Transthoracic echocardiography presents a risk of COVID-19 transmission between an echocardiographer and the patient. Reducing the scanning time is likely to mitigate this risk for them both. British Society of Echocardiography (BSE) level 1 echocardiography offers a potential framework for focused scanning in an outpatient setting. There were 116 outpatients scheduled for a level 1 scan supplemented with additional pre-defined views, if required. Unexpectedly, a fifth of the scans were performed as an unintended full scan for a variety of reasons. Our results showed that focused scans were performed more quickly than full scans and below the NHS Test and Trace exposure cut-off of 15 minutes. However, if more than three sets of additional measurements were required then a full scan could be performed more quickly. Seniority of the echocardiographer and scan time had an inverse relationship. By examining the patients’ clinical records we were confident that all of the scans, whether focused or full, had answered the requestor’s clinical question. Although the COVID-19 vaccination programme should reduce the necessity of minimising exposure time during a scan there could still be a role for level 1 scanning during the COVID-19 recovery programme to tackle the vast lists of patients waiting for an echocardiogram.
Introduction
Performing a transthoracic echocardiogram (TTE) usually involves an echocardiographer and a patient spending about 30 minutes in close proximity. This presents a risk for COVID-19 transmission for them both. In March 2020, at the start of the COVID-19 pandemic, the British Society of Echocardiography (BSE) released guidance about inpatient scanning advocating triage of requests, targeted scanning and use of personal protective equipment (PPE).1 Their subsequent COVID-19 recovery advice relating to outpatient services outlined risk mitigation and performing ‘as focused a study as the referral allows’ if the patient had been scanned historically.2 Focused scans are very different from standard outpatient full TTEs, which are directed by comprehensive and detailed minimum dataset protocols.3 Adopting focused scanning during the pandemic required our workforce to alter their practice extremely quickly with limited time or opportunity for retraining.
The BSE level 1 TTE protocol was devised for use in acute echocardiography. It was launched in 2018 and had been in regular use in acute settings at our institution for over a year. A level 1 scan differs from a full TTE by consisting of fewer 2D images and no spectral Doppler. However, it includes parasternal, apical and subcostal views and uses colour-flow Doppler to interrogate the mitral, aortic and tricuspid valves. Its strength is the identification of clinically significant findings quickly, but it is not designed to detect more subtle abnormalities, and its use for quantifying and monitoring valve disease is limited. Since the level 1 protocol was familiar and well established on our acute wards we decided to pilot it as a framework for outpatient scanning during the COVID-19 pandemic, but with the option of incorporating additional views and measurements, as required. We postulated that the level 1 protocol would help the echocardiographers systematically focus their scans, reduce the likelihood of missing abnormalities due to over-focusing, and reduce scan duration.
Method
The Great Western Hospital (GWH), Swindon, is a district general hospital with a BSE-accredited echocardiography department. The use of BSE level 1 scanning during the COVID-19 pandemic had already been approved by the Trust Clinical Audit and Effectiveness team and had been used for most inpatient scans from May 2020.
Table 1. The ‘add-on’ protocols. Each represents a + 1 addition to the basic level 1 protocol
| More than mild valve disease (aortic stenosis, aortic regurgitation, mitral stenosis, mitral regurgitation) |
| Replacement valves |
| Suspected endocarditis |
| Left ventricular function |
| Right ventricular function with pulmonary pressure |
| Pericardial effusion |
| Congenital scans |
| Atrial fibrillation scans |
A standard operating procedure was developed for the GWH echocardiography department, outlining all aspects of performing echocardiography during the COVID-19 pandemic. This included the minimum views required for a level 1 scan. The views were listed on a wipeable printed aide memoire fixed to each echo machine while echocardiographers gained familiarity with the new protocol. A set of ‘add-on’ protocols were used to direct the abnormal, or suspected abnormal, level 1 studies (table 1). These included additional measurements specified in the BSE protocols focused for specific pathology, excluding those requiring a stand-alone Doppler probe. The left ventricular (LV) ‘add-on’ included assessment of LV systolic and diastolic function. A steerable continuous wave Doppler trace was recorded routinely if there was mild or more tricuspid regurgitation. Thus, a completely normal scan could be performed as a level 1 dataset only. However, if the level 1 views suggested LV dysfunction, the LV ‘add-on’ would be applied and the scan would be level 1 + 1. If the level 1 images had also shown moderate mitral regurgitation (MR) the MR ‘add-on’ would also be applied so the scan was level 1 + LV + MR and classed as level 1 + 2. More than mild tricuspid regurgitation would be interrogated with continuous wave Doppler routinely, if it caused concern or if pulmonary pressures were required then the right ventricle (RV)/pulmonary pressure ‘add-on’ would be applied and the scan would become level 1 + 3.
Level 1 outpatient TTE was offered to the cardiology and stroke services during Summer 2020 as the first peak of the pandemic diminished. A backlog of outpatient echocardiography requests had developed during the first lockdown and social distancing combined with enhanced infection control measures were reducing echo activity during the initial recovery period. With knowledge of the pressures on the echo service, doctors were advised that they could request level 1 scans as an alternative to a full scan. It was hoped that this would increase the number of scans performed and reduce scan time – and, therefore, contact time – for staff and patients. The arrhythmia service agreed that a level 1 scan with assessment of left atrial size could be used for patients in atrial fibrillation prior to cardioversion. The rapid access chest pain service team were willing for their requests to be level 1 scans with the LV ‘add-on’, to rule out LV impairment. The stroke physicians were actively consulted to find out what they required from their scans and they agreed that a focused level 1 scan would be adequate for their needs to rule out a substrate for cardiac thrombus.
Unexpectedly, some level 1 scans were requested from outside the cardiology and stroke services. However, level 1 scanning had been used successfully across the hospital for most inpatient scans since the start of the pandemic, so this may have led to these requests.
The echocardiographers were advised to plan their study, based on the request, before they started scanning. They were provided with our Trust’s designated PPE (surgical masks, aprons, gloves and visors) and the waiting areas were socially distanced. Patients were asked to report their height and weight if they knew it and asked to wear their own face mask. A brief symptom history was taken as the patient undressed and their blood pressure was recorded if the equipment was available. This had been requested by the medics because most medical clinic visits were virtual at this stage of the pandemic. Some scans were performed on dedicated level 1 lists at a temporary non-COVID site; others were added at the end of routine full TTE lists at our acute site, which had COVID-19 positive inpatients elsewhere in the hospital. Appointment slot times were 30 minutes to include time for patient set up, scanning and cleaning. All measurements were performed offline to minimise the face-to-face study duration. A specific level 1 reporting template was used to generate the report. The images and reports were archived according to usual processes and in accordance with BSE recommendations for accredited departments.
Wherever technically feasible, the BSE level 1 protocol was used for all patients, but with additional views and measurements added depending on the reason for the scan and any abnormalities found or suspected when acquiring the level 1 views. The echocardiographer could extend their study by as many ‘add-on’ protocols as they deemed appropriate for the patient.
The Philips CVIS system was used to identify all outpatients of the GWH, with a planned procedure listed as “Transthoracic Echocardiography (BSE Level 1 Study)” between 3 September and 18 December 2020. Data were collected using CVIS, the Intellispace Cardiovascular (ISCV) image archive and Medway (electronic patient record system). Patient demographics, clinical details, request details and any previous echocardiography were recorded. Each study was reviewed twice. It was reviewed initially to collect information about the images, study duration, the echocardiographer and the reported findings (by KD). It was then re-studied by an expert echocardiographer (HR) to check the quality of the study, whether it answered the clinical question and whether the appropriate protocol had been followed.
Results
Between 3 September and 18 December 2020, 136 focused outpatient TTE’s were requested by medical practitioners at the GWH. Twenty of these were excluded because a different type of focused scan was specified; most of these studied the left ventricle only. Thus, 116 were suitable for a level 1 scan. Their average age was 66.5 years, range 25–92 years; 52 (45%) were female and 64 (55%) male.
Of the referrals for a level 1 scan, 69% were from cardiology, 12% from the stroke team, 6% from the respiratory department and 13% from other specialties. Most (28%) were to rule out heart failure, 24% were to monitor a known cardiac abnormality such as valve disease or an impaired left ventricle, 22% were for an arrhythmia and 14% for stroke or transient ischaemic attack (TIA). Smaller numbers were performed for abnormal electrocardiogram (ECG) (5%), before routine non-cardiac surgery (3%) or a murmur (3%).
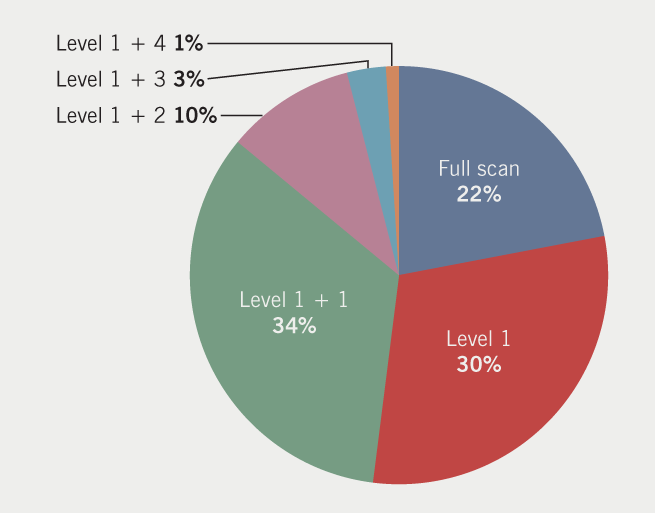
Despite all of the studies being requested as a level 1 scan, 25 (22%) full scans were performed (figure 1). Half of the scans were performed on dedicated level 1 lists, the rest were fitted in around full study lists.
It was not always clear why a full scan was performed when a level 1 scan had been requested. Several reasons were given including:
- Prevailing BSE COVID-19 guidance suggested a full scan should be performed if there was no previous echo. We found that 60% of the full scans had no previous scan.
- Band 6 members of staff were keen to perform full scans for training or for their BSE logbook.
- The level 1 labelling on the CVIS request was not easily noticed so missed on several occasions.
- Staff thought they could perform a full scan more quickly than a level 1 scan.
- Multiple pathologies were noticed during the scan so a full scan was performed.
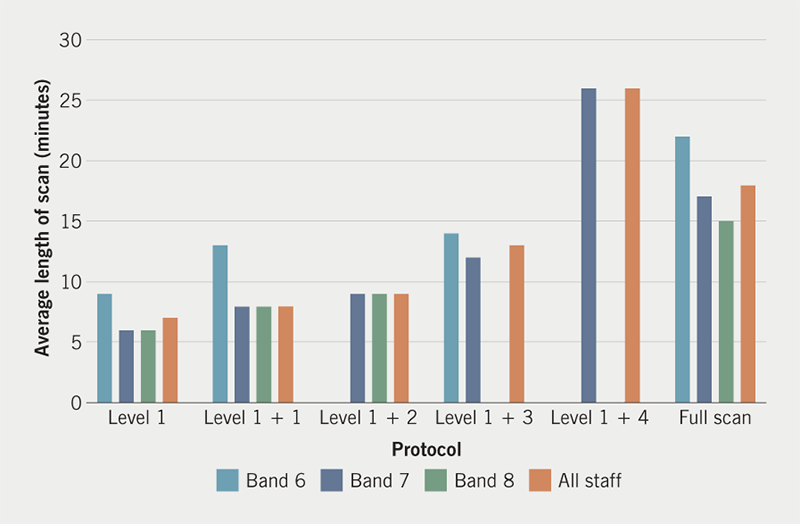
The average total scan time was 10 minutes (range 3–30 minutes) for all scans including full. On average a full scan was performed in 18 minutes (ranging from 9–30 minutes). Band 6 echocardiographers took an average of 22 minutes to perform a full scan, while band 7 and 8 echocardiographers performed these scans in 17 and 15 minutes, respectively. All level 1 scans without an ‘add-on’ were performed in an average of less than 10 minutes, regardless of banding. While all level 1 + scans (except level 1 + 4) were performed on average in less than 13 minutes, with slight variation based on banding (figure 2).
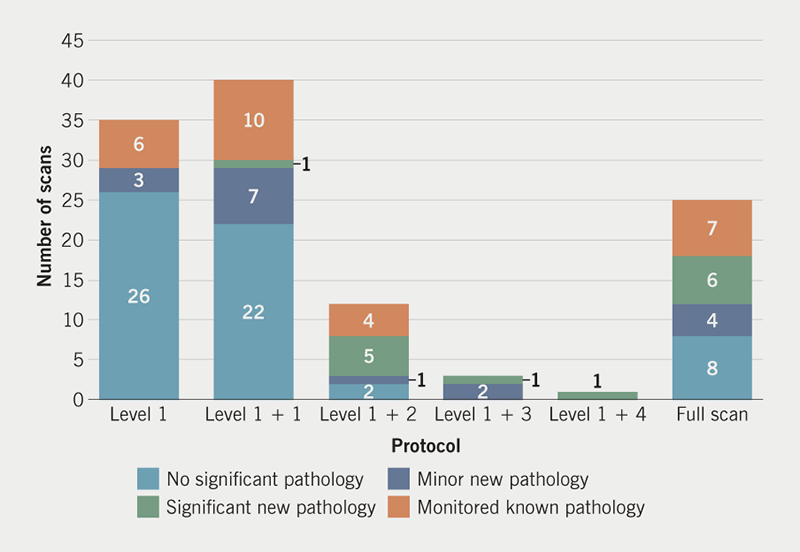
In total, 50% of all scans performed had no significant pathology. Of the 25 full scans performed, 32% had no significant pathology. Of the 35 level 1 only scans, 74% of these showed no significant pathology. Of all the scans performed, 12% showed a significant new pathology, most of which were identified from a level 1 + 2 scan (42%) (figure 3).
The second review of the 116 scans was reassuring. Obviously, only the images recorded could be examined but they were scrutinised carefully for secondary effects of pathology that might not have been immediately evident from the images supplied. When quality assuring the studies, it was discovered that one potentially clinically relevant finding had been unreported. This was a regional wall abnormality in a full study. The finding would have been visible in a level 1 scan. The study was re-reported after the review.
Following a team discussion part way through this pilot, we decided to change the reporting template for level 1 studies. The level 1 report previously used in the acute setting, which was brief with a small number of drop-down optional sentences, was replaced by the usual full study report template. This allowed more detailed reporting and less prescribed descriptions. It also included a section to report the left atrium, which was not present in the level 1 report template.
Discussion
We were surprised how hard it was to change practice, despite a dangerous pandemic and an unvaccinated patient population and workforce. As a BSE-accredited department, our team often expressed their preference to work to our long-established and strongly promoted protocols and felt it was easier to continue as usual, despite the potential risks to themselves and their patients. However, our results have challenged our views. The data show that it is undoubtedly quicker to perform a level 1 study. The Track and Trace exposure limit of 15 minutes is a useful, if arbitrary, benchmark. The average time for all of the level 1 studies, apart from a level 1 + 4 ‘add-on’, fell below this cut-off. For full studies, only band 8s achieved this. The banding issue also merits consideration. It is unsurprising that the junior echocardiographers took longer to acquire images, and while this may be acceptable in low-risk situations, it should be considered very carefully when risks are high. Even when their average scanning times might be acceptable the range of their scan durations looks less safe.
We need to be confident that our patients are not being disadvantaged by having a level 1 scan. We don’t have a ‘gold-standard’ imaging modality to refer to for our population and it would not have been appropriate to put them at any additional risk of infection with further imaging. However, we did examine their requests, their clinic letters before and after their echo and any other relevant medical information available on our database. We did not find any cases where a level 1 echo was categorised as inadequate. The images were reviewed twice and the scans definitely ‘did the job’ of addressing the clinical question. The level 1 scan protocol should exclude serious abnormality, but we may have missed minor findings, such as an atrial septal defect without haemodynamically significant shunting or mild pulmonary valve disease. The other side to this issue is that inviting patients to a hospital during a pandemic also has the potential to disadvantage them if they become exposed to COVID-19 during their visit. Therefore, we also need to be certain that the echo is necessary at the given time, that appropriate triage processes are being followed and all risk mitigation measures are followed.
One of the questions that arose was when to stop ‘adding on’ and convert to a full study. Most of the focused scans we did were level 1 or level 1 + 1. Level 1 + LV was the most common ‘add-on’. There was only one level 1 + 4, and it took longer than any of the full scans. Our results suggest that if more than three ‘add-ons’ are required it will be quicker to convert to a full study. The average level 1 + 3 duration remains below the 15-minute exposure threshold.
This change to our service required a different way of scanning. It involved planning the study beforehand and thinking during the scan in a way that felt different from our traditional approach to image acquisition, which generates comprehensive standard datasets from which we extract the relevant information after the study has been performed. In our level 1 lists we applied this focus while still scanning. To assist with the study planning we have started to incorporate focusing guidance for the echocardiographer as we triage requests.
As the COVID-19 vaccination programme continues to roll out, the pressure to focus scans for safety reasons should reduce, but there could still be a role for shorter scans to tackle the backlog of echocardiograms. They could be particularly useful when there is a low expectation of abnormality or an obviously focused and discrete clinical question. The creation of diagnostic hubs is currently under discussion to help with COVID-19 recovery, and there could be potential for carefully triaged level 1 lists alongside other types of echocardiography and complementary imaging techniques. By reducing the time spent on normal or near-normal scans, there would be the prospect of preserving longer scan times for abnormal or complex studies. This would maximise immediate access to echocardiography and reduce waiting lists while longer-term definitive solutions are developed. Unsurprisingly, the COVID-19 pandemic has shone a light on the historical workforce issues in echocardiography, but addressing these will take some time and be of no benefit to the patients on today’s waiting lists.
Conclusion
If exposure time is important for safety reasons, there is a role for focused scanning. Our results suggest that a level 1 scan with three ‘add-ons’ is likely to be the maximum worthwhile focused protocol, so in multiple pathologies a full scan would be quicker. Focused scanning is different from the conventional approach of universally applying comprehensive minimum standards and requires some different skills and training. It relies on careful pre-planning, evaluating as you scan and having a wider appreciation of the role of the scan in patient management. In selected patients, focused echocardiography could play a role in the COVID-19 recovery programme.
Key messages
- Structured, focused echocardiograms reduced the contact time between the echocardiographer and the patient
- A level 1 scan, with focused add-ons as needed, answered the clinical question
- If a level 1 scan required more than three add-ons, it was quicker to perform a full echocardiogram
- In selected patients, focused echocardiography could play a role in the COVID-19 recovery programme
Conflicts of interest
None declared.
Funding
None.
Study approval
The evaluation of level 1 scanning was registered with the Great Western Hospital’s Audit and Effectiveness department (reference number USC-234/1). The Trust’s locally published clinical audit algorithm showed that ethical approval was not required.
References
1. British Society of Echocardiography. COVID-19 guidance: updated guidance on provision of echocardiography. London: BSE, March 2020 (updated January 2021). Available from: https://bsecho.org/Public/News/Articles/2020/2020-03/202003-COVID-guidance-3.aspx
2. British Society of Echocardiography. Post COVID-19 guidance: TTE. London: BSE, May 2020. Available from: https://bsecho.org/Public/News/Articles/2020/2020-05/202005-COVID-guidance-TTE.aspx
3. British Society of Echocardiography. Level 1 (L1) accreditation. Minimum dataset. London: BSE, 2020. Available from: https://www.bsecho.org/Public/Accreditation/Personal-accreditation/Level-1/Public/Accreditation/Accreditation-subpages/Personal-accreditation-subpages/Level-1-accreditation.aspx?hkey=6099b4b8-5cb9-4425-a201-1874aadcb73f
