This supplement has been written by a medical writer with national insight gained from:
Craig Barr Consultant Cardiologist
The Dudley Group NHS Foundation Trust, Dudley
Evaun Teoh
Arrhythmia Nurse Specialist
St George’s Hospital, London
Shaumik Adhya
Clinical Lead for Cardiology
Medway NHS Foundation Trust, Medway
Sponsorship Statement: This supplement was commissioned and funded by Bayer. A medical writer was used to write this article which was developed following interviews with a number of clinicians and nurses who were not paid for their contribution.
Xarelto (rivaroxaban) prescribing information can be found here.
UKXAR07160212
Date of preparation: October 2016
Multiple clinical risk factors, electrocardiographic/echocardiographic features and biochemical markers are associated with an increased risk of atrial fibrillation (AF). AF poses a significant challenge from a public health perspective as it is associated with a four- to five-fold increased risk of stroke. The aim of treatment is to prevent stroke and alleviate symptoms.
Drug therapies include anticoagulants to reduce the risk of stroke and anti-arrhythmics to restore/maintain the normal heart rhythm or slow the heart rate in patients who remain in AF. Non-pharmacological management options include electrical cardioversion, which may be used to ‘shock’ the heart back to its normal rhythm.
The high risk of stroke associated with electrical cardioversion can be reduced by oral anticoagulation. Although effective in reducing the risk of thromboembolism, the limitations of warfarin present considerable challenges for its use in clinical practice. The challenges of maintaining warfarin within an appropriate therapeutic range combined with increased bleeding risk may contribute to issues with long-term treatment compliance.
Non-vitamin K oral anticoagulants (NOACs) have demonstrated comparable efficacy and safety profiles with warfarin for thromboprophylaxis in non-valvular AF patients undergoing cardioversion.
It is important that local arrangements for use of antithrombotic therapies in non-valvular AF should be reviewed and policies developed for integration of NOACs into the care pathways. Primary care prescribing of NOACs needs local leadership and, as the AF ‘epidemic’ continues to increase, local anticoagulant ‘champions’ will be required to take the lead.
This supplement, which has been initiated and funded by Bayer looks at developments in the use of oral anticoagulants in direct current cardioversion. It has been written by a medical writer with national insight gained from:
Craig Barr – Consultant Cardiologist, The Dudley Group NHS Foundation Trust, Dudley
Evaun Teoh – Arrhythmia Nurse Specialist, St George’s Hospital, London
Shaumik Adhya – Clinical Lead for Cardiology, Medway NHS Foundation Trust, Medway
Disclaimer: Medinews Cardiology Limited advises healthcare professionals to consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews Cardiology Limited cannot accept responsibility for any errors in prescribing which may occur.
This supplement has been written by a medical writer with national insight gained from:
Craig Barr Consultant Cardiologist
The Dudley Group NHS Foundation Trust, Dudley
Evaun Teoh
Arrhythmia Nurse Specialist
St George’s Hospital, London
Shaumik Adhya
Clinical Lead for Cardiology
Medway NHS Foundation Trust, Medway
Sponsorship Statement: This supplement was commissioned and funded by Bayer. A medical writer was used to write this article which was developed following interviews with a number of clinicians and nurses who were not paid for their contribution.
Xarelto (rivaroxaban) prescribing information can be found here.
UKXAR07160212
Date of preparation: October 2016
Atrial fibrillation (AF) is the most common type of sustained cardiac arrhythmia, with an overall prevalence in the UK of 1.6% in women and 2.4% in men.1 AF is most common in the elderly (prevalence of 0.2% in patients aged 45–54 to 8.0% in patients aged 75 years and older) and those with clinical risk factors such as myocardial infarction, hypertension, angina and diabetes.1 Importantly, AF poses a significant challenge from a public health perspective as it is associated with a four- to five-fold increased risk of stroke.2
Understanding the mechanisms of AF lies at the heart of its treatment. AF occurs when structural and/or electrophysiological abnormalities alter atrial tissue to promote abnormal impulse formation and/or propagation (figure 1).3 Multiple clinical risk factors, electrocardiographic/echocardiographic features and biochemical markers are associated with an increased risk of AF (table 1), and, AF can be described in terms of the duration of episodes using a simplified scheme (table 2).3
Figure 1. Mechanisms of atrial fibrillationTable 1. Risk factors3
The aim of treatment is to prevent stroke and alleviate symptoms.4 Drug therapies include anticoagulants to reduce the risk of stroke and anti-arrhythmics to restore/maintain the normal heart rhythm or slow the heart rate in patients who remain in AF.4 Non-pharmacological management options include electrical cardioversion, which may be used to ‘shock’ the heart back to its normal rhythm.4
Direct current (DC) cardioversion of AF was first reported in 1959,5 and this technique remains a reliable, safe and effective method to restore normal sinus rhythm.6 However, it has long been recognised that DC cardioversion is associated with a high risk of thromboembolic complications.7-9 It is now well established that anticoagulant therapy reduces the risk of stroke with the greatest benefit seen in patients at highest absolute risk.10-11 For several years, experts have recommended that patients who have had AF for more than two days should receive anticoagulation therapy for three weeks before elective cardioversion, and that anticoagulant should be continued until sinus rhythm has been maintained for four weeks.12 Unfortunately, anticoagulation therapy remains underused, particularly in the elderly, who doubtless have the most to gain from stroke prevention.10
Table 2. Definitions of atrial fibrillation3Table 3. CHA2DS2-VASc assessment of stroke risk and recommendation for anticoagulation13,15
Risk stratification schemas are used to categorise patients into low, moderate and high stroke risk in order to initiate anticoagulant therapy in patients at highest risk.13 Historically, the most common stroke risk stratification system has been the CHADS2 score (Congestive heart failure, Hypertension, Age ≥75, Diabetes mellitus, and prior Stroke or transient ischaemic attack [TIA]) within which a score of 0 categorises a patient as ‘low risk’, 1–2 as ‘moderate-to-intermediate risk’ and ≥3 as ‘high risk’.14 The most recent European Society of Cardiology (ESC) guidelines on AF recommend a new schema; CHA2DS2-VASc.15 The CHA2DS2-VASc scoring system places greater emphasis on the ‘major risk factors’ by allocating two points to each, with one point allocated for the presence of each of the other ‘clinically relevant non-major’ risk factors and anticoagulation thromboprophylaxis is initiated accordingly (table 3).13,15
Until recently, vitamin K antagonists (VKA), including warfarin, were the only oral anticoagulants recommended for antithrombotic therapy in patients at moderate-to-high risk of stroke, and, as such, warfarin has historically been the standard of care and foundation of thromboprophylaxis for stroke prevention in patients with AF.3,16 It is well established that the use of prophylactic warfarin in DC cardioversion significantly reduces the risk of ischaemic stroke and thromboembolism in patients with AF.11,17
DC cardioversion within the NHS
Under current National Institute for Health and Care Excellence (NICE) guidelines, rate control is the first-line treatment strategy for many adults with AF within the NHS.4 The guidelines recommend that DC cardioversion is used in AF patients whose symptoms continue after heart rate has been controlled (with beta blockers [first line], rate-limiting calcium-channel blockers, digoxin monotherapy or combination therapy) or for patients in whom a rate-control strategy has been unsuccessful.4
NICE guidelines advocate electrical (rather than pharmacological) cardioversion in patients with AF that has persisted for more than 48 hours.4 Also, as recommended by NICE, the CHA2DS2-VASc stroke risk score is routinely used within the NHS to assess stroke risk in patients with AF and in patients with AF for more than 48 hours, therapeutic anticoagulation is given for three to four weeks before cardioversion, and for at least four weeks afterwards, to minimise the risk of stroke.4 If the cardioversion is successful, anticoagulation may be stopped, however, patients at high risk of AF recurrence or increased risk of a stroke require continued treatment.4
In an emergency situation in patients with life-threatening instability caused by new-onset AF, NICE guidelines recommend that emergency electrical cardioversion should be performed without delay to achieve anticoagulation.4
Initiation and maintenance of warfarin in AF within the NHS
In the UK, anticoagulation is generally initiated within a secondary care setting, a dedicated hospital clinic or an outreach clinic in primary care.18 It takes 48–72 hours for the anticoagulant effect of warfarin to fully develop and warfarin should be taken at the same time each day.18
In direct contrast to patients with deep vein thrombosis or pulmonary embolism, rapid anticoagulation is not required in most patients with AF and a ‘slow-loading’ regimen is a safe and effective method of achieving therapeutic anticoagulation in the majority of patients within three to four weeks.18
Initiation at a dose of 1–2 mg per day is generally acceptable, with a lower starting dose in frail or elderly people and patients at high risk of bleeding.18 Warfarin treatment is usually long term for patients with AF, and the daily maintenance dose depends on the international normalised ratio (INR). A target INR of 2.5 is recommended for AF and, to achieve this, the daily maintenance dose of warfarin is usually 3–9 mg.18 However, significant variations in individual response due to a wide range of factors (age, genetics, concomitant drugs, diet, disease state) necessitate a daily dose between 1 mg and 15 mg in some patients.18
Cardioversion patients should achieve the target INR at least three weeks before cardioversion and four weeks after (if normal sinus rhythm is maintained).18
Non-vitamin K oral anticoagulants in cardioversion
Although effective in reducing the risk of thromboembolism, the limitations of warfarin, including a narrow therapeutic window, multiple drug and food interactions and the need for regular INR monitoring, present considerable challenges for its use in clinical practice.19-21 The challenges of maintaining warfarin within an appropriate therapeutic range combined with increased bleeding risk may contribute to issues with long-term treatment compliance.22
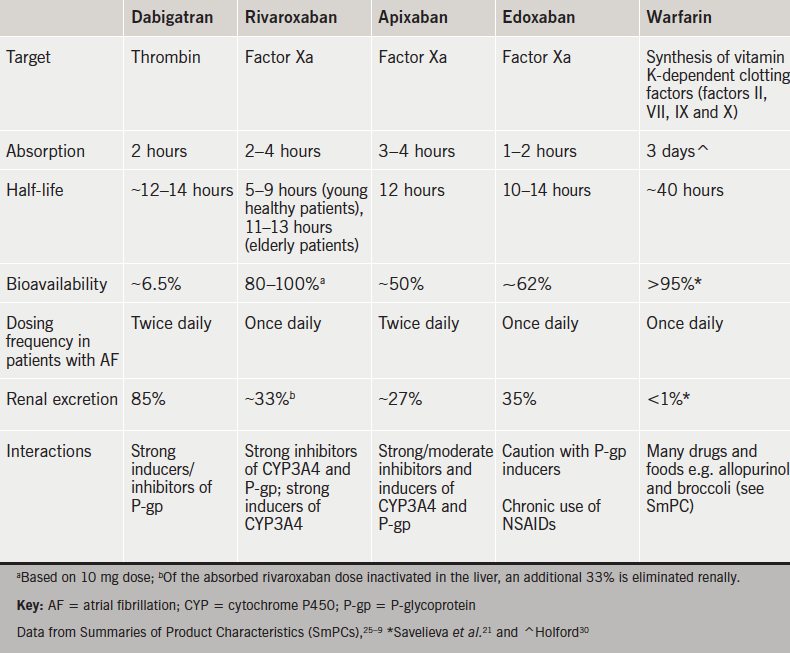
Four NOACs targeting either thrombin (dabigatran) or factor Xa (rivaroxaban▼, apixaban and edoxaban▼) have become available as alternative agents to warfarin.19,20,23–9 These NOACs offer the advantages of rapid onset of action, increased bioavailability, reduced half-life, fewer drug interactions and more predictable pharmacokinetic profiles compared with warfarin, thereby eliminating the need for routine coagulation monitoring (table 4).21,25–30
Table 4. Properties of warfarin and non-vitamin K oral anticoagulants
“NOACs represent an innovative treatment option and they are now generally being used as a default strategy for thromboprophylaxis in patients with AF,” reports Dr Craig Barr (Dudley Group NHS Trust). The use of NOACs for thromboprophylaxis is further supported by Dr Shaumik Adhya (Medway Foundation Trust and Honorary Consultant Cardiologist at Guy’s and St Thomas’ NHS Foundation Trust) who confirms, “Clinicians are confident in the use of NOACs and favour their flexibility.”
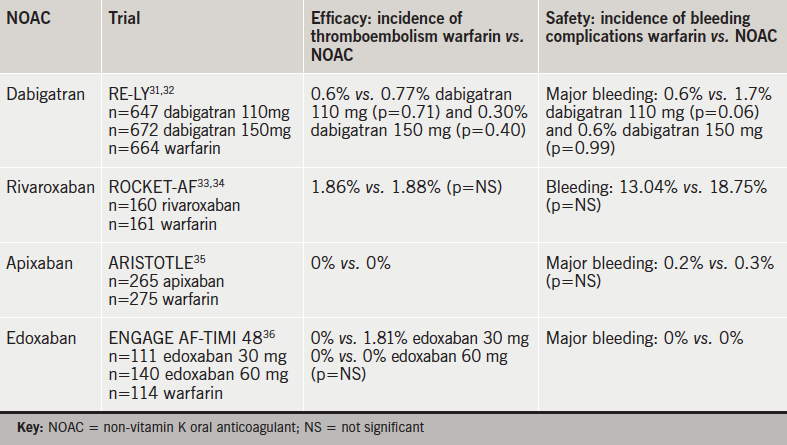
Large randomised-clinical trials (RCTs), as well as post hoc analysis, have demonstrated comparable efficacy and safety profiles compared with warfarin in non-valvular AF patients undergoing cardioversion (table 5).31–6
Table 5. Non-vitamin K oral anticoagulants in patients with atrial fibrillation undergoing cardioversion
Although the RE-LY (Randomized Evaluation of Long-term anticoagulation therapY) trial was not powered to detect differences in the absolute risk of embolism in patients undergoing cardioversion, results indicate comparable efficacy and safety profile of dabigatran versus warfarin and suggest that dabigatran may be a realistic alternative to warfarin in these patients.31,32
A post-hoc analysis of AF patients who underwent cardioversion in the ARISTOTLE study (Apixaban for Reduction In STroke and Other ThromboemboLic Events in atrial fibrillation) demonstrated comparable data for apixaban versus warfarin, as no stroke or systemic embolisms occurred in either warfarin or apixaban patients during a 30-day post-cardioversion follow-up.35
A post hoc analysis of the ENGAGE AF-TIMI 48 study concluded that thromboembolic and major bleeding events post cardioversion were infrequent and similar with edoxaban and warfarin.36,37
Comparable efficacy and safety profiles of rivaroxaban in patients undergoing cardioversion was demonstrated by post-hoc analysis of the ROCKET-AF (Rivaroxaban Once-daily oral direct Factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) trial.33,34 Results show a similar rate of stroke/systemic embolism with no significant difference in the incidence of major bleeding, but increased gastrointestinal bleeding, suggesting that rivaroxaban may be used as an alternative to warfarin in these patients.33,34
There is currently limited evidence supporting the use of NOACs in elective cardioversion (elective cardioversion was an exclusion criteria in the ROCKET-AF trial).33 The X-VeRT trial was designed to investigate the efficacy and safety profiles of rivaroxaban versus VKA in non-valvular AF patients undergoing elective cardioversion.38,39 The trial included 1,504 adult patients with haemodynamically stable non-valvular AF for more than 48 hours (or unknown duration) scheduled for elective cardioversion. Patients were randomised in a 2:1 ratio to anticoagulation with rivaroxaban (20 mg once daily [od]; 15 mg od in patients with renal impairment) or standard VKA therapy using one of two cardioversion strategies (early or delayed) and all patients received study treatment for six weeks post-cardioversion (figure 2). Early cardioversion involved rivaroxaban or standard VKA therapy one to five days before cardioversion, while delayed cardioversion involved rivaroxaban or standard VKA therapy 21 to 56 days before cardioversion.39
Figure 2. X-VERT study design
Results from X-VeRT demonstrate that rivaroxaban is comparable in efficacy and safety profiles to VKA therapy in non-valvular AF patients undergoing elective cardioversion. Overall, thromboembolism events occurred in 0.51% of rivaroxaban patients versus 1.02% of VKA patients (risk ratio 0.50; 95% confidence interval [CI] 0.15–1.73). In the rivaroxaban group, 0.71% of patients experienced thromboembolism events following early cardioversion and 0.24% following delayed cardioversion. In the VKA group, 1.08% of patients experienced thromboembolism events following early cardioversion and 0.93% following delayed cardioversion. Rivaroxaban was also associated with a significantly shorter time to cardioversion compared with VKAs (p<0.001) and risk of major bleeding was low and similar to that observed with VKA treatment (0.6% vs. 0.8% in the VKA group [risk ratio 0.76; 95% CI 0.21–2.67]). The results of the X-VeRT trial are aligned with the conclusions drawn from the ROCKET-AF study; rivaroxaban has the safety profile and is an effective alternative to warfarin in patients requiring anticoagulation therapy prior to, and following, cardioversion and may facilitate more rapid cardioversion.33,34,39
In January 2015, the European label for rivaroxaban was updated based on the findings from the X-VeRT study. Rivaroxaban is currently the only NOAC for initiation or continuation of anticoagulation in patients with non-valvular AF to demonstrate specific data for elective cardioversion within its SmPC.26 By comparison, the current data available support the use of dabigatran, apixaban and edoxaban only in patients to be continued on these agents if scheduled for cardioversion; the licences do not allow physicians to switch patients currently on warfarin to any of these NOACs.25,27
According to the current ESC guidelines and the joint recommendations by the European Society of Cardiology (ESC), the American College of Cardiology Foundation (ACCF), the American Heart Association (AHA) and the Heart Rhythm Society (HRS), NOACs should be considered in most patients with non-valvular AF as an alternative to an adjusted dose VKA,3,16 and specific recommendations at a European level are described in table 5.
Due to the heterogeneity of key RCTs and lack of head-to-head data, it is difficult for the guidelines to recommend one NOAC over the other. However, several practical considerations can be helpful in the selection of an appropriate agent for individual patients (figure 3).20
Figure 3. A proposed algorithm for non-vitamin K oral anticoagulant selection in patients with non-valvular atrial fibrillation
UK experience of NOACs in cardioversion
All four currently licensed NOACs have been approved by NICE as options for the prevention of stroke and systemic embolism in patients with non-valvular AF4 and are recommendations by the ESC for prevention of stroke and systemic embolism in patients with non-valvular AF (table 6).20
Table 6. European Society of Cardiology recommendations for the use of non-vitamin K oral anticoagulants in patients with non-valvular atrial fibrillation for prevention of stroke and systemic embolism
Kent
Kent’s regional experience of the use of NOACs in cardioversion to date has been very positive, reports Dr Shaumik Adhya (Medway Foundation Trust). Healthcare professionals (HCPs) from centres across the region have offered positive ‘real-world’ feedback on the initiation of patients on NOACs, particularly rivaroxaban, in their practices. Overall, clinicians are confident in their use of NOACs; they favour the flexibility and report that NOACs make surgical procedures more convenient.
Dr Adhya notes that the centres were in agreement that the need to counsel patients on the importance of adherence, and the possible consequences of non-adherence, remain the priority when initiating or continuing NOAC therapy prior to cardioversion. One concern associated with NOACs in this setting relates to compliance; many centres insist on signed pro-forma patient consent forms, clearly stating the responsibility of the patient in adhering to their treatment with NOACs prior to the procedure.
Dr Adhya reports that rivaroxaban remains the most frequently prescribed NOAC in the region, and the benefits, thus far, include a reduction in clinician consultation times and a reduction in cardioversion waiting lists due to a decrease in the number of patients previously unable to undergo scheduled cardioversion due to sub-therapeutic INR levels.
The Midlands
With three years and nearly 2,000 patient-years of experience of routine NOAC use at Russells Hall Hospital in Dudley, HCPs report positive clinical results and encouraging patient feedback. Dr Craig Barr (Dudley Group NHS Trust) highlighted how NOACs are now generally being used as a default strategy in patients with non-valvular AF to prevent stroke. He highlighted how rivaroxaban has generally been chosen as the preferred NOAC for a variety of reasons, including its once-daily dosing, its multiple indications and few drug interactions. This strategy, he said, had led to highly effective predictable anticoagulation, and no need for dietary restrictions or routine coagulation monitoring in patients.
Experience of using NOACs with patients undergoing cardioversion has been encouraging, reports Dr Barr. Ease of use and rapid onset of action are beneficial from both a patient and HCP perspective, with patients reporting an overall more favourable experience compared with warfarin. Patients are confident that the benefits outweigh the disadvantages and are reassured by the lower risk of bleeding.
HCPs in Dudley report clear-cut clinical advantages of NOACs including comparable efficacy to warfarin without the disadvantages and inconvenience associated with INR testing and drug/food interactions. The routine use of NOACs in the Midlands has resulted in timelier cardioversions (which may impact upon a greater long-term maintenance of sinus rhythm), very few cancellations and a shorter waiting time for cardioversion procedures.
HCPs report that, although NOAC compliance is an important aspect that is discussed with all patients in nurse-led clinics that are run on a weekly basis, after more than three years of experience, adherence is not a significant issue and patient consent is considered unnecessary and not routinely sought.
London
After more than two years of routine use, arrhythmia nurse Evaun Teoh (St George’s University Hospitals NHS Foundation Trust) reports “HCPs are extremely comfortable using all three of the currently available NOACs for cardioversion and stroke prevention.”
She further reports that, although clinician preference is a factor, choice of specific NOAC is primarily guided by specific protocols that take into consideration renal clearance and a patient’s prospects of compliance; younger patients are generally prescribed a daily NOAC, while older patients are considered more compliant (unless evidence of memory impairment) and are prescribed a twice-daily NOAC.
She feels that clinicians are reassured by the immediacy of effects, and patient feedback has been overwhelmingly positive, with patients reporting benefits in terms of ease of use and feelings of independence. Although some patients report rashes or gastrointestinal side effects, these usually occur following a change in dose and are generally mild.
St George’s have adopted a comprehensive specialist nurse-led patient-counselling programme to ensure NOAC compliance. The vital importance of compliance to ensure continuous efficacy is explained to the patient before a NOAC is initiated. The specialist nurse remains a long-term point of contact and various strategies, such as smart phone alerts, are in place to help patients remain compliant. The concept of ‘degrees of bleeding’ is also explained and all patients are advised to carry a patient alert card in case of internal/severe bleeding.
Setting up a pathway for a NOAC in cardioversion
The management of AF is complex and costly, and integrated care pathways (ICPs) are required to ensure optimal management and outcomes.
ICPs are a vital mechanism to ensure consistency and quality in healthcare; the overall purpose of ICPs is to improve outcome by providing a mechanism to coordinate care and to reduce fragmentation and ultimately cost.40
According to continuous quality improvement principles, the primary goal of clinical pathways for NOACs in cardioversion should be to improve clinical efficacy and efficiency within the healthcare system. Pathways are an evidence-based response to specific problems and care needs.
Although there are many potentially ‘ideal’ pathways, developing ICPs as part of an improvement project should follow the outline of ‘Improving the patient pathway’ published by the NHS Institute for Innovation and Improvement,41 and it has been documented that pre-cardioversion ‘work-up’ may be improved by installing clinical pathways led by nurse practitioners or physician assistants.42
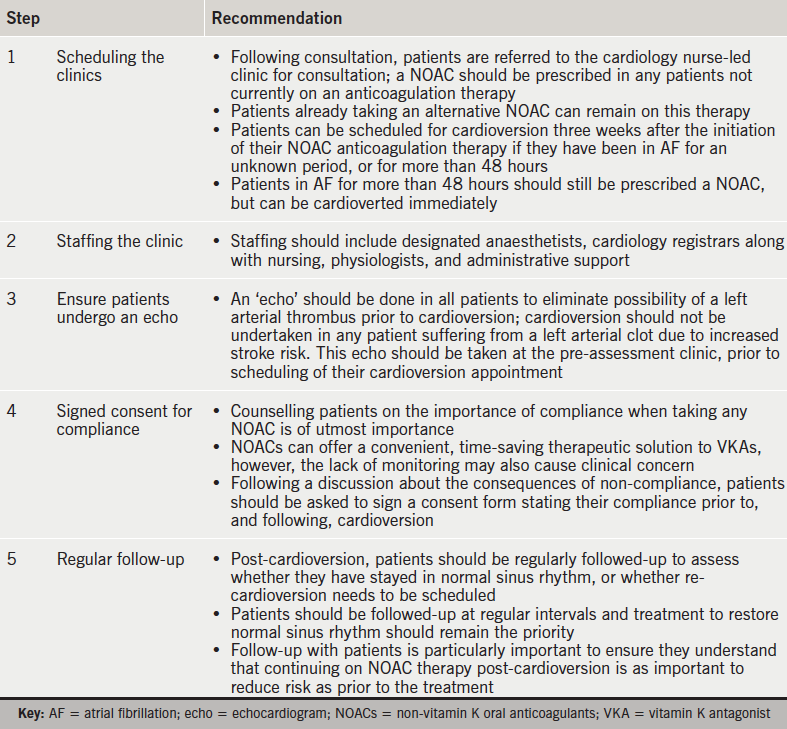
Figure 4 describes a potential pathway for the use of NOACs in cardioversion as used in various hospitals in Kent.
Figure 4. Potential pathway for the use of non-vitamin K oral anticoagulants in cardioversion. A starting point
Real-life experience: typical patient pathways on a NOAC versus warfarin
The ‘real-life’ experiences of two cardiologists and a nurse specialist from three regional centres have provided important insights into ‘typical’ patient pathways in the ‘real-world’. These are described in this section.
The experts note that a typical patient will present in primary care and, as a result, anticoagulation will be initiated by the GP. However, in reality a significant proportion of patients (around 40%) present as emergency or coronary care cases.
It is clear that the use of warfarin versus NOACs in a ‘real-life’ primary care setting is highly variable, and often based on historical anticoagulant use by the GP, lack of knowledge and potentially a lack of confidence in NOACs. As a consequence, warfarin is often initiated as the anticoagulant within the primary care setting. However, patients with a history of labile INRs, frequent travellers or patients taking antibiotics are often switched to NOACs for convenience.
In contrast, demonstrated efficacy and the advantages of simplicity of use have meant that NOACs are increasingly accepted and regularly initiated in the secondary care setting as the ‘default’ procedure. The experts interviewed report that HCPs in secondary care routinely initiate anticoagulation with NOACs (primarily rivaroxaban) no more than 21 days after presentation.
The experts note that potential for compliance may be a ‘real-life’ issue affecting the decision to initiate NOAC versus warfarin and HCPs report that warfarin may be a preferable option in potentially non-compliant patients. Conversely, diet, alcohol and use of over-the-counter medications impact the efficacy of warfarin, and the experts report these may be ‘real-life’ factors affecting choice of anticoagulant.
Once initiated, patients remain on anticoagulation for four weeks, after which, they are assessed to see if longer-term anticoagulation is required. This is subsequently initiated in the vast majority of cases, with many patients requiring life-long NOAC treatment. After a year of monitoring in secondary care, patients are usually then followed-up by their GP.
The experts reported that patients experience less challenging side effects with NOACs and although INR testing has become more easily accessible (self-testing/pharmacy testing now available), most patients prefer the convenience and flexibility offered by NOACs.
