Patients with amyloid heart disease have historically been considered to have a very poor prognosis and were considered almost untreatable. However, recent therapeutic advances are encouraging and likely to have a marked effect on management across the amyloid spectrum. This message needs to be conveyed to cardiologists, not least because there is now benefit to performing an endomyocardial biopsy to determine amyloid type. We provide an update on the significant progress in managing the three most common forms of amyloid heart disease in the UK.
Our objective was to compare the performance of computed tomography coronary angiography (CTCA) with exercise tolerance testing (ETT) in patients presenting with stable chest pain with low-to-intermediate predicted risk of coronary artery disease (CAD) as defined by the UK National Institute for Health and Care Excellence (NICE) clinical guideline 95. We investigated 85 patients with ETT and 102 patients with CTCA as first-line investigations after clinical assessment. Outcome measures assessed were diagnosis or exclusion of CAD, referral for second-line investigations, false-positive rate and cost of investigation to reach diagnosis for each modality.
CTCA was diagnostic in more patients than ETT (95.1% vs. 80.0%, p<0.05), had a lower false-positive rate (2.9% vs. 17.6%), led to fewer referrals for second-line investigations (4.9% vs. 21.2%, p<0.05) and resulted in overall comparable cost of investigation per patient (£183.44 vs. £165.16, p=0.49).
In conclusion, CTCA outperforms ETT as a first-line investigation in the investigation of patients presenting with stable chest pain with low-to-intermediate predicted risk of CAD as defined by NICE clinical guideline 95.
Introduction
For many years, the exercise tolerance test (ETT) has been the first-line investigation in patients presenting with stable chest pain. However, equivocal and false-positive results often lead to additional investigations. In recent years, computed tomography (CT) coronary angiography (CTCA) has been demonstrated to have excellent negative predictive value, making it a useful test to rule out obstructive coronary artery disease (CAD).1-3
In 2010, the UK National Institute for Health and Care Excellence (NICE) published clinical guideline 95: ‘Chest pain of recent onset’. This guideline advocates the use of a new risk estimation of CAD (CADScore); a calculation based on age, gender, nature of chest pain and cardiovascular risk factors using a modification of the Diamond Forrester criteria.4 The guideline recommends selecting the first-line investigation according to this calculated score: if CADScore 10–29%, CT calcium scoring ± CTCA is recommended; if CADScore 30–60%, functional imaging is recommended; if CADScore 61–90%, invasive coronary angiography (ICA) is recommended.5
Our experience is that the majority of patients presenting with stable chest pain are ultimately diagnosed with non-cardiac chest pain. A previous audit in our local area (from 2009 to 2010) of 401 consecutive patients presenting with stable chest pain, documented an overall incidence of 13.2% CAD requiring treatment (percutaneous coronary intervention [PCI], coronary artery bypass grafting [CABG] or medical therapy).6 The incidence in the low predicted risk subgroup (CADScore 10–29%) was 4.8%. In the intermediate predicted risk subgroup (CADScore 30–60%) the incidence was 6.4%.
In contrast with NICE clinical guideline 95, the current joint American College of Cardiology (ACC)/American Heart Association (AHA) guidelines7 recommend CTCA for the investigation of patients with stable chest pain and both low and intermediate predicted risk. In this study we compared the previous standard of care (ETT) with CTCA in patients with stable chest pain and low-to-intermediate predicted risk as determined by CADScore.
Methods
Patients
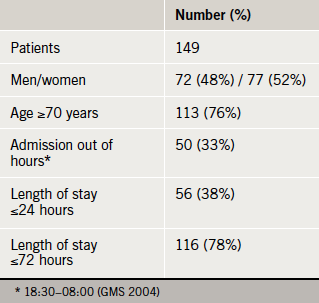
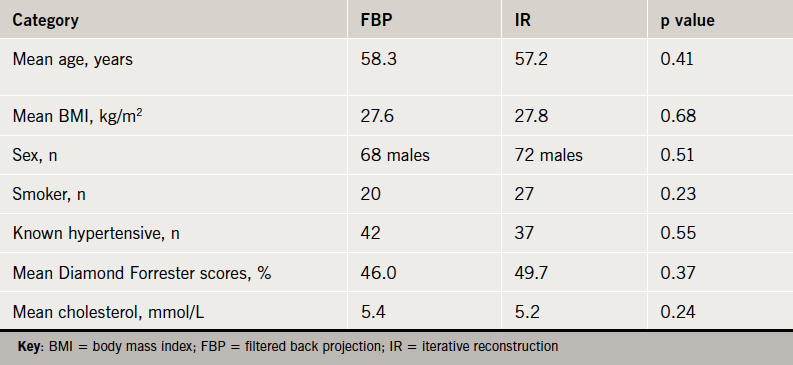
Two cohorts of consecutive patients presenting with stable chest pain were retrospectively compared. The first cohort consisted of patients referred for ETT as a first-line investigation over a six-month period, as per standard of care prior to introduction of CTCA in our hospital. The second cohort of consecutive patients consisted of patients referred for CTCA as a first-line investigation over a further six-month period, after the introduction of CTCA in our hospital. Each patient was retrospectively risk assessed according to NICE clinical guideline 95, and a CADScore was calculated. Only those with low-to-intermediate predicted risk (CADScore 10–60%) were included in this analysis: 85 patients from the first cohort (ETT) and 102 patients from the second cohort (CTCA). Baseline patient characteristics and statistical comparison of the two cohorts are summarised in table 1. Patients were followed until conclusion of investigations and final diagnosis was reached. Three patients in the ETT cohort did not complete their investigations and were lost to follow-up.
Table 1. Baseline patient characteristics
The exercise tolerance test
Bruce protocol was employed according to our hospital guidelines. The target heart rate (HR) was calculated as 85 × (220 – age). The test was terminated when the target HR was reached or the patient developed persistent chest pain and/or a shift in the ST segment of 1 mm in one or more leads.
Second-line investigations
Patients with a positive ETT were referred for ICA. Patients in whom target HR was not achieved, or in whom the test was considered equivocal, were further investigated with a functional test (stress echocardiography or nuclear myocardial perfusion stress test) and/or ICA as per standard clinical practice. Significant CAD found during ICA was defined as ≥70% diameter stenosis of at least one major epicardial coronary artery segment or ≥50% diameter stenosis in the left main coronary artery.
CTCA
Patients were either previously orally beta-blocked by the referring clinician and/or were intravenously beta-blocked with intravenous metoprolol (5–30 mg) aiming to achieve a heart rate of <60 bpm. All patients received two 400 µg doses of sublingual glycerol trinitrate. For the contrast part of the scan, 100 ml of loversol (Optiray 350 mg/ml, Covidien UK, Hampshire, UK), at a flow rate of 5 ml/s followed by 100 ml of saline solution, were injected into an antecubital vein via an 18-gauge peripheral venous catheter. Bolus tracking was used with a region of interest placed into the ascending aorta.
All CTCA were performed with a 64-slice LightSpeed VCT XTe GE scanner (GE Healthcare) and prospective gating. Using the commercially available protocol (SnapShot Pulse, GE Healthcare) and the following scanning parameters: slice acquisition 64 × 0.625 mm, selected field of view (SFOV) Cardiac, Z-axis detector coverage 40 mm, gantry rotation time of 350 ms. Patients’ size was visually judged for adapted tube voltage; 100 kV was used for small patients, 120 kV for average size patients, and two very large patients required 140 kV. Similarly, effective tube-current ranged between 500 mA and 650 mA based on patient’s size judged visually. A scout scan was followed by a prospectively gated calcium score scan. If the calcium score was >400, the CTCA was not performed and the patient was referred for an alternative investigation. Otherwise, the CTCA was performed from below the tracheal bifurcation to the diaphragm to just below the inferior border of the heart, with displayed field of view (DFOV) of 25 cm. By choosing the smallest possible window and limiting the acquisition to the 75% end-diastolic phase of the RR-cycle, we lowered the dose as much as possible. The effective radiation dose of CTCA was calculated as the product of the dose-length product (DLP) times a conversion factor coefficient for the chest (κ=0.014 mSv/mGy·cm). CTCA images were reconstructed with slice thickness of 0.625 mm, using a medium-soft tissue convolution kernel (standard). All images were transferred to an external workstation (ADW 4.5, GE Healthcare) for analysis.
Second-line investigations
Patients in whom CTCA demonstrated severe coronary artery stenoses (defined as >70% luminal narrowing) were referred for ICA. Patients in whom CTCA demonstrated moderate coronary artery stenoses (defined as 50–70% luminal narrowing) were referred for functional testing (stress echocardiography or nuclear myocardial perfusion stress test) and/or ICA. Functional imaging test was considered positive if there was significant ischaemia (≥10% myocardial ischaemia by nuclear perfusion imaging or ≥3 segments ischaemia on stress echocardiography). Significant CAD found during ICA was defined as ≥70% diameter stenosis of at least one major epicardial artery segment or ≥50% diameter stenosis in the left main coronary artery.
Statistical methods
Statistical analysis was performed with SPSS version 18.0 for Windows.
Cost analysis
The total cost of investigation to reach diagnosis was calculated for each patient based on the pricing scheme recommended in the NICE ‘Chest Pain of Recent Onset’ costing report 2011 (£75 for ETT and £173 for CTCA).8 If the first-line test was positive (i.e. >70% luminal narrowing on CTCA or positive ETT) and subsequent ICA confirmed obstructive CAD, then the cost of ICA was not included in the cost of investigation.
Results
Results were analysed by cohort (ETT or CTCA). Within each cohort, analysis was also performed in two subgroups defined by predicted risk: low predicted risk (CADScore 10–29%) and intermediate predicted risk (CADScore 30–60%).
ETT cohort
A total of 85 patients were referred for ETT as first-line investigation. ETT was reported as negative in 72.9%, positive in 7.1% and equivocal in 20.0% of patients. There were 11.8% of patients referred for second-line functional testing and 5.9% were referred for second-line ICA. Eventually, 4.7% of patients were confirmed to have obstructive CAD requiring treatment (PCI, CABG or medical therapy).
In the low predicted risk subgroup (CADScore 10–29%), ETT was reported as negative in 79.2%, positive in 8.3% and equivocal in 12.5% of patients. There were 8.3% of patients referred for second-line functional testing and 0% were referred for second-line ICA. Eventually, 4.2% of patients were confirmed to have obstructive CAD requiring treatment (PCI, CABG or medical therapy).
In the intermediate predicted risk subgroup (CADScore 30–60%), ETT was reported as negative in 70.5%, positive in 6.6% and equivocal in 23.0% of patients. There were 13.1% of patients referred for second-line functional testing and 8.2% were referred for second-line ICA. Eventually, 4.9% of patients were confirmed to have obstructive CAD requiring treatment (PCI, CABG or medical therapy).
CTCA cohort
A total of 102 patients were referred for calcium scoring ± CTCA as first-line investigation. The scan was performed without complication in all patients. Calcium scoring was performed in all but four patients, who were young, to minimise radiation dose. There were 2.9% of patients with a calcium score >400, who did not proceed to the contrast phase and were referred for alternative investigations (functional testing or ICA). Because of data from the Coronary Artery Evaluation Using 64-Row Multidetector Computed Tomography Angiography (CORE64) trial6 and Coronary CT Angiography Evaluation for Clinical Outcomes (CONFIRM) registry,7 which documented the presence of obstructive CAD in patients with zero calcium score, we elected to perform the contrast phase of the scan in all patients. Using the heart rate control measures described above, we were able to perform prospective gated studies in 97.8% of patients. Overall, this resulted in mean radiation dose of 3.19 ± 1.45 mSv per patient.
Calcium score
Overall, 70.6% of patients had zero calcium score. By subgroup, 73.1% of patients with low predicted risk (CADScore 10–29%) and 68.0% with intermediate predicted risk (CADScore 30–60%) had zero calcium score. Overall, 2.0% of patients had a calcium score >400 (0% in those with low predicted risk and 4.0% of those with intermediate predicted risk). A further 22.5% of patients had calcium score 1–400 (21.2% of those with low predicted risk and 24.0% of those with intermediate predicted risk).
Overall, the contrast phase of the scan demonstrated unobstructed coronary arteries in 92.1%, moderate stenoses in 1.0% and severe stenoses in 4.9% of patients (2.0% of patients did not proceed to the contrast phase of the scan because their calcium score was >400). There were 4.9% of patients referred for second-line functional testing and 0% were referred for second-line ICA. Eventually, 2.9% of patients were confirmed to have obstructive CAD requiring treatment (PCI or CABG).
In the low predicted risk subgroup (CADScore 10–29%), CTCA demonstrated unobstructed coronary arteries in 96.2%, moderate stenoses in 0% and severe stenoses in 3.8% of patients. There were 0% of patients referred for second-line functional testing and 0% were referred for second-line ICA. Eventually, 3.8% of patients were confirmed to have obstructive CAD requiring treatment (PCI or CABG).
In the intermediate predicted risk subgroup (CADScore 30–60%), CTCA demonstrated unobstructed coronary arteries in 88.0%, moderate stenoses in 2.0% and severe stenoses in 6.0% of patients. There were 4.0% of patients who did not have the contrast phase performed because their calcium score was >400 and were referred for alternative investigations (functional testing or ICA). There were 10.0% of patients referred for second-line functional testing and 0% were referred for second-line ICA. Eventually, 4.0% of patients were confirmed to have obstructive CAD requiring treatment (PCI or CABG).
