
Introduction
The British Journal of Cardiology (BJC) recently convened a round table discussion at the Royal Society of Medicine on 12th November 2012 between representatives from primary and secondary care to discuss the most recent 2011 NICE/BHS hypertension guideline, its implementation and future progress. The meeting also considered best practice measures that could be taken to aid its implementation to improve the diagnosis of hypertension and reduce the number of uncontrolled patients with hypertension. This supplement summarises these discussions. The meeting was sponsored by and convened on behalf of Takeda UK Limited. Throughout the text, supporting materials can be accessed by clicking on the following symbol (![]() ).
).
Round table meeting faculty

Chair
Dr Terry McCormack
General Practitioner, Whitby Group Practice, Whitby, North Yorkshire; Secretary, British Hypertension Society
Panel
Dr Chris Arden
General Practitioner, Park Surgery, Chandlers Ford; GP with a Special Interest in Cardiology, Southampton
Dr Alan Begg
General Practitioner with a Special Interest in Cardiology, Links Health Centre, Montrose, Angus; Honorary Lecturer, University of Dundee
Professor Mark Caulfield
Director William Harvey Research Institute
Barts and the London School of Medicine and Dentistry, Queen Mary, University of London
Dr Kathryn Griffith
General Practitioner with a Special Interest in Cardiology, Unity Health, University Health Centre, University of York
Ms Helen Williams
Consultant Pharmacist for Cardiovascular Disease, South London Cardiac and Stroke Network
Why do we need hypertension guidelines?
Hypertension is a serious public health problem because it is a major risk factor for cardiovascular events, chronic kidney disease (CKD), cognitive decline and premature death.1 The risk conferred by hypertension is continuous.1 Based on a definition of blood pressure ≥140/90 mmHg or receiving treatment, 31.5% of men and 29.0% of women in England are hypertensive.2
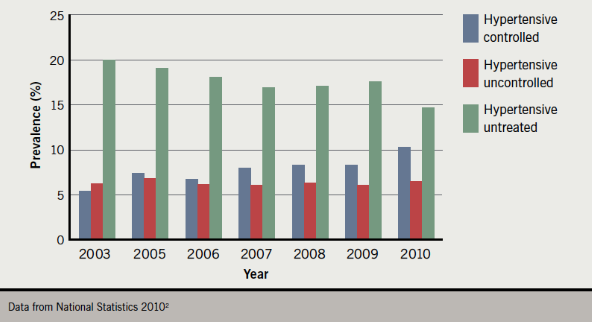
Over the last decade, there has been an improvement in the management of hypertension in the UK (figure 1). Between 2003 and 2010 in England, the proportion of adults in the population with controlled hypertension increased from 5.4% to 10.3% in men and from 6.0% to 10.9% in women. Between 2003 and 2010, the proportion of adults in the population with untreated hypertension fell from 20.1% to 14.7% among men and from 15.8% to 10.3% among women.2
(Click to enlarge any figure)
Randomised clinical trials demonstrate that lowering blood pressure in people with hypertension substantially reduces the risk of cardiovascular morbidity and mortality and, as a result, the management of hypertension is one of the most common interventions in medicine.3 The diagnosis, treatment and follow-up of hypertensive patients is a core part of primary care workload. In 2006, hypertension accounted for 12% of primary care consultations,1 or an estimated 400 consultations per 2,000 list patients each year.4 Regular blood pressure checks are now routine in the UK as part of the NHS health checks.
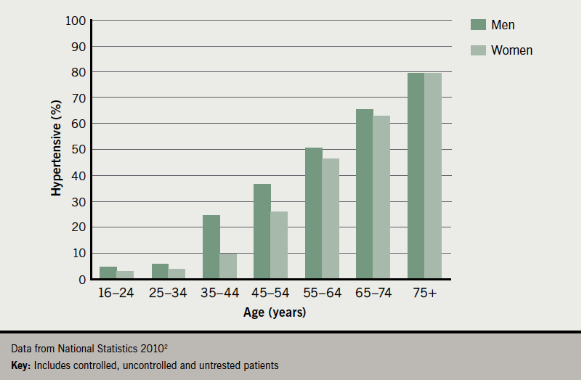
In contrast, the proportion of patients taking medication for blood pressure with uncontrolled hypertension has hardly changed since 2003, remaining at 6–8% in men and women.2 These overall statistics also mask continuing problems among people aged >60 years, who account for more than half of all people with hypertension.1 In 2010, 20.7% of men and 19.4% of women aged 65–74 years had uncontrolled hypertension, while 17.9% of men and 20.0% of women were untreated.2 Figure 2 shows the prevalence of hypertension with age in 2010.
The prevalence of hypertension and hence the workload for primary care can only continue to rise as the UK population becomes older, more sedentary and obese.1 This supplement aims to offer practical advice and guidance on implementing the National Institute for Health and Clinical Excellence (NICE) 2011 hypertension guideline1 in order to optimise blood pressure control in the majority of hypertensive patients who are managed in primary care.
The new hypertension guidelines
 Published in August 2011 in collaboration with the British Hypertension Society (BHS), NICE Clinical Guideline 1271 is a partial update of NICE Clinical Guideline 185 published in 2004 on the management of hypertension in primary care and NICE Clinical Guideline 346 published in 2006 with an update of advice on pharmacological treatment.
Published in August 2011 in collaboration with the British Hypertension Society (BHS), NICE Clinical Guideline 1271 is a partial update of NICE Clinical Guideline 185 published in 2004 on the management of hypertension in primary care and NICE Clinical Guideline 346 published in 2006 with an update of advice on pharmacological treatment.
