A 22-year-old man was admitted to a general district hospital with a three-day history of epigastric pain and shoulder discomfort. He reported shortness of breath on exertion, but denied any chest pain or flu-like symptoms. He had no past medical history of note. Vital signs assessment confirmed low blood pressure of 90 mmHg systolic, and tachycardia of 130 beats per minute. Physical examination of the abdomen revealed mild epigastric tenderness. A computerised tomography (CT) scan for suspected cholecystitis showed a normal gall bladder, but revealed a large rim of pericardial effusion measuring 2.8 cm. He was then urgently transferred to a tertiary cardiac centre for assessment and consideration of pericardiocentesis.
On admission to the tertiary centre, he had evidence of pulsus paradoxus, raised jugular venous pressure, and muffled heart sounds, but no murmurs. Subsequently, he underwent pericardiocentesis, which drained 600 ml of turbid straw-coloured fluid with immediate improvement in the haemodynamic status.
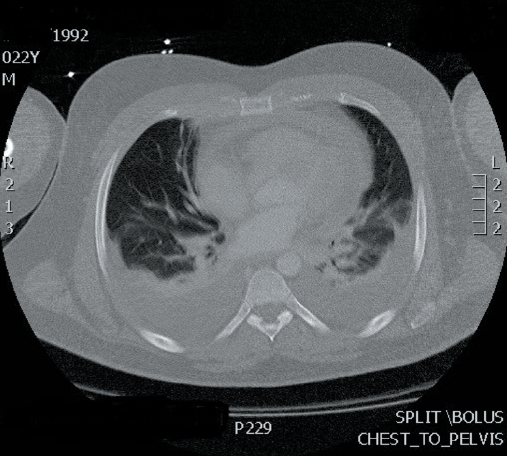
showing pericardial thickening and bilateral pleural effusions
The patient was commenced on regular colchicine and ibuprofen. The initial blood tests showed raised inflammatory markers. The biochemical, microbiological and histopathological analysis of the pericardial fluid was normal, including viral serology and tuberculosis studies. The patient improved clinically and biochemically over a few days. He then self-discharged, against medical advice. Three weeks later he presented to the hospital with progressive breathlessness and shoulder pain. Biochemical tests showed raised inflammatory markers. Cardiac imaging showed a severely thickened pericardium with a 1.0 cm rim of pericardial effusion with bilateral moderate pleural effusions (figure 1). Monitoring his vital signs showed intermittent fever. With an appropriate work-up for suspected sepsis, he was commenced on intravenous piperacillin–tazobactam 4.5 g eight hourly, empirically. Despite antibiotic therapy, he remained symptomatic with no clinical improvement, and his blood and pleural fluid cultures were all negative. On review by the rheumatology team, he had no symptoms or signs to suggest a systemic rheumatological condition. The autoimmune profile was repeated and remained negative. A whole body CT scan did not show any inflammatory process elsewhere. A diagnosis of idiopathic effusive constrictive pericarditis was made.
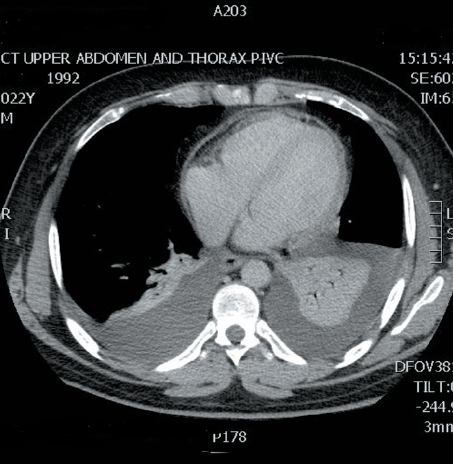
A multi-disciplinary team (MDT) meeting recommendation suggested commencing steroids to cover a possible non-infective inflammatory pericardial disease. The patient was started on 0.5 mg/kg/day prednisolone and made a good recovery, both clinically and biochemically over 48 hours. The repeated cardiac imaging after a week of steroids showed significant reduction in the pericardial thickness (figure 2). He was then discharged on a slow tapering dose of steroids, with a plan of an outpatient review in four-weeks’ time, which he failed to attend. Unfortunately, the patient was re-admitted again with shoulder pain and an ongoing breathlessness. The echocardiogram, on this occasion, showed recurrence of the pericardial thickening and new areas of calcification. Despite clinical improvement with steroids and supportive care, the pericardial thickening persisted. The patient was discharged on a tapering dose of steroids.
Discussion
Idiopathic effusive-constrictive pericarditis is an uncommon pericardial syndrome1 that is often challenging, especially when it is recurrent. This young man had three admissions with symptomatic effusive pericarditis. His symptoms were generally atypical and non-specific. On the first presentation, the clinical assessment was suggestive of cholecystitis. On subsequent admissions, he presented with shoulder discomfort and breathlessness without chest pain. The systemic inflammatory response was generally severe, with extreme tachycardia, tachypnoea, pyrexia and raised inflammatory markers on biochemical laboratory tests. The presentation was similar to sepsis almost every time he was admitted to hospital. The initial response to steroids in the second admission was associated with significant reduction in the pericardial thickening radiologically. However, on the third flare-up, the patient had evidence of recurrence of the pericardial thickening on admission despite being asymptomatic between the two admissions. The investigations done to identify the aetiology of this recurrent pericarditis failed to uncover any potential cause, including viral and rheumatological conditions. Although there were no features of constriction on the last admission, the persistence of the pericardial thickening and the multiple foci of calcifications may predict significant constriction should pericarditis recur again. In this otherwise healthy man, the need for pericardiectomy might be unavoidable at some stage.2
While the majority of patients have a significant improvement in symptoms following pericardiectomy, there is a significant peri-operative morbidity and mortality related to the complex nature of surgery. This is because the removal of the thickened and inflamed pericardium is technically challenging.3,4 Long-term survival after pericardiectomy is inferior to that of an age- and sex-matched population.3,5 In one series, the five- and 10-year survival rates were 78% and 57%, respectively.5 In two other case series, the five-year survival rates after surgery for patients with idiopathic constrictive pericarditis were 80% and 81%.6,7
Conflict of interest
None declared.
Key messages
- The presentation of acute pericarditis can sometimes be atypical and needs a high index of suspicion
- Severe systemic inflammatory response of pericarditis can mimic sepsis and may delay the initiation of steroids in recurrent presentations
- The management of recurrent pericarditis remains a true challenge, and close follow-up is always needed
- The decision to take the surgical option in constrictive pericarditis can be difficult in the young population
References
1. Sagrista-Sauleda J, Angel J, Sanchez A et al. Effusive-constrictive pericarditis. N Engl J Med 2004;350:469–75. http://dx.doi.org/10.1056/NEJMoa035630
2. Hancock EW. Subacute effusive-constrictive pericarditis. Circulation 1971;43:183–92. http://dx.doi.org/10.1161/01.CIR.43.2.183
3. Bertog SC, Thambidorai SK, Parakh K et al. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol 2004;43:1445. http://dx.doi.org/10.1016/j.jacc.2003.11.048
4. Chowdhury UK, Subramaniam GK, Kumar AS et al. Pericardiectomy for constrictive pericarditis: a clinical, echocardiographic, and hemodynamic evaluation of two surgical techniques. Ann Thorac Surg 2006;81:522. http://dx.doi.org/10.1016/j.athoracsur.2005.08.009
5. Ling LH, Oh JK, Schaff HV et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation 1999;100:1380. http://dx.doi.org/10.1161/01.CIR.100.13.1380
6. George TJ, Arnaoutakis GJ, Beaty CA et al. Contemporary etiologies, risk factors, and outcomes after pericardiectomy. Ann Thorac Surg 2012;94:445. http://dx.doi.org/10.1016/j.athoracsur.2012.03.079
7. Szabó G, Schmack B, Bulut C et al. Constrictive pericarditis: risks, aetiologies and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg 2013;44:1023. http://dx.doi.org/10.1093/ejcts/ezt138
