Emergency transvenous temporary pacing is a potentially lifesaving procedure that can be associated with significant complications. Historically, this procedure was performed by relatively inexperienced doctors. In recent years, there have been moves to improve the delivery of emergency pacing in UK hospitals.
We aimed to identify trends in temporary pacing experience among medical registrars in the southwest of England between 2008 and 2016. Registrars currently or previously accrediting with General Internal Medicine (GIM) were surveyed about experience in emergency transvenous pacing.
There have been significant changes in the delivery of temporary pacing over the two time points. Significantly fewer temporary pacing wires had been inserted by medical registrars in 2016 compared with 2008: mean 4.51 versus 9.82 (p<0.0001). Significantly more medical registrars had never inserted a temporary pacing wire in 2016 compared with 2008: 57/84 (67.9%) versus 18/94 (19.1%), p<0.0001. Registrars increasingly did not rate themselves to be fully competent to perform the procedure in 2016, 76/84 (90%), compared with 54/92 (59%) in 2008, p=0.0097. Perceptions regarding who should provide this service have changed. In 2008, 65/92 (79.6%) thought cardiologists should be the sole operators compared with 81/84 (96.4%) in 2016.
In conclusion, there has been a significant change in the provision of emergency temporary pacing services from 2008 to 2016. UK medical registrars no longer have the experience to perform this procedure. It is hoped that a rapidly delivered, cardiology-led pacing service will continue to improve safety and patient care.
Introduction
The insertion of an emergency temporary pacing wire is a potentially lifesaving treatment in acute bradycardia. However, this procedure can be associated with significant morbidity and, occasionally, mortality. In UK district general hospitals (DGH), the responsibility of performing emergency transvenous cardiac pacing historically rested with general physicians. In practice, most procedures were performed by potentially inexperienced trainees.1 Over the previous decade there have been numerous calls for change in the provision of emergency pacing.1-5 It has been shown that doctors with variable experience perform the procedure, and that cardiologists or cardiology trainees take less time to complete the procedure with fewer immediate complications.4 Recent data have emerged on complications occurring in 360,223 patients in the US, based on analysis of the US National Inpatient Sample.6
In January 2016, the British Heart Rhythm Society (BHRS) issued a position statement on the out-of-hours management of bradyarrhythmias. It recommended that patients presenting to the ambulance service with an arrhythmia emergency should be directed to a hospital where they can be appropriately monitored and managed. This hospital should have the ability to insert temporary pacing wires on a 24/7 basis. If presenting to the emergency department, patients should be stabilised before being transferred to an appropriate inpatient specialty, or to an alternative centre that can manage their arrhythmia.7
The last decade has seen a large change in the provision of emergency cardiology services in the UK, as a result of the introduction of primary percutaneous coronary interventions (PCI). This has led to an expansion in the consultant cardiology workforce. In parallel, there have been changes to junior doctor training with a reduction in working hours, development of competency based skill acquisition and, arguably, less exposure to patients with cardiac emergencies.
We sought to determine changes in registrar ability to implant temporary pacing wires over an eight-year time interval.
Objective
To assess trends in the emergency temporary pacemaker insertion in the southwest of England between 2008 and 2016.
Method
A repeated cross-sectional survey of medical registrars working in the southwest of England was performed. The first survey was performed in 2008 during a general internal medicine (GIM) training day in the Severn and Peninsula deaneries. Doctors were asked to complete a paper questionnaire on their experience of emergency temporary transvenous cardiac pacing. The questionnaire explored whether they had received any formal training; how many procedures they had performed in total and how many they had performed in the last six and 12 months. They were also asked which specialists provided the temporary pacing service in their own hospital. Free text was given for comments on how training could be improved. Trainees were asked to self-assess their current level of competency.
Table 1. Hospital and specialty of respondents
| 2008 | 2016 | p value | |
|---|---|---|---|
| Bristol Royal Infirmary | 9 | 12 | |
| Derriford Hospital | 11 | 3 | |
| Cheltenham General Hospital | 4 | 3 | |
| Dorset County Hospital | 3 | 0 | |
| Gloucester Royal Hospital | 6 | 10 | |
| Great Western Hospital | 2 | 2 | |
| Musgrove Park Hospital | 4 | 5 | |
| North Bristol NHS Trust | 6 | 6 | |
| North Devon District | 2 | 5 | |
| Royal Cornwall Hospital | 8 | 3 | |
| Royal Devon and Exeter Hospital | 15 | 7 | |
| Royal United Hospital Bath | 9 | 10 | |
| Torbay Hospital | 7 | 9 | |
| Weston General Hospital | 4 | 2 | |
| Yeovil District Hospital | 3 | 6 | |
| Other | 1 | 1 | |
| Total | 94 | 84 | |
| District General Hospital | 68 | 63 | 0.69 |
| Specialty | |||
| Acute medicine | 9 | 12 | 0.33 |
| Cardiology | 8 | 19 | 0.22 |
| Care of the elderly medicine | 13 | 8 | 0.37 |
| Endocrinology | 15 | 5 | 0.035 |
| General internal medicine (not stated) | 0 | 27 | <0.0001 |
| Gastroenterology | 12 | 4 | 0.06 |
| Renal Medicine | 15 | 1 | 0.0009 |
| Respiratory medicine | 19 | 6 | 0.0122 |
| Rheumatology | 1 | 2 | 0.5 |
| Other | 2 | 0 | |
| Total responses | 2 | 2 | |
| Non-cardiology specialty | 86 | 65 | 0.0088 |
The second survey was performed in 2016 using a survey monkey online questionnaire. Trainees were provided with links to complete the survey through a group email and social media platforms. Medical registrars enrolled in GIM in the Severn and Peninsula deaneries in the 2016 survey were asked to rate their competence relative to the descriptors used in directly observed practical skills (DOPS) assessments,8 or to declare that they were not competent to perform the procedure. These were level 1: able to perform the procedure under direct supervision/assistance, level 2: able to perform the procedure under limited supervision/assistance and level 3: competent to perform the procedure unsupervised and deal with complications. Level 1 competency and not competent were combined in assessing differences between groups. DOPS graded descriptors were not used in the original survey. Trainees describing themselves as competent, fairly competent or not competent were grouped into level 3, level 2 and level 1/not competent to allow comparison.
Data regarding number of procedures were collected as integers in 2008 and as categories for any numbers above five in the 2016 survey. For analysis, the 2008 values were grouped to match the categories used in 2016, and the midpoint of these categories was used.
Assessment for differences between counts for the two time intervals was performed with a Chi-squared test. Assessments for differences in number of procedures performed between the two time periods were performed with a Mann-Whitney test, as the data were not normally distributed (GraphPad Prism Version 7.04).
Results
In 2008, 94 questionnaires were completed. In 2016, 84 were returned. Responder rates were not available. Doctors from 16 different hospitals provided answers (table 1). An equal proportion of respondents were based in DGHs in both years. In 2016, 92 respondents were in registrar training and 82 respondents in 2016 were at ST3 level or above.
Of note, in the 2016 survey, non-cardiological specialties were less well represented, comprising 77% of the respondents compared with 91% previously (p=0.0088).
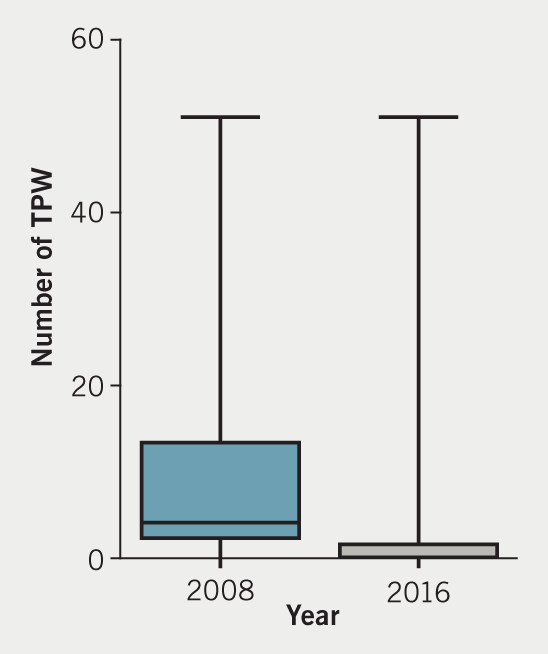
Numbers of temporary pacing wires implanted
The numbers of temporary pacing wires (TPW) inserted by respondents has markedly changed between the two time periods, as represented in figure 1 and table 2. The data for both time points was positively skewed with a small number of respondents completing a high number of procedures.
Table 2. Number of temporary pacing wires (TPW) inserted
| 2008 | 2016 | |
|---|---|---|
| Total number of TPW implants undertaken by registrars (all) | ||
| Mean | 9.82 | 4.51 |
| Median | 4 | 0 |
| Interquartile range | 2–13 | 0–3 |
| Total number of TPW implants undertaken by registrars (all) | ||
| Mean | 0.42 | 0.2 |
| Median | 0 | 0 |
| Interquartile range | 1 | 0 |
A Mann-Whitney test was used to assess for difference between the two time periods. There was a significant difference in the number of TPW placed by trainees (p<0.0001).
Furthermore, there was a significant difference in the proportion of respondents who had never inserted a TPW. In 2008, 18/94 (19.1%) of respondents had never placed a TPW compared with 57/84 (67.9%) in 2016, p<0.0001. On the previous survey, 32/94 (34.0%) had implanted 10 or more TPW in 2008 compared with 7/84 (8.3%) in 2016, p<0.0001.
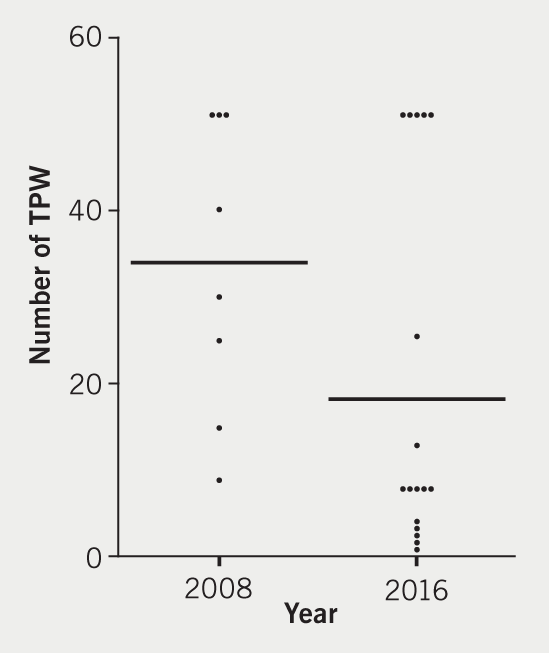
Effects of cardiology trainees
In 2008, some non-cardiology trainees had achieved high numbers of TPW procedures. Reviewing raw data from 2008, two geriatric trainees had recorded that they had achieved 50 and 100 cases. Excluding cardiology trainees from the data, there remained a significant difference between the two periods (p<0.001).
Despite lower numbers of cardiology respondents in 2008, there was still a significant difference in the number of procedures performed, (p=0.0321 Mann-Whitney). The distribution is shown in table 3 and figure 2.
Table 3. Number of temporary pacing wires (TPW) inserted
| Number of TPW | 0 | 1 | 2 | 3 | 4 | 5 | 6–10 | 11–15 | 16–20 | 21–30 | 31–40 | 41–50 | 51+ |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2008 (n=8) | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 | 1 | 0 | 3 |
| 2016 (n=19) | 2 | 1 | 1 | 1 | 1 | 1 | 5 | 1 | 0 | 1 | 0 | 0 | 5 |
Competence
In 2008, 36/92 (39%) respondents rated themselves as not competent versus 61/84 (72%) respondents in 2016 (p<0.0001). With the numbers surveyed there was not a significant difference in the numbers rating themselves as level 3 competent to insert a TPW. However, when level 1 and level 2 ratings of competencies are combined (i.e. less than independent), there is a significant increase in the number of trainees in 2016 rating themselves as less than fully competent. Results are shown in table 4.
In addition to the self-rating of competency, if we assume the threshold of competency, as recommended in 1994 by the American Heart Association, to be having performed 25 TPW,9 83/92 (90%) respondents would be deemed not competent to pace in 2008 versus 78/84 (92%) in 2016 (p=0.53).
Table 4. Self-rated competency and grade when first starting implanting
| 2008 | 2016 | p value | |
|---|---|---|---|
| Self-rated competency | |||
| Level 1/not competent | 36 | 66 | <0.0001 |
| Level 2/fairly competent | 28 | 10 | 0.0028 |
| Level 3/competent | 18 | 8 | 0.0866 |
| Total responses | 92 | 84 | 0.0235 |
| Not independent (Level 1 or 2) | 54 | 76 | 0.0097 |
| At what grade did you implant your first temporary pacing wire? | |||
| Not performed | 18 | 57 | <0.0001 |
| PRHO/foundation training | 2 | 2 | 0.91 |
| SHO/core medical training | 52 | 11 | <0.0001 |
| Registrar training | 22 | 14 | 0.2639 |
| Total responses | 94 | 84 | |
| Key: PRHO = pre-registration house officer; SHO = senior house officer | |||
In 2008, 84/88 (95%) of all doctors surveyed had never received any formal, structured training in inserting emergency pacemakers versus 76/83 (92%) in 2016 (p=0.30).
There has been a shift in perceptions of who should be responsible for providing temporary pacing cover. In 2008, 65/94 felt that cardiology should provide the service. By 2016 this had risen to 81/84 (p<0.001).
Discussion
In this repeated survey of medical registrars working in the southwest of England we have demonstrated a significant reduction in the amount of temporary pacing systems being placed by registrars and physician self-rated competencies.
The ability of medical registrars to implant TPW has declined. In 2016, most medical registrars have not inserted a TPW or rate themselves as not competent to do so, compared to a minority of respondents in 2008.
There are three possible reasons for the changes observed.
First, reduced need. There have been improvements in reperfusion rates post-STEMI (ST-elevation myocardial infarction). It is thought that this has reduced the need for TPW in the context of an inferior STEMI. Data on this are relatively limited.10 As TPW insertion is associated with morbidity it is best avoided if possible and revascularisation performed.11 A local level review of procedural data for 717 patients who had a TPW inserted at the Bristol Royal Infirmary between May 2014 and May 2019 identified that 413 cases had a TPW inserted for transcatheter aortic valve implantation (TAVI), 88 for balloon valvuloplasty and 77 for extraction of a cardiac device. Only 66 TPW were inserted in the absence of another procedure and an additional 30 cases had a TPW placed to facilitate the insertion of a permanent system as an emergency case. Only 31 were inserted at the time of angiography.
Second, changes to registrar training have occurred. A reduction in working hours because of the European Working Time Directive has led to more focused specialty training. In the authors’ opinion much junior doctor work focuses on basic ward care, limiting opportunities to learn new skills. There are few opportunities to undertake critical care placements. However, there are attempts to increase critical care exposure in the new internal medicine curriculum.12
Lastly, we speculate that the change in the provision of a dedicated on-call cardiology service has had the biggest impact on who performs emergency TPW insertion. We expect that medical registrar skills in this area will decline further. This appears to have been understood and appreciated in the current Joint Royal Colleges of Physicians Training Board (JRCPTB) GIM curriculum. In the 2009 guidance “Temporary cardiac pacing by internal wire or external pacemaker” featured.13 This did not feature in the 2012 amendments.14 There has been a shift in opinion among all medical registrars as well, with the feeling that temporary transvenous pacing should now be a cardiology-led procedure. For registrars training in acute medicine, temporary pacing via the transvenous route remains listed (alongside the insertion of a Sengstaken-Blakemore tube) as a procedural competence where clinical independence is desirable.15 Our investigation has highlighted that this is challenging for the current cohort of cardiology trainees, let alone acute medical trainees. In the new GIM curriculum there is a requirement to perform temporary cardiac pacing using an external device.
Developing and maintaining the skills of the cardiology specialty trainee is also a challenge. This can be achieved by participating in placing TPW during TAVI procedures, electrophysiology studies and device extractions. However, it is noted that these procedures are generally performed in tertiary centres. Access can be a challenge to the DGH trainee.
Conclusion
There have been significant changes in the proportion of medical trainees able to perform temporary pacing by the transvenous route both in numbers and self-ratings of competency. Additionally, we have demonstrated that the number of cases performed by cardiology registrars has also decreased.
Key messages
- The number of temporary wires inserted by both medical and cardiology registrars has fallen over the past decade
- Few registrars now self-assess themselves as competent in inserting a temporary wire
- A cardiology delivered temporary pacing service should be the norm and efforts must be taken to ensure that the current generation of cardiology trainees acquire this skill
Conflicts of interest
None declared.
Funding
None.
Study approval
This was a survey of medical registrars conducted in 2008 and 2016 with voluntary participation and no study approval was required.
References
1. Murphy JJ. Current practice and complications of temporary transvenous cardiac pacing. BMJ 1996;312:1134. https://doi.org/10.1136/bmj.312.7039.1134
2. Petch MC. Temporary cardiac pacing. Postgrad Med J 1999;75:577–8. https://doi.org/10.1136/pgmj.75.888.577
3. Murphy JJ. Problems with temporary cardiac pacing. Expecting trainees in medicine to perform transvenous pacing is no longer acceptable. BMJ 2001;323:527. https://doi.org/10.1136/bmj.323.7312.527
4. Betts TR. Regional survey of temporary transvenous pacing procedures and complications. Postgrad Med J 2003;79:463–5. https://doi.org/10.1136/pmj.79.934.463
5. Rajappan K, Fox KF. Temporary cardiac pacing in district general hospitals – sustainable resource or training liability? QJM 2003;96:783–5. https://doi.org/10.1093/qjmed/hcg135
6. Metkus TS, Schulman SP, Marine JE, Eid SM. Complications and outcomes of temporary transvenous pacing: an analysis of over 360,000 patients from the National Inpatient Sample. Chest 2018;155:749–57. https://doi.org/10.1016/j.chest.2018.11.026
7. Linker N, Earley M. Position statement on the out of hours management of bradyarrhythmia emergencies. London: British Heart Rhythm Society, 2016. Available from: https://bhrs.com/position-statements/
8. Joint Royal Colleges of Physicians Training Board (JRCPTB). Specialty training curriculum for cardiology, August 2010 (Amendments August 2016). Available from: https://www.jrcptb.org.uk/sites/default/files/2010%20Cardiology%20Curriculum%20%28amendments%202016%29.pdf [accessed 2 August 2019].
9. Francis GS, Williams SV, Achord JL et al. Clinical competence in insertion of a temporary transvenous ventricular pacemaker. A statement for physicians from the ACP/ACC/AHA Task Force on Clinical Privileges in Cardiology. Circulation 1994;89:1913–16. https://doi.org/10.1161/01.CIR.89.4.1913
10. Lee SN, Hwang YM, Kim GH et al. Primary percutaneous coronary intervention ameliorates complete atrioventricular block complicating acute inferior myocardial infarction. Clin Interv Aging 2014;9:2027–31. https://doi.org/10.2147/CIA.S74088
11. Hwang YM, Kim CM, Moon KW. Periprocedural temporary pacing in primary percutaneous coronary intervention for patients with acute inferior myocardial infarction. Clin Interv Aging 2016;11:287–92. https://doi.org/10.2147/CIA.S99698
12. Joint Royal Colleges of Physicians Training Board (JRCPTB). Curriculum for Internal Medicine Stage 1 Training. London: The Federation of the Royal Colleges of Physicians, 2019. Available from: https://www.jrcptb.org.uk/internal-medicine
13. Joint Royal Colleges of Physicians Training Board (JRCPTB). Specialty training curriculum for general internal medicine, August 2009. Available from: https://www.gmc-uk.org/-/media/documents/2009_GIM_curriculum_FINAL__2_.pdf_30562900.pdf
14. Joint Royal Colleges of Physicians Training Board (JRCPTB). Specialty training curriculum for general internal medicine, August 2009 (Amendments 2012). Available from: https://www.jrcptb.org.uk/sites/default/files/2009%20GIM%20%28amendment%202012%29.pdf
15. Joint Royal Colleges of Physicians Training Board (JRCPTB). Specialty training curriculum for acute internal medicine, August 2009 (Amendments made August 2012). Available from: https://www.jrcptb.org.uk/sites/default/files/2009%20AIM%20%28amendment%202012%29.pdf