The new guideline concerns only the clinical management of primary hypertension in adults who may, or may not, have pre-existing cardiovascular disease (CVD). ‘Primary hypertension’ describes the approximately 90% of people encountered in clinical practice with sustained high blood pressure for which there is no obvious, identifiable cause. The recommendations do not apply to the remaining 10% of patients with secondary hypertension for which there is a specific underlying cause, such as renovascular disease, Conn’s adenoma or phaeochromocytoma. Nor does the guideline apply to people with diabetes, accelerated or acute hypertension, or to pregnant women, children, and young people aged under 18 years.1
The 2011 guideline’s use of the term ‘primary hypertension’ represents a change from the 2004/2006 guidelines,5,6 which were intended for people with ‘essential hypertension’. This terminology was previously used because high blood pressure was thought to be ‘essential’ to perfuse diseased and sclerotic arteries, but this is now regarded as inaccurate since arteries become diseased and sclerotic due to the effects of high blood pressure.1
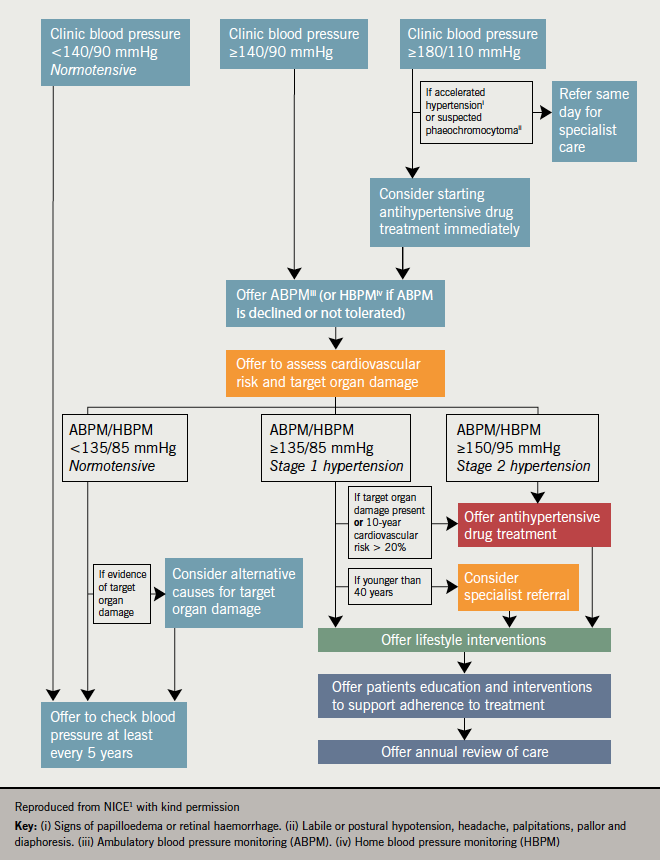
Other changes in the 2011 guideline include new blood pressure targets for people on treatment, recommendations for pharmacological treatment, managing hypertension in elderly people (aged >80 years), younger adults (age <40 years) and drug-resistant hypertension.1 However, perhaps one of the most significant changes for primary care – and, according to the faculty, a potential challenge for implementation – may be the recommendation to use 24-hour ambulatory blood pressure monitoring (ABPM) to confirm the diagnosis of primary hypertension (figure 3).1
Like all NICE guidelines, the 2011 hypertension guideline1 follows a review of the best available published evidence based on a pre-determined, carefully defined scope.7 This approach, which is designed to ensure evidence-based rather than opinion-based recommendations, is internationally recognised for its rigour8 and is influencing the formulation of other cardiovascular guidelines, such as the US Joint National Committee’s guidelines on cardiovascular risk reduction.9 The faculty noted that the NICE/BHS 2011 guideline1 states there is only weak evidence for fourth-line antihypertensive therapy; and a paucity of data for the management of hypertension in patients aged <40 years, but this does not mean that this patient group should not be intensively treated.
Diagnosing hypertension
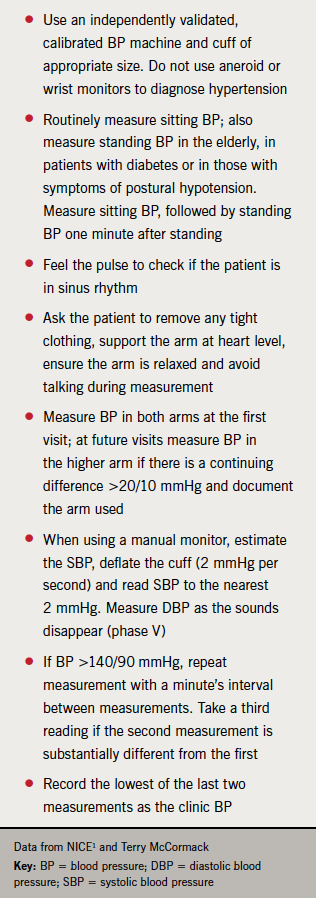
The new NICE/BHS guideline1 stresses that blood pressure should be measured carefully and by adequately trained health professionals (table 1). Blood pressure devices that have been tested and meet BHS criteria are listed on the BHS website (see ![]() 1). Since automated devices may not measure blood pressure accurately in a patient with an irregular pulse, the first step is to palpate the radial or brachial pulse to check that the patient is in sinus rhythm. If the pulse is irregular, blood pressure should be measured manually using direct auscultation over the brachial artery.1 The faculty also felt that this could be an opportunity to recommend an ECG appointment to confirm/exclude atrial fibrillation.
1). Since automated devices may not measure blood pressure accurately in a patient with an irregular pulse, the first step is to palpate the radial or brachial pulse to check that the patient is in sinus rhythm. If the pulse is irregular, blood pressure should be measured manually using direct auscultation over the brachial artery.1 The faculty also felt that this could be an opportunity to recommend an ECG appointment to confirm/exclude atrial fibrillation.
If the clinic blood pressure measurement (CBPM) is ≥140/90 mmHg on two more readings, the diagnosis of hypertension should be confirmed by ABPM. According to the NICE/BHS 2011 guideline,1 there are several reasons for this new recommendation. ABPM measures blood pressure regularly while patients undertake their usual activities, provides more information than either home or clinic measurements, and is a better predictor than clinic measurement of cardiovascular risk and target organ damage.1 ABPM is also cost effective, since initial extra costs – for example, from the acquisition of the monitors – are balanced by cost savings associated with the avoidance of unnecessary treatment and the reduction in the number of consultations required to arrive at a diagnosis.10
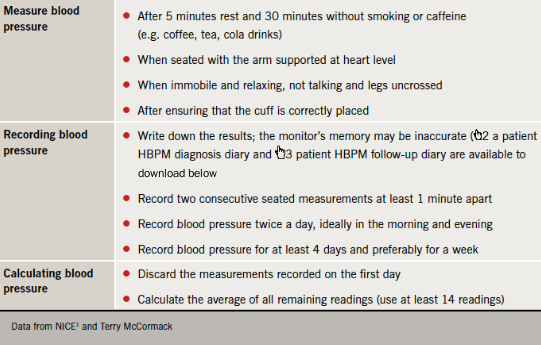
There is no need for most patients to wear the monitor at night, since ABPM measurements to confirm the diagnosis of hypertension are generally taken during the individual’s usual waking hours. If ABPM is unavailable or it is refused or not tolerated, patients can be offered home blood pressure monitoring (HBPM), though careful advice is essential to ensure accurate readings (table 2).1
Stages of hypertension
In its 2004 hypertension guideline,5 NICE defined two grades of hypertension – Grade 1 (140–159/90–99 mmHg) and Grade 2 (≥160/100 mmHg). NICE recommended that patients with Grade 2 hypertension should be offered pharmacological treatment, but was cautious about treating patients with uncomplicated Grade 1 hypertension (i.e. without target organ damage, CVD, CKD, diabetes, or 10-year CVD risk <20%).
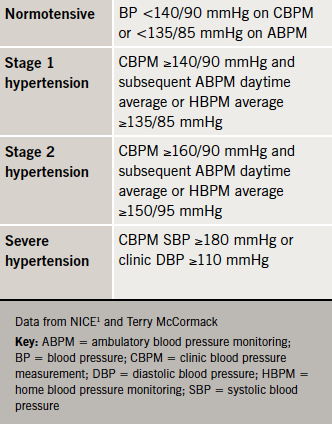
Based on a review of evidence published since 2003 (the cut-off point for the 2004/06 recommendations5,6), the 2011 guideline has introduced two new stages of hypertension, and definitions of normotensive and severe hypertension (table 3).1 In the experience of the primary care members of the faculty, this new, staged definition of hypertension has caused some confusion, but it necessarily follows from the recommendation to use ABPM to confirm a finding of hypertension on CBPM.