CTCA vs. ETT
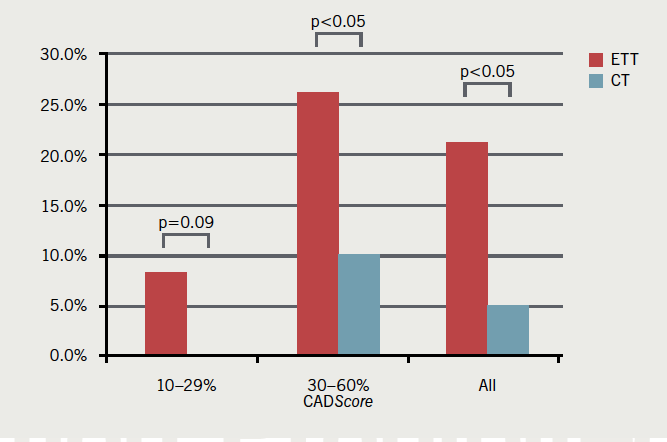
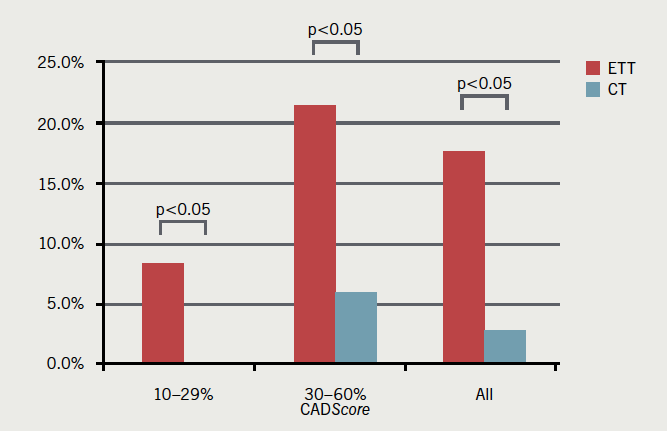
As a first-line investigation, CTCA was diagnostic in more patients than ETT (95.1% vs. 80.0%, p<0.05). False-positive rates were calculated after invasive angiography. CTCA had a lower false-positive rate (2.9% vs. 17.6%). CTCA resulted in fewer referrals than ETT for second-line investigations (4.9% vs. 21.2%, p<0.05). These results are summarised in table 2 and figures 1–3.
Table 2. Comparison of the performance of computed tomography coronary angiography (CTCA) versus exercise tolerance testing (ETT)
Figure 1. Percentage of patients in whom the first-line investigation was diagnostic (CTCA vs. ETT)
Figure 2. Referrals for second-line investigations after CTCA and ETT
Figure 3. False-positive rates for CTCA and ETT
In the low predicted risk subgroup (CADScore 10–29%), CTCA was diagnostic in more patients than ETT (100% vs. 87.5%, p<0.05) and had a lower false-positive rate (0% vs. 8.3%). CTCA resulted in fewer referrals than ETT for second-line investigations (0% vs. 8.3%, p=0.09).
In the intermediate predicted risk subgroup (CADScore 30–60%), CTCA was diagnostic in more patients than ETT (90.0% vs. 77.0%, p=0.07) and had a lower false-positive rate (6.0% vs. 21.3%). CTCA resulted in fewer referrals than ETT for second-line investigations (10.0% vs. 26.2%, p<0.05).
Cost analysis
Despite the higher cost of CTCA compared with ETT, overall mean cost per patient was not significantly higher in the CTCA cohort (£183.44 vs. £165.16, p=0.49). In the low predicted risk subgroup (CADScore 10–29%) mean cost per patient was 86.6% higher (£173.00 vs. £92.75, p<0.05), but In the intermediate predicted risk subgroup (CADScore 30–60%), mean cost per patient was only 0.3% higher (£193.66 vs. £194.30, p=0.98). These results are summarised in figure 4.
Figure 4. Mean cost per patient for CTCA and ETT
Study limitations
One limitation of this study is the comparison of two different cohorts of patients. However, statistical comparison of the two cohorts confirms very similar age, gender divide and burden of cardiovascular risk factors (table 1). CADScores were calculated retrospectively using clinical information gathered at the time of first presentation and so were potentially subject to error with regards to description of symptoms. However, all other elements of the CADScore were obtained from objective records (e.g. measured blood pressure, fasting glucose and serum cholesterol levels). Another potential limitation of this study is that not all patients with negative CTCA underwent ICA, which is considered the gold-standard test to rule out CAD. However, Maffei et al.9 demonstrated CTCA to be superior to ETT when compared with ICA in a similar low-to-intermediate predicted risk cohort (all patients underwent all three tests). The sensitivity, specificity, positive and negative predictive values for CTCA compared with ICA were, respectively, 100%, 98.7%, 92.9% and 100% compared with 46.2%, 16.6%, 8.7% and 64.1% for ETT. The prevalence of significant CAD (defined as >50% stenoses) in that study was 14.7%, which is a little higher than in our data. Similarly, patients in our study with negative functional imaging tests did not undergo further investigation with ICA. Although there is a potential for false-negative results, this represents standard clinical practice across the UK.
Discussion
In the CT cohort we performed CTCA on all patients, including those with zero calcium score. Published data from the CORE64 trial10 and the CONFIRM registry11 demonstrated the presence of CAD in patients with zero calcium score. This is particularly true for patients under 40 years of age in whom soft plaque coronary atheroma has not yet developed calcifications. The literature on calcium scoring has mostly been validated in asymptomatic populations and its application to symptomatic patients (albeit with low likelihood of CAD) remains under debate.12 With good heart rate control and optimisation of scanning protocols, our results show that mean radiation dose from CTCA can be kept very low.
Most patients presenting with stable chest pain with low-to-intermediate predicted risk do not have obstructive CAD after investigation. CTCA has been shown to be an excellent rule out test for CAD in patients with normal coronary arteries. The current NICE guideline only recommends calcium scoring ± CTCA in patients with low predicted risk of CAD (CADScore 10–29%). These results suggest that CTCA is also superior to ETT in patients with intermediate predicted risk (CADScore 30–60%). In patients with low-to-intermediate predicted risk, CTCA was diagnostic in more patients and led to fewer second-line investigations compared with ETT. As a result, the mean cost per patient was comparable, despite the higher upfront cost of CTCA compared with ETT. Furthermore, had we not proceeded to the contrast phase of the scan in patients with zero calcium score, the cost could have been lower.
A multi-centre clinical trial comparing ETT with CTCA in patients with stable chest pain and a low-to-intermediate risk of CAD (CRESCENT) is under way in the Netherlands and will report in 2016.13 Several North American multi-centre trials (PROSPECT,14 RESCUE15 and PROMISE16) are under way, comparing standard care ± functional testing versus CTCA in patients with stable chest pain and low-to-intermediate cardiovascular risk, and will report over the next few years. Furthermore, the use of CTCA in the emergency room to rule out CAD in patients presenting with possible acute coronary syndromes has already been shown to reduce length of stay, reducing overall cost, compared with standard of care and single-photon emission computed tomography (SPECT) in three clinical trials from the USA.17-19 Ultimately, the goal is to reduce the number of patients with normal coronary arteries having invasive coronary angiography, which is reported at up to 39% at present.20
Conclusion
These results support our hypothesis that CTCA is a clinically useful, safe and cost-efficient diagnostic test in patients with both low and intermediate predicted risk of CAD. Based on these results, we support NICE recommendations that patients with low predicted risk (CADScore 10–29%) would be most effectively investigated with cardiac CT as a first-line test. Furthermore, as the incidence of CAD in the intermediate risk patients is low, we suggest that CTCA would also be effective in patients with intermediate predicted risk (CADScore 30–60%)
Conflict of interest
None declared.
Key messages
NICE guidance recommends risk assessment to direct choice of investigation in patients with stable chest pain
Computed tomography coronary angiography (CTCA) has excellent negative predictive value in both low and intermediate risk patients
CTCA leads to fewer second-line investigations than exercise tolerance testing (ETT), offsetting its higher upfront cost
Several randomised-controlled trials comparing CTCA with functional imaging tests are currently recruiting
References
Budoff MJ, Dowe D, Jollis JG et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for the evaluation of coronary artery stenoses in individuals without known coronary artery disease. Results from the prospective multicentre ACCURACY trial. J Am Coll Cardiol 2008;52:1724–32. http://dx.doi.org/10.1016/j.jacc.2008.07.031
Meijboom WB, Meijs MF, Schuijf JD et al. Diagnostic accuracy of 64 slice computed tomography coronary angiography: a prospective multicentre multivendor study. J Am Coll Cardiol 2008;52:2135–44. http://dx.doi.org/10.1016/j.jacc.2008.08.058
Min JK, Dunning A, Lin FY et al. CONFIRM Investigators. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter Registry) of 23,854 patients without known coronary artery disease. J Am Coll Cardiol 2011;58:849–60. http://dx.doi.org/10.1016/j.jacc.2011.02.074
Pryor DB, Shaw L, McCants CB et al. Value of the history and physical in identifying patients at increased risk for coronary artery disease. Ann Intern Med 1993;118:81–90. http://dx.doi.org/10.7326/0003-4819-118-2-199301150-00001
National Institute for Health and Clinical Excellence. Chest pain of recent onset – clinical guideline 95. London: NICE, 2010. Available from: http://www.nice.org.uk/CG95
Rogers T, Dowd D, Yap HL, Claridge S, Alfakih K, Byrne J. Strict application of NICE Clinical Guideline 95 ‘chest pain of recent onset’ leads to over 90% increase in cost of investigation. Int J Cardiol 2012;published online. http://dx.doi.org/10.1016/j.ijcard.2012.09.180
Taylor AJ, Cerqueira M, Hodgson JM et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR appropriate use criteria for cardiac computed tomography. Circulation 2010;122:e525–e555. http://dx.doi.org/10.1016/j.jacc.2010.07.005
Maffei E, Seitun S, Martini C et al. CT coronary angiography and exercise ECG in a population with chest pain and a low to intermediate pre-test likelihood of coronary artery disease. Heart 2010;96:1973–9. http://dx.doi.org/10.1136/hrt.2009.191361
Gottlieb I, Miller JM, Arbab-Zadeh A et al. The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography (CORE64). J Am Coll Cardiol 2010;55:627–34. http://dx.doi.org/10.1016/j.jacc.2009.07.072
Villines TC, Hulten EA, Shaw LJ et al. CONFIRM Registry Investigators. Prevalence and severity of coronary artery disease and adverse events among symptomatic patients with coronary artery calcification scores of zero undergoing coronary computed tomography angiography: results from the CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) registry. J Am Coll Cardiol 2011;58:2533–40. http://dx.doi.org/10.1016/j.jacc.2011.10.851
Clinicaltrials.gov. Computed tomography versus exercise testing in suspected coronary artery disease (CRESCENT). Available from: http://clinicaltrials.gov/ct2/show/NCT01393028 [accessed 25 February 2013].
Clinicaltrials.gov. Study comparing CT scan and stress test in diagnosing coronary artery disease in patients hospitalized for chest pain (PROSPECT). Available from: http://clinicaltrials.gov/ct2/show/NCT00705458 [accessed 25 February 2013].
Clinicaltrials.gov. Randomized evaluation of patients with stable angina comparing diagnostic examinations (RESCUE). Available from: http://clinicaltrials.gov/ct2/show/NCT01262625 [accessed 25 February 2013].
Clinicaltrials.gov. Prospective multicenter imaging study for evaluation of chest pain (PROMISE). Available from: http://clinicaltrials.gov/ct2/show/NCT01174550 [accessed 25 February 2013].
Litt HI, Gatsonis C, Snyder B et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med 2012;366:1393–403. http://dx.doi.org/10.1056/NEJMoa1201163
Goldstein JA, Chinnaiyan KM, Abidov A et al. The CT-STAT (Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment) trial. J Am Coll Cardiol 2011;58:1414–22. http://dx.doi.org/10.1016/j.jacc.2011.03.068
Hoffmann U, Truong QA, Schoenfeld DA et al. Coronary CT angiography versus standard of evaluation in acute chest pain. N Engl J Med 2012;367:299–308. http://dx.doi.org/10.1056/NEJMoa1201161
Patel MR, Peterson ED, Dai D et al. Low diagnostic yield of elective coronary angiography. N Engl J Med 2010;362:886–95. http://dx.doi.org/10.1056/NEJMoa0907272
Incidence of stroke attributable to atrial fibrillation increases from 1.5% at age 50–59 years to 23.5% at age 80–89 years. The use of oral anticoagulants to reduce the risk of stroke is well established, but all the available agents can cause bleeds if used in excess dose, in high-risk patients or in patients with reduced kidney function.
This article highlights the need to assess kidney function as stated in the newly published European Heart Rhythm Association (EHRA) of the European Society of Cardiology (ESC) practical guide on the use of the new oral anticoagulants (NOACs).1 The EHRA guide has a section on NOACs for patients with chronic kidney disease (CKD) where it is stated that “a careful follow-up of renal function is required in CKD patients, since all (NOACs) are cleared more or less by the kidney”. It continues “in the context of NOAC treatment, creatinine clearance is best assessed by the Cockcroft method, as this was used in most NOAC trials”.
The authors discuss the issues and present a simple guide on why and how to use the Cockcroft Gault equation for kidney function estimation. They also note that for drug and dosing decisions, reduced kidney function, for whatever reason (not just where a patient has been assessed as having CKD), needs to be assessed to reduce the risk of harm.
Chronic kidney disease (CKD) adversely affects cardiovascular outcomes and mortality in the general population. We sought to determine the impact of renal function on angiographic and clinical results in ST-elevation myocardial infarction (STEMI) patients treated with primary percutaneous coronary intervention (pPCI).
Analyses were based on the prospective ‘all-comer’ registry of 1,064 consecutive STEMI patients treated with pPCI in our tertiary centre between February 2001 and October 2002. Admission serum creatinine concentration was known in 894 patients (84%). Mean serum creatinine was 105 ± 27 µmol/L and estimated glomerular filtration rate (eGFR) was 67 ± 18 ml/min/1.73 m2. Thrombolysis in Myocardial Infarction grade 3 (TIMI3) flow was achieved in 751 patients (84%). During hospitalisation, 29 (3%) major bleedings, five (1%) strokes and 12 (1%) re-infarctions occurred. By day 30, two patients were lost to follow-up and 41 (5%) were dead. Renal function was independently associated with 30-day mortality (hazard ratio [HR] 1.6, 95% confidence interval [CI] 1.2–2.1, p=0.003). In CKD patients (eGFR <60 ml/min/1.73 m2), TIMI3 flow was restored less frequently (79% vs. 87%), in-hospital major adverse cardiac and cerebrovascular events (MACCE) were more frequent (15% vs. 4%) and 30-day mortality was higher than in non-CKD patients (9% vs. 2%). Lower eGFR was associated with increased risk of major bleeding (HR 1.6, 95% CI 1.3–2.1, p<0.0005). In the subgroup of conscious patients with normal serum creatinine, eGFR remained significantly associated with 30-day mortality.
