Reduction in low-density lipoprotein-cholesterol (LDL-C) in patients with hypercholesterolaemia is associated with a lower risk of cardiovascular (CV) events. Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibiting therapy is approved by the National Institute for Health and Care Excellence (NICE) and the Scottish Medicines Consortium (SMC) for use in high-risk patients who are unable to achieve the LDL-C target levels, despite other maximum tolerated lipid-lowering therapies. Our prior publication analysed the records of patients in a large Scottish health board with familial hypercholesterolaemia and high CV risk and confirmed the real-world efficacy of PCSK9 inhibiting monoclonal antibodies (mAbs) in routine clinical care.
In this follow-up study, we examined the comparative efficacy of inclisiran, a small-interfering ribonucleic acid (siRNA) therapeutic, in a similar patient cohort to provide real-world data that can guide clinicians in optimising lipid-lowering strategies.
Introduction
Our previous study on the efficacy and tolerability of proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibiting monoclonal antibodies (mAbs), such as alirocumab and evolocumab, in real-world clinical practice confirmed significant and sustained reductions in LDL-C levels. These findings were observed in high-risk, statin-intolerant patients and others with known cardiovascular (CV) disease risks.1 Notably, our real-world results aligned with outcomes reported in pivotal trials, such as the ODYSSEY OUTCOMES (Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab) and FOURIER (Further cardiovascular OUtcomes Research with PCSK9 Inhibition in subjects with Elevated Risk) studies, underscoring the effectiveness of anti-PCSK9 mAbs in reducing LDL-C and CV risk.2,3
Inclisiran represents another novel approach to PCSK9 inhibition. Unlike monoclonal antibodies, inclisiran is a small-interfering ribonucleic acid (siRNA) that targets hepatic PCSK9 synthesis. By binding to the messenger RNA of the PCSK9 precursor, inclisiran promotes its degradation, thereby reducing PCSK9 production. This mechanism enhances the availability of LDL-receptors on hepatocytes, facilitating increased clearance of LDL-C from the bloodstream.4
The bi-annual administration of inclisiran by healthcare professionals may enhance patient adherence compared with the self-administered fortnightly dosing required for PCSK9 inhibiting mAbs. However, while mAbs have demonstrated CV event reduction, similar outcome data for inclisiran is still awaited.
The ORION-4 trial, an event-driven outcomes study, will provide valuable insights into whether inclisiran reduces cardiovascular events in high-risk dyslipidaemic patients.5 There is a need for further research into inclisiran’s real-world efficacy as these data are still evolving.
Method
Inclisiran is the first-line PCSK9 inhibiting agent (PCSK9i) at NHS Tayside, a territorial health board in the East of Scotland, UK. The clinical records of all patients prescribed inclisiran (n=23) at NHS Tayside Cardiovascular Risk Clinic between 2022 and 2024 were retrospectively reviewed for this audit.
Patients were included if they had at least one recorded cholesterol measurement at baseline (defined as the last cholesterol measurement prior to inclisiran administration) and a follow-up measurement at six months. Patients were excluded if they were lost to follow-up (n=3) or if their clinic reviews fell outside the audit timeframe (n=1), resulting in a final sample size of 19 patients.
The primary end points were the percentage reductions in LDL-C and total cholesterol (TC) from baseline to six months post-inclisiran administration. LDL-C is a key marker of cardiovascular risk and the primary target of inclisiran therapy, and TC is often measured alongside LDL-C to reflect the overall cholesterol burden. Lipid levels were obtained from routinely collected clinical laboratory data.
Among the 19 patients, three did not demonstrate a reduction in LDL-C levels at the first three-month clinic review and were subsequently switched to evolocumab, a PCSK9i mAb. Lipid levels for these patients were further monitored three months after the switch to evaluate the efficacy of anti-PCSK9 mAb therapy.
Descriptive statistics were used to summarise patient characteristics and lipid reductions. The necessary Caldicott approval from NHS Tayside was obtained for this audit.
| Key: LDL-C = low-density lipoprotein cholesterol; mAb = monoclonal antibody; PCSK9 = proprotein convertase subtilisin/kexin type 9; TC = total cholesterol |
Results
Between 2022 and 2024, 23 high-risk patients (10 female, 13 male) with hypercholesterolaemia attending the cardiovascular risk clinic were initiated on inclisiran therapy to reduce LDL-C levels. For secondary prevention, the therapeutic indications for inclisiran in NHS Tayside included adults with familial hypercholesterolaemia (HeFH) and LDL-C ≥3.5 mmol/L or those with polyvascular disease and LDL-C ≥3.5 mmol/L. Of the 23 patients in our audit, three had HeFH, while 20 were categorised as having polyvascular disease.
Four patients were excluded from the final analysis due to loss to follow-up or clinic reviews falling outside the audit timeframe, leaving 19 patients for evaluation. Among these, three (16%) showed minimal LDL-C reduction with inclisiran at the initial three-month clinic review and were subsequently switched to evolocumab, with no adverse effects reported during inclisiran therapy. Their LDL-C reductions were –29%, –39% and +3%, respectively, at the three-month review.
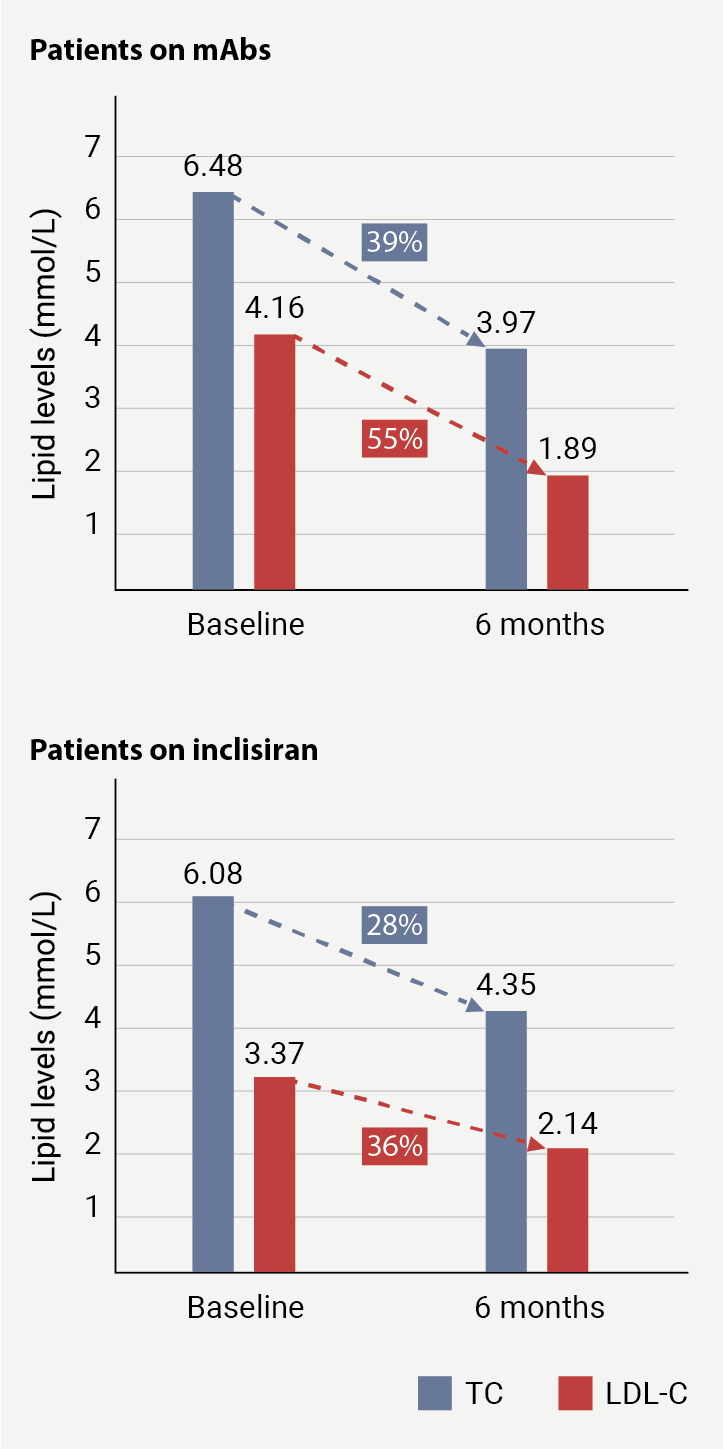
At six months post-administration, patients treated with inclisiran demonstrated a mean reduction in TC of 28% and LDL-C of 36%. In comparison, results from our previous audit on patients receiving anti-PCSK9 mAbs (evolocumab/alirocumab) reported superior reductions of 39% in TC and 55% in LDL-C over the same period (figure 1).1
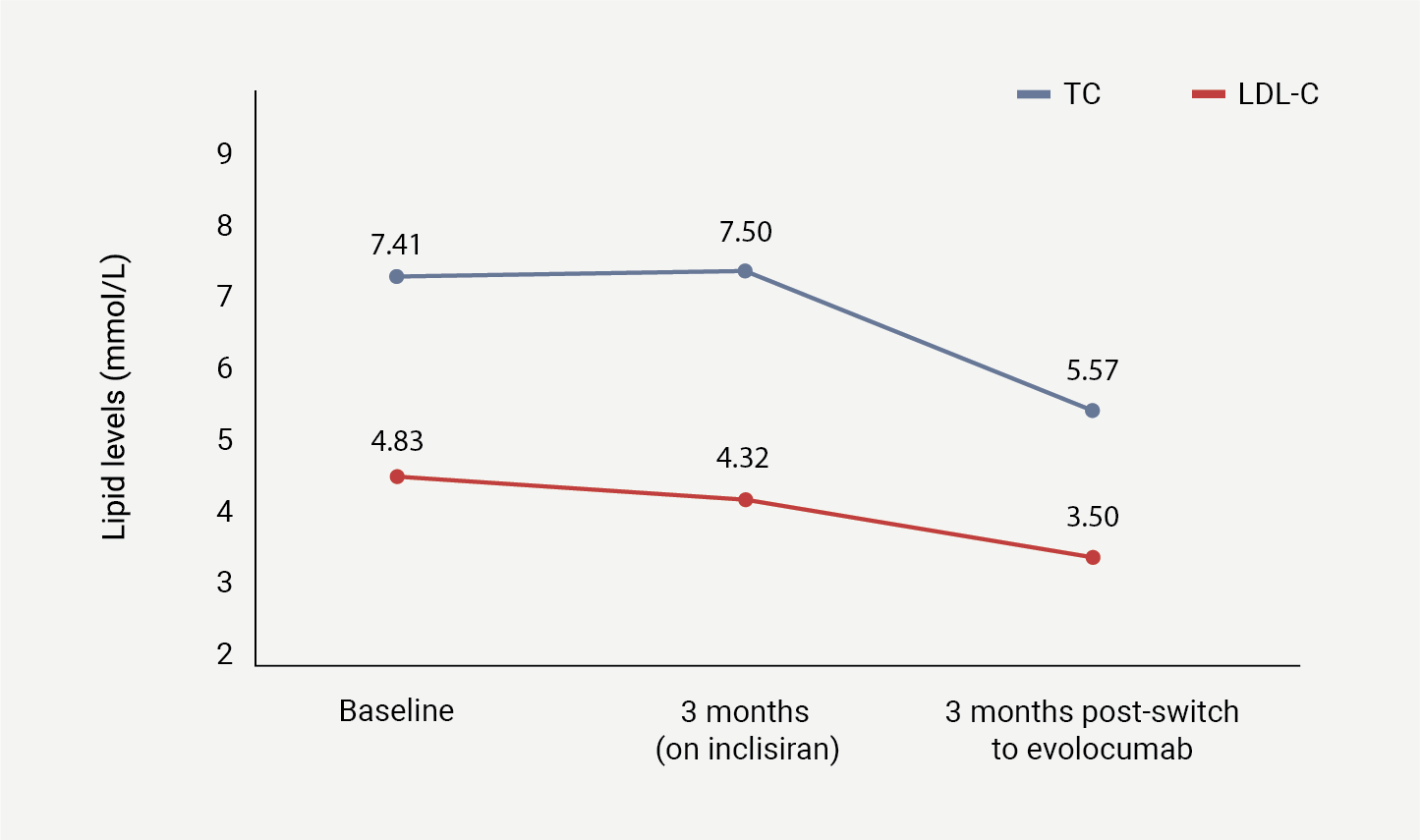
Additionally, the three patients switched from inclisiran to evolocumab achieved further reductions of 26% in TC and 19% in LDL-C within three months of the switch, although the small sample size limits broader applicability (figure 2).
The results reviewed from this study highlight the greater potency of anti-PCSK9 mAbs in comparison with inclisiran, with a more immediate and pronounced effect on LDL-C reduction, consistent with data seen in the pivotal trials of these agents. As seen in the FOURIER and ODYSSEY phase 3 trials, evolocumab achieved a 59% reduction in LDL-C and alirocumab demonstrated LDL-C reductions between 44.1 and 54.0%, respectively.2,6 In the ORION 11 trial, inclisiran shows a 49.2% reduction in LDL-C.7
| Key: LDL-C = low-density lipoprotein-cholesterol; TC = total cholesterol |
Discussion
While the results of our audit confirm the real-world LDL-C lowering efficacy of inclisiran, they also reveal that PCSK9i mAbs, such as evolocumab and alirocumab, provide superior and more immediate reductions in LDL-C, aligning with data from pivotal trials.2,3
The clinical significance of differences in LDL-C reduction between therapies warrants further exploration. A recent comprehensive meta-analysis analysed 60 randomised-controlled trials and found that for each 1 mmol/L reduction in LDL-C, there was a 22% reduction in the risk of major vascular events. Notably, for secondary prevention, this effect remained stable over the follow-up time of nearly 10 years, indicating that the benefits of LDL-C reduction are sustained over the long term for high-risk patients.8 If the superior LDL-C reduction observed with PCSK9i mAbs in our audit is maintained long term, it could potentially translate to greater reductions in CV events compared with inclisiran. However, this projection assumes sustained efficacy over time, which requires further long-term comparative studies to confirm. The potential impact on CV outcomes must be weighed against other factors, such as adherence and individual patient characteristics, when selecting therapy.
Inclisiran’s bi-annual dosing regimen offers the potential for improved patient compliance compared with the fortnightly administration required for mAbs. Additionally, the professional medication administration for inclisiran reduces the likelihood of compliance issues. The reduced frequency of injections may also be more suitable for patients with lipoatrophy.
On the other hand, PCSK9i mAbs offer advantages in LDL-C reduction, and their fortnightly clinical administration could also provide opportunities for closer clinical monitoring and management in a high-risk patient group. These distinctions highlight the importance of individualised treatment strategies that balance efficacy with adherence and patient-specific factors, particularly in high-risk CV patients.
A key limitation of this audit was the small sample size, which restricts the generalisability of the findings. Nonetheless, our study provides valuable insights into the clinical performance of inclisiran in real-world settings and emphasises the need for further research.
Larger studies with extended follow-up periods and direct comparisons to other lipid-lowering therapies, including statins, are essential to assess the long-term benefits of inclisiran and its role in reducing cardiovascular morbidity and mortality.
Key messages
- Both the proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibition therapies involving monoclonal antibodies (mAbs) and small-interfering ribonucleic acid (siRNA) therapy are aimed at prevention of PCSK9-mediated low-density lipoprotein (LDL)-receptor destruction
- While PCSK9i mAbs have demonstrated significant reduction in the LDL-cholesterol (LDL-C) levels of high-risk patients, head-to-head trials and real-world clinical audits will help provide a better understanding of the roles each drug can play in managing dyslipidaemia
- Clinicians can make patient-centred decisions between a favourable dosing regimen (biannual for inclisiran vs. fortnightly for mAbs) for improved patient compliance versus increased efficacy of evolocumab/alirocumab
Conflicts of interest
None declared.
Funding
None.
Study approval
Necessary Caldicott approval for this audit was obtained from NHS Tayside health board (Caldicott approval number IGTCAL-2023-129).
References
1. Devaiah P, Handjiev S, George J. Efficacy and tolerability of PCSK9 inhibitors in real-world clinical practice. Br J Cardiol 2023;30:153–6. https://doi.org/10.5837/bjc.2023.044
2. Sabatine MS, Giugliano RP, Keech AC et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017;376:1713–22. https://doi.org/10.1056/NEJMoa1615664
3. Schwartz GG, Steg PG, Szarek M et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med 2018;379:2097–107. https://doi.org/10.1056/NEJMoa1801174
4. Ray KK, Landmesser U, Leiter LA et al. Inclisiran in patients at high cardiovascular risk with elevated LDL cholesterol. N Engl J Med 2017;376:1430–40. https://doi.org/10.1056/NEJMoa1615758
5. ClinicalTrials.gov. A randomized trial assessing the effects of inclisiran on clinical outcomes among people with cardiovascular disease (ORION-4). Available at: https://clinicaltrials.gov/study/NCT03705234#more-information
6. Kastelein JJP, Kereiakes DJ, Cannon CP et al. Effect of alirocumab dose increase on LDL lowering and lipid goal attainment in patients with dyslipidemia. Coron Artery Dis 2017;28:190–7. https://doi.org/10.1097/MCA.0000000000000438
7. Ray KK, Wright RS, Kallend D et al. Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol. N Engl J Med 2020;382:1507–19. https://doi.org/10.1056/NEJMoa1912387
8. Burger PM, Dorresteijn JAN, Koudstaal S et al. Course of the effects of LDL-cholesterol reduction on cardiovascular risk over time: a meta-analysis of 60 randomized controlled trials. Atherosclerosis 2024;396:118540. https://doi.org/10.1016/j.atherosclerosis.2024.118540
