The National Institute for Health and Care Excellence (NICE) has made an important change to Clinical Guideline 64 (CG64)1 adding the word ‘routinely’ to Recommendation 1.1.3: “Antibiotic prophylaxis against infective endocarditis is not recommended routinely for people undergoing dental procedures”. In a letter about the change,2 Sir Andrew Dillon, CEO of NICE, confirmed that “… in individual cases, antibiotic prophylaxis may be appropriate”.
This change followed approaches to Sir Andrew Dillon by the widow of a patient with a replacement aortic valve who died from infective endocarditis (IE) developing after unprotected dental scaling. Her case included: evidence that antibiotic prophylaxis is effective in people at high risk of IE having high-risk dental procedures;3 the observation that the incidence of IE in the UK has accelerated above the global background rise since the original 2008 NICE guidance;4 a change in the law on consent.5-7
It is now necessary for dentists to appraise their patient of the differences between NICE and other guidelines, if it is likely that they would have a special interest, for example if they have a replacement heart valve or prior IE.8 Their general practitioner or cardiologist could consider advising the patient and their dentist on the level of risk in a letter. The patient should then be allowed to make up their own mind whether or not to have antibiotic prophylaxis. General Medical Council (GMC)/General Dental Council (GDC) standards and the advice of the medical/dental defence organisations highlight the need for this discussion (and the patient’s decision) to be recorded in the clinical records.
Prophylaxis should be with amoxicillin 3 g by mouth one hour before the procedure or, for patients with penicillin hypersensitivity, clindamicin 600 mg orally. Adverse effects from oral amoxicillin prophylaxis are uncommon with no deaths reported in Europe since records began.8 Clindamicin has a slightly higher level of risk.9 Both are cost-effective in high-risk patients having high-risk dental procedures.8
Staff in general practices and specialist valve clinics should emphasise that good oral hygiene and regular dental review are as important as antibiotic prophylaxis, if not more so, in reducing the risk of IE. The European Society of Cardiology (ESC) recommend10 strict dental and cutaneous hygiene with regular dental surveillance. It is also important to educate patients at risk in recognising the possibility of IE. Typically, there may be persistent night sweats, general malaise and weight loss. At least two sets of blood cultures should be taken before starting antibiotics. The British Heart Foundation produce warning cards that can be given to patients – available at: https://www.bhf.org.uk/publications/heart-conditions/m26a-endocarditis-card
The subtle change makes NICE guidance less dogmatic and allows clinicians to use their clinical judgement, follow well-accepted international guidelines,10 and provide the care their patients want.
Summary of guidance
People at high risk: replacement heart valves or prior endocarditis
People at moderate risk: native valve disease
High-risk dental procedure: extractions, root canal treatment, dental scaling and other procedures involving manipulation of the gums
Antibiotic prophylaxis: indicated for people at high risk having high-risk dental procedures. Record details of consent process in the dental notes. Use amoxicillin 3 g or clindamicin 600 mg orally one hour before
Other advice: dental surveillance six monthly (high-risk people) or annually (medium-risk people), avoid tattoos and intravenous drug use
Warning: consider infective endocarditis with persistent fever or night sweats especially with systemic symptoms. Consider blood cultures before starting an antibiotic course
Conflict of interest
None declared.
References
1. National Institute for Health and Care Excellence. Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures. Clinical Guideline 64. London: NICE, July 2016. Available from: http://www.nice.org.uk/guidance/cg64/chapter/Recommendations
2. Thornhill MH, Dayer M, Lockhart PB et al. A change in the NICE guidelines on antibiotic prophylaxis. Br Dent J (in press).
3. Chambers JB, Thornhill M, Shanson D, Prendergast B. Antibiotic prophylaxis of endocarditis: a NICE mess. Lancet Infect Dis 2016;16:275–6. http://dx.doi.org/10.1016/S1473-3099(16)00048-7
4. Dayer MJ, Jones S, Prendergast B, Baddour LM, Lockhart PB, Thornhill MH. Incidence of infective endocarditis in England, 2000–13: a secular trend, interrupted time-series analysis. Lancet 2015;385:1219–28. http://dx.doi.org/10.1016/S0140-6736(14)62007-9
8. Thornhill MH, Dayer M, Lockhart PB et al. Guidelines on prophylaxis to prevent endocarditis. Br Dent J 2016;220:51–6. http://dx.doi.org/10.1038/sj.bdj.2016.49
9. Thornhill MH, Dayer MJ, Prendergast B, Baddour LM, Jones S, Lockhart PB. Incidence and nature of adverse reactions to antibiotics used as endocarditis prophylaxis. J Antimicrob Chemother 2015;70:2382–8. http://dx.doi.org/10.1093/jac/dkv115
10. Habib G, Lancellotti P, Antunes MJ et al. 2015 ESC Guidelines for the management of infective endocarditis. Eur Heart J 2015;36:3075–128. http://dx.doi.org/10.1093/eurheartj/ehv319
Compared with other diseases, cardiovascular diseases (CVD) are responsible for the greatest burden of disease both globally1 and in the UK.2 Drugs for CVD and its risk factors have always been represented in the list of international blockbuster drugs. Important research innovations, such as ‘learning health systems’, ‘precision medicine’ and electronic health record (EHR)-based trials, have been led by professionals in the field of cardiology. Cardiovascular scientists from the UK have a long and strong history of research contributions with international impact. Training in cardiology is critical, not only in preparing and mentoring the clinical and academic cardiologists of the future, but also in shaping how the specialty is perceived from inside and outside. Global health and data science are overarching themes that offer new lenses through which to view CVD and cardiology. However, cardiology training in the UK barely pays lip service to either of these issues, when their implications have never been greater or more acute on our specialty.
Opportunity for global health
Over 40% of UK medical students gain experience in a developing country during their elective rotation, broadening perspective on disease and healthcare, as well as personal development by experiencing different cultures.3 Experience in low- and middle-income countries (LMICs) during postgraduate training offers similar benefits, but the number of trainees who embark on such rotations is comparatively small and restricted to particular specialties in the UK.
According to the 2012 British Junior Cardiologists Association trainee survey, 66% of trainees had completed or planned to undertake a clinical fellowship, with the majority planning to go overseas, but rarely to a LMIC.4 A similar pattern is seen in the research domain, with the vast majority of trainees taking time out of their programme for research, but very few undertaking work in CVD prevention, implementation research or CVD in LMICs. Specialties such as infectious diseases and obstetrics have a tradition of encouraging training in LMICs and have a greater global outlook in their research priorities, which better positions trainees to adapt to changing disease epidemiology worldwide.5
CVD is the biggest cause of disability and death internationally,1 and while rheumatic heart disease and conditions such as Chagas’ cardiomyopathy are more prevalent in certain regions of the world than the UK, the vast majority of CVD burden is myocardial infarction, heart failure or stroke. Contrary to the impression held by many, the risk factors for CVD in LMICs are largely the same as those in high-income countries.6 There is a certain irony in the lack of a global perspective within cardiology given that clinical and research knowledge and skills in cardiology are genuinely transferable between more developed and less developed regions of the world. This is in contrast with the field of infectious diseases, for example, where the aetiology and presentation of disease varies greatly across different regions worldwide. The World Health Organisation, the World Heart Federation, international policy makers and UK research funding bodies such as the Medical Research Council have made reducing the global burden of CVD a priority, and the cardiology community in countries, such as the UK, have a great deal to contribute to achieving this goal.7,8
Medical training in North America has been quicker to embrace the opportunities of taking a greater global perspective. Funding initiatives such as the National Institute of Health’s Fogarty International Fellows Programme supports trainees, including those in cardiology, to develop skills to be independent researchers in the field of global health.9 A number of residency programmes have established global health-themed programmes, allowing trainees to gain experience at international centres, usually in LMICs, in a clinical and/or research capacity.10 Such programmes facilitate two-way transfer of knowledge and skills between clinicians and researchers in both countries and can establish strong collaborative networks for ongoing research. Establishing, maintaining and capitalising on such networks is vital to reduce the burden of CVD worldwide. Examples of institutions that have embedded and integrated clinicians with global health and/or data science expertise are the Population Health Research Institute, McMaster University in Canada and the Institute for Health Metrics and Evaluation, University of Washington in the US. The value of perspective from practising cardiologists, with their in-depth knowledge of disease and the underpinning science, should not be underestimated, and, indeed, the number of cardiologists undertaking research in this space is increasing, albeit slowly.
Using data science to break down silos
Concerns for a speciality, which has embraced subspecialisation, but not cross-cutting themes, are not new or specific to cardiology. UK cardiologists have been instrumental in developing and evaluating many of the treatments that are now standard of care for patients with, or at risk of, CVD. However, a failure to adequately emphasise the most pressing issues in cardiovascular science in the core training curriculum will have consequences on the readiness of cardiologists to research and practise in the health system of tomorrow.
Data science embraces epidemiology, ‘big data science’, health informatics, e-health and m-health. Use of large clinical datasets, increased technology and devices, expansion in mobile healthcare and an exponential rise in publications are already shaping the field of cardiovascular research and integrating into routine clinical practice. The age of ‘–omics-based’, ‘personalised medicine’ and ‘learning health systems’ demands knowledge of data science from clinicians and academics alike, and cuts across the subspecialties, whether electrophysiology, intervention or imaging. There is currently little training in these areas as part of the UK core cardiology curriculum. Lack of knowledge or awareness of these areas is against trends in other countries, such as the US, where opportunities in big data science are recognised. For example, organisations such as the American Heart Association, are engaging trainees to optimise the environment for acquisition, sharing, and governance of large-scale healthcare data.11
Benefits to UK cardiology
Some of the most influential work affecting prevention and treatment of CVD, and other diseases more broadly, in the last 50 years, originates from non-clinical research, including social determinants of health, health and treatment inequalities and the global burden of disease. Epidemiology and prevention still occupy a relatively small part of cardiology training, yet these areas have contributed to the UK being a world leader in epidemiological research and clinical trials, with many seminal trials led by cardiologists in the UK.
To not incorporate data science and global health into the training curriculum has two negative implications. First, cardiologists will not be engaged in global health and data science agendas, leaving other disciplines, such as public health, to lead, as has historically been the case for epidemiology and prevention in the UK. Second, both clinical and academic cardiologists will fail to capitalise on the potential for research and implementation in the UK and beyond. In order to be competitive, data science and a global perspective are crucial to training cardiologists.