In conclusion, renal function expressed by eGFR is an independent predictor of procedural success and short-term outcomes in STEMI patients treated with pPCI, even in patients with normal serum creatinine. Thus, eGFR should be estimated in all STEMI patients to help identify a high-risk subgroup.
Introduction
Myocardial infarction with persistent ST-elevation (STEMI) continues to be a major public health problem. In a recent report, the incidence of hospital admissions for STEMI in Europe varied between 44 and 142 per 100,000 inhabitants per year, and in-hospital mortality reached 13.5%.1 More than 30% of STEMI patients have chronic kidney disease (CKD).2 On the other hand, half of deaths in advanced CKD patients are of cardiovascular causes with myocardial infarction (MI) being the most frequent event.3
Patients with CKD are routinely excluded from cardiovascular clinical trials, and certain medications and treatment modalities are less frequently employed in this group;4 often these patients are treated less aggressively, possibly making proven life-saving therapies underused in this population.5
The objective of this study was to evaluate the impact of renal function on angiographic and short-term clinical outcomes in a homogenous, real-life cohort of patients with STEMI treated with primary percutaneous coronary intervention (pPCI), as this has not been extensively studied so far.
Methods
Study design and patient population
This prospective, observational, single-centre study was conducted at the Institute of Cardiology in Warsaw (Anin). All consecutive patients with STEMI (diagnosed according to European Society for Cardiology [ESC]/American College of Cardiology [ACC] guidelines current at the time6) treated with pPCI between February 2001 and October 2002 were included in a prospective registry (ANIN Myocardial Infarction Registry). There were no exclusion criteria; in particular, patients with cardiogenic shock, pulmonary oedema, known renal failure or advanced age were not excluded.
The study complies with the Declaration of Helsinki and the ethics committee approved its research protocol.
Clinical setting
The Institute of Cardiology in Warsaw is a tertiary cardiology centre performing about 4,000 coronary angiographies and 2,500 PCIs, including about 700 pPCI for STEMI, per year, where round-the-clock interventional duty for acute coronary syndrome patients was started in February 2001.
The majority of patients were transferred to our centre from non-PCI hospitals. Informed consent for interventional procedures was obtained in the emergency department, and patients were transported directly to the cath lab (not via the cardiac care unit [CCU]). The aim was to reduce door-to-balloon time. Blood samples for baseline serum creatinine were drawn from the arterial sheath prior to contrast administration. The operator was unaware of the lab results while performing the procedure.
Primary angioplasty was performed in all patients in accordance with generally accepted standards. At the time of this study, the pre-procedure protocol included a loading dose (300–500 mg orally) of acetylsalicylic acid. Unfractionated heparin (bolus intravenous injection of 100 IU per kg body weight or 70 IU if prophylactic abciximab was planned) and a loading dose of clopidogrel (at that time 300 mg orally) were usually given at the start of the procedure. Prophylactic abciximab use was left to the discretion of the operator. Reperfusion success was defined as a Thrombolysis in Myocardial Infarction (TIMI) grade 3 flow.
Data collection
Baseline demographic, clinical, laboratory and angiographic data were collected on admission and angiographic data on completion of the pPCI using pre-printed forms. Data regarding in-hospital course (death, major bleeding, stroke, re-infarction) were obtained from patients’ charts. Major adverse cardiac and cerebrovascular events (MACCEs) were defined according to the approved criteria (in particular, major bleeding as in TIMI bleeding score, and re-infarction as in the GUSTO-I trial). Vital status at 30 days was established by telephone calls to patients or their cardiologists. Missing data were obtained from the National Census Registry. A dedicated computerised database was set up and regularly updated.
Estimation of renal function
Renal function was assessed by estimation of glomerular filtration rate (eGFR) using abbreviated Modification of Diet in Renal Disease formula, as recommended by the National Kidney Foundation: eGFR = 32,788 × (serum creatinine)–1.154 × age–0.0203 × (1.210 if black) × (0.742 if female).
Patients were staged according to Kidney Disease Outcomes Quality Initiative (K-DOQI) guidelines.7 CKD was defined as eGFR below 60 ml/min/1.73 m2 with or without evidence of kidney damage. The clinical laboratory at our institution reported creatinine values greater than 133 µmol/L as abnormal for either gender.
Statistics
Typical statistical methods were used. Continuous data were expressed as means ± standard deviation (SD) and categorical data as numeric values and percentages. Additionally, age was expressed as a range. Comparison of continuous variables was performed by means of student t-test. Chi square test or Fisher exact test was used for comparison of categorical variables, as appropriate. Time-to-event data were summarised as Kaplan–Meier estimates and compared with log-rank test.
To adjust for baseline differences between study groups, all variables associated with the clinical end points at univariate analysis (p<0.1 for selection) were tested in multi-variate analyses; Cox proportional hazards model and logistic regression were used to identify independent predictors of mortality and final TIMI grade 3 flow, respectively (tested variables were sex, age, history of hypertension, diabetes mellitus, smoking status, prior MI or PCI, heart rate [HR] and systolic blood pressure [SBP] on admission, eGFR, Killip class, localisation of MI, abciximab usage, multi-vessel disease [MVD], initial TIMI grade flow and final TIMI grade flow exclusively for mortality). Final models were built by forward stepwise variable selection, with a p value <0.05 used as a criterion for entry and p >0.1 for removal of variables. Results were presented as hazard ratios (HRs) with 95% confidence intervals (CIs).
All reported p values are two-tailed, and a p value <0.05 was considered statistically significant unless otherwise specified. All statistical analyses were carried out using the Statistical Package for Social Sciences version 15.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics
In 894 of 1,064 consecutive patients enrolled in the registry, blood samples for baseline serum creatinine (SCr) were taken before the administration of the contrast media, and they formed the study group. The baseline characteristics of studied patients are shown in table 1.
Table 1. Baseline characteristics of patients treated with primary percutaneous coronary intervention (pPCI) for ST-elevation myocardial infarction (STEMI) with respect to presence of chronic kidney disease (CKD)
Mean SCr was 105 ± 27 µmol/L and eGFR was 67 ± 18 ml per minute per 1.73 m2, following a normal distribution. A total of 97 patients (11%) had abnormal serum creatinine. The prevalence of CKD was 36%.
Compared with the non-CKD group, patients with CKD were older and more likely to be female. They were less likely to be current smokers or to have a family history of coronary artery disease (CAD). However, they were more likely to have a history of MI, diabetes and hypertension. They were also more likely to be in a higher Killip class or unconscious post-cardiac arrest on admission.
Figure 1. Kaplan–Meier curves of cumulative mortality by CKD stages (log-rank p<0.0005)
Angiographic and procedural characteristics and outcomes
Angiographic characteristics and procedural results were typical for a cohort of STEMI patients treated with pPCI. Most often the infarct-related artery (IRA) was the right coronary artery. More than half of patients had multi-vessel disease (MVD). On the initial angiography, TIMI 0 or 1 flow in the IRA was observed in 732 patients (82%).
In most patients, only the IRA was treated, and the majority of procedures (78%) included stent implantation. Abciximab was given in almost 50% of patients, mostly prophylactically. Final TIMI grade 3 flow was achieved in 751 cases (84%).
CKD patients had MVD more often (60% vs. 48%, p=0.004), and received stents less often (73% vs. 80%, p=0.03). They required intra-aortic balloon pump (IABP) more frequently (3% vs. 1%, p=0.02) and had a lower procedural success rate (79% vs. 87%, p=0.004) when compared with patients with normal renal function.
The independent predictors of procedural failure (final TIMI grade <3), after adjustment for covariates, were decreased eGFR (HR 1.1, 95% CI 1.0–1.3, p=0.01), initial TIMI flow <2 (HR 2.9, 95% CI 1.6–5.6, p=0.001) and history of smoking (HR 2.5, 95% CI 1.7–3.3, p<0.0005).
Clinical outcomes
During a mean of 8 ± 7 days of hospitalisation, MACCEs occurred in 69 patients (8%). Vital status at day 30 was known in 892 out of 894 patients. Forty-one patients (5%) died by day 30.
Major bleeding was significantly associated with renal function. Any decrease in eGFR by 10 ml/min/1.73 m2 increased the risk of major bleeding (HR 1.6, 95% CI 1.3–2.1, p<0.0005). Frequency of re-infarction or stroke was not statistically different with regard to eGFR. Both mortality and MACCE rates increased in higher stages of CKD (table 2). Cumulative mortality was higher in higher stages of CKD as demonstrated by Kaplan–Meier method (figure 1).
Table 2. Angiographic and short-term clinical outcomes by stages of CKD
Prognostic factors for short-term mortality
After adjustment for covariates, 30-day mortality was significantly associated with eGFR (HR 1.6, 95% CI 1.2–2.1, p=0.001 for each 10 ml/min/1.73 m2), age (HR 1.1, 95% CI 1.0–1.1, p=0.005 for each 10 years), prior PCI (HR 5.8, 95% CI 1.7–20.0, p=0.005), unconscious state (HR 18.6, 95% CI 6.7–51.8, p<0.0005) and use of IABP (HR 40.0, 95% CI 9.7–166.7, p<0.0005).
After exclusion of unconscious patients from the analyses, eGFR continued to demonstrate statistically significant independent association with short-term mortality (HR 1.6, 95% CI 1.2–2.3, p=0.004).
Estimated GFR remained an independent predictor of short-term mortality in conscious patients with serum creatinine within normal range (HR 1.8, 95% CI 1.16–2.75, p=0.009 for each 10 ml/min/1.73 m2).
Discussion
The main finding of our study was that every decrease in kidney function as measured by eGFR in STEMI patients was associated with adverse outcomes, even if serum creatinine was within normal range. Thus, eGFR should be considered a continuous parameter, which influences prognosis without any specific cut-off value.
Over one-third of our STEMI patients were in stage 3 or 4 of renal disease. Prevalence of CKD (particularly stage 4) among our patients was higher than in randomised clinical trials,8 in which patients with CKD were systematically excluded, and was similar to that found in registries.2,9 One must, however, bear in mind significant variability of definitions of renal dysfunction employed by different studies.10 Of note, many authors used serum creatinine rather than the eGFR recommended by the National Kidney Foundation.7
In the whole cohort of patients, the 30-day mortality rate was relatively low (5%). This could be due to short ‘door-to-balloon time’, which is a recognised prognostic factor.11 This was achieved through round-the-clock presence of an interventional cardiologist on the premises, as opposed to on-call duty, and direct transfer of patients from admissions to the cath lab rather than via CCU. Despite the fact that we included all consecutive patients, regardless of haemodynamic status and renal function, angiographic success was obtained in more than 80% of patients. As a result, prevalence of in-hospital MACCEs was low. This could be an explanation for no significant difference in re-infarction and stroke between groups in different CKD stages.
The adverse impact of renal impairment on mortality in various cardiovascular diseases has been previously published by several authors.12 Coronary revascularisation procedures, both surgical and percutaneous, were also shown to have worse results in CKD patients than in patients with normal renal function.13 This might be partly explained by the relatively common co-existence of CKD and atherosclerosis, as most of the classical risk factors for these conditions are shared, e.g. age, diabetes, hypertension, obesity, smoking and dyslipidaemia.14 To make it even worse, kidney failure speeds up development of atherosclerosis; such patients have more extensive coronary and peripheral artery disease, e.g. more often have MVD.15 In our study, it was shown that CKD need not be severe or even mild, as demonstrated in a recent study,16 to worsen the prognosis. Mild decrease of eGFR, even within normal range, was also of importance and, actually, any drop in this parameter worsened the prognosis without a specific cut-off value.
We noted more bleeding events in the CKD group. Correlation of renal impairment with bleeding disorders is a well-recognised issue.17 Renal failure may be associated with uraemic platelet dysfunction and decreased thrombopoiesis.18 It also causes impaired aggregability in response to such thrombogenic triggers as adenosine diphosphate (ADP), collagen and epinephrine.
In addition to traditional cardiac risk factors, which are highly prevalent in patients with CKD, CKD patients exhibit marked nephroangiosclerosis (intimal hyperplasia, hyalinosis, smooth muscle cell hypertrophy),19 abnormal coronary flow reserve, inflammation, oxidative stress, insulin resistance, accelerated vascular calcification, activation of the renin–angiotensin system, anaemia and vitamin D deficiency, which might contribute directly to adverse outcomes. Moreover, endothelial dysfunction and chronic inflammation, which play an important role in atherothrombosis, are present even with mild impairment of renal function. This may lead to a worse prognosis, not only in patients with early stages of CKD,16 but also in patients with normal renal function, as was demonstrated in our study.
The available data on immediate angiographic results of pPCI in STEMI patients with different degrees of kidney failure is inconclusive. However, in some studies, similar to ours, angiographic success rate has been shown to differ between stages of kidney disease.20 It may be related to the combined effect of endothelial dysfunction and higher extent of atherosclerosis. Both in vivo and in vitro studies performed on microvessels obtained from patients with advanced CKD confirmed dysfunction of their endothelium.21
Adverse outcomes in MI patients associated with depressed renal function have already been reported.22 However, there are three features that, taken all together, differentiate our study from the previous. First, it was conducted in a homogenous, single centre cohort of STEMI patients that received uniform treatment. Therefore, the potential influence of some confounding factors (such as diagnosis: non-ST-segment elevation MI [NSTEMI] vs. STEMI, type of treatment: interventional vs. fibrinolytic, experience of the centre, volume of procedures, different algorithms of management of STEMI patients) was avoided. Furthermore, and in opposition to most other studies,7 our population is unselected and represents a high prevalence of kidney disease. It reflects frequency of CKD among acute coronary syndrome in real-life practice.23 All patients received modern reperfusion therapy, without any pre-selection based on renal function or other variables (pPCI with high rate of stenting and abciximab usage). Finally, some prior studies,24 have used serum creatinine rather than the eGFR to detect renal function. The accuracy of serum creatinine level as a marker of renal function is limited, owing to nonlinear associations with eGFR that vary according to age, sex and race.25 We found that the prognostic significance of renal function expressed by eGFR was also present in a subgroup of patients with serum creatinine within the normal range. Thus, eGFR should be determined in all patients with STEMI.