 The guideline recommends that alternative causes should be sought if a normotensive patient shows findings, such as left-ventricular hypertrophy, albuminuria or proteinuria, which would suggest target organ damage in a person with hypertension. Other normotensive patients should be offered a blood pressure check at least every five years.1 The faculty considered that more frequent follow-up is advisable for patients with white coat hypertension (when a patient has a consistently elevated clinic blood pressure and a normal home or ambulatory blood pressure day-time average of <135/80 mmHg) since their risk of future cardiovascular events is similar to that seen in patients with established hypertension.11
The guideline recommends that alternative causes should be sought if a normotensive patient shows findings, such as left-ventricular hypertrophy, albuminuria or proteinuria, which would suggest target organ damage in a person with hypertension. Other normotensive patients should be offered a blood pressure check at least every five years.1 The faculty considered that more frequent follow-up is advisable for patients with white coat hypertension (when a patient has a consistently elevated clinic blood pressure and a normal home or ambulatory blood pressure day-time average of <135/80 mmHg) since their risk of future cardiovascular events is similar to that seen in patients with established hypertension.11
Treating hypertension
All patients with Stages 1 and 2 hypertension should be offered appropriate lifestyle intervention. As shown in table 4, antihypertensive drug therapy should be offered to all adult patients with Stage 2 hypertension and higher-risk patients aged <80 years with Stage 1 hypertension. Since hypertension is a cardiovascular risk factor rather than a disease, NICE strongly recommends that all patients should undergo formal assessment of their global cardiovascular risk before commencing treatment.1

The new NICE/BHS hypertension guideline1 follows NICE’s lipid modification guideline in recommending using the estimated 10-year cardiovascular risk of ≤20% (see ![]() 4) as the threshold for treatment.12 At the same time, NICE recognises that 10-year risk assessment will underestimate lifetime risk in people aged <40 years with Stage 1 hypertension.1 In the faculty’s opinion, the availability of lifetime risk calculation using an appropriately validated tool represents an important advance for all patients. One example of such tools is the QRISK Lifetime Risk Calculator (
4) as the threshold for treatment.12 At the same time, NICE recognises that 10-year risk assessment will underestimate lifetime risk in people aged <40 years with Stage 1 hypertension.1 In the faculty’s opinion, the availability of lifetime risk calculation using an appropriately validated tool represents an important advance for all patients. One example of such tools is the QRISK Lifetime Risk Calculator (![]() 5). Not only does lifetime risk assessment help to avoid under-treatment in at-risk younger patients, but sharing this information may also reinforce advice to any patient concerning the benefits of lifestyle changes and medication to reduce future cardiovascular risk. The faculty believes there is a need for the use of lifetime calculators to become standard practice in the near future.
5). Not only does lifetime risk assessment help to avoid under-treatment in at-risk younger patients, but sharing this information may also reinforce advice to any patient concerning the benefits of lifestyle changes and medication to reduce future cardiovascular risk. The faculty believes there is a need for the use of lifetime calculators to become standard practice in the near future.
While the 2011 hypertension guideline1 retains the familiar four-step approach to therapy (figure 4), there are some important changes from the 2004/06 guidelines.5,6 In 2006 at Step 1, NICE recommended either a thiazide-type diuretic or a calcium channel blocker (CCB) in people aged ≥55 years or of black African or Caribbean descent of any age, but this has changed in the new guideline (figure 4).
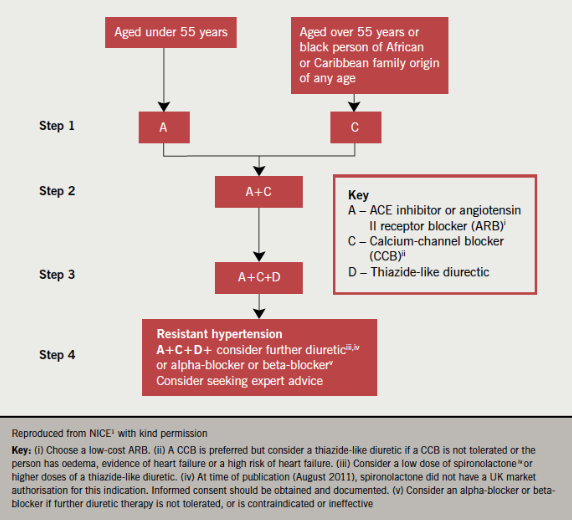
An angiotensin-converting enzyme inhibitor (ACE inhibitor) was recommended for people aged <55 years, with angiotensin receptor blockers (ARBs) reserved for patients in whom ACE inhibitors were not tolerated or were contraindicated.6 The 2011 treatment algorithm (figure 4) recommends either ACE inhibitors or low-cost ARBs for this group and takes into account recent studies demonstrating equivalent clinical outcomes with these classes of drug.13-15 Similarly, a diuretic is no longer routinely recommended as an alternative to a CCB at Steps 1 and 2, because of superior outcomes for CCBs in clinical trials. It is also now more cost effective to use ARBs and CCBs since many are available as generics.1
Thiazide-like diuretics (such as chlortalidone [12.5–25.0 mg once daily] or indapamide [1.5 mg modified-release or 2.5 mg once daily]), should generally be introduced at Step 3, though there is the option to offer one of these drugs at Steps 1 and 2 if a CCB is inappropriate – for example, due to intolerance, oedema or risk of heart failure. In the faculty’s experience, there is a continuing lack of awareness concerning the NICE/BHS recommendation to use a thiazide-like diuretic, rather than conventional thiazide diuretics such as bendroflumethiazide.1 This new recommendation has been prompted by the superior evidence base for thiazide-like diuretics, but there is no need to switch patients who are established on thiazide diuretics if their blood pressure is stable and well controlled.1
Step 4 now specifically concerns patients with ‘resistant hypertension’. At first glance, the recommendations are similar to those for 2006 in terms of adding in further diuretic therapy, an alpha blocker or beta blocker, and seeking specialist advice.6 However, the 2011 guideline recommends use of further diuretics as fourth-choice therapy, with alpha blockers or beta blockers reserved for patients in whom further diuretic therapy is not tolerated, contraindicated or ineffective. People with serum potassium ≤4.5 mmol/l can be offered low-dose spironolactone (25 mg once daily), but this should be used with caution in patients with reduced estimated glomerular filtration rate (eGRF) because of a higher risk of hyperkalaemia. If serum potassium is >4.5 mmol/l, then higher-dose thiazide- like diuretic treatment may be considered as an alternative.1
NICE was cautious in the 2004/6 hypertension guidelines about the balance of risk and benefit in treating elderly hypertensive patients, because these patients had largely been excluded from clinical trials.5,6 Since then, studies such as HYVET16 have demonstrated the clinical benefits of treating hypertension in people aged ≥80, while health economic analysis has confirmed the cost effectiveness of this strategy.1 As a result, NICE now recommends that patients aged ≥80 years should be offered treatment only if they have Stage 2 hypertension.1
In the opinion of the faculty, the decision to prescribe antihypertensive medication in the elderly population should be made only after the individual patient has been supported to make an informed decision on the basis of the risks and benefits of treatment. The 2011 hypertension guideline also recommends that the decision to treat should be based on standing blood pressure, and should take into account the presence of co-morbidities such as dementia. The guideline also makes a distinction between initiating treatment in the over-80s and continuing long-term and well-tolerated treatment when patients reach this age. In other words, patients who were started on treatment when younger should not have their current therapy back-titrated when they celebrate their 80th birthday.1
Blood pressure targets and audit standards
After reviewing the evidence, NICE concluded that CBPM should generally be used to monitor response to treatment in hypertensive patients. ABPM or HBPM can be used to support CBPM monitoring in patients with white coat hypertension or if the patient prefers to monitor their own blood pressure.1
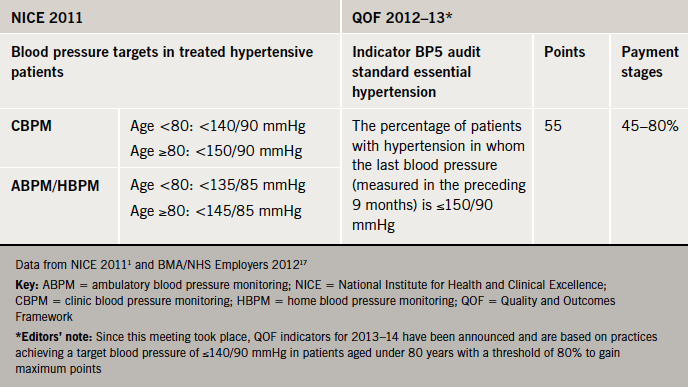
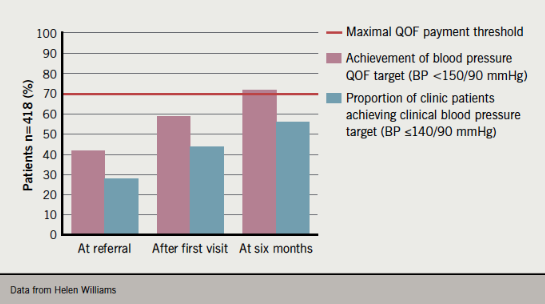
With the exception of the CBPM target for patients aged ≥80 years, the current Quality and Outcomes Framework (QOF) blood pressure audit standard is higher than the 2011 NICE/BHS treatment targets (table 5). According to the faculty, since the NICE/BHS target of <140/90 mmHg has been shown to improve outcomes in treated hypertensive patients,1 there could be many patients who remain at higher risk if they are treated only to the QOF audit target. For example, while 72% of 418 patients at a community hypertension clinic achieved the current QOF blood pressure target of <150/90 mmHg six months after referral, only 46% reached the clinical target of <140/90 mmHg (figure 5),18 which suggests that some GPs may consider the audit standard as the treatment target.
A lower QOF audit standard will be introduced (see editors’ note in table 5) following NICE’s recommendations for indicators in QOF 2013/14.19 (This will not be introduced in Scotland where separate negotiations are being carried out.) The faculty suggested that it will be less challenging to achieve this more stringent target if the NICE/BHS 2011 clinical blood pressure targets are already part of the practice protocol – a strategy that is being followed by some primary care organisations (see ![]() 6).
6).
Hypertension in practice
 Based on QOF data for England, the prevalence of hypertension in adults increased from 11.3% to 13.6% between 2005 and 201220 and the proportion of practices achieving the QOF BP5 indicator rose from 70% in 2005 to almost 80% in 2012,20 which suggests a success for QOF. This overall statistic, however, hides some important variations in exception reporting. In 2010/11, there was ≤5% exception reporting in more than 78% of GP practices, but the range for exception reporting was 0–50% across England with 5% of practices reporting over 10% exceptions for this indicator.21 According to the faculty, this indicates that there are likely to be wide variations in the implementation of the 2011 hypertension guideline – a suggestion borne out by faculty members’ own experience (see boxes 1–3 at bottom of article).
Based on QOF data for England, the prevalence of hypertension in adults increased from 11.3% to 13.6% between 2005 and 201220 and the proportion of practices achieving the QOF BP5 indicator rose from 70% in 2005 to almost 80% in 2012,20 which suggests a success for QOF. This overall statistic, however, hides some important variations in exception reporting. In 2010/11, there was ≤5% exception reporting in more than 78% of GP practices, but the range for exception reporting was 0–50% across England with 5% of practices reporting over 10% exceptions for this indicator.21 According to the faculty, this indicates that there are likely to be wide variations in the implementation of the 2011 hypertension guideline – a suggestion borne out by faculty members’ own experience (see boxes 1–3 at bottom of article).
Equally, there is some evidence of changes in prescribing habits that may to some extent reflect the influence of the 2011 NICE/BHS treatment recommendations. The number of annual prescriptions for ACE inhibitors rose from about 8.4 million in June 2007, for example, to 10.5 million in June 2012, and there has been similar growth in ARB prescribing, which has risen from 3.2 million to over 4 million. CCB prescribing has also increased, rising from 6.5 million annual prescriptions in June 2007 to about 8.5 million in June 2012. There has, however, been little change in diuretic prescribing. Although there is some indication of growth in use of indapamide, bendroflumethiazide remains by far the most commonly prescribed diuretic.22
Implementing the guideline: overcoming the challenges
Coding
 Accurate data entry has been essential for practices since the introduction of the QOF and, more recently, audit and revalidation. In the faculty’s experience, uncertainty about precise Read coding has been an unforeseen consequence of the change of terminology from ‘essential’ to ‘primary’ hypertension in the NICE/BHS 2011 hypertension guideline. Since there is currently no Read code for primary hypertension, the faculty strongly recommended that practices should continue to use the G20 Read code designated for essential hypertension and also for people with secondary hypertension so these patients will be included in monitoring and follow-up. It is also important that private patients with newly diagnosed hypertension have a cardiovascular risk assessment at the time of diagnosis and are coded appropriately.
Accurate data entry has been essential for practices since the introduction of the QOF and, more recently, audit and revalidation. In the faculty’s experience, uncertainty about precise Read coding has been an unforeseen consequence of the change of terminology from ‘essential’ to ‘primary’ hypertension in the NICE/BHS 2011 hypertension guideline. Since there is currently no Read code for primary hypertension, the faculty strongly recommended that practices should continue to use the G20 Read code designated for essential hypertension and also for people with secondary hypertension so these patients will be included in monitoring and follow-up. It is also important that private patients with newly diagnosed hypertension have a cardiovascular risk assessment at the time of diagnosis and are coded appropriately.
Recording blood pressure readings with a Read code means they are less likely to be lost to computerised searches. Read code 662L can be used for ABPM to record 24-hour blood pressure; Read code 246d can be used for HBPM to record the average home systolic blood pressure levels, although diastolic values can also be entered.
 The faculty considered that failure to appropriately code patients, including individual blood pressure values, increases the risk that some patients, e.g. those with white coat hypertension, will not be recalled for follow-up – a potentially serious issue given their known cardiovascular risk.11 For this reason, and to support audit and revalidation, the faculty recommended that practices consider using embedded computer templates to record blood pressure and related data when patients with hypertension attend for review, since this is more likely to ensure correct coding for subsequent searches of the practice registers. The use of clinical templates also improves the accuracy of data and coding.
The faculty considered that failure to appropriately code patients, including individual blood pressure values, increases the risk that some patients, e.g. those with white coat hypertension, will not be recalled for follow-up – a potentially serious issue given their known cardiovascular risk.11 For this reason, and to support audit and revalidation, the faculty recommended that practices consider using embedded computer templates to record blood pressure and related data when patients with hypertension attend for review, since this is more likely to ensure correct coding for subsequent searches of the practice registers. The use of clinical templates also improves the accuracy of data and coding.
Measuring blood pressure
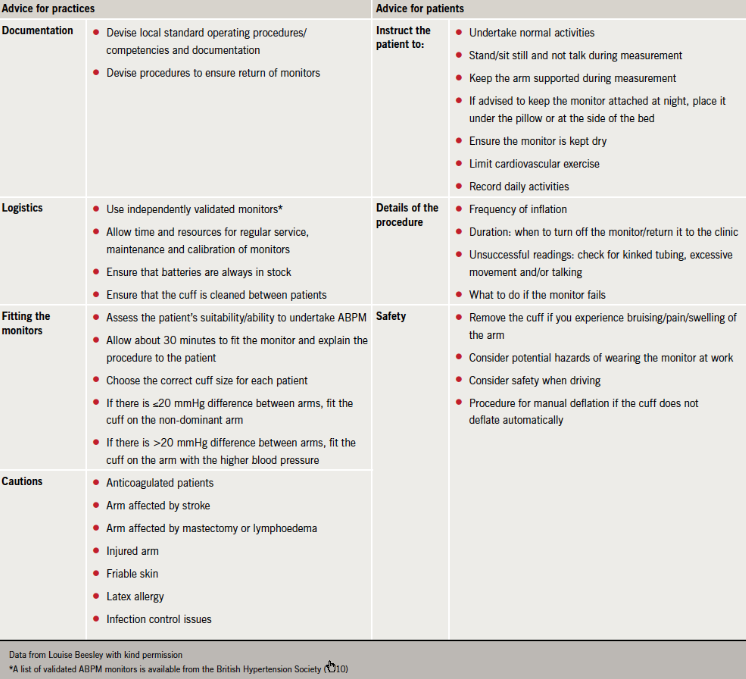
The importance of careful blood pressure measurement in the clinic (table 3) is well established. However, the faculty considered that some practices might be less aware of potential problems when implementing ABPM. Table 6 outlines some practical advice for practices and patients. More detailed information, including standard operating procedures and a clinic checklist, is available from the BHS (![]() 7). The BHS also provides a patient information leaflet on ABPM (
7). The BHS also provides a patient information leaflet on ABPM (![]() 8) and a patient diary (
8) and a patient diary (![]() 9) to help ensure that daily activities are recorded during monitoring.
9) to help ensure that daily activities are recorded during monitoring.
(see ![]() 10)
10)
The faculty considered that using HBPM will help patients to self-monitor their hypertension. Some patients may also record their blood pressure on devices that link with smartphone apps or computer programs and record measurements for output in graphic format. Although these technologies have yet to be validated, they represent, in the opinion of the faculty, an important opportunity to engage with patients who are sufficiently motivated to bring their own readings for discussion during clinic appointments. Patients should be encouraged to keep written diaries (see ![]() 2,
2, ![]() 3,
3, ![]() 9 for downloadable patient diary forms).
9 for downloadable patient diary forms).
Concordance
Concordance with antihypertensive drug regimens is an especially important challenge since long-term persistence is known to be low. Based on drug dispensing records from community pharmacies and linked hospital discharge records, a Dutch study on patients with hypertension found that only 39% of patients used their medication continuously during the 10 years of follow-up. About 22% temporarily discontinued and restarted treatment but 39% discontinued permanently.23
It is clearly important to check that hypertensive patients are taking their medication and also to check the prescribing records when performing a hypertension review. The faculty strongly endorsed a non-judgemental approach when making these enquiries. Comments such as “It can be difficult to remember to take tablets. How many doses do you think you miss?” are more likely to lead to an open, positive discussion with the patient than accusatory remarks such as “You haven’t been taking your drugs, have you?” (see ![]() 11 – NICE Clinical Guideline 76 Medicines Adherence).
11 – NICE Clinical Guideline 76 Medicines Adherence).
Devices such as tablet organisers or smartphone reminders can be helpful for patients who forget to take their tablets. It may be more challenging if patients make a deliberate decision not to take their medication. Switching to another drug or class may encourage concordance if the patient is concerned about side effects. The faculty also considered that visual demonstration of CV risk on calculators such as JBS2 (![]() 4) or QRISK (
4) or QRISK (![]() 5) computer risk devices may be helpful in encouraging future concordance.
5) computer risk devices may be helpful in encouraging future concordance.
Maximising medication
Most patients need combination therapy with two or more antihypertensive drugs if they are to reach their target blood pressure.24,25 The faculty agreed on the importance of maximising medication but noted that side effects or complicated drug regimens may undermine concordance. While it may be appropriate to uptitrate to a more effective dose of the current medication, the faculty also recommended considering low doses of several drugs for patients who are particularly sensitive to side effects. Similarly, choosing fixed-dose combination preparations or drugs with once- or twice-daily dosing can help to simplify treatment regimens. Cost may also be an issue for younger patients who are not in receipt of free prescriptions.
According to the faculty, it may also be helpful to switch to another class of antihypertensive drug. Blood pressure may improve, for example, if patients switch from an ACE inhibitor to an ARB, or vice versa, since individuals respond differently to these classes of drug.26 An alternative strategy highlighted by the faculty is to switch to a more effective antihypertensive agent within the same class. Of the diuretics, for example, chlortalidone may be more effective than hydrochlorothiazide in lowering blood pressure.27 ARBs also differ in their potency. At their current standard doses, newer ARBs such as irbesartan, candesartan, olmesartan and telmisartan have been shown to lower blood pressure more effectively than losartan and valsartan at comparable doses.28 More recently, studies have shown that azilsartan medoxomil, the most recent ARB, is more effective at lowering clinic and ambulatory blood pressure than either the ACE inhibitor ramipril or the ARBs, olmesartan and valsartan, in patients with primary hypertension when compared at their
maximal doses.29-31
The faculty recognised that this approach may be challenging in areas where use of ARBs is still discouraged on perceived grounds of high cost despite the updated 2011 NICE/BHS guideline and the fact that many ARBs are now available generically. In the opinion of the faculty, discouragement of ARB use may not be cost saving in the longer term, especially when lower QOF blood pressure targets are introduced. The faculty considered that it may be helpful to share information with local colleagues on comparative potency of these agents in enabling more patients to achieve clinical targets and reduce their cardiovascular risk. A key challenge for primary care is to reduce the number of unplanned admissions and reducing cardiovascular risk could help achieve this.
Resistant hypertension
According to the NICE/BHS 2011 guideline, hypertension is truly resistant when blood pressure remains uncontrolled to <140/90 mmHg despite treatment with at least optimal or best-tolerated doses of Step 3 treatment (i.e. ACE inhibitor or ARB plus CCB plus thiazide-like diuretic).1 Device-based therapies, such as renal denervation, are emerging as an option for patients with resistant hypertension. Before considering such an interventional procedure or referral to secondary care, UK guidelines recommend that patients should have confirmed sustained systolic blood pressure ≥160 mmHg on CBPM, and >150 mmHg daytime average on ABPM (>150 mmHg CBPM and >140 mmHg ABPM for patients with diabetes).32
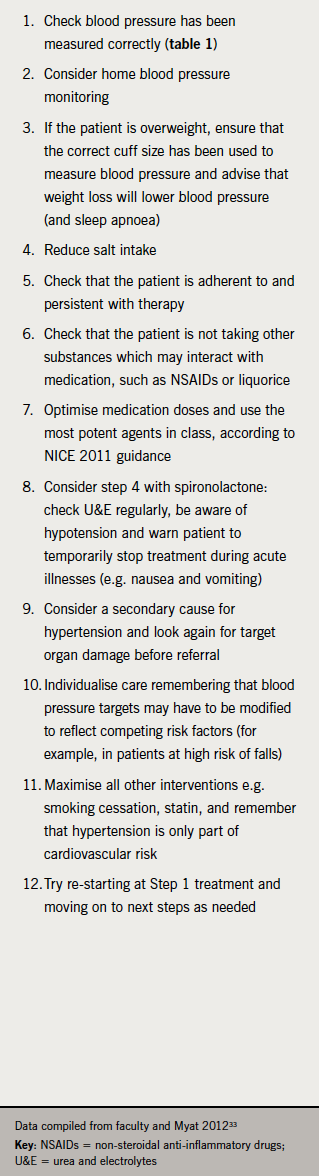
In addition, because patients in trials of renal denervation were taking an average of five medications before intervention or referral, all patients should have tried medical therapy, up to and including Step 4 of the NICE/BHS 2011 guideline (figure 4), with additional diuretic therapy.32 In light of these consensus recommendations and the challenges discussed above, the faculty recommended adopting the pathway demonstrated in table 7
to exclude alternative explanations for resistant hypertension.
Insufficient medical therapy is the most common reason for apparently resistant hypertension.34 According to the faculty, this ‘pseudoresistance’ can be addressed, first, by ensuring that the patient is concordant with medication, and then by optimising medication by adjusting the dose, adding in additional therapies and using the most effective drugs in a particular class. Similarly, ensuring that ABPM has been administered correctly will help to rule out ‘white coat’ hypertension in many patients. For example, a study using data from the Spanish Ambulatory Blood Pressure Monitoring Registry found that of 8,295 patients with resistant hypertension on clinic readings, 37.5% had white coat hypertension on ABPM.35 Finally, since 10% of patients have secondary hypertension,1 a thorough medical history and examination is essential to ensure that uncontrolled blood pressure is not caused or exacerbated by other diseases or drugs.
Referral options
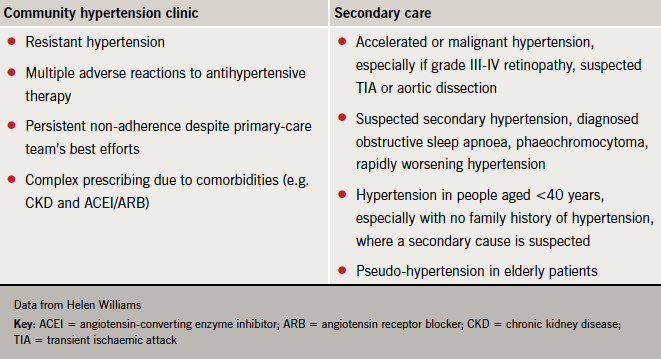
Table 8 outlines indications for referral suggested by the faculty. In some areas it may be possible to refer patients to community hypertension clinics run by GPs with a Special Interest or community pharmacists. These facilities can not only deal with much of the workload involved in identifying patients with truly resistant hypertension but can also manage other challenging patients.18
Future developments
Initiatives are now underway that could help to support practices in meeting the challenges of managing primary hypertension, including more stringent QOF audit standards.
A patient decision aid relating to the NICE/BHS 2011 guideline is being developed in co-operation with the Department of Health. By taking patients step-by-step through the effects of high blood pressure, and the role of lifestyle measures and drug treatment in improving outcomes, the aim is to help patients to make an informed decision about their treatment that may help to improve their concordance. According to the faculty, similar motivating information could also be provided by universal adoption of lifetime risk calculation, which may be recommended by the Joint British Societies in their next guidelines (JBS3).
Preparations for a UK ABPM hypertension register are also in their early stages. Such registers already exist in Ireland and Spain, where they enable the collection of more accurate retrospective data that has helped, for example, to identify patients with truly resistant hypertension.35 The system used in Ireland also makes it possible to produce an online summary report that can be discussed with each patient during the consultation – again, offering a tool that could potentially improve concordance so that more patients can achieve the clinical targets in the new NICE 2011 hypertension guideline.
Revalidation
If you would like to reflect on what you have learned from this supplement and use it towards your revalidation activities, that can be done at the bottom of this page.
Box 1. South of England
 Regional prescribing data* suggest that the 2011 NICE/BHS hypertension guideline is being implemented. Since 2009, there has been an approximately 11% decline in diuretic prescribing, while CCB prescribing has increased by about 4% and ACE inhibitor and ARB prescribing by 5% each. However, despite NICE guidance and the availability of generic ARBs, there has been no significant change since 2009 in the prescribing ratio between ACE inhibitor and ARB with about 2.5 times more ACE inhibitor prescribing, which probably reflects previous efforts to curtail prescribing costs.
Regional prescribing data* suggest that the 2011 NICE/BHS hypertension guideline is being implemented. Since 2009, there has been an approximately 11% decline in diuretic prescribing, while CCB prescribing has increased by about 4% and ACE inhibitor and ARB prescribing by 5% each. However, despite NICE guidance and the availability of generic ARBs, there has been no significant change since 2009 in the prescribing ratio between ACE inhibitor and ARB with about 2.5 times more ACE inhibitor prescribing, which probably reflects previous efforts to curtail prescribing costs.
The local Clinical Commissioning Group’s focus on the 2011 hypertension guideline, especially during health checks, is identifying many patients with Stage 1 hypertension. This had led to an expanding role for ABPM, which is increasingly being administered by community pharmacists. Locally, the next challenge is to ensure that patients are taking optimal tolerated therapy. In one practice for example, two-fifths of patients are receiving monotherapy, which may represent an under-treated group, who might need to be moved to Step 2 combination therapy to achieve their NICE/BHS target blood pressures.
