The Government is soon to publicly disclose a league table for cardiac surgical units within National Health Service (NHS) England. While this information may be useful and raise questions as to why one unit may be better or worse than another, we are also to be made aware of surgeons who are performing significantly better or worse than expected in terms of risk-adjusted mortality. But are patient deaths following surgery caused exclusively by the surgeon, as surgeon-specific mortality data (SSMD) would imply? And is the surgeon with the lowest operative mortality the best doctor? In my opinion the answer to both these questions is a resounding no.
Dr Ravi De Silva (Papworth Hospital NHS Foundation Trust)
Many factors influence patient outcomes after surgery.1,2 Broadly speaking these may be categorised into factors present prior to hospital admission (e.g. comorbidities), factors occurring during the operation (e.g. technical error, unexpected operative findings), and factors occurring post-operatively (e.g. infections, medication error). A single individual is not able to control all of these variables, so patient deaths should not be attributed to an individual. The public may also be unaware that there exists great variation in the quantity and quality of staffing, expertise and equipment between hospitals. These infrastuctural inequalities are bound to effect patient outcomes, and are not accounted for in hospital league tables. Having moved from a safe, respected, cardiac centre to one that is soon to be acknowledged as the best by the criteria of risk-adjusted mortality, I have considerable insight into what, other than the surgeons, should make one institution have better mortality data than another.
Life-saving technology
Mechanical cardiac and/or respiratory support in the form of extra corporeal membrane oxygenation (ECMO) and ventricular assist devices (VADs) are well-established, highly effective, and may be used to support sick patients peri-operatively.3 They can provide a surgical safety net for the sickest patients. However, due to cost, very few hospitals in the NHS have been allowed to use these technologies, obviously disadvantaging patients in units where it is unavailable and potentially increasing mortality as a consequence.
Resident theatre team
Cardiac arrest following cardiac surgery invariably needs emergency re-sternotomy. Out of normal working hours many hospitals have on-call staff at home, needing travel time to attend the emergency. Other hospitals have staff on-site at all times. While the latter may be more costly and require a larger workforce, it is clearly an advantage in emergency situations.
Consultant-delivered care
Consultant delivered care is the aspiration for the modern NHS, and although this is achievable during normal working hours, in most heart units, overnight one consultant is in charge of all the patients in the critical care area, as well as, if needed, running an emergency operating theatre. Increased mortality for patients undergoing surgery out of normal working hours is well recognised.4 Other units have invested in larger workforces, allowing for multiple consultants to be on-call to cover different clinical areas, resulting in the sickest patients managed by the most experienced clinicians around the clock.
Alert teams
It is recognised that one of the main differentiators between hospitals is not how often patients encounter difficulties, but the ability to rescue patients from these situations.5,6 Many factors helping to rescue the patient have already been discussed. Another important contributor is adequate ward staff7 and the presence of an ‘alert team’, who closely manage and treat patients who become unwell, directly liaising with consultants and the intensive-care team. They are an additional tier of surveillance on the ward, and in my hospital the alert team have halved the incidence of cardiac arrest in ward patients.
The theatre team
Cardiac surgery involves a multi-skilled team of doctors and nurses. The patient may be operated on several body sites simultaneously, with junior doctors and allied health professionals (AHPs) all working under the supervision of a consultant surgeon. In the UK, the practice of AHPs performing surgical procedures was pioneered in cardiac surgery, although now commonplace in other specialties. Some hospitals do not have enough surgical AHPs to staff all theatres, this work being done by junior doctors or temporary staff from other hospitals. This can negatively impact on the quality of the operation. The surgical team is no different to any other high-performing team, consistency and familiarity with each other, are corner stones to excellent outcomes.
As a surgeon with better than expected results, working in the ‘best’ cardiac centre in the UK, I have nothing to hide. However, I feel strongly that SSMD is important for medical professionals but can be hugely misleading to the public. We must have a mechanism to identify and help failing surgeons, but unless there has been a criminal act, this information should be held by the professional bodies that are best placed to deal with it. Similarly, the ‘best’ surgeons may be very good doctors, but may also be extremely risk-averse,8 disadvantaging the sickest patients who may have the most to gain from an operation. We must appreciate that mortality is inherent in the health system, and the only way to improve it is to improve the system, using high-performing centres as benchmarks and templates. The complexity of modern medicine and why patients die in hospitals can be difficult for doctors to fathom, to throw this out to the general public is sensationalist and disingenuous. Hospital-specific data are better understood by the public, and should be used to improve infrastructure and funding, thereby reducing inequalities in the health service.
Conflict of interest
None declared.
References
1. Westaby S, De Silva R, Petrou M, Bond S, Taggart D. Surgeon specific mortality data disguise wider failings in delivery of safe surgical services. Eur J Cardiothoracic Surg 2015;47:341–5. http://dx.doi.org/10.1093/ejcts/ezu380
2. Shannon FL, Fazzalari FL, Theurer PF, Bell GF, Sutcliffe KM, Prager RL. A method to evaluate cardiac surgery mortality: phase of care mortality analysis. Ann Thorac Surg 2012;93:36–43. http://dx.doi.org/10.1016/j.athoracsur.2011.07.057
4. Aylin P, Alexandrescu R, Jen MH, Bottle A. Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ 2013;346:f2424. http://dx.doi.org/10.1136/bmj.f2424
5. Reddy HG, Shih T, Englesbe MJ et al. Analyzing “failure to rescue”: is this an opportunity for outcome improvement in cardiac surgery. Ann Thorac Surg 2013;95:1976–81. http://dx.doi.org/10.1016/j.athoracsur.2013.03.027
6. Ahmed EO, Butler R, Novick RJ. Failure-to-rescue rate as a measure of quality of care in a cardiac surgery recovery unit: a five-year study. Ann Thorac Surg 2014;97:147–52. http://dx.doi.org/10.1016/j.athoracsur.2013.07.097
7. Needleman J, Buerhaus P, Pankratz VS, Liebson CL, Steven SR. Nurse staffing an inpatient hospital mortality. N Engl J Med 2011;364:1037–45. http://dx.doi.org/10.1056/NEJMsa1001025
8. Hannan EL, Cozzens K, King SB, Walford G, Shah NR. The New York State cardiac registries: history, contributions, limitations and lessons for future efforts to assess and publically report healthcare outcomes. J Am Coll Cardiol 2012;59:2309–16. http://dx.doi.org/10.1016/j.jacc.2011.12.051
This is an audit of 10 Anglia region cardiac rehabilitation (CR) programmes against the British Association of Cardiovascular Prevention and Rehabilitation (BACPR) seven core standards. Methods included a questionnaire that encapsulated these standards, a SWOT (strengths, weaknesses, opportunities, threats) analysis and assessment of local outcomes.
Overall, all 10 CR services were compliant with the vast majority of basic standards set by BACPR but the audit also highlighted gaps in ideal care processes, such as a shortage of psychologists, occupational therapists and pharmacists, and inadequate audit processes. Local strengths were highlighted that will encourage future cross-pollination across the network. Outcomes were collected variably ad hoc but there was some consistency that CR across the region improved exercise tolerance, reduced anxiety and reduced smoking, but had little effect on blood pressure and body mass index, comparable to the national audit.
Anglia CR services were shown to be fit-for-purpose and there were local areas of excellence, but local areas of need and gaps in CR were highlighted that will cross-pollinate to improve all CR services in East Anglia.
Introduction
ACRAN healthcare team
Cardiac rehabilitation (CR) services are comprehensive, long-term programmes involving medical evaluation, prescribed exercise, cardiac risk factor modification, education and counselling. CR has been extensively reviewed in the literature,1 and, in patients after myocardial infarction, has been shown to reduce all-cause and cardiovascular mortality rates in a Cochrane review.2 However, it has also been shown by others to have little effect on outcomes.3
Doubts over the efficacy of CR have led commissioners to question the value of such services. While the debate continues, the Anglia region CR services (rebooted last year as the Alliance of Cardiac Rehabilitation Anglia Network [ACRAN] under new consultant cardiologist leadership) set out to, not only audit their services against a contemporary standard, but also to identify local areas of good practice for communal learning and service development. We sought to reassure commissioners and patients of the need and utility of CR. The British Association of Cardiovascular Prevention and Rehabilitation (BACPR) has previously prescribed the standards of what a CR programme should entail in its 2012 publication in which seven core standards are set out,4 and it was this standard we measured ourselves against.
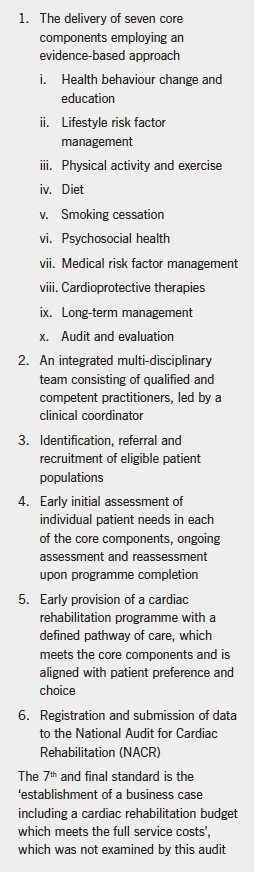
Box 1. The British Association of Cardiovascular Prevention and Rehabilitation (BACPR) Standards and Core Components for Cardiovascular Disease Prevention and Rehabilitation 2012
This is the first audit of all CR services presented in this way in this region, and this paper summarises the results of the audit presented as a half-day meeting organised by the East of England Clinical Network. There are 11 CR services across the Anglia region, of which 10 took part in this audit.
Methods
Audit of current services
A questionnaire was devised that encapsulated standards 1–6 of the BACPR 2012 document and was sent out to all CR service leads. This was designed by ACRAN Lead Consultant Cardiologist Dr Justin Zaman and edited by Jo Haywood, lead ACRAN CR Healthcare Professional and nurse at the Norfolk and Norwich University Hospital. For each standard, relevant questions were designed. The standards are listed in box 1.
The Anglia CR network local strengths
This part of the audit allowed each CR service to present briefly on their own services, to allow specialist skills and local issues to be aired. Such granularity would not be possible with the main regional audit presented above. The general format of each presentation was a SWOT (strengths, weaknesses, opportunities, threats) analysis followed by highlighting of a particular skill of that service, and if applicable, a patient case history or testimonial to give qualitative detail to the dry quantitative audit presented above.
Outcome data and future challenges
We, as a region, further looked at local outcomes that individual services collected – not all services can input into the national audit funded by the British Heart Foundation and run by the University of York and the UK government’s Health and Social Care Information Centre (National Audit of Cardiac Rehabilitation, NACR). We looked at data from 1 April 2014 to 30 September 2014 (quarters 1 and 2) for all 10 services. In particular, we looked at outcome data showing changes in physical activity, psychological health, behaviours like smoking, and also biological parameters, such as weight loss and change in blood pressure.
Results
Audit of current services
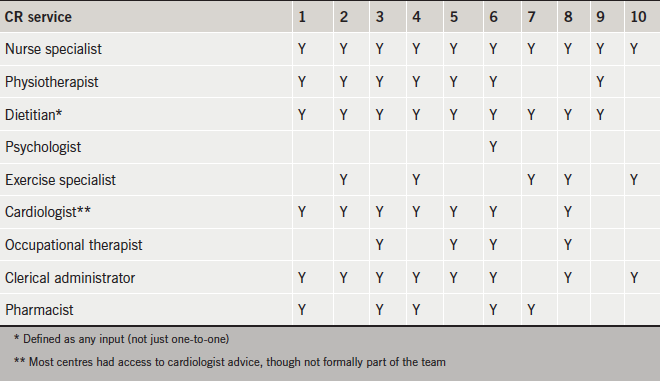
The results from these CR services are presented in tables. Table 1 shows that there was a tendency for a shortage of psychologists, occupational therapists and pharmacists in CR teams (BACPR stipulate an ideal CR team needs a cardiologist/community cardiologist/physician or general practitioner with special interest, nurse specialist, physiotherapist, dietitian, psychologist, exercise specialist, occupational therapist and clerical administrator) – however, most teams had a nurse, physiotherapist/exercise specialist and also administrative support.