Electrical cardioversion of non-valvular AF with the NOACs: a single-centre UK-based registry experience
This registry-based study involved analysis of all consecutive patients undergoing electrical cardioversion between January 2013 and March 2014.43 A total of 229 procedures were performed during this period; 122 were anticoagulated with a NOAC (rivaroxaban 120, dabigatran 2, and mean age 63 ± 12, female 31%) and 107 with warfarin (mean age 67 ± 10, female 41%).
Overall, the results from the study revealed:43
No major bleeding episodes, stroke, thromboembolic events or death occurred in either group
Significantly fewer cancellations in the rivaroxaban group (1 patient [0.8%] due to dose omission vs. 11 patients [10.3%] in the warfarin group due to subtherapeutic INRs on the day of the procedure, p=0.004)
Shorter mean procedural waiting time in the NOAC group in comparison with warfarin group (mean ± standard deviation [SD] = 67 ± 49 vs. 95 ± 66 days, p=0.006)
A trend towards greater procedural success in the NOAC group, 94% (115/122), compared with warfarin, 79% (85/107, p=0.001).
This single-centre experience of cardioversion along with the NOACs demonstrates that the procedure is effective and has a good safety profile. Cardioversion is performed in a more timely fashion, with very few cancellations and shorter waiting time, which may impact upon a greater long-term maintenance of sinus rhythm.43
Looking to the future
The NOACs are set to provide a realistic therapeutic alternative to VKAs in non-valvular AF patients undergoing cardioversion, providing a therapeutic option that reduces clinic waiting times, reduces time spent in hospital for patients and minimises rescheduling of procedures due to subtherapeutic INRs.
The use of NOACs in cardioversion should involve an approach based on the published data, patient comorbidities and procedural factors,20 and policies need to be developed for integration of NOACs into local care pathways.44 There is a requirement for alignment of treatment protocols across primary and secondary care and a NOAC should be considered for newly diagnosed patients and as a ‘switch’ in certain VKA patients.44
In patients scheduled for cardioversion, a NOAC should be the preferred option to enable early cardioversion, which can occur approximately three weeks after initiation of the NOAC. Extra counselling should be performed to ensure that the patient fully understands the necessity for compliance, as non-compliance would leave the patient unprotected against thromboembolism. A proforma is signed by the patient and counsellor, with emphasis on drug compliance pre- and post-cardioversion.44
Practical steps to ensure correct clinic set-up are outlined in table 7.
Table 7. Practical steps on introducing non-vitamin K oral anticoagulants
Summary
The high risk of stroke associated with DC cardioversion can be reduced by oral anticoagulation, and NOACs have demonstrated comparable efficacy and safety profiles with warfarin for thromboprophylaxis in AF patients undergoing cardioversion.
It is important that local arrangements for use of antithrombotic therapies in non-valvular AF should be reviewed and policies developed for integration of NOACs into the care pathways.44 Primary care prescribing of NOACs needs local leadership, as GPs should not be expected to be experts in the area of anticoagulation for AF, and as the AF ‘epidemic’ continues to increase, local anticoagulant ‘champions’ will be required to take the lead.44
References
1. Davis RC, Hobbs FD, Kenkre JE et al. Prevalence of atrial fibrillation in the general population and in high-risk groups: the ECHOES study. Europace 2012;14:1553–9. http://dx.doi.org/10.1093/europace/eus087
3. January CT, Wann LS, Alpert JS et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014;130:2071–104. http://dx.doi.org/10.1161/CIR.0000000000000040
4. National Institute for Health and Care Excellence. Atrial fibrillation: the management of atrial fibrillation. CG180. London: NICE, June 2014. Available from: https://www.nice.org.uk/guidance/cg180 [accessed July 2015].
5. Vishnevskii AA, Tsukerman BM, Smelovskii SI. Control of fibrillating arrhythmia by the method of electrical defibrillation of the atrium. Klin Med (Mosk) 1959;37:26–9.
8. Resnekov L, McDonald L. Complications in 220 patients with cardiac dysrhythmias treated by phased direct current shock, and indications for electroconversion. Br Heart J 1967;29:926–36. http://dx.doi.org/10.1136/hrt.29.6.926
9. McCarthy C, Varghese PJ, Barritt DW. Prognosis of atrial arrhythmias treated by electrical counter shock therapy. A three-year follow-up. Br Heart J 1969;31:496–500. http://dx.doi.org/10.1136/hrt.31.4.496
11. Gallagher MM, Hennessy BJ, Edvardsson N et al. Embolic complications of direct current cardioversion of atrial arrhythmias: association with low intensity of anticoagulation at the time of cardioversion. J Am Coll Cardiol 2002;40:926–33. http://dx.doi.org/10.1016/S0735-1097(02)02052-1
12. Singer DE, Albers GW, Dalen JE et al. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133(suppl 6):546S–592S.
14. Gage BF, Waterman AD, Shannon W et al. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA 2001;285:2864–70. http://dx.doi.org/10.1001/jama.285.22.2864
15. Camm AJ, Kirchhof P, Lip GY et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J 2010;31:2369–429. http://dx.doi.org/10.1093/eurheartj/ehq278
16. Camm AJ, Lip GY, De Caterina R et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012;33:2719–47. http://dx.doi.org/10.1093/eurheartj/ehs253
17. Arnold AZ, Mick MJ, Mazurek RP et al. Role of prophylactic anticoagulation for direct current cardioversion in patients with atrial fibrillation or atrial flutter. J Am Coll Cardiol 1992;19:851–5. http://dx.doi.org/10.1016/0735-1097(92)90530-Z
18. National Institute for Health and Care Excellence. NICE Clinical Knowledge Summaries. Anticoagulation oral. London: NICE, February 2015. Available from: http://cks.nice.org.uk/anticoagulation-oral#!changes [accessed July 2015].
19. Mann A, Ruskin J, Heist EK. Cardioversion and catheter ablation of atrial fibrillation using novel oral anticoagulants. The Journal of Innovations in Cardiac Rhythm Management 2014;5:1792–9.
20. Maan A, Heist EK, Ruskin JN, Mansour M. Practical issues in the management of novel oral anticoagulants – cardioversion and ablation. J Thorac Dis 2015;7:115–31. http://dx.doi.org/10.3978/j.issn.2072-1439.2014.11.35
21. Savelieva I, Camm AJ. Practical considerations for using novel oral anticoagulants in patients with atrial fibrillation. Clin Cardiol 2014;37:32–47. http://dx.doi.org/10.1002/clc.22204
22. Kneeland PP, Fang MC. Current issues in patient adherence and persistence: focus on anticoagulants for the treatment and prevention of thromboembolism. Patient Prefer Adherence 2010;4:51–60.
30. Holford NH. Clinical pharmacokinetics and pharmacodynamics of warfarin. Understanding the dose-effect relationship. Clin Pharmacokinet 1986;11:483–504. http://dx.doi.org/10.2165/00003088-198611060-00005
31. Connolly SJ, Ezekowitz MD, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–51. http://dx.doi.org/10.1056/NEJMoa0905561
32. Nagarakanti R, Ezekowitz MD, Oldgren J et al. Dabigatran versus warfarin in patients with atrial fibrillation: an analysis of patients undergoing cardioversion. Circulation 2011;123:131–6. http://dx.doi.org/10.1161/CIRCULATIONAHA.110.977546
33. Patel MR, Hellkamp AS, Lokhnygina Y et al. Outcomes of discontinuing rivaroxaban compared with warfarin in patients with nonvalvular atrial fibrillation: analysis from the ROCKET AF trial (Rivaroxaban Once-Daily, Oral, Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation). Am Coll Cardiol 2013;61:651–8. http://dx.doi.org/10.1016/j.jacc.2012.09.057
34. Piccini JP, Stevens SR, Lokhnygina Y et al. Outcomes after cardioversion and atrial fibrillation ablation in patients treated with rivaroxaban and warfarin in the ROCKET AF trial. J Am Coll Cardiol 2013;61:1998–2006. http://dx.doi.org/10.1016/j.jacc.2013.02.025
35. Flaker G, Lopes RD, Al-Khatib SM et al. Efficacy and safety of apixaban in patients after cardioversion for atrial fibrillation: insights from the ARISTOTLE Trial (Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation). J Am Coll Cardiol 2014;63:1082–7. http://dx.doi.org/10.1016/j.jacc.2013.09.062
36. Plitt A, Ezekowitz MD, De Caterina R, et al. on behalf of the ENGAGE AF-TIMI 48 Investigators. Cardioversion of atrial fibrillation in ENGAGE AF-TIMI 48. Clin Cardiol 2016;39:345–6. http://dx.doi.org/10.1002/clc.22537
37. Giugliano RP, Ruff CT, Braunwald E, et al. for the ENGAGE AF-TIMI 48 Investigators. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;369:2093–104. http://dx.doi.org/10.1056/NEJMoa1310907
38. Ezekowitz MD, Spahr J, Ghosh P, Corelli K. Stroke prevention in atrial fibrillation: established oral anticoagulants versus novel anticoagulants – translating clinical trial data into practice. J Interv Card Electrophysiol 2014;40:261–8. http://dx.doi.org/10.1007/s10840-014-9893-z
39. Cappato R, Ezekowitz MD, Klein AL et al. Rivaroxaban vs. vitamin K antagonists for cardioversion in atrial fibrillation. Eur Heart J 2014;35:3346–55. http://dx.doi.org/10.1093/eurheartj/ehu367
40. Panella M, Marchisio S, Di Stanislao F. Reducing clinical variations with clinical pathways: do pathways work? Int J Qual Health Care 2003;15:509–21. http://dx.doi.org/10.1093/intqhc/mzg057
42. Deuling JH, Vermeulen RP, Smit MD et al. Planning and monitoring of patients for electrical cardioversion for atrial fibrillation. Neth Heart J 2012;20:148–54. http://dx.doi.org/10.1007/s12471-011-0208-z
43. Arujuna A, Ooues G, Abbas A et al. Electrical cardioversion of atrial fibrillation with the novel oral anticoagulants: a single centre UK-based registry experience. Europace 2014;16(suppl 3):iii14. http://dx.doi.org/10.1093/europace/euu239.11
Disclaimer: Medinews Cardiology Limited advises healthcare professionals to consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews Cardiology Limited cannot accept responsibility for any errors in prescribing which may occur.
Watch our podcast from the recent European Society of Cardiology (ESC) Congress, which highlights some of the key studies presented there with an interpretation by experts who give us their practice messages.
For advances in atrial fibrillation, we talk to Professor John Camm (St George’s, University of London), who analyses new AF guidance and the registry ‘real world’ data emerging in this field.
Dr Jubin Joseph (St Thomas’ Hospital, London, and President of the British Junior Cardiologists’ Association) speaks about the implications of some of the coronary artery disease studies, and also the use of telemonitoring in heart failure.
Finally, Professor Patrick Moriarty (University of Kansas Medical Center, Kansas City, USA) discusses what effect the new PCSK9 inhibitors are likely to have on life for patients with familial hypercholestorolaemia.
Sponsorship Statement: The writing of this report was supported by Bayer through a hands-off grant. The company had no input into its content
First published online October 27th 2016
With so much going on in the field of anticoagulation, our round-up of news in this area from the European Society of Cardiology (ESC) Congress, which took place in Rome, Italy, from 27th–31st August 2016, will ensure you keep up-to-date.
New AF guidelines
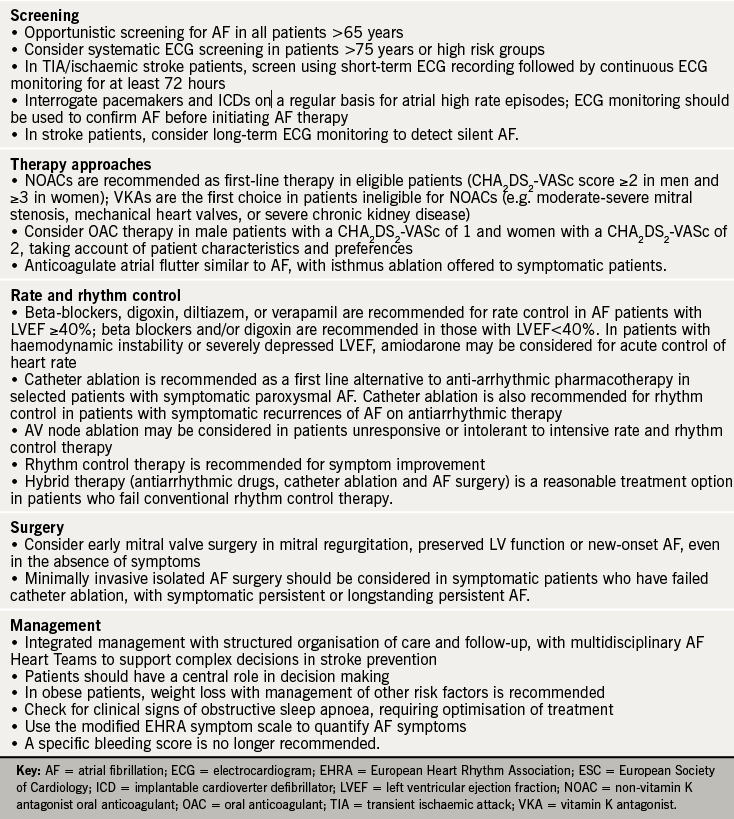
The first collaborative European Society of Cardiology (ESC) and European Association for Cardio-Thoracic Surgery (EACTS) Guidelines on Atrial Fibrillation (AF) were published at the start of the congress.1 These multidisciplinary guidelines focus on early detection of asymptomatic AF, recommending both opportunistic and targeted screening for all patients aged ≥65 years, or with stroke or transient ischaemic attack (TIA).
In addition, the guidelines deal with long-term challenges in the management of AF patients, with recommendations on what to do when patients develop complications on anticoagulation, re-initiation of anticoagulation after a bleed, how to manage bleeds, and how to manage patients who have an ischaemic stroke on anticoagulation.
Key new recommendations are summarised in table 1. Free smartphone tools are provided for patients with AF and their healthcare professionals via the ESC Pocket Guidelines App.
Table 1. What’s new in the ESC-EACTS guidelines on AF?
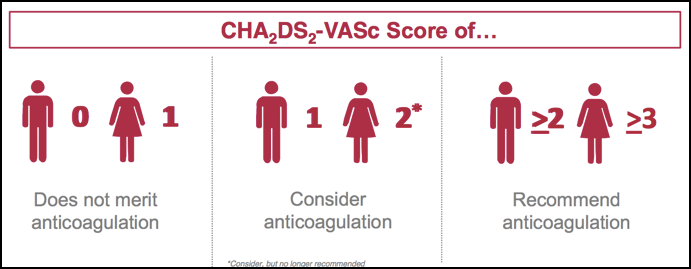
Professor John Camm (St George’s, University of London) speaks about the changes in the guidance in our podcast. The guidance, he says, has shifted in favour of real world data that has questioned the need for anticoagulant treatment in low-risk patients. This has led to patients often being unnecessarily anticoagulated, particularly women with a CHA2DS2-VASc score of 2, who are no longer recommended for anticoagulation (see figure 1).
Inappropriate anticoagulation shown by registry data
Analyses of registry data have shown that there is still much room for improvement in the use of anticoagulants in routine clinical practice.
Analyses from the ongoing GARFIELD-AF (Global Anticoagulant Registry in the Field – Atrial Fibrillation) Registry* have shown that while anticoagulation usage has risen in patients with AF, many patients are now being given inappropriate anticoagulation.
Figure 1. Changes to the CHA2DS2-VASc Scores in the new ESC/ESCTS 2016 guidelines for the management of AF
The Registry has shown that – contrary to international guidelines – 28% of high-risk patients (i.e. those with a CHA2DS2-VASc ≥2) are not receiving anticoagulation while 51% of very low-risk patients (i.e those with a CHA2DS2-VASc score of 0) are receiving anticoagulation.
It has also been revealed that unexpectedly high proportions of patients tend to be prescribed the lower dose of NOACs. Phase 3 studies suggest that the proportion of patients prescribed low-dose NOACs is 49.7% for dabigatran 110 mg BID, 20.7 % for rivaroxaban 15 mg OD and 4.7% for apixaban 2.5 mg BID; real world data has shown that the proportions of patients prescribed low-dose NOACs is much higher – 53.7%, 24.5% and 35.5% for dabigatran, rivaroxaban and apixaban, respectively. Professor Camm talks about inappropriate anticoagulation in our podcast.
New GARFIELD tool developed to assess risk more accurately
“Factors beyond those in current risk scores appear to be influencing prescribing decisions on anticoagulation and improved risk stratification tools are needed to better identify truly low-risk AF patients,” said Professor Keith A A Fox (Duke of Edinburgh Professor of Cardiology, University of Edinburgh) at an industry press conference during the ESC.
The GARFIELD-AF Score was developed using a machine-learning risk modeling approached based on analyses of data from 38,984 patients, enrolled in GARFIELD-AF between March 2010 and July 2015.2 A simplified model was also developed to facilitate web development.
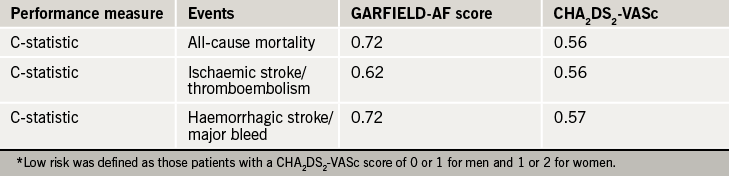
The performance of both models was compared with the CHA2DS2-VASc system in all patients and validated using an independent contemporary registry ORBIT AF. Compared to CHA2DS2-VASc, the performance of the GARFIELD-AF Score offered superior discriminatory value in predicting all-cause mortality, ischaemic stroke/systemic embolism, or haemorrhagic stroke/major bleed in low-risk patients (see table 2), and in predicting ischaemic stroke or major bleed in all patients.
Table 2. Performance of the GARFIELD-AF Score and CHA2DS2-VASc systems in low-risk patients*
It is hoped the new GARFIELD-AF score will help doctors better assess the appropriateness of anticoagulation in low-risk patients. “The more comprehensive GARFIELD-AF Score includes multiple variables, beyond that of CHA2DS2-VASc, and this increased granularity will help to optimise the management of low-risk patients,” said Professor Fox.
He also highlighted how a simplified version of the new scoring system has the potential to be incorporated into routine patient electronic record systems via web-based or mobile device applications, “enabling users to base treatment decisions on more precise and tailored values, as well as more complete estimates of risk based on multiple outcomes,” he added.
Further risk factors, such as biomarkers, diabetes and heart failure, could also potentially be added into the new GARFIELD-AF tool in the future.
Professor John Camm (St George’s, University of London) talks about changes to the guidance and the new risk tool in our podcast
As data from GARFIELD-AF registry grows, the GARFIELD risk score generated will become more and more accurate. If you want to find out more about the novel machine learning technique used and more about the GARFIELD-AF score, then watch our podcast from ESC.
*GARFIELD-AF has now recruited over 57,000 patients (over five cohorts) with AF in more than 1,000 sites in 35 countries, who will be followed-up for a minimum of two years and up to eight years after diagnosis. The GARFIELD-AF Registry is led by an international steering committee led by the Thrombois Research Insitutite, London, and is funded by an unrestricted research grant from Bayer Pharma AG.
Data from other risk scoring systems were also presented during the meeting, including the ENGAGE-AF TIMI score which is addressing how to identify those patients with AF who are likely to have adverse effects with warfarin and thus likely to benefit from NOAC therapy.
Anticoagulation Hotline studies
Great anticipation surrounds studies presented at the Hotline sessions during the congress. This year there was much excitement about the ENSURE-AF and ANNEXA-4 studies chosen for presentation at the Hotline Preventive Strategies 2 session.
ENSURE-AF
The non-vitamin K antagonist oral anticoagulant (NOAC) edoxaban was an effective and safe alternative to enoxaparin/warfarin in non-valvular AF (NVAF) patients undergoing cardioversion, offering hope for simplifying the therapeutic approach to anticoagulation in this setting.3
ENSURE-AF (Edoxaban versus Enoxaparin/Warfarin in Subjects Undergoing Cardioversion of Atrial Fibrillation) included 2,199 patients with documented NVAF, who were randomly allocated to an open-label anticoagulation strategy, either edoxaban 60 mg/day (n=1,095) or warfarin with enoxaparin bridging (n=1,104), using early or delayed cardioversion. The edoxaban dose was reduced to 30 mg/day if patients had creatinine clearance 15-50 mL/min, low bodyweight (≤60 kg), and/or concomitant use of P‑glycoprotein inhibitors. There were no differences between the two treatment groups; mean age was 64.3 years, 66% male, mean CHA2DS2-VASc score was 2.6, and 72% had previously received anticoagulation.
The primary end point was a composite of stroke, systemic embolism, myocardial infarction, and cardiovascular mortality, analysed by intention to treat. The primary safety end point was major and clinically relevant non-major bleeding in patients who received at least one dose of study drug. Patients were followed up for 28 days on study drug after cardioversion, as well as a further 30 days.
Edoxaban treatment was associated with significant reduction in the primary end point, both for the intention-to-treat population (from 1.0% to 0.5%, odds ratio [OR] 0.46, 95% 0.12-1.43), as well as the group undergoing transoesophageal echocardiography, about half of the study group (from 0.8% to 0.3%, OR 0.40, 95% CI 0.04-2.47). The treatment effect was independent of anticoagulation status or any other factor.
There was no difference between the two groups with respect to the primary safety outcome (16 events with edoxaban versus 11 with warfarin/enoxaparin), major bleeding (3 versus 5), clinically relevant non-major bleeding (14 versus 7), or any bleeding (32 versus 35). There was also a trend (although not statistically significant) towards a better net clinical outcome in patients in the edoxaban group versus those allocated warfarin/enoxaparin (OR 0.50, 95% CI 0.19–1.25).
While the results were clearly favourable, the lead author Professor Andreas Goette (St Vincenz-Hospital, Paderborn, Germany) did acknowledge that the trial was not powered to demonstrate differences in efficacy and safety end points, as well as the wide confidence intervals for the end points. Despite these limitations, the trial findings suggest that it is probably safe to maintain patients on edoxaban if they are already on this therapy, and longer-term, the possibility of moving over to NOAC therapy in this challenging clinical setting.
ANNEXA 4: reversal agent shows efficacy in acute bleeding
Preliminary results in the ongoing ANNEXA-4 study4 have shown that andexanet can rapidly reverse anti-factor Xa activity in acutely bleeding patients and is associated with excellent or good haemostasis in most.
ANNEXA-4 (Andexanat Alfa, a Novel Antidote to the Anticoagulation Effects of FXA inhibitors) is the first study to look at andexanet in acutely bleeding patients. The study was not randomised for ethical reasons and interim results in 67 patients, who required urgent reversal of acute major bleeding within 18 hours of receiving either a direct or indirect factor Xa inhibitor, looks promising.
Real world data for OAC therapy
There was much interest in real world data for oral anticoagulation at the meeting with analyses helping support the management of patients in routine clinical practice. Here, we report a selection of the data addressing some key issues.
Efficacy
REVISIT-US (Realworld Evidence on Stroke prevention in patients with Atrial Fibrillation in the United States)5 was a retrospective analysis of the US MarketScan administrative claims database (January 2013–October 2014) of NVAF patients newly initiated on the NOACs dabigatran (n = 15,679, 10.3% on 75 mg twice daily [BID]), rivaroxaban (n=11,411, 17.3% on 15 mg once daily [OD]), apixaban (n=4,083, 15.5% on 2.5 mg BID), or the VKA warfarin. Patients in each group were propensity-score matched with warfarin users (mean age 70.7 years, 54% male, CHA2DS2-VASC score 3.46–3.48 across the groups).
All three NOACs were associated with reduction in the primary composite end point of ischaemic stroke/intracranial haemorrhage (ICH) versus warfarin (significant for rivaroxaban, hazard ratio [HR] 0.61, 0.45–0.82, but non-significant for apixaban (HR 0.63, 0.35–1.12) and dabigatran (0.79, 0.62–1.02). Rivaroxaban and apixaban were also associated with significantly lower rates of ICH versus warfarin (by 47% and 62%), although the reduction with dabigatran (by 29%) was not significant.
Added to this, retrospective analysis in the German outpatient setting using data from the Primary Care Physician panel (January 2013–March 2015) in 1,670 AF patients newly initiated on apixaban or VKA (propensity-score matched) showed no difference in the primary end point (ischaemic stroke, TIA, MI, ICH, or other nontraumatic intracranial haemorrhage) between the groups (HR 0.77, 95% CI 0.43-1.40).6
Bleeding risk
While the use of NOACs has been associated with significant reductions in haemorrhagic stroke, all-cause mortality and intracranial haemorrhage, one of the key concerns for the use of NOACs in the real world is the risk of bleeding complications. This was covered in a number of presentations at the 2016 congress. Most of the data related to retrospective analyses of large healthcare databases, with additional insights from nationwide studies and registries.
Retrospective cohort data from the MarketScan and Medicare databases of NVAF patients newly prescribed NOACs showed a significantly lower risk of major bleeding with apixaban or rivaroxaban compared with warfarin.7 The analysis included data for 45,361 eligible patients: 15,461 (34%) initiated on warfarin, 7,436 (16%) on apixaban, 4,661 (10%) on dabigatran and 17,801 (39%) on rivaroxaban. Propensity score matching was used to balance patient baseline characteristics, co-morbidities, and co-medications.
There were:
6,964 warfarin-apixaban patients (mean follow-up 148.1 and 161.1 days)
4,515 warfarin-dabigatran patients (mean follow-up 178.1 and 160.5 days)
12,625 warfarin-rivaroxaban patients (mean follow-up 177.9 and 162.7 days).
The incidence of major bleeding (per 100 person-years) was:
38 (apixaban) versus 4.48 for the apixaban-warfarin matched cohort
23 (dabigatran) versus 4.80 for the dabigatran-warfarin matched cohort
92 (rivaroxaban) versus 5.09 for the rivaroxaban-warfarin matched cohort.
Compared with warfarin, there was a significantly lower risk of major bleeding for patients starting on apixaban (by 47%) or dabigatran (by 41%) but not for rivaroxaban. For elderly patients (≥75 years), only those initiating apixaban had a significantly lower risk of major bleeding (by 38%) compared with warfarin; there was no difference between warfarin and dabigatran or rivaroxaban.8
Professor Greg Lip (University of Bimingham, UK) also presented data from the US Humedica electronic health records (January 2013–March 2015) in NVAF patients initiating warfarin (n=47,215), apixaban 5 mg BID (n=5,003), dabigatran 150 mg BID (n=3,886), or rivaroxaban 20 mg OD (n=7,326).9
Patients were followed up until the earliest of OAC switch, bleeding event, last encounter or 180 days after first initiation of therapy. Bleeding was defined as any bleeding event during follow-up. The patient groups were comparable with mean age 67–74 years, >50% male and a mean CHADS2 score of 1.3–1.7.
Compared with warfarin, there was significant (p<0.0001) reduction in bleeding risk with either apixaban (adjusted HR 0.811, 0.732–0.899) or dabigatran (HR 0.698, 0.621–0.785), although bleeding risk did not differ for rivaroxaban (HR 0.985, 0.911–1.066). Similar results were reported in elderly patients.
Added to this, a Swedish post-authorisation study in a random sample of AF patients (761 of 78,022 treated in Stockholm county) showed no differences in the risk of major bleeding between rivaroxaban and warfarin.10 The data were analysed using both intention-to-treat (based on first prescribed drug) and on-treatment (drug on ≥80% of days) approaches. Major bleeding (i.e. fatal or requiring hospitalisation) was comparable for the two treatments in each analysis, despite the rivaroxaban group being on average older (mean age 75.1 versus 73.9 years), and at higher risk (mean CHA2DS2-VASc 3.35 versus 3.26). However, the risk of intracranial haemorrhage was significantly lower with rivaroxaban than warfarin (HR 0.63, 0.40–0.99).
Finally, there was evidence from a nationwide Finnish study that bleeding complications are uncommon (<1%) in AF patients undergoing elective cardioversion (October 2011– December 2015).11 In total, 732 patients (mean age 63 years, 73% men, mean CHA2DS2– VASc score 1.8) underwent 893 procedures using dabigatran (57.9%), rivaroxaban (31.1%) or apixaban (11.0%).
During the month follow-up period, the AF recurrence rate was 28.4%. There were two strokes, although each patient was receiving adequate NOAC therapy in the four weeks preceding the intervention, and four clinically relevant bleeding events in two patients each on dabigatran or rivaroxaban.
Persistence, adherence and crossover between OACs
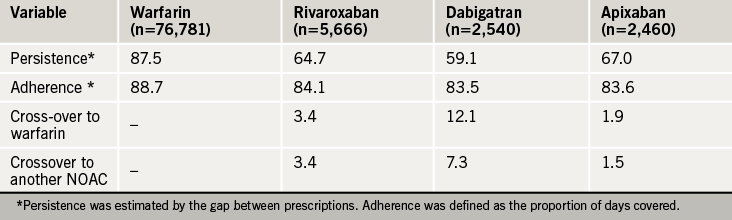
Dr Amitava Banerjee (UCL Hospital and Barts Health) evaluated UK real world persistence, adherence and cross-over across the OACS using prescription data (April 2011–December 2015) from The Health Improvement Network for NVAF patients newly initiated on warfarin, rivaroxaban, dabigatran and apixaban.12 Edoxaban was not included as it was only approved in the UK in September 2015.
The patient groups were comparable (mean age 75 years, 44% female, median CHA2DS2-VASc score 3.0). Persistence with NOACs at one year was less than that observed during a trial (76.3% with rivaroxaban, 78.8-79.3% with dabigatran, 74.7% with apixaban) highlighting the need for further evaluation of the tolerability and acceptability profiles of the NOACs (table 3).
Table 3. One-year persistence, adherence and cross-over (%) between OACs
Geographical variability
Marked geographical variations in outcomes have been shown in patients with newly diagnosed AF. Analyses of GARFIELD-AF registry data have shown that event rates persisted after adjustment for CHA2DS2-VASc risk factors and other key variables, including ethnicity, smoking, type of AF, and moderate-to-severe chronic kidney disease.
Lower mortality was seen in Eastern Asia (Japan and South Korea) and higher mortality was seen in countries such as India and South Africa.13 Wide variations in baseline characteristics were also shown between regions and countries with:
Wide variability in the reporting of vascular disease
Patients in North America were less likely to have a history of congestive heart failure than patients in Europe, Asia and Latin America.
Patients from Asia with newly diagnosed AF were less likely to have a history of coronary artery disease or a history of bleeding relative to patients in Europe and North America.
More data from a prospective analysis of patients with newly diagnosed AF in Asia treated with VKA therapy suggests that the lowest rates of stroke/systemic embolism and major bleeding occur at the INR level of 1.6–2.0.14 This does not contradict the regional practice of a lower INR than in non-Asian countries.
Currently international guidelines for AF differ in their recommended target INR range: European and American guidelines recommend a target INR of 2.0–3.0, while the Asia Pacific Heart Rhythm Society and Japanese Circulation Society recommend an INR of 2.0–3.0, with a target of 1.6 – 2.6 for those aged 70 years and over.
More data are required now to determine whether there are significant differences in outcomes among Asian and non-Asian populations.
Management: first four months after diagnosis most risky
The first four months after a new diagnosis of atrial fibrillation (AF) have been seen to be the riskiest out of two years of follow-up following analysis of data from the GARFIELD-AF Registry.
During this period, there was 29% greater risk in all-cause death, 35% more risk of stroke and 56% more risk of bleeding. Those patients with prior myocardial infarction, unstable angina, moderate-to-severe chronic kidney disease and prior stroke, are the most at risk.15
“These data indicate the importance of comobidities in predicting the risk of early mortality in patients with AF,” said Professor Samuel Goldhaber (Harvard Medical School and Brigham and Women’s Hospital, Boston, USA).
This driving of mortality from earlier comorbidities highlights how a comprehensive approach to management must be adopted when treating AF. Patients should be given individualised care and put at the centre of the management planning.
Patients in the real word range from the elderly, those with comorbidities such as the renally impaired, those with diabetes and acute coronary syndromes (ACS). Many patients are on polypharmacy. “Accumulating real-world evidence from a broad range of sources provides reassurance of phase 3 results and confidence in managing subgroups where data are more limited,” said Dr Walid Amara (Le Reincy, Montfermeil, France).16
Studies are currently ongoing in various special groups of patients including a new study GALILEO, which is looking at the use of rivaroxaban-based antithrombotic strategy compared to an antiplatelet-based strategy after successful transcatheter aortic valve replacement to find out whether one is superior in reducing death or first thromboembolic events.
Results from the X-TRA study using the CLOT-AF registry support the use of rivaroxaban as an alternative to the current standard of care for left atrial/left atrial appendage (LA/LAA) thrombus in NVAF/flutter.17
This prospective, single-arm, multicentre study included 60 patients (median CHADS2 and CHA2DS2-VASc score ≥2), mostly with persistent, persistent longstanding or permanent AF, and no prior VKA or NOAC therapy. Overall, 81.7% were on rivaroxaban 20 mg OD (18.3% on 15 mg OD) for a mean of 46 days. In the modified ITT population (n=53), 42% had adjudicated complete thrombus resolution, and 60% resolved or reduced thrombus. These results suggest that rivaroxaban could be a potential option for the treatment of LA/LAA thrombi.
References
1. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016. http://dx.doi.org/10.1093/eurheartj/ehw210
2. Fox KAA. Identifying patients with atrial fibrillation and “truly low” thromboembolic risk who are poorly characterized by CHA2DS2-VASc: Superior performance of a novel machine learning tool in GARFIELD-AF. Abstract 2950. Eur Heart J 2016;37:(Abstract Supplement), xi-xviii. http://dx.doi.org/10.1093/eurheartj/ehw430
3. Goette A, Merino JL, Ezekowitz MD, et al. Edoxaban versus enoxaparin-warfarin in patients undergoing cardioversion of atrial fibrillation (ENSURE-AF): a randomised, open-label, phase 3b trial. Lancet 2016;pii. http://dx.doi.org/10.1016/S0140-6736(16)31474-X
4. Connolly SJ et al. Andexanet alfa in factor Xa inhibitor-associated acute major bleeding. Presentation at European Society of Cardiology Congress (Hotline Preventive Strategies 2). Tuesday, 30th August 2016.
5. Coleman C, Antz M, Simard E et al. Real world evidence of stroke prevention in patients with nonvalvular atrial fibrillation in the United States: the REVISITUS study. Abstract: P2576. Eur Heart J 2016;37(Abstract Supplement):504.
6. Coleman C, Antz M. Real world evidence of stroke prevention in patients with nonvalvular atrial fibrillation. Abstract P2570. Eur Heart J 2016;37(Abstract Supplement):502.
7. Lip GYH, Keshishian A, Kamble S, et al. Is major bleeding risk for oral anticoagulants similar between nonvalvular atrial fibrillation patients newly initiated on warfarin and propensity score matched NOAC initiators? A real world study. Abstract: P2543. Eur Heart J 2016;37(Abstract Supplement):493.
8. Lip GYH, Keshishian A, Kamble S, et al. Major bleeding risk in patients 75 years of age or older with nonvalvular atrial fibrillation initiating oral anticoagulants: a real world comparison of warfarin, apixaban, dabigatran, or rivaroxaban. Abstract: P2567. Eur Heart J 2016;37(Abstract Supplement):500–1. http://dx.doi.org/10.1160/TH16-05-0403
9. Lin I, Masseria C, Mardekian J, et al. Bleeding risk for nonvalvular AF patients prescribed warfarin, or standard doses of apixaban 5mg BID, dabigatran 150mg BID or rivaroxaban 20mg QD in real world practice: Findings from HER. Abstract: 2065. Eur Heart J 2016;37(Abstract Supplement):402.
10. Friberg L. Major bleeding among patients with atrial fibrillation treated with rivaroxaban or warfarin in Sweden. Interim results from an ongoing post-authorization study. Abstract: 2067. Eur Heart J 2016;37(Abstract Supplement): 402–403.
11. Itainen S, Lehto M, Vasankari T, et al. Direct oral anticoagulants in atrial fibrillation patients undergoing cardioversion. Nationwide multicentre study. Abstract: 1355. Eur Heart J 2016;37(Abstract Supplement):235.
12. Banerjee A, Burnell J, Ryan R, et al. Real world persistence, adherence and switchover across anticoagulants in atrial fibrillation a national population based study. Abstract: 1351. Eur Heart J 2016;37(Abstract Supplement): 233.
13. Fox KAA, et al. Do baseline characteristics account for geographical variations in event rates in patients with newly diagnosed atrial fibrillation? The GARFIELD-AF registry. Abstract P4100. Eur Heart J 2016;37(Abstract supplement):801.
14. Goto S, et al. Vitamin K antagonist control for patients with nonvalvular atrial fibrillation in Eastern and South Eastern Asia: an analysis of event rates from GARFIELD-AF. Abstract P4971. Eur Heart J 2016;37(Abstract supplement):1007–8.
15. Goldhaber SZ. Presentation at Satellite Symposium ‘Practical dimensions of novel anticoagulant-based prevention of stroke in atrial fibrillation and management of acute venous thromembolism’. European Society of Cardiology, 29th August 2016, Rome, Italy.
16. Amara W. Presentation at Satellite Symposium ‘Practical management of patients with atrial fibrillation – individualized approaches to stroke prevention’. European Society of Cardiology, 30th August 2016, Rome, Italy.
17. Lip GYH, Hammerstingl C, Marin F, et al. Left atrial thrombus resolution in atrial fibrillation or flutter: results of a prospective study with rivaroxaban (XTRA) and a retrospective observational registry providing baseline data (CLOT AF). Abstract: P2569. Eur Heart J 2016;37(Abstract Supplement):501.
Sponsorship Statement: Actelion have funded the production of this article but have had no input into its content.
First published online October 26th 2016
We round up the latest news in pulmonary hypertension (PH) from recent congresses. Dr Logan Thirugnanasothy (Clinical Research Fellow, Newcastle Pulmonary Hypertension Service, Freeman Hospital, Newcastle) reports from the European Respiratory Society (ERS) Congress, held in London from 3rd– 7th September 2016 while we report PH highlights from the recent European Society of Cardiology (ESC) Congress, held in Rome, Italy, from 28th – 31st August 2016.
PH update from ERS
The 2015 ESC/ERS guidelines for the diagnosis and treatment of PH
Updated collaborative guidelines from the ERS and ESC on the diagnosis and management of pulmonary hypertension (PH) were presented at the ERS by Professor Marc Humbert (chairperson of the ERS taskforce). PH diseases continue to be classified into one of five groups and its haemodynamic definition remains unchanged, with a mean pulmonary artery pressure ≥ 25 mmHg at right heart catheterisation.
Right heart catheterisation
There is a high prevalence of left heart disease in the PH population. As the pulmonary arterial wedge pressure (PAWP) may be normal in patients on diuretics, the guidelines remind clinicians of the utility of other haemodynamic measurements. Both pulmonary vascular resistance (PVR) and the diastolic pulmonary gradient (DPG) can be helpful in determining whether there is a co-existing element of pre-capillary PH. The DPG, defined as diastolic pulmonary artery pressure minus PAWP, can help clarify the subtype of PH in left heart disease. A DPG ≥7, with or without a PVR ≥3 wood units, suggests the presence of pre-capillary PH.
In relation to diagnostic right heart catheterisation, the guidelines continue to advocate the use of acute vasodilator response testing, which can identify those patients with pulmonary arterial hypertension (PAH), who may respond well to calcium channel blocker therapy as a first-line treatment.
Treatment of PAH
There are now several types of specific pulmonary vasodilator drugs available for the treatment of PAH and either a single or combination of drugs can be commenced at diagnosis. The guidelines describe a simple traffic light risk assessment model, which can guide escalating pulmonary vasodilator therapy at further patient reviews. The model stratifies patients in to low, intermediate and high-risk groups, based on the estimated one-year mortality, and it details certain treatment goals for patients. Other treatment considerations include warfarin as the only recommended anticoagulant in PAH due to the lack of any evidence on the newer, non-vitamin K anatagonist oral anticoagulants (NOACs). Beta blockers should also be avoided in the treatment of PAH.
New treatments and devices in pulmonary hypertension
Selexipag
The GRIPHON (Prostacyclin [PGI2 ] receptor agonist in pulmonary arterial hypertension) study was further analysed at the congress. GRIPHON has established that selexipag, an oral, selective prostacyclin receptor agonist, can reduce the risk of a primary composite end point of death or complication from PAH compared to placebo in PAH patients.
Currently prostacyclin therapy is given parenterally and there is a risk of rebound PH if there is a treatment interruption. Dr Iona Preston (Tufts University School of Medicine, Boston, USA) discussed further analysis of the GRIPHON data to provide insight on the effects of treatment interruption with selexipag.
A treatment interruption for three or more days required repeat titration from the starting dose (200 μg), which affected 7% (34/509) patients in the selexipag arm. The median duration of the treatment interruption was 10.5 days and three patients experienced one or more adverse events, that were independently adjudicated to be unrelated to PAH. After repeat titration, 68% (23/34) of patients attained a dose similar to that prior to treatment interruption, with subsequent median treatment duration of 35 weeks. Thus selexipag treatment interruptions were generally well tolerated in the GRIPHON study.
Implantable prostaglandin devices
Current standard administration of parenteral prostacyclin therapy is either intravenously or subcutaneously and such access can be complicated by local side effects or even systemic infections. Professor Ardershir Ghofrani’s group (University Hospital, Giessen, Germany) presented their experience of 51 patients who received a new, fully implantable pump for delivery of intravenous treprostinil. Devices were implanted either under local or general anaesthetic and there were no major intraoperative complications of pump implantation. Two patients required treatment in intensive care for acute right ventricular and respiratory failure. Two further patients died of progressive right heart failure not relating to pump implantation. Further trials are required to establish the long-term efficacy and safety of this treatment modality.
Novel assessment tools in clinical practice
The PAH-SYMPACT (Pulmonary arterial hypertension-symptoms and impact) questionnaire is a patient-reported outcome (PRO) instrument consisting of both symptom and impact items based on interviews of patients with PAH. Dr Kelly Chin (University of Texas Southwestern Medical Center, Dallas, USA) presented the evaluation of PAH-SYMPACT using data from a phase IIIb PAH study with macitentan (SYMPHONY). Data from 278 patients were included and the finalised PRO instrument consisted of 11 symptom and 11 impact items. Adherence in completing the questionnaire was 83% so PAH-SYMPACT could potentially be a useful clinical and research tool in PAH.
Digital feedback to guide therapy in pulmonary hypertension
Professor Paul Corris (Freeman Hospital, Newcastle upon Tyne) presented the results of a pilot study, which looked at using a digital system to measure adherence and activity (in steps) in order to support self-management and optimise therapy in PH. Proteus Discover, a digital feedback system, consists of sensor-enabled medicines, a wearable sensor and a patient app. The study included 21 patients who were prescribed sildenafil over 12 weeks. Results showed the mean adherence was 94% and the daily step count was 1,890. When the previous day’s adherence was low (0-25%), there was a reduction in 381 steps the following day, compared to patients with a high adherence (>75%). The digital system confirmed high adherence in seven patients whose clinical state declined and therefore required escalation of treatment.
Updates in thromboembolic disease and pulmonary hypertension
A review of key publications on thromboembolic disease and PH over the past year was given by Professor Marius Hoeper (Hannover Medical School, Hannover, Germany).
One study he reviewed, carried out by Becattini et al., investigated the ESC 2014 pulmonary embolism (PE) guideline risk assessment to predict mortality at 30 days in 960 consecutive patients presenting with acute confirmed PE. The mortality rate was 22% in high-risk and 0.5% in low-risk patients. The mortality rate in the intermediate-high and intermediate-low risk groups were 7.7% and 6%, respectively, highlighting a need for improvement for risk stratification in this group.
He also discussed the PADIS-PE (Six Months vs Extended Oral Anticoagulation After a First Episode of Pulmonary Embolism) study. The optimum duration of anticoagulation after a first, unprovoked PE is uncertain and the PADIS-PE study looked at patients who had received six months of warfarin therapy after an acute unprovoked PE. Patients were randomised to either a further 18 months of treatment or to placebo. Results showed that those receiving an extension of warfarin treatment had a reduced composite outcome of recurrent embolism and major bleeding compared to placebo, but the benefit was lost after eventually discontinuing anticoagulation. Professor Hoeper commented that he expects there will now be a shift towards indefinite anticoagulation after an unprovoked, acute PE.
Pulmonary endarterectomy (PEA) is the treatment of choice in chronic thromboembolic pulmonary hypertension (CTEPH) as it has the potential to cure the disease. Data on the long-term outcomes following PEA have been published, for the first time, by Dr John Cannon and colleagues from Papworth Hospital, Cambridge. They analysed 880 consecutive patients undergoing PEA for CTEPH and found that haemodynamics on the first day after surgery were not predictive of long-term outcome whereas haemodynamics measured at three, six and 12 months all enabled risk stratification in terms of recurrent PH and survival. Most patients with residual PH following PEA do not require any treatment given its mild severity, although some patients will eventually need medical therapy.
PH update from ESC
Women with PH have a high risk of morbidity and mortality during pregnancy and in 2007 the ESC initiated the European Registry on Pregnancy and Heart Disease (ROPAC). This on-going worldwide registry enrols consecutive patients with all forms of cardiovascular disease, presenting with pregnancy, with the aim of investigating pregnancy outcomes.
Data were presented from this registry by Dr Iris van Hagen (Erasmus University Medical Centre, Rotterdam, The Netherlands) from a cohort of 151 women with PH. Some 26% had PAH in three different subgroups: idiopathic (iPAH); associated with congenital heart disease (CHDPAH); or associated with other disease (oPAH). The remaining 74% (n=112) had PH due to left heart disease (LHDPH). Maternal mean age was 29.2 ± 5.6years and 37% were nulliparous.
The degree of PH was classed as mild (i.e. right ventricular systolic pressure [RVSP] <50mmHg) in 59.6% of patients, moderate (RVSP 50–70 mmHg) in 28.5% and severe (>70mmHg) in 11.9% of patients. In more than 75% of patients, the diagnosis of PH had been made prior to pregnancy.
Maternal mortality and morbidity
Maternal death up to one week after delivery occurred in five patients (3.3%). Another two out of 78 patients with follow up available (2.6%) died within six months of delivery. Highest mortality was found in iPAH. Heart failure during pregnancy occurred in 27%. Caesarean section was performed in 63.4% (23.9% as emergency). Therapeutic abortion was performed in 4.0%.
Offspring complications included miscarriage (5.6%), fetal mortality (2%), premature delivery (21.7%), low birth weight (19.0%) and neonatal mortality (0.7%).
Only 4% of the patients received a calcium channel blocker and 5.9% advanced PAH therapy during pregnancy.
As specialised care during pregnancy and delivery was available, however, the mortality reported in these patients with various sub-classifications of PH was lower than previously reported. But Dr van Hagen stressed that we should carefully distinguish between, mild, moderate and severe PH and carefully investigate the reasons for increased pressures since maternal and fetal mortality remains prohibitively high in women with iPAH.
She concluded by saying that early advice on contraception, pregnancy risk and fetal outcome remains paramount in this patient population and it should be delivered by “a dedicated specialist team with expertise in pulmonary hypertension“.
PH patients with congenital heart disease
PAH associated with congenital heart disease is increasingly common. Many patients still have a poor prognosis following a correction to their structural heart defect. Data from randomised controlled studies in this patient population are limited. The global phase III GRIPHON study enrolled 1,156 PAH patients and the overall population included 110 patients with congenital cardiac shunts at least one year after correction.
Dr Maurice Beghett (University Hospital Geneva, Switzerland) presented analyses on the efficacy and safety of selexipag in PAH patients with repaired congenital cardiac shunts (PAHCHD). Of the 110 patients enrolled with PAHCHD (selexipag: n=60; placebo: n=50), 55 (50%) had corrected atrial septal defect, 38 (35%) had a corrected ventricular septal defect, 14 (13%) had corrected persistent ductus arteriosus and three patients did not have the type of defect specified. Mean age was 40.3 years, mean time from diagnosis was 3.6 years, 61% were in WHO functional class I/II and 68% were on background therapy at baseline.
Outcomes observed
By the end of treatment, 13 patients (26%) in the placebo group and nine patients (15%) in the selexipag group had a primary end point event. Selexipag reduced the risk of morbidity/mortality events by 42% versus placebo, which Dr Beghetti reported, is consistent with the overall treatment effect. By the end of the study, five patients in the placebo group and two patients in the selexipag group had died.
Common prostacyclin-associated side effects observed with selexipag in PAHCHD patients (e.g. headache, diarrhoea, jaw pain) generally occurred at a similar incidence to that seen in PAH patients without congenital heart disease. No serious adverse events were reported more frequently (i.e. >2% difference between selexipag and placebo) in the selexipag group compared to placebo.
Dr Beghetti concluded that the beneficial treatment effect of selexipag, as well as the safety and tolerability profile, in this analysis of congenital heart disease patients with persistent or recurrent PAH following defect correction, were consistent with that of the overall GRIPHON population.
Surgery superior to medical therapy in CTEPH…
Pulmonary endarterectomy (PEA) may be the treatment of choice for CTEPH but operability must be assessed by a multidisciplinary CTEPH team. Also, specific medical treatment (MT) should be offered to non-operable patients, according to Dr Maria Jesus Lopez Gude (University Hospital 12 de Octubre, Cardiac Surgery Department, Madrid, Spain).
Dr Lopez Gude and co-authors presented details of a study, which compared the survival of patients undergoing PEA versus MT in a cohort of patients attending a Spanish referral centre, where 205 consecutive patients were referred from 1999 to 2014: 100 and 105 patients received MT and PEA, respectively. All patients were followed up for one year and assessed. Significant differences between patients under MT and under PEA were found in the age at diagnosis (61 ± 15 years vs. 52 ± 14 years); patient gender (65% women vs. 44% men); and evidence of previous venous or pulmonary embolism (75% vs. 88%), and in the number of patients receiving baseline medical treatment (33% vs. 49%).
Analysis of survival (defined as event-free survival, no death or lung transplantation) data showed that PEA patients had a significantly better survival than MT patients: 72% versus 44%, respectively. This survival advantage occured even during the ‘learning curve’ phase of the technique highlighting the recommendation that PEA surgery should be the first treatment of choice for CTEPH patients, according to Dr Lopes Gude.
…and balloon angioplasty for inoperable patients?
Findings from another study at the same centre by Dr M Velazquez et al., showed that balloon pulmonary angioplasty (BPA) is effective and safe in chronic CTEPH non-operable patients.
Having performed 80 BPA sessions in 23 distal type CTEPH non-operable patients (3.5 sessions per patient), these workers suggest that BPA can be considered an effective therapeutic approach in this patient group. From their experience, it improves haemodynamics, functional capacity and biomarkers, and allows prostanoid discontinuation in some patients, but it is also associated with major, possibly fatal complications, including reperfusion pulmonary oedema (7.5%).
Dr Logan Thirugnanasothy
Clinical Research Fellow
Newcastle Pulmonary Hypertension Service, Freeman Hospital, Newcastle
Over and over we hear the message that healthcare spending is out of control, the National Health Service (NHS) needs to save £20 billion and that is before the baby boom* generation fully enters the most expensive part of their healthcare journey…
National Institute for Health and Care Excellence (NICE) guidance supports the introduction of sacubitril/valsartan under the supervision of a heart failure specialist with access to a multi-disciplinary heart failure team. Clinical information was obtained retrospectively on all patients with a primary coded diagnosis of heart failure discharged from the Conquest Hospital, Hastings, UK during the calendar year 2015. We recorded the proportion of patients meeting the NICE recommendation and those patients meeting the additional PARADIGM-HF (Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure) study inclusion criteria.
In a total of 205 assessable patients discharged with a primary diagnosis of heart failure during the calendar year 2015, inpatient mortality was 11%, with a crude readmission rate during the year of 17%. The number of patients meeting the NICE criteria was 26 (13%). In hierarchical analysis taking the major PARADIGM-HF inclusion criteria, 20 patients (10%) patients met the inclusion criteria.
In conclusion, the findings from this audit suggest that the number of patients potentially suitable for sacubitril/valsartan therapy is low. Given the PARADIGM-HF study run-in design, the optimal dose and stability of angiotensin-converting enzyme (ACE) inhibitor and angiotensin-receptor blocker medication may need to be clarified if sacubitril/valsartan is to be commenced during or shortly after hospitalisation.
The first-in-class drug sacubitril/valsartan (EntrestoTM) has been recommended for use in the UK by the National Institute for Health and Care Excellence (NICE) following evidence from the PARADIGM-HF (Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure) trial. To qualify, patients should have severe left ventricular dysfunction (ejection fraction ≤35%), New York Heart Association (NYHA) grade II–IV symptomatic heart failure, and be on a stable dose of angiotensin-converting enzyme inhibitor (ACEi) or angiotensin-receptor blocker (ARB). We evaluated all patients seen in our nurse-led heart failure clinics over a six-month period to assess suitability for sacubitril/valsartan and the resulting cost implication.
Of 553 patients seen, more than two thirds (69%) were unsuitable, of whom most had an ejection fraction greater than 35%. Other reasons included hypotension, NYHA class I, renal dysfunction, intolerance of ACEi/ARB and compliance concerns. There were 49 patients who died within nine months of the study period end. Of these, most (84%) were unsuitable for sacubitril/valsartan. Compared with current local use of ACEi and ARB, switching the 174 suitable patients to sacubitril/valsartan would cost £171,816 per year.
In our real-world experience, 31–37% of patients attending a specialist nurse-led heart failure clinic may be suitable for sacubitril/valsartan therapy. While the clinical benefits of this treatment are well proven and a recent NICE technology assessment has demonstrated cost-effectiveness, the medication has significant upfront cost implications for healthcare commissioners.
Drug-eluting stents (DES) have revolutionised the treatment of acute coronary syndrome, resulting in improvement in mortality and morbidity. However, there have been safety concerns, mainly involving a small, but long-term, risk of stent thrombosis (ST) and in-stent restenosis (ISR). Stent fracture (SF) is a lesser-known complication that can predispose to both ST and ISR and for which there is no general consensus for treatment. We present an interesting case and a new approach to treating this complex problem.
Case history
Figure 1. Intravascular ultrasound (IVUS) image showing gross malapposition between the original stent (black arrow) and the vessel wall (transparent arrow)
A 44-year-old smoker with a history of hypertension, high cholesterol and positive family history presented with inferior wall ST-elevation myocardial infarction (STEMI). Angiography revealed the culprit was an occluded right coronary artery (RCA). A drug-eluting stent (Taxus element) 2.75 by 24 mm was deployed and the patient discharged with follow-up on dual antiplatelet therapy (DAPT) (aspirin and clopidogrel).
Three years later he was re-admitted with another inferior STEMI. Angiography revealed occlusion of the previously stented segment. Aspiration thrombectomy followed by intravascular ultrasound imaging (as optical coherence tomography [OCT] was being serviced) clearly demonstrated gross mal-apposition of the stent: the RCA diameter was 4.5 mm and the stent 3 mm (figure 1). The stent was dilated with 4.5 mm balloon only, with a good result. The patient was discharged on aspirin and ticagrelor.
Figure 2. Optical coherence tomography (OCT) image of right coronary artery (RCA) during the third admission showing a well-endothelialised stent (black arrow)
He re-presented six months later with repeated inferior STEMI, but confirmed good DAPT compliance. Again, the culprit was the occluded RCA stent. OCT imaging revealed thrombosis at the site of restenosis within the stented segment and coincided with a total discontinuity of the stent (stent fracture with a gap), caused by previous over-sized balloon angioplasty (figures 2 and 3). This would be considered type V stent fracture (SF) in view of complete discontinuity with separation of stent segments, hence, more likely to be associated with adverse clinical outcomes (table 1).1
Management
The RCA had to be treated, so the question is how best to treat the fractured stent with protruding stent struts?
Our case was complex, as stenting in mal-apposed stent struts would result in a double layer of metal, leading to an increased risk of thrombogenicity and in-stent restenosis (ISR) long term. Coronary artery bypass grafting (CABG) could be considered, but would be the last treatment choice in the setting of single-vessel disease, and would not be appropriate in the acute setting. We chose to perform drug-coated balloon (DCB) angioplasty to reduce the potential risk of further stent thrombosis (ST) or ISR, although we accept there is little current evidence for its use in such cases.
Figure 3. OCT image showing complete discontinuity of stent struts suggestive of stent fracture
Following aspiration thrombectomy, and imaging and vessel measurement with OCT, a decision was made to treat the RCA with a DCB 3 by 26 mm, and a good result was obtained (figure 4). The patient made an uneventful recovery and was discharged on DAPT (aspirin and prasugrel in view of ST). Six months post-procedure, the patient was readmitted electively for repeat angiogram and OCT, which showed complete coverage of the stent struts with evidence of mild ISR only.
SF was first reported in 2002 after a bare metal stent (BMS) implantation in a venous bypass graft,2 and in DES two years later.3 The incidence of SF is reported to be between 1% and 8%,4 and the presentation may range from asymptomatic to angina, myocardial infarction and sudden death.
Table 1. Classification of stent fractures
SF have been defined and classified according to severity depending on the presence of isolated strut fractures (least severe), partial or complete stent fractures and fractures with separation of stent segments (being most severe), as was in our case. The severe ones have been associated with increased incidence of adverse clinical outcomes, i.e. ST and ISR.1
In addition, increased incidence of SF is also reported in vessels with excessive movement and hinge motion, which is assessed by the change in the angle at the fracture site (that is, the difference between end-systolic and end-diastolic angles in different views) using quantitative coronary angiography.5 Therefore, SF is more commonly seen in the RCA and saphenous vein grafts as their dynamic motion during the cardiac contractions exposes them to distortive forces.4
Figure 4. Angiogram showing the final result after treating vessel with a drugeluting balloon
A number of predicting factors have been described in the literature, including the type of stent, handling, technique, length, balloon over-expansion and the type of vessel being stented.4 Among the stents, Cypher sirolimus stents have frequently been associated with SF, possibly because of their rigid closed-cell structure and, secondly, because of their radio-opaque nature, hence, making them more visible.
An association with aneurysm formation has also been reported, presumably caused by arterial or intimal tears and inflammation caused by polymer. In addition, there are reports of increased ST and ISR related to interruption of drug delivery as a result of strut fracture, leading to neo-intimal overgrowth and stenosis.
As far as treatment options are concerned, there is no general consensus, making it a complex complication to treat. The management of SF depends on the type, presentation, symptoms and the presence of factors predicting recurrence (i.e. calcified lesions, tortuous vessel, technically difficult angioplasty). The treatment options vary from stenting, ballooning and, in some cases, CABG. Long-term DAPT has also been suggested.
In our case, the patient had multiple admissions, presenting first with inferior STEMI, followed by re-occlusion due to very late mal-apposition, most probably caused by a combination of positive remodelling of the vessel and under-sized stent, and, finally, a further re-occlusion due to SF caused by over expansion of the stent with a large balloon leading to ISR and ST. Successful treatment of SF in the context of ST with a DCB, to our knowledge, has not been reported before.
In conclusion, DES is the mainstay treatment of acute coronary syndrome. Despite the growing evidence base for acute coronary syndrome treatment, management of SF remains challenging and poorly researched. The concept of using DCB for treating SF is both novel and unique, and it comes with the advantage of a low-risk of thrombogenicity, shorter duration of DAPT and is also reported to be associated with positive remodelling of the vessel. With the help of this case report we present a new approach to treating the complex problem of stent fractures.
Conflict of interest
SCE has received an unrestricted research grant from, and consulted for, B. Braun. UR and TJG: none declared.
References
1. Nakazawa G, Finn AV, Vorphal M et al. Incidence and predictors of drug eluting stent fractures in human coronary artery: a pathologic analysis. J Am Coll Cardiol 2009;54:1924–31. http://dx.doi.org/10.1016/j.jacc.2009.05.075
3. Sianos G, Hofma S, Ligthart JM et al. Stent fracture and restenosis in the drug-eluting stent era. Catheter Cardiovasc Interv 2004;61:111–16. http://dx.doi.org/10.1002/ccd.10709
5. Mitomo S, Naganuma T, Takagi K et al. Comparison between plain old balloon angioplasty and drug eluting stent implantation for the treatment of stent fracture. J Interven Cardiol 2015;28:365–73. http://dx.doi.org/10.1111/joic.12215
This year’s European Society of Cardiology (ESC) Congress took place in Rome, Italy, from 27th–31st August 2016 and attracted over 33,000 delegates from across the globe, including His Holiness Pope Francis. Here we present some of the highlights from this key event in the cardiology calendar.
More news from ESC available online
More news reports from the ESC are available online at www.bjcardio.co.uk/news including:
• His Holiness Pope Francis (below) makes historic visit
• REM-HF study shows no benefit with remote monitoring of cardiac devices
• ODYSSEY ESCAPE: alirocumab reduces need for apheresis in FH
• Apheresis shows promise in refractory angina
• Pulmonary hypertension and anticoagulation highlights at congress
• Our practice message podcasts (see below)
ENSURE AF: edoxaban allows prompt cardioversion in AF
Patients with atrial fibrillation (AF) who need anticoagulation before undergoing cardioversion may benefit from treatment with the non-vitamin K antagonist oral anticoagulant (NOAC), edoxaban, compared to best possible conventional therapy (warfarin and enoxaparin), according to results from the ENSURE-AF study presented during a hotline session at the meeting.
The study also showed that newly diagnosed non-anticoagulated AF patients can start edoxaban as early as two hours prior to their cardioversion procedure if they have access to transoesophageal echocardiography (TOE) or three weeks prior to the procedure without.
ENSURE-AF (Edoxaban versus Enoxaparin/Warfarin in Subjects Undergoing Cardioversion of Atrial Fibrillation), the largest randomised clinical trial of anticoagulation for cardioversion in AF patients, involved 239 study sites in 19 countries in Europe and the USA, and included 2,199 patients with non-valvular AF.
At the discretion of the physician, patients either received delayed cardioversion (non-guided TOE stratum) or early cardioversion (TOE stratum). They were then randomised equally into two anticoagulation treatments groups per stratum receiving either edoxaban (60/30 mg once daily) or enoxaparin and warfarin (INR 2.0–3.0). Some 1,095 patients were randomised to receive edoxaban and the remaining 1,104 received enoxaparin/warfarin.
Primary efficacy outcomes (a composite of stroke, systolic embolic event, myocardial infarction and cardiovascular death) were not significant being reached in 0.5% patients (n=5) in the edoxaban arm versus 1.0% (n=11) in the enoxaparin and warfarin arm.
Safety outcomes showed no increased risk of major or clinically relevant non-major bleeding, which were similarly low between the two arms.
Net clinical outcome showed a trend to better outcome in the edoxaban arm but this was not significant.
The study presenter Dr Andreas Goette (St Vincenz Hospital, Paderborn, Germany) said that while conventional anticoagulation works well, it has a major limitation in that it requires regular monitoring and dose adjustment to ensure that patients reach anticoagulation targets, which means cardioversion can sometimes be delayed for several weeks.
“Edoxaban,” he continued “may allow prompt cardioversion to be performed following the start of anticoagulation.”
Discussant of the study at the hotline session, Dr Riccardo Cappato (Policlinico San Donato, Milan, Italy) said: “Edoxaban administered at the maximally tolerated single daily dose in the peri-procedural phase of elective AF cardioversion can be considered a safe and effective alternative to VKA therapy”.
The study was simultaneously published in The Lancet (doi: 10.1016/S0140-6736(16)31474-X) on August 30th 2016.
ANNEXA-4: reversal agent shows efficacy in acute bleeding
Preliminary results in the ongoing ANNEXA-4 study have shown that andexanet can rapidly reverse anti-factor Xa activity in acutely bleeding patients and is associated with excellent or good haemostasis in most.
ANNEXA-4 (Andexanat Alfa, a Novel Antidote to the Anticoagulation Effects of FXA inhibitors) is the first study to look at andexanet in acutely bleeding patients. The study was not randomised for ethical reasons and 67 patients, who required urgent reversal of acute major bleeding within 18 hours of receiving either a direct or indirect factor Xa inhibitor, were given andexanet alfa in a bolus over 15–30 minutes followed by a two-hour infusion.
An efficacy assessment carried out in 47 patients showed an 89% decrease in anti-factor Xa activity from baseline to end of bolus for those exposed to rivaroxaban (n=26) and 93% for those exposed apixaban (n=20). At 12 hours, clinical haemostatic efficacy was rated as good to excellent in 79% of patients.
Thrombotic events occurred in 18% of patients during the 30-day follow up. “This rate of events is not unexpected considering the thrombotic potential of the patients and the fact that in most of them anticoagulation was discontinued at the time of bleeding and not restarted,” said Dr Stuart J Connolly (McMaster University, Hamilton, Ontario, Canada) speaking at the ESC hotline session where the data was presented.
Initial investigation of patients with suspected coronary heart disease (CHD) using functional imaging – rather than National Institute for Health and Care Excellence (NICE) guideline-directed care – resulted in significantly less unnecessary angiography, according to results of the CE-MARC 2 trial.
Findings from CE-MARC 2 (Clinical Evaluation of Magnetic Resonance Imaging in Coronary Heart Disease 2) presented in a hotline session at the meeting could have an important impact on referral rates for invasive coronary angiography, and potentially healthcare costs, according to principal investigator Professor John Greenwood (University of Leeds).
The study included 1,202 patients with suspected CHD from six UK centres. Patients were randomised to functional imaging-based investigation with either:
cardiac magnetic resonance (CMR) (n = 481)
myocardial perfusion scintigraphy (MPS) (n = 481)
guideline-directed investigation (n=240) based on current NICE guidelines. Within this group, those with a pre-test likelihood of 10–29% (meaning low risk for CHD based on age, gender, symptom characteristics and clinical history) were scheduled for cardiac computed tomography (CCT); those with a pre-test likelihood of 30–60% (intermediate risk) were scheduled MPS; and those with a high pre-test likelihood were sent directly to coronary angiography.
The primary end point was unnecessary coronary angiography within 12 months, (defined by absence of significant stenosis measured by fractional flow reserve or quantitative coronary angiography), with secondary end points of major adverse clinical events (MACE), and positive angiography within this same time period.
Overall, 22% of the study population underwent coronary angiography within 12 months, with unnecessary angiograms occurring in 28.8% of the NICE guidelines group, 7.5% of the CMR group, and 7.1% of the MPS group, reported Professor Greenwood.
The adjusted odds ratio of unnecessary angiography for the CMR group versus the NICE guidelines group was 0.21 (95% CI, 0.12–0.34; P < .001), with no statistically significant difference between the CMR and MPS groups. Between the three strategies, there was no difference in short-term MACE or positive angiography rates.
“Rates of invasive angiography are considered too high among patients with suspected coronary heart disease,” explained Professor Greenwood. “Our findings show that both cardiovascular magnetic resonance (CMR) and myocardial perfusion scintigraphy (MPS) significantly reduced rates of unnecessary angiography compared to guideline-directed care, with no penalty in terms of major adverse cardiovascular events (MACE). This suggests that functional imaging should be adopted on a wider basis, even in high-risk patient subgroups.”
“Worldwide, MPS is the most commonly used test to assess suspected CHD, but CMR is increasingly recognised as having high diagnostic accuracy and prognostic value,” noted Professor Greenwood. “Although the results of CE-MARC 2 showed no difference between the CMR and MPS strategies in terms of unnecessary angiography rates, our original CE-MARC study showed that CMR had a higher diagnostic accuracy compared to MPS2 and was also a stronger predictor of risk for MACE.3
He concluded that “these results show that a broader use of functional imaging (CMR or MPS), in low, intermediate and high risk patient groups, could reduce the rates of invasive angiography that ultimately show no obstructive coronary disease. In addition, CE-MARC and CE-MARC 2 further support the role of CMR as an alternative to MPS for the diagnosis and management of patients with suspected CHD.”
The study is discussed in our podcast from the meeting by Dr Jubin Joseph (St Thomas’ Hospital, London, and President of the British Junior Cardiologists’ Association). He says the results show that functional imaging should be adopted on an even wider basis than currently even in high-risk subgroups, which could potentially reduce rates of coronary angiography and costs.
Greenwood JP, Maredia N, Younger JF, et al. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial. Lancet 2012;379:453–60. http://dx.doi.org/10.1016/S0140-6736(11)61335-4
Hunink MGM, Fleischmann KE. The role of randomized and nonrandomized studies in evaluating diagnostic strategies. Ann Intern Med 2016;165:61–2. http://dx.doi.org/10.7326/M16-0811
NORSTENT: drug-eluting stents no better than bare-metal stents
New generation drug-eluting stents (DES) are not superior to contemporary bare-metal stents (BMS) according to a surprise finding of the largest randomised stent trial to date, NORSTENT (the Norwegian Coronary Stent Trial).
“The efficacy of new DES versus contemporary BMS is lower than expected,” said Professor Kaare Harald Bønaa (University of Tromso – The Arctic University of Norway, and the Norwegian University of Science and Technology, Trondheim, Norway) at the ESC hotline session where the data was presented.
“Patients treated with DES do not live longer and they do not live better (in terms of quality of life) than patients treated with BMS,” he said.
With 9,013 patients and more than 40,000 patient years of follow-up, NORSTENT was an all-comers study in a usual care setting, and therefore had “the potential to yield outcomes of great relevance to clinical practice,” he added.
The multi-centre study included patients with stable angina pectoris (n=2,636) or acute coronary syndromes (n=6,377) who needed percutaneous coronary intervention (PCI). Patients were randomised to receive either BMS or DES, with 83% of DES patients receiving everolimus-eluting stents and 12% receiving zotarolimus-eluting stents.
After six years of follow-up, there was no significant difference between the DES and the BMS groups in the primary outcome of total mortality or nonfatal myocardial infarction (cumulative rate of 16.9% in the DES group versus 17.4% in the BMS group; HR 0.98), as well as secondary outcomes of unstable angina, or quality of life.
“As expected, the need for repeat revascularisation was lowered by DES, but this effect was much less than anticipated,” said Professor Bønaa. “The six-year cumulative rate of repeat revascularisation was 14.9% in the DES group versus 17.7% in the BMS group – an absolute risk reduction of 2.8%.
“Although ESC guidelines recommend new DES over BMS as default for coronary revascularisation, this recommendation may need to be modified in light of the NORSTENT findings…both stent types may be recommended,” Professor Bønaa concluded.
But discussant of the study, Professor Stefan James (Univeristy of Uppsala, Sweden), disagreed. While noting that the results were surprising, he thought the ESC guidelines should stand. “DES (new generation) should remain recommended over BMS due to better performance with 5% (53% relative risk reduction) reduction of target lesion revascularisation, 3.3% (24% relative) of any revascularistaion and a 0.4% (36% relative) reduction in stent thrombosis.
The study was published simultaneously in the New England Journal of Medicine on August 30th 2016 (doi: 10.1056/NEJMoa1607991).
REM-HF trial: no benefit with remote monitoring of cardiac devices
Remote monitoring of cardiac implantable electronic devices (CIEDs) does not improve outcomes (mortality or hospitalisations) in heart failure compared to usual care, according to results from the REM-HF (The Remote Management of Heart Failure Using Implantable Electronic Devices) study.
The study was conducted in a setting “intended to maximise the benefit of remote monitoring,” commented Professor Martin Cowie (Imperial College London, and Royal Brompton Hospital, London) the co-principal investigator of the study, at the hotline session where he presented the results.
Thus the results “do not support its routine use in the management of patients with CIEDs…If patients are well-treated already, and have well-controlled symptoms, looking at remotely collected data weekly is no better than usual care,” he said.
CIEDs that are equipped with remote monitoring capabilities store data that can be downloaded and transmitted via the internet or telephone connections to their physicians for interpretation. The REM-HF study was conducted at nine British hospitals in 1,650 heart failure patients (mean age 70 years), with one of three types of CIEDs equipped for remote monitoring:
cardiac resynchronization therapy (CRT) device with pacemaker (CRT-P);
CRT device with defibrillator function (CRT-D);
or implantable cardioverter-defibrillator (ICD);
Patients were randomised to receive either usual care (UC) or remote monitoring (RM).
RM patients had data downloaded automatically from their device on a weekly basis, which was transmitted to their healthcare professional who used it to advise them about medication and lifestyle, need for additional clinic visits, or recommendations to visit their general practitioner or the emergency room. They also had the usual care delivered by their local heart failure service.
UC patients did not have weekly automatic downloads, but had usual remote monitoring of the device (typically three to six monthly) in addition to usual care from their heart failure service.
The study’s primary end point was the first event of death from any cause or unplanned hospitalisation for cardiovascular reasons. Secondary end points included death from any cause, death from cardiovascular reasons, and unplanned hospitalisation.
After a median follow-up period of 2.8 years, no significant difference was seen between the groups in the primary end point, which occurred in 42.4% of the RM group and 40.8% of the UC group (hazard ratio 1.01; 95% confidence interval [CI] 0.87 to 1.18; P=0.87).
Secondary end points also occurred at a similar rate in both groups. “Although some studies investigating a range of remote monitoring strategies have suggested potential benefit, and adoption of remote monitoring is quite widespread, results of the REM-HF trial offer a new perspective that has the potential to change clinical practice,” said Professor John Morgan (University of Southampton) co-principal investigator of the study.
“Despite a large number of patients, considerable follow-up time, acceptable patient adherence to weekly downloads, and additional contacts with patients driven by the remotely collected data, we did not demonstrate any improvement in outcome for patients randomised to remote monitoring compared to usual care in nine English hospitals,” said Professor Cowie.
“It is possible that an effect could be demonstrated in health care systems with less well developed usual care, where patients are less-well treated and have more severe symptoms”, he concluded.
ODYSSEY ESCAPE: alirocumab reduces need for apheresis in FH
Treatment with the PCSK9 monoclonal antibody alirocumab offered the possibility of sparing lipoprotein apheresis, a therapy which is used to filter excess cholesterol from the blood, in patients with severe heterozygous familial hypercholesterolaemia (FH), according to results from the ODYSSEY ESCAPE study.6
In the UK, lipoprotein apheresis is being performed with increasing frequency, but still lags behind use in other European countries. Despite this, it is an essential treatment for homozygous FH, as well as severe heterozygous FH with progressive cardiovascular disease (CVD) refractory to combined drug therapy.
“Being able to reduce or eliminate apheresis would be a major breakthrough for these patients who spend US$50,000 to US$75,000 a year, and three to four hours every one to two weeks to clear their blood of excess LDL-C’” said Professor Patrick Moriarty (University of Kansas Medical Center, Kansas City, USA) at the hotline session where he presented the results.
ODYSSEY ESCAPE (Effect of Alirocumab on the Frequency of Lipoprotein Apheresis) was conducted in 62 patients from 14 centres in the USA and Germany undergoing regular (either every week or two weeks) lipoprotein apheresis. Patients were randomised to treatment with alirocumab 150 mg (n=41) or placebo (n=21) every two weeks for 18 weeks, while still continuing other lipid-lowering treatment. During the first six weeks, apheresis frequency was fixed to the individual’s established schedule but from week seven was only performed if low-density lipoprotein (LDL) cholesterol was <30% lower than the baseline pre-apheresis value.
Results showed that treatment with alirocumab significantly reduced the need for apheresis treatment in 75% of patients versus placebo (p<0.0001). In patients receiving alirocumab, LDL cholesterol was reduced by 54% (versus an increase of 2% on placebo), led to avoidance of at least half of apheresis treatments in 93% of patients (compared to 14.3% on placebo), and all apheresis treatment in 63% of patients.
There was some discussion about the comparability of patients enrolled by the two countries, as fewer US patients were on maximally tolerated statin (due to more statin intolerance), and consequently had higher LDL-C levels at baseline than those in Germany. Additionally, apheresis was used every two weeks in the USA but weekly in Germany. Despite these confounders, the findings have important implications for patient care and cost, according to lead author Professor Patrick Moriarty (University of Kansas Medical Center, Kansas City, USA).
According to Professor Moriarty, who speaks about the study in our podcast from the meeting, “We now have a class of drugs that should be implemented before transferring a patient for apheresis.”
The study was published simultaneously in the European Heart Journal (doi: 10.1093/eurheartj/ehw388)
Apheresis shows promise in refractory angina
A UK study presented at the lipids hotline session suggested a potential role for lipoprotein apheresis in the management of patients with refractory angina (RA) and high lipoprotein(a) [Lp(a)] levels >500 mg/dL.
Elevated Lp(a) is a cardiovascular risk factor which may promote atherosclerosis via both lipid-related, prothrombotic and anti-fibrinolytic actions. In the study ‘Apheresis as a Novel Treatment for RA and Lp(a),’ 20 patients were randomised to weekly lipoprotein apheresis or sham treatment for three months following a one month washout, crossed over to the alternative treatment for a further three months.
There was a sharp rise in myocardial blood flow post-apheresis. Compared with sham, apheresis treatment significantly improved (increase from 1.45 to 1.93, p<0.001) the primary outcome of myocardial perfusion reserve (MPR), the ratio of the myocardial blood flow at stress versus rest measured by cardiac magnetic resonance imaging. There were also significant improvements in the secondary end points of carotid wall volume and distensibility, exercise capacity, symptoms of angina, and quality of life scores.
“These findings suggest a much needed novel treatment option for these therapeutically challenging patients,” said study presenter Dr Tina Zubaida Khan (Royal Brompton and Harefield NHS Trust and Imperial College, London).
Discussant Dr Peter Libby (Brigham and Women’s Hospital, Boston, USA) said that as PCSK9 inhibitors were able to reduce Lp(a), “we may be entering an era when we could be offering patients and their families a non-apheresis treatment for reducing Lp(a)”.
New ESC clinical practice guidelines published
Four new clinical practice guidelines were published by the ESC at the Congress on:
ESC guidelines for the diagnosis and treatment of acute and chronic heart failure
ESC and European Association for Cardio-Thoracic Surgery (EACTS) guidelines for the management of atrial fibrillation
ESC and European Atherosclerosis Society (EAS) guidelines for the management of dyslipidaemia (see Appendix 1, below)
ESC Position paper on Cancer Treatments and Cardiovascular Toxicity (see Appendix 2, below).
ESC practice messages podcasts available
Watch our podcasts from the meeting, which highlights key studies and their implications for your everyday practice. We interview Professors John Camm (St George’s, University of London), Patrick Moriarty (University of Kansas Medical Center, Kansas City, USA), and Dr Jubin Joseph (St Thomas’ Hospital, London, and President of the British Junior Cardiologists’ Association).
Appendix 1: New lipid guidelines
Updated Joint ESC/European Atherosclerosis Society (EAS) Guidelines for the Management of Dyslipidaemia were published at the start of ESC Congress.1 According to EAS President, Professor Alberico L. Catapano (University of Milan and Multimedica IRCCS, Italy) lead author of this initiative, there are three key messages for clinicians.
Although LDL-C targets have not changed, for both high and very high risk patients, a secondary target is to attain at least 50% reduction from baseline LDL‑C
Nonfasting – rather than fasting – lipid measurement is recommended for screening, supported by evidence from a recent consensus statement2
The guidelines re-emphasise the importance of lifestyle intervention in prevention of cardiovascular disease (CVD), across the spectrum of cardiovascular risk.
The guidelines include added information on the benefits of dietary intervention such as adoption of the Mediterranean diet. This is not just relevant for the primary prevention setting,3 but also in patients with established CVD, as shown by a report from the MOLI-SANI study.4 Among 1,197 patients with established CVD followed for a median of 7.3 years, improved adherence to the Mediterranean diet (i.e. a 2-point increase in the 9-point Mediterranean diet score) led to a 21% reduction in mortality. For patients with the highest adherence, there was a 37% risk reduction, exceeding the effects of statins.
In addition, a hotline report of a Mendelian randomisation study (a type of ‘natural clinical trial’) reinforced the potential benefit from ‘the earlier the better’ CVD prevention.5 Data from over 100,000 individuals (mean age 60.5 years, 57% women, mean LDL-C 3.4 mmol/L and mean systolic blood pressure [SBP] 126 mmHg) were evaluated using genetic scores for LDL-C (based on 46 polymorphisms or genetic variants associated with lower LDL-C) and SBP (based on 33 polymorphisms associated with lower blood pressure). Long-term exposure to even modestly lower LDL-C (by 1 mmol/L) and SBP (by 10 mmHg) was associated with 86.1% reduction in the risk of major vascular events, dramatically reducing lifetime CVD risk.
Appendix 2: New position paper on cardio-oncology
This ESC position paper aims to raise awareness of the cardiac toxicity of anticancer therapies.11 It offers guidance on how to define patients at risk; detect and prevent toxicity; and treat and follow up affected patients. The development of multidisciplinary teams, including cardiologists, oncologists, nurses, and heart failure and imaging specialists, is key to provision of best patient care.
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits

 Drug therapies include anticoagulants to reduce the risk of stroke and anti-arrhythmics to restore/maintain the normal heart rhythm or slow the heart rate in patients who remain in AF. Non-pharmacological management options include electrical cardioversion, which may be used to ‘shock’ the heart back to its normal rhythm.
Drug therapies include anticoagulants to reduce the risk of stroke and anti-arrhythmics to restore/maintain the normal heart rhythm or slow the heart rate in patients who remain in AF. Non-pharmacological management options include electrical cardioversion, which may be used to ‘shock’ the heart back to its normal rhythm.