Several limitations should be considered when interpreting our results. This was a single-centre study, which may cause an unrecognised bias normally avoided in multi-centre analyses. We had no information about baseline serum creatinine in 170 patients, however, mortality in this excluded subgroup was not significantly different from the study population.
We also had no knowledge about renal function before index STEMI, therefore, we were not able to distinguish between the types of renal dysfunction (acute vs. chronic). We were not able to demonstrate the association between renal function and incidence of re-infarction or stroke due to low numbers of events. Adjunctive therapy used at the time of the study differed from the present routine. Although acetylsalicylic acid was given pre-hospital, most of the patients received heparin and clopidogrel only during the procedure and not in the ambulance or in the referring hospital.
The loading dose of clopidogrel was 300 mg, and not 600 mg as later recommended in STEMI patients. For obvious reasons newer antiplatelet agents (e.g. prasugrel, ticagrelor), drug-eluting stents or thrombectomy were not used at that time.
In conclusion, renal function expressed by eGFR is an independent predictor of procedural success and short-term outcomes in STEMI patients treated with pPCI, even in patients with normal serum creatinine. Thus, eGFR should be estimated in all STEMI patients to help identify a high-risk subgroup.
Acknowledgement
This work was presented in part at the Congress of the European Society of Cardiology in Stockholm, Sweden, on August 31, 2010. [P4562]
Conflict of interest
None declared.
Key message
Renal function expressed by eGFR is an independent predictor of procedural success and short-term outcomes in STEMI patients treated with pPCI.
References
Widimsky P, Wijns W, Fajadet J et al. Reperfusion therapy for ST elevation acute myocardial infarction in Europe: description of the current situation in 30 countries. Eur Heart J 2010;31:943–57. http://dx.doi.org/10.1093/eurheartj/ehp492
Fox CS, Muntner P, Chen A et al. Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction in patients with chronic kidney disease. A report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network Registry. Circulation 2010;121:357–65. http://dx.doi.org/10.1161/CIRCULATIONAHA.109.865352
Charytan D, Kuntz RE. The exclusion of patients with chronic kidney disease from clinical trials in coronary artery disease. Kidney Int 2006;70:2021–30. http://dx.doi.org/10.1038/sj.ki.5001934
Dumaine R, Montalescot G, Steg G et al. Renal function, atherothrombosis extent, and outcomes in high-risk patients. Am Heart J 2009;158:141–8. http://dx.doi.org/10.1016/j.ahj.2009.05.011
Antman E, Bassand JP, Klein W et al. Myocardial infarction redefined – a consensus document of The Joint European Society of Cardiology/American College of Cardiology committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000;36:959–69. http://dx.doi.org/10.1016/S0735-1097(00)00804-4
Levey AS, Coresh J, Balk E et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39(2 suppl 1):S1–S266. http://dx.doi.org/10.1016/S0272-6386(02)70081-4
Kim JY, Jeong MH, Ahn YK et al. Decreased glomerular filtration rate is an independent predictor of in-hospital mortality in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Korean Circ J 2011;41:184–90. http://dx.doi.org/10.4070/kcj.2011.41.4.184
El-Menyar A, Zubaid M, Sulaiman K et al. In-hospital major clinical outcomes in patients with chronic renal insufficiency presenting with acute coronary syndrome: data from a registry of 8176 patients. Mayo Clin Proc 2010;85:332–40. http://dx.doi.org/10.4065/mcp.2009.0513
Polonski L, Gasior M, Gierlotka M et al. Polish registry of acute coronary syndromes (PL-ACUTE CORONARY SYNDROME). Characteristics, treatments and outcomes of patients with acute coronary syndromes in Poland. Kardiol Pol 2007;65:861–72; discussion 873–4.
McNamara R, Wang Y, Herrin J et al. Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol 2006;47:2180–6. http://dx.doi.org/10.1016/j.jacc.2005.12.072
Anderson RJ, O’Brien M, MaWhinney S et al. Renal failure predisposes patients to adverse outcome after coronary artery bypass surgery. VA Cooperative Study #5. Kidney Int 1999;55:1057–62. http://dx.doi.org/10.1046/j.1523-1755.1999.0550031057.x
Sarnak MJ, Levey AS, Schoolwerth AC et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003;108:2154–69. http://dx.doi.org/10.1161/01.CIR.0000095676.90936.80
Yogi H, Kawai M, Komura K et al. Impact of chronic kidney disease on the severity of initially diagnosed coronary artery disease and the patient prognosis in the Japanese population. Heart Vessels 2011;26:370–8. http://dx.doi.org/10.1007/s00380-010-0061-9
Campbell NG, Varagunam M, Sawhney V et al. Mild chronic kidney disease is an independent predictor of long-term mortality after emergency angiography and primary percutaneous intervention in patients with ST-elevation myocardial infarction. Heart 2012;98:42–7. http://dx.doi.org/10.1136/heartjnl-2011-300024
Steg PG, Huber K, Andretti F et al. Bleeding in acute coronary syndromes and percutaneous coronary interventions: position paper by the Working Group on Thrombosis of the European Society of Cardiology. Eur Heart J 2011;32:1854–64. http://dx.doi.org/10.1093/eurheartj/ehr204
Norris, Benign A, Bacardi P et al. Enhanced nitric oxide synthesis in uremia: implications for platelet dysfunction and dialysis hypotension. Kidney Int 1993;44:445–50. http://dx.doi.org/10.1038/ki.1993.264
Rubenstein MH, Harrell LC, Sheynberg BV et al. Are patients with renal failure good candidates for percutaneous coronary revascularization in the new device era? Circulation 2000;102:2966–72. http://dx.doi.org/10.1161/01.CIR.102.24.2966
Anavekar NS, McMurray JJ, Velazquez EJ et al. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl J Med 2004;351:1285. http://dx.doi.org/10.1056/NEJMoa041365
Reddan DN, Szczech LA, Tuttle RH et al. Chronic kidney disease, mortality, and treatment strategies among patients with clinically significant coronary artery disease. J Am Soc Nephrol 2003;14:2373–80. http://dx.doi.org/10.1097/01.ASN.0000083900.92829.F5
Saltzman AJ, Stone GW, Claessen BE et al. Long-term impact of chronic kidney disease in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) trial. JACC Cardiovasc Interv 2011;4:1011–19. http://dx.doi.org/10.1016/j.jcin.2011.06.012
McClatchey KD. Clinical laboratory medicine. Second edition. Philadelphia: Lippincott Williams & Wilkins, 2002.
Authors: Peter McKavanagh, Lisa Lusk, Peter A Ball, Tom R Trinick, Ellie Duly, Gerard M Walls, Sarah McCusker, Mohammad Alkhalil, Claire Louise McQuillan, Mark T Harbinson, Patrick M Donnelly
Peter McKavanagh
Cardiology Research Fellow
Lisa Lusk Cardiovascular Research Nurse
Peter A Ball Consultant Radiologist
Tom R Trinick
Consultant Physician / Biochemist
Ellie Duly Consultant Biochemist
Gerard M Walls FY Doctor / Research Assistant
Sarah McCusker Medical Student / Research Assistant
Mohammad Alkhalil Cardiology Trainee
Claire Louise McQuillan Cardiology Trainee
Ulster Hospital, South Eastern Health and Social Care Trust, Upper Newtownards Road, Dundonald, Belfast, BT16 1RH
Mark T Harbinson Consultant Cardiologist
Patrick M Donnelly Consultant Cardiologist
Queen’s University Belfast, Centre for Vision and Vascular Science, Institute of Clinical Science A, Royal Victoria Hospital, Belfast, BT12 6BA
This study was designed to evaluate the impact of a novel iterative reconstruction (IR) algorithm on an established UK cardiac computerised tomography (CT) service. Areas assessed included image quality and effective radiation dose (ED).
A total of 250 consecutive patients with suspected coronary artery disease were enrolled as a substudy of a larger trial. Examinations were performed on a 64-channel detector CT with data sets reconstructed with the standard filtered back projection (FBP) or IR technique. Image noise was measured within predefined regions of interest (ROI), and image quality qualitatively assessed by two clinicians blinded to the reconstruction method. ED was calculated using a chest-specific conversion coefficient.
Four patients withdrew. So, 246 patients (140 males) underwent cardiac CT: 124 consecutive patients underwent a routine scanning protocol, with images reconstructed with FBP, and 122 patients with IR technique. The mean estimated EDs were 6.5 mSv (FBP) and 4.3 mSv (IR) (dose savings 34%) for all patients (p<0.00001). There was no statistical difference in noise or mean attenuation between the IR and FBP images. The mean IR image quality score was 3.67 ± 1.04 compared with 3.29 ± 1.17 for FBP images (p<0.001).
IR in cardiac CT offers substantial ED reduction without compromise in image quality.
Introduction
The use of cardiac computerised tomography (CT) in the UK is changing. National Institute for Health and Clinical Excellence (NICE) clinical guideline 95 (CG95) defined its role in the assessment of stable chest pain patients.1 Further, recent NICE diagnostics guidance 3 (DG3) has recommended the use of newer scanners for difficult patients and specifically addressed the concerns about the effective radiation dose (ED) of earlier CT platforms.2
However, the commercial availability of the latest CT scanners is not yet widespread within the National Health Service (NHS). The 64-detector CT is presently the workhorse of the NHS and is the recommended technological minimum for a new cardiac CT service. Recent meta-analyses have quoted its per-patient specificity for detecting >50% lesions as between 89 and 96% with sensitivity of 93 and 99%.3-6 In the absence of dedicated higher detector models, the 64 scanner will be the cornerstone for CG95 adoption in most institutions.
The past five years has witnessed unprecedented advances in ED reduction, with individualised protocol selection, retrospective tube dose modulation, bismuth breast shields7 and low-dose prospective axial electrocardiogram (ECG)-triggered gated image acquisition.8,9 More recently, the rebirth of iterative reconstruction (IR) techniques has been heralded as another significant development for cardiac CT image acquisition. IR is not a new concept. Initial reports by Brooks and Di Chiro appear in the literature as early as 1975.10 IR algorithms create more accurate final images by performing repeated ‘iterative’ reconstruction cycles on image data, reducing the amount of electronic noise. Although the concept was sound, helical CT systems lacked the ability to facilitate clinical IR adoption until recently.11,12
The purpose of this study was to assess the impact of the introduction of a novel hybrid IR platform on an established UK cardiac CT service. Outcome measures included image noise, diagnostic image quality and radiation exposure.
Methods
The CAPIR study (CT assessment of chest pain with iterative reconstruction) recruited patients that were enrolled in an ongoing current trial, the Cardiac CT for the Assessment of Pain and Plaque (CAPP) study [ISRCTN52480460]. The CAPP study is a randomised-controlled trial designed to evaluate the use of cardiac CT as a primary imaging test for patients attending a rapid access chest pain clinic (RACPC) within the UK. The study protocol was approved by the Office for Research Ethics Committee Northern Ireland (ORECNI) and the South Eastern Health and Social Care Trust (SEHSCT) Research and Development Committee.
Patients
The CAPIR study population consisted of the 250 patients with suspected CAD that had been randomised to the CT-imaging arm of CAPP. The exclusion criteria were: previous known coronary disease; a history of contrast media reaction; a body mass index greater than 35 kg/m2; tachyarrhythmias; impaired renal function with an estimated glomerular filtration rate (eGFR) of less than 35 ml/minute; severe aortic stenosis; acute myocarditis or pericarditis; uncontrolled hypertension >220/100 mmHg; severe peripheral vascular disease or impaired mobility; left bundle branch block; or any other clinical reason that the attending clinician thought would compromise the patient’s safety.
CT image acquisition
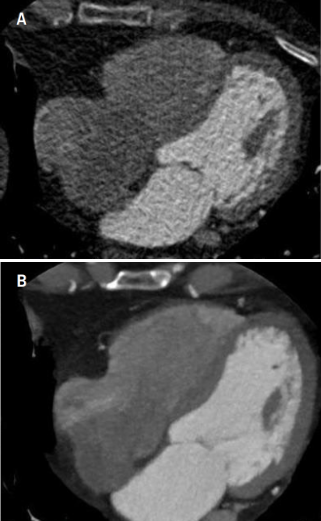
Figure 1. A shows a four-chamber view of a 90 kg patient’s heart taken without iterative reconstruction (IR), using a 120 kV and 600 mAs. B shows a four-chamber view of a 90 kg patient’s heart taken with IR using 120 kV and 600 mAs. The window settings for both images were the same, illustrating the improved image quality with IR
CT was performed on a first generation 64-channel scanner (Brilliance CT, Philips Healthcare, Cleveland, Ohio, USA). As per departmental policy, both oral and intravenous beta blockers were used for heart rate control prior to scanning, and targeted a rate below 65 beats per minute.
A non-contrast enhanced prospective axial calcium score (CS) was performed. Patients were allocated into two cohorts. Cohort A underwent CT coronary angiography (CTCA) using a standard protocol, with images reconstructed with a standard filtered back projection (FBP) technique. Cohort B underwent CTCA with images reconstructed with a novel IR technique, iDose4 (Philips Healthcare, Cleveland, Ohio, USA). The reduction in tube output for Cohort B was based on initial phantom study experience.13 All patients underwent a standardised 120 kV protocol. Other scan parameters (mAs, and scan-length) were optimised by the imaging clinician and were patient specific. The choice of retrospective or prospective ECG triggering (figure 1) was at the discretion of the clinician and influenced by factors such as the resting heart rate, heart rate variability, and pre-test likelihood of coronary artery disease (CAD). For all retrospective ECG-gated examinations, ECG dose modulation algorithms were applied (DoseRight Cardiac, Philips Healthcare, Cleveland, Ohio, USA).
