A man in his eighties presented with a two-week history of left-arm swelling and bruising. Twelve years earlier, he had undergone dual-chamber pacemaker implantation for bradycardia and syncope. His past medical history included hypertension, paroxysmal atrial fibrillation (pAF), and coronary artery bypass grafting (CABG) 15 years prior.
Upon further investigation with ultrasound Doppler, and computerised tomography (CT) of his chest, a thrombus was confirmed in the left subclavian vein, associated with a pacing lead. He was initiated on a three-week course of low molecular weight heparin (LMWH). Although his symptoms initially improved, traces of the thrombus remained on his follow-up CT after commencing treatment, and he was continued on lifelong direct oral anticoagulant (DOAC).
Pathogenesis, incidence, investigations and management of pacemaker-induced thrombosis are discussed. This case illustrates a rare, delayed presentation of pacemaker-induced thrombosis in the context of a symptomatic presentation and highlights the potential need for prolonged anticoagulation.
Background
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), arises from Virchow’s triad: venous stasis, endothelial injury, and hypercoagulability. Upper extremity DVT (UEDVT) represents ~10% of all DVTs, with an annual incidence of 0.4–1.0 per 10,000 people.1 Symptomatic disease is rarer. Causes are primary or, more commonly (~60%), secondary to central venous catheters, pacemaker leads, malignancy, or other prothrombotic states.2,3
Pacemaker leads substantially increase UEDVT risk. A 2021 meta-analysis (Duijzer et al.) reported a >10-fold higher incidence after transvenous lead insertion,4 although whether this excess risk is transient or persistent remains uncertain. We report a case of symptomatic UEDVT 12 years after pacemaker implantation without another identifiable trigger.
Case presentation
An active man in his 80s presented with two weeks of bruising of the proximal left forearm, extending distally with oedema and discomfort. He had no fever, haemodynamic instability, dyspnoea, or hypoxia. There had been no recent immobilisation, surgery, long-haul travel, trauma, malignancy, or prior thrombosis. He had no history suggestive of repetitive arm activity or exercises (as to suggest Paget-Schroetter’s syndrome). His past medical history included hypertension, coronary artery bypass graft (CABG) 15 years prior, and paroxysmal AF (pAF), which was diagnosed prior to pacemaker insertion and not identified in the pacing interrogations in preceding years to his presentation.
Twelve years earlier, a dual-lead pacemaker (right atrial and right ventricular) was implanted via the cephalic vein for symptomatic bradycardia. He had annual pacemaker checks, all of which were within expected parameters with no evidence of wire malfunction.
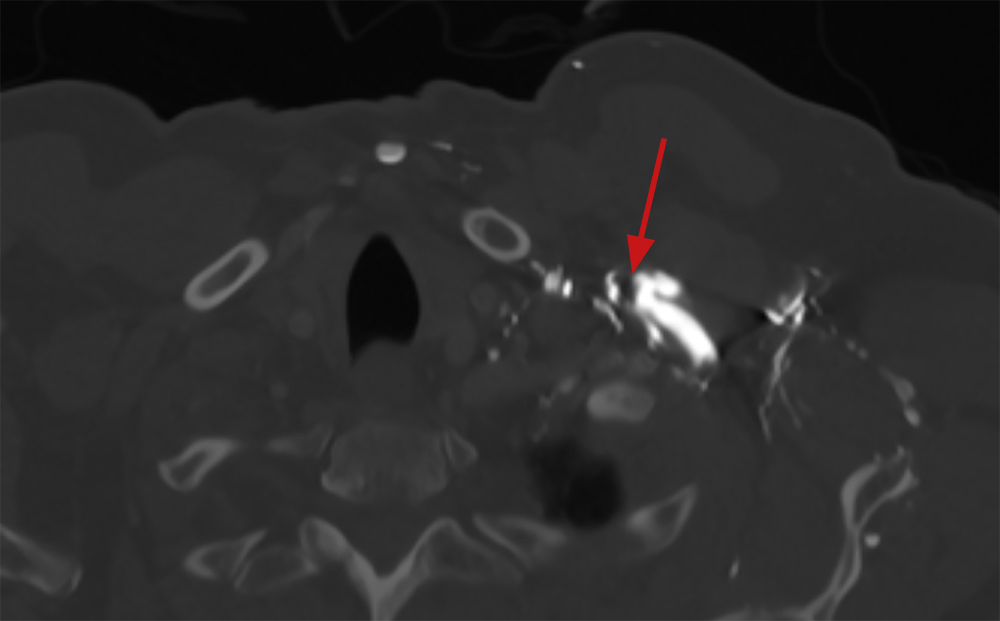
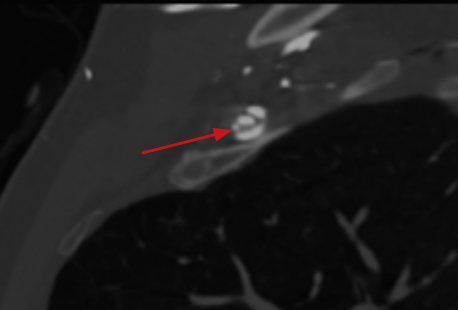
At ambulatory care review after referral from his general practitioner, Doppler ultrasound demonstrated a thrombus in the distal subclavian vein around the pacemaker lead. Following initial management, contrast computed tomography (CT) of the thorax confirmed a non-occlusive thrombus around the lead at the mid-subclavian vein (figures 1 and 2), without proximal propagation or collateral circulation.
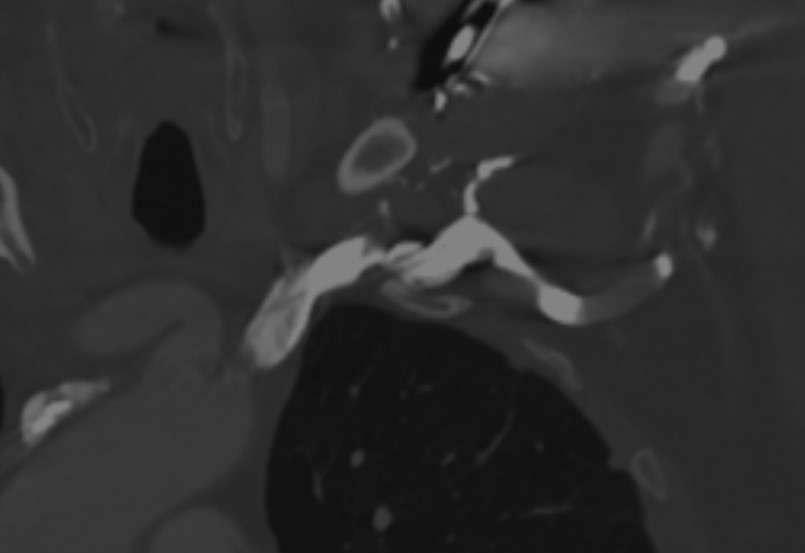
After the Doppler ultrasound, he was reviewed by his cardiology consultant, where he received treatment-dose dalteparin for three weeks, he was then transitioned to a direct oral anticoagulant (DOAC). At three-month follow-up, symptoms had resolved, but residual thrombus persisted (figure 3). Anticoagulation was continued, supported by his pAF history. AF had been documented previously, though not on recent pacing checks.
Discussion
Pathogenesis and incidence
Most pacemaker-related thromboses are asymptomatic and found incidentally.1,5 Silent lead thrombus occurs in 35–45% of pacemaker recipients.3 When symptomatic occlusion develops, ipsilateral arm swelling is typical.6 Duijzer et al. observed a 0.9% incidence of symptomatic UEDVT beyond two months post-implantation in 8,671 patients.4
Collateral venous channels may mask symptoms, despite substantial obstruction.4,7 Proposed mechanisms include endothelial trauma at insertion, chronic lead irritation, and progressive venous stenosis.3,4,7 No stenosis or collateralisation was seen in this case.
The patient’s pAF may have conferred additional thrombogenic risk, although no AF episodes were captured in the preceding three years.
Delayed presentation
Most lead-associated UEDVT arises within three months of implantation,5,6 and few cohorts extend surveillance beyond one year. Duijzer et al. reported a mean onset of 26 months.4 A prior case described UEDVT 26 years post-implant, but involved lead fracture and epicardial device revision.8 In contrast, our patient’s leads were intact and functioning 12 years post-implant, underscoring the unusual delay.
Investigations and management
Ultrasound is the first-line investigation for suspected UEDVT, owing to high sensitivity and specificity.1-3 CT or magnetic resonance (MR) venography can confirm equivocal studies; venography remains the gold standard, but is seldom required.
Anticoagulation is the mainstay of therapy. Although UEDVT-specific trials are lacking, DOACs are increasingly used by extrapolation from lower limb DVT data.9 Catheter-directed thrombolysis may be reserved for severe symptoms or extensive clot burden.3
Lead extraction is generally avoided unless the system is non-functional, because removal of long-dwelling pacemaker leads carries procedural risk. The vast majority of patients tolerate venous lead insertion without thrombosis, so anticoagulation is not used routinely in pacemaker patients. Especially when considering the bleeding risk of long-term anticoagulation.1
Complications of UEDVT include PE (12%) and post-thrombotic syndrome (13%),2,3 as well as potential loss of vascular access, which is particularly relevant for pacemaker-dependent patients who may require another wire sited in the future.
Conclusion
This case illustrates a rare instance of symptomatic UEDVT 12 years post-pacemaker implantation, in the absence of other thrombotic risk factors. It suggests that transvenous leads may represent a persistent thrombogenic stimulus in some individuals. Because many such patients present through emergency departments, the association with an indwelling pacing system may be missed unless specifically considered. A careful device history, comparative upper limb examination, and early imaging are, therefore, warranted. Prompt anticoagulation remains key, and long-term anticoagulation may be justified in selected patients, even when traditional risk scores are low. Optimal treatment length with anticoagulation and the role of serial imaging remain uncertain; prospective data are needed to guide practice, and individualised clinical judgement remains essential. Further investigation for prothrombotic conditions could also be considered, especially in younger patients. Further research should address whether repeated imaging to document thrombus resolution can safely guide discontinuation of anticoagulation, as well as the length of anticoagulation treatment.
Conflicts of interest
None declared.
Funding
None.
Patient consent
Written informed consent was obtained from the patient for publication of the clinical details and accompanying images included in this report.
References
1. Mazzolai L, Aboyans V, Ageno W et al. Diagnosis and management of acute deep vein thrombosis: a joint consensus document from the European Society of Cardiology working groups of aorta and peripheral vascular diseases and pulmonary circulation and right ventricular function. Eur Heart J 2018;39:4208–18. https://doi.org/10.1093/eurheartj/ehx003
2. Margey R, Schainfeld R. Upper extremity deep vein thrombosis: the oft-forgotten cousin of venous thromboembolic disease. Curr Treat Options Cardiovasc Med 2011;13:146–58. https://doi.org/10.1007/s11936-011-0113-1
3. Rozmus G, Daubert J, Huang D et al. Venous thrombosis and stenosis after implantation of pacemakers and defibrillators. J Interv Card Electrophysiol 2005;13:9–19. https://doi.org/10.1007/s10840-005-1140-1
4. Duijzer D, Winter M, Nijkeuter M et al. Upper extremity deep vein thrombosis and asymptomatic vein occlusion in patients with transvenous leads: a systematic review and meta-analysis. Front Cardiovasc Med 2021;8:698336. https://doi.org/10.3389/fcvm.2021.698336
5. Stoney WS, Addlestone RB, Alford WC Jr et al. The incidence of venous thrombosis following long-term transvenous pacing. Ann Thorac Surg 1976;22:166–70. https://doi.org/10.1016/S0003-4975(10)63980-X
6. Van Rooden C, Molhoek S, Rosendaal F et al. Incidence and risk factors of early venous thrombosis associated with permanent pacemaker leads. J Cardiovasc Electrophysiol 2004;15:1258–62. https://doi.org/10.1046/j.1540-8167.2004.04081.x
7. Goto Y, Abe T, Sekine S et al. Long-term thrombosis after transvenous permanent pacemaker implantation. Pacing Clin Electrophysiol 1998;21:1192–5. https://doi.org/10.1111/j.1540-8159.1998.tb00177.x
8. Basar N, Cagli K, Basar O et al. Upper-extremity deep vein thrombosis and downhill esophageal varices caused by long-term pacemaker implantation. Texas Heart Inst J 2010;37:714–16. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3014125/
9. Bosch FTM, Nisio MD, Büller HR, van Es N. Diagnostic and therapeutic management of upper extremity deep vein thrombosis. J Clin Med 2020;9:2069. https://doi.org/10.3390/jcm9072069
