44:3720–826. https://doi.org/10.1093/eurheartj/ehad191
7. Campeau L, Enjalbert M, Lespérance J et al. The relation of risk factors to the development of atherosclerosis in saphenous-vein bypass grafts and the progression of disease in the native circulation. N Engl J Med 1984;311:1329–32. https://doi.org/10.1056/NEJM198411223112101
8. Warth DC, Leon MB, O’Neill W, Zacca N, Polissar NL, Buchbinder M. Rotational atherectomy multicenter registry: acute results, complications and 6-month angiographic follow-up in 709 patients. J Am Coll Cardiol 1994;24:641–8. https://doi.org/10.1016/0735-1097(94)90009-4
9. Don CW, Palacios I, Rosenfield K. Use of rotational atherectomy in the body of a saphenous vein coronary graft. J Invasive Cardiol 2009;21:E168–E170. Available from: https://www.hmpgloballearningnetwork.com/site/jic/articles/use-rotational-atherectomy-body-saphenous-vein-coronary-graft
10. Ponangi UP, Baveja S. Successful angioplasty of saphenous venous graft in-stent restenosis using rotational atherectomy. BMJ Case Rep 2019;12:e230907. https://doi.org/10.1136/bcr-2019-230907
11. Gedela M, Li S, Bhatnagar U, Stys A, Stys T. Orbital atherectomy and heavily calcified saphenous vein graft intervention. Tex Heart Inst J 2020;47:41–3. https://doi.org/10.14503/THIJ-18-6640
12. Cardenas JR, Strumpf RK, Heuser RR. Rotational atherectomy in restenotic lesions at the distal saphenous vein graft anastomosis. Cathet Cardiovasc Diagn 1995;36:53–7; discussion 58. https://doi.org/10.1002/ccd.1810360113
13. Pellicano M, Floré V, Barbato E, De Bruyne B. From debulking to delivery: sequential use of rotational atherectomy and GuidezillaTM for complex saphenous vein grafts intervention. BMC Cardiovasc Disord 2018;18:122. https://doi.org/10.1186/s12872-018-0860-y