Call for action
The cardiology community in the UK needs to adapt to the changing landscape of research and clinical practice. Training must evolve to address global and national trends in CVD epidemiology, as well as grounding in data science. Interested trainees undertaking a higher degree should consider further training in data science, placing them in a strong position to be at the forefront of a new, but essential, part of future cardiovascular research. Basic knowledge of big data is relevant to all cardiologists, not just researchers, in order to interpret and contextualise the research of tomorrow. It is encouraging that the theme of the British Cardiovascular Society Annual Meeting in 2016 was ‘Prediction and prevention’ with a keynote speech entitled ‘Big data: a big deal for cardiology’.
Cardiologists with interest in global cardiovascular health should provide mentorship to interested trainees. Opportunities for trainees to gain clinical or research experience in LMICs and collaboration with physicians and scientists in LMICs should be viewed as a valuable two-way relationship, whether ‘within’ or ‘out of’ programme.
In an already crowded curriculum, e-learning modules may represent the most feasible and relevant way to introduce data science and global health to trainees. Bespoke training days are another possibility. Just as leadership/management and basic science are part of the core curriculum, which can be further developed as out-of-programme or post-certificate of completion of training (CCT) experiences, data science and global health can be considered in the same way. More than other aspects of the curriculum, these two new areas are cross-cutting and must not be considered in isolation, which allows them to contribute to other training and competencies. Both trainees and their mentors will need to be creative, but their efforts alone are unlikely to prompt culture change. Engagement from multiple stakeholders across the NHS, universities, Royal Colleges, General Medical Council and other medical specialties is required, but cardiology has the chance to lead the way.
Conflict of interest
None declared.
References
1. Global Burden of Disease Study C. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;386:743–800. http://dx.doi.org/10.1016/S0140-6736(15)60692-4
2. Newton JN, Briggs AD, Murray CJ et al. Changes in health in England, with analysis by English regions and areas of deprivation, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;386:2257–74. http://dx.doi.org/10.1016/S0140-6736(15)00195-6
6. Yusuf S, Hawken S, Ounpuu S et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 2004;364:937–52. http://dx.doi.org/10.1016/S0140-6736(04)17018-9
7. Medical Research Council. Research strategy. Available from: http://wwwmrcacuk/research/strategy/
8. Yusuf S, Wood D, Ralston J, Reddy KS. The World Heart Federation’s vision for worldwide cardiovascular disease prevention. Lancet 2015;386:399–402. http://dx.doi.org/10.1016/S0140-6736(15)60265-3
9. Bloomfield GS, Huffman MD. Global chronic disease research training for fellows: perspectives, challenges, and opportunities. Circulation 2010;121:1365–70. http://dx.doi.org/10.1161/CIRCULATIONAHA.109.923144
10. Miller WC, Corey GR, Lallinger GJ, Durack DT. International health and internal medicine residency training: the Duke University experience. Am J Med 1995;99:291–7. http://dx.doi.org/10.1016/S0002-9343(99)80162-4
11. Antman EM, Benjamin EJ, Harrington RA et al. Acquisition, analysis, and sharing of data in 2015 and beyond: a survey of the landscape. A conference report from the American Heart Association Data Summit 2015. J Am Heart Assoc 2015;4:e002810. http://dx.doi.org/10.1161/JAHA.115.002810
The ability to perform invasive diagnostic coronary angiography is a core requirement for cardiologists and fellows in training programmes. However, although key to their independence is the ability to obtain high-quality images that allow visualisation of the entire coronary vasculature, there exists no formal systematic method or teaching aid. This article provides an overview of the radiological equipment used in the catheter laboratory, details the naming of the different angiographic projections, and gives key tips and tricks to improve image quality. In addition, the coronary vasculature is broken down into segments, with descriptions provided of the essential views required to image each one. Using this approach, it aims to provide an essential aid to trainees and other healthcare professionals at the start of their careers.
There is variable adoption in same-day discharge for pacing procedures across Europe. We compared length of hospital stay and complication rates in two cohorts, using a same-day and next-day discharge protocol. Case notes were reviewed for 229 consecutive patients attending our tertiary centre for device implantation to establish the rate of hospital readmission and complications. These comprised 106 patients in the next-day discharge cohort, and 123 from the same-day cohort. All pacing procedures, including cardiac resynchronisation therapy (CRT) and implantable cardioverter-defibrillators (ICDs), were included.
No significant differences were observed between cohorts in age, gender, device indication, device type, procedure urgency or venous access route. Median length of stay post-implant significantly reduced from 1.2 days in the next-day cohort (25th–75th centile 1.06–3.24) to 0.99 days in the same day cohort (0.3–1.3) and from 1.08 days (0.94–1.2) to 0.36 (0.27–0.97), respectively, for the subgroup of elective patients (n=95). Death, complication, and readmission rates were similar between the two cohorts. Morning procedures were associated with shorter hospitalisation. No same-day cohort CRT recipients (n=28) suffered complications.
In conclusion, same-day discharge for pacing (including CRT and ICDs) results in decreased length of stay without increasing complications.
Introduction
In many centres, patients stay overnight after their pacing procedure. Most would prefer to get home quicker, and reduced length of stay would result in healthcare savings. Various centres have reported high rates of patient satisfaction,1 and significant cost-savings with day-case pacing,2,3 although this practice is not widespread. A recent survey,4 revealed variation in practice across Europe with many centres routinely mandating a one or two night hospital stay.
The safety of day-case pacing was described more than 25 years ago.5,6 Since then, the implant rates of both bradycardia (simple) and more complex devices (cardiac resynchronisation therapy [CRT] and implantable cardioverter-defibrillator devices [ICDs]) have increased significantly.7-10 We are not aware of any published data on the safety of day-case pacing for complex devices.
Due to a recent change in our institution’s implantation policy from a mandatory overnight stay to same-day discharge, we were in a unique position to review the efficacy, safety and cost-effectiveness of such a change. We describe a single-centre, retrospective, cohort study, comparing a next-day discharge with same-day discharge for both simple and complex pacing procedures.
Methods
In our tertiary centre, outcomes and complications of pacing procedures were retrospectively reviewed before and after a change to same-day discharge. Pacing procedures were reviewed for consecutive patients for 60 days prior to the change in protocol (next-day cohort) and compared with consecutive patients for 60 days afterwards (same-day cohort).
Data were collected from the cardiology department at the university teaching hospital in Sheffield, UK. In May 2014, a change in operating protocols was introduced, allowing uncomplicated pacemaker recipients to be discharged on the same day as their procedure. All patients were discharged on the same day as their procedure, unless they were medically unfit, had procedural complications, or presented with high-grade block or syncope, where immediate lead displacement would have had significant consequences. All patients attending for device therapy during March and April 2014, and during June and July 2014 were included.
Baseline demographic data, device type and procedural urgency were collected. Pacing and clinical records were reviewed for any 30-day readmission to hospital, early complications of the procedure (pneumothorax, haematoma requiring intervention/prolonged observation, cardiac tamponade, immediate lead displacement), late complications (lead repositioning, requirement for urgent device reprogramming after 30 days) and death. No other procedural changes were made during the period of study.
Both elective and urgent/inpatient pacing procedures were included in the analysis. The inpatient group comprised patients who had been admitted acutely but could not be safely discharged before device implantation. All patients were followed up for four months post-procedure.
Student’s t-test was used when continuous data were normally distributed and Wilcoxon’s rank-sum test when it was not. Fisher’s exact test was used for binomial variables, and Chi-squared used for categorical data. P values <0.05 were considered significant. Calculations were performed with Stata SE 10 for Mac.
Results
Two hundred and twenty-nine patients attended for device insertion, of which, 106 patients were in the next-day cohort and 123 in the same-day cohort. Across both cohorts, there were 56 CRT devices (24%) and 36 ICDs (16%). Just under half of these were elective (n=95, 41%) with the remainder being inpatients. No significant differences were observed between the cohorts in age, gender, status of primary operator, device indication, device type, venous access or procedure urgency (table 1).
Table 1. Patient demographics
Length of stay
Figure 1. Time from elective pacemaker implantation to hospital discharge (excludes outside values)
In the same-day cohort, 41 individuals (33.4%) were discharged on the day of their procedure, compared with one patient (1%) from the next-day cohort. After the change of protocol, the median time from device implantation to discharge reduced from 1.2 days (25th–75th centile, 1.06–3.24) to 0.99 days (0.3–1.3, p<0.001) for all patients, with the data positively skewed. Taking only elective procedures into account, this reduced from 1.08 days (0.94–1.2) to 0.36 (0.27–0.97, p<0.001) (figure 1). With inpatients, the median time similarly reduced from 1.56 days (1.11–4.57) to 1.25 days (0.99–6.03, p=0.101).
With the new protocol, 54% of our elective patients were discharged on the same day as their procedure. Reasons cited for overnight stay include social concerns (13 patients, 52%), monitoring of bleeding (one patient, 4%), concern regarding lead stability (one patient, 4%), pacing checks (two patients, 8%), inpatient up-titration of medication (one patient, 4%), delay attaining the post-implantation chest X-ray (one patient, 4%) and operator discretion (six patients, 24% – significant inter-operator variability noted).
Implant timing
In the same-day cohort, 22 of 30 elective patients who had morning procedures were discharged later that day, compared with only nine of 27 elective individuals who had their procedures in the afternoon (p=0.002).
In our study period, no devices were inserted outside of 8am to 5pm, but four of 135 acute inpatients had their devices implanted at the weekend. These were associated with a non-significant trend towards longer stays (median 88.4 hours, 25th–75th centile 26.9–196.2) post-implant compared with weekday procedures (31.2 hours, 25.6–123.5) (p=0.59). During the working week, no significant difference was observed relating to the day of the week a procedure was performed.
Complications
Table 2. Complications
No deaths were directly associated with device implantation, and mortality was similar for the two cohorts (table 2). Two patients developed pneumothoraces, and two patients had cardiac tamponade; in both cases this was identified during the procedure and was treated successfully. There were no observed lead displacements within 30 days, although six patients required lead repositioning at some stage after the six-week device check. Overall, complication and readmission rates were similar between the two cohorts.
We reviewed the cases of those patients who were readmitted within 30 days of discharge. In the next-day cohort, three patients were readmitted with unrelated medical problems, and a fourth patient was readmitted four days after discharge with non-cardiac chest pain, possibly relating to bruising at the pacemaker implantation site. Of the 12 patients readmitted from the same-day cohort, one patient was readmitted the day after the procedure with diaphragmatic twitch (dual-chamber device, reprogrammed), and another after 25 days with early device infection. There were no other procedure-related readmissions. Device interrogation in readmitted patients revealed no pacing complications.
We observed a trend that those patients discharged more than two days after their procedure had a higher adverse outcome rate (33%) than those discharged on the day of their procedure (7.1%).
Complex devices
In the same-day cohort, 14 of 28 patients receiving CRT devices and six of 22 patients receiving ICDs were discharged on the day of their procedure. No CRT recipients in this cohort required device reprogramming at or before the routine six-week follow-up. This compares with two of 28 CRT patients (7%) from the next-day cohort, with twitch identified at or before the six-week check.
Financial impact
We examined the potential cost savings available by moving to a same-day discharge protocol. This change reduced the mean post-implantation stay from 1.1 to 0.54 days per elective patient (p<0.001), and from 4.6 to 4.3 days for inpatients (p=0.19). Our institution implants approximately 690 devices per year. A conservative estimate based on these figures suggests the same-day discharge approach could save 280 bed-days over the course of one year. Given an average excess bed-day cost of £275,11 this would result in savings of £77,000 per year in our institution alone.
Discussion
For the first time, we compare two cohorts of real-world patients following device implantation, before and after a change to same-day discharge. Our data demonstrate the safety of this in the setting of expanded pacing indications.10 Additionally, we include complex device recipients whom we have shown can be safely discharged on the day of their procedure.
The new discharge policy did not result in an increased rate of readmission. Interestingly, most of the 12 patients in the same-day cohort that were readmitted within 30 days, had been kept in hospital overnight post-implant due to social reasons or being medically unfit for discharge. Moreover, across both cohorts, complications were more frequent in those discharged later. Such patients are generally frailer with diminished physiological reserve, and, therefore, it is unsurprising that they were soon readmitted to hospital for reasons unrelated to their pacing procedure.
One patient in the same-day cohort was readmitted the day following his procedure with diaphragm twitch from a dual-chamber device, which potentially would have been identified at a next-day device interrogation, though this was identified and treated promptly with device reprogramming.
Overall, complication rates were similar for the two cohorts. In the same-day discharge cohort, no issues were identified at the six-week post-implant check that would have otherwise been highlighted on a next-day device interrogation. Thus, it seems little is to be gained by keeping pacing patients in hospital for the night after their implant.
Elective patients
For both cohorts, the number of inpatient procedures was similar, suggesting a uniform demand for urgent pacing services. However, in the same-day discharge cohort a greater number of elective procedures were undertaken compared with the next-day cohort. This could have been partly due to the extra bed capacity created by the new discharge policy.
We found a significant increase in the same-day discharge rate in those patients receiving their device in the morning. Further study is required to investigate this trend. Nevertheless, institutions aiming to increase their same-day discharge rate may consider moving pacing sessions to earlier in the day.
Few devices were inserted at weekends, and weekend device implantation was associated with longer inpatient stays, though this probably represents illness severity rather than organisational factors. We hypothesised that device implantation on a Friday might be associated with increased length of stay, though our data did not show this. Indeed, except for devices inserted acutely over the weekend, day of the week did not appear to be a factor in determining length of stay.
In the same-day cohort, more than half of elective patients were discharged on the day of their procedure, though some 46% still waited until the following day. This is a lower same-day discharge rate than has been reported elsewhere.1,2 However, we describe an early experience of a new protocol. Often there was a clear post-implantation intention for overnight stay. As a unit, we are considering ways to increase the same-day discharge rate, for example by removing the current requirement for post-implantation chest radiograph,12 and ensuring that discharges delayed for non-medical reasons are better anticipated. Additionally, we expect the discharge rate to increase as familiarity with the protocol increases among ward staff. Eventually, we expect the same-day discharge rate for elective patients to reach 90%, with overnight stay provision only for unexpected medical complications.
Our study was performed in a high-volume tertiary implant centre with 24-hour cardiologist resident on-call (specialty trainee or consultant). This potentially facilitates evening and weekend discharges, which may be difficult to achieve in smaller centres with a non-specialised on-call service.
There was concern among operators that same-day discharge of CRT recipients would fail to identify those with left-ventricular lead micro-displacement causing diaphragmatic twitch in the 12 hours post-implant. Previously, this was detected at the next-day interrogation. We have seen that, even with biventricular devices, same-day discharge is safe, as no patients required device reprogramming for twitch in the six-week period post-device. We accept that this is a small group (n=14) and further work in this area is required.
The reduction in excess bed-days has the potential for significant cost-saving. Moreover, in the UK, day-case surgical procedures are rewarded by commissioning groups with Best Practise Tariffs (BPTs). BPTs do not currently incentivise same-day discharge for cardiac pacing procedures, but this could change in the future.
Limitations
Our same-day discharge rate, even in the ‘same-day’ cohort was low. This may reflect operator caution, particularly in patients in whom the risk of complications was perceived to be greater, which may have biased our results. Nevertheless, we have shown that taking a cautious approach results in low rates of complications in patients discharged the same day.
Our duration of follow-up was limited, however, any difference in complication or readmission rates would be evident within 90 days. Some patients may have been readmitted to neighbouring centres, but with the close links with our secondary care centres, it is unlikely our unit would not have been notified of the readmission. Furthermore, this would have been constant for both cohorts studied.
Conclusion
Same-day discharge for patients attending for pacemaker insertion resulted in a reduction in length of hospital stay and does not compromise patient safety. This may have significant cost-saving implications for institutions. Same-day discharge was more likely following a morning implant. We took a pragmatic approach with a low threshold for overnight stay in patients considered to be at risk of complications. Our findings also applied to individuals with clinical heart failure and CRT devices, though our sample size was small and more work is required in this
regard.
Author contributions
Study design and manuscript preparation: NK, TN. Data collection: TN, AB, JL, RB, PS, JS, NK. Analysis and statistics: TN, AB, NK. Critique: TN, AB, JL, RB, PS, JS, NK.
Conflict of interest
None declared.
Key messages
A same-day discharge policy for device implantation is safe in a real-world setting
Patients receiving implantable cardioverter-defibrillator (ICD) and cardiac resynchronisation therapy (CRT) devices can also be safely discharged on the day of their procedure
2. Osman F, Krishnamoorthy S, Nadir A, Mullin P, Morley-Davies A, Creamer J. Safety and cost-effectiveness of same day permanent pacemaker implantation. Am J Cardiol 2010;106:383–5. http://dx.doi.org/10.1016/j.amjcard.2010.03.038
3. Fanourgiakis J, Simantirakis E, Maniadakis N et al. Cost-of-illness study of patients subjected to cardiac rhythm management devices implantation: results from a single tertiary centre. Europace 2013;15:366–75. http://dx.doi.org/10.1093/europace/eus363
4. Todd D, Bongiorni MG, Hernandez-Madrid A, Dagres N, Sciaraffia E, Blomström-Lundqvist C. Standards for device implantation and follow-up: personnel, equipment, and facilities. Results of the European Heart Rhythm Association Survey. Europace 2014;16:1236–9. http://dx.doi.org/10.1093/europace/euu209
7. National Institute for Health and Care Excellence. Implantable cardioverter defibrillators for arrhythmias. TA95. London: NICE, January 2006. Available from: https://www.nice.org.uk/guidance/ta95 [cited 3 January 2015].
8. National Institute for Health and Care Excellence. Cardiac resynchronisation therapy for the treatment of heart failure. TA120. London: NICE, May 2007. Available from: http://www.nice.org.uk/guidance/ta120 [cited 3 January 2015].
9. National Institute for Health and Care Excellence. Implantable cardioverter defibrillators and cardiac resynchronisation therapy for arrhythmias and heart failure. TA314. London: NICE, June 2014. Available from: http://www.nice.org.uk/guidance/ta314/chapter/1-guidance [cited 3 January 2015].
10. Brignole M, Auricchio A, Baron-Esquivias G et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2013;34:2281–329. http://dx.doi.org/10.1093/eurheartj/eht150
12. Edwards N, Varma M, Pitcher D. Routine chest radiography after permanent pacemaker implantation: is it necessary? J Postgrad Med 2005;51:92–7. Available from: http://www.jpgmonline.com/text.asp?2005/51/2/92/16369
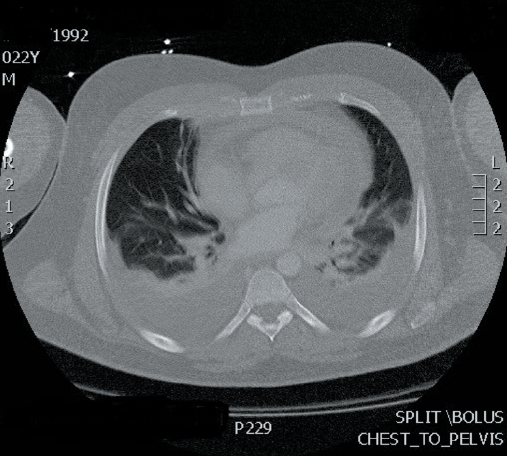
A 22-year-old man was admitted to a general district hospital with a three-day history of epigastric pain and shoulder discomfort. He reported shortness of breath on exertion, but denied any chest pain or flu-like symptoms. He had no past medical history of note. Vital signs assessment confirmed low blood pressure of 90 mmHg systolic, and tachycardia of 130 beats per minute. Physical examination of the abdomen revealed mild epigastric tenderness. A computerised tomography (CT) scan for suspected cholecystitis showed a normal gall bladder, but revealed a large rim of pericardial effusion measuring 2.8 cm. He was then urgently transferred to a tertiary cardiac centre for assessment and consideration of pericardiocentesis.
On admission to the tertiary centre, he had evidence of pulsus paradoxus, raised jugular venous pressure, and muffled heart sounds, but no murmurs. Subsequently, he underwent pericardiocentesis, which drained 600 ml of turbid straw-coloured fluid with immediate improvement in the haemodynamic status.
The patient was commenced on regular colchicine and ibuprofen. The initial blood tests showed raised inflammatory markers. The biochemical, microbiological and histopathological analysis of the pericardial fluid was normal, including viral serology and tuberculosis studies. The patient improved clinically and biochemically over a few days. He then self-discharged, against medical advice. Three weeks later he presented to the hospital with progressive breathlessness and shoulder pain. Biochemical tests showed raised inflammatory markers. Cardiac imaging showed a severely thickened pericardium with a 1.0 cm rim of pericardial effusion with bilateral moderate pleural effusions (figure 1). Monitoring his vital signs showed intermittent fever. With an appropriate work-up for suspected sepsis, he was commenced on intravenous piperacillin–tazobactam 4.5 g eight hourly, empirically. Despite antibiotic therapy, he remained symptomatic with no clinical improvement, and his blood and pleural fluid cultures were all negative. On review by the rheumatology team, he had no symptoms or signs to suggest a systemic rheumatological condition. The autoimmune profile was repeated and remained negative. A whole body CT scan did not show any inflammatory process elsewhere. A diagnosis of idiopathic effusive constrictive pericarditis was made.
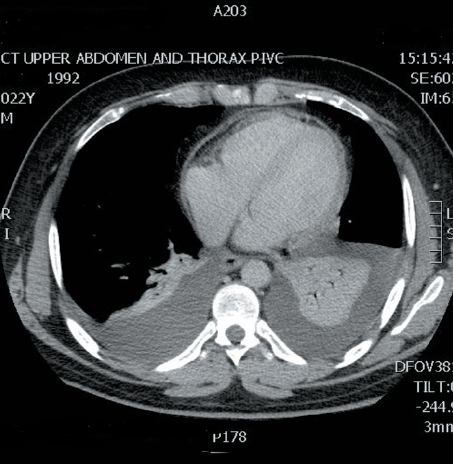
Figure 2. CT scan showing significant reduction of the pericardial thickening
A multi-disciplinary team (MDT) meeting recommendation suggested commencing steroids to cover a possible non-infective inflammatory pericardial disease. The patient was started on 0.5 mg/kg/day prednisolone and made a good recovery, both clinically and biochemically over 48 hours. The repeated cardiac imaging after a week of steroids showed significant reduction in the pericardial thickness (figure 2). He was then discharged on a slow tapering dose of steroids, with a plan of an outpatient review in four-weeks’ time, which he failed to attend. Unfortunately, the patient was re-admitted again with shoulder pain and an ongoing breathlessness. The echocardiogram, on this occasion, showed recurrence of the pericardial thickening and new areas of calcification. Despite clinical improvement with steroids and supportive care, the pericardial thickening persisted. The patient was discharged on a tapering dose of steroids.
Discussion
Idiopathic effusive-constrictive pericarditis is an uncommon pericardial syndrome1 that is often challenging, especially when it is recurrent. This young man had three admissions with symptomatic effusive pericarditis. His symptoms were generally atypical and non-specific. On the first presentation, the clinical assessment was suggestive of cholecystitis. On subsequent admissions, he presented with shoulder discomfort and breathlessness without chest pain. The systemic inflammatory response was generally severe, with extreme tachycardia, tachypnoea, pyrexia and raised inflammatory markers on biochemical laboratory tests. The presentation was similar to sepsis almost every time he was admitted to hospital. The initial response to steroids in the second admission was associated with significant reduction in the pericardial thickening radiologically. However, on the third flare-up, the patient had evidence of recurrence of the pericardial thickening on admission despite being asymptomatic between the two admissions. The investigations done to identify the aetiology of this recurrent pericarditis failed to uncover any potential cause, including viral and rheumatological conditions. Although there were no features of constriction on the last admission, the persistence of the pericardial thickening and the multiple foci of calcifications may predict significant constriction should pericarditis recur again. In this otherwise healthy man, the need for pericardiectomy might be unavoidable at some stage.2
While the majority of patients have a significant improvement in symptoms following pericardiectomy, there is a significant peri-operative morbidity and mortality related to the complex nature of surgery. This is because the removal of the thickened and inflamed pericardium is technically challenging.3,4 Long-term survival after pericardiectomy is inferior to that of an age- and sex-matched population.3,5 In one series, the five- and 10-year survival rates were 78% and 57%, respectively.5 In two other case series, the five-year survival rates after surgery for patients with idiopathic constrictive pericarditis were 80% and 81%.6,7
Conflict of interest
None declared.
Key messages
The presentation of acute pericarditis can sometimes be atypical and needs a high index of suspicion
Severe systemic inflammatory response of pericarditis can mimic sepsis and may delay the initiation of steroids in recurrent presentations
The management of recurrent pericarditis remains a true challenge, and close follow-up is always needed
The decision to take the surgical option in constrictive pericarditis can be difficult in the young population
References
1. Sagrista-Sauleda J, Angel J, Sanchez A et al. Effusive-constrictive pericarditis. N Engl J Med 2004;350:469–75. http://dx.doi.org/10.1056/NEJMoa035630
3. Bertog SC, Thambidorai SK, Parakh K et al. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol 2004;43:1445. http://dx.doi.org/10.1016/j.jacc.2003.11.048
4. Chowdhury UK, Subramaniam GK, Kumar AS et al. Pericardiectomy for constrictive pericarditis: a clinical, echocardiographic, and hemodynamic evaluation of two surgical techniques. Ann Thorac Surg 2006;81:522. http://dx.doi.org/10.1016/j.athoracsur.2005.08.009
5. Ling LH, Oh JK, Schaff HV et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation 1999;100:1380. http://dx.doi.org/10.1161/01.CIR.100.13.1380
6. George TJ, Arnaoutakis GJ, Beaty CA et al. Contemporary etiologies, risk factors, and outcomes after pericardiectomy. Ann Thorac Surg 2012;94:445. http://dx.doi.org/10.1016/j.athoracsur.2012.03.079
7. Szabó G, Schmack B, Bulut C et al. Constrictive pericarditis: risks, aetiologies and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg 2013;44:1023. http://dx.doi.org/10.1093/ejcts/ezt138
A new portable monitoring device (CardioMessenger Smart, Biotronik) has been launched in the USA. Roughly the size of a smartphone, the device keeps pacemaker, implantable cardioverter defibrillator, and insertable cardiac monitor patients connected to their physician remotely.
The device automatically transmits daily reports of cardiac activity via worldwide cellular networks to physicians without intervention from the patient. It also provides fully customisable alerts that can be programmed to the physician’s specifications. Studies have found that home monitoring can significantly reduce hospitalisation, stroke and mortality.
The manufacturers claim the device’s portability will help to ensure patient compliance, and that the consistent transmission of data will enable physicians to identify and prevent potential cardiac events.
One hour of activity could offset health risk of eight hours of sitting
A new study of over one million people finds that doing at least one hour of physical activity per day, such as brisk walking or cycling for pleasure, may eliminate the increased risk of death associated with sitting for eight hours a day.
In the first paper in the series, researchers analysed data from 16 studies. The research team wanted to see how many hours of daily physical activity would be required to eliminate the association between prolonged sitting time and increased risk of death. They found people who sat for eight hours a day but were physically active had a much lower risk of death compared to people who sat for fewer hours a day, but were not physically active. Examples of physical activity were brisk walking at 5.6 km/h or cycling for pleasure at 16 km/h.
Other authors of papers in the series warn there has been too little progress in tackling the global pandemic of physical inactivity since the 2012 Olympics, with a quarter of adults worldwide still failing to meet current recommendations on physical activity. Physical inactivity costs the global economy US$ 67.5 billion.
ATMOSPHERE shows no benefit of aliskiren in heart failure
A subgroup analysis in heart failure patients with diabetes from ATMOSPHERE (the Aliskiren Trial to Minimize OutcomeS in Patients with HEart failure) has failed to show benefit and may signal the end of the road for aliskiren in heart failure. The findings were presented for the first time in a late-breaking trial session at Heart Failure 2016 and the 3rd World Congress on Acute Heart Failure, Florence, Italy.
Following the results of two separate trials – ALTITUDE (The Aliskiren Trial in Type 2 Diabetes Using Cardiorenal Endpoints) and ASTRONAUT (The Aliskiren Trial on Acute Heart Failure Outcomes) – the European Medicines Agency (EMA) requested the withdrawal of all patients with diabetes from ATMOSPHERE. ALTITUDE had been stopped after patients with diabetes and a high risk of cardiovascular events were found to have an excess risk of cardiovascular and renal events with aliskiren, while ASTRONAUT had found a tendency towards harm in patients with diabetes.
“This was a subgroup analysis with the inherent limitations of this type of study. It failed to show superiority or non-inferiority of aliskiren over the angiotensin-converting enzyme inhibitor enalapril in heart failure patients with diabetes,” said principal investigator Professor Lars Kober (Rigshospitalet, Copenhagen University Hospital, Denmark).
Exercise associated with longer life in patients with heart failure
Exercise is associated with a longer life in patients with heart failure, regardless of heart failure severity, age and gender, according to a recent analysis of more than 4,000 patients.
An international research group, ExTraMATCH II (Exercise Training Meta-Analysis of Trials in Heart Failure), identified 23 randomised trials of exercise that included at least 50 heart failure patients who were followed up for six months or longer. After asking the authors of all 23 studies for individual patient data, they received the information from 20 trials.
The investigators found that exercise was associated with an 18% lower risk of all-cause mortality and an 11% reduced risk of hospitalisation compared with no exercise. Lead author Professor Rod Taylor (Exeter Clinical Trials Unit, University of Exeter Medical School, Exeter) said: “This is about increasing one’s routine physical activity – for example walking for 20 to 30 minutes three times at week at an intensity that makes you feel a little bit breathless but not necessarily symptomatic”.
Twice as many stroke patients have correct diagnosis with thumb-ECG
In a recently completed project at Queen Alexandra Hospital in Portsmouth, twice as many stroke patients received the correct atrial fibrillation (AF) diagnosis with thumb-ECG (Zenicor) compared to current standard of care. The aim of the project was to develop and improve the diagnosis of AF for stroke patients in Portsmouth and to prevent recurrent strokes. The study was presented recently at the European Stroke Organisation Conference, Venice, Italy.
The thumb-ECG device has been used at Queen Alexandra Hospital in Portsmouth by 70 stroke patients over six months. The patients were investigated with thumb-ECG for three weeks in combination with continuous 24 hours Holter-ECG. With thumb-ECG, 14% of the patients were diagnosed with AF but only 7% were detected with the Holter ECG. The results are consistent with previous research from Sweden, where 7–11% of AF has been diagnosed with thumb-ECG and 1.5–4% with Holter-ECG.
Project lead Dr Ugnius Sukys (Queen Alexandra Hospital, Portsmouth) said: “We could repeat the results from the Swedish studies, and the investigation with Zenicor thumb-ECG even proved to be more effective in the Portsmouth population of stroke patients. We detected AF in a number of patients who would have been missed otherwise, and could therefore provide a better treatment for our stroke patients”.
Flu jab associated with fewer hospitalisations in heart failure…
The flu jab is associated with a reduced risk of hospitalisation in patients with heart failure, according to research presented recently at Heart Failure 2016 and the 3rd World Congress on Acute Heart Failure, Florence, Italy. The study in about 60,000 patients ends the controversy over flu vaccination in heart failure patients and provides more robust evidence for current recommendations, say the authors.
Primary care and hospital records of 4.9 million adults from the UK Department of Health’s Clinical Practice Research Datalink 1990–2013 were used to assess the impact of flu vaccination on the risk of cause-specific hospitalisation in heart failure patients. The risk of hospitalisation for cardiovascular disease, respiratory disease, and all causes was compared between a year in which a patient was vaccinated and an adjacent year when they were not, excluding the peri-vaccination period to minimise the risk of confounding.
Flu vaccination was associated with a 30% lower risk of hospitalisation for cardiovascular diseases, 16% lower risk of hospitalisation due to respiratory infections, and 4% lower risk of all-cause hospitalisation in the period 31 to 300 days after vaccination, compared with the corresponding period in an adjacent vaccination-free year.
Professor Kazem Rahimi (The George Institute for Global Health, University of Oxford) said while we cannot entirely rule out the possibility of residual confounding, “the findings do provide further evidence that there are likely worthwhile benefits and on that basis more efforts are needed to ensure that heart failure patients receive an annual flu jab”.
…and linked to lower dementia risk
Flu vaccination is associated with a lower risk of dementia in patients with heart failure, according to a recent study of more than 20,000 patients.
Authors led by Dr Ju-Chi Liu, (Taipei Medical University, New Taipei City, Taiwan) investigated whether heart failure patients who had received the flu vaccine had a lower risk of dementia. The study included all patients over 60 years of age who visited healthcare facilities in Taiwan with a diagnosis of heart failure during 2000–2012. Those who had dementia prior to being diagnosed with heart failure were excluded from the study. Patients were recruited from the National Health Insurance Research Dataset, which holds information on 98% of Taiwan residents.
When they examined the association by age, the researchers found that vaccinated heart failure patients had a 44% lower risk of dementia if they were over 70 years old and a 26% lower risk if they were between 60 and 69 years old. Vaccinated male heart failure patients had a 40% lower risk of dementia while vaccinated female heart failure patients had a 31% lower dementia risk.
Heart failure hospital visits rise 36% in decade
The number of heart failure hospital visits has increased by more than a third in the last 10 years as more people are diagnosed with the condition, according to latest statistics from the British Heart Foundation (BHF). Figures show the number of hospital visits by heart failure patients increased by 36% from 107,000 to 146,000 between 2004–2005 and 2014– 2015.
The BHF warns that more research is urgently needed to reduce the number of people with heart failure and improve treatments to halt the alarming increase in hospital visits. It says this rapidly rising trend in hospital visits is down to the ageing population and improving myocardial infarction (MI) survival rates.
Male GPs more likely to consider heart disease a “man’s issue”
Male GPs are more likely to consider heart disease a “man’s issue” and neglect to assess cardiovascular risk in female patients, reports a study of 52 GPs and more than 2,200 patients.
The study (Eur J Prevent Cardiol doi: 10.1177/2047487316648476) included 52 GPs and 2,262 patients who completed a questionnaire about their personal characteristics. For GPs this included age, gender, and office hours, while for patients there were questions about educational level and medical insurance. Medical files were used to obtain data on patients’ gender, age, history of diabetes, and standard cardiovascular risk factors.
The investigators found that information on smoking, blood glucose and cholesterol were reported less often in the files of female patients. Because of insufficient information in the medical files, both cardiovascular risk scales could be assessed less frequently in female than in male patients (36% less often for the French scale and 37% less often for the SCORE scale).
Lead author Dr Raphaëlle Delpech (Paris XI University and INSERM U1018, Paris, France) said: “I think most GPs will be surprised by our findings, and I hope this will help them ensure they assess cardiovascular risk equally in their male and female patients”.
Action required to minimise heart failure in breast cancer survivors
Despite the known toxic effects of chemotherapy on the heart, the majority of women undergoing breast cancer treatment are not getting the recommended follow-up heart scans, according to research presented at the British Cardiovascular Society (BCS) Conference in Manchester recently (abstract available at http://www.bcs.com/abstracts3/marker_view.asp?AbstractID=1913).
Researchers analysed medical records from the CHEMOCARE database focusing on the 1,229 breast cancer patients who were treated with either anthracyclines alone or combined with the monoclonal antibody trastuzumab at Ninewells Hospital, Dundee between January 2003 and December 2014.
Despite clear guidelines that women receiving these treatments should have their heart function monitored, only 625 (51%) of the women underwent an echocardiogram before starting chemotherapy. Of these, only 238 (38% of those screened) had follow-up scans during the course of their treatment, as recommended by the guidelines. Although the researchers expect their findings to be representative of cancer treatment across Scotland and the wider UK, broader analysis is needed to confirm this.
Three-year telehealth study builds case for supported self-care
The results from a large, self-care programme in Liverpool among 1,808 people living with long-term conditions (LTCs), including diabetes, heart failure and chronic obstructive pulmonary disease has highlighted clear benefits among study participants.
Reductions in emergency admissions and secondary care costs ranging from 22% to 32% for patients with above average risk (25% or more) were seen and patient-reported outcomes suggested that 90% felt more in control of their condition, had gained confidence, and/or felt better able to cope.
The study sought to improve patient independence and emotional well-being using innovative telemonitoring equipment alongside the support of a clinical hub and structured programme of case management, monitoring, education and coaching for populations living with varying levels of LTCs.
The programme results have been published by Royal Philips, working in partnership with the NHS Liverpool Clinical Commissioning Group (CCG) in Evidence for Supported Self Care.
“The results from this telehealth program are really game changing,” said Dr Simon Bowers (Digital Care and Innovation Clinical Director, NHS Liverpool Clinical Commissioning Group). “This is good for the NHS, but more importantly it’s good for the individual patients, who are being empowered to take control of their health and having the opportunity of a better quality of life as a result.”
Virtual reality and treadmill training could help prevent falls in elderly
Combining virtual reality and treadmill training helps prevent falls in older adults better than treadmill training alone, according to a new randomised controlled trial published in The Lancet (doi: 10.1016/S0140-6736(16)31325-3). The authors from the Tel Aviv Medical Centre, Israel, say that the intervention, which combines the physical and cognitive aspects of walking, could potentially be used in gyms, rehabilitation centres or nursing homes to improve safe walking and prevent falls in older adults or people with disorders which affect movement such as Parkinson’s disease.
Data were analysed from 282 participants from five clinical sites in Belgium, Israel, Italy, the Netherlands, and the UK (University of Newcastle) between 2013 and 2015. Participants were assigned to treadmill training with virtual reality (146), or treadmill training alone (136). The virtual reality component consisted of a camera that captured the movement of participants’ feet and projected it onto a screen in front of the treadmill, so that participants could ‘see’ their feet walking on the screen in real time.
The game-like simulation was designed to reduce the risk of falls in older adults by including real life challenges such as avoiding and stepping over obstacles like puddles or hurdles, and navigating pathways. On average, participants in each group took part in 16 training sessions over six weeks, with each session lasting about 45 minutes.
During the six months after training, the incidence rate of falls decreased in both groups, but the decrease was only statistically significant in the treadmill plus virtual reality group (11.9 to 6.0 falls in the virtual reality group – a 42% reduction; compared to a decrease from 10.7 to 8.3 in the treadmill only group).
NICE draft guidance recommends ticagrelor
The National Institute for Health and Care Excellence (NICE) has published draft guidance recommending anti-clotting drug ticagrelor 60 mg (Brilique®, AstraZeneca) with aspirin for people who have had a myocardial infarction (MI).
A higher dose of ticagrelor is already recommended for 12 months post- MI. Now new draft guidance is recommending it is continued in these people at a lower dose for a further three years to reduce their risk of a further MI or stroke.
This draft guidance looks at the use of ticagrelor at a lower dose beyond the initial 12-month period as a continuation of their previous ticagrelor treatment. It recommends ticagrelor 60 mg, which costs about £1 per tablet, with aspirin, taken twice a day for up to three years for people who have had an MI at least 12 months ago and who remain at high risk of having a further MI or stroke. The draft guidance states there should no interruption between treating at the higher 90 mg dose and the lower 60 mg dose.
SMC recommends alirocumab in patients at high-risk for MI and stroke
The Scottish Medicines Consortium (SMC) has recommended alirocumab (Praluent ®, Sanofi) as a treatment option for people who are at high risk of a myocardial infarction (MI) or stroke and who have raised levels of low-density lipoprotein (LDL) cholesterol and are unable to reach target levels despite modifying their diet and taking the maximum tolerated dose of a statin and/or other lipid-lowering therapies.
Sacubitril/valsartan (Entresto™, Novartis), the first angiotensin receptor blocker (ARB) and neprilysin inhibitor (NEP) combination – known as an angiotensin-receptor-neprilysin inhibitor (ARNI) – has recently been approved by the National Institute for Health and Care Excellence (NICE) in the treatment of patients with chronic heart failure.1 The guidance, largely based on results from the landmark PARADIGM- HF study,2 recommends sacubitril/valsartan as an “option” for symptomatic patients (New York Heart Association [NYHA] class II– IV) who have an ejection fraction of 35% or less and are established on a “stable dose” of an angiotensin-converting enzyme (ACE) inhibitor or ARB (it is unclear in the guidance whether or not optimisation is implied). Although NICE do recommend that treatment should be initiated by a heart failure specialist, there are no other caveats to widespread prescription. The implication from the guidance is that the majority of patients with heart failure associated with reduced ejection fraction (HFREF) are potential candidates for treatment and sacubitril/valsartan has been widely acclaimed and indeed marketed as “a breakthrough in heart failure”.
The question now is whether the size of the breakthrough is sufficient to justify a wholescale change in clinical practice or whether a more cautious approach should be adopted initially. Widespread adoption of the new therapy would potentially lead to the abandonment of the current ACE inhibitor-based treatment pathway in which ARBs are generally considered second line to ACE inhibitors. Instead, it would be replaced by one with an ARB (valsartan) at its core.
The key to answering this question lies with the PARADIGM-HF data and specifically its extrapolation to the wider UK heart failure population. The headline results are undoubtedly impressive and widely publicised. As in any trial, however, there are caveats, most of which have been taken into consideration during the NICE appraisal process.1 For example, the mean age at study entry was just 64 years, over a decade younger than the UK National Heart Failure Audit (NHFA) population.3 Only 21% were female (versus 44% in NHFA). More importantly, the study population appears to have been relatively well and likely to have been in the early stages of heart failure (72% NYHA class II, median brain natriuretic peptide [BNP] 255 pg/ml, 7% receiving cardiac resynchronisation therapy) with a mortality of less than 10% at one-year post-randomisation. Moreover, just 80% were receiving diuretics at randomisation, which is a potentially important confounder given the likely natriuretic effect of sacubitril-induced BNP enhancement. It is plausible, for instance, that the diuretic effect of sacubitril contributed significantly to the observed reduction in hospitalisation for heart failure, and that this effect may be attenuated in a less diuretic naïve population.
Dose equivalence
There is also the issue of dose equivalence. Unusually, PARADIGM-HF tested sacubitril/valsartan directly against another active and proven treatment (the ACE inhibitor, enalapril). The usual format for heart failure trials has been to compare the study drug with placebo as an addition to standard optimised therapy. Use of a combination drug (sacubitril/valsartan) further adds to the complexity. The design rationale is presumably accounted for by the difficulties of combining sacubitril with an ACE inhibitor (high risk of angioedema) and the hitherto disappointing performance of BNP-enhancing therapies used as single agents.4 The doses of valsartan and enalapril chosen for each arm of the study were considered to be broadly equivalent. Any disparity, however, is likely to have impacted on outcome and it is difficult to exclude the possibility that the trial was essentially one between an ACE inhibitor and an ARB at non-equivalent dosage. Furthermore, in the UK at least, ramipril (up-titrated to 10 mg daily) is the usual ACE inhibitor of choice.
More fundamental is the apparent paradox of a pharmacotherapy (i.e. neprilysin inhibition) designed to enhance the levels of a peptide (BNP), which rises naturally with disease progression and is associated negatively with prognosis. In contrast, other heart failure therapies are essentially system inhibiting rather than system enhancing. The paradox is, of course, easily explained. Unlike sympathetic and renin-angiotensin activation, BNP promotes natriuresis and, alongside its related peptides, has a number of complex but ultimately beneficial actions. However, it does raise the question as to whether or not the benefit of neprilysin inhibition may be attenuated in the more advanced stages of heart failure where BNP levels are already raised through natural production (a subgroup analysis of the PARADIGM-HF data does lend some support to this notion with a trend towards greatest benefit in patients with lower pre-treatment levels of BNP).
Sacubitril/valsartan is an exciting and novel addition to the heart failure treatment arsenal which, with NICE approval, is now available for widespread prescription. Heart failure guidelines will require major revision to accommodate the new therapy but it remains to be seen where sacubitril/valsartan sits in the overall treatment pathway. There may be a rationale for its use in targeting younger patients in the relatively early stages of heart failure in the hope of slowing disease progression. Its effectiveness in older patients with more disordered physiology requiring high-dose diuretics may be more questionable. Finally, it would seem premature to totally abandon ACE inhibition.
Conflict of interest
None declared.
Robert Stevenson Consultant Cardiologist Calderdale and Huddersfield NHS Trust, Huddersfield Royal Infirmary, Lindley, Huddersfield, HD3 3EA ([email protected])
References
1. National Institute for Health and Care Excellence (NICE). Technology appraisal guidance (TA388). Sacubitril valsartan for treating symptomatic chronic heart failure with reduced ejection fraction. London: NICE, 27 April 2016. Available from: http://www.nice.org.uk/guidance/ta388 (accessed 09 August 2016)
2. McMurray JJ, Packer M, Desai AS et al.; for the PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure (PARADIGM-HF). N Engl J Med 2014;371:993–1004. http://dx.doi. org/10.1056/NEJMoa1409077
3. National Institute for Cardiovascular Outcomes Research (NICOR) and British Society for Heart Failure. National Heart Failure Audit April 2013–March 2014 (published 20 October 2015). http://www.ucl.ac.uk/nicor/audits/heartfailure/reports
4. O’Conner CM, Starling RC, Hernandez AF et al. Effect of nesiritide in patients with acute decompensated heart failure. N Engl J Med 2011;365:32–43. http://dx.doi. org/10.1056/NEJMoa1100171
Sponsorship Statement: Actelion have funded the production of this article but have had no input into content
In this report we review two major American meetings: the 36th Annual Meeting and Scientific Sessions of the International Society for Heart and Lung Transplantation (ISHLT), held in Washington DC, USA, from 27th–30th April 2016; and the Annual Meeting of the American Thoracic Society (ATS), held in San Francisco, USA, from 13th–18th May 2016.
ISHLT overview: advances in transplantation
Presenters shared the importance of increasing the source of hearts for transplantation through donation after cardiac death (DCD). “The lack of suitable donor hearts for transplantation has severely limited access to this life saving therapy for patients with advanced heart failure,” said Andrew Fisher (Professor of Respiratory Transplant Medicine, University of Newcastle). “The ability to safely perform DCD heart transplant together with improved overall management of potential heart donors represents a substantial step forward in addressing this clinical challenge,” he concluded.
40% increase in transplant activity
A study presented by Dr Simon Messer (Papworth NHS Trust Hospital, Cambridge) sought to discover if DCD hearts could help to increase the donor pool. Normothermic regional perfusion (NRP) was utilised to restore function to the DCD heart to allow robust assessment of heart function prior to proceeding to clinical transplantation (pictured). Over the last year, 10 patients were successfully transplanted thanks to this pioneering technique with 100% survival and a median five day intensive care stay.
Heart from the donor is removed after it stops beating and, depending on the transplant centre protocol, is reactivated and monitored for about 50 minutes before it is approved for transplantation. The restarted heart is then supplied with blood and nutrition in an “organ care system” (OCS™ Heart), for as long as needed to monitor and improve the state of the organ until it is transplanted. Supplying blood and nutrients inside the heart in the Organ Care System helps reduce the damage caused to the cardiac muscle compared with the traditional way of storing it in an ice box. The OCS™ Heart System is manufactured by TransMedics, Inc. in the United States. Each unit reportedly costs approximately £150,000 plus £25,000 per patient transplanted. (Photo courtesy of TransMedics, Inc.)
Their proficiency with NRP has allowed practitioners to safely redefine the limits of DCD heart transplantation. Using both NRP and direct procurement, they have established a successful programme with 19 successful DCD heart transplants to date. This has resulted in an unprecedented 40% increase in their overall heart transplant activity. Their vision for the future is to share their expertise and replicate this programme for the global transplant community.
USA and European management consensus
Dr Kiran Khush (Stanford University, California, USA) discussed the standardisation of donor selection for heart transplantation. Altogether at the Consensus Conference, over 95 participants including cardiologists, cardiac surgeons, and transplant coordinators from over 40 transplant centres, participated in the discussion. A primary observation of the group was that donor heart management and selection criteria varied greatly across centres. Additionally, they prioritised the most important risk factors in donor selection, which included older age, left ventricular function, and distance from transplant centres.
A highlight of the European Consensus meeting was discussion of DCD and organ preservation (heart and lung) focused on how to select the candidates and manage end-of- life care, ex vivo preservation strategies, and the potential for ex vivo resuscitation of the organs.
ATS overview: higher rates of vitamin D deficiency…
All pulmonary hypertension (PH) patients should be screened for vitamin D deficiency, according to a study presented by Dr Basheer Tash and colleagues (Cleveland Clinic, Florida, USA). Vitamin D is known to have a protective immunomodulatory and antiproliferative effect on vascular smooth muscle. The retrospective study found a 22% prevalence of vitamin D deficiency among a group of 77 PH patients (mean age 63 years) who had levels measured within one month of their diagnostic right heart catheterisation (RHC).
The prevalence of sub-optimal (insufficient and deficient) levels was 53%. The deficiency rates are significantly higher compared to other USA national survey datasets and they appear to serve as a consistent marker of a significantly higher mean pulmonary artery pressure (PAP). But the authors suggest that larger prospective studies are needed to verify the prognostic implications of vitamin D deficiency in PH and the effect of replacement therapy on disease outcomes.
…and schizophrenia associated with pulmonary hypertension
Chronic thromboembolic pulmonary hypertension (CTEPH) is characterised by persistent thromboemboli in the pulmonary arteries, which cause pulmonary hypertension and resultant right heart failure and death. CTEPH has been reported to develop in approximately 2–4% of patients with acute pulmonary embolism (PE), suggesting a common pathophysiology between the two disorders. Several common risk factors for CTEPH and PE have been demonstrated, such as certain medical therapies, thrombophilia and a genetic predisposition. However, little is known about the possible association between CTEPH and schizophrenia, although the association between PE and schizophrenia has been suggested. Now a team from Tohoku University, Sendai, Japan, have reported a significantly higher prevalence of schizophrenia in CTEPH patients compared with those with pulmonary arterial hypertension (PAH) and the general population.
The prevalence of schizophrenia was 8/110 (7.3%) in CTEPH, 1/150 (0.7%) in PAH and 795,000/127,692,000 (0.6%) in the general population, respectively, and thus was significantly higher in CTEPH patients compared with the other two groups (both P<0.01). The Japanese workers propose two possible mechanisms involved in the increase of schizophrenia in CTEPH. First, CTEPH may be directly induced by activation of blood coagulation and enhanced blood clotting in schizophrenia. Second, such hypercoagulable states in schizophrenia may prevent thrombolysis and anticoagulation of PE with resultant development of CTEPH.
Right heart catheterisation safe in the elderly
RHC is the reference test in diagnosing PH. A study conducted by Dr Marylise Ginoux (Louis Pradel Hospital, Bron, France) questioned whether RHC is justified in very elderly patients. They retrospectively analysed 1,060 RHCs performed by a single operator over a four year period. 228 (21.5%) of the patients were >75 years and 832 (78.5%) were below 75 years. Nine procedures led to complications (0.9%) three in >75 year olds and six (0.7%) in those younger. Eight were related to femoral vein puncture; “which should be avoided whenever possible,” the authors suggest. Some 24 procedures (2.3%) could have been obviated as results did not influence management. The authors conclude however that RHC can be performed regardless of age, and complication rate is not increased in older patients.
‘Breath signature’ for PAH
In PAH and other diseases, cells/tissues produce a spectrum of volatile organic compounds (VOCs) that diffuse, eventually, from blood to exhaled breath. This way, the detection of exhaled VOCs could serve as a non-invasive diagnostic test, especially for respiratory diseases, due to their proximity to blood-air barrier. Dr Morad Nakhleh (Université Paris-Sud, France) and co-authors hypothesised that PAH-induced specific profiles of VOCs, (referred to as volatolomes) could serve for the non-invasive diagnosis of PAH.
Breath samples from 22 PAH patients, were compared to healthy controls as well as to over 1,380 samples obtained from patients diagnosed with 15 different diseases (including but not only, lung cancer, neurological disorders, inflammatory diseases, gastric cancer and others). They compared the breath composition of 22 PAH patients and 23 control subjects and discovered that the concentration of nine breath VOCs was significantly altered in association with PAH. The investigators then determined the collective PAH breath-signature, using the nano-arrays, discriminating PAH patients from controls with an accuracy of 92%. Based on the meta-analysis of 1,404 breath samples, they found that PAH-induced volatolome is unique and distinctive from the remaining 15 diseases with an accuracy of 86%, when blindly validated.
Targeting the prostacyclin pathway…
Despite available therapies, patients with connective tissue disease associated PAH (PAH-CTD) have a particularly poor prognosis. The global phase III GRIPHON (Prostacyclin [PGI2] Receptor Agonist In Pulmonary Arterial Hypertension) study investigated the use of the oral, selective IP receptor agonist, selexipag, which is pharmacologically distinct from prostanoids and which has recently become available for use in Europe. The study enrolled 1,156 PAH patients including 334 with PAH-CTD. Compared with placebo, selexipag significantly reduced the risk of the primary outcome composite of morbidity/mortality by 41% among patients with PAH-CTD.
Professor Sean Gaine (Mater Misericordiae Hospital, Dublin, Ireland) on behalf of the GRIPHON Investigators, presented findings on the effect of selexipag vs. placebo in patients with PAH associated with CTD subtypes, including systemic sclerosis (PAH-SSc), systemic lupus erythematous (PAH-SLE) and mixed CTD (PAH-MCTD).
Selexipag reduced the risk of morbidity/mortality events by 44% in PAH-SSc, by 34% in PAH-SLE, and by 53% in PAH-MCTD patients. The treatment effect was consistent across the PAH-CTD subgroups which suggests that targeting the prostacyclin pathway with selexipag is an effective therapeutic option in these difficult-to-treat patients, according to the investigators.
…and benefits of combination therapy
Combined targeted (CT) therapy is associated with a significant reduction in clinically relevant outcomes compared to monotherapy in PAH, according to a meta-analysis involving 4,095 patients.
The analysis was conducted by Dr Annie Lajoie, and co-investigators (Centre de Recherche de l’Institut Universitaire de Cardiologie et de Pneumologie de Québec, Quebec, Canada). The primary outcome in the trials was the risk of clinical worsening, and secondary outcomes included the components of the clinical worsening definition, functional class, exercise capacity and treatment discontinuation.
CT was associated with significant risk reduction for clinical worsening (P<0.00001), with treatment effect being consistent across subgroups. CT was also associated with a risk reduction for hospitalisation, treatment escalation and symptomatic progression. Moreover, all-cause (P=0.09) and PAH-related (P=0.06) mortality tended to be reduced by CT compared to monotherapy, whereas CT had no effect on lung transplantation. Finally, CT resulted in WHO functional class improvement and six-minute walked distance (+22.1 m; 95% CI 17.6–26.5 m; p<0.00001).
The coronary artery calcium (CAC) score is widely believed to be an important tool in determining the risk of developing heart disease. The measurement of this score has traditionally been based on using electrocardiography triggered computed tomography (CT). This confers an advantage over non-gated CT scanning by acquiring images during diastole, which reduces motion artefact and avoids missing areas of coronary artery calcification. Radiologists are, therefore, cautious when reporting CAC on non-gated CT scans due to concerns that it may not be accurate. This means that there is currently no obligation, from a radiology perspective, to report on the degree of CAC on non-gated CT scans. While this has been acceptable for a long time, emerging evidence may force us to change our practise.
Emerging evidence
In an issue of Circulation: Cardiovascular Imaging, Xie et al.1 performed a systematic review and meta-analysis to validate the prognostic importance of CAC scoring in non-triggered thoracic CT. The authors of this study performed a meta-analysis of five studies that compared CAC obtained using non-gated CT scans versus gated CT scans. This study demonstrated an excellent correlation between the two techniques with a pooled Cohen κ agreement being 0.89 (95% confidence interval [CI] 0.83–0.95). While this is promising, the authors have also highlighted some discrepancy between the two techniques, and this is important to note. Non-triggered CT scan will yield a false-negative calcium score in 8.8% of individuals and underestimated calcification in 19.1% of the individuals. Despite this difference, the authors recommend that we must not disregard CAC picked up using non-gated CT scans, and it must be reported like any other important incidental finding.
This is useful knowledge as it is well known that respiratory disease is an independent risk factor for developing heart disease. Therefore, patients coming in for lung cancer screening or follow-up for interstitial lung disease undergoing non-gated CT scanning must be screened for CAC. For example, preliminary data at our trust has revealed that 56% of patients who have undergone non-gated high-resolution CT (HRCT) scanning for follow-up of interstitial lung disease have severe CAC (CAC score >1,000). A significant proportion of these people are not on any secondary prevention medications either, despite having cardiovascular risk factors (hypertension, hyperlipidaemia and renal disease). A similar study by Jacobs et al.2 looking at adults referred for lung cancer screening corroborates our findings.
Another study (by Margolies et al.3) recently published in JACC: Cardiovascular Imaging has shown a link between breast arterial calcification (BAC) and CAC. This study included 325 women who underwent a non-gated CT scan and a digital mammogram within a year of the other. The degree of CAC and BAC was measured on a 12-point ordinal scale. Moderate CAC (≥4) was noted in 47.6% of women. The degree of BAC, based on the density of calcium in the lumen, number and length of vessels involved, was similarly scored on a 12-point ordinal scale: 42.5% of women had BAC, which was significantly associated with chronic kidney disease, high blood pressure and increasing age. More importantly, the authors report a highly significant agreement between BAC and CAC.
This is the first study of its kind to quantitatively link BAC and CAC. The authors of this paper hope that this study will encourage regular reporting of BAC in mammography reports as it will help identify women at risk of developing cardiovascular disease.
Conclusion
The emerging body of evidence that non-gated CT scanning may have a role in determining the degree of CAC compels us to consider how this can be applied to a clinical setting. We believe that there may be scope, for example, to mention the degree of CAC as a standard when reporting non-gated HRCT scans, positron emission tomography or single photon emission CT of the chest. This will allow us to risk-stratify patients and potentially refer them to cardiologists for further investigations, such as stress echocardiography. Moreover, patients can be commenced on medications, such as statins or aspirin, for primary prevention of cardiovascular disease. The images of calcified coronary arteries may potentially have a role in convincing people to make correct lifestyle choices.
It will take time for CAC scoring to fully penetrate the world of cardiology and radiology. There are questions that still remain unanswered and, ultimately, electrocardiogram (ECG)-gated CT scanning will remain the gold standard for picking up CAC. We are, however, fascinated by the findings reported by Xie et al.1 and Margolies et al.3 and hope that further studies will bring to light this novel topic.
We believe that a perceptual tool to quantify CAC should be developed. If such a tool can be validated against the standard quantitative method of using Agatston scores, then this will allow radiologists to very easily report the level of CAC within the limited time slot they have for reporting each scan. This may help to simplify a potentially cumbersome activity of measuring CAC using semi-quantitative tools, which will eventually mean that CAC score is more regularly incorporated in radiology reporting of non-gated CT scans.
Acknowledgements
We would like to acknowledge Dr Divya Raj and Dr David Zhu in the data collection process for the study conducted in our trust (unpublished data).
Conflict of interest
None declared.
References
1. Xie X, Zhao Y, de Bock GH et al. Validation and prognosis of coronary artery calcium scoring in non-triggered thoracic computed tomography: systematic review and meta-analysis. Circ Cardiovasc Imaging 2013;6:514–21. http://dx.doi.org/10.1161/CIRCIMAGING.113.000092
2. Jacobs PC, Gondrie MJ, van der Graaf Y et al. Coronary artery calcium can predict all-cause mortality and cardiovascular events on low-dose CT screening for lung cancer. AJR Am J Roentgenol 2012;198:505–11. http://dx.doi.org/10.2214/AJR.10.5577
3. Margolies L, Salvatore M, Hecht HS et al. Digital mammography and screening for coronary artery disease. JACC Cardiovasc Imaging 2016;9:350–60. http://dx.doi.org/10.1016/j.jcmg.2015.10.022
In 2012, the British Association for Cardiovascular Prevention and Rehabilitation (BACPR) published guidance on the standards and core components of cardiac rehabilitation (CR). However, annual reports from the UK National Audit of Cardiac Rehabilitation (NACR) have shown that, while there are examples of excellent practice in the UK, many CR programmes do not meet the BACPR standards. It is difficult for service managers, patients and commissioners to assess how a particular CR programme meets minimum standards of service delivery. These findings led the BACPR and NACR to work together to develop a UK National Certification Programme for CR that would be mainly based on assessment of quality-assured patient-level NACR data. The development of the certification process was built on surveys and interviews with CR service providers, patients and commissioners. Minimum standards for certification were developed by an expert group. The resulting process for certification of meeting minimum standards of CR service was then successfully pilot-tested with 16 CR programmes, of which 13 programmes have since met minimum certification standards. CR programmes that submit data to the NACR can now apply for assessment under the BACPR/NACR National Certification Programme.
Introduction
Table 1. The British Association for Cardiovascular Prevention and Rehabilitation (BACPR) standards for cardiac rehabilitation (CR)1
In 2012, the British Association for Cardiovascular Prevention and Rehabilitation (BACPR) published guidance for the service standards and core components (SCCs) for the delivery of cardiovascular rehabilitation (CR) in the UK (table 1).1,2 The SCCs were evidence based3-5 and set out seven core components (figure 1) that aimed to ensure delivery of a quality assured, high-standard CR programme.1
Publishing guidance on a set of national service standards is obviously important, however, measuring the level of adherence to guidance is even more important. This is best done through an independent audit on a national scale, which, until recently, was not really feasible. The British Heart Foundation (BHF) National Audit of Cardiac Rehabilitation (NACR) has now reached a point of quality reporting of CR programmes that is highlighting significant success, alongside significant shortfalls.
The majority of CR programmes in the UK (up to 90%) provide data to the NACR via either patient level data submitted to the online database (held within the Health and Social Care Information Centre), or via an annual survey of all CR programmes in the UK. The annual NACR reports detail the very large variability in service delivery across UK CR programmes, with many examples of suboptimal delivery, which has been the topic of much debate.6-8 For example, the National Institute for Health and Care Excellence (NICE) and BACPR recommend that CR should commence within 28 days of myocardial infarction (MI) and/or percutaneous coronary intervention (PCI),1,9 yet the UK median time for commencement of CR is 38 days, with large variability across the UK (from a swift seven days to a greatly delayed 69 days).10 Concerns have also been raised on other aspects of delivery of CR within the UK, which do not meet the standards recommended by BACPR, including omissions in undertaking pre- and post-CR assessment, and services delivering too small a ‘dose’ of CR by reducing length and frequency of programmes.10
Figure 1. The British Association for Cardiovascular Prevention and Rehabilitation (BACPR) seven core components of cardiovascular rehabilitation
The NACR reports highlight the gulf between the previously defined BACPR standards and actual service delivery, demonstrating that BACPR service standards are clearly aspirational for the majority of services in the UK.1,10 Additionally, it was difficult for CR commissioners, service managers, staff and patients to assess how a programme met minimum standards in order to ensure a reasonable quality of service. For example, BACPR recommends (standard 21) that CR should be delivered by a multi-disciplinary team drawn from any of 10 or more professions, but the minimum requirement to demonstrate this was not clear. These discussions led to the proposal to develop more realistic minimum criteria against which services could be benchmarked, and to use these criteria to develop and assess the feasibility of a certification scheme for CR. A certification scheme would:
Signal essential standards of care delivery in CR
Promote excellence and reward improvement in the delivery of CR
Encourage greater conformity of services across the countries within the UK
Provide information for patients (their caregivers and family) on the level of service they can expect from a CR programme
Provide commissioners with a badge of quality assurance for their local CR services.
Aims
Assess the acceptability of a potential certification scheme to service staff and patients, and its utility for service commissioners.
To develop minimum standards for the delivery of CR against which it would be possible to assess concordance.
To develop and pilot a certification scheme within the UK to assess its feasibility.
Design
The study was undertaken in three stages. Stage 1 assessed the acceptability of a UK certification scheme. This involved:
1a. A survey of CR service staff
1b. Consultation with a national patient group
1c. Interviews with a small number of service commissioners.
Stage 2 developed the minimum standards for certification from expert consensus. Stage 3 piloted the certification process.
Stage 1: assessment of acceptability of a certification of CR scheme
Procedure
1a. CR professionals
Following ethical approval via Coventry University ethics system, a survey was undertaken of BACPR members using both paper-based and online formats, covering topics such as:
attitude to a certification scheme
potential data sources for the scheme
options for the organisation of the scheme
frequency of certification/recertification
potential price of undertaking the scheme.
Questionnaire responses were a mix of multiple choice, Likert-scale, and open responses. The online questionnaire was made available via emails to BACPR members (~900) during summer 2013, and both formats were made available during the annual BACPR conference (attended by ~200 people) in October 2013. The survey was closed in late October 2013.
1b. Patients/carers
A face-to-face meeting with additional facility for teleconference was held in London in February 2014 between members of the project steering group and members of the UK Cardiovascular Care Partnership (CCP-UK), a patient group affiliated with the British Cardiovascular Society.
1c. Service commissioners
Face-to-face or telephone interviews were conducted with three service commissioners, giving them a description of the aims and possible format of the scheme for their comment.
Results stage 1
1a. CR professionals
Table 2. Survey respondent profile
Seventy-five completed questionnaires were received, and once duplicate submissions (using both paper and online versions) were removed, 72 questionnaires were analysed. More than half of the respondents were nurses (table 2), which will reflect the BACPR membership to some extent. Respondents were drawn from a range of different sized CR programmes.
The overwhelming majority (90%) of respondents agreed/strongly agreed that a certification scheme would improve the standard of CR services across the UK, but there were some qualifying statements (e.g. “So long as relevant and not a paper exercise”). Over 65% of respondents agreed/strongly agreed that the NACR database should be the main source of data to assess adherence to minimum standards. There were concerns that programmes that did not submit audit data to NACR (e.g. currently the whole of Scotland) would not be eligible for certification. The annual NACR survey was preferred by those programmes not submitting patient level data to NACR, but there were concerns that the survey information was too basic to achieve the level of detail required for a certification scheme.
1b. Patients/carers
The potential certification scheme for CR was discussed via email and in meetings of CCP-UK prior to a face-to-face meeting between the project steering group and CCP-UK representatives. Queries and comments were raised by CCP-UK members, including a major concern that many programmes do not include patient and public participation in the development, design and evaluation of CR programmes beyond patient satisfaction. Points raised by CCP-UK were included in the design of certification documentation to ensure that these details were captured.
1c. Commissioners
Three commissioners from different clinical commissioning groups in England were interviewed for their perspectives of a certification programme and the different options for data assessment. They raised queries regarding the honesty of the process if it relied on self-report (rather than on patient-level data taken from the NACR), and whether BACPR would be able to give an assurance regarding data quality (this is a strong aspect of using NACR as it is overseen by the Health and Social Care Information Centre). All three interviewees commented that they were interested in outcomes (such as drop-out rates) rather than the more subjective ‘patient satisfaction’. Two commissioners were supportive of the potential for the scheme to feed into the commissioning cycle, providing that the threshold for certification was clear. The third was neutral on the idea – wishing more detail regarding data quality before giving a response on this.
From these three approaches (staff, patient, commissioner) to assessing the acceptability or utility of a certification scheme, it can be seen that there was a great deal of support for the proposal.
Stage 2: development of minimum standards for CR
Procedure
An expert consensus group (n=14) was convened which comprised highly skilled CR clinicians and managers, academics working in the field, members of the NACR team and patient representation. The health professionals included cardiologists, nurses, exercise professionals and other allied health professionals. Three meetings were held face-to-face between October 2013 and November 2014, with email contact between meetings, to decide the minimum standards for certification, based on the BACPR SCCs.1
Results stage 2
Table 3. Development of the minimum standards for certification of cardiac rehabilitation
The expert group discussed which of the standards could be assessed using NACR data, whether it would be possible to assess programmes for certification if they did not submit patient-level data to the NACR database, and what data points would be used to signify whether a minimum standard was reached or not. The results of the discussions are given in table 3.
From these discussions it became imperative that NACR data should underpin the certification process, in order to provide quality assurance. A draft set of minimum standards was developed and agreed by the expert group, which were finalised after comment by BACPR council.
Stage 3: pilot of the certification scheme
Procedure
CR teams were invited to provide comments on versions of the certification application and guidance documents. Members from 45 CR teams commented on early versions of the application documents. Additionally, the NACR team developed a programme-level report for assessment of meeting those minimum standards derived from NACR data. Guidance documents were developed to support the process, and a number of CR experts were recruited to the Certification Assessment Panel.
Once the certification scheme was developed, CR programmes that had participated in the development stage and submitted audit data to NACR were invited to become pilot sites for the whole certification process.
Results stage 3
Participating teams who submitted data to NACR were invited to participate in a pilot of the complete process of certification, and 16 teams agreed. The majority of the teams had no difficulty in completing the application forms. The NACR data report and application form for each pilot programme was assessed by three members of the Assessment Panel who provided feedback on the submission. There were three potential outcomes of assessment: Pass (all standards met), Defer (failed on one standard but passed the remainder) or Fail (failed on more than one standard). In the case of Defer or Fail, the panel gave guidance on what was needed to achieve a pass. If it was possible to remedy the area(s) where they were failing within the following 12 months (with new NACR data, if required) they would be able to gain certification as part of that submission. If it would take longer than 12 months to amend, then they would need to undertake a new, full application for certification. Eight of the 16 programmes passed immediately, seven were deferred and one failed. Of those programmes marked as deferred, five have so far been able to improve the areas where they did not meet the minimum standards and so become BACPR/NACR certified programmes. Feedback from all of the different groups demonstrated that the certification process worked well. Certification is for three years, after which the programmes must apply for recertification.
Conclusion
As this paper demonstrates, the development of the BACPR/NACR UK National Certification Programme for CR (NCP_CR) has been undertaken with input from a full range of stakeholders to achieve a scheme that is fully quality assured. The NCP_CR is now available (at a small cost to cover administration fees) to all CR programmes that submit data to NACR. For more details see the BACPR website (http://www.bacpr.com/pages/page_box_contents.asp?PageID=911). To request the guidance document (which contains the most recent version of the minimum standards) please email: [email protected]. Certification is for three years, after which the programmes must apply for recertification.
Acknowledgements
The authors would like to thank the many people who contributed to the development of the BACPR/NACR NCP_CR, including the cardiac rehabilitation professionals who completed the surveys, the commissioners who agreed to be interviewed and Cardiovascular Care Partnership UK who provided important feedback from a patient viewpoint. Particular thanks must go to the 16 programmes who agreed to participate in the pilot and to the experts who not only supported the development of the NCP_CR programme but who have continued to contribute to the certification programme by undertaking roles on the BACPR/NACR Certification Assessment Panels.
Funding
This project was supported by an unrestricted educational grant provided to BACPR by Janssen Healthcare Innovation, part of Janssen-Cilag UK. This sponsorship provided funding for CG-P to undertake the survey, patient group engagement and commissioner interviews.
Conflict of interest
None declared.
Key messages
Audit data have consistently demonstrated that there is substantial variation in UK cardiac rehabilitation (CR) service delivery
While there are national standards for CR, it is difficult for CR services to demonstrate to patients, managers and commissioners that they meet minimum standards
The British Association for Cardiovascular Prevention and Rehabilitation has worked with the National Audit of Cardiac Rehabilitation to develop and test a National Certification Programme for CR. This programme is based on quality-assured patient-level data that allows assessment of whether CR programmes meet minimum service standards
References
1. British Association for Cardiovascular Prevention and Rehabilitation. Standards and core components of cardiovascular prevention and rehabilitation: 2nd Edition. London: BACPR, 2012.
2. Buckley JP, Furze G, Doherty P et al. BACPR scientific statement. British standards and core components for cardiovascular disease prevention and rehabilitation. Heart 2013;99:1069–71. http://dx.doi.org/10.1136/heartjnl-2012-303460
3. Lawler PR, Filion KB, Eisenberg MJ. Efficacy of exercise-based cardiac rehabilitation post-myocardial infarction: a systematic review and meta-analysis of randomized controlled trials. Am Heart J 2011;162:571.e2–584.e2. http://dx.doi.org/10.1016/j.ahj.2011.07.017
5. Anderson L, Oldridge N, Thompson DR et al. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol 2016;67:1–12. http://dx.doi.org/10.1016/j.jacc.2015.10.044
6. West RR, Jones DA, Henderson AH. Rehabilitation after myocardial infarction trial (RAMIT): multi-centre randomised controlled trial of comprehensive cardiac rehabilitation in patients following acute myocardial infarction. Heart 2012;98:637–44. http://dx.doi.org/10.1136/heartjnl-2011-300302
7. West R, Jones D. Cardiac rehabilitation and mortality reduction after myocardial infarction: the emperor’s new clothes? Evidence against cardiac rehabilitation. Heart 2013;99:911–13. http://dx.doi.org/10.1136/heartjnl-2013-303705
8. Lewin R, Doherty P. Cardiac rehabilitation and mortality reduction after myocardial infarction: the emperor’s new clothes? Evidence in favour of cardiac rehabilitation. Heart 2013;99:909–11. http://dx.doi.org/10.1136/heartjnl-2013-303704
9. National Institute for Health and Care Excellence. MI – secondary prevention. NICE Clinical Guideline 172. London: NICE, 2013.
10. National Audit of Cardiac Rehabilitation. Annual statistical report 2015. London: British Heart Foundation, 2015.
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits