Physio-Control, a global leader in lifesaving emergency response technology, is launching a new automated external defibrillator (AED) in European countries (LIFEPAK® CR2).
The LIFEPAK® AED Response System:
Features a new design intended for ease of use by bystanders and rescuers
Launches new technology that supports high quality cardiopulmonary resuscitation
Has been demonstrated to offer faster time-to-first-shock
Deploys a new remote monitoring and connectivity capability through the online LIFELINKcentral™ AED Program Manager. The CR2 can be remotely monitored and can even, in some areas, transmit a heart rhythm to emergency medical professionals before they arrive on the scene.
Manifesto for a ‘health-creating’ society
Brexit and the troubled state of the NHS call for re-thinking the UK’s approach to health, according to a call-to-action from clinicians, scientists, social entrepreneurs and crossbench peers published recently in The Lancet (doi: 10.1016/ S0140-6736(16)31801-3).
The EU referendum vote reveals deep social divisions as well as presenting the country with important decisions and negotiations about the future, say the authors. At the same time, health problems are growing, they argue: “the NHS faces severe financial constraints and appears to lurch from crisis to crisis, with leaving the European Union likely to exacerbate many problems including staffing issues across the whole sector”.
They review new scientific developments and digital technologies which could offer societies everywhere massive and unprecedented opportunities for improving health.
NICE recommends ticagrelor post-MI
The National Institute for Health and Care Excellence (NICE) has published a Final Appraisal Determination (FAD) recommending ticagrelor 60 mg with aspirin as an option for preventing atherothrombotic events in adults who have had myocardial infarction (MI) and who are at high risk of a further event.
“Secondary prevention for heart attack patients is critically important for their physical and psychological wellbeing,” said Professor Rob Storey (University of Sheffield). “Today’s NICE recommendation is an important step forward in enabling us as clinicians to continue reducing patients’ risk of a further atherothrombotic event, including another heart attack or stroke, in the first few years following an initial heart attack,” he added.
Medication to prevent MI linked to reduced severity
Medications prescribed to prevent myocardial infarction (MI), such as statins and aspirin, are also associated with reduced MI severity, according to research published recently in PLOS ONE (doi: 10.1371/journal.pone.0163068). The observational study in nearly 15,000 patients provides further evidence of the benefits of taking these medications.
This study assessed the relationship between prior use of four preventive medications (antiplatelet agents such as aspirin, angiotensin converting enzyme inhibitors/angiotensin receptor blockers, statins, and beta blockers) and in-hospital outcomes in patients with acute coronary syndromes (ACS).
Prior use of each medication was significantly associated with less severity of disease, less arrhythmia, and reduced risk of major adverse cardiovascular events during hospitalisation.
Semaglutide benefits – SUSTAIN-6 study
In patients with type 2 diabetes at high cardiovascular risk, the rate of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke is significantly lower among patients receiving semaglutide than among those receiving placebo, according to data from the SUSTAIN-6 study.
Patients were randomised in a 1:1:1:1 ratio to receive either 0.5 mg or 1.0 mg of once-weekly subcutaneous semaglutide or volume-matched placebo, which maintained blinding within dose. The trial consisted of a planned observation period of 109 weeks for all patients.
Statin use reviewed
A major review of the available evidence on the safety and efficacy of statin therapy, published in The Lancet (doi: 10.1016/ S0140-6736(16)31357-5), intends to help doctors, patients and the public make informed decisions about the use of the drugs. The authors warn that the benefits of statin therapy have been underestimated.
Lowering cholesterol by 2 mmol/L with an effective low-cost statin therapy (e.g. atorvastatin 40 mg daily, which costs about £2 per month in the UK) for five years in 10,000 patients would:
Prevent major cardiovascular events in 1,000 people with pre-existing vascular disease, and in 500 people who are at increased risk but have not yet had a vascular event.
Cause five cases of myopathy (which might progress to rhabdomyolysis, if the statin is not stopped), 5–10 haemorrhagic strokes, 50–100 new cases of diabetes and up to 50–100 cases of symptomatic adverse events.
HEART UK – The Cholesterol Charity has given its support to the review, endorsing the use of statins as safe and effective treatments for individuals with high cholesterol.
With help from Dr Jubin Joseph, President, British Junior Cardiologists Association (BJCA), we are very pleased to have invited a panel of junior cardiologists to work closely with us on the Journal. They will advise us on current and future developments in training and also with reviewing papers, books and advising on the ‘movers and shakers’ in the cardiology world.
Coronary artery disease
In the section on coronary artery disease we have Dr Satpal Arri, who is BHF Clinical Research Fellow and Cardiology SpR South Thames Rotation, Dr TiffanyPatterson, who is BCIS Trainee Representative and BHF Clinical Research Fellow, Cardiology SpR, Kings College, London and Dr Kully Sandhu, who is Cardiology Interventional Trainee, Royal Stoke University Hospital, West Midlands Deanery.
Dr Satpal Arri (South Thames Rotation)
Dr Jubin Joseph (St Thomas’ Hospital, London)
Dr Kully Sandhu (Royal Stoke University Hospital)
Dr Tiffany Patterson (Kings College London)
Cardiac electrophysiology
In this section we have Dr Rahul Mukherjee, who is Cardiology SpR and NIHR BRC Clinical Research Fellow in Cardiac Electrophysiology, Guy’s and St Thomas’ Hospital Biomedical Research Centre, Dr Rohan Wijesurendra, who is Clinical Lecturer in Cardiovascular Medicine, Honorary Cardiology Registrar, John Radcliffe Hospital, Oxford.
Dr Rohan Wijesurendra (John Radcliffe Hospital)
Dr Rahul Mukherjee (Guy’s and St Thomas’ Hospital Biomedical Research Centre
General cardiology
In this section we have Dr Christopher Allen, NIHR Academic Clinical Fellow and Cardiology SpR, St Thomas’ Hospital, London and Dr Joyee Basu, ST5 in Cardiology, CRY Clinical Research Fellow, St George’s Hospital, London.
Dr Joyee Basu (St George’s Hospital)
Dr Christopher Allen (St Thomas’ Hospital)
Heart failure
In this section we have Dr Resham Baruah, Cardiology SpR, North Thames Heart Failure Representative, and CT Fellow, Royal Brompton Hospital, London. Dr Rosita Zakeri, NIHR Clinical Lecturer, Heart Failure and Advanced Cardiovascular Imaging Fellow, Royal Brompton & Harefield NHS Trust, London.
Dr Rosita Zakeri (Royal Brompton & Harefield NHS Trust)
Dr Resham Baruah (Royal Brompton Hospital)
Heart valve disease
In this section we have Dr Nicholas D Gollop, who is MRC Doctoral Research Fellow in Cardiology, Norwich Medical School, University of East Anglia, Dr Margaret Loudon, who is a ST7 in the Oxford Deanery and BJCA Committee Representing the British Heart Valve Society and Dr Hannah McConkey, BHF Clinical Research Training Fellow, Cardiology SpR, King’s College and St Thomas’ Hospital, London.
Dr Margaret Loudon (Oxford Deanery)
Dr Nicholas D Gollop (University of East Anglia)
Dr Hannah McConkey (King’s College and St Thomas’ Hospital)
I wish to comment on recent work linking non-alcholic fatty liver disease (NAFLD) with a high risk of cardiovascular mortality.1,2 One issue which has not been addressed in these studies is the potential role of coenzyme Q10 (CoQ10) deficiency in the pathogenesis both of NAFLD and subsequent cardiovascular disease.
CoQ10 is a vitamin-like substance that plays a key role in the biochemical process supplying all cells with energy. CoQ10 also has antioxidant and anti-inflammatory action. An adequate supply of CoQ10 is particularly important in tissues with a high energy requirement, such as the heart and liver. Most of the body’s daily requirement for CoQ10 is provided by endogenous synthesis. Although CoQ10 is synthesised throughout the body, because of its size and high metabolic capacity, the liver serves as the major site of CoQ10 synthesis. In NAFLD patients where hepatic metabolic capacity has been compromised, reduction in CoQ10 production is likely to have a deleterious effect on both liver and cardiovascular function. Thus NAFLD is associated with heart failure, arrhythmias, valvular dysfunction and atherosclerosis. Depleted CoQ10 levels may be a particular problem in NAFLD patients prescribed statins, which inhibit both cholesterol and CoQ10 synthesis.
The question arises as to whether supplementation with CoQ10 in NAFLD could reduce the risk of cardiovascular disease, either by direct systemic replacement, or by stimulating the liver to synthesise more CoQ10. Recent controlled clinical trials (Q-SYMBIO and KISEL-103,4) have demonstrated, via direct supplemental replacement of systemic CoQ10, significant benefit in reducing the risk of cardiovascular mortality in patients with, or at risk of, cardiovascular disease.
In addition, Yessilova et al,5 reported depleted blood CoQ10 levels in NAFLD patients, with the decrease in CoQ10 correlating with increased liver inflammation and cirrhosis. Randomised controlled trials6,7 have shown CoQ10 supplementation significantly reduced levels of inflammation and oxidative stress in liver tissue, and improved liver function, and hence the capacity for increased endogenous CoQ10 synthesis.
In conclusion, we therefore suggest that supplementation with CoQ10 (3 x 100 mg Bio-Quinone daily) may reduce the risk of cardiovascular disease in NAFLD, initially by direct replacement, and subsequently by increased endogenous synthesis following improved liver function.
Conflict of interest
Dr Mantle is medical adviser to Pharma Nord (UK) Ltd.
David Mantle (FRSC FRCPath) Pharma Nord (UK) Ltd Morpeth Northumberland NE61 2DB ([email protected])
References
1. Pais R, Giral P, Khan J, et al. Fatty liver as an independent predictor of early carotid athersclerosis: results from a large transversal and long term follow-up. J Hepatol 2016;65:95–102. http://dx.doi.org/10.1016/j.jhep.2016.02.023
3. Mortensen SA, Rosenfeldt F, Kumar A, et al. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure. J Am Coll Cardiol HF 2014;2:641–9. http://dx.doi.org/10.1016/j.jchf.2014.06.008
4. Alehagen U, Johansson P, Bjornstedt M, et al. Cardiovascular mortality and N-terminal proBNP reduced after combined selenium and CoQ10 supplementation. Int J Cardiol 2012;167:1860–6. http://dx.doi.org/10.1016/j.ijcard.2012.04.156
5. Yesilova Z, Yaman H, Oktenli C, et al. Systemic markers of lipid peroxidation and antioxidants in patients with non-alcoholic fatty liver disease. Am J Gastroenterol 2005;100:850–5. http://dx.doi.org/10.1111/j.1572-0241.2005.41500.x
6. Farhangi MA, Alipour B, Jafarvand E, et al. Oral CoQ10 supplementation in patients with NAFLD: effects on serum vaspin, chemerin, pentraxin, insulin resistance and oxidative stress. Arch Med Res 2014;45:589–95. http://dx.doi.org/10.1016/j.arcmed.2014.11.001
7. Farsi F, Mohammadshahi M, Alavinejad P, et al. Functions of CoQ10 supplementation on liver enzymes, markers of inflammation and adipokines in patients with NAFLD: a double blind randomized placebo controlled clinical trial. J Am Coll Nutr 2016;35:346–53. http://dx.doi.org/10.1080/07315724.2015.1021057
The rationale behind secondary prevention post-ST-elevation myocardial infarction (STEMI) is well established. Guidelines recommend titration of several medications for secondary prevention up to a maximally tolerated dose in order to confer maximum benefit. Due to decreasing duration of inpatient stays post-myocardial infarction (MI), this up-titration must often take place in primary care. Guidelines also recommend clearly informing GPs regarding duration of dual antiplatelet therapy and monitoring cardiovascular risk factors. Clear communication between secondary/tertiary and primary healthcare practitioners is essential in order to ensure our patients are receiving optimum care.
We examined all discharge summaries for patients discharged post-STEMI in our tertiary referral centre. This encompassed rates of prescribing of the National Institute for Health and Care Excellence (NICE) recommended medications post-MI, rates of therapeutic prescribing of these medications and communication with GPs regarding duration of dual antiplatelet therapy, up-titration of medications and repeat checking of fasting lipid profiles. In order to improve compliance with guidelines, incoming junior staff were educated on guidelines for communication post-STEMI at our journal club. We then re-audited our practice in order to see if compliance with the guidelines improved.
Our results showed that, while the majority of our patients were discharged on the correct medications post-MI, most were receiving subtherapeutic doses of angiotensin-converting enzyme (ACE) inhibitors and beta blockers. In addition, we exhibited poor communication with primary healthcare practitioners. Compliance with the NICE guidelines on communication significantly improved after our intervention.
In conclusion, education of junior staff can significantly improve communication with GPs. This, in turn, could help optimise secondary prevention strategies post-MI.
Introduction
Coronary artery disease remains one of the leading causes of death in Ireland,1 the UK,2 and worldwide. Despite advances in management, it is a major source of morbidity and mortality in our healthcare system. Numerous trials (PROVE-IT,3 ISIS-1,4 ISIS-2,5 ISIS-3,6 ISIS-4,7 AIRE,8 CAPRICORN9) have established the prognostic benefits associated with adequate secondary prevention post ST-elevation myocardial infarction (STEMI).
National Institute for Health and Care Excellence (NICE) guidelines10 recommend all patients discharged post-STEMI should be offered treatment with an angiotensin-converting enzyme inhibitor (ACEi), beta blocker (BB), dual antiplatelet therapy (DAPT) and a statin. The evidence for these medications is based on trials in which the drugs were used at high doses. The benefit at lower doses is not clear and best practice dictates titrating medications up to the maximally tolerated dose. This has been shown to reduce morbidity and mortality for these patients, reducing recurrent hospital admissions, re-infarction and death.3–9
The guidelines10 also state that patients should be discharged with clear information for their general practitioner (GP) regarding incomplete dose titrations and plans for antiplatelet and anticoagulant treatment.
Clear instructions are essential, as GPs may be reluctant to make changes to medications prescribed by specialists. Given many medications cannot be up-titrated to maximally tolerated doses during brief inpatient stays,11 the GP plays a key role in ensuring this is done as an outpatient.
If the medication is not titrated up to the maximally tolerated dose, the patient may not derive maximum benefit and may suffer an increased risk of major adverse cardiac events (MACEs).
We hope that a focus on improved communication will lead to improved clinical outcomes, patient experience and continuity of care between primary and secondary or tertiary care services.
Materials and methods
In this study, we aimed to assess the compliance with guidelines on communication with GPs. Subsequently, we sought to improve this through education of our junior staff.
Using our STEMI database and the computerised discharge prescriptions on our electronic patient record (EPR) system, we analysed the prescribing rates of BB, DAPT, ACEi and statins for all patients presenting as STEMI calls in 2015. We also analysed the percentage of patients discharged on therapeutic doses of these medications. The presence or absence of clear instructions for GPs regarding up-titration of medication doses, duration of DAPT and repeating fasting lipid profiles was also noted.
For study purposes, the subtherapeutic doses of NICE recommended drugs for use post-MI were defined as those used in a previous audit on medication dosage post-STEMI:10
ACEi: lisinopril <10 mg per day, perindopril <4 mg per day, ramipril <5 mg per day
BB: atenolol <50 mg per day, bisoprolol <5 mg per day, carvedilol <25 mg per day, metoprolol <50 mg per day
Statins: atorvastatin <80 mg per day, rosuvastatin <10 mg per day, simvastatin <40 mg per day
Antiplatelets: aspirin <75 mg per day, clopidogrel <75 mg per day, ticagrelor <180 mg per day.
These were selected arbitrarily based on similar studies on therapeutic prescribing in the UK. Patients with no dose specified on the discharge prescription were classified as non-therapeutic.
It was felt that lack of education was a significant factor in our disappointing initial results. In order to tackle this, a short talk was delivered to the new junior doctors assigned to our service at the beginning of their cardiology rotation. This comprised of a brief overview of the NICE guidelines on communication with GPs post-STEMI, in addition to the results from our initial audit of practice over the previous year. A random sample of 34 consecutive STEMI discharges was then audited from the following three months (all STEMIs between 14 May 2016 to 14 June 2016) using similar methodology.
Rates of compliance were compared using the Z-test for two population proportions using a two-tailed test at a significance level of p<0.05.
Results
Our results are summarised in tables 1 and 2.
Table 2. GP instructions post-STEMI
Our initial study highlighted that there was significant room for improvement in communication with GPs. Only 19.87% of our discharge summaries informed the GP to up-titrate BB and ACEi to the maximally tolerated dose, however, therapeutic prescribing rates for these medications were only 17.4% and 14.14%, respectively. While some patients may have had contraindications to higher doses of these medications (bradycardia, hypotension, renal disease), it was felt to be unlikely that this was the case in over 80% of our patients.
Just over half of our discharge summaries informed the GP of the duration of antiplatelet therapy and only 36.8% informed them to repeat fasting lipids. This was despite only two-thirds of our patients being prescribed a therapeutic dose of a statin.
After our intervention, we achieved a statistically significant improvement in rates of communication with GPs with regard to duration of antiplatelet therapy and up-titration of medications. There was no statistically significant difference in communication regarding repeat testing of fasting lipid profiles (p=0.1936).
Discussion
Numerous trials have demonstrated the benefit of secondary prevention post-STEMI.3–9 This consists of medical treatment with DAPT, a statin and a BB. In patients with evidence of left ventricular dysfunction, ACEi have also been shown to confer a prognostic benefit.12 Adequate secondary prevention reduces major adverse cardiac events.10.
With improvements in management, inpatient stays for patients with acute infarcts have shortened considerably.13 This may make it difficult to up-titrate medication regimens to therapeutic dosages while under the care of the specialist team. In addition, some medications require monitoring of haemodynamic parameters like heart rate and blood pressure, or biochemical parameters like electrolytes and renal function, before deciding on dose up-titration. As such, the GP plays a crucial role in performing this as an outpatient. In order to facilitate this, it is essential that specialist care providers explicitly detail the need for up-titration of medications with instructions for the same.
The need to optimise outcomes post-MI is well described. Coronary artery disease is the leading cause of death in Ireland1 and amounts to a significant cost burden on the healthcare system. A study from the UK estimated the financial burden of suboptimal care post-MI to be in the region of £9 billion.14
Discharge summaries are a crucial component of the patient care pathway. They represent the continuation of care between specialist services and primary healthcare practitioners. They are an opportunity to communicate future plans for ongoing patient management and to provide guidance on long-term care with regard to medication regimens. However, these are usually completed by junior staff, who may be unaware of the guidelines regarding communication with primary care. They may also be uncomfortable explicitly dictating plans for up-titration of medications unless they themselves are explicitly informed of the same by their senior colleagues.
Our junior doctors rotate at three-monthly intervals through our service. Such frequent turnover presents a further challenge. In order to tackle this, an educational session was delivered to the incoming doctors regarding the results of our previous study and NICE guidelines on communication with GPs post-STEMI. As seen in table 2, this resulted in statistically significant improvements in rates of compliance with guidelines on communication with regard to medication up-titration and duration of DAPT.
This highlights the importance of continuous education of junior staff with regard to guidelines for communication. Improving this communication may, in turn, improve our patients’ long-term outcomes, by ensuring they are on the optimum secondary prevention regimen post-STEMI.
Conflict of interest
None declared.
Editors’ note
See also the editorial by Dr Terry McCormack (page 127) in this issue.
Key messages
Myocardial infarction is a significant cause of mortality and morbidity in modern healthcare
Adequate secondary prevention reduces major adverse cardiac events post-discharge
This requires communication with general practitioners regarding up-titration of medication regimens and plans for future treatment
Communication between secondary/tertiary services and primary healthcare providers can be substandard, potentially compromising patient care
Education of junior staff, who are often responsible for composing discharge summaries, is essential to ensure compliance with guidelines.
3. Cannon C, Braunwald E, McCabe C et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes (PROVE IT-TIMI 22). N Engl J Med 2004;350:1495–504. http://dx.doi.org/10.1056/NEJMoa040583
4. First International Study of Infarct Survival Collaborative Group. Randomised trial of intravenous atenolol among 16 027 cases of suspected acute myocardial infarction: isis-1. Lancet 1986;328:57–66. http://dx.doi.org/10.1016/S0140-6736(86)91607-7
5. ISIS-2 (Second International Study of lnfarct Survival) Collaborative Group. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17 187 cases of suspected acute myocardial infarction: ISIS-2. Lancet 1988;332:349–60. http://dx.doi.org/10.1016/S0140-6736(88)92833-4
6. ISIS-3 (Third International Study of lnfarct Survival) Collaborative Group. ISIS-3: a randomised comparison of streptokinase vs tissue plasminogen activator vs anistreplase and of aspirin plus heparin vs aspirin alone among 41 299 cases of suspected acute myocardial infarction. Lancet 1992;339:753–70. http://dx.doi.org/10.1016/0140-6736(92)91893-D
7. ISIS-4 (Fourth International Study of lnfarct Survival) Collaborative Group. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58 050 patients with suspected acute myocardial infarction. Lancet 1995;345:669–82. http://dx.doi.org/10.1016/S0140-6736(95)90865-X
8. The AIRE Study Investigators. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. The acute infarction ramipril efficacy (AIRE) study investigators. Lancet 1993;342:821–8. http://dx.doi.org/10.1016/0140-6736(93)92693-N
9. McMurray JJ, Dargie HJ, Ford I et al. Carvedilol reduces supraventricular and ventricular arrhythmias after myocardial infarction: evidence from the CAPRICORN study. Presented at American Heart Association Scientific Sessions in Anaheim, CA; November 11–14, 2001: abstract 3303.
12. Cleland JGF, Puri S. How do ACE inhibitors reduce mortality in patients with left ventricular dysfunction with and without heart failure: remodelling, resetting, or sudden death? Br Heart J 1994;72(3 suppl):S81–S86. http://dx.doi.org/10.1136/hrt.72.3_Suppl.S81
13. Saczynski JS, Lessard D, Spencer FA et al. Declining length of stay for patients hospitalized with AMI: impact on mortality and readmissions. Am J Med 2010;123:1007–15. http://dx.doi.org/10.1016/j.amjmed.2010.05.018
Following Brexit, like many other people with Irish parents, I started the process of applying for an Irish passport. The Irish embassy website informed me, to my surprise, that I had become an Irish citizen on the day I was born. Despite that status, and despite owning a home in County Kerry, I have to admit I know very little about the Irish healthcare system. In fact, having worked my entire life in English healthcare, I do not fully understand the systems in the other three constituent countries of the UK either. My career has mostly involved both primary and secondary care, so I do understand the issues and difficulties of communication between hospitals and general practitioners (GPs).
Terry McCormack (Spring Vale Medical Centre, North Yorkshire)
It was, therefore, with great interest that I read the paper by Coughlan et al. (see pages 138–40). The authors raise very important points regarding both the importance of adequate discharge information and the poor delivery of appropriate up-titration of medicines when the patient has arrived home post-ST-elevation myocardial infarction (STEMI). They cite the failure of junior doctors to give adequate instructions to GPs on how to up-titrate medications and how educating the juniors improved performance. But they raise more questions than they answer. Why not have a pre-printed pro forma to attach to discharge summaries with this information on it? Why educate the juniors who rotate every four months and not the GPs, who do not? Why not cut out the middleman?
Discharge summaries
Discharge summaries should be produced at the point of discharge and given to the patient. The information on them should be in a form that the GP understands and, ideally, the patient can also understand. Discussions with GP colleagues could facilitate better discharge information. One of our local tertiary care centres admits to writing the discharge summary to comply with the Myocardial Infarction National Audit Project (MINAP). As a result of this, the GP receives lots of highly technical information, which is meaningless. An ideal discharge summary is on one, maximum two, sheets of paper and only contains relevant material.
I would take issue with the instruction to perform a fasting lipid profile. There is little to gain in requiring the patient to fast when they are on a statin. I would also take issue with the definitions of subtherapeutic doses of statins including rosuvastatin <10 mg per day. I would want to have at least 20 mg of this statin after my STEMI.
Questions not asked
Then there are the questions not raised in the paper, which are of equal importance, i.e. down-titration and stopping medications. The authors point out that National Institute for Health and Care Excellence (NICE) guidelines state that there should be clear information for the GP regarding plans for antiplatelet and anticoagulant treatment. Quite right, we say. But who really knows the answers to these questions? When should antiplatelets be stopped? What should we do about the vexed question of mixing an antiplatelet with an anticoagulant? Indeed should we be stopping beta blockers at some point? There are plenty of outstanding research questions.
I must thank the authors for highlighting this issue and hopefully sparking some debate. The journal would welcome more contributions regarding best practice in discharge communication.
P.S. I have some news relevant to my previous comments about Brexit. I have just stepped down as Secretary of the British Hypertension Society. One of my duties this year was to organise a poll of members regarding a change of name for the society. We ran the poll at the same time as the Brexit referendum. As a result of our poll, and subsequent ratification at our annual business meeting held in Dublin on 20 September 2016, we are now known as the British and Irish Hypertension Society (BIHS).
Conflict of interest
TM has previously received honoraria from AstraZeneca, Bayer, BMS/Pfizer, Boehringer-Ingelheim and Daiichi-Sankyo who market statins, anti-platelets and/or anticoagulant medications.
Editors’ note
See also the article by Coughlan et al. on pages XXX of this issue.
Ischaemic heart disease (IHD) is the leading cause of mortality worldwide.1 It is a debilitating, life-changing illness that can reduce quality of life and life-expectancy. While surgical, percutaneous and optimal medical interventions can significantly improve the clinical course of the disease, our understanding of the biopsychosocial mechanisms promoting survival following an acute IHD event, such as an acute coronary syndrome (ACS), is still limited.
The role of marital status and social support is becoming increasingly recognised as an important factor promoting recovery and rehabilitation following ACS.2
Marital benefits
There are several large and robust studies that show that marriage infers a survival benefit following an ACS.3–6 The mechanisms behind these survival benefits are not fully understood, but are thought to be associated with living a healthier lifestyle, improved social support, assistance with medication, and rehabilitation compliance. There are opposing claims that an ‘unhappy marriage’ may infer cardiovascular health complications.7 However, in most cases, people who are at highest risk of suffering ACS are often older (in our data, mean age was 66.6 years [standard deviation 14.3]), and many marriages at this stage are considered stable and ‘happy’.
Nicholas D Gollop (The University of East Anglia and Norfolk and Norwich University Hospitals)
Our group has recently analysed data investigating marital status on mortality and length of stay in patients admitted with ACS in England, using the ACALM (Algorithm for Comorbidities, Associations, Length of Stay and Mortality) study protocol. We, and others, have successfully used and published our methodology previously.8,9
We anonymously analysed over 929,000 patients National Health Service (NHS) health records and identified over 25,000 new diagnoses of ACS over a 13-year period. Our results showed that being married inferred a 14% survival benefit over being single following an ACS. We also showed that being divorced resulted in an increased mortality of 21% versus being married.2 These data highlight the impact and importance of key biopsychosocial factors contributing to mortality following an ACS, including the effects of anxiety, depression, use of tobacco, alcohol excess, worsening lifestyle, and social isolation.10
A second factor to consider is that, to date, there is limited evidence investigating how marital status relates to length of stay (LOS) following ACS. The average cost for a patient to stay on a cardiology ward is up to £400 per day. The numbers really start to add up when you scale this up across the entire NHS. It is estimated that reducing LOS in cardiology alone carries a potential cost saving opportunity to the NHS of £9.8 million/year.11,12
We showed that being married reduced the LOS in hospital by two days compared with being single (6 days vs. 8 days) following admission with ACS, and that being widowed resulted in an extended LOS of 10 days.2 These findings highlight a key issue; the NHS is spending millions of pounds per year on keeping people in hospital following an ACS, who may be better served in the community with increased social support and rehabilitation.
Emerging evidence suggests that being married reduces the incidence of IHD, reduces the LOS following ACS and infers a survival benefit following this event. Being married may provide positive modifications in lifestyle behaviours, inferring protection from recognised cardiovascular risk factors. Benefit is greatest for men and in early marriage, as is consistent with the gendered life course perspective and cumulative disadvantage framework.13
Compared with married people, individuals who are in the process of divorce or recently divorced who suffer a serious health event may experience negative modifications in lifestyle behaviours, resulting in increased levels of cardiovascular risk (such as increased incidence of smoking, alcohol excess, obesity, reduced physical activity), may suffer increased levels of anxiety, depression and social isolation following ACS.14
Thus, addressing biopsychosocial cardiovascular risk factors may be a key step in promoting survival in single and divorced people.15 It is important for clinicians, local/national cardiac charities and the NHS to acknowledge the potential benefits that additional biopsychosocial support may provide for patients.
Providing support
Following ACS, access to education and medical advice is crucial. Often people are not sure ‘what they can do to help themselves’. This point highlights the significance of education and multi-disciplinary care following ACS. Clear medical advice, structured specialist follow-up, psychological, physical therapy, and dietetic input, can all provide excellent support to help rehabilitate people after ACS.16 The focus of rebuilding patient confidence, physical state and emotional wellbeing is of the utmost importance.
A novel and potentially important concept is the introduction of an integrated social support programme for single and divorced people following ACS. The creation of a specialist, community-based social support network, may provide an additional level of care that people often need following a life-changing illness. Support groups (for those without the support of a spouse) may help reduce some of the biopsychosocial issues faced by single and divorced people following ACS. These groups could be organised by local/national cardiac charities and could be facilitated by patients who have survived an ACS event and who want to share their experiences and provide advice to others. They could be attended by members of the multi-disciplinary team to provide continuity of support, ease of access to services and, maybe, help avoid unscheduled hospitalisations by initiating community services and outpatient referrals when indicated.
A final consideration is that specialist psychological input may be important for those people who are in the process of, or who are recently divorced, following ACS. The divorce process is incredibly stressful and, as discussed, may result in poorer health outcomes.14,17 We acknowledge the increased mortality in this subgroup and suggest that targeted psychological therapy may be an important intervention. Divorce counselling may provide individuals, who have suffered ACS with a focus on making sense of what has happened. This may help people move on and progress with their lives. This intervention may enable these people to focus on their recovery, and to enter into an integrated social support programme.18
In England and Wales, the provision of health education, social support networks, and psychological intervention is limited for people who have suffered ACS. Often, these people are seen in clinic, surgically or medically optimised and then discharged back to their GP without being offered any psychological or social support.
Evidence is accumulating to suggest that management of biopsychosocial cardiovascular risk factors is central for successful recovery and rehabilitation following ACS. It is important to note that single and divorced people may have reduced access to this support based on their marital status and social circumstances, and that the National Institute for Health and Care Excellence (NICE) does not suggest routine referral for psychological support.
Integrated specialist social networks, pragmatic community-based multi-disciplinary care and targeted psychological support may improve quality of life, reduce mortality, and reduce LOS for this subgroup following ACS.17 All of which, may help fix thousands of
broken hearts and save the NHS millions of pounds.19
Conflict of interest
Dr Nicholas D Gollop is an investigator for the ACALM Study Group.
References
1. Piccolo R, Giustino G, Mehran R, Windecker S. Stable coronary artery disease: revascularisation and invasive strategies. Lancet 2015;386:702–13. http://dx.doi.org/10.1016/S0140-6736(15)61220-X
2. Hayes RM, Carter PR, Gollop ND et al. The impact of marital status on mortality and length of stay in patients admitted with acute coronary syndrome. Int J Cardiol 2016;212:142–4. http://dx.doi.org/10.1016/j.ijcard.2016.03.066
3. Koskenvuo M, Kaprio J, Romo M, Langinvainio H. Incidence and prognosis of ischaemic heart disease with respect to marital status and social class: a national record linkage study. J Epidemiol Commun 1981;H35:192–6. http://dx.doi.org/10.1136/jech.35.3.192
4. Chandra V, Szklo M, Goldberg R, Tonascia J. The impact of marital status on survival after an acute myocardial infarction: a population-based study. Am J Epidemiol 1983;117:320–5.
5. Frisch M, Simonsen J. Marriage, cohabitation and mortality in Denmark: national cohort study of 6.5 million persons followed for up to three decades (1982–2011). Int J Epidemiol 2013;42:559–78. http://dx.doi.org/10.1093/ije/dyt024
6. Floud S, Balkwill A, Canoy D et al. Marital status and ischemic heart disease incidence and mortality in women: a large prospective study. BMC Med 2014;12:42–50. http://dx.doi.org/10.1186/1741-7015-12-42
7. Donoho CJ, Seeman TE, Sloan RP, Crimmins EM. Marital status, marital quality, and heart rate variability in the MIDUS cohort. J Fam Psychol 2015;29:290–5. http://dx.doi.org/10.1037/fam0000068
8. Green B, Gollop ND, Baig M, Uppal H, Chandran S, Potluri R. Prolonged length of hospital stay in Far-East Asian and Afro-Caribbean patients with cardiomyopathy. Int J Cardiol 2014;176:230–1. http://dx.doi.org/10.1016/j.ijcard.2014.06.012
9. Thakker C, Gollop ND, Carter P et al. Prevalence and length of hospital stay in patients with aortic valve disease is lower amongst South Asians. Int J Cardiol 2014;177:34–6. http://dx.doi.org/10.1016/j.ijcard.2014.09.040
10. Burkauskas J, Brozaitiene J, Bunevicius A, Neverauskas J, Zaliunaite V, Bunevicius R. Association of depression, anxiety, and type D personality with cognitive function in patients with coronary artery disease. Cogn Behav Neurol 2016;29:91–9. http://dx.doi.org/10.1097/WNN.0000000000000093
13. Liu H, Waite L. Bad marriage, broken heart? Age and gender differences in the link between marital quality and cardiovascular risks among older adults. J Health Soc Behav 2014;55:403–23. http://dx.doi.org/10.1177/0022146514556893
14. Dupre ME, George LK, Liu G, Peterson ED. Association between divorce and risks for acute myocardial infarction. Circ Cardiovasc Qual Outcomes 2015;8:244–51. http://dx.doi.org/10.1161/CIRCOUTCOMES.114.001291
15. Bahremand M, Alikhani M, Zakiei A, Janjani P, Aghei A. Emotion risk-factor in patients with cardiac diseases: the role of cognitive emotion regulation strategies, positive affect and negative affect (a case-control study). Glob J Health Sci 2015;8:173–9. http://dx.doi.org/10.5539/gjhs.v8n1p173
18. Gostoli S, Roncuzzi R, Urbinati S, Morisky DE, Rafanelli C. Unhealthy behaviour modification, psychological distress, and 1-year survival in cardiac rehabilitation. Br J Health Psychol 2016;18. [Epub ahead of print]. http://dx.doi.org/10.1111/bjhp.12204
19. Azeredo-Da-Silva AL, Perini S, Rigotti Soares PH, Anne Polaczyk C. Systematic review of economic evaluations of units dedicated to acute coronary syndromes. Value Health 2016;19:286–95. http://dx.doi.org/10.1016/j.jval.2015.11.015
Postural tachycardia syndrome (PoTS) is a form of dysautonomia, a term used to describe dysfunction of the autonomic nervous system. The condition can cause marked physical and cognitive impairment that can significantly impact upon activity. Although the exact UK prevalence is unknown, its frequency has stimulated an increase in studies. Occupational therapy services should place themselves in a position to respond to the potential need.
This study aimed to determine how PoTS impacts upon activity, in order for occupational therapists to understand the implications of this condition and develop appropriate interventions.
We recruited 201 adults (aged 18–70 years) via two patient support charities to participate in an online quantitative survey. Participants rated their experiences pre-symptoms versus present day in relation to their occupations, producing ordinal data under self-care, leisure and productivity domains, including their physical ability, motivation and fatigue levels.
The pre-symptom versus present day probability scores of <0.001 can be viewed as ‘very significant’ and confirm that PoTS has a significant negative impact across all three occupational domains.
In conclusion, PoTS has a significant negative impact upon occupation and is associated with considerable morbidity. With their understanding of the central role of occupation in wellbeing, occupational therapists may need to support people with PoTS in achieving a satisfying balance of occupations that will support their health.
Introduction
Postural tachycardia syndrome (PoTS) is a form of dysautonomia, a term used to describe dysfunction of the autonomic nervous system. Those living with PoTS can experience a vast array of symptoms that can be life-altering and debilitating.1 As well as a significant increase in heart rate upon standing, as a result of orthostatic intolerance, syncope and presyncope can occur, along with headaches, fatigue, palpitations, nausea and dizziness, which are usually relieved by lying down.2 Other autonomic functions, such as digestion, bladder control, temperature regulation and stress responses, may also be affected. Onset can be sudden or gradual, and for some individuals, there will be no known cause.1
The combination of physical and cognitive symptoms can significantly impact upon activity and, although the exact UK prevalence of this condition is unknown, there is an increased interest in the condition reflected in a greater frequency of studies within the literature. Therefore, occupational therapy services may anticipate additional opportunities to work with clients diagnosed with PoTS who experience mobility decline and disruption across employment, education and leisure pursuits.3 Occupational therapists recognise the purpose and power of these occupations and their role in health and wellbeing.4 Many researchers within the field have discussed the importance of individual choice and control over occupation in the lives of people who have been diagnosed with illness or impairment.5 Yerxa et al. state that “to engage in occupations is to take control”.6
The current published literature base primarily explores health-related quality of life,7,8 fatigue1 and cognitive function9 among those with a diagnosis of PoTS. However, information on the extent to which these factors impact upon activities of daily living remains sparse. Consequently, there was a need to carry out a UK-based, national quantitative investigation in order to gain a scoping view.
Methods
Our objective was to determine how PoTS impacts upon activity in order for occupational therapists to understand the implications of this condition and develop appropriate interventions.
We hypothesised that occupation will be affected by PoTS. This hypothesis was non-directional, as there is a lack of published literature to indicate a likely direction of the relationship between these two variables.
A web-based survey was selected to form the quantitative design of the study. This was hosted on Bristol Online Surveys for a period of 10 weeks and provided access to a national sample of individuals with a diagnosis of PoTS. Participants were recruited via two charity websites; STARS and PoTS UK.
Table 1. Employment status for people with postural tachycardia syndrome (PoTS) (n=201 – participants were able to select multiple choices)
The survey used demographic questions in order to learn more about the target population in conjunction with Likert scales. The Likert scales produced ordinal data under three clearly defined sections: self-care, leisure and productivity. Each scale was ranked 1–5 (1=low value, 5=high value), which allowed participants to rate their experiences pre-symptoms (PS) versus present day (PD) in relation to their day-to-day activities, including their physical ability, motivation and fatigue levels.
The theoretical heterarchy developed in Kielhofner’s Model of Human Occupation10 informed the development of the survey and acted as a body of knowledge to explore occupational impact.
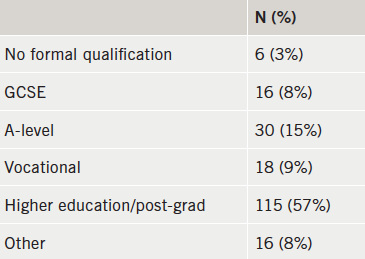
Table 2. Level of education (n=201)
Data analysis was performed within Statistical Packages for Social Sciences (SPSS) v23. The Wilcoxon signed-rank test located change within the sample by comparing PS versus PD.
Results
Participants
Formal data analysis took place on 201 adults including 194 women (96.6%) and seven men (3.4%). The age range of the sample was vast (18–70 years) with a mean age of 32.97 years. The mean age of first symptoms reported was 23.36 years with formal diagnosis being received at 30.35 years. The average period of time between first symptoms and diagnosis was found to be 6.99 years. There were 70 participants (34.5%) who were parents compared with 133 (65.5%) who were not. Employment status is shown in table 1.
Table 2 displays responses to the following question: “What is the highest level of education you have completed? (If currently enrolled, please state the level you are working toward)”.
A focus on occupation: PS versus PD
The occupational variables explored were: motivation, performance capacity and fatigue. These were considered along with the occupational domains (table 3). The PS versus PD median scores provided a significance level of p≤0.001 across every Wilcoxon signed-rank test (table 4).
Table 3. Impact of PoTS on occupation across age groups (difference in median score, significance)Table 4. Impact of PoTS on occupation, pre-symptoms versus present dayTable 5. Assistance with self-care activities (n=161)
In addition to the self-care questions included in the study, participants were asked: “If you responded to the previous question with a number 4 or 5, do you have help to complete self-care activities from another person?” (table 5).
Discussion
Demographics
The mean age of participants in this study is 32.97 years, with 30.35 being the average age of diagnosis and this appears to be quite typical across the current literature base.1,7-9
This study has a sizeable sample and reports an excessive mean diagnosis delay of 6.99 years. This reflects a significant period of time that individuals are living with debilitating, often life-changing symptoms with no formal explanation of their cause. Within this period of time a significant proportion of this population are diagnosed with anxiety or panic disorder due to tachycardia and adrenaline sensitivity.11 However, research has shown that those with PoTS are similarly, or even less likely, to experience anxiety than the general population.12,13
It could be suggested that misdiagnosis coupled with such a significant diagnostic delay could often result in a lack of support and resources from health professionals for a number of years. One important issue that cannot be overlooked is that the types of changes involved in positive adaptation require clear support and validation from the environment. People living with chronic illness require significant others, peers and health professionals to acknowledge and validate the illness, in order for support and practical advice to be provided.14
The impact of PoTS on occupation
The PS versus PD occupational scores of ≤0.001 can be viewed as ‘very significant’15 and confirm that PoTS has a significant negative impact upon motivation, performance capacity and fatigue, across all three occupational domains.
Self-care
Within the sample, 60 participants (37.3%) required assistance from their partner to complete self-care activities, including washing, dressing and bathing, followed by assistance from family members at 29.2% (n=47). The PS versus PD scores revealed that performance capacity and fatigue were affected more than motivation. All three variables were, however, significantly affected at the <0.001 level.
There is evidence to suggest that support from an individual’s social network increases in response to a significant change in health needs or function.16 Thoits17 suggests that this can have a positive effect on the health of those living with chronic illness. However, having to rely on family to support basic activities such as self-care can lead to a sense of powerlessness and a loss of autonomy for some.18
Employment
There were 140 (57%) participants in some form of employment or education, while 72 participants (29.3%) were unable to work or study as a direct result of their symptoms.
One of the most significant effects on occupation in the current study was demonstrated in relation to employment and performance capacity. Participants were far less physically able to manage in employment in the PD versus PS. Participation in work is an important occupation, offering income, socialisation, daily rhythms and often, wellbeing and meaning in life.19
Education
A large proportion of 91 participants (44.8%) were educated/working at degree level, followed by 30 (14.8%) at A-level. The distribution of responses for masters, vocational training and GCSE was equal at 8.9%. While motivation to engage in education was significantly affected, it was marginally less affected than performance capacity and fatigue.
These statistics could reflect a number of possibilities. The first is that PoTS is more likely to affect younger people and younger people are more likely to be at a stage in their lives where education is considered an important, meaningful occupation. Second, education has been found to directly influence health behaviours and access to healthcare by a range of researchers.20,21 Therefore, it could be possible that educated young women are more likely to persist in their quest for answers as to why they have moved from being healthy and able to engage in a range of occupations to being limited by fatigue and reduced performance capacity.
Parenting
The PS/PD scores of 1.00 versus 4.00 in the parenting domain demonstrated a significant difference in performance capacity. According to Barnado’s,22 61% of British parents describe parenting as ‘fairly’ or ‘very difficult’ and these difficulties are increased for those who are living with a chronic illness, such as PoTS.23
Occupational therapists recognise that many adults living with a long-term condition have parenting responsibilities. The ways in which services for adults and families are designed, accessed and delivered should ensure that the parenting role is fully supported.22 Meeting the, often, conflicting needs of a variety of parents and families will be a challenge to occupational therapy services, nevertheless, providing personalised support to parents living with PoTS and their families is a goal worth attaining.
Social and recreational activity
The greatest observable effect within the current study can be found within social and recreational activity. The effect of fatigue upon this occupational domain was particularly marked (PS=5.00, PD=1.00). This investigation has touched upon functional limitations that can hinder social engagement and similar limitations have been found in other studies.24
Stout and Finlayson25 found that those living with a chronic health condition decrease their participation in social and leisure occupations due to the fact that such activities are viewed optional in comparison to activities, such as self-care, parenting and work. Stout and Finlayson go on to suggest that eliminating social activities may leave more energy for basic activities of daily living. However, quality of life may be negatively influenced as a consequence.25
Conclusion
Health is strongly influenced by having choice and control in everyday occupations, and this study demonstrates that those living with the symptoms of PoTS are restricted in those opportunities. People with PoTS experience significant disruption in relation to their motivation, performance capacity and fatigue, across all three occupational domains.
Occupational therapists have a vast skill
set, which is adaptable to multiple and complex problems, or minor coping difficulties. 26 This skill set could be utilised to facilitate people with PoTS to achieve a satisfying performance and balance of occupations that will support their health, wellbeing and social participation.
Conflict of interest
None declared.
Key messages
Postural tachycardia syndrome (PoTS) has a significant negative impact upon motivation, performance capacity and fatigue, across all occupational domains
Occupational therapists have the skill set to work with those who have PoTS in order to facilitate a balance of occupations that will support health, wellbeing and social participation.
References
1. McDonald C, Koshi S, Busner L, Kavi L, Newton J. Postural tachycardia syndrome is associated with significant symptoms and functional impairment predominantly affecting young women: a UK perspective. BMJ Open 2014;4:e004127. http://dx.doi.org/10.1136/bmjopen-2013-004127
3. Kavi L, Nuttall M, Low D et al. A profile of patients with postural tachycardia syndrome and their experience of healthcare in the UK. Br J Cardiol 2016;23:33. http://dx.doi:10.5837/bjc.2016.010
4. Wilcock A. An Occupational Perspective of Health. 2nd ed. Thorofare: Slack, 2006.
5. Hammell KW. Using qualitative evidence to inform theories of occupation. In: Hammell KW, Carpenter C, eds. Qualitative Research in Evidence-based Rehabilitation. Edinburgh: Churchill Livingstone, 2004; pp. 14–26. http://dx.doi.org/10.1016/B978-0-443-07231-4.50006-7
6. Yerxa E. An introduction to occupational science: a foundation for occupational therapy in the 21st century. Occup Ther Health Care 1990;6:1–17. http://dx.doi.org/10.1080/J003v06n04_04
7. Bagai K, Song Y, Ling JF et al. Sleep disturbances and diminished quality of life in postural tachycardia syndrome. J Clin Sleep Med 2011;7:204–10.
8. Benrud-Larson LM, Dewar MS, Sandroni P, Rummans T, Haythornthwaite J, Low P. Quality of life in patients with postural tachycardia syndrome. Mayo Clin Proc 2002;77:531–7. http://dx.doi.org/10.4065/77.6.531
9. Anderson JW, Lambert EA, Sari CI et al. Cognitive function, health-related quality of life, and symptoms of depression and anxiety sensitivity are impaired in patients with the postural orthostatic tachycardia syndrome (POTS). Front Physiol 25 June 2014. http://dx.doi.org/10.3389/fphys.2014.00230
10. Kielhofner G. A Model of Human Occupation. 4th ed. Baltimore: Williams & Wilkins, 2008.
11. Grubb B, Rowe P, Calkins H. Postural tachycardia, orthostatic intolerance and the chronic fatigue syndrome. In: Grubb B, Olshansky B, eds. Syncope: Mechanisms and Management. 2nd ed. Maiden: Blackwell/Future Press, 2005;pp. 225–44. http://dx.doi.org/10.1002/9780470994801.ch13
12. Khurana RK. Experimental induction of panic-like symptoms in patients with postural tachycardia syndrome. Clin Auton Res 2006;16:371–7. http://dx.doi.org/10.1007/s10286-006-0365-0
13. Masuki S, Eisenach JH, Johnson C et al. Excessive heart rate response to orthostatic stress in postural tachycardia syndrome is not caused by anxiety. J Appl Physiol 2007;102:896–903. http://dx.doi.org/10.1152/japplphysiol.00927.2006
15. Field A. Discovering Statistics Using IBM SPSS Statistics. 4th ed. London: Sage Publications, 2014.
16. Vassilev I, Rogers A, Blickem C et al. Social networks, the ‘work’ and work force of chronic illness self-management: a survey analysis of personal communities. PLoS ONE 2013;8. http://dx.doi.org/10.1371/journal.pone.0059723
18. Asbring P. Chronic illness – a disruption in life: identity-transformation among women with chronic fatigue syndrome and fibromyalgia. J Adv Nursing 2001;34:312–19. http://dx.doi.org/10.1046/j.1365-2648.2001.01767.x
19. van Campen C, Cardol M. When work and satisfaction with life do not go hand in hand: health barriers and personal resources in the participation of people with chronic physical disabilities. Soc Sci Med 2009;69:56–60. http://dx.doi.org/10.1016/j.socscimed.2009.04.014
Authors: Peregrine Green, Stephanie Jordan, Julian O M Ormerod, Douglas Haynes, Iwan Harries, Steve Ramcharitar, Paul Foley, William McCrea, Andy Beale, Badri Chandrasekaran, Edward Barnes
Peregrine Green
Cardiology Specialist Registrar
Douglas Haynes
Cardiology Specialty Doctor
Iwan Harries
Cardiology Specialist Registrar
Steve Ramcharitar
Consultant Cardiologist
Paul Foley
Consultant Cardiologist
William McCrea
Consultant Cardiologist
Badri Chandrasekaran
Consultant Cardiologist
Edward Barnes
Consultant Cardiologist
Wiltshire Cardiac Centre, Great Western Hospital, Marlborough Road, Swindon, SN3 6BB
Stephanie Jordan
Core Medical Trainee
Andy Beale
Consultant Radiologist
Great Western Hospital, Marlborough Road, Swindon, SN3 6BB
Julian O M Ormerod
Cardiology Specialist Registrar
Oxford Heart Centre, Oxford University Hospitals, Headley Way, Headington, Oxford, OX3 9DU
National Institute for Health and Care Excellence (NICE) clinical guideline 95 (CG95) was introduced to rapid-access chest pain clinics (RACPC) to aid investigation of possible stable angina based on pretest probability of coronary artery disease (CAD). Following a six-month audit of its implementation we introduced a modified version: patients with low/moderate risk of CAD were referred for computed tomography coronary angiography (CTCA), while those at high/very high risk were referred for invasive angiography.
Patient records of 546 patients referred to our RACPC over a six-month period were retrospectively analysed. Pretest probability of CAD, referral for initial investigation, and outcomes at a minimum follow-up time of six months were documented.
Incidence of CAD correlated well with pretest probability. Moderate-risk patients had a low incidence of CAD and revascularisation. High/very high-risk patients had a high incidence of revascularisation, and this was predominantly for prognostically significant disease.
In conclusion, low rates of CAD in low- and moderate-risk groups justifies the use of CTCA as a first-line investigation in these patients. Routine investigation of very high-risk patients allows a high proportion to undergo revascularisation for prognostically significant disease. Strict adherence to NICE CG95 could lead to these patients being missed.
Introduction
The National Institute for Health and Care Excellence (NICE) clinical guideline 95 (CG95) was published in March 2010 and offers guidance to National Health Service (NHS) institutions on the further investigation of possible diagnoses of stable angina, based on pretest probability of coronary artery disease (CAD).1 Some recommendations were controversial, however, including the recommendation that patients with a very high risk of CAD (>90%) could be treated without further routine investigation with invasive coronary angiography. In addition, use of computed tomography (CT) calcium scoring or CT coronary angiography (CTCA) is recommended in low-risk patients (10–29%), with functional imaging for intermediate-risk patients (30–60%). However, previous studies have demonstrated that a negative CTCA can rule out CAD in low- and intermediate-risk patients.2 More recent European Society of Cardiology (ESC) guidelines have, therefore, recommended the use of CTCA as a first-line test in suitable patients with a lower range of intermediate pretest probability of CAD (15–50%), where it is a class IIa recommendation to be considered as an alternative to stress imaging.3
Our institution has previously audited the implementation of NICE CG95 in our rapid-access chest pain clinic (RACPC).4 This demonstrated that patients in the moderate-risk group (30–60%) had a low incidence of CAD, and those in the high-risk (61–90%) or very high-risk (>90%) groups had a high incidence of prognostically significant disease with subsequent high rates of revascularisation. As a result of this, we adjusted our local guidelines in a modification of the NICE CG95 protocol, such that patients with a high or very high risk of CAD (>60%) were referred for invasive coronary angiography, and those with low or moderate risk (≤60%) were referred for CTCA.
Method
A retrospective review was carried out of 546 consecutive electronic case records of patients referred to our RACPC from primary care and clinically assessed during the six-month period from 1 January 2014 to 30 June 2014. Patients were assessed by senior specialist nurses according to the locally modified version of NICE CG95 and, where indicated, referred for further testing.
Time from date of referral to being seen in clinic was documented, as well as initial pretest probability of significant CAD and investigations requested. Time to initial investigation was also recorded. The incidence of significant CAD (defined by the guideline as ≥70% diameter stenosis of at least one major epicardial artery segment or ≥50% diameter stenosis in the left main coronary artery at invasive coronary angiography1) and of revascularisation by percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG) was assessed at a minimum of six months following the end of the study period.
Results
A large group of patients were discharged without testing or referred on to cardiology outpatients
Of the 546 patients referred, 299 were male and 247 female, with a mean age of 62 ± 0.6 years (median 62 years). The mean and median time from date of referral to date seen was 12 days (data not available for four patients). One hundred and eighty-one patients (33%) were discharged from the RACPC without a test (figure 1). The large majority of these were assessed as having either no chest pain or chest pain that was clearly non-anginal in origin. A small number (five patients) had probable angina but further investigation was deemed inappropriate or declined by the patient, and so they were managed medically. The proportion directly discharged was higher than that in the original audit (25%).4 Thirty-six patients (7%) were referred directly to the cardiology outpatients department (OPD). These patients were judged to be suffering from problems other than angina, such as arrhythmia or heart failure. Fifty-five patients assessed (10%) had known CAD and were excluded from the study.
Figure 1. Summary of patient outcomes over the six-month period
Predicted risk of significant CAD correlated well with observed incidence
A breakdown of the investigations for which patients in each risk category were referred is given in table 1. No patients with very low (<10%) or low (10–29%) predicted risk of CAD were found to have significant CAD (figure 2a). Thirty-nine (81%) of the total patients in the very low- and low-risk groups were investigated with CTCA. None underwent revascularisation in the follow-up period. Only seven patients in the moderate-risk group (30–60%) had significant CAD (10% of the group) (figure 2a), with one uncertain (positive myocardial perfusion scan but no angiogram done). Four of these (6% of the group) underwent revascularisation in the follow-up period, of which two were for prognostically significant disease, as per the 2013 ESC guidelines (figure 2b).3
Table 1. Referral for each diagnostic test, stratified by predicted risk groupFigure 2a. Incidence of coronary artery disease (CAD) by pretest probability group
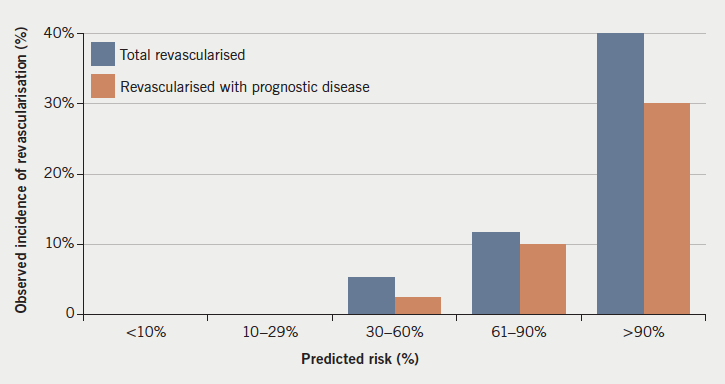
Twenty-four patients in the high-risk group (61–90%) had significant CAD (29% of the group) (figure 2a). Ten patients (12%) underwent revascularisation, of which, eight (10%) were for prognostically significant disease (figure 2b). Twenty-eight patients in the very high-risk (>90%) group had significant CAD (53% of the group) (figure 2a), plus one uncertain (positive exercise tolerance test [ETT] but no further testing). Twenty-one of these (40% of group) underwent revascularisation and one was referred for CABG, but died before surgery. Sixteen of those revascularised (30% of group) had prognostically significant disease (figure 2b).
Figure 2b. Incidence of revascularisation by pretest probability group
Over all risk groups, four patients who had a positive CTCA went on to have functional testing, of which, three tests were negative (two stress echoes [SEs], one myocardial perfusion scan [MPS]). One SE was positive, but this was possibly due to left bundle branch block, and, as symptoms settled, no further investigation was carried out. One is awaiting a SE. Three patients with significant CAD at angiography went on to have functional testing, of which two were negative (one SE, one MPS). One MPS was positive and the patient went on to have PCI.
Wait for CTCA was shorter than for stress echo
The mean time taken from being seen in the RACPC to having a CTCA was 32 days (median 30 days, data not available for one patient). For SE it was 96 days (median 84 days).
Frequent deviation from protocol
One patient (10%) in the very low-risk group, eight (22%) in the low-risk group and 33 (49%) in the moderate-risk group were referred for a test other than CTCA. If not referred for CTCA, the majority of the remainder of the moderate-risk group were referred for SE (18 patients, 26%). However, adherence to the protocol had improved in the low-risk groups from previously, when 33% of the very low-risk group and 32% of the low-risk group were referred for tests other than CTCA.4
Only 17 (21%) of the high-risk group and five (9%) of the very high-risk group were referred for tests other than invasive coronary angiography. Only four ETTs were carried out across all groups.
CTCA had a number of false-positive results
Ten patients (12% of total done) had CTCA suggestive of significant CAD and were referred for further investigation that was subsequently negative. Seven underwent diagnostic invasive coronary angiography, two had a SE and one a MPS. In addition, one patient is awaiting a SE. However, it should be noted that two of these scans only had calcium scoring carried out, rather than full angiography, due to technical difficulties. However, four positive scans (40% of false-positives) did have moderate CAD at invasive angiography, which did not reach criteria for significance, but would, nevertheless, have benefited from secondary prevention.
For comparison, the patient who had a positive SE was found to have significant coronary disease at invasive angiography.
Discussion
Overall, incidence of CAD correlated well with pretest predicated risk. However, the moderate-risk group (30–60%) had a low overall incidence (10%), which correlated well with the original audit (15%).4 This continues to lend support to our strategy to use CTCA as the first-line investigation in this group, freeing up more resource-intensive functional imaging for patients with known CAD. Indeed, this approach is in line with current ESC guidelines.3 The difference in time to investigation between CTCA and SE supports the hope that this will further improve waiting times.
A number of patients in the moderate-risk group continued to be referred for SE as a first-line investigation, reflecting continued deviation from the protocol. This could be due to issues implementing a guideline in real-world practice, and may also reflect residual adherence to the original CG95 protocol, and so a need for further assessor education in the RACPC. In addition, some patients may be unsuitable for referral for CTCA, for example those with a large body habitus or unable to have beta blockade to ensure optimal imaging during CTCA.
This continued use of SE in the moderate-risk group may partly account for the continued high waiting time for a SE found in this re-audit. However, it should also be noted that a large number of SEs were carried out in the known CAD group, which was excluded from the study (16 patients, 29% of patients with known CAD). The high waiting time may, therefore, also reflect the use of SE to assess known CAD in this cohort, and as fewer requests are made by the RACPC, this labour-intensive resource will be more available for this use.
Although CTCA had a false-positive rate of 12%, care should be taken in interpreting this. Although these patients did not have significant CAD at invasive angiography, as defined by NICE CG95, 40% did still have moderate CAD. This could be seen as a further advantage of CTCA over functional imaging, as detection of moderate CAD in these patients would allow aggressive risk factor modification to limit disease progression. In addition, the reliability of a negative CTCA in ruling out significant CAD, which has previously been demonstrated,2,5 should not be overlooked.
We have continued to show a high incidence of revascularisation in the very high-risk (>90%) group, predominantly for prognostically significant disease (30% of all patients in the group). This was larger than the rate of 10% found previously.4 This, therefore, continues to demonstrate that implementation of the NICE recommendations to treat this group medically, and not refer routinely for angiography, would likely lead to a significant number not undergoing prognostically beneficial revascularisation. This supports our decision to treat patients in this group in the same manner as high-risk (61–90%) patients, and carry out invasive coronary angiography.
Conclusion
Following our recently published study of the implementation of NICE CG95 in our RACPC, we introduced a locally modified version of this protocol, such that all low- and moderate-risk (≤60%) patients were referred for CTCA, while all high- or very high-risk (>60%) patients were referred for invasive angiography. Although significant deviation from the protocol was still found in some areas, there was a continued low incidence of CAD in low- and moderate-risk patients. In addition, a high incidence of revascularisation for prognostically significant disease in very high-risk (>90%) patients lends support to our approach to carry out angiography routinely in this group. We shall, therefore, continue to implement our modified version of NICE CG95 in our RACPC.
Acknowledgements
The authors would like to acknowledge the contributions of Harriet McCullough, Terri Thompson and Deborah Price.
Conflict of interest
None declared.
Key messages
Low incidence of coronary artery disease (CAD) in low- and moderate-risk patients justifies the use of computed tomography coronary angiography (CTCA) as a first-line investigation in these patients
A high proportion of very high-risk patients have prognostically significant CAD, which undergoes revascularisation
Use of a modified version of National Institute for Health and Care Excellence clinical guideline 95 (NICE CG95) should be considered given the above findings.
References
1. National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. CG95. London: NICE, 2010. Available from: http://www.nice.org.uk/guidance/CG95
2. Meijboom WB, van Mieghem CA, Mollet MR et al. 64-slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol 2007;50:1469–75. http://dx.doi.org/10.1016/j.jacc.2007.07.007
3. The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. 2013 ESC guidelines on the management of stable coronary artery disease. Eur Heart J 2013;34:2949–3003. http://dx.doi.org/10.1093/eurheartj/eht296
4. Ormerod JO, Wretham C, Beale A et al. Implementation of NICE clinical guideline 95 on chest pain of recent onset: experience in a district general hospital. Clin Med (Lond.) 2015;15:225–8. http://dx.doi.org/10.7861/clinmedicine.15-3-225
5. Mowatt G, Cummins E, Waugh N et al. Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease. Health Technol Assess 2008;12:iii–iv, ix–143. http://dx.doi.org/10.3310/hta12170
Bleeding is one of the complications associated with percutaneous coronary intervention from the femoral route due to the use of potent antiplatelet therapies including adenosine diphosphate receptor blockers and glycoprotein IIb/IIIa inhibitors. Complications include haematoma, retroperitoneal haemorrhage, pseudoaneurysm, arteriovenous fistula, arterial occlusion, femoral neuropathy and infection. Complications for diagnostic procedures are lower due to the lack of antiplatelet therapies on board. Often, incorrect location of the femoral artery puncture site results in complications. Puncturing below the femoral bifurcation can result in psedoaneurysm, haematoma and arteriovenous fistulas, whereas retroperitoneal haemorrhage is caused by high femoral punctures. Identification of bleeding and vascular complications is paramount as bleeding is associated with adverse events. Techniques to reduce the risk of femoral arterial complications include the use of ultrasound scan or fluoroscopy guided femoral punctures. Furthermore, the micropuncture technique has been shown to reduce complications but is not widely adopted. Ultimately, the radial route is preferable to the femoral route as vascular complications are significantly lower.
Released 17 November 2016 Expires: 17 November 2018 Programme: Angiography1 CPD/CME credit
Learning objectives
Upon completing this module, participants should be better able to appreciate that:
Knowledge of catheter lab equipment and coronary anatomy is vital to obtaining optimal diagnostic coronary angiogram images, while limiting radiation exposure and contrast load to the patient
Breaking the coronary vasculature down into segments when performing angiography helps to ensure that coronary stenoses are not missed
Optimal imaging of each segment depends on the use of the correct angiographic views
Faculty
Dr Peregrine Green, Cardiology Specialty Registrar
Dr Paul Frobisher, Superintendent Radiographer, Cardiology Catheter Laboratories
Dr Steve Ramcharitar, Consultant Cardiologist
Wiltshire Cardiac Centre, Great Western Hospital, Marlborough Road, Swindon, SN3 6BB
With thanks to Dr Chris Allen, Cardiology SpR, London Deanery, for assistance on the self-assessment aspect of the programme
Accreditation
BJC Learning suggests that one hour of learning on this ‘Learning with reflection’ activity should be equivalent to 1 CPD/CME point
You need to login to take this module
You need to be a registered member to view this page. It's quick, free and offers you a host of other benefits, including the facility to print and download articles and supplements, access our archived issues and receive email updates when new issues and other content are online.
 Physio-Control, a global leader in lifesaving emergency response technology, is launching a new automated external defibrillator (AED) in European countries (LIFEPAK® CR2).
Physio-Control, a global leader in lifesaving emergency response technology, is launching a new automated external defibrillator (AED) in European countries (LIFEPAK® CR2).