*Courtesy of the Associate Director of Medicines Management, Southampton, Hampshire, Isle of Wight and Portsmouth PCT Cluster
Box 2. York
 By contrast, data from York suggest little uniformity of approach, and it appears that NICE guidelines are not optimally followed. In some cases, patients are started on inappropriate treatment – for example, some patients have been started on a diuretic at Step 1. Locally, there have been delays in obtaining ABPM devices, but now most practices will offer this test to confirm a diagnosis of hypertension or monitor response to treatment. There has been a comprehensive training scheme for the clinical staff who will be fitting the devices. This is important, since in the past, where ABPM has been used, technical problems have led to a high number of repeat tests, thus becoming much less cost effective. Using ABPM also appears to have led to fewer patients being offered treatment, and there is no clear follow-up for those who have proven white coat hypertension, who remain at increased risk.
By contrast, data from York suggest little uniformity of approach, and it appears that NICE guidelines are not optimally followed. In some cases, patients are started on inappropriate treatment – for example, some patients have been started on a diuretic at Step 1. Locally, there have been delays in obtaining ABPM devices, but now most practices will offer this test to confirm a diagnosis of hypertension or monitor response to treatment. There has been a comprehensive training scheme for the clinical staff who will be fitting the devices. This is important, since in the past, where ABPM has been used, technical problems have led to a high number of repeat tests, thus becoming much less cost effective. Using ABPM also appears to have led to fewer patients being offered treatment, and there is no clear follow-up for those who have proven white coat hypertension, who remain at increased risk.
Locally, there are no plans to commission a hypertension service. Although there is a need to reduce referrals to secondary care, there is also no local pathway that includes advice on the investigation and management of resistant hypertension. This is an important issue, since many of these patients have multiple co-morbidities and it can be difficult to decide whether to refer them to renal, cardiology or endocrine secondary care services.
Box 3. Scotland
 In Scotland as a whole, the number of prescribed items for diseases of the cardiovascular system (British National Formulary Group 2) rose from <18 million in 2002 to >24 million in 2011, but the cost has remained approximately the same due to increasing availability of generic versions of recommended drugs.
In Scotland as a whole, the number of prescribed items for diseases of the cardiovascular system (British National Formulary Group 2) rose from <18 million in 2002 to >24 million in 2011, but the cost has remained approximately the same due to increasing availability of generic versions of recommended drugs.
There is no specific Scottish Intercollegiate Guideline Network (SIGN) hypertension guideline, so practices are encouraged to follow the NICE guideline. The SIGN 97 guideline on prevention of cardiovascular disease endorses the previous JBS 2/BHS guidance on targets and the A/CD algorithm. There are, however, wide variations between health boards in use of all classes of antihypertensive drug. For example, NHS Western Isles is the highest user of ARBs with the relative number of defined daily doses being 160* – double the amount of the lowest user, NHS Lothian. Prescribing of thiazide diuretics remains high, with low-dose bendroflumethiazide the most commonly prescribed antihypertensive medication in Scotland. A study is planned that involves substitution of bendroflumethiazide with chlortalidone, but it has yet to get underway.
*Data courtesy of Information Services Division, Scotland. Comparisons are based on the ‘defined daily dose’ – the assumed average maintenance dose of a drug per day and a proxy measure for the number of patients taking the drug.
Take home messages
- Hypertension is the most common cardiovascular risk factor condition and its diagnosis, treatment and management are a significant part of primary care workload
- While more people are being treated for hypertension, the numbers of people with uncontrolled blood pressure remain largely unchanged, and many people still remain undiagnosed
- This persisting burden of hypertension results in part from non-concordance, medication intolerance, undiagnosed secondary causes, white coat and true resistant hypertension
- Clear messages about diagnosis and treatment are needed to help support primary care to implement current guidance
- Audit can help identify where practices are not following guidance and can provide the support and encouragement to implement current guidelines. It can also identify people newly diagnosed in private practice
- More effective strategies need to be developed to identify patients not already diagnosed who would benefit from treatment
- ABPM and HBPM are useful tools for accurate diagnosis
- Uniform coding of patients at practice level is required. Patients with ‘primary’ hypertension need to be identified as such and differentiated from those with raised blood pressure who are in disease categories that can be considered end organ damage (vascular disease) or high-risk category for vascular damage (diabetes) where the targets and audit standard for treatment are more stringent
- There is a trend towards more rational prescribing in line with the NICE/BHS ACD algorithm
- Reluctance and barriers to the use of newer agents need to be addressed at clinical and medicine management levels
- Efforts should be made to address non-adherence, including identifying and addressing any underlying health beliefs
- A check list for those people who are thought to have resistant hypertension is a useful tool to help identify those who truly do have drug-resistant hypertension and to reduce unnecessary referrals
- There remains a case for development of new medicines and interventions to address these needs
- The introduction of new lower QOF targets for hypertension in England and Wales will help prevent more heart attacks and stroke
- Successful treatment of hypertension requires a partnership between educated and motivated clinicians to educate and motivate patients
Conflict of interest
Dr Chris Arden has received honoraria for advisory boards and speaker’s fees from Boehringer Ingelheim, Merck Sharp & Dohme, Pfizer and Takeda. Dr Alan Begg has received honoraria and educational grants from Bayer, Boehringer Ingelheim, Merck Sharp & Dohme, Pfizer, Roche and Takeda. Professor Mark Caulfield has been a member of the NICE Guideline Development Group and a past President of British Hypertension Society, where he has held various offices. He is on the Council of the European Society of Hypertension and currently chairs a group developing a Hypertension Patient Decision Aid for the Department of Health. He has received honoraria from Medtronic, Novartis and Takeda, and has undertaken research with Ardian/Medtronic, the British Heart Foundation, Servier and Takeda. Dr Kathryn Griffith has received honoraria for educational work from Boehringer Ingelheim and Roche. Dr Terry McCormack is a member of the NICE Guideline Development Group and Topic Expert Group, and Secretary of the British Hypertension Society. He has received research grants, educational grants and advisory board honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi-Sankyo, Menarini, Medtronic, Merck Sharp & Dohme, Roche Diagnostics, Servier and Takeda. Ms Helen Williams has received an honorarium from Takeda.
References
- National Clinical Guideline Centre (NCGC). Hypertension: the clinical management of primary hypertension in adults. Clinical Guideline 127. Methods, evidence and recommendations. August 2011. Commissioned by the National Institute for Health and Clinical Excellence. London: NCGC, 2011. Available at http://www.nice.org.uk/nicemedia/live/13561/56007/56007.pdf (accessed 1 December 2012).
- National Statistics. Health Service for England 2010—trend tables. NHS Information Centre 2011. Available at http://www.ic.nhs.uk/statistics-and-data-collections/health-and-lifestyles-related-surveys/health-survey-for-england/health-survey-for-england–2010-trend-tables (accessed 1 December 2012).
- Williams B. Hypertension and “J-curve”. J Am Coll Cardiol 2009;54:1835–6. http://dx.doi.org/10.1016/j.jacc.2009.06.043
- MeRec Bulletin. The management of hypertension in primary care: updated guidance from NICE. MeRec Bulletin 2006;17(1 part 2).
- North of England Hypertension Guideline Development Group. Essential hypertension: managing adults in primary care. Clinical Guideline 18. Newcastle: August 2004. Available at http://www.guidance.nice.org/uk/CG18 (accessed 24 January 2013).
- National Collaborating Centre for Chronic Conditions. Hypertension: management of hypertension in adults in primary care: partial update. London: Royal College of Physicians, 2006. Available at http://www.nice.org.uk/nicemedia/pdf/CG34fullguideline.pdf (accessed 3 December 2012).
- National Institute for Health and Clinical Excellence (NICE). How NICE clinical guidelines are developed: an overview for stakeholders, the public and the NHS (4th edition). January 2009. London: NICE, 2009. Available at http://www.nice.org.uk/media/62F/36/How_NICE_clinical_guidelines_are_developed
_4th_edn_FIANL_LR.pdf (accessed 1 December 2012). - Laine C, Taichman DB, Mulrow C. Trustworthy clinical guidelines. Ann Intern Med 2011;154:774–5.
- Oparil S (chair of JNC8) speaking at the European Society of Hypertension Annual Scientific Meeting, London, 2012.
- Lovibond K, Jowett S, Barton P, et al. Cost-effectiveness of options for the diagnosis of high blood pressure in primary care: a modelling study. Lancet 2011;378:1219–30. http://dx.doi.org/10.1016/S0140-6736(11)61184-7
- Gustavsen PH, Hoegholm A, Bang LE, Kristensen KS. White coat hypertension is a cardiovascular risk factor: a 10-year follow-up study. J Hum Hypertens 2003;17:811–17. http://dx.doi.org/10.1038/sj.jhh.1001643
- National Institute for Health and Clinical Excellence. Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. May 2008 (reissued March 2010). London: NICE, 2008. Available at http://www.nice.org.uk/CG67 (accessed 1 December 2012).
- Spinar J, Vitovec J, Soucek M, Dusek L, Pavlik T, Investigators CORD. CORD: COmparison of Recommended Doses of ACE inhibitors and angiotensin II receptor blockers. Vnitrni Lekarstvi 2009;55(5):481–8.
- Tedesco MA, Natale F, Calabro R. Effects of monotherapy and combination therapy on blood pressure control and target organ damage: a randomized prospective intervention study in a large population of hypertensive patients. J Clin Hypertens 2006;8(9):634–41. http://dx.doi.org/10.1111/j.1524-6175.2006.05504.x
- Yusuf S, Teo K, Pogue J, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008;358:1547–59. http://dx.doi.org/10.1056/NEJMoa0801317
- Beckett NS, Peters R, Fletcher AE, et al., HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008;358:1887–98. http://dx.doi.org/10.1056/NEJMoa0801369
- British Medical Association/NHS Employers. Quality and Outcomes Framework for 2012/13. Guidance for PCOs and practices. 2012. Available at http://www.nhsemployers.org/Aboutus/Publications/Documents/QOF_2012-13.pdf (accessed 2 December 2012).
- Williams H (personal communication).
- National Institute for Health and Clinical Excellence. Summary of recommendations for the NICE menu and recommendations for retirement of indicators. August 2012. London: NICE, 2012. Available at http://www.nice.org.uk/media/1E3/79/QOFACJune12SummaryRecommendations.pdf (accessed 1 December 2012).
- NHS Information Centre. The Quality and Outcomes Framework. Available at http://www.ic.nhs.uk/statistics-and-data-collections/audits-and-performance/the-quality-and-outcomes-framework (accessed 5th December 2012).
- Health and Social Care Information Centre: Quality and Outcomes Framework 2011–12, practice level: clinical domain, hypertension data tables. Health and Social Care Information Centre 2012. Available from http://www.ic.nhs.uk/article/2021/Website-Search?productid=9587&q=qof+data+2010%2f11&sort=Relevance&size=10&page=2&area
=both#top (accessed 7 January 2013). - NHS Business Services Authority. NHS Prescription Services. Cardiovascular system national charts. NHS Business Services Authority, 2012. Available from http://www.nhsbsa.nhs.uk/PrescriptionServices/Documents/PPDPrescribingAnalysis
Charts/Cardio_National_Sep_2012.pdf (accessed 7 January 2013). - Van Wijk BL, Klungel OH, Heerdink ER, de Boer A. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens 2005;23:2101–7. http://dx.doi.org/10.1097/01.hjh.0000187261.40190.2e
- Wald N, Law M, Morris J. Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy. HTA 2003;7:1–94. Available from http://www.hta.ac.uk/execsumm/summ731.htm (accessed 7 January 2013).
- Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11,000 participants from 42 trials. Am J Med 2009;122:290–300. http://dx.doi.org/10.1016/j.amjmed.2008.09.038
- Johnson A, Stafylas P, Stergiou GS. Effectiveness, safety and cost of drug substitution. Br J Clin Pharmacol 2010;70:321–34. http://dx.doi.org/10.1111/j.1365-2125.2010.03681.x
- Ernst ME, Carter BL, Goerdt CJ, et al. Comparative antihypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension 2006;47:352–8. http://dx.doi.org/10.1161/01.HYP.0000203309.07140.d3
- Asmar R. Targeting blood pressure control with angiotensin receptor blockers. Int J Clin Pract 2006;60:315–20. http://dx.doi.org/10.1111/j.1368-5031.2006.00784.x
- Bakris GL, Sica D, Weber M, et al. The comparative effects of azilsartan medoxomil and olmesartan on ambulatory and clinic blood pressure. J Clin Hypertens (Greenwich) 2011;13:81–8. http://dx.doi.org/10.1111/j.1751-7176.2010.00425.x
- Sica D, White WB, Weber MA et al. Comparison of the novel angiotensin II receptor blocker azilsartan medoxomil vs valsartan by ambulatory blood pressure monitoring. J Clin Hypertens (Greenwich) 2011;13:467–72. http://dx.doi.org/10.1111/j.1751-7176.2011.00482.x
- White WB, Weber Ma, Sica D, et al. Effects of the angiotensin receptor blocker azilasartan medoxomil versus olmesartan and valsartan on ambulatory and clinic blood pressure monitoring in patients with stages 1 and 2 hypertension. Hypertension 2011;56:413–20. http://dx.doi.org/10.1161/HYPERTENSIONAHA.110.163402
- Caulfield M, De Belder M, Cleveland T, et al. The Joint British Societies’ consensus statement on renal denervation for resistance hypertension. January 2012. Available at http://www.bcs.com/documents/The_Joint_UK_Societies_Consensus_on_Renal_
Denervation_for_resistant_hypertension.pdf (accessed 1 December 2012) - Myat A, Redwood SR, Qureshi AC, Spertus JA, Williams B. Resistant hypertension. BMJ 2012;345:e7473. http://dx.doi.org/10.1136/bmj.e7473
- Tobe SW, Lewanczuk R. Resistant hypertension. Can J Cardiol 2009;25:315–17. http://dx.doi.org/10.1016/S0828-282X(09)70496–9
- De la Sierra A, Segura J, Banegas JR, et al. Clinical features of 8,295 patients with resistant hypertension classified on the basis of ambulatory blood pressure monitoring. Hypertension 2011;57:898–902. http://dx.doi.org/10.1161/HYPERTENSIONAHA.110.168948