Table 1. Constitution of the cardiac rehabilitation (CR) team
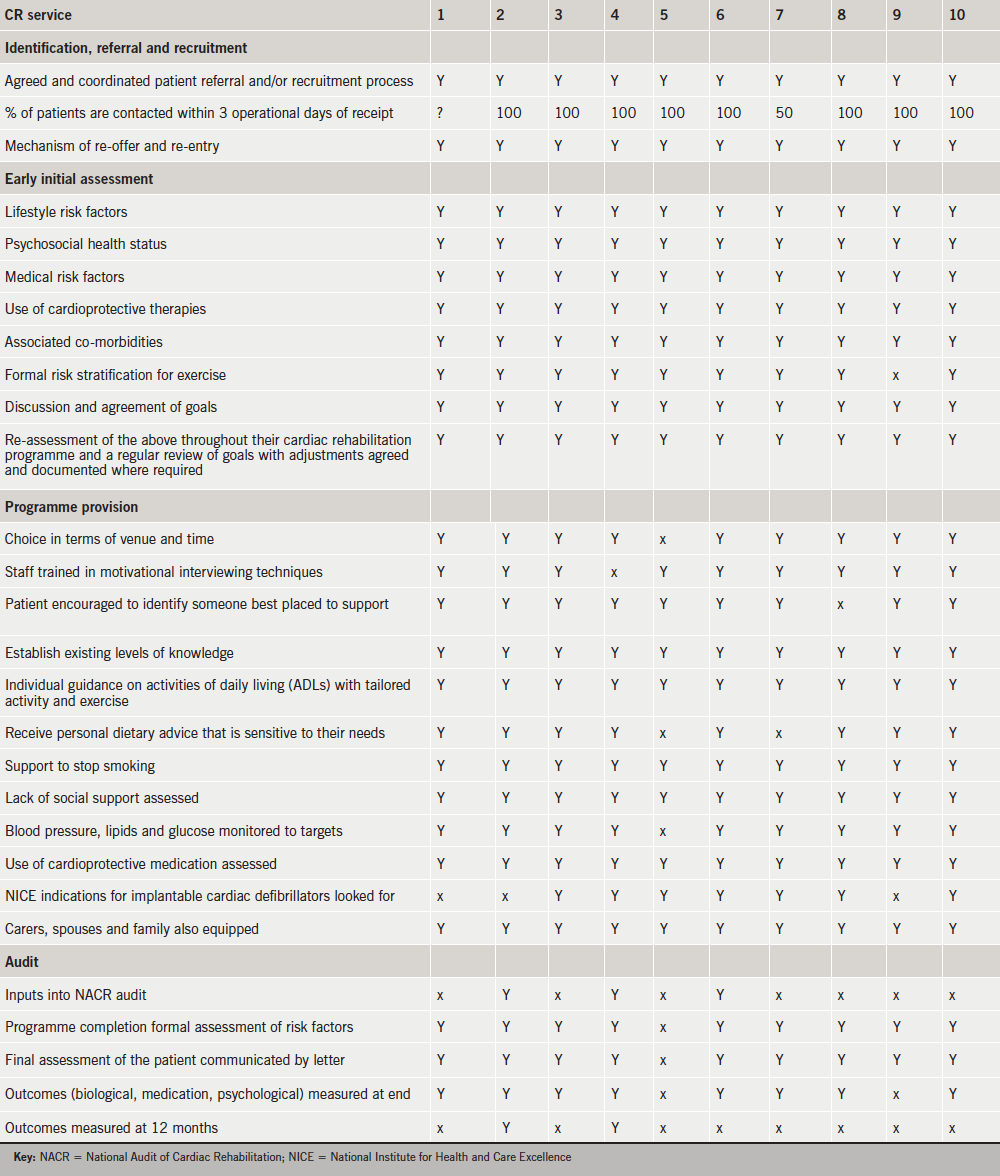
Table 2 shows the results of the main body of the audit.
There was a region-wide excellence in the identification and referral process, with very quick initial contact of patients as emphasised strongly in BACPR guidance. The audit did not assess which types of patient group were eligible as that was specific to the centre (for example tertiary centres had more non-ischaemic patients, e.g. valve disease, dilated cardiomyopathy). Only one centre had a cultural issue with a reasonably high proportion of South Asian patients, and the way in which this was dealt with is discussed further below.
Early initial assessment was excellent in all centres, with a thorough initial appraisal evident in all, a prerequisite to a patient-centred approach. BACPR state that “a formal assessment of lifestyle risk factors (smoking, diet and physical activity), psychosocial health status, medical risk factors (blood pressure, lipids and glucose) and use of cardioprotective therapies” is needed, and all centres follow these guidelines. All services set goals, and most did risk stratification.
Programme provision was very good – the region’s CR programmes demonstrated a great deal of flexibility in their services (e.g. in terms of times and venues of CR programmes), as well as the broad-based approach recommended in CR, with lots involving family/carers. Audit was patchier, with only a minority of centres contributing to the national audit – feedback was that this was mostly down to an issue of time and lack of administrative skills, most CR services felt they were not resourced for this, but more for programme delivery.
Overall, all 10 CR services were compliant with the vast majority of basic standards set by BACPR. In particular, all 10 services were able to demonstrate that they were delivering the seven core components of cardiac rehabilitation, though more work was needed to ensure all were able to fully deliver the final component, audit and evaluation.
Table 2. Main results of audit
The Anglia CR network local strengths
Exercise specialist
One hospital had a highly individualised approach, particularly in activity. It chooses to employ an exercise specialist, rather than a physiotherapist, to focus, it argues, on health, not illness. The exercise prescription is novel within the Anglia region, and tailored to each patient.
Low impact class
Another service offered a low-impact class that extends out to those patients who would not normally have come to traditional exercise classes – this broadens the inclusion criteria when resources are limited towards providing a more generic service to the cardiac population.
Psychological rehabilitation
Another two services reminded all those involved in CR that broad outcome data can only say so much. One highlighted the case of a 70-year-old man who, after his heart attack, suffered so emotionally that he purchased a sofa bed and commode as he felt unable to climb stairs, and he was even unwilling to lift his head from the pillow. He would not even attend for the coronary angiogram. With much CR effort and education, GP review, help from a local hospice and careful liaison with his consultant cardiologist with regards to timing and logistics of his angiogram, he made it through the angiogram and at six-month follow-up was found to be doing very well and walking for half a mile with only slight breathlessness, as well as being free from anginal symptoms. On a 12-month audit sheet of ‘hard’ data, this would reveal little of the extensive multi-disciplinary work that was undertaken by the CR team and others to fully rehabilitate this patient after his heart attack, a time-consuming but ultimately highly rewarding care process. One CR service uniquely provides a cognitive behavioural therapy (CBT) service. Overall, however, the lack of formal psychological service support was highlighted.
Social inequality
One service was relatively unique in the area having a high ethnic (South Asian) population, a population that is known to have a higher burden of cardiac disease but often less access to cardiac services.5 However, this CR service maintained a very high proportionate uptake among ethnic groups (e.g. by using specially trained healthcare professionals of South Asian background) and, thus, was able to avoid potential local health inequalities in using specialist services to ensure equitable uptake of CR.
Phase 4 classes
Another service presented their follow-on exercise class after the CR programme with the local council. It was initially funded from the Academic Health Science Network which piloted a Phase 4/follow-on class for patients. Funding was then continued from the council for this follow-on class, which had been oversubscribed from the start.
Education exhibition
One service has been running an Education Exhibition since April 2011; they wanted to target a wider group of patients and partners that would not traditionally receive education, i.e. heart failure, patients awaiting intervention (valve surgery, bypass surgery, complex pacing, angina). Every eight weeks they invite patients and partners to attend the event, held in their Hospital Education Centre. British Heart Foundation (BHF) literature and magazines are available for patients to take away near the refreshments. They also have information regarding erectile dysfunction and place some of these in the men’s toilets. They have two projector screens playing educational videos, so patients and partners can sit and watch while drinking coffee, and waiting for the next health professional to become available. Health professionals that attend are: pharmacist, dietitian, occupational therapist, smoking cessation advisor (level 3) (also targets partners and passive smoking), UPBEAT (patient support group), cardiac rehab nurse specialists/cognitive behavioural therapist and physiotherapist.
Community services
Two community-based CR services exist within Anglia, and allow these patients to access a CR programme nearer to home. Home visiting is also possible, and community venues aid accessibility and increase uptake. These CR services are particularly flexible, even offering evening classes to aid accessibility. Strong links with community cardiac support groups also exist, and they work in partnerships with Phase 4 exercise instructors based in the communities, for instance through the local council.
Menu-based services
One CR service from a tertiary centre offered a menu-based, flexible, inclusive programme. In addition to an in-house programme offering three levels of exercise, there is a home-based programme for those who cannot attend the usual CR programme – these patients get an initial assessment via telephone or email, and then patients are given a diary and DVD, heart rate monitor or pedometer depending on their needs. Weekly telephone calls/emails are planned for the first six weeks, then at nine weeks and a final assessment (can be visit or telephone call) at 12 weeks, with an education topic for each weekly call to cover what would be traditionally done at group education. This home programme enables patients to complete a CR programme if returning to work, have transport issues or simply that they do not wish to exercise as part of a group. It even allows patients to continue on the programme if they live or plan to travel overseas (recent patients on this programme have lived in Spain, Portugal, Hong Kong, Oman and Australia).
Outcome data and future challenges
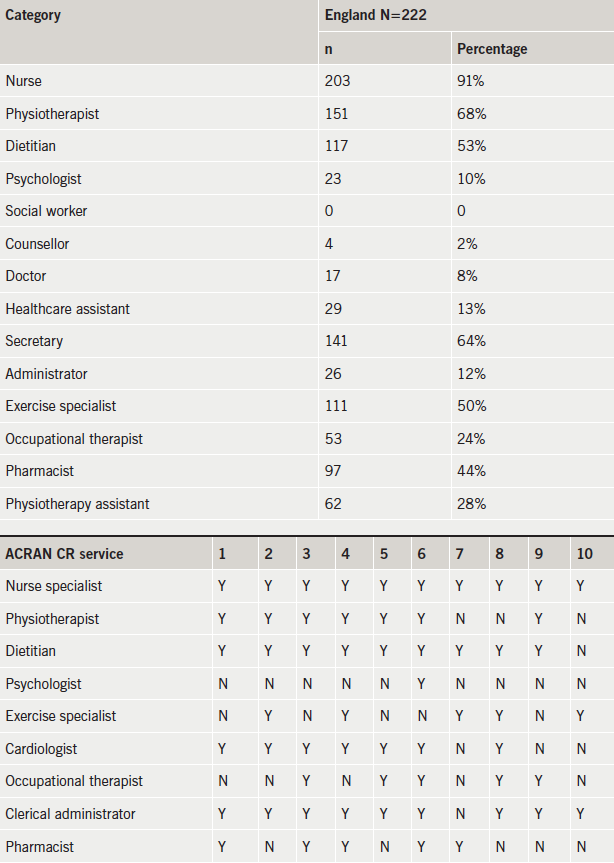
We found that outcomes were collected variably (no standard agreement for instance on best physical activity variable), and ad hoc across the region. Some services collected no outcomes at all. This was mostly down to lack of time and resources (personnel and financial) to collect either local outcomes, let alone input into the national audit. The practitioners fed back that CR services were not set-up to audit themselves, as they focus on delivering the actual care process. We were unable to compare clinical outcomes pre- and post-programmes in a formal and consistent manner, but there was some consistency from locally collected before-and-after data (available on request) that CR across the region improved exercise and anxiety, reduced smoking but had little effect on blood pressure and body mass index. We compared our regional results with the NACR audit and found many similarities, in particular that CR over a 12-week period impacted mostly on physical activity, smoking cessation and, to a degree, psychological health (though the latter depends on baseline levels of anxiety – as illustrated in the individual case examples above, CR can be very effective in very anxious patients) – there was less impact on weight. Our levels of staffing regionally, also looked remarkably similar to national figures (box 2). Using questionnaires and testimonials that local services collected, overall patient satisfaction was very positive overall.
Box 2. Comparison between England staffing and Anglia staffing profiles
Discussion
We have conducted a comprehensive and rigorous audit across the region to establish a baseline position from BACPR standards. We present data that show that all our region’s CR services met the vast majority of the exacting standards in the BACPR standards publication. By conducting this survey in the way we have (driven by a consultant cardiologist who is not directly involved in CR delivery), we have stood back from our services. The rebooting of our network into an Alliance has led to us working more collaboratively than ever before, and in the process of this audit (one that took one year to plan and do), we have succeeded in terms of cross-pollination of knowledge. We used the same care process benchmarking tool (BACPR) across the network to ensure consistency of approach across all services and this helps to standardise services across the patch – what we lacked were consistent outcome measures. By presenting these data at an open-invite East of England Clinical Network organised meeting, we consulted with and incorporated views from all key stakeholders – the day’s attendees included consultant cardiologists, cardiac service managers, commissioners, clinical leads from neighbouring regions, senior academics (a professor of nursing and a professor of public health), and patient representatives. We aspire to include commissioners further in plans for future service redesign.
Strengths and weaknesses
We accept this is a self-completed audit by the CR practitioners themselves. The audit questionnaire was broad and pragmatic, given the time constraints of the practitioners, and the variation of services across the region. It sought mostly to demonstrate, to any interested outside observers or internal commissioners, the degree to which local services conformed to broad standards as taken from BACPR. The other key issue was to highlight gaps, and it did highlight areas of deficiency, which though few, had a degree of consistency across the region (e.g. in lack of certain types of healthcare professional, lack of audit). We acknowledge that this was not a clinical trial seeking to counter-balance recent research suggesting CR is not effective, and for that, we would look to future large, multi-centre CR randomised trials that examined outcomes in standard CR against another care pathway following myocardial infarction.
Conclusion
We show here that CR services within the Anglia region of the East of England are fit-for-purpose and we present local areas of excellence for wider learning for others; we also highlight local areas of need and gaps in CR that we will cross-pollinate to improve all CR services in East Anglia. Whether or not the current format of CR is valid remains up for debate, and research is needed into whether a more flexible and tailored approach6 is of greater benefit to this population. CR is likely to continue to get more referrals as survival improves quicker than incidence falls. The indications for CR will further broaden (e.g. into angina, heart failure, post-surgical) and there remain a lot of patients that do not attend, often the ones who really need CR.7 EUROASPIRE (European Action on Secondary and Primary Prevention through Intervention to Reduce Events) shows secondary prevention behaviour change outcomes remain very poor8 and, thus, given all this, CR remains the vital other ‘bookend’ to coronary care, a continuous pathway of care for a condition, which usually starts with the patient with chest pain calling for an ambulance.
Acknowledgement
The ACRAN team would like to thank Delyth Williams (Quality Improvement Lead, Strategic Clinical Networks – Cardiovascular, NHS England, East Anglia Area Team) for providing the infrastructure and support to be able to present our audit idea and subsequent results to all interested parties in the region. Without her, this work would not have been given the platform it ultimately was.
Conflict of interest
None declared.
Key messages
British Association of Cardiovascular Prevention and Rehabilitation (BACPR) espouses seven core standards for cardiac rehabilitation (CR)
In this audit, all 10 CR services in Anglia were compliant with the vast majority of basic standards set by BACPR
The audit highlighted gaps in multi-disciplinary staff (psychologists, occupational therapists and pharmacists) and audit
Local strengths were highlighted that will encourage future cross-pollination across the network
CR across the region improves exercise tolerance, reduces anxiety and reduces smoking, but had little effect on blood pressure and body mass index, comparable to the national audit
2. Heran BS, Chen JMH, Ebrahim S et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2011;(7):CD001800-CD. http://dx.doi.org/10.1002/14651858.cd001800.pub2
3. West RR, Jones DA, Henderson AH. Rehabilitation after myocardial infarction trial (RAMIT): multi-centre randomised controlled trial of comprehensive cardiac rehabilitation in patients following acute myocardial infarction. Heart 2012;98:637–44. http://dx.doi.org/10.1136/heartjnl-2011-300302
5. Zaman MJ, Philipson P, Chen R et al. South Asians and coronary disease: is there discordance between effects on incidence and prognosis? Heart 2013;99:729–36. http://dx.doi.org/10.1136/heartjnl-2012-302925
6. Redfern J, Maiorana A, Neubeck L, Clark AM, Briffa T. Achieving coordinated secondary prevention of coronary heart disease for all in need (SPAN). Int J Cardiol 2011;146:1–3. http://dx.doi.org/10.1016/j.ijcard.2010.08.046
8. Kotseva K, Wood D, De Backer G et al. EUROASPIRE III. Management of cardiovascular risk factors in asymptomatic high-risk patients in general practice: cross-sectional survey in 12 European countries. Eur J Cardiovasc Prev Rehabil 2010;17:530–40. http://dx.doi.org/10.1097/HJR.0b013e3283383f30
Sponsorship Statement: Actelion have funded the production of this article but have had no input into content.
First published online 27 October 2015
Pulmonary hypertension moves into new era
The launch of new pulmonary hypertension (PH) guidelines was covered in several sessions at the recent European Society of Cardiology (ESC) Congress, held recently in London.
Life-expectancy is now approaching 90 years, and it won’t stop there. Healthy life-expectancy is also extending, so that the average 60 year old can expect a further 11 years of healthy life. Currently, 35% of the UK population is over 50 years, and growing – and on the whole they are healthier, more skilled, better educated and more dynamic than ever before.
Dr Jonathan Collie (Co-Founder, The Age of No Retirement)
The fact that people are living healthier for longer is good news, right? Well, you’d think it would be. But, the concept of retirement has not evolved to match the needs and demands of the modern retiree. And, more importantly, pension values in real terms are a small fraction of what they once were. More and more of us are still working at an age when previous generations were out to grass and on the golf course.
When retirement was invented, people didn’t survive much beyond retirement age, so it was understandable that most wanted to spend what little healthy time they had left on leisure activities and relaxing. This was the old-style or cliff-edge retirement in the purest definition of the term – an abrupt cessation of all work-related activities and the commencement of family, hobby and leisure activities.
The term ‘retirement’ doesn’t really fit in a modern society, largely because most early ‘retirees’ continue to work in some form or another. They may not continue to work full-time, nine-to-five, but flexible, occasional, part-time work, even if only for a few hours a week, is still work. And volunteering, caring and grandchild-minding is also work, even if it is unpaid.
Economic pressures have meant that the Government cannot afford to pay (even lower) pensions until much later – the state pension age has been shifted to 68 years, with further legislation put in place to move this even further to 70 or beyond – so more and more people will find it necessary to work or start new businesses well into their 60s, and probably into their 70s too.
To facilitate the trend in working longer, the Government published a ‘Fuller Working Lives’ policy document in 2014 to champion the skills and experience of an older workforce. It has also commissioned a research project called ‘The Mid-Life Career Review’ to provide older workers with counselling and support services to best match their skills with new career opportunities.
With all the aforementioned, one would be forgiven for thinking that older people would be playing a more active and more central role in modern society – in the workplace, in the economy and in the community. And this could very well be the case, but for the dominant ageist stereotypes, misperceptions and attitudes of wider society – perpetuated by the media, advertising and entertainment industries, even employers – that over-50s are past their prime and over the hill.
There is increasing evidence of the drift between the experience, capabilities and productivity of the modern retiree and the misperception of their value by community leaders and employers. This is concerning, particularly in a time of economic growth and rising skills shortages.
A new debate is needed. A new breed of social activism and leadership is needed to champion the value of multi-generational integration. New thinking is required, driven by a creativity and innovation that is unlikely to be found in local government or academic institutions.
The Age of No Retirement
‘The Age of No Retirement’ (TAONR) was established in 2014 in London by myself and Georgina Lee to lead such a movement – a movement for age-positive social change and Britain’s first ever national debate to discover the value in a society in which people are living and working longer.
TAONR uses the principles of collaborative design to bring people and organisations together to rethink and rework the role of older people in British society – with a hope, optimism and drive rarely seen in the ‘Age’ space.
TAONR is a collaborative movement including employers, policy makers, innovators, designers, academics and citizens in creating a society without age barriers; where skills, capabilities, knowledge and wisdom are valued whatever your age – young or old.
Since October last year, more than 800 people from 300 organisations (including Barclays, Aviva, GSK, BT, Google, Microsoft, Capita, Government, public sector and third sector organisations) have been brought together to identify some of the main challenges of an ageing society – and work together to solve them.
Through a series of live debates in London and Manchester, TAONR has identified six themes that need to be addressed as a matter of priority:
Intergenerational integration – it’s not us and them. We’re in this together.
Adopting the principles of creative design to drive positive change.
Create a new plain language for ageing, and avoid euphemistic deflections.
Changing the narrative of ageing, and capturing and telling real stories of real people.
Taking a whole-life approach (0–100 years), and not viewing life as a series of disconnected life stages.
Rethink work and employability, and the productivity of the modern retiree – and obliterate the myth of the tech-illiterate, crumbly-health, outdated-skills stereotype.
But TAONR is not just coming up with new ideas – it is far from being yet another talk-shop. Through the creation of 24 co-design labs, each with 15 participants from across the societal spectrum and facilitated by a designer, TAONR has created 22 prototypes for age-positive action. Each prototype is a radical new idea that can be easily (and cheaply) implemented in a local community, and has the promise of significant social and economic impact.
And the impact is not limited to societal (re)design and economic productivity. The implications of a more integrated multi-generational society for the health of the nation are significant too. A more engaged citizenry drives greater social contact between neighbours; which drives more social activity; which drives richer more dynamic social networks – which leads to more informal community-based caring; less social isolation; and ultimately to better mental and physical health.
Together, the 22 prototypes represent the most powerful recipe for age-positive social action that the UK has seen for a long time, if ever. TAONR is now in the process of building local collaborative delivery teams to bring these prototypes to life. TAONR network will then help to amplify and share the inspiring stories that will emerge through this learn-by-doing approach.
Contemporary guidelines have lowered the threshold for statin use in primary prevention (7.5% risk of a cardiovascular event over 10 years in the USA,1 10% risk according to National Institute for Health and Care Excellence [NICE] guidelines in the UK).2 Applying these thresholds, the majority of men over 50 years and more than half of women over 60 years will qualify for statin use. Countering the more widespread uptake of statin use in primary prevention advocated by these guidelines are claims, popularised by the lay press and uncritically published in some medical journals,3,4 that statin use is accompanied by an unacceptable incidence of side effects that adversely compromise lifestyle and which challenge whether the small absolute benefits in some lower risk groups are worth the intolerance of the statin.
High-risk atherosclerotic cardiovascular disease (ASCVD), including recent history of acute coronary syndrome, cerebrovascular atherosclerotic disease, peripheral arterial disease, and coronary artery disease with diabetes mellitus, requires lipid-level monitoring and treatment. Data for patients with high-risk ASCVD from 2008–2011 were obtained from the UK Clinical Practice Research Datalink. Across two years of follow-up, analyses examined lipid-altering drug use, statin adherence (medication possession ratio [MPR]), and persistence (continuous time on drug). Initial statin dose, upward dose titration, and use of high-intensity statins were also studied. Lipid levels were examined overall and by statin use. A total of 131,603 high-risk ASCVD patients were included. Within six months of diagnosis, 63.1% of patients received a statin prescription. Patients typically remained on the initial statin (MPR ≥80% for 71.3% of patients at two years) and dose; 16.4% of patients used high-intensity statins. During the first year of follow-up, 69.3% of patients were either at the low-density lipoprotein cholesterol goal of <2.5 mmol/L or using a high-intensity statin. Considerable room for improvement remains with respect to optimal management of patients with ASCVD.
Introduction
Atherosclerotic cardiovascular disease (ASCVD), including peripheral arterial disease (PAD), coronary artery disease (CAD), acute coronary syndrome (ACS), and cerebrovascular disease (CeVAD), together account for approximately half of the morbidity and mortality in the adult population of Europe aged 50 years and older.1,2 The 2012 Coronary Heart Disease Statistics from the British Heart Foundation reported nearly 180,000 deaths in the UK from cardiovascular disease (CVD), 292 million prescriptions for CVD treatments, and over 87,000 percutaneous coronary interventions (PCIs) during a one-year span.3 In addition, diabetes mellitus (DM) has a prevalence of over 5% in the UK. Studies have found that roughly 27% to 58% of CAD patients also have DM, which is an independent risk factor for poor CVD outcomes.3-11
Recommendations on the secondary prevention of CVD for patients with ASCVD have been published in guidelines from the National Institute for Health and Care Excellence (NICE).12,13 Statin therapy is recommended for adults with clinical evidence of CVD. The 2008 NICE guidelines suggested starting with simvastatin 40 mg for secondary prevention of cardiovascular events other than ACS and with a higher-intensity statin following ACS, increasing the dose to 80 mg simvastatin or a drug of similar efficacy and cost if lipid levels showed insufficient response.12 The 2014 guidelines, however, recommend atorvastatin 80 mg (or maximum tolerated dose) in place of simvastatin 40 mg for secondary prevention.13
The European Society of Cardiology (ESC) guidelines provide target low-density lipoprotein cholesterol (LDL-C) levels of <1.8 mmol/L for patients at very high risk of CVD (including post-ACS patients), and <2.5 mmol/L for patients at slightly lower but still high risk of cardiovascular events, including other ASCVD patients.14
The present study was designed to produce real-world, population-based evidence from the UK on the treatment patterns and lipid levels of a group of high-risk ASCVD patients, including patients with a recent history of ACS within the past year (hACS), CeVAD, PAD, and diabetes with confirmed CAD (DM/CAD), who are at elevated risk of having another cardiovascular event. For brevity, we, heretofore, use the simpler abbreviation of ASCVD to refer specifically to the high-risk ASCVD population of interest.
Methods
Data source
Data were obtained from the Clinical Practice Research Datalink (CPRD), a large database containing anonymised medical information on approximately 8% of the UK population from 630 general practices. At the time of this study, there were 11 million patients in the data repository, with 5.2 million current, active registrants and approximately 67 million patient-years of data. Information in the database includes diagnoses, procedures, referrals, lab tests with results, prescriptions, and demographics. The general practitioner (GP) data were linked to data from the Hospital Episode Statistics (HES) database, which was used to identify hospitalisation events in England, and to the Office for National Statistics mortality data.
Patient selection
Data were extracted for ASCVD patients (≥18 years of age) with a qualifying diagnosis from 1 April 2008 to 31 March 2011 (identification window), with a minimum of 12 months of continuous enrolment prior to a qualifying diagnosis in either CPRD or HES. ASCVD was defined as having a diagnosis of at least one of the following:
hACS: ≥30 days through 365 days after discharge for ACS based on an ACS diagnosis in the HES data
CeVAD: record in the GP or HES data indicating any CeVAD with or without ischaemic stroke
PAD: GP or HES diagnosis, or an appropriate drug for treatment of PAD
DM/CAD: GP or HES diagnosis of CAD recorded on or after the earliest date of diabetes, where diabetes was defined as having either a diagnosis of diabetes (either type 1 or type 2) or prescribed treatment for diabetes.
The index date was defined as the earliest diagnosis date of any of the above diseases within the identification window. Four patient groups were defined: hACS, CeVAD, PAD, and DM/CAD, according to the diagnosis that occurred on the index date.
Baseline characteristics
Patient characteristics included age, gender, body mass index (BMI), and smoking status. Baseline procedures for PCI and coronary artery bypass graft (CABG) were assessed from the 12 months prior to the index date. Comorbidities were coded using all available data from prior to the index date, as chronic conditions may not be re-recorded following initial diagnosis; these included diabetes, hypertension, hypercholesterolaemia, chronic obstructive pulmonary disease, renal impairment, hepatic impairment, congestive heart failure, metabolic syndrome, myopathy, atrial fibrillation, and the Charlson comorbidity index.15 Medication use assessed during the 12-month baseline included antiplatelets, anticoagulants, non-steroidal anti-inflammatory drugs, antidiabetic drugs, cardiovascular agents, and lipid-altering drugs.
Outcome variables
Use of lipid-lowering agents was noted in six-month blocks for the first two years of follow-up for each patient. The drugs examined included statins, ezetimibe, niacin, and fibrates, both alone and in combinations of a statin with another lipid-lowering drug. Combinations of other lipid-lowering agents with a statin required use of each of these at any time during the interval, not necessarily overlapping prescriptions.
For all patients treated with statins during the follow-up period, adherence, persistence, and dosing of the first statin received on or after the index date was tracked. The purpose of this analysis was to examine the use of statins beginning at the earliest date of qualification for the cohort; thus, patients were not required to be new users of a statin. Prevalent statin users were included, but their treatment patterns were assessed from only the index date forward. Patients prescribed more than one statin on the same day were excluded from these analyses.
Adherence was estimated with the medication possession ratio (MPR), calculated as the total days’ supply of prescribed medication during a given time period divided by the total number of days in that time period. Patients whose resulting MPR was over 100%, which can occur when a medication is refilled early, had their MPR truncated at 100%. The MPR was calculated for the first six, 12, and 24 months after the index date among patients enrolled for those durations. Persistence was estimated as the time from earliest statin use on or after the index date until the last date of exposure prior to a gap of more than 30 days; up to a 30-day prescription refill gap was considered continuous treatment.
To calculate the average daily dose, patients were required to have at least two prescriptions indicating at least daily use of the index statin. The prescribed doses of the index statin and any instance of high-intensity statin use were noted; atorvastatin 40–80 mg and rosuvastatin 20–40 mg were classified as high intensity, based on the high-intensity statin definition in the 2013 American College of Cardiology/American Heart Association guideline,16 which was the most recent guideline available at the time of the analysis. Upward dose titration was defined as any increase in dose over the initially prescribed dose.
Lipid levels were examined from the first and second years of follow-up separately and the first two years combined. The most favourable level (i.e. the lowest level, except for high-density lipoprotein cholesterol [HDL-C], where the highest level was most favourable) found during each interval for each patient was used. In addition to the numeric levels of each of these lab tests, levels were also categorised as follows:
1. Total cholesterol
Ideal for CVD patients (<4.0 mmol/L or <155 mg/dL)3,14
Recommended for CVD patients (4.0 to <4.5 mmol/L or 155–174 mg/dL)14
Normal for patients without CVD but above recommended levels for CVD patients (4.5 to <5.0 mmol/L or 174–193 mg/dL)14
Elevated (≥5 mmol/L or ≥193 mg/dL)14
Unknown
2. LDL-C
Recommended for non-ST-elevation myocardial infarction/unstable angina patients, ideal for PAD (<1.8 mmol/Lor 70 mg/dL) 14
Recommended for other high-risk CVD patients (ST-elevation myocardial infarction [STEMI] patients with high risk) (1.8 to <2.0 mmol/L or 70–77 mg/dL)14
Recommended for other CVD patients (STEMI) (2.0 to <2.5 mmol/L or>77–97 mg/dL)14
Normal for patients without CVD but above recommended level for ASCVD (2.5–3.3 mmol/L or >97–128 mg/dL)17
Slightly elevated (>3.3–4.1 mmol/L or >128–159 mg/dL)17
High risk for men and women (<1.0 mmol/L or 39 mg/dL)14
High risk for women (1.0–1.2 mmol/L or 39–46 mg/dL)14
Recommended (>1.2 mmol/L or >46 mg/dL)
Unknown
4. Triglycerides
Recommended (<1.7 mmol/L or <151 mg/dL)14
Moderately high (1.7 to <10 mmol/L or 151 to <886 mg/dL)18
Very high (10–20 mmol/L or 886–1,771 mg/dL)18
Extremely high (>20 mmol/L or 1,771 mg/dL)18
Unknown.
Statistical analysis
Persistence with the index statin was examined using the Kaplan-Meier median time to discontinuation; adherence was summarised as with the distribution of MPR values. Frequencies of initial dose were computed among patients with at least six months of follow-up, and of upward titration and prescription of high-intensity dose among patients followed for two years. Categories of lipid levels were examined among patients with known values, both overall and separately by statin use, high-intensity, non-high-intensity, and non-use. Analyses were descriptive only; no statistical comparisons were performed.
Results
Baseline characteristics
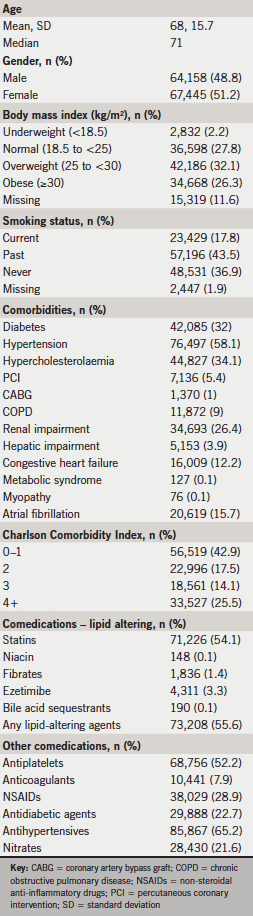
In total, 131,603 ASCVD patients met the inclusion criteria, including 16,629 patients with hACS, 34,044 with CeVAD, 54,492 with PAD, and 26,438 with DM/CAD. Median age was 71 years, and 48.8% of patients were male (table 1). Over half (58.4%) of the ASCVD cohort was overweight or obese, with 27.8% having normal BMI. Current smoking was reported for 17.8% of the cohort. Frequent comorbidities included hypertension (58.1%), hypercholesterolaemia (34.1%), diabetes (32.0%), and renal impairment (26.4%). Charlson Comorbidity Index scores were low (0–1) for 42.9% of the cohort, although about a quarter of patients (25.5%) had scores of 4 or higher. Antiplatelets were used by 52.2% of patients, and lipid-altering drugs, primarily statins, were used during baseline by 55.6% of patients.
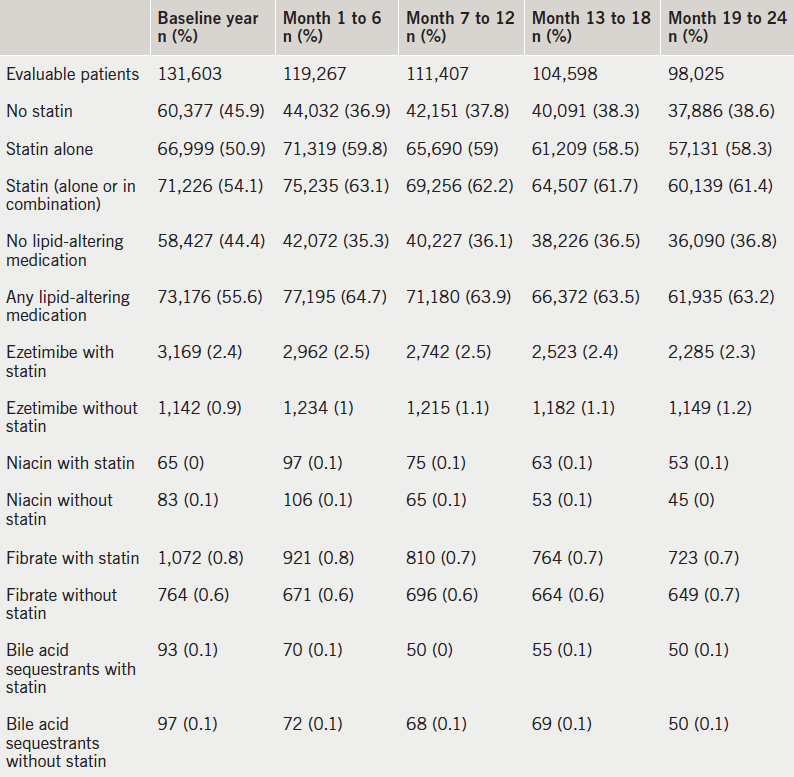
Treatment patterns
During each six-month follow-up window, 63–65% of ASCVD patients were on any lipid-lowering medication, typically statin monotherapy (table 2). Ezetimibe was the most commonly used lipid-lowering drug other than a statin, but was used by <4% of patients.
Table 2. Use of lipid-lowering medications among ASCVD patients
Simvastatin was by far the most commonly used statin (69.6%, n=44,227), followed by atorvastatin (23.3%, n=14,831) (table 3). Simvastatin was most often initiated at 40 mg per day (48.5% out of 63,549 eligible statin users); only 1,066 patients (1.7%) received the maximum allowable dose of 80 mg simvastatin. Atorvastatin 20 mg was prescribed to 5.3% of all patients; 8.2% received the 40 mg dose, and 5.4% the 80 mg dose, both of which were considered high-intensity levels. Across all prescriptions of the index statin across two years, atorvastatin was prescribed at high dose (40–80 mg) to 15.2% of all statin users, with rosuvastatin 20–40 mg prescribed to 1.2%. Overall, high-intensity statins (defined as atorvastatin 40–80 mg or rosuvastatin 20–40 mg) were prescribed to 16.4% of all statin users. Upward dose titrations were seen in 8.9% of patients overall, with little variation among drugs.
Table 3. Initial daily dose of statins, upward dose titration, and high-intensity statin use among statin users with ASCVD
Most patients (71.0%) remained on the index statin continuously (with no more than a 30-day gap) for the first six months of follow-up, leading to a Kaplan-Meier median days on treatment of the full time window (six months; table 4). High adherence, defined as an MPR ≥80%, was observed in 76.9% of patients at six months. Extending the time window to 12 months had little impact on the patterns of results. With a two-year time window, a Kaplan-Meier median time to discontinuation of the index statin was finally found, at 523 days. The percentage of patients with MPR ≥80% dropped only slightly from the six-month results, to 71.3%.
Table 4. Persistence and adherence of the index statin among ASCVD patients
Lipid levels
Across the first two years combined, 80.2% of patients had total cholesterol levels recorded. Ideal levels (<4.0 mmol/L) were achieved by 48.2% of patients with known values, with another 18.9% at recommended levels (4.0 to <4.5 mmol/L) (table 5). Overall, 32.9% of patients with known lipid values had not achieved the recommended total cholesterol goal.
Table 5. Lipid levels during two years of follow-up among ASCVD patients
LDL-C levels were available for 58.7% of patients, of whom 68.5% had LDL-C within recommended levels for general CVD patients (LDL-C <2.5 mmol/L) over the two-year period, and 34.6% had the stricter recommended goal of LDL-C <1.8 mmol/L (table 5). HDL-C was available for 71.2% of patients; 61.1% were within the recommended range of >1.2 mmol/L. Triglyceride levels were available for 64.6% of patients, with 74.3% having results within the recommended range (<1.7 mmol/L).
The ideal level of total cholesterol (<4.0 mmol/L) in the first year was found in 54.4% of patients on high-intensity statins, 50.4% on non-high-intensity statins, and 11.9% among statin non-users (table 6). The lowest category of LDL-C levels (<1.8 mmol/L) was seen in 41.3%, 35.5% and 5.3% of patients in the high-intensity, non-high-intensity and non-use statin groups in the first year, respectively. Differences in distribution of HDL-C and triglyceride levels across the three statin use groups were smaller than those of total cholesterol and LDL-C levels. Similar patterns were seen in the second year of follow-up.
During the first year of follow-up, 69.3% of patients (table 6) were either at the LDL-C goal of <2.5 mmol/L or using a high-intensity statin; the proportion was similar during the second year of follow-up (68.7%). Using the stricter recommended LDL-C level of <1.8 mmol/L, 40.2% of patients were either at the goal or were using a high-intensity statin (39.9% during the second year).
Discussion
In this large cohort of ASCVD patients from the UK, the majority of patients received statin treatment. Simvastatin was the most frequently prescribed statin and was generally used at the standard dose of 40 mg; when more intensive statin therapy was needed, it appears likely that patients were instead prescribed atorvastatin at high doses. Use of high-dose atorvastatin is consistent with the 2014 NICE guidelines,13 although the NICE guidelines in effect during the study period recommended either increasing the dose of simvastatin to 80 mg or changing to a higher-intensity statin.12 Use of simvastatin 80 mg may have already declined during the study period due to concerns regarding safety, especially myopathy and rhabdomyolysis.19 Overall, 16.4% of patients were prescribed high-intensity statins during two years of follow-up, and dose increases were seldom seen.
Table 6. Lipid levels by statin use during two years of follow-up among ASCVD patients
Patients usually remained on the same statin that was prescribed first on or after their date of diagnosis with the ASCVD condition. Adherence appeared excellent in these cohorts, with more than 70% of patients having an MPR of 80% or higher across two years of follow-up. Persistence with statins was also high, at a median of 523 days. An earlier study of statin treatment patterns in ACS patients using the same data source reported that 43% of patients remained on statin treatment at four-year follow-up.20 The current study found 44.7% persistence among ACS patients at two years, although the allowable gap duration in this study was only 30 days, compared to 145 days in the previous study.
Lipid levels, especially LDL-C, either were not consistently measured annually or were measured but not entered into the database. During the first year of follow-up, 69.3% of patients were either at the LDL-C goal of <2.5 mmol/L or using a high-intensity statin, while 40.2% of patients were either at the LDL-C goal of <1.8 mmol/L or using a high-intensity statin. These percentages remained stable across the second year, at 68.7% and 39.9%, respectively. Therefore, for over 30% of ASCVD patients, treatment of lipid level elevations is not meeting any guideline recommendations, placing patients at greater risk of suffering further cardiovascular events.
Data in the CPRD should be complete with respect to events in the GP’s clinic, but data on hospitalisations and specialist visits may be missing or incomplete. The HES data contain hospitalisation data only for England. Thus, the hACS patients, identified only through the HES data, represent patients from England only, in contrast with the other patient groups. Drug use is recorded at the prescription level; patients may not have filled the prescriptions and taken the drug as prescribed, and dose titrations may be incompletely recorded. Measures such as lipid levels and BMI were available only when these measurements were taken and entered into the database.
The study cohort included a combination of patients experiencing either their first or recurrent ASCVD events. Treatment patterns and lipid levels may differ following a recurrent event compared with a first event. In addition, the inclusion of prevalent users of statins in the adherence and persistence analyses may have biased results relative to use of a pure inception cohort; prevalent users were included to provide a more complete view of the treatment patterns following an ASCVD diagnosis.
Despite these limitations, the study has many important strengths. This study is the first, to our knowledge, to examine the treatment patterns and lipid levels in a broad cohort of ASCVD patients in the UK. The source population for the cohort is large and generally highly representative of the UK population. Each of the disease groups contained tens of thousands of patients, and data for these patients included relevant lab values, prescription drug information, comorbidities, and linked hospital and mortality data.
In conclusion, the present study found that statin use is highly prevalent among ASCVD patients in the UK. Adherence and persistence with statins appear excellent, based on the prescription data available in the database, yet optimal lipid levels were not consistently achieved. Greater use of high-intensity statin treatment may be needed in this high-risk population to reduce the risk of further CVD events.
Funding
This study and resultant manuscript were funded by Eli Lilly and Company, Indianapolis, IN, USA.
Conflict of interest
Antje Tockhorn, Yajun Zhu, and Zhenxiang Zhao are employees and shareholders of Eli Lilly and Company, Indianapolis, IN, USA. Beth Nordstrom and Robert Donaldson are current employees of Evidera, which provides consulting and other research services to pharmaceutical, device, government, and non-government organisations. William Engelman and Jenna Collins were Evidera employees who participated in research for this study. In their salaried positions, they work with a variety of companies and organisations and are precluded from receiving payment or honoraria directly from these organisations for services rendered. Evidera received funding from Eli Lilly and Company for their work on this project.
Key messages
In a large cohort of UK patients with high-risk atherosclerotic cardiovascular disease (ASCVD), 63% received statin therapy within six months of diagnosis
Dose titration of statins or switching among different statins were seldom seen, with 71% of patients having at least 80% statin adherence across two years
More than 30% of patients had lipid levels above the recommended level and were not taking high-intensity statins
Considerable room for improvement remains with respect to optimal management of patients with high-risk ASCVD
References
1. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study. Lancet 1997;349:1498–504. http://dx.doi.org/10.1016/S0140-6736(96)07492-2
3. British Heart Foundation, Townsend N, Wickramasinghe K et al. Coronary heart disease statistics, 2012 edition. London: British Heart Foundation, December 2012. Available from: https://www.bhf.org.uk/publications/view-publication.aspx?ps=1002097 (accessed 21 February 2014).
4. Krempf M, Parhofer KG, Steg PG et al. Cardiovascular event rates in diabetic and nondiabetic individuals with and without established atherothrombosis (from the REduction of Atherothrombosis for Continued Health [REACH] Registry). Am J Cardiol 2010;105:667–71. http://dx.doi.org/10.1016/j.amjcard.2009.10.048
6. Odden MC, Coxson PG, Moran A et al. The impact of the aging population on coronary heart disease in the United States. Am J Med 2011;124:827–33.e5. http://dx.doi.org/10.1016/j.amjmed.2011.04.010
7. Mahoney EM, Wang K, Cohen DJ et al. One-year costs in patients with a history of or at risk for atherothrombosis in the United States. Circ Cardiovasc Qual Outcomes 2008;1:38–45. http://dx.doi.org/10.1161/CIRCOUTCOMES.108.775247
8. Mahoney EM, Wang K, Keo HH et al. Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States. Circ Cardiovasc Qual Outcomes 2010;3:642–51. http://dx.doi.org/10.1161/CIRCOUTCOMES.109.930735
10. Fox CS, Sullivan L, D’Agostino RB Sr, Wilson PW. The significant effect of diabetes duration on coronary heart disease mortality: the Framingham Heart Study. Diabetes Care 2004;27:704–08. http://dx.doi.org/10.2337/diacare.27.3.704
11. Lee PG, Cigolle C, Blaum C. The co-occurrence of chronic diseases and geriatric syndromes: the health and retirement study. J Am Geriatr Soc 2009;57:511–16. http://dx.doi.org/10.1111/j.1532-5415.2008.02150.x
12. National Institute for Health and Care Excellence. NICE clinical guideline 67. Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. London: NICE, May 2008. Available from: http://www.nice.org.uk/nicemedia/pdf/CG067NICEGuideline.pdf (accessed 10 February 2014).
13. National Institute for Health and Care Excellence. NICE clinical guideline 181. Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. London: NICE, July 2014. Available from: http://www.nice.org.uk/guidance/cg181 (accessed 5 August 2014).
14.Perk J, De Backer G, Gohlke H et al. European guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2012;33:1635–701. http://dx.doi.org/10.1093/eurheartj/ehs092
15. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 1992;45:613–19. http://dx.doi.org/10.1016/0895-4356(92)90133-8
16. Stone NJ, Robinson J, Lichtenstein AH et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2889–934. http://dx.doi.org/10.1016/j.jacc.2013.11.002
19. Study of the Effectiveness of Additional Reductions in Cholesterol Homocysteine Collaborative Group, Armitage J, Bowman L, et al. Intensive lowering of LDL cholesterol with 80 mg versus 20 mg simvastatin daily in 12,064 survivors of myocardial infarction: a double-blind randomised trial. Erratum in Lancet 2011;377:126. Lancet 2010;376:1658–69. http://dx.doi.org/10.1016/S0140-6736(10)60310-8
20. Boggon R, Eaton S, Timmis A et al. Current prescribing of statins and persistence to statins following ACS in the UK: a MINAP/GPRD study. Br J Cardiol 2012;19:24. http://dx.doi.org/10.5837/bjc.2012.003
Hull and East Yorkshire Hospitals NHS Trust offers a primary percutaneous coronary intervention (PPCI) service accessed via a coronary care unit (CCU) nurse-based pre-alert system. We reviewed our pre-alert calls for 2013 to determine their appropriateness and assess whether patients were being correctly accepted/declined for PPCI by comparison with final discharge diagnosis.
There were 1,343 calls received, only 52% had chest pain and electrocardiogram (ECG) changes meeting criteria. There were 508 patients with a discharge diagnosis of ST-elevation myocardial infarction (STEMI), 89% of whom were accepted directly.
There were 54 cases with a final diagnosis of STEMI initially declined: 14 in cardiac arrest were directed to the emergency department (ED) as per policy; 18 had documented clinical reasons for declining; seven did not meet the criteria. There were 15 patients (3%) with chest pain and ECG criteria declined without a documented reason; three were subsequently accepted after assessment at their local hospital. Patients >80 years, female and with atypical presentation were more likely to be declined.
Of accepted patients, 132 (23%) had a diagnosis other than STEMI at discharge, 65% with an alternative cardiac diagnosis.
In conclusion, patients are frequently referred who do not meet symptom or ECG criteria. Most STEMI patients are appropriately accepted via our pre-alert pathway. Review of pre-alert services is essential to ensure timely and appropriate PPCI.
Introduction
Primary percutaneous coronary intervention (PPCI) is the preferred management for ST-elevation myocardial infarction (STEMI),1 and guidance committees have universally adopted this strategy as the ‘gold standard’ of care.2-4 National Institute for Health and Care Excellence (NICE) guidelines mandate that PPCI is not only accessible to the entire population of the UK, but also that this is delivered in a timely fashion.4 Therefore, the early identification of appropriate STEMI patients for PPCI is essential, but this can be complicated due to the volume of patients, inadequate training and experience of frontline emergency care staff, and the implications of incorrect diagnoses. Consequently, PPCI centres have introduced local, structured, pre-alert systems to streamline assessment and service provision.
Hull and East Yorkshire (HEY) NHS Trust has provided a 24/7 reperfusion service to a population of 1.2 million since 2009, with the Emergency Department (ED) and PPCI centre on separate sites. The PPCI pathway is accessed by a centralised pre-alert telephone system managed by an experienced coronary care nurse team. The aim of this study was to review the PPCI pre-alert calls and patient discharge diagnoses for the calendar year 2013 to assess the appropriateness of calls and ensure that referrals were being correctly accepted/declined.
Materials and methods
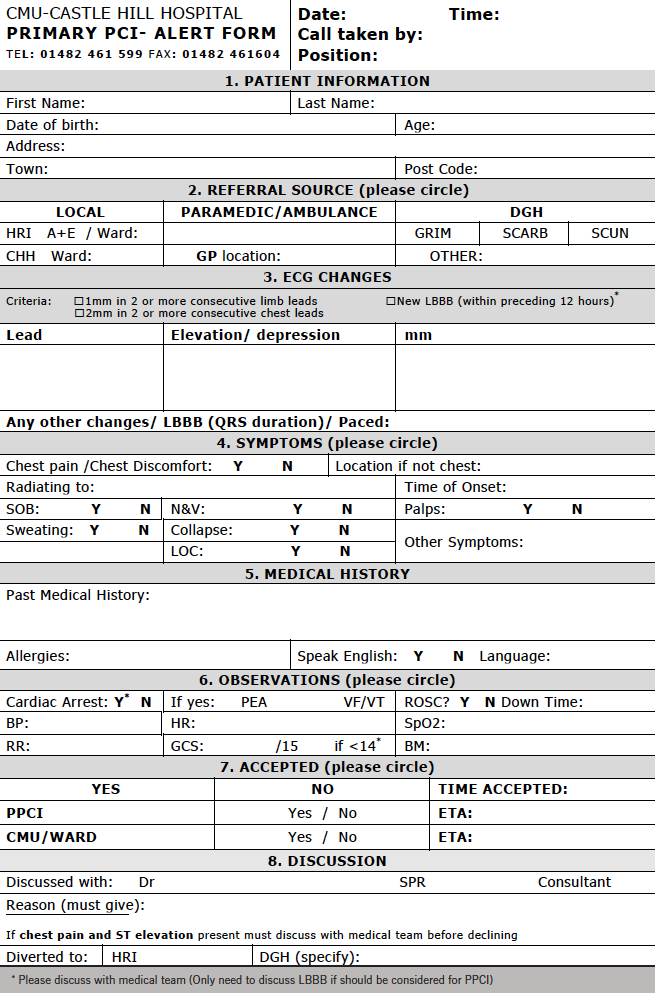
Pre-alert calls are received on a dedicated pre-alert telephone and triaged by senior nursing staff on the coronary care unit (CCU). All calls are documented on a standardised locally agreed proforma, designed to rapidly capture relevant information and facilitate a timely decision based on clinical and electrocardiogram (ECG) criteria. Criteria for referral and acceptance include the presence of symptoms consistent with STEMI within the last 12 hours, combined with ST-elevation (≥1 mm in two or more contiguous limb leads, or ≥2 mm in two or more contiguous precordial leads) or presumed new left bundle branch block (LBBB) on the ECG. ECGs are not routinely transmitted to the triage nurse, and decisions are based on the ECG findings reported by the referring paramedic or clinician. In cases of uncertainty, the triage nurse will discuss the decision with the on-site cardiology registrar or interventional consultant on-call. Cases accepted into the PPCI pathway are brought directly to the cardiac catheterisation laboratory at the PPCI centre.
All pre-alert proformas from 2013 were retrospectively reviewed to determine demographic data, symptoms, ECG findings, and the pre-alert decision. The final diagnosis relating to the episode of care was ascertained from hospital case records at the PPCI centre and surrounding district hospitals. In cases where a discharge diagnosis could not be established, the appropriateness of the triage decision was independently adjudicated by two interventional cardiologists.
Statistical analysis was performed on StatView version 5.0. Continuous variables were expressed as a mean ± standard deviation and categorical variables were documented as numbers (percentages). Categorical variables were compared using the Chi-squared test, with two-sided p values of <0.05 considered to indicate statistical significance.
Results
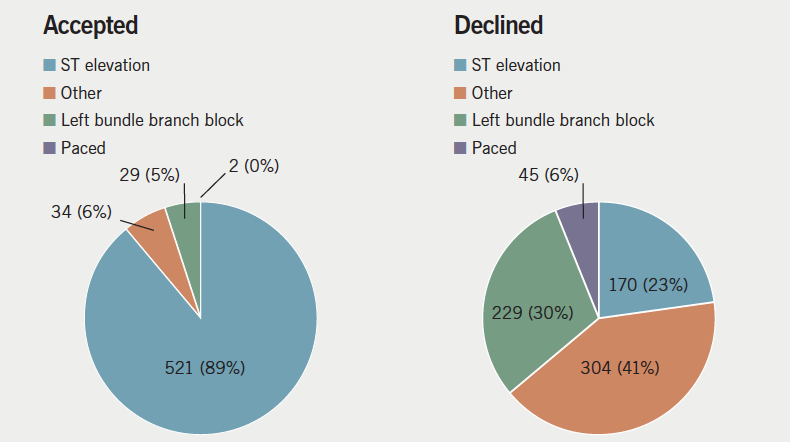
A total of 1,343 pre-alert referrals were made during 2013, of which 586 (44%) were accepted into the PPCI pathway. The mean age of referred patients was 68 ± 15 years and 853 (66%) were male. Most referred patients had chest pain (956, 71%), but only 701 (52%) had both chest pain and satisfied ECG criteria. A substantial proportion of referred patients (137, 10%) had neither chest pain nor satisfied ECG criteria for referral. Regarding those referred, 691 (51%) had ST elevation and 258 (19%) had LBBB. The ECG findings differed significantly between patients that were accepted and declined for PPCI (figure 1).
Figure 1. Interpretation of patients’ electrocardiogram (ECG) by paramedic/referring physician documented on proforma, in those accepted and declined
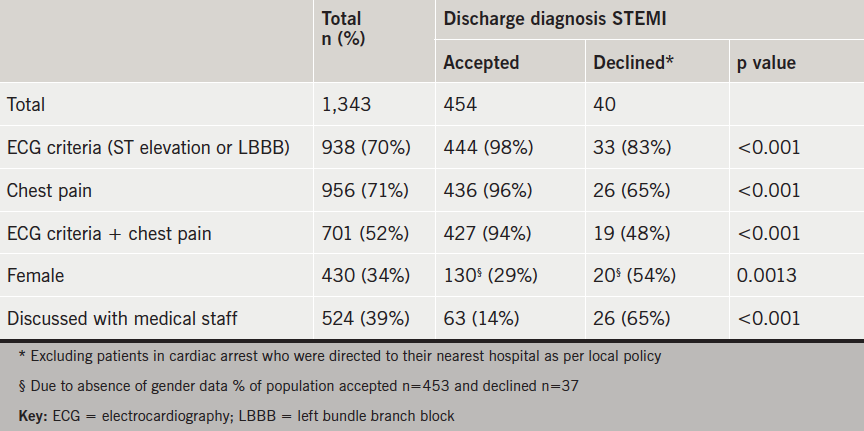
The final discharge diagnosis was STEMI for 508 (38%) patients (table 1). Of these, 454 (89%) were accepted directly from the initial pre-alert referral. There were 54 cases with a final diagnosis of STEMI initially declined: 14 in cardiac arrest were directed to their local emergency department (ED) as per regional policy; seven did not meet criteria for acceptance; 18 had clinical reasons for declining documented on the proforma, such as delayed presentation or significant comorbidities, for example end-stage metastatic disease. Fifteen patients (3% of STEMIs) satisfied clinical and ECG criteria but were declined without a documented explanation on the referral proforma; three of these patients were subsequently accepted following assessment at a local district hospital.
Table 1. Symptoms and electrocardiogram (ECG) characteristics documented on proforma of patients with final diagnosis of ST-elevation myocardial infarction (STEMI)
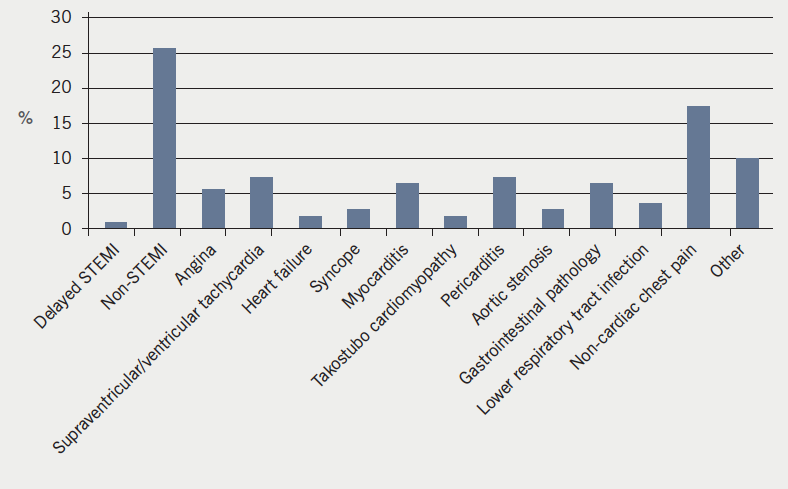
Of patients accepted into the PPCI pathway, 454 (77%) were discharged with a final diagnosis of STEMI, 86 (15%) had an alternative cardiac diagnosis, and 46 (8%) had a non-cardiac diagnosis. The alternative cardiac and non-cardiac diagnoses are shown in figure 2.
Figure 2. Distribution of discharge diagnoses of patients accepted onto primary percutaneous coronary intervention (PPCI) pathway without final diagnosis of STelevation myocardial infarction (STEMI)
Of the 258 pre-alert calls for LBBB, 29 (12%) were accepted into the PPCI pathway. Three referred LBBB patients had a final diagnosis of STEMI, all of whom were accepted. On review of these cases, one was incorrectly labelled LBBB at the time of referral (ECG actually showed anterior ST elevation), and the other two cases underwent PCI to significant coronary stenoses but on retrospective review did not have acute coronary artery occlusion at the time of coronary angiography despite the documented discharge diagnosis of STEMI.
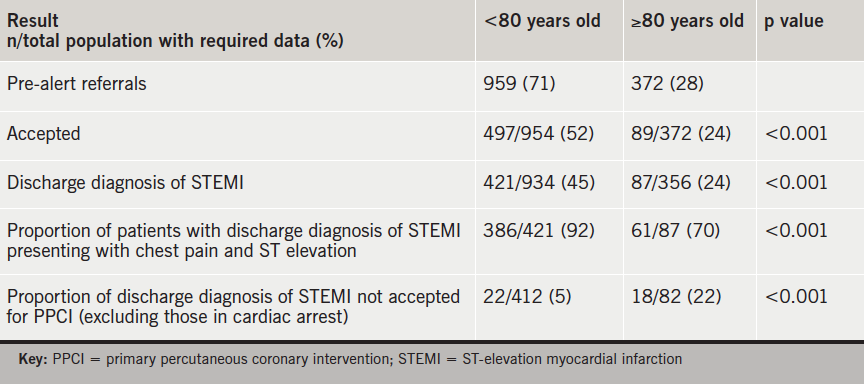
There were 372 (28%) patients referred aged ≥80 years, of which 119 (32%) had LBBB on ECG. Detailed results related to age comparison are described in table 2.
Table 2. Comparison of results dependent on age of patient referred
Of referrals, 430 (32%) were female. There were 167 (39%) accepted for PPCI, compared with 417 (49%) of males. Of females discharged with a diagnosis of STEMI, 127 (84%) were referred with chest pain and ST elevation on ECG, compared with 318 (91%) of males.
Of referrals, 1,217 (91%) came directly from paramedic crews. The remaining 126 (9%) were from local or regional hospitals, predominately ED. There were 60% (n=75) of referrals from the medical staff accepted compared with 42% (n=510) of paramedic referrals. Of patients referred by the medical team, 46% (n=57) were discharged with a diagnosis of STEMI versus 37% (n=451) of those referred from paramedics.
There were 52 (4%) documented calls with no identifiable patient information, which prevented recovery of final discharge diagnosis. Eight patients had no ECG or symptom data on which a judgement could be made. Of the remaining 44 patients; 42 had clear clinical or electrocardiographic reasons for declining. Two patients appeared to meet referral criteria but had no documented reason for declining. Therefore, maximally, 17 (3%) patients with a discharge diagnosis of STEMI were not accepted without documented reason.
Discussion
This study provides the first detailed analysis of PPCI pre-alert referrals in contemporary UK practice. A high proportion of calls to the pre-alert pathway do not fulfil referral criteria, but even without routine ECG transmission the pre-alert triage process effectively selects appropriate patients for PPCI, with 92% of accepted patients having a cardiological final diagnosis that would have been likely to require cardiology input, and only 3% of STEMI patients declined without a reason documented on the proforma. A number of these patients may have had a clinical reason for declining that was not documented on the pre-alert proforma, but this could not be ascertained in the present study. Comparative assessment of the overall performance is limited by the absence of published data from other centres or clear standards for benchmarking. Discussion with other UK PPCI centres suggests that access to the pathway via a dedicated nurse- or coordinator-led pre-alert phone line is widespread, but variation exists with regard to the availability of ECG transmission and routine blanket acceptance, the latter being, in practice, limited to same-site PPCI centre and EDs.
Other data suggest that paramedic interpretation of ECGs with ST elevation is robust (positive predictive value 82%).5 Therefore, the high referral level of patients not meeting criteria, particularly from the paramedic crews, may be the result of the paramedics’ perceived vulnerability in community assessment of patients with chest pain and desire for further expert support. Our aim is to maintain sound communication and supportive links with our referring paramedics, thus, maximising direct calls from the crews, as immediate ambulance transfer shortens door-to-balloon time,5 which is a key goal of the pathway. Providing an effective ECG transmission service would be the ideal long-term addition to optimise this support.
The findings that females and patients aged over 80 years with a discharge diagnosis are more likely to be declined for PPCI is likely attributed to atypical presentation and increased comorbidity, affecting appropriateness of acceptance for the PPCI pathway. Certainly, the atypical nature of the presentation is supported by the lower proportion of patients presenting with both chest pain and ST elevation on ECG in the population diagnosed with STEMI on discharge. The relationship between these demographics is apparent in published data6,7 and reflected in our study (53% of referred patients over 80 are female compared with 26% of those under 80). The importance of this is the poorer prognosis in both groups6,7 and evidence of delayed symptom to balloon time.7
Encouragingly, a high percentage (77%) of those accepted had a discharge diagnosis of STEMI, and, of the accepted not discharged with a diagnosis of STEMI, two thirds had a cardiological diagnosis. There is likely to be an acceptance bias towards those perceived to have a cardiological presentation, if not a STEMI, e.g. dysrhythmia with possible ST elevation or widespread ST elevation.
Amendments to our pathway have been supported in light of the results. We have questioned the role for acceptance of LBBB, which accounted for 19% of pre-alert calls, since in the present study no cases of acute thrombotic coronary occlusion were seen in these patients. Other UK data have reported a similar proportion of LBBB in patients accepted for PPCI of 5.5%, with only 17% of these having coronary occlusion in that series.8 At present, our approach is to continue to receive referrals for LBBB, but to only accept cases whose presentation is highly suggestive of acute myocardial infarction (MI), with mandatory discussion with the medical team prior to acceptance. We have mandated that no cases with chest pain and ST-elevation on the ECG can be declined without discussion with medical personnel, and that all declined cases must have a reason documented for declining the patient. This will help to improve our data, optimise patient care, and provide support to the pre-alert nursing team.
The results have additionally highlighted specific populations of patients that do not fulfil referral criteria, but should be considered unstable and high risk. This has led to a unified departmental decision for direct acceptance to the PPCI centre, particularly focusing on patients with transient ECG change and those now pain free but with persistent ECG changes.
Following this study, the pre-alert proforma has been redesigned to streamline data retrieval at the time of the pre-alert call and improve the completeness of data for further audit (appendix 1).
Limitations
This study only included activations of the PPCI pathway that occurred via the pre-alert call system. Other PPCI activation mechanisms, such as patients already on the cardiology wards or referrals made directly to medical staff would not have pre-alert proformas and would not be captured in this study. However, correlation with the PCI database for 2013 demonstrated that 93% of PPCI procedures performed were referred via the pre-alert system.
As our service currently has no facility for remote community ECG transmission, the ECG diagnosis was based on interpretation reported by on-scene staff rather than direct visualisation. Any inaccuracy in interpretation only reflects the information available at the time of the initial management decision.
There were some missing data, due to the nature of retrospective analysis of clinical data captured in a busy emergency setting. However, the amount of incomplete data was low, and unlikely to have substantially altered the analysis, as suggested by assessment of the absent data accounted for in the final results.
Since there are no data for comparison, or to act as a benchmark for our service, assessment of successful service provision must be interpreted with caution.
Conclusion
Patients are frequently referred who do not meet symptom and ECG criteria, however, our pre-alert system correctly identifies the majority of appropriate STEMI patients without burdening the service with non-cardiological patients. Without comparable data, we cannot conclusively comment on our department’s performance, but hope minor alterations will enable improvement to an already acceptable service.
Acknowledgements
Thanks to the Yorkshire Ambulance Service and East Midlands Ambulance Service for support in establishing our pre-alert system and continuing input. Many thanks to Dr Pierluigi Constanza, Dr Ali Ali, Dr Ali Razaand Dr Rachel Davidson for their assistance in data retrieval from our regional district general hospitals. Further thanks to Liverpool Heart and Chest Hospital, Queen Elizabeth Hospital Birmingham, St George’s Hospital London, Southampton General Hospital, Royal Edinburgh Infirmary, Leeds General Infirmary, Nottingham City Hospital and Freeman Hospital Newcastle for liaising with us regarding their service structure.
Conflict of interest
None declared. No funding was received for this research.
Key messages
Only 52% of pre-alert referrals had both chest pain and an electrocardiogram (ECG) meeting criteria
38% of all referrals had a discharge diagnosis of ST-elevation myocardial infarction (STEMI)
77% of accepted patients had a discharge diagnosis of STEMI, with two thirds of the remainder having an alternative cardiac diagnosis
3% of patients meeting PPCI referral criteria were declined without a documented clinical reason
Patients over 80 years and females with a discharge diagnosis of STEMI were less likely to present with ST elevation and chest pain and more likely to be declined
Appendix 1. New design pre-alert proforma
References
1. Grines CL, Brown KF, Marco J et al. A comparison of immediate angioplasty with thrombolytic therapy for acute myocardial infarction. The Primary Angioplasty in Myocardial Infarction Study Group. N Engl J Med 1993;328:673–9. http://dx.doi.org/10.1056/NEJM199303113281001
2. Steg G, James SK, Badano LP, Borger MA, Ducrocq G, Gershlick AH. ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology. Eur Heart J 2012;33:2569–619. http://dx.doi.org/10.1093/eurheartj/ehs215
3. O’Gara PT, Kushner FG, Ascheim DD et al. ACCF/AHA guideline 2013. ACCF/AHA guideline for the management of ST-elevation myocardial infarction. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013;127:e362–e425. http://dx.doi.org/10.1161/CIR.0b013e3182742cf6
4. National Institute for Health and Care Excellence. NICE guidelines 167. The acute management of myocardial infarction with ST-segment elevation. London: NICE, 2013. Available from: http://guidance.nice.org.uk/cg167
5. Le May MR, Dionne R, Maloney J, Poirier P. The role of paramedics in a primary PCI program for ST elevation myocardial infarction. Prog Cardiovasc Dis 2010;53:183–7. http://dx.doi.org/10.1016/j.pcad.2010.08.003
6. Claussen PA, Abdelnoor M, Kvakkestad KM, Eritsland, Halvorsen S. Prevalence of risk factors at presentation and early mortality in patients aged 80 years or older with ST-segment elevation myocardial infarction. Vasc Health Risk Manag 2014;10:683–9. http://dx.doi.org/10.2147/VHRM.S72764
7. Van der Meer MG, Nathoe HM, van der Graaf Y, Doevendans PA, Appelman Y. Worse outcomes in women with STEMI: a systematic review of prognostic studies. Eur J Clin Invest 2015;45:226–35. http://dx.doi.org/10.1111/eci.12399
8. Brown AJ, Hoole SP, McCormick LM, Malone-Lee M, Cacciottolo PJ, Schofield PM, West NE. Left bundle branch block with acute thrombotic occlusion is associated with increased myocardial jeopardy score and poor clinical outcomes in primary percutaneous coronary intervention activations. Heart 2013;99:774–8. http://dx.doi.org/10.1136/heartjnl-2012-303194
Left-sided dropped shoulder syndrome (DSS) can present with anterior chest pain that radiates to the left scapula and arm. Patients with atypical chest pain (ACP) of unknown cause (n=47) were investigated for left-sided DSS. Sixteen patients (34%) were diagnosed with left DSS. All the 47 patients were provided physiotherapy in two groups: the left DSS patients group (n=16) and a control group of 31 patients who did not show the criteria for the diagnosis of DSS.
Fourteen (87.5%) patients reported a satisfactory improvement of the ACP after physiotherapy. Satisfactory improvement has been judged by the reduction of the pain intensity, duration and frequency according to the patient’s report. Two (12.5%) patients showed no satisfactory improvement of the ACP. The control group showed no beneficial effect regarding their ACP after physiotherapy.
Physiotherapy aimed to strengthen the muscles that elevate the shoulder, could provide a treatment for atypical chest pain caused by left-sided DSS.
Introduction
Atypical or non-anginal chest pain (ACP) is any chest pain that has no cardiac cause. ACP is a common clinical condition encountered in everyday cardiology practice and constitutes about half of the cases of chest pain presented to emergency departments.1-5
Figure 1. X-ray showing dropped shoulder syndrome in an 18-year-old woman
The causes of this complaint are varied, and controversial aetiologies (musculoskeletal, neurological, psychological, mediastinal, pulmonary and gastrointestinal) have been suggested.3,4,6-9 ACP may result from cervical root compression, which can be confirmed by magnetic resonance imaging (MRI) findings.10
Scapular region pain is generally the initial symptom in cervical radiculopathy and can present alone before the arm or finger symptoms develop. The site of the pain is valuable for determining the localisation of the involved root.11
Cervical radiculopathy of C7, C8 and T1 roots could be caused by dropped shoulder syndrome (DSS) (figure 1).12 Left-sided DSS is presented with anterior chest pain that radiates to the left scapula, left upper arm and could be associated with numbness of the arm down to the hand.
Patients and methods
There were 112 patients with ACP who fulfilled the inclusion criteria included in this study between January 2013 to October 2014. The ethics committee of Welfare hospital has approved the research proposal and every patient has signed the consent form accepting the limited disclosure of his/her medical record according to the international standards of investigations on human subjects.
The inclusion criteria of the patients with ACP were:
History of chest pain with at least one admission to an emergency department with normal cardiac enzymes and troponin T.
Aged less than 40 years, of both sexes.
Non-diabetic, normotensive, nonsmoker and not obese (central obesity: waist circumference ≥102 cm male, ≥88 cm female).
Normal fasting blood sugar, complete blood count, renal function tests, lipid profile and thyroid function tests.
Normal electrocardiogram (ECG) and stress ECG.
Normal echocardiography.
The patients’ data were collected from their medical files. Diagnosis at discharge was: musculoskeletal (36 patients, 32%), gastrointestinal (13 patients, 12%), psychiatric (11 patients, 10%) and pulmonary (5 patients, 4%). The remaining 47 patients (42%) were labelled with ACP of unknown cause.
Those 47 patients were investigated for left DSS as a cause of their ACP. The ACP was central and/or left sided, of 1–6 years’ duration (average of 3.2 years). Pain lasted for more than 2–3 hours and came in varied frequencies. In 36 (76.6%) patients, the frequency was 1–3 times a week, while in the other 11 (23.4%) patients, pain occurred 1–2 times a month. In all the patients, pain was precipitated by heavy and/or prolonged manual work, and partially relieved by rest and over-the-counter (OTC) pain medications.
These 47 patients were sent for cervical plain X-ray, MRI, and electromyography/nerve conduction study (EMG/NC study). Single-blinded EMG/NC study of left (biceps, deltoid, triceps, flexor carpi ulnaris, abductor pollicis brevis, abductor digiti minimi, first dorsal interosseous, and the paraspinal) muscles and (musculocutaneous, axillary, median, ulnar, medial and lateral antebrachial) nerves were performed.
Table 1. Symptoms and signs of the dropped shoulder syndrome (DSS) patients
Sixteen patients (34%) were diagnosed with left DSS. The patients’ age was between 19 and 39 years. Three were males and 13 were females providing a male:female ratio of 1:4. Physiotherapy designed to elevate the shoulders was initiated for 12–16 weeks,12 and a fortnightly evaluation of the responses to the exercise were recorded.
All the 47 patients were included in the physiotherapy in two groups. The left DSS patients group and a control group of 31 patients who did not show the criteria for the diagnosis of DSS.
Results
Left DSS was found to be the cause of ACP in 16 patients (14.3%). Three major criteria were used for diagnosing left DSS: shoulder pain that radiates to the chest, neck, left scapular region, and the left upper limb down to the hand; lateral view of cervical X-ray showing eight or more vertebrae (the first, second, and, rarely, the third dorsal vertebrae) and a denervation EMG pattern of the C7, C8 and T1 innervated muscles.12
The other 31 patients were having ACP without left DSS. The MRI of one patient (0.9%) showed a prolapsed inter-vertebral disc at the level of C7–T1. The symptoms of the patients with left DSS are summarised in table 1. Clinical examination showed no evidence of vascular disorder. Motor power and tone examination were normal. Other clinical signs in left DSS patients are shown in table 1.
The cervical X-ray of DSS patients showed seven cervical vertebrae plus the first ± second thoracic vertebrae. No cervical rib could be detected on both sides. Neck muscle spasm was suggested by loss of normal lordosis in 12 patients (75.0%). The MRI and NC studies of all the patients with DSS were normal. Denervation EMG pattern was detected at left C7, C8 and T1 roots territories in 14 patients (87.5%), while two (12.5%) patients showed a denervation EMG pattern at left C8/T1 roots. All the patients showed a denervation EMG pattern of the lower segment of cervical paraspinal muscles (table 2).
Table 2. Findings of the patients’ tests
Fourteen (87.5%) patients reported a satisfactory improvement of the ACP after physiotherapy. Satisfactory improvement has been judged by the reduction of the pain intensity, duration and frequency according to the patient’s report. Two (12.5%) patients showed no satisfactory improvement of the ACP. The control group showed no beneficial effect regarding their ACP after physiotherapy.
Discussion
Diagnosing the cause of a patient with ACP broadly as ‘neurogenic’ or ‘musculoskeletal’, without defining the real specific diagnosis, will lead, in most of the cases, to an empirical management approach. Most of these patients are treated by pain killers ± muscle relaxant, which is not always proved to be effective.
In this study, 14.3% of the ACP patients have been diagnosed with left DSS after fulfilling the criteria of the diagnosis.12 The neurogenic ACP caused by DSS has an explainable anatomical origin. In 2010, Mizutamari et al. demonstrated the anatomy behind the clinical presentations of pain in patients with C6, C7, C8/T1 radiculopathy.13
The vast majority of the patients (87.5%) who were diagnosed with left DSS reported a satisfactory improvement of their pain after physiotherapy. Physiotherapy aimed to strengthen the muscles that elevate the shoulder, which could also affect the natural history of the pain-producing mechanism/s in the cervical spine. This indicates that left DSS is a rather treatable cause and should be considered as one of the causes of ACP.
Conflict of interest
None declared.
Key messages
Atypical chest pain in young adults could be caused by lower cervical radiculopathy due to left-sided dropped shoulder syndrome
The diagnosis is based on history of chest pain with characteristic features of radiation, cervical plain X-ray and electromyography findings
Physiotherapy aimed at strengthening the muscles that lift the shoulders showed a satisfactory improvement of atypical chest pain in most of the patients
References
1. Spalding L, Reay E, Kelly C. Cause and outcome of atypical chest pain in patients admitted to hospital. J R Soc Med 2003;96:122–5. http://dx.doi.org/10.1258/jrsm.96.3.122
2. Summers RL, Cooper GJ, Carlton FB, Andrews ME, Kolb JC. Prevalence of atypical chest pain descriptions in a population from the southern United States. Am J Med Sci 1999;318:142–5. http://dx.doi.org/10.1097/00000441-199909000-00008
4. Hung Cl, Hou CJY, Yeh HI, Chang WH. Atypical chest pain in the elderly: prevalence, possible mechanisms and prognosis. Int J Gerontology 2010;4:1–8. http://dx.doi.org/10.1016/s1873-9598(10)70015-6
5. Adamek RJ, Roth B, Zymanski CH, Hagemann B. Esophageal motility patterns in patients with and without coronary heart disease and healthy controls. Hepatogastroenterology 1999;46:1759–64.
6. Basha I, Mukerji V, Matt PL, Alpert M, Beitman B. Atypical angina in patients with coronary artery disease suggests panic disorder. Int J Psychiatry Med 1989;1914:341–6. http://dx.doi.org/10.2190/AK3T-V52N-7D5Y-GFF6
13. Mizutamari M, Sei A, Tokiyoshi A, Fujimoto T, Taniwaki T, Togami W, Mizuta H. Corresponding scapular pain with the nerve root involved in cervical radiculopathy. J Orthop Surg (Hong Kong) 2010;18:356–60. Available from: http://www.josonline.org/pdf/v18i3p356.pdf
Coenzyme Q10 (CoQ10) is a naturally occurring vitamin-like substance that has three functions of relevance to cardiovascular function: (i) its key role in the biochemical process supplying cardiac cells with energy; (ii) its role as a cell membrane protecting antioxidant; (iii) its direct effect on genes involved in inflammation and lipid metabolism. Although some CoQ10 is obtained from the diet, most is manufactured within the liver, the capacity for which declines with age. These data therefore provide a rationale for the importance of CoQ10 in cardiovascular function, and its dietary supplementation. The objective of this article is therefore to provide a brief overview of the pharmacology of CoQ10, and its role in the prevention and treatment of cardiovascular disease.
A record-breaking meeting of the European Society of Cardiology (ESC) was held in London this year with over 37,000 delegates from all over the world attending. There were 28 clinical presentations at Hot Line sessions, 18 clinical trial updates, 20 registry studies, five new ESC guidelines published, and 4,533 abstracts presented during the five-day meeting from 29th August–2nd September 2015. We present its highlights.