A 73-year-old woman, with a history of deep vein thrombosis (DVT) in her legs, presented two years following coronary artery bypass graft (CABG) with left internal mammary artery (LIMA), left radial artery and left cephalic vein, with a massive right atrial mass. Pre-operative work up also showed a left adrenal mass on computed tomography (CT) scan. We discuss the diagnostic possibilities within such a scenario and review the literature for right atrial masses of diverse aetiology, including right atrial myxomas, benign and malignant tumours of right atrium and right atrial thrombosis. The case is unusual on account of the concomitant history of DVT and the presence of left adrenal mass, rapid growth of the mass within two years following CABG, the atypical origin of the myxoma near inferior vena caval opening and the near total obliteration of the right atrial myxoma by rapid growth of myxoma to a massive size.
Case presentation
A 73-year-old woman presented with six-month history of progressively worsening exertional shortness of breath. The patient had previously undergone coronary artery bypass grafting (CABG) two years ago for symptomatic, severe, left-sided coronary artery disease using left internal mammary artery (LIMA) graft to left anterior descending (LAD) artery, left radial artery to obtuse marginal branch of circumflex artery and left cephalic vein graft to diagonal branch of LAD artery with good symptomatic relief. The choice of conduits at the initial operation had been dictated by a history of deep vein thrombosis (DVT) and varicose veins in both legs.

On examination, she had engorged neck veins but little else of note. Chest X-ray and electrocardiogram (ECG) were unremarkable. Echocardiogram showed a large right atrial mass filling up almost the whole of the right atrium, part of which prolapsed through the tricuspid valve opening during diastole. The mass seemed to arise from the inferior surface of right atrium very close to the inferior vena caval opening (figure 1). Computed tomography (CT) scan confirmed the presence of a large right atrial mass (figure 2), no secondary pulmonary emboli and a left adrenal mass (figure 3), the significance of which was unclear. Magnetic resonance imaging (MRI) confirmed the presence of large right atrial mass, with its origin from the inferior surface of the right atrium close to the inferior vena caval opening. Intraoperative transoesophageal echocardiography (TOE) pictures were equally striking and further delineated the sheer massive size of the mass, occupying the whole of the right atrium, arising from the inferior wall of the right atrium close to the inferior vena cava and prolapsing through the tricuspid valve into the right atrium (figure 4).
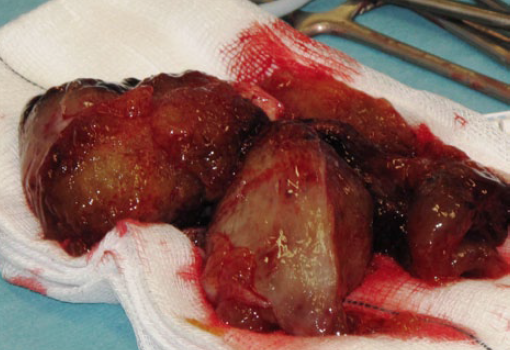
After secondary median sternotomy and dissection of heart, in general, and right atrium and ascending aorta, in particular, cardiopulmonary bypass was instituted with right femoral and direct superior and inferior vena caval cannulations. Right atrium was opened by a long oblique incision, with heart beating, and the large mass visualised (figure 5).This was adherent by a broad attachment to the inferior surface of the right atrium just above the inferior vena cava. The mass was excised completely, along with its attachment to the right atrial wall with a circumferential 1 cm clearance (figure 6). Tricuspid valve and right ventricle were inspected for additional masses. Primary right atrial closure was performed and bypass terminated.
Patient made uncomplicated recovery and was discharged home in a week. Postoperative CT scan of chest was normal and did not show, in particular, any secondary lung masses. Echocardiogram of the heart showed complete clearance of the mass and no residual masses in the heart chambers. Histopathology of the mass confirmed myxoma. On six-week follow-up, patient was asymptomatic and had made good recovery.
Discussion
Myxomas

A right atrial mass following CABG, two years earlier, in a patient with previous history of DVT and a suspicious shadow in the left adrenal gland could be a benign tumour, a malignant primary or secondary tumour, or a thrombus.
Approximately 75% of primary cardiac tumours are benign: 50% of benign tumours are myxomas, and 10–20% of all myxomas arise from the right atrium. About 95% of myxomas arise sporadically, are more common in middle aged women, are unassociated with other abnormal conditions, do not recur after adequate excision and 80% of these have a normal DNA genotype. About 5%, in contrast, show a familial pattern of tumour development based on autosomal dominance inheritance, are present in younger patients and equally likely to present in males. They have multi-centric origin (22%), higher recurrence rates after excision (21–67%), and, in 20% of patients, associated abnormalities like testicular, pituitary, adrenocortical, breast or skin tumours or pigmented spots may be present.1 Carney complex is an inherited autosomal dominant disorder with marked familial trend, found in younger patients, comprising atypical myxomas and extracardiac involvement including pigmented skin lesions, cutaneous myxomas, adrenal cortical disease, myxoid mammary fibroadenomas, testicular tumours, pituitary adenomas, melanotic schwanommas and thyroid disease.2-4

Common clinical presentation of myxomas in general includes intracardiac obstruction with cardiac failure (67%), thromboembolism (29%), and constitutional and immunological symptoms (22%), with most patients having multiple symptoms. Grossly, two-thirds of myxomas are relatively compact and polypoid and unlikely to fragment spontaneously,5 while the other one-third are gelatinous and fragile and, thus, prone to fragmentation and embolisation.6 Histologically, myxomas are composed of polygonal cells with irregular, slightly hyperchromatic nuclei without mitoses, containing parallel filaments similar to the contractile components of the smooth muscle cells, seen in particular abundance in the region of fossa ovalis in the left atrium. These polygonal cells with vasoformative tendencies are found with primitive capillaries and foci of extramedullary haematopoeisis within an acid mucopolysaccharide myxoid matrix containing, in addition, reticulocytes, smooth muscle cells and elastic and collagen deposits, with, in 10% of patients, foci of calcium and metaplastic bone.7
Traditionally, myxomas have been thought to arise from the multi-potential mesenchymal cells present in the endocardium of the atrial septum in the fossa ovalis region,8 although Krikler suggested origin from endocardial sensory nerve tissue, based on identification of three neuroendocrine markers in 24 excised atrial myxomas.9 There have been increasing reports documenting the malignant potential of the myxomas with respect to local invasion of vessel wall, recurrence, independent growth and distant metastases.10-12
Right atrial myxomas demonstrate a wide spectrum of histomorphological diversity. Mallick et al. reported prominent glandular differentiation mimicking a metastatic adenocarcinoma in a 10-year-old child.13 Hwang et al. described a large, thin-walled, cystic mass filled with arterial blood arising by a broad base between superior vena cava and the appendage.14 Fox et al. reported a right atrial myxoma associated with vascular malformation supplied by the right coronary artery.15

While the most common site of origin continues to be the interatrial septum, as in the more common left atrial myxomas, origin from the free wall with phrenic stimulation,16 from tricuspid valve,17 and from suprahepatic vena cava associated with asplenia,18 have been described. In a comprehensive review of over 100 cases of Myxoma syndrome or Carney’s complex, Edwards et al. described the occurrence of right atrial myxomas in as many as 44%, multiple myxomas in 41% and a 20% incidence of recurrence. They recommended four-chamber examination of heart at surgery for atypical myxomas by a right atriotomy and combined superior transseptal approach, careful screening of the first-degree relatives and careful long-term follow-up.3 While a large number of right atrial myxomas may be asymptomatic, presentation with tricuspid valve obstruction,19 pulmonary embolism20 with cor pulmonale,21 Budd- Chiarri syndrome with hepatic and portal vein thrombosis and ascites,22 and, finally and unusually, with infection of the mass,23 have been described. Pulmonary embolism is a particularly dreaded complication of right atrial myxoma, and pulmonary seeding should be assiduously sought and excluded by CT scan before embarking on surgery.24,25 Canale et al. described right atrial myxoma excision and bilateral pulmonary embolectomy, utilising a brief period of circulatory arrest, in a patient presenting with tricuspid obstruction.20
Other tumours
Other benign tumours that can arise from right atrium are lipomas, lipomatous hypertrophy of interatrial septum, papillary fibroelastoma of tricuspid valve and haemangioma.26
Secondary metastatic tumours of the heart are 20 to 40 times more common than the primary malignancies,27 and almost 10% of all metastatic tumours eventually reach the heart or mediastinum.28 Although every type of malignant tumour has been known to involve the heart, leukaemia and melanoma comprised 53.9% and 34% of all metastatic disease in one large series.29 Lung cancer, sarcoma, breast cancer, oesophageal cancer, ovarian cancer and renal cancer comprised 10.2%, 9.2%, 8.3%, 7.7%, 5.7% and 5.3%, respectively, in a large series.29 Cardiac involvement by prostatic or gastrointestinal tumours, with the exception of carcinoid tumours, is rare. Carcinoid heart disease involves white fibrous deposits on the tricuspid and pulmonary valves causing predominantly tricuspid regurgitation and pulmonary stenosis in patients with primary tumours arising from the argentaffin cells of the ileum, pancreas, biliary vessels, ovary or testes, complicated by hepatic metastases.30 Lymphomas are known to involve the pericardium and not specifically the heart.29 On the other hand, in a large Chinese study of 33,108 open-heart operations and 242 cardiac tumours, all the secondary cardiac tumours were located to the right side of the heart.31 The most common mode of metastatic spread to the heart is haematogenous, although lymphatic, inferior vena caval and pulmonary venous spread and spread through direct extension of lung, oesophageal, thymic and breast tumours is well recognised. Renal, hepatic, adrenal and uterine malignancies spread into the right atrium through inferior vena cava. As many as 10% of all renal malignancies involve inferior vena cava and 40% of these invade the right atrium.32

About 25% of all primary cardiac tumours are malignant, and angiosarcomas, which have a predilection for the right heart, constitute 33% of all malignant tumours. Right atrium may also be involved by malignant mesothelioma or fibrosarcoma. Lynch et al. reported 18 right-sided tumours of the heart over a sevenyear period, out of which, 15 involved right atrium, comprising five hypernephromas, four myxomas, two angiosarcomas, and one each of lipoma, cavernous haemangioma, hepatoma and chondrosarcoma.33
Intracardiac thrombosis
Endocardial injury, stasis or turbulence of blood flow and hypercoagulability of blood are the three classical factors that predispose, in general, to intracardiac thrombosis.34 Endocardial injury may result from transmural myocardial infarcts, myocardial infections, immunological myocardial reactions, inflammatory valve disease, prosthetic heart valves with or without complications, radiation, chemotherapeutic agents, instrumentation, bacterial toxins or endotoxins and immunological insults, as in transplant rejection.34
Generally, stasis contributes more to venous thromboembolism, while turbulence predisposes to arterial and intracardiac thrombosis, but considerable overlap is seen in many clinical situations. In myocardial infarction, in addition to endocardial injury, there is an element of stasis due to failure of necrotic muscle to contract.
In mitral and tricuspid stenoses, atria empty inadequately. When atrial fibrillation supervenes, there is further stasis and turbulence and a great potential for atrial and auricular thrombosis. Hyperviscosity syndromes, like polycythaemia, cryoglobulinaemia, macroglobulinaemia and sickle cell anaemia, partly act through promoting stasis. Hypercoagulability per se is an unusual cause of intracardiac thrombosis and can be primary, due to a genetic defect in one or several coagulation proteins, or secondary, occurring in a variety of clinical conditions associated with recurrent thrombosis.
Primary or genetic causes of hypercoagulability mainly include deficiencies in antithrombin III, protein C, protein S and fibrinolytics, factor V Leiden gene mutation and prothrombin gene mutation.35 Secondary causes include cancer, acute leukaemia, myeloproliferative disorders, nephrotic syndrome, oral contraceptives, pregnancy, disseminated intravascular coagulation (DIC), thrombotic thrombocytopenia, antiphospholipid antibody syndrome, homocystinuria, thrombocytosis, sickle cell anaemia, systemic lupus erythematosus (SLE) and others.34
While right atrial thrombosis shares in some of the aetiological narrative of thrombosis mentioned above, there are important differences as well. Right atrial thrombosis has been described with DVT of leg and pelvic veins, atrial fibrillation,36 constrictive pericarditis with tricuspid thrombotic obstruction37 and non-specific pericarditis,38 restrictive cardiomyopathy,39 and after Fontan operation.40,41 Genetic causes like methylenetetrahydrofolate (MTHF) reductase gene polymorphism,42 hypercoagulability characterised by factor V Leiden gene, thrombophilia genes and high serum homocysteine,43 myeloid leukaemia,44 heparin-induced thrombocytopenia,45,46 lung cancer47 and amoebic liver abscess,48 have all been reported with right atrial thrombosis. Biatrial thrombosis with mitral stenosis and leg DVT treated with mitral valve replacement and bi-atrial thrombectomy has been reported.49
On the other hand, there are reports of bi-atrial thrombosis across a patent foramen ovale, with resolution following anticoagulation.50 Some of the right atrial thrombi might be entrapped ‘in transit’ across a patent foramen ovale.43,51 However, the most common causes of right atrial thrombosis relate to the host of artificial devices inserted into the right atrium for a variety of indications. These include central venous catheters and Hickman lines for longterm use for antibiotics, hyperalimentation52 and chemotherapy,53,54 pulmonary artery catheters,55 permanent pacemaker56 and defibrillator leads,57 umbilical catheters,58 dialysis catheters59 and port-a-caths,60 extracorporeal membrane oxygenation (ECMO) catheters,61 and ventriculoatrial shunts for hydrocephalus62 or peritoneovenous shunts for intractable recurrent malignant ascites.63
Some of the device-related thrombosis has a septic component to it.64,65 Yang et al. reviewed the available literature on right atrial thrombosis in 2010 and identified 122 cases: 91% of patients had central venous catheters, 40.8% were premature, 27.2% were postcardiac surgery patients, 19.2% had underlying malignancies and 45.6% of patients received intravenous hyperalimentation.66 Aksu et al. and Khurana et al. separately described two inferior cavo-atrial masses with pulmonary thromboembolism masquerading as myxomas and vegetations, where histopathology revealed thrombus.67,68
A solitary unilateral adrenal mass may be a cyst, an adenoma or a carcinoma. An adrenal cortical adenoma or carcinoma may be functional or non-functional. A cortisolsecreting adenoma or carcinoma gives rise to Cushing’s syndrome, an aldosterone-secreting adenoma (Conn’s syndrome) or carcinoma leads to primary hyperaldosteronism, and an androgen-secreting adrenal cortical carcinoma can cause the virilising adrenogenital syndrome. Again there might be non-functional cortical adenomas or carcinomas, but these are much less common. Adrenal medullary tumours include phaeochromocytomas, neuroblastomas, ganglioneuromas and variants of these neoplasms.69
Our patient had a massive right atrial mass arising from the inferior right atrial wall very close to the inferior vena caval opening. In the presence of a left adrenal mass shadow, there was a possibility of an adrenal metastasis coming up the renal vein and inferior vena cava into the right atrium. In light of her previous history of leg DVT and CABG, a right atrial thrombosis could not be entirely ruled out.
Between 10 and 20% of myxomas arise from the right atrium and, although origin from the inferior wall close to inferior vena cava is unusual, there are at least two case reports of origin from the inferior vena cava.18 This atypical origin further increased the diagnostic doubt. Origin of the tumour near the inferior vena caval opening and filling up of the whole of the right atrium by the myxoma made direct cannulation of the cavae mandatory and direct cannulation of supradiaphragmatic inferior vena cava difficult, but in the event it was possible to negotiate a Pacifico size 24 F venous cannula into the inferior vena cava just below the tumour, and the tumour was excised in its entirety, along with the adjoining right atrial wall close to the inferior vena cava, with adequate tumour clearance, while the heart was beating without aortic cross clamp.
Had the direct inferior vena cava cannulation not been possible due to involvement by the tumour, the tumour would have to be excised under profound hypothermia with low flows or circulatory arrest. A thrombus would have mandated excision with or without an inferior vena cava filter and aggressive postoperative anticoagulation. An adrenal metastasis would have required an in-continuity excision of the left adrenal gland and suprarenal veins. An on-table TOE confirmed absence of concomitant myxomas elsewhere in cardiac chambers, as well as complete removal of tumour. A pre-operative CT scan had ruled out any pulmonary emboli and postoperative CT scan excluded any spilling of myxomatous debris in pulmonary circulation. All three grafts including LIMA to LAD, left radial artery to obtuse marginal branch of circumflex artery and, specifically, left cephalic vein to diagonal artery were patent.
Conflict of interest
None declared.
References
- Carney JA. Differences between nonfamilial and familial cardiac myxoma. Am J Surg Pathol 1985;64:53–5. http://dx.doi.org/10.1097/00000478-198501000-00009
- Lee B, Sir JJ, Park SW. Right sided myxomas with extramedullary hematopoeisis and ossification in Carney complex. Int J Cardiol 2008;130:e63–e65. http://dx.doi.org/10.1016/j.ijcard.2007.11.061
- Edwards A, Bermudez C, Piwonka G, et al. Carney’s syndrome: complex myxomas. Report of four cases and review of literature. Cardiovasc Surg 2002;10:264–75. http://dx.doi.org/10.1016/S0967-2109(01)00144-2
- Affronti A, Di Bella I, Prontera P, Da Col U. Obstruction of the tricuspid valve orifice by a huge right atrial myxoma associated with the Carney complex: a case report. J Cardiac Surg 2010;25:674–6. http://dx.doi.org/10.1111/j.1540-8191.2010.01114.x
- McAllister HA, Fenoglio JJ. Tumours of the cardiovascular system, atlas of tumour pathology, series 2. Washington DC: Armed Forces Institute of Pathology, 1978;2:pp. 20.
- Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma: a series of 112 consecutive cases. Medicine 2001;80:159–72. http://dx.doi.org/10.1097/00005792-200105000-00002
- Prichard RW. Tumours of the heart: review of the subject and report of one hundred and fifty cases. Arch Pathol 1951;51:98–128.
- Lie JT. The identity and histogenesis of cardiac myxomas: a controversy put to rest. Arch Pathol Lab Med 1989;113:724–6.
- Krikler DM, Rode J, Davies MJ. Atrial myxoma: a tumour in search of its origins. Br Heart J 1992;67:89–91. http://dx.doi.org/10.1136/hrt.67.1.89
- Pastakia B. Malignant atrial myxoma presenting as intracranial mass. Chest 1979;75:531–2. http://dx.doi.org/10.1378/chest.75.4.531
- Read RC, White HJ, Murphy ML, Williams D, Sun CN, Flanagan WH. The malignant potentiality of left atrial myxoma. J Thorac Cardiovasc Surg 1974;68:857–68.
- Seo IS, Warner TF, Colyer RA, Winkler RF. Metastasizing atrial myxoma. Am J Surg Pathol 1980;4:391–9. http://dx.doi.org/10.1097/00000478-198008000-00008
- Mallick SR, Das P, Shukla B, Kothari S. Right atrial myxoma with glandular differentiation. A rare entity in pediatric age group. Ann Pediatr Cardiol 2010;3:159–62. http://dx.doi.org/10.4103/0974-2069.74046
- Hwang JJ, Lien WP, Kuan P, Hung CR, How SW. Atypical myxoma. Chest 1991;100:550–1. http://dx.doi.org/10.1378/chest.100.2.550
- Fox JJ, Bonavita GJ, Sethi V. Right atrial myxoma associated with vascular malformation and atypical chest pain. Catheter Cardiovasc Diagn 1992;26:127–9. http://dx.doi.org/10.1002/ccd.1810260210
- Fatimi SH, Deedar-Ali-Khwaja R, Kiani SK. Imaging and intervention of paraneoplastic effect of a right atrial myxoma on factor VII activity levels. Ann Thorac Surg 2011;91:278–81. http://dx.doi.org/10.1016/j.athoracsur.2010.06.120
- Vizzardi E, D’Aloia A, Chiari E, Nardi M. Tricuspid valve myxoma in a patient with congestive heart failure. Cases J 2010;3:21. http://dx.doi.org/10.1186/1757-1626-3-21
- Elmusa K, Haddad R, Arnaut MS. Atypical and unusual myxoma. J Med Liban 2004;52:48–50.
- Azevedo O, Aleida J, Nolasco T, Medeiros R. Massive right atrial myxoma presenting as syncope and exertional dyspnea: case report. Cardiovasc Ultrasound 2010;8:23. http://dx.doi.org/10.1186/1476-7120-8-23
- Canale LS, Colafranchesci AS, Leal Botelho ES, de Oliveira Monteiro AJ. Surgical treatment of right atrial myxoma complicated with pulmonary embolism. Interact Cardiovasc Thorac Surg 2009;9:535–6. http://dx.doi.org/10.1510/icvts.2009.206318
- Lorentz MN, Vrandecic EC, Drumond LF, Soares RR. Right atrial myxoma associated with acute cor pulmonale. Case report. Rev Bras Anestesiol 2008;58:169–72.
- Anagnostopoulos GK, Marganitis G, Kostopoulos P, Papadopoulou G. Budd-Chiari syndrome and portal vein thrombosis due to right atrial myxoma. Ann Thorac Surg 2004;78:333–4. http://dx.doi.org/10.1016/S0003-4975(03)01265-7
- Puvaneswary M, Thompson D. Magnetic resonance imaging of an infected right atrial myxoma. Australas Radiol 2001;45:501–03. http://dx.doi.org/10.1046/j.1440-1673.2001.00963.x
- Daga CB, Gonzalez CM, Ortas NR, Ferreira MI. Pulmonary embolism and myxoma of right atrium. An Med Interna 2005;22:478–80.
- Idir M, Oysel N, Guibaud JP, Labouyrie E, Roudaut R. Fragmentation of a right atrial myxoma presenting as pulmonary embolism. J Am Soc Echocardiogr 2000;13:61–3.
- Kouchoukus NT, Blackstone EH, Doty DB, Hanley FL, Karp RB. Kirklin/Barrat-Boyes cardiac surgery. Philadelphia: Churchill Livingstone, 2003; pp. 1922.
- Hallahan ED, Vozelzang NJ, Borow KM. Cardiac metastasis from soft tissue sarcomas. J Clin Oncol 1986;4:1662–9.
- Fine G. Neoplasms of the pericardium and heart. In: Gould SE (ed). Pathology of the Heart and Blood Vessels. Springfield, IL: Charles C Thomas, 1968; pp. 851.
- Perry MC. Cardiac metastasis. In: Kapoor AS (ed). Cancer and the Heart. New York: Springer-Verlag Publishers, 1986. http://dx.doi.org/10.1007/978-1-4612-4898-9_7
- Roberts WC. A unique heart disease associated with a unique cancer: carcinoid heart disease. Am J Cardiol 1997;80:251. http://dx.doi.org/10.1016/S0002-9149(97)00340-8
- Yu K, Liu Y, Wang H, Hu S, Long C. Epidemiological and pathological characteristics of cardiac tumours: a clinical study of 242 cases. Interact Cardiovasc Thorac Surg 2007;6:636–9. http://dx.doi.org/10.1510/icvts.2007.156554
- Reardon MJ, Smythe WR. Cardiac neoplasms. In: Cohen LH, Edmunds LH Jr (eds). Cardiac Surgery in the Adult. New York: McGraw Hill, 2003; pp. 1392.
- Lynch M, Clements SD. Right sided cardiac tumours detected by transesophageal echocardiography and its usefulness in differentiating the benign from malignant ones. Am J Cardiol 1979;6:781–4.
- Cotran RS, Kumar V, Robbins SL. Hemodynamic disorders and shock. In: Schoen FJ (ed). Robbin’s Pathologic Basis of Disease. Philadelphia: WB Saunders, 1994; pp. 105–06.
- Konkle BA, Schaffer AI. Hemostasis, thrombosis, fibrinolysis and cardiovascular disease. In: Zipes DP, Libby P, Bonow RO, Braunwald E (eds). Braunwald’s Heart Disease. Philadelphia: Elsevier Saunders, 2005; pp. 2075.
- Lanjewar DN, Ramraje S, Lanjewar SD. Right atrial appendage thrombus with atrial infarct in a case of thyrotoxicosis: an autopsy report. Indian J Pathol Microbiol 2010;53:538–40. http://dx.doi.org/10.4103/0377-4929.68295
- Priestley KA, Wallwork J, Schofield PM. Right atrial thrombus in constrictive pericarditis. Int J Cardiol 1992;37:256–8. http://dx.doi.org/10.1016/0167-5273(92)90217-Q
- Toda R, Yuda T, Nishida T, Toyohira H, Taira A. Right atrial mural thrombus associated with pericarditis. Ann Thorac Surg 1996;62:1505–06. http://dx.doi.org/10.1016/0003-4975(96)00399-2
- Turgut O, Yalta K, Yilmaz MB, Dizman R, Tandogan I. Free-floating biatrial thrombi with concomitant saddle pulmonary embolism. Int J Cardiol 2010;144:e11–e13. http://dx.doi.org/10.1016/j.ijcard.2008.12.035
- Masqura VX, Marini M, Portela F, Cao I. A complication of classical Fontan operation: giant right atrial thrombus and massive pulmonary thromboembolism. J Card Surg 2008;23:776–8. http://dx.doi.org/10.1111/j.1540-8191.2008.00656.x
- Hedrick M, Elkins RC, Knott-Craig CJ, Razook JD. Successful thrombectomy for thrombosis of the right side of the heart after the Fontan operation. Report of two cases and review of the literature. J Thorac Cardiovasc Surg 1993;105:297–301.
- Motovska Z, Widimsky P, Bilkova D, Penicka M. An embolus in the right atrium caught in the Chiari network and resistant to thrombolysis. J Thromb Thrombolysis 2010;30:114–18. http://dx.doi.org/10.1007/s11239-009-0403-6
- Eweda II, Samir S, Abbas O, El-Gohary GM, Nammas W. Right heart thrombus-in-transit with pulmonary embolism in a patient with primary hypercoagulable state. Cardiol J 2010;17:408–11.
- Nanjappa MC, Shankarappa RK, Kalpana SR, Bhat P, Moorthy N. Intracardiac thrombi in acute myeloid leukemia: an echocardiographic and autopsy correlation. Echocardiography 2010;27:E4–E8. http://dx.doi.org/10.1111/j.1540-8175.2009.01047.x
- Chun KR, Bansch D, Bauer R, Schneider C, Kuck KH. Massive right atrial thrombus due to heparin-induced thrombocytopenia type II. Herz 2008;33:464–5. http://dx.doi.org/10.1007/s00059-008-3165-6
- Morgan JA, Kherani AR, Vigilance DW, Cheema FH, Colletti NJ, Sahar DI. Off-pump right atrial thrombectomy for heparin-induced thrombocytopenia with thrombosis. Ann Thorac Surg 2003;76:615–17. http://dx.doi.org/10.1016/S0003-4975(03)00159-0
- Sabharwal P, Ruggles S, Gharagozloo F. Right atrial thrombus in a patient with stage IV carcinoma of the lung: is the surgical treatment the correct choice? J Cardiovasc Surg 1998;39:689–90.
- Zia-ur-Rehman, Alvi AR, Bibi S. Hepatic vein and inferior vena cava thrombus extending into the right atrium: a rare complication of amoebic abscess. J Coll Physicians Surg Pak 2010;20:57–9.
- Tasdemir K, Sarli B, Kaya MG, Gunebakmaz O. Mobile biatrial thrombus in a patient with mitral stenosis under heparin infusion. Interact Cardiovasc Thorac Surg 2008;7:667–9. http://dx.doi.org/10.1510/icvts.2008.179093
- Genc C, Uzun M, Yiginer O, Baysan O. Thrombus entrapped in a patent foramen ovale, causing only vague symptoms. Turk Kardiyol Dern Ars 2009;37:563–5.
- Cakir C, Duygu H, Eren NK, Akyildiz ZI, Nazli C, Ergene O. Witnessing a rare event – thrombus seeking its route in the right atrium: “thrombus in transit”. J Cardiovasc Med 2008;9:1166–8. http://dx.doi.org/10.2459/JCM.0b013e328311eed8
- Kouchoukus NT, Blackstone EH, Doty DB, Hanley FL, Karp RB. Kirklin/Barrat-Boyes Cardiac Surgery. Philadelphia: Churchill Livingstone, 2003; pp. 1922.
- Kinova E, Zlatareva N, Goudev A. Right atrial thrombus from inferior vena cava after acute cardiotoxicity of 5-Fluorouracil. Cardiol J 2008;15:284–5.
- Gadomski A, Jaranowska D, Ebinger K, Ozimek W, Brzewski M. Right atrial thrombus complicating chemotherapy by central venous catheterization in a child with Hodgkin’s disease. Wiadomosci Lekarskie 1998;51:266–9.
- Sakai T, Shimotsuma M, Yamada Y. A case of right atrial thrombus adhering to an intravenous hyperalimentation catheter. Rinsho Byori 2000;48:67–70.
- Coleman DB, Debarr DM, Morales DL, Spotnitz HM. Pacemaker lead thrombosis with atrial thrombectomy and biventricular pacemaker and defibrillator insertion. Ann Thorac Surg 2004;78:e83–e84. http://dx.doi.org/10.1016/j.athoracsur.2003.09.115
- Kurisu S, Inoue I, Kawagoe T. Right atrial thrombosis after upgrading to a biventricular pacing/defibrillation system. Intern Med 2009;48:2101–04. http://dx.doi.org/10.2169/internalmedicine.48.2453
- Paupe A, Lenclen R, Blanc P, Chassevent J. Thrombosis of the right atrium after umbilical venous catheterization. Favourable outcome after early thrombectomy. Arch Fr Pediatr 1992;49:105–08.
- Ghani MK, Boccalandro F, Denktas AE, Barasch E. Right atrial thrombus formation associated with central venous catheters utilisation in hemodialysis patients. Intensive Care Med 2003;29:1829–32. http://dx.doi.org/10.1007/s00134-003-1907-8
- Vicol C, Nollert G, Mair H, Reichart B. Port-a-cath complicated by right atrial thrombus. Minimally invasive thrombectomy without cardiopulmonary bypass. Z Kardiol 2004;93:706–08. http://dx.doi.org/10.1007/s00392-004-0121-1
- Nunez L, Celemin D, Larrea JL. Right atrial thrombosis caused by a Swan Ganz catheter. Presentation of 2 cases. Rev Esp Cardiol 1982;35:91–3.
- Kiefer M, Eymann R. Huge thrombosis as consequence of VA-shunts. Acta Neurochir Suppl 2010;106:95–9. http://dx.doi.org/10.1007/978-3-211-98811-4_16
- Mestres CA, de lacy AM, Pomar JL. Massive right atrial and ventricular thrombosis after peritoneovenous shunting treated by thrombectomy and tricuspid valvectomy. Ann Thorac Surg 1987;44:205–06. http://dx.doi.org/10.1016/S0003-4975(10)62045-0
- Kentos A, Dufaye P, Jacobs F, De Smet JM, Serruys E, Thys JP. Candida albicans septic thrombosis of the right atrium is associated with a central venous catheter. Clin Infect Dis 1995;21:440–2. http://dx.doi.org/10.1093/clinids/21.2.440
- Sontiseni SP, White M, Singh S et al. Thrombectomy reduces the systemic complications in device-related right atrial septic thrombosis. Can J Cardiol 2009;25:e36–e41. http://dx.doi.org/10.1016/S0828-282X(09)70482-9
- Yang JY, Williams S, Brandao LR, Chan AK. Neonatal and childhood right atrial thrombosis: recognition and a risk-stratified treatment approach. Blood Coagul Fibrinolysis 2010;21:301–07. http://dx.doi.org/10.1097/MBC.0b013e3283333c7c
- Aksu T, Güler ET, Tüfekçioglu O, Aksu AO. Thrombi in the right atrium and inferior vena cava mimicking myxoma in a patient with recurrent pulmonary thromboembolism. Turk Kardiyol Dern Ars 2008;36:555–7.
- Khurana A, Tak T. Venous thromboembolic disease presenting as inferior vena cava thrombus extending into the right atrium. Clin Med Res 2004;2:125–7. http://dx.doi.org/10.3121/cmr.2.2.125
- Cotran RS, Kumar V, Robbins SL. The heart. In: Schoen FJ (ed). Robbin’s Pathologic Basis of Disease. Philadelphia: WB Saunders, 1994;569.