Assessment of image quality
Each patient had their data anonymised and transferred to a remote workstation. Images were then assessed for noise and signal quality within circular regions of interest (ROIs) on axial images. Noise was defined as the standard deviation of the measured Hounsfield unit (HU), and signal as the HU mean attenuation value. The ROIs were in the ascending aorta, interventricular septum and left ventricular cavity.
Subjective image qualities were rated by an experienced cardiologist and radiologist in a blinded fashion using a five-point Likert scale. Images were scored according to the degree of image noise, quality of coronary contour delineation, general image impression, reconstruction artefact, and ease of diagnosis (1=non-diagnostic; 2=fair; 3=moderate; 4=good; 5=excellent).
The ED of each CTCA was estimated by multiplying the dose-length product (DLP) by a chest-specific conversion coefficient (κ=0.014 mSv×mGy−1×cm−1).14,15
Statistical analysis
Statistical analyses were performed using SPSS 19.0 (SPSS Inc., Chicago, Illinois, USA). Continuous variables are presented as mean ± standard deviation (SD) and compared using an independent t-test for normally distributed data. P values <0.05 were considered statistically significant for all data analyses. Inter-observer agreements for subjective image quality were quantified using kappa statistics.
Results
Patient demographics
A total of 250 patients were eligible for the CAPIR study. Four patients withdrew. The remaining 246 patients proceeded to have a CS followed by CTCA. Cohort A consisted of 124 patients who received a FBP protocol. Cohort B consisted of 122 patients who received an IR protocol. Of the 246 there were 140 males and 106 females. There were no significant differences between the two cohorts’ demographics (table 1).
Table 1. Patient demographics. Characteristics in terms of age, sex, body mass index (BMI), risk factors and pre-test probability in each cohort
Protocol selection
Of the 124 consecutive patients in the FBP cohort, 72 underwent a helical retrospectively ECG-gated protocol and 52 a prospectively ECG-triggered protocol. Of the 122 that received an IR study, 112 received a retrospective protocol and 10 a prospective.
Radiation dose estimates
The mean ED of Cohort A was 6.5 mSv. Cohort B had a lower mean ED of 4.3 mSv, thus, representing dose savings of 2.2 mSv (33.6%) (p<0.00001) (table 2). The mean ED for FBP retrospectively ECG-gated studies in Cohort A was 8.3 mSv, with an equivalent mean ED in Cohort B of 4.4 mSv. IR appeared to provide a mean dose saving of 3.9 mSv or 46.5% dose reduction for retrospectively ECG-gated examinations.
Table 2. Computed tomography (CT) characteristics showing contrasting dose-length products (DLPs) and effective radiation doses (EDs) within cohorts, mean ± standard deviation
Image noise, attenuation and image quality
There was no statistical difference in noise or mean attenuation between the IR and FBP images in all three ROI (table 3). The observers’ image quality scores were similar for both IR and FBP scans, with Kappa coefficients of 0.82 and 0.84, respectively. The mean image quality score obtained from the IR images was 3.7 ± 1.0 compared with the FBP images of 3.3 ± 1.2, which was statistically different with a p value of 0.0067 (figure 1).
Table 3. Image noise and attenuation in regions of interest (ROI) for both cohorts, mean ± standard deviation
Discussion
DG3 emphasised the importance of low radiation dose diagnostic cardiac CT examinations. Adoption of DG3 in the NHS will be determined by the availability of the latest generation of cardiac platforms. This study has identified some benefits of IR introduction to an established NHS cardiac CT service using a first generation 64-detector platform, without the need for substantial investment.
The last 10 years has witnessed an unprecedented growth in diagnostic CT imaging. Cardiovascular imaging represents at least a third of the medical imaging examinations performed annually worldwide.16 Between 1993 and 2002, cardiovascular imaging grew more than twice as rapidly as medical imaging for non-cardiovascular disease.17 At present, CT is the single greatest source of medical radiation exposure.18 Iatrogenic CT exposure is thought to contribute to 2.0% of all cancers.18 Recent multi-centre, multi-vendor studies have highlighted the importance of radiation dose reduction, the potential carcinogenic effects, and the importance of adherence to the ALARA (as low as reasonably achievable) principle in cardiac CT imaging.19,20
Guidelines from the American Heart Association21 suggested that an ED of 10 mSv increases the lifetime risk of a fatal malignancy by approximately 0.05%. Therefore, it is the responsibility of all clinicians to reduce this risk to an acceptable level without image quality degradation. In addition, clinicians must be mindful of the cumulative radiation exposure a patient may receive in the investigation of chest pain. Myocardial perfusion imaging with a two-day stress–rest Technetium protocol typically results in an ED of 10–15 mSv,22,23 and invasive coronary angiogram 4–7 mSv.24,25
There have been a number of studies published on the use of IR in cardiac CT imaging. These have highlighted the theoretical benefits of retrospective IR reconstruction to FBP data within the image domain.26-28 To our knowledge, this is the first study to prospectively compare FBP and IR in consecutive patients undergoing cardiac CT for the assessment of stable chest pain.
This study has a number of limitations. First, it was not a randomised-controlled trial, but two distinct cohorts of consecutive patients that underwent CTCA for the assessment of chest pain. Second, there were a number of exclusion criteria, which excluded a number of patients from the study. Third, image quality assessment was based on a subjective Likert score. Fourth, there were fewer prospective ECG-triggered exams in the IR group. Despite this, cohort B had a significantly lower radiation dose. It is likely that the adaption of IR to axial prospective gated protocols with associated ‘ECG padding’ could convey substantial further dose reduction and maintain diagnostic accuracy. Finally, 100 kV imaging was not commercially available at the time of study design and initiation. Consequently, all patients underwent a standardised 120 kV protocol. It is likely that the routine application of 100 kV imaging in appropriate patients would have yielded further substantial dose savings.
The key to successful cardiac CT is image quality. This study has demonstrated that the application of IR algorithms for cardiac CT can offer substantial radiation dose reductions without image quality compromise, on existing cardiac CT platforms.
Funding
This work was supported by the South Eastern Health and Social Care Trust [SET/10/52].
Conflict of interest
None declared.
Key messages
The key to successful cardiac imaging must balance diagnostic image quality with the lowest possible radiation exposure
The as low as reasonably achievable (ALARA) principle must be adhered to at all times. However, accurate initial diagnostic imaging quality is vital to prevent cumulative radiation doses from multiple tests
In cardiac CT, all operators have a responsibility to reduce radiation doses through individualised optimisation of scan protocols (kV, mAs, tube dose modulation)
Iterative reconstruction is a novel technique that allows a significant further reduction in radiation dose without compromise in image quality or noise
References
Skinner JS, Smeeth L, Kendall JM et al. NICE guidance. Chest pain of recent onset: assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin. Heart 2010;96:974–8. http://dx.doi.org/10.1136/hrt.2009.190066
National Institute for Health and Clinical Excellence (NICE). New generation cardiac CT scanners (Aquilion ONE, Brilliance iCT, Discovery CT750 HD and Somatom Definition Flash) for cardiac imaging in people with suspected or known coronary artery disease in whom imaging is difficult with earlier generation CT scanners. London: NICE, December 2012. Available from: http://guidance.nice.org.uk/DG3/Guidance/pdf/English [accessed 20 December 2012].
Salavati A, Radmanesh F, Heidari K et al. Dual-source computed tomography angiography for diagnosis and assessment of coronary artery disease: systematic review and meta-analysis. J Cardiovasc Comput Tomogr 2012;6:78–90. http://dx.doi.org/10.1016/j.jcct.2011.10.018
Takakuwa KM, Keith SW, Estepa AT, Shofer FS. A meta-analysis of 64-section coronary CT angiography findings for predicting 30-day major adverse cardiac events in patients presenting with symptoms suggestive of acute coronary syndrome. Acad Radiol 2011;18:1522–8. http://dx.doi.org/10.1016/j.acra.2011.08.013
Mowatt G, Cook JA, Hillis GS et al. 64-Slice computed tomography angiography in the diagnosis and assessment of coronary artery disease: systematic review and meta-analysis. Heart 2008;94:1386–93. http://dx.doi.org/10.1136/hrt.2008.145292
Vanhoenacker PK, Heijenbrok-Kal MH, Van Heste R et al. Diagnostic performance of multidetector CT angiography for assessment of coronary artery disease: meta-analysis. Radiology 2007;244:419–28. http://dx.doi.org/10.1148/radiol.2442061218
Yilmaz MH, Yasar D, Albayram S et al. Coronary calcium scoring with MDCT: the radiation dose to the breast and the effectiveness of bismuth breast shield. Eur J Radiol 2007;61:139–43. http://dx.doi.org/10.1016/j.ejrad.2006.08.012
Brooks RA, Di Chiro G. Theory of image reconstruction in computed tomography. Radiology 1975;117:561–72.
Sagara Y, Hara AK, Pavlicek W. Abdominal CT: comparison of low-dose CT with adaptive statistical iterative reconstruction and routine-dose CT with filtered back projection in 53 patients. Am J Roentgenol 2010;195:713–19. http://dx.doi.org/10.2214/AJR.09.2989
Prakash P, Kalra MK, Ackman JB et al. Diffuse lung disease: CT of the chest with adaptive statistical iterative reconstruction technique. Radiology 2010;256:261–9. http://dx.doi.org/10.1148/radiol.10091487
Noël PB, Fingerle AA, Renger B et al. Initial performance characterization of a clinical noise-suppressing reconstruction algorithm for MDCT. Am J Roentgenol 2011;197:1404–09. http://dx.doi.org/10.2214/AJR.11.6907
Bischoff B, Hein F, Meyer T et al. Comparison of sequential and helical scanning for radiation dose and image quality: results of the Prospective Multicenter Study on Radiation Dose Estimates of Cardiac CT Angiography (PROTECTION) I study. Am J Roentgenol 2010;194:1495–9. http://dx.doi.org/10.2214/AJR.09.3543
Bongartz G, Golding SJ, Jurik AG et al. European guidelines for multislice computed tomography. Brussels, Belgium: European Commission, 2004; FIGM-CT2000-20078-CT-TIP.
Levin DC, Rao VM, Parker L et al. Recent trends in utilization of cardiovascular imaging: how important are they for radiology? J Am Coll Radiol 2005;2:736–9. http://dx.doi.org/10.1016/j.jacr.2005.01.015
Brenner DJ, Hall EJ. Computed tomography – an increasing source of radiation exposure. N Engl J Med 2007;357:2277–84. http://dx.doi.org/10.1056/NEJMra072149
Hausleiter J, Meyer T, Hermann F et al. Estimated radiation dose associated with cardiac CT angiography. JAMA 2009;301:500–07. http://dx.doi.org/10.1001/jama.2009.54
Gerber TC, Carr JJ Arai AE et al. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation 2009;119:1056–65. http://dx.doi.org/10.1161/CIRCULATIONAHA.108.191650
Einstein AJ. Radiation risk from coronary artery disease imaging: how do different diagnostic tests compare? Heart 2008;94:1519–21. http://dx.doi.org/10.1136/hrt.2007.135731
Berrington de Gonzalez A, Kim K-P, Smith-Bindman R, McAreavey D. Myocardial perfusion scans. Projected population cancer risks from current levels of use in the United States. Circulation 2010;122:2403–10. http://dx.doi.org/10.1161/CIRCULATIONAHA.110.941625
Anonymous. Sources and effects of ionizing radiation. United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2000 report to the General Assembly, with scientific annexes. New York: United Nations, 2000. Available from: http://www.unscear.org/unscear/en/publications/2000_1.html [accessed 20 December 2012].
Vijayalakshmi K, Kelly D, Chapple CL et al. Cardiac catheterisation: radiation doses and lifetime risk of malignancy. Heart 2007;93:370–1. http://dx.doi.org/10.1136/hrt.2006.098731
Gosling O, Loader R, Venables P et al. A comparison of radiation doses between state-of-the-art multislice CT coronary angiography with iterative reconstruction, multislice CT coronary angiography with standard filtered back-projection and invasive diagnostic coronary angiography. Heart 2010;96:922–6. http://dx.doi.org/10.1136/hrt.2010.195909
Renker M, Nance JW Jr, Schoepf UJ et al. Evaluation of heavily calcified vessels with coronary CT angiography: comparison of iterative and filtered back projection image reconstruction. Radiology 2011;260:390–9. http://dx.doi.org/10.1148/radiol.11103574
Moscariello A, Takx RA, Schoepf UJ et al. Coronary CT angiography: image quality, diagnostic accuracy, and potential for radiation dose reduction using a novel iterative image reconstruction technique – comparison with traditional filtered back projection. Eur Radiol 2011;21:2130–8. http://dx.doi.org/10.1007/s00330-011-2164-9
Chronic heart failure (CHF) affects 900,000 people in the UK and consumes almost 2% of the National Health Service (NHS) budget. These figures are set to rise as the prognosis of coronary artery disease improves and the population ages. Heart failure currently accounts for approximately 5% of all emergency medical admissions to hospital, and over the next 25 years the proportion will rise by 50% – largely due to an older population.1
In the USA, in 2008 the total inflation-adjusted cost of heart failure admissions was US$10.7 billion, compared with US$6.9 billion in 1997.2 So heart failure admissions are expensive and there is considerable interest in how we might reduce admissions, thereby reducing costs and leading to an improved quality of life (QoL) for patients with heart failure.3
One solution might be the Observation Unit (OU) proposed by Collins et al.4 as an alternative to hospital admission for patients needing a brief period (under 24 hours) of intravenous diuretic therapy. Observation, by definition, is the use of appropriate monitoring, diagnostic testing, therapy, and assessment of patient symptoms, signs, laboratory tests, and response to therapy in order to decide whether a patient will require further treatment as an inpatient or can be discharged from the hospital. OUs are present in almost one third of US hospitals. They are short-stay units for emergency departments (EDs) and have been introduced as an economically viable and clinically safe solution to the growing problem of overcrowding in hospitals. They are typically situated within (or adjacent to) the ED. Patients who do not improve within 24 hours are admitted, but most (around 70%) are discharged. Patients on OUs are still under the auspices of the ED and are not considered inpatients. Their admissions are cheaper because OUs have a lower nurse-to-patient ratio than inpatient units and they are associated with a reduced length of stay. Not only that, but, because the patients are not counted as admissions, hospitals are not subject to 30‑day re‑admission penalties, another potential cost saving. In the US healthcare model, one of the problems associated with this approach is that while hospital costs are reduced, the bill for the patient can be increased. They are treated as outpatients when staying in an OU and insurers will often only ‘part cover’ outpatient expenses, whereas inpatient treatment is usually fully covered.
In the UK, short-stay units have become common following an NHS plan launched in 2000.5 They are more commonly associated with medical admissions units than accident and emergency departments. By the time patients have reached such units they have been classified as inpatients and the hospital trust may then be subject to 30‑day re-admission penalties. There is little point in operating an OU (or short-stay ward) as an accountancy trick to reduce hospital costs or avoid re-admission penalties: changes to the structure of healthcare should be to the benefit of patients.
Observation Units – a UK model
Individual hospitals are unlikely ever to have a large enough number of heart failure admissions to allow a dedicated heart failure OU to be viable. Managing patients with heart failure in a generic short-stay unit without expert input, however, will make the problem of lack of integration of care worse, as yet another group become involved in patient management. A solution might be to have outreach from the heart failure service into OUs from a team of heart failure specialist nurses who work in the community as well as in hospital, so that patients who need a day or two of intravenous therapy can be managed by the group of nurses who know them. Intense initial follow-up post-discharge, with relaxation of appointments once remission and stability are achieved, is likely to reduce re‑admissions. Whether such a model is actually better for the patient than simply being admitted to cardiology for appropriate management must be tested in formal trials before it is widely taken up.
The benefits of specialist heart failure clinics on survival and hospitalisation are well known.6,7 Despite this, the National Heart Failure Audit for 2011–12 showed that only half of patients were referred to a heart failure liaison service on discharge. Women with heart failure, or those patients over the age of 75, had a less than 50% chance of being followed up appropriately post-discharge.8 While Desai et al.9 may be correct in saying that “Even with widespread implementation of a package of post-discharge strategies that successfully address the triggers of re-admission, episodes of heart failure decompensation will continue to occur”, we are a long way from widespread implementation of the package.
The modern management of CHF has led to improved life expectancy and QoL.10 Recurrent admission to hospital has a significant effect on QoL, but measuring QoL is difficult. Although there are a number of disease-specific questionnaires available, many of them address symptoms that are thought to be important by the physician but may not be important to the patient.10,11 The Kansas City Cardiomyopathy Questionnaire has the merit of specifically addressing the impact that symptoms have on the patient, which is particularly important as healthcare professionals often underestimate the social functioning of patients with heart failure.10 Swinburn et al. in the present issue (see pages 72–6) compared the rating of symptoms made by a patient’s relatives with the rating made by a specialist nurse. Relatives tended to grade symptoms as being less severe at day one following an admission for acute heart failure than the specialist nurses. It is important to emphasise, however, that patients’ appreciation of their symptoms is not the same as that of healthcare professionals, and after all, it is the patient who experiences the symptoms.12,13 A proxy assessment via the relatives may be a way of assessing QoL in very sick patients who are unable to speak, but this only applies to a very small number of heart failure admissions, most of whom can answer for themselves.
Conflict of interest
None declared.
Editors’ note
See the article by Swinburn et al. on page 72–6 of
this issue.
Takeda A, Taylor SJ, Taylor RS, Khan F, Krum H, Underwood M. Clinical service organisation for heart failure. Cochrane Database Syst Rev 2012;9:CD002752. http://dx.doi.org/10.1002/14651858.CD002752.pub3
Collins S, Pang P, Fonarow G et al. Is hospital admission for heart failure really necessary? The role of the Emergency Department and Observation Unit in preventing hospitalization and rehospitalization. J Am Coll Cardiol 2013;61:121–6. http://dx.doi.org/10.1016/j.jacc.2012.08.1022
Cook MW, Higgins J, Kidd P. Use of emergency observation and assessment wards: a systematic literature review. Emerg Med J 2003;20:138–42. http://dx.doi.org/10.1136/emj.20.2.138
Thomas R, Huntley A, Mann M et al. Specialist clinics for reducing admissions in patients with heart failure: a systematic review and meta-analysis of randomised controlled trials. Heart 2013;99:233–9. http://dx.doi.org/10.1136/heartjnl-2012-302313
Stromberg A, Mårtensson J, Fridlund B, Levin LA, Karlsson JE, Dahlström U. Nurse led heart failure clinics improve survival and self-care behaviour in patients with heart failure. Eur Heart J 2003;24:1014–23. http://dx.doi.org/10.1016/S0195-668X(03)00112-X
Desai A, Stevenson LW. There must be a better way. Piloting alternate routes around heart failure hospitalizations. J Am Coll Cardiol 2013;61:127–30. http://dx.doi.org/10.1016/j.jacc.2012.10.015
Dunderdale K, Thompson DR, Miles JN, Beer SF, Furze G. Quality-of-life measurement in chronic heart failure: do we take account of the patient perspective?Eur J Heart Fail 2005;7:572–82. http://dx.doi.org/10.1016/j.ejheart.2004.06.006
Garin O, Ferrer M, Pont A et al. Disease-specific health-related quality of life questionnaires for heart failure: a systematic review with meta-analyses. Qual Life Res 2009;18:71–85. http://dx.doi.org/10.1007/s11136-008-9416-4
Goode KM, Nabb S, Cleland JG, Clark AL. A comparison of patient and physician-rated New York Heart Association class in a community-based heart failure clinic. J Card Fail 2008;14:379–87. http://dx.doi.org/10.1016/j.cardfail.2008.01.014
Cleland JG, Freemantle N, Daubert JC, Toff WD, Leisch F, Tavazzi L. Long-term effect of cardiac resynchronisation in patients reporting mild symptoms of heart failure: a report from the CARE-HF study. Heart 2008;94:278–83. http://dx.doi.org/10.1136/hrt.2007.128991
The National GPSI Cardiology Forum was established in 2005 and, despite the demise of the Primary Care Cardiovascular Society (PCCS) to which it was affiliated, it has remained active in the national cardiovascular arena. At a recent meeting at Warwick University, a decision was made to change our name to CVGP (CardioVascular General Practitioners: the Society for GPs with an interest in Cardiovascular Medicine). This name change does not alter our stated aims or direction of travel, but acknowledges the need to embrace all GPs involved in cardiovascular care rather than just GPs with a special interest (GPSIs) in cardiology. We believe this is essential in the evolving NHS clinical commissioning environment.
The Forum has contributed a great deal to the advancement of cardiovascular medicine across the UK and beyond over the last seven years.
This has been achieved through successful fulfillment of our main aims, which the CVGP will continue to pursue:
to represent primary care cardiovascular health needs at policy level
to promote best practice in primary care cardiovascular health through education, training and service development
to support the development of primary care healthcare professionals and teams in the delivery of cardiovascular medicine
to facilitate and lead primary care cardiovascular research.
Enthusiastic membership
Much has been made possible by the sheer enthusiasm of our members in becoming involved in many aspects of cardiovascular disease (CVD)care, over and above their day job as GPs. Many of our members have provided a cohesive and coordinated voice for primary care cardiology, working with other organisations, such as the Royal College of General Practitioners, the Royal College of Physicians, the British Cardiovascular Society, the European Society of Cardiology, the Department of Health, and the National Institute for Health and Clinical Excellence. This has enabled them to influence and guide national and European policy. Virtually all guidelines in evidence-based cardiovascular medicine over the past five years bear the name of at least one Forum member.
We believe that our role as GPSIs is to up-skill and educate primary healthcare teams in evidence-based cardiovascular practice through communication, collaboration and sharing good practice. We believe that the better management of cardiovascular diseases such as heart failure, atrial fibrillation, angina and hypertension by GPs and practice nurses has been facilitated in many areas by local GPSIs in cardiology education and support. Furthermore, we have managed to provide programmes of education tailored to the more specialist needs of GPSIs in cardiology. In order to remain up to date in our chosen specialist fields, we undoubtedly have different educational needs to those of many of our primary care colleagues.
Sharing knowledge
The not inconsiderable challenges of a new commissioning era create opportunities for GPSIs in cardiology-led service developments. We believe that sharing our cardiovascular knowledge, practical experience and service development models through the pages of the BJC will contribute to primary care education and ultimately to better patient care across the UK. We believe that all GPs involved in cardiovascular care, including practice-based and clinical commissioning group (CCG) primary care CVD leads, will need to collaborate, share ideas and work closely together in order to drive forward quality care in the NHS. We invite any GPs with an interest in cardiovascular medicine, not only those providing GPSI services but also those acting as practice CVD leads or CCG CVD leads, to join the CVGP by contacting us.
We shall be advertising forthcoming educational initiatives and meetings through the pages of the BJC. The formation of the CVGP is an exciting development and we look forward to working closely with the BJC
A 73-year-old woman, with a history of deep vein thrombosis (DVT) in her legs, presented two years following coronary artery bypass graft (CABG) with left internal mammary artery (LIMA), left radial artery and left cephalic vein, with a massive right atrial mass. Pre-operative work up also showed a left adrenal mass on computed tomography (CT) scan. We discuss the diagnostic possibilities within such a scenario and review the literature for right atrial masses of diverse aetiology, including right atrial myxomas, benign and malignant tumours of right atrium and right atrial thrombosis. The case is unusual on account of the concomitant history of DVT and the presence of left adrenal mass, rapid growth of the mass within two years following CABG, the atypical origin of the myxoma near inferior vena caval opening and the near total obliteration of the right atrial myxoma by rapid growth of myxoma to a massive size.
Case presentation
A 73-year-old woman presented with six-month history of progressively worsening exertional shortness of breath. The patient had previously undergone coronary artery bypass grafting (CABG) two years ago for symptomatic, severe, left-sided coronary artery disease using left internal mammary artery (LIMA) graft to left anterior descending (LAD) artery, left radial artery to obtuse marginal branch of circumflex artery and left cephalic vein graft to diagonal branch of LAD artery with good symptomatic relief. The choice of conduits at the initial operation had been dictated by a history of deep vein thrombosis (DVT) and varicose veins in both legs.
Figure 1. Transthoracic echocardiogram showing a large mass prolapsing through the tricuspid valve and filling the right atrium nearly completely
On examination, she had engorged neck veins but little else of note. Chest X-ray and electrocardiogram (ECG) were unremarkable. Echocardiogram showed a large right atrial mass filling up almost the whole of the right atrium, part of which prolapsed through the tricuspid valve opening during diastole. The mass seemed to arise from the inferior surface of right atrium very close to the inferior vena caval opening (figure 1). Computed tomography (CT) scan confirmed the presence of a large right atrial mass (figure 2), no secondary pulmonary emboli and a left adrenal mass (figure 3), the significance of which was unclear. Magnetic resonance imaging (MRI) confirmed the presence of large right atrial mass, with its origin from the inferior surface of the right atrium close to the inferior vena caval opening. Intraoperative transoesophageal echocardiography (TOE) pictures were equally striking and further delineated the sheer massive size of the mass, occupying the whole of the right atrium, arising from the inferior wall of the right atrium close to the inferior vena cava and prolapsing through the tricuspid valve into the right atrium (figure 4).
After secondary median sternotomy and dissection of heart, in general, and right atrium and ascending aorta, in particular, cardiopulmonary bypass was instituted with right femoral and direct superior and inferior vena caval cannulations. Right atrium was opened by a long oblique incision, with heart beating, and the large mass visualised (figure 5).This was adherent by a broad attachment to the inferior surface of the right atrium just above the inferior vena cava. The mass was excised completely, along with its attachment to the right atrial wall with a circumferential 1 cm clearance (figure 6). Tricuspid valve and right ventricle were inspected for additional masses. Primary right atrial closure was performed and bypass terminated.
Patient made uncomplicated recovery and was discharged home in a week. Postoperative CT scan of chest was normal and did not show, in particular, any secondary lung masses. Echocardiogram of the heart showed complete clearance of the mass and no residual masses in the heart chambers. Histopathology of the mass confirmed myxoma. On six-week follow-up, patient was asymptomatic and had made good recovery.
Discussion
Myxomas
Figure 2. Computed tomography (CT) scan showing a large right atrial mass
A right atrial mass following CABG, two years earlier, in a patient with previous history of DVT and a suspicious shadow in the left adrenal gland could be a benign tumour, a malignant primary or secondary tumour, or a thrombus.
Approximately 75% of primary cardiac tumours are benign: 50% of benign tumours are myxomas, and 10–20% of all myxomas arise from the right atrium. About 95% of myxomas arise sporadically, are more common in middle aged women, are unassociated with other abnormal conditions, do not recur after adequate excision and 80% of these have a normal DNA genotype. About 5%, in contrast, show a familial pattern of tumour development based on autosomal dominance inheritance, are present in younger patients and equally likely to present in males. They have multi-centric origin (22%), higher recurrence rates after excision (21–67%), and, in 20% of patients, associated abnormalities like testicular, pituitary, adrenocortical, breast or skin tumours or pigmented spots may be present.1 Carney complex is an inherited autosomal dominant disorder with marked familial trend, found in younger patients, comprising atypical myxomas and extracardiac involvement including pigmented skin lesions, cutaneous myxomas, adrenal cortical disease, myxoid mammary fibroadenomas, testicular tumours, pituitary adenomas, melanotic schwanommas and thyroid disease.2-4
Figure 3. Computed tomography (CT) scan showing a left adrenal mass
Common clinical presentation of myxomas in general includes intracardiac obstruction with cardiac failure (67%), thromboembolism (29%), and constitutional and immunological symptoms (22%), with most patients having multiple symptoms. Grossly, two-thirds of myxomas are relatively compact and polypoid and unlikely to fragment spontaneously,5 while the other one-third are gelatinous and fragile and, thus, prone to fragmentation and embolisation.6 Histologically, myxomas are composed of polygonal cells with irregular, slightly hyperchromatic nuclei without mitoses, containing parallel filaments similar to the contractile components of the smooth muscle cells, seen in particular abundance in the region of fossa ovalis in the left atrium. These polygonal cells with vasoformative tendencies are found with primitive capillaries and foci of extramedullary haematopoeisis within an acid mucopolysaccharide myxoid matrix containing, in addition, reticulocytes, smooth muscle cells and elastic and collagen deposits, with, in 10% of patients, foci of calcium and metaplastic bone.7
Traditionally, myxomas have been thought to arise from the multi-potential mesenchymal cells present in the endocardium of the atrial septum in the fossa ovalis region,8 although Krikler suggested origin from endocardial sensory nerve tissue, based on identification of three neuroendocrine markers in 24 excised atrial myxomas.9 There have been increasing reports documenting the malignant potential of the myxomas with respect to local invasion of vessel wall, recurrence, independent growth and distant metastases.10-12
Right atrial myxomas demonstrate a wide spectrum of histomorphological diversity. Mallick et al. reported prominent glandular differentiation mimicking a metastatic adenocarcinoma in a 10-year-old child.13 Hwang et al. described a large, thin-walled, cystic mass filled with arterial blood arising by a broad base between superior vena cava and the appendage.14 Fox et al. reported a right atrial myxoma associated with vascular malformation supplied by the right coronary artery.15
Figure 4. Intraoperative transoesophageal echocardiogram showing the prolapsing right atrial mass
While the most common site of origin continues to be the interatrial septum, as in the more common left atrial myxomas, origin from the free wall with phrenic stimulation,16 from tricuspid valve,17 and from suprahepatic vena cava associated with asplenia,18 have been described. In a comprehensive review of over 100 cases of Myxoma syndrome or Carney’s complex, Edwards et al. described the occurrence of right atrial myxomas in as many as 44%, multiple myxomas in 41% and a 20% incidence of recurrence. They recommended four-chamber examination of heart at surgery for atypical myxomas by a right atriotomy and combined superior transseptal approach, careful screening of the first-degree relatives and careful long-term follow-up.3 While a large number of right atrial myxomas may be asymptomatic, presentation with tricuspid valve obstruction,19 pulmonary embolism20 with cor pulmonale,21 Budd- Chiarri syndrome with hepatic and portal vein thrombosis and ascites,22 and, finally and unusually, with infection of the mass,23 have been described. Pulmonary embolism is a particularly dreaded complication of right atrial myxoma, and pulmonary seeding should be assiduously sought and excluded by CT scan before embarking on surgery.24,25 Canale et al. described right atrial myxoma excision and bilateral pulmonary embolectomy, utilising a brief period of circulatory arrest, in a patient presenting with tricuspid obstruction.20
Other tumours
Other benign tumours that can arise from right atrium are lipomas, lipomatous hypertrophy of interatrial septum, papillary fibroelastoma of tricuspid valve and haemangioma.26
Secondary metastatic tumours of the heart are 20 to 40 times more common than the primary malignancies,27 and almost 10% of all metastatic tumours eventually reach the heart or mediastinum.28 Although every type of malignant tumour has been known to involve the heart, leukaemia and melanoma comprised 53.9% and 34% of all metastatic disease in one large series.29 Lung cancer, sarcoma, breast cancer, oesophageal cancer, ovarian cancer and renal cancer comprised 10.2%, 9.2%, 8.3%, 7.7%, 5.7% and 5.3%, respectively, in a large series.29 Cardiac involvement by prostatic or gastrointestinal tumours, with the exception of carcinoid tumours, is rare. Carcinoid heart disease involves white fibrous deposits on the tricuspid and pulmonary valves causing predominantly tricuspid regurgitation and pulmonary stenosis in patients with primary tumours arising from the argentaffin cells of the ileum, pancreas, biliary vessels, ovary or testes, complicated by hepatic metastases.30 Lymphomas are known to involve the pericardium and not specifically the heart.29 On the other hand, in a large Chinese study of 33,108 open-heart operations and 242 cardiac tumours, all the secondary cardiac tumours were located to the right side of the heart.31 The most common mode of metastatic spread to the heart is haematogenous, although lymphatic, inferior vena caval and pulmonary venous spread and spread through direct extension of lung, oesophageal, thymic and breast tumours is well recognised. Renal, hepatic, adrenal and uterine malignancies spread into the right atrium through inferior vena cava. As many as 10% of all renal malignancies involve inferior vena cava and 40% of these invade the right atrium.32
Figure 5. Intraoperative picture showing a large dusky, purple mass filling the entire right atrium
About 25% of all primary cardiac tumours are malignant, and angiosarcomas, which have a predilection for the right heart, constitute 33% of all malignant tumours. Right atrium may also be involved by malignant mesothelioma or fibrosarcoma. Lynch et al. reported 18 right-sided tumours of the heart over a sevenyear period, out of which, 15 involved right atrium, comprising five hypernephromas, four myxomas, two angiosarcomas, and one each of lipoma, cavernous haemangioma, hepatoma and chondrosarcoma.33
Intracardiac thrombosis
Endocardial injury, stasis or turbulence of blood flow and hypercoagulability of blood are the three classical factors that predispose, in general, to intracardiac thrombosis.34 Endocardial injury may result from transmural myocardial infarcts, myocardial infections, immunological myocardial reactions, inflammatory valve disease, prosthetic heart valves with or without complications, radiation, chemotherapeutic agents, instrumentation, bacterial toxins or endotoxins and immunological insults, as in transplant rejection.34
Generally, stasis contributes more to venous thromboembolism, while turbulence predisposes to arterial and intracardiac thrombosis, but considerable overlap is seen in many clinical situations. In myocardial infarction, in addition to endocardial injury, there is an element of stasis due to failure of necrotic muscle to contract.
In mitral and tricuspid stenoses, atria empty inadequately. When atrial fibrillation supervenes, there is further stasis and turbulence and a great potential for atrial and auricular thrombosis. Hyperviscosity syndromes, like polycythaemia, cryoglobulinaemia, macroglobulinaemia and sickle cell anaemia, partly act through promoting stasis. Hypercoagulability per se is an unusual cause of intracardiac thrombosis and can be primary, due to a genetic defect in one or several coagulation proteins, or secondary, occurring in a variety of clinical conditions associated with recurrent thrombosis.
Primary or genetic causes of hypercoagulability mainly include deficiencies in antithrombin III, protein C, protein S and fibrinolytics, factor V Leiden gene mutation and prothrombin gene mutation.35 Secondary causes include cancer, acute leukaemia, myeloproliferative disorders, nephrotic syndrome, oral contraceptives, pregnancy, disseminated intravascular coagulation (DIC), thrombotic thrombocytopenia, antiphospholipid antibody syndrome, homocystinuria, thrombocytosis, sickle cell anaemia, systemic lupus erythematosus (SLE) and others.34
While right atrial thrombosis shares in some of the aetiological narrative of thrombosis mentioned above, there are important differences as well. Right atrial thrombosis has been described with DVT of leg and pelvic veins, atrial fibrillation,36 constrictive pericarditis with tricuspid thrombotic obstruction37 and non-specific pericarditis,38 restrictive cardiomyopathy,39 and after Fontan operation.40,41 Genetic causes like methylenetetrahydrofolate (MTHF) reductase gene polymorphism,42 hypercoagulability characterised by factor V Leiden gene, thrombophilia genes and high serum homocysteine,43 myeloid leukaemia,44 heparin-induced thrombocytopenia,45,46 lung cancer47 and amoebic liver abscess,48 have all been reported with right atrial thrombosis. Biatrial thrombosis with mitral stenosis and leg DVT treated with mitral valve replacement and bi-atrial thrombectomy has been reported.49
Figure 6. Excised right atrial mass
On the other hand, there are reports of bi-atrial thrombosis across a patent foramen ovale, with resolution following anticoagulation.50 Some of the right atrial thrombi might be entrapped ‘in transit’ across a patent foramen ovale.43,51 However, the most common causes of right atrial thrombosis relate to the host of artificial devices inserted into the right atrium for a variety of indications. These include central venous catheters and Hickman lines for longterm use for antibiotics, hyperalimentation52 and chemotherapy,53,54 pulmonary artery catheters,55 permanent pacemaker56 and defibrillator leads,57 umbilical catheters,58 dialysis catheters59 and port-a-caths,60 extracorporeal membrane oxygenation (ECMO) catheters,61 and ventriculoatrial shunts for hydrocephalus62 or peritoneovenous shunts for intractable recurrent malignant ascites.63
Some of the device-related thrombosis has a septic component to it.64,65 Yang et al. reviewed the available literature on right atrial thrombosis in 2010 and identified 122 cases: 91% of patients had central venous catheters, 40.8% were premature, 27.2% were postcardiac surgery patients, 19.2% had underlying malignancies and 45.6% of patients received intravenous hyperalimentation.66 Aksu et al. and Khurana et al. separately described two inferior cavo-atrial masses with pulmonary thromboembolism masquerading as myxomas and vegetations, where histopathology revealed thrombus.67,68
A solitary unilateral adrenal mass may be a cyst, an adenoma or a carcinoma. An adrenal cortical adenoma or carcinoma may be functional or non-functional. A cortisolsecreting adenoma or carcinoma gives rise to Cushing’s syndrome, an aldosterone-secreting adenoma (Conn’s syndrome) or carcinoma leads to primary hyperaldosteronism, and an androgen-secreting adrenal cortical carcinoma can cause the virilising adrenogenital syndrome. Again there might be non-functional cortical adenomas or carcinomas, but these are much less common. Adrenal medullary tumours include phaeochromocytomas, neuroblastomas, ganglioneuromas and variants of these neoplasms.69
Our patient had a massive right atrial mass arising from the inferior right atrial wall very close to the inferior vena caval opening. In the presence of a left adrenal mass shadow, there was a possibility of an adrenal metastasis coming up the renal vein and inferior vena cava into the right atrium. In light of her previous history of leg DVT and CABG, a right atrial thrombosis could not be entirely ruled out.
Between 10 and 20% of myxomas arise from the right atrium and, although origin from the inferior wall close to inferior vena cava is unusual, there are at least two case reports of origin from the inferior vena cava.18 This atypical origin further increased the diagnostic doubt. Origin of the tumour near the inferior vena caval opening and filling up of the whole of the right atrium by the myxoma made direct cannulation of the cavae mandatory and direct cannulation of supradiaphragmatic inferior vena cava difficult, but in the event it was possible to negotiate a Pacifico size 24 F venous cannula into the inferior vena cava just below the tumour, and the tumour was excised in its entirety, along with the adjoining right atrial wall close to the inferior vena cava, with adequate tumour clearance, while the heart was beating without aortic cross clamp.
Had the direct inferior vena cava cannulation not been possible due to involvement by the tumour, the tumour would have to be excised under profound hypothermia with low flows or circulatory arrest. A thrombus would have mandated excision with or without an inferior vena cava filter and aggressive postoperative anticoagulation. An adrenal metastasis would have required an in-continuity excision of the left adrenal gland and suprarenal veins. An on-table TOE confirmed absence of concomitant myxomas elsewhere in cardiac chambers, as well as complete removal of tumour. A pre-operative CT scan had ruled out any pulmonary emboli and postoperative CT scan excluded any spilling of myxomatous debris in pulmonary circulation. All three grafts including LIMA to LAD, left radial artery to obtuse marginal branch of circumflex artery and, specifically, left cephalic vein to diagonal artery were patent.
Lee B, Sir JJ, Park SW. Right sided myxomas with extramedullary hematopoeisis and ossification in Carney complex. Int J Cardiol 2008;130:e63–e65. http://dx.doi.org/10.1016/j.ijcard.2007.11.061
Edwards A, Bermudez C, Piwonka G, et al. Carney’s syndrome: complex myxomas. Report of four cases and review of literature. Cardiovasc Surg 2002;10:264–75. http://dx.doi.org/10.1016/S0967-2109(01)00144-2
Affronti A, Di Bella I, Prontera P, Da Col U. Obstruction of the tricuspid valve orifice by a huge right atrial myxoma associated with the Carney complex: a case report. J Cardiac Surg 2010;25:674–6. http://dx.doi.org/10.1111/j.1540-8191.2010.01114.x
McAllister HA, Fenoglio JJ. Tumours of the cardiovascular system, atlas of tumour pathology, series 2. Washington DC: Armed Forces Institute of Pathology, 1978;2:pp. 20.
Read RC, White HJ, Murphy ML, Williams D, Sun CN, Flanagan WH. The malignant potentiality of left atrial myxoma. J Thorac Cardiovasc Surg 1974;68:857–68.
Mallick SR, Das P, Shukla B, Kothari S. Right atrial myxoma with glandular differentiation. A rare entity in pediatric age group. Ann Pediatr Cardiol 2010;3:159–62. http://dx.doi.org/10.4103/0974-2069.74046
Fox JJ, Bonavita GJ, Sethi V. Right atrial myxoma associated with vascular malformation and atypical chest pain. Catheter Cardiovasc Diagn 1992;26:127–9. http://dx.doi.org/10.1002/ccd.1810260210
Fatimi SH, Deedar-Ali-Khwaja R, Kiani SK. Imaging and intervention of paraneoplastic effect of a right atrial myxoma on factor VII activity levels. Ann Thorac Surg 2011;91:278–81. http://dx.doi.org/10.1016/j.athoracsur.2010.06.120
Vizzardi E, D’Aloia A, Chiari E, Nardi M. Tricuspid valve myxoma in a patient with congestive heart failure. Cases J 2010;3:21. http://dx.doi.org/10.1186/1757-1626-3-21
Elmusa K, Haddad R, Arnaut MS. Atypical and unusual myxoma. J Med Liban 2004;52:48–50.
