Cardiovascular medicine is undergoing transformation driven by machine learning (ML) technologies.1 Algorithms now assist in imaging interpretation, electrocardiogram (ECG) analysis, and outcome prediction, with increasing sophistication.1,2 The adoption of ML-powered diagnostic tools in cardiology is growing, yet training programmes remain largely unchanged, creating a disconnect between skills taught and those required in contemporary practice.1–4
Despite rigorous clinical preparation, many cardiology trainees complete their education with insufficient knowledge of the ML technologies increasingly present in clinical workflows.5,6 As these applications become more prevalent, training programmes must integrate relevant ML education to ensure cardiologists can effectively evaluate, implement, and collaborate with artificial intelligence (AI) systems, rather than merely function as passive end-users of increasingly sophisticated technology.
The current landscape of ML in cardiology
ML has established a presence across various domains of cardiology practice. In cardiovascular imaging, deep learning algorithms assist in echocardiographic interpretation, supporting functions such as ejection fraction calculation and abnormality detection.7 Advances in cardiac magnetic resonance imaging (MRI) applications have contributed to automating tasks like myocardial segmentation, while ML approaches to coronary computed tomography (CT) analysis aim to improve coronary plaque assessment.4,7
Electrocardiography has also seen ML integration. Algorithms designed to detect arrhythmias and identify patterns associated with structural heart disease have received regulatory clearance in multiple jurisdictions.8
Beyond diagnostics, risk-prediction models utilising patient data seek to forecast adverse cardiovascular events, potentially offering advantages over traditional scoring systems.3,7 Treatment optimisation approaches aim to support medication selection, while predictive analytics tools are being developed to identify high-risk patients for preventive interventions.7
The educational gap
Despite ML’s increasing presence in cardiovascular practice, formal education on these technologies remains notably absent from the UK cardiology training programme. The current JRCPTB (Joint Royal Colleges of Physicians Training Board) cardiovascular medicine curriculum does not explicitly address AI or ML competencies, creating a potential gap in preparing trainees for contemporary practice.9 Surveys of cardiology trainees’ preparedness for using and evaluating ML tools would be valuable for quantifying this gap.10
Analysis of curricula internationally suggests similar limitations in ML education.11 The incorporation of computational methods in cardiovascular medicine training appears limited across major cardiology programmes, though some institutions, particularly in the US, have begun developing focused ML pathways.12 Some US institutions have established dedicated AI fellowships and computational cardiology tracks, while European programmes are beginning to integrate ML modules into core curricula. UK programmes have generally not yet established similar initiatives, potentially placing UK cardiologists at a disadvantage relative to international counterparts in engaging with these emerging technologies.
Many practising cardiologists express concerns about implementing ‘black-box’ algorithms whose mechanisms they cannot adequately evaluate.13,14 Without fundamental ML literacy, clinicians face challenges in assessing whether algorithms are appropriate for their patient populations, understanding limitations, or recognising potential biases. Fields, such as radiology and pathology, appear to have incorporated computational training into their educational frameworks more extensively than cardiology.15,16
Core ML competencies for cardiologists
To address this educational gap, defining essential ML competencies for cardiologists is necessary. These should provide sufficient literacy to function effectively in an AI-augmented environment without requiring cardiologists to become data scientists.
Cardiologists need a fundamental understanding of ML concepts – supervised versus unsupervised learning, training and validation datasets, and basic principles underlying common cardiovascular ML applications. This foundational knowledge enables engagement with technical literature and communication with specialists.
Development of skills for critical evaluation of ML research and commercial algorithms is essential, including understanding of performance metrics, recognition of study limitations, and identification of potential bias sources. The same critical appraisal skills applied to pharmaceutical trials should extend to ML tools.
Awareness of the ethical dimensions of ML implementation is crucial, including consideration of algorithmic bias, transparency, privacy, and clinical decision-making responsibility in algorithm-assisted practice.
Finally, practical knowledge of the data requirements and regulatory pathways governing these technologies prepares cardiologists to participate in implementation decisions and collaborate effectively with technical professionals in multi-disciplinary teams.
Implementation strategies
Integrating ML competencies into already crowded cardiology curricula requires thoughtful strategies. Programmes with adequate resources might consider dedicated rotations allowing trainees to gain immersive experience in computational methods. Specialised ML pathways pairing fellows with data science mentors can serve as models. Figure 1 presents a conceptual circuit model showing how ML education integrates across four key areas in cardiology training: foundational knowledge, teaching methods, clinical skills, and practical applications. The interconnected design reflects how these elements reinforce each other, with clinical experience feeding back to improve curriculum development.
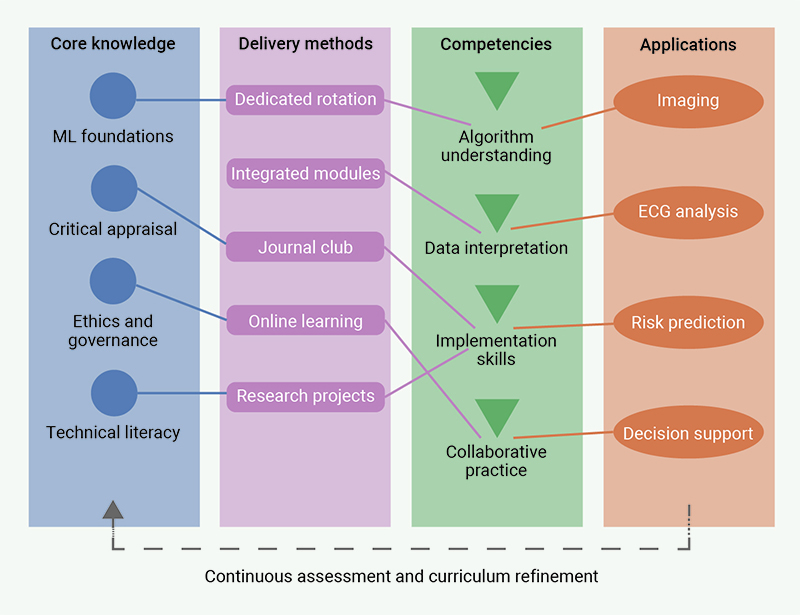
| This circuit model conceptualises the integration of machine learning into cardiology education through four interconnected domains: Core Knowledge (blue circles), Educational Delivery Methods (pink rectangles), Competencies (green triangles), and Clinical Applications (orange ovals). The dashed grey feedback loop illustrates how clinical experience informs curriculum development, creating a dynamic educational ecosystem. Unlike traditional sequential curricula, this circuit approach promotes parallel skill development across multiple domains, reflecting the integrated nature of ML in modern cardiovascular practice. |
For programmes with limited capacity, existing educational components can incorporate ML concepts – imaging rotations can introduce ML applications, while journal clubs can develop critical appraisal skills for ML literature. Online modules offer flexible options for addressing core knowledge requirements, potentially supplemented by workshops using relevant datasets.
Implementation requires collaboration beyond traditional boundaries. Partnerships between cardiology departments and computer science programmes can create cross-disciplinary learning opportunities, while industry collaborations can provide exposure to real-world ML development processes.
Assessment methods should evolve as well, with traditional examinations for conceptual understanding complemented by project-based assessments for practical competencies in data handling and algorithm evaluation.
Barriers and solutions
Implementing ML education in cardiology training faces several barriers. Limited faculty expertise presents a significant challenge, as few educators possess sufficient computational background. Resource constraints affect content development, computational access, and dataset provision in resource-limited programmes. Resistance may also emerge from competing priorities and concerns about diluting clinical training.
Solutions include faculty development through workshops and certificate programmes, external partnerships with computer science departments or industry to supplement expertise gaps, and phased implementation, beginning with modest initiatives. Evidence demonstrating ML education’s clinical impact will build consensus for curriculum reform, while professional societies can establish standards for computational competencies among trainees.
Future directions
Looking ahead, cardiologists must approach ML algorithms as partners in care delivery. Professional societies should develop ML competency frameworks, formally recognising computational literacy alongside traditional clinical skills.
Key messages
- Educational imperative: UK cardiology training must incorporate machine-learning (ML) literacy to prepare physicians for technology-augmented practice
- Clinical partnership: ML tools should enhance, not replace, clinical judgement and expertise
- Cross-disciplinary approach: implementing ML education requires collaboration between clinical, technical and regulatory stakeholders
Conflicts of interest
None declared.
Funding
None.
References
1. Khera R, Oikonomou EK, Nadkarni GN et al. Transforming cardiovascular care with artificial intelligence: from discovery to practice: JACC state-of-the-art review. J Am Coll Cardiol 2024;84:97–114. https://doi.org/10.1016/j.jacc.2024.05.003
2. Shameer K, Johnson KW, Glicksberg BS, Dudley JT, Sengupta PP. Machine learning in cardiovascular medicine: are we there yet? Heart 2018;104:1156–64. https://doi.org/10.1136/heartjnl-2017-311198
3. Kasartzian DI, Tsiampalis T. Transforming cardiovascular risk prediction: a review of machine learning and artificial intelligence innovations. Life (Basel) 2025;15:94. https://doi.org/10.3390/life15010094
4. Henglin M, Stein G, Hushcha PV et al. Machine learning approaches in cardiovascular imaging. Circ Cardiovasc Imaging 2017;10:e005614. https://doi.org/10.1161/CIRCIMAGING.117.005614
5. Russak AJ, Chaudhry F, De Freitas JK et al. Machine learning in cardiology-ensuring clinical impact lives up to the hype. J Cardiovasc Pharmacol Ther 2020;25:379–90. https://doi.org/10.1177/1074248420928651
6. Barrios JP, Tison GH. Advancing cardiovascular medicine with machine learning: progress, potential, and perspective. Cell Rep Med 2022;3:100869. https://doi.org/10.1016/j.xcrm.2022.100869
7. Khalpey Z, Khalpey A, Jha S. Enhancing diagnostic accuracy and procedural outcomes in interventional cardiology through machine learning algorithms. J Soc Cardiovasc Angiogr Interv 2025;4(3part B):102511. https://doi.org/10.1016/j.jscai.2024.102511
8. Krittanawong C, Rogers AJ, Johnson KW et al. Integration of novel monitoring devices with machine learning technology for scalable cardiovascular management. Nat Rev Cardiol 2021;18:75–91. https://doi.org/10.1038/s41569-020-00445-9
9. Joint Royal Colleges of Physicians Training Board. Curriculum for cardiology training: implementation August 2022. London: JRCPTB, 2022. https://www.thefederation.uk/training/specialties/cardiology
10. Brown OI, Morgan H, Jenner WJ et al. Joint British Societies’ position statement on cardiology training in the United Kingdom. Heart 2025;111:e2. https://doi.org/10.1136/heartjnl-2024-325037
11. Ledziński Ł, Grześk G. Artificial intelligence technologies in cardiology. J Cardiovasc Dev Dis 2023;10:202. https://doi.org/10.3390/jcdd10050202
12. Johnson KW, Torres Soto J, Glicksberg BS et al. Artificial intelligence in cardiology: present and future. J Am Coll Cardiol 2018;71:2668–79. https://doi.org/10.1016/j.jacc.2018.03.521
13. Krittanawong C, Johnson KW, Rosenson RS et al. Deep learning for cardiovascular medicine: a practical primer. Eur Heart J 2019;40:2058–73. https://doi.org/10.1093/eurheartj/ehz056
14. Cabitza F, Rasoini R, Gensini GF. Unintended consequences of machine learning in medicine. JAMA 2017;318:517–18. https://doi.org/10.1001/jama.2017.7797
15. Jha S, Topol EJ. Adapting to artificial intelligence: radiologists and pathologists as information specialists. JAMA 2016;316:2353–4. https://doi.org/10.1001/jama.2016.17438
16. Tajmir SH, Alkasab TK. Toward augmented radiologists: changes in radiology education in the era of machine learning and artificial intelligence. Acad Radiol 2018;25:747–50. https://doi.org/10.1016/j.acra.2018.03.007
