Diagnostic coronary angiography (CA) remains the gold-standard assessment of coronary artery disease (CAD). Transfemoral access remains a commonly used approach. Arterial tortuosity can lead to difficulties in coronary engagement, particularly when intubating the right coronary artery (RCA). Excessive catheter manipulation may result in knotting.
Gentle application of counter-rotational torque may permit guidewire passage to release the knot, but usually distal catheter fixation is required. Previous reports describe ‘grabbing forceps’ or snare delivery from the contra-lateral femoral approach.1,2
We present three transfemoral CA cases, complicated by catheter knotting resolved using transradial snare delivery for distal fixation (figure 1).
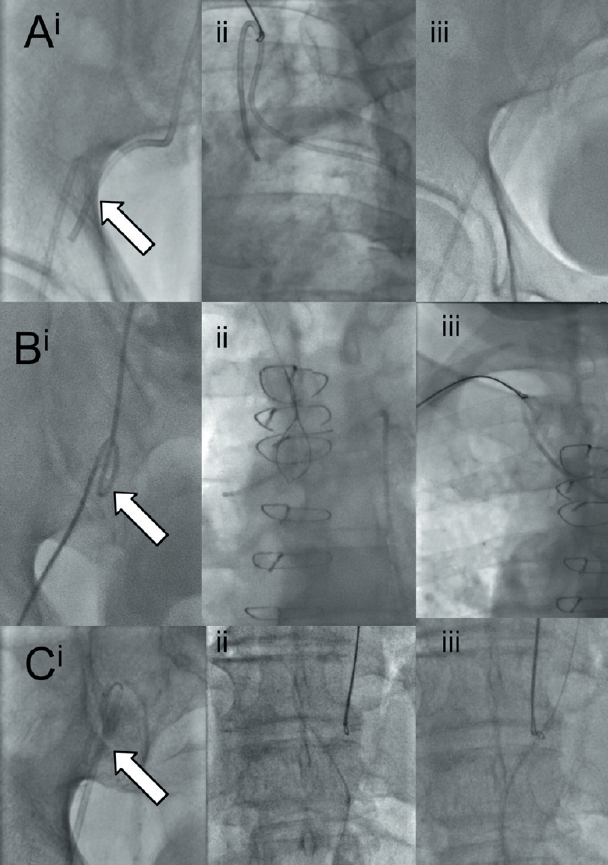
Case 1: A man with known CAD presented for repeat angiography. During RCA intubation the Judkins right 4 (JR4) catheter knotted in the iliac artery (figure 1A).
Case 2: A man with previous coronary artery bypass surgery required CA. Femoral tortuosity and over manipulation of a JR4 resulted in a catheter knot forming in the iliac artery (figure 1B).
Case 3: A man attended for RCA percutaneous coronary intervention (PCI). An 8F Amplatz left 1 (AL1) guide catheter knot developed at the secondary curve during intubation and remained despite retracting into descending aorta (figure 1C).
Discussion
In each case, the catheter knot was undone by distal catheter fixation with an Amplatz gooseneck snare (ev3 endovascular, Plymouth, USA) delivered transradially (figure 1). While the use of transfemoral snares has been described,2,3 this is the first report utilising a transradial approach.
The snare catheter is delivered to the aortic root on a 0.035″ guidewire. The snare is introduced and the distal knotted catheter is manoeuvred into the open lasso. Tightening the loop around the distal catheter permits fixation and, with effective counter-torque on the proximal catheter, it is removed.
This technique, through a 6F sheath, avoids further femoral puncture so reducing vascular
access complications.
Conflict of interest
None declared.
References
- Tanner MA, Ward D. Percutaneous technique for the reduction of knotted catheters. Heart 2003;89:1132–3. http://dx.doi.org/10.1136/heart.89.10.1132
- Rafie IM, Viswanathan G, Penny WJ. Transfemoral contralateral technique to retrieve knotted coronary artery catheter using Amplatz Goose Neck snare catheter. BMJ Case Reports 2010. http://dx.doi.org/10.1136/bcr.12.2009.2598
- Khoubyari R, Arsanjani R, Habibzadeh MR, Echeverri J, Movahed MR. Successful removal of an entrapped and kinked catheter during right transradial cardiac catheterization by snaring and unwinding the catheter via femoral access. Cardiovasc Revasc Med 2012;13:202.e1–202.e3. http://dx.doi.org/10.1016/j.carrev.2012.01.001