Azevedo O, Aleida J, Nolasco T, Medeiros R. Massive right atrial myxoma presenting as syncope and exertional dyspnea: case report. Cardiovasc Ultrasound 2010;8:23. http://dx.doi.org/10.1186/1476-7120-8-23
Canale LS, Colafranchesci AS, Leal Botelho ES, de Oliveira Monteiro AJ. Surgical treatment of right atrial myxoma complicated with pulmonary embolism. Interact Cardiovasc Thorac Surg 2009;9:535–6. http://dx.doi.org/10.1510/icvts.2009.206318
Lorentz MN, Vrandecic EC, Drumond LF, Soares RR. Right atrial myxoma associated with acute cor pulmonale. Case report. Rev Bras Anestesiol 2008;58:169–72.
Anagnostopoulos GK, Marganitis G, Kostopoulos P, Papadopoulou G. Budd-Chiari syndrome and portal vein thrombosis due to right atrial myxoma. Ann Thorac Surg 2004;78:333–4. http://dx.doi.org/10.1016/S0003-4975(03)01265-7
Daga CB, Gonzalez CM, Ortas NR, Ferreira MI. Pulmonary embolism and myxoma of right atrium. An Med Interna 2005;22:478–80.
Idir M, Oysel N, Guibaud JP, Labouyrie E, Roudaut R. Fragmentation of a right atrial myxoma presenting as pulmonary embolism. J Am Soc Echocardiogr 2000;13:61–3.
Hallahan ED, Vozelzang NJ, Borow KM. Cardiac metastasis from soft tissue sarcomas. J Clin Oncol 1986;4:1662–9.
Fine G. Neoplasms of the pericardium and heart. In: Gould SE (ed). Pathology of the Heart and Blood Vessels. Springfield, IL: Charles C Thomas, 1968; pp. 851.
Yu K, Liu Y, Wang H, Hu S, Long C. Epidemiological and pathological characteristics of cardiac tumours: a clinical study of 242 cases. Interact Cardiovasc Thorac Surg 2007;6:636–9. http://dx.doi.org/10.1510/icvts.2007.156554
Reardon MJ, Smythe WR. Cardiac neoplasms. In: Cohen LH, Edmunds LH Jr (eds). Cardiac Surgery in the Adult. New York: McGraw Hill, 2003; pp. 1392.
Lynch M, Clements SD. Right sided cardiac tumours detected by transesophageal echocardiography and its usefulness in differentiating the benign from malignant ones. Am J Cardiol 1979;6:781–4.
Cotran RS, Kumar V, Robbins SL. Hemodynamic disorders and shock. In: Schoen FJ (ed). Robbin’s Pathologic Basis of Disease. Philadelphia: WB Saunders, 1994; pp. 105–06.
Konkle BA, Schaffer AI. Hemostasis, thrombosis, fibrinolysis and cardiovascular disease. In: Zipes DP, Libby P, Bonow RO, Braunwald E (eds). Braunwald’s Heart Disease. Philadelphia: Elsevier Saunders, 2005; pp. 2075.
Lanjewar DN, Ramraje S, Lanjewar SD. Right atrial appendage thrombus with atrial infarct in a case of thyrotoxicosis: an autopsy report. Indian J Pathol Microbiol 2010;53:538–40. http://dx.doi.org/10.4103/0377-4929.68295
Toda R, Yuda T, Nishida T, Toyohira H, Taira A. Right atrial mural thrombus associated with pericarditis. Ann Thorac Surg 1996;62:1505–06. http://dx.doi.org/10.1016/0003-4975(96)00399-2
Turgut O, Yalta K, Yilmaz MB, Dizman R, Tandogan I. Free-floating biatrial thrombi with concomitant saddle pulmonary embolism. Int J Cardiol 2010;144:e11–e13. http://dx.doi.org/10.1016/j.ijcard.2008.12.035
Masqura VX, Marini M, Portela F, Cao I. A complication of classical Fontan operation: giant right atrial thrombus and massive pulmonary thromboembolism. J Card Surg 2008;23:776–8. http://dx.doi.org/10.1111/j.1540-8191.2008.00656.x
Hedrick M, Elkins RC, Knott-Craig CJ, Razook JD. Successful thrombectomy for thrombosis of the right side of the heart after the Fontan operation. Report of two cases and review of the literature. J Thorac Cardiovasc Surg 1993;105:297–301.
Motovska Z, Widimsky P, Bilkova D, Penicka M. An embolus in the right atrium caught in the Chiari network and resistant to thrombolysis. J Thromb Thrombolysis 2010;30:114–18. http://dx.doi.org/10.1007/s11239-009-0403-6
Eweda II, Samir S, Abbas O, El-Gohary GM, Nammas W. Right heart thrombus-in-transit with pulmonary embolism in a patient with primary hypercoagulable state. Cardiol J 2010;17:408–11.
Nanjappa MC, Shankarappa RK, Kalpana SR, Bhat P, Moorthy N. Intracardiac thrombi in acute myeloid leukemia: an echocardiographic and autopsy correlation. Echocardiography 2010;27:E4–E8. http://dx.doi.org/10.1111/j.1540-8175.2009.01047.x
Chun KR, Bansch D, Bauer R, Schneider C, Kuck KH. Massive right atrial thrombus due to heparin-induced thrombocytopenia type II. Herz 2008;33:464–5. http://dx.doi.org/10.1007/s00059-008-3165-6
Morgan JA, Kherani AR, Vigilance DW, Cheema FH, Colletti NJ, Sahar DI. Off-pump right atrial thrombectomy for heparin-induced thrombocytopenia with thrombosis. Ann Thorac Surg 2003;76:615–17. http://dx.doi.org/10.1016/S0003-4975(03)00159-0
Sabharwal P, Ruggles S, Gharagozloo F. Right atrial thrombus in a patient with stage IV carcinoma of the lung: is the surgical treatment the correct choice? J Cardiovasc Surg 1998;39:689–90.
Zia-ur-Rehman, Alvi AR, Bibi S. Hepatic vein and inferior vena cava thrombus extending into the right atrium: a rare complication of amoebic abscess. J Coll Physicians Surg Pak 2010;20:57–9.
Tasdemir K, Sarli B, Kaya MG, Gunebakmaz O. Mobile biatrial thrombus in a patient with mitral stenosis under heparin infusion. Interact Cardiovasc Thorac Surg 2008;7:667–9. http://dx.doi.org/10.1510/icvts.2008.179093
Genc C, Uzun M, Yiginer O, Baysan O. Thrombus entrapped in a patent foramen ovale, causing only vague symptoms. Turk Kardiyol Dern Ars 2009;37:563–5.
Cakir C, Duygu H, Eren NK, Akyildiz ZI, Nazli C, Ergene O. Witnessing a rare event – thrombus seeking its route in the right atrium: “thrombus in transit”. J Cardiovasc Med 2008;9:1166–8. http://dx.doi.org/10.2459/JCM.0b013e328311eed8
Kinova E, Zlatareva N, Goudev A. Right atrial thrombus from inferior vena cava after acute cardiotoxicity of 5-Fluorouracil. Cardiol J 2008;15:284–5.
Gadomski A, Jaranowska D, Ebinger K, Ozimek W, Brzewski M. Right atrial thrombus complicating chemotherapy by central venous catheterization in a child with Hodgkin’s disease. Wiadomosci Lekarskie 1998;51:266–9.
Sakai T, Shimotsuma M, Yamada Y. A case of right atrial thrombus adhering to an intravenous hyperalimentation catheter. Rinsho Byori 2000;48:67–70.
Coleman DB, Debarr DM, Morales DL, Spotnitz HM. Pacemaker lead thrombosis with atrial thrombectomy and biventricular pacemaker and defibrillator insertion. Ann Thorac Surg 2004;78:e83–e84. http://dx.doi.org/10.1016/j.athoracsur.2003.09.115
Paupe A, Lenclen R, Blanc P, Chassevent J. Thrombosis of the right atrium after umbilical venous catheterization. Favourable outcome after early thrombectomy. Arch Fr Pediatr 1992;49:105–08.
Ghani MK, Boccalandro F, Denktas AE, Barasch E. Right atrial thrombus formation associated with central venous catheters utilisation in hemodialysis patients. Intensive Care Med 2003;29:1829–32. http://dx.doi.org/10.1007/s00134-003-1907-8
Vicol C, Nollert G, Mair H, Reichart B. Port-a-cath complicated by right atrial thrombus. Minimally invasive thrombectomy without cardiopulmonary bypass. Z Kardiol 2004;93:706–08. http://dx.doi.org/10.1007/s00392-004-0121-1
Nunez L, Celemin D, Larrea JL. Right atrial thrombosis caused by a Swan Ganz catheter. Presentation of 2 cases. Rev Esp Cardiol 1982;35:91–3.
Mestres CA, de lacy AM, Pomar JL. Massive right atrial and ventricular thrombosis after peritoneovenous shunting treated by thrombectomy and tricuspid valvectomy. Ann Thorac Surg 1987;44:205–06. http://dx.doi.org/10.1016/S0003-4975(10)62045-0
Kentos A, Dufaye P, Jacobs F, De Smet JM, Serruys E, Thys JP. Candida albicans septic thrombosis of the right atrium is associated with a central venous catheter. Clin Infect Dis 1995;21:440–2. http://dx.doi.org/10.1093/clinids/21.2.440
Sontiseni SP, White M, Singh S et al. Thrombectomy reduces the systemic complications in device-related right atrial septic thrombosis. Can J Cardiol 2009;25:e36–e41. http://dx.doi.org/10.1016/S0828-282X(09)70482-9
Yang JY, Williams S, Brandao LR, Chan AK. Neonatal and childhood right atrial thrombosis: recognition and a risk-stratified treatment approach. Blood Coagul Fibrinolysis 2010;21:301–07. http://dx.doi.org/10.1097/MBC.0b013e3283333c7c
Aksu T, Güler ET, Tüfekçioglu O, Aksu AO. Thrombi in the right atrium and inferior vena cava mimicking myxoma in a patient with recurrent pulmonary thromboembolism. Turk Kardiyol Dern Ars 2008;36:555–7.
Khurana A, Tak T. Venous thromboembolic disease presenting as inferior vena cava thrombus extending into the right atrium. Clin Med Res 2004;2:125–7. http://dx.doi.org/10.3121/cmr.2.2.125
Cotran RS, Kumar V, Robbins SL. The heart. In: Schoen FJ (ed). Robbin’s Pathologic Basis of Disease. Philadelphia: WB Saunders, 1994;569.
A ‘practical guide’ to the new oral anticoagulants that have recently become available as an alternative to warfarin for patients with atrial fibrillation has been issued by the European Heart Rhythm Association (EHRA) of the European Society of Cardiology (ESC).
The guide, which has been published online in the European Heart Journal and Europace, covers four new oral anticoagulants: dabigatran, rivaroxaban and apixaban (which are all now on the market for AF), and edoxaban, which is included provisionally, as it is not yet approved.
The guide notes that: “Both physicians and patients will have to learn how to use these drugs effectively and safely in clinical practice,” and “Many unresolved questions on how to optimally use these drugs in specific clinical situations remain”.
It sets out 15 clinical scenarios and gives “as practical answers as possible” for each one. The topics are:
Practical start-up and follow-up scheme for patients on new anticoagulants
How to measure the anticoagulant effect of the new drugs
Drug–drug interactions and
pharmacokinetics
Switching between anticoagulant regimens
Ensuring compliance
How to deal with dosing errors
Patients with chronic kidney disease
What to do if there is a (suspected) overdose without bleeding, or a clotting test is indicating a risk of bleeding?
Management of bleeding complications
Patients undergoing a planned surgical intervention or ablation
Patients undergoing an urgent surgical intervention
Patients with AF and coronary artery disease
Cardioversion
Patients presenting with acute stroke
Patients with a malignancy.
Since new information is becoming available at a rapid pace, the guide will be updated regularly on the EHRA website.
The full guide is available at: Europace 2013;15:625-51; and Eur Heart J (published online 26th April 2013, doi:10.1093/eurheartj/eht134).
The European Society of Cardiology has issued a consensus statement, which says that catheter-based renal denervation can be considered a therapeutic option in patients with drug-resistant hypertension who cannot get to goal with a combination of lifestyle and pharmacologic therapy.
The statement, published online in the European Heart Journal (25th April 2013, doi: 10.1093/eurheartj/eht154), is written by a committee led by Dr Felix Mahfoud (Saarland University, Saar, Germany). They state that the data support the concept that radiofrequency ablation of the renal nerves reduces blood pressure and improves blood-pressure control in these difficult-to-treat patients, with results now extending to 36 months.
The statement also reviews the appropriate screening measures necessary to select patients eligible for renal denervation. These are:
office-based blood pressure >160 mmHg (>150 mmHg in patients with type 2 diabetes)
use of three or more antihypertensive drugs in adequate dosage and combination, including use of a diuretic
have attempted to modify blood pressure with lifestyle changes
secondary hypertension has been excluded
pseudoresistance has been excluded with the use of ambulatory blood-pressure monitoring
patients have preserved renal function (glomerular filtration rate >45 ml/min/1.732)
absence of polar or accessory arteries, no renal artery stenosis, and no prior renal revascularisation.
The statement acknowledges that it is not yet clear how renal denervation works, but the mechanism is likely the result of a reduction in peripheral resistance, reduced renin release, and favourable changes in water and salt handling. “The fact that renal denervation also reduces whole-body sympathetic-nerve activity suggests that this therapy may also be beneficial in other clinical states characterised by sympathetic nervous system activation – this may ultimately lead to new indications,” it says.
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits