We report a case of a patient that presented with typical angina pain and associated risk factors for coronary artery disease (CAD). Subsequent cardiac catheterisation led to the discovery of an isolated R-IIP modified Lipton classification coronary artery anomaly with follow-up coronary computed tomography angiography (CCTA) confirmation. This case report includes images of the CCTA and left heart catheterisation results, along with a discussion of the potential for increased risk of atherosclerosis in our patient, and a proposed explanation of his presentation with prototypical angina pain, despite lack of apparent atherosclerosis.
Introduction
The human coronary system is normally comprised of a right and left coronary artery that feed respective regions of the heart. The right and left coronary arteries usually arise from the area superior to their respective coronary cusp, known as the sinus of Valsalva. However, it has been found that approximately 1.33% of humans have coronary artery anomalies. R-II Lipton classification coronary artery anomalies are found in only 0.015% of the population and 1.1% of coronary anomalies.1 We present the case of a 55-year-old man with a R-IIP modified Lipton classification coronary artery anomaly.
Case presentation
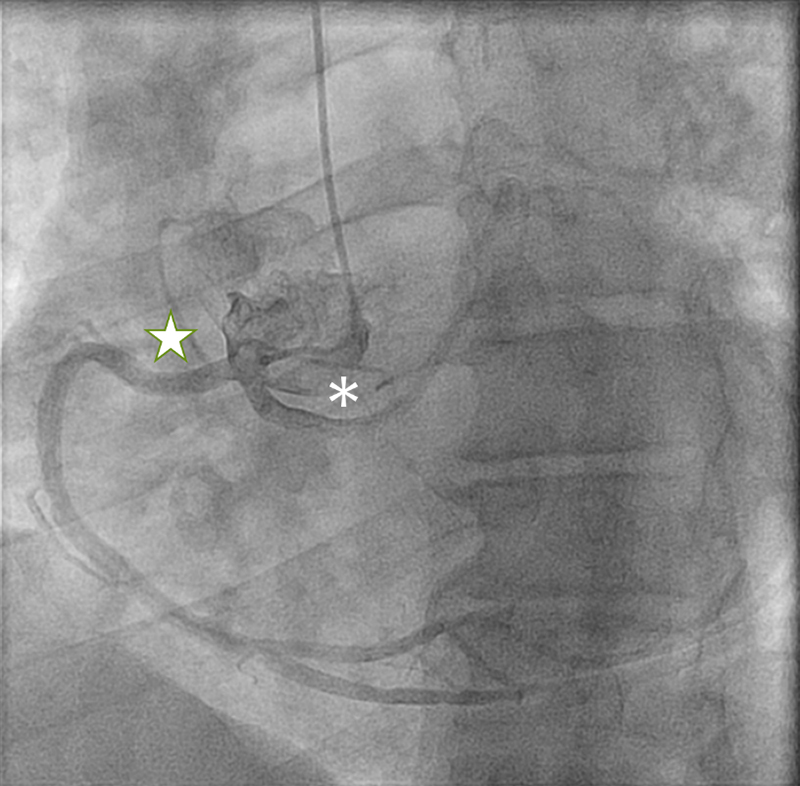
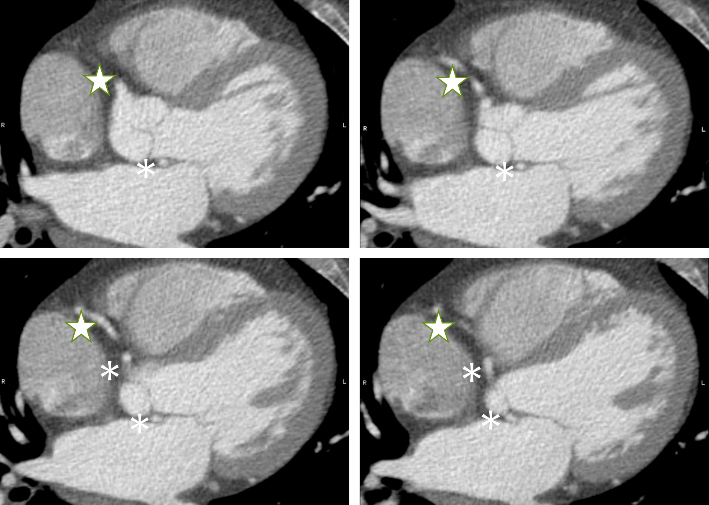
A 55-year-old man with a history of obesity, hypertension, uncontrolled diabetes, dyslipidaemia, and cerebral vascular accident presented with chest tightness, shortness of breath, and increased palpitations. An echocardiogram previously revealed a left ventricular ejection fraction of >55%. Cardiac catheterisation was performed, given the patient’s high risk for coronary artery disease (CAD) and typical anginal complaints. The catheterisation revealed no apparent obstructive CAD, but it did reveal that the left main coronary artery anomalously originated from the right coronary cusp, as can be seen in figure 1. Coronary computed tomography angiography (CCTA) was subsequently ordered to further assess the anatomy and pinpoint the origin of the coronary arteries. This study revealed a single coronary artery with common origin of the right and left coronary arteries arising from the right sinus of Valsalva with the left coronary artery coursing posteriorly between the aortic root and left atrium, as can be seen in figure 2. The patient was provided with supportive treatment and continued on prior medical therapy.
Discussion
Single coronary arteries are associated with other cardiac abnormalities approximately 40% of the time, which was not apparent in our patient.2 R-IIP single coronary abnormalities have been proposed to be a class II clinical classification, which means that these abnormalities are ‘related per se to myocardial ischaemia’. This rating was mostly attributed to the potential risk of myocardial ischaemia.3
R-IIP single coronary abnormalities could specifically have increased incidence of CAD. A case-control study found that anomalous left circumferential arteries that arose from the right side of the heart, and ran posteriorly to the great vessels, had a statistically significant increase in mean stenosis by 12.5% due to atherosclerotic disease compared with non-anomalous left circumferential arteries. These individuals were matched for age, gender, predominant symptoms, and degree of stenosis in non-anomalous coronary arteries. The act of running posterior to the great vessels most likely contributed to atherosclerosis due to the course the coronary arteries followed resulting in more tortuosity and angulation of the artery.4 This is most likely due to micro-environmental sheer forces and flow turbulence acting on different segments of the arteries due to their tortuosity and angulation, which leads to independent rates of atherosclerosis development in different regions of a coronary artery and between coronary arteries.3
However, the patient in this case report was found to have no apparent atherosclerotic disease. Thus, his angina pain could be the result of a combination of proposed processes. One proposed process is that a small coronary ostium size, relative to large distal coronary branches, may lead to angina symptoms. Similarly, a diseased or relatively small proximal vessel of a single coronary artery may make normally insignificant distal lesions more haemodynamically significant due to the idea of resistance in series.5 No uniform guidelines are established for the treatment of coronary artery abnormalities, with Rigatelli and Rigatelli recommending no pharmacological treatment, close follow-up, and immediate treatment only for coronary abnormalities associated with sudden cardiac death, such as anomalous coronary arteries running between the great vessels, or those that have superimposed CAD.3
Conclusion
Coronary artery anomalies are a rarity. Isolated R-IIP single coronary artery disease is an even rarer subtype seen in a small fraction of the population. This subtype can lead to myocardial ischaemia through increased risk of atherosclerosis in the anomalous coronary artery. Even without clear-cut atherosclerotic disease, mechanisms for blood flow restriction may lead to typical anginal presentation.
Conflicts of interest
None declared.
Funding
None.
Patient consent
The patient consented to anonymised publication of their case. All patient identifying information has been removed from this report.
References
1. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21:28–40. https://doi.org/10.1002/ccd.1810210110
2. Sharbaugh AH, White RS. Single coronary artery: analysis of the anatomic variation, clinical importance, and report of five cases. JAMA 1974;230:243–6. https://doi.org/10.1001/jama.1974.03240020033019
3. Rigatelli G, Rigatelli G. Coronary artery anomalies: what we know and what we have to learn. A proposal for a new clinical classification. Ital Heart J 2003;4:305–10. Available from: https://www.federcardio.it/pdf/2003/05/20030113.pdf
4. Click RL, Holmes DR, Vlietstra RE, Kosinski AS, Kronmal RA. Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival – a report from the Coronary Artery Surgery Study. J Am Coll Cardiol 1989;13:531–7. https://doi.org/10.1016/0735-1097(89)90588-3
5. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology 1979;130:39–47. https://doi.org/10.1148/130.1.39
