Transcatheter aortic-valve implantation (TAVI) was performed in around 34,500 patients in 11 European countries in the first five years following European approval of the devices in 2007, new data show.
Writing in the Journal of the American College of Cardiology (published online 15th May 2013, doi: 10.1016/j.jacc.2013.03.074), the authors point out that the number of potential TAVI candidates in the 11 countries surveyed was 158 371, meaning that TAVI remains “greatly underutilised”, with a penetration rate of 17.9%.
Use of the procedure appears to be greatly influenced by how much each country spends on healthcare. Countries, such as the UK, where taxation is the principle source of healthcare funding, have a lower TAVI usage. Almost half of all implants were performed in Germany (45.9%), with Italy (14.9%) and France (12.9%) the next most frequent implanters. The UK was fourth, accounting for 8% of TAVI procedures. Ireland accounted for the smallest proportion of implants (0.4%).
The authors led by Dr Darren Mylotte (McGill University, Montreal, Canada) estimate that in 2011, 36% of patients eligible for TAVI received the procedure in Germany, compared to just 9% in the UK.
However, in an accompanying editorial, Drs John Webb and Marco Barbanti (St Paul’s Hospital, Vancouver, Canada), argue that TAVI may not be so underused and that Mylotte et al. had based their estimate of patients eligible on a “liberal interpretation” of the indication for TAVI.
They point out that TAVI is very expensive, and that “Even a country with a strong economy might find TAVI too costly for individuals in whom conventional surgery or medical management might be considered clinically and socially acceptable”. They conclude that: “Perhaps as the cost differential between transcatheter and surgical valves falls, at least some of the resistance to greater penetration will fade”.
Tissue-engineered human organs – the next generation of treatments for chronic heart diseases – will soon become a multi-billion dollar medical market according to an analysis by the research and consulting firm GlobalData.
But research is still in early stages and a long way from meeting regulatory approval. A team in Spain is currently building on the pioneering work of Dr Doris Taylor at the University of Minnesota, USA, who was able to develop a lab-grown beating rat heart in 2010, by implanting human stem cells into a rat heart scaffold which served as a blueprint for the stem cells to follow.
Dr Francisco Fernandez-Aviles and his team in Madrid are looking at bioengineering replacement human body parts, working to grow a human heart. They have already grown early-stage valves and patches that could one day be used to repair tissue damaged by heart attacks, and hope to produce a working heart in the next five to six years. A bioreactor will provide oxygen and nutrients to the growing organ and remove waste products, and blood will be pumped through the organ to mimic circulation in the human heart. Electrical connections in the heart will also be modelled, with a pacemaker generating electrical activity.
Can you tell right from left bundle branch block? Are they clinically important?
Dr Heather Wetherell
And what (if anything) can you do about it?
If you find ECGs intimidating, you are not alone. Help is at hand!
We are pleased to announce this new BJC series which is aimed at, “keeping the art of ECG interpretation alive in primary care”, in the words of series author, Dr Heather Wetherell (above).
Heather, a general practitioner and a GP with a Special interest in Cardiology at James Cook University Hospital, Middlesbrough, recently launched an educational blog Keeping ECGs simple. This runs alongside the Twitter forum, #ECGclass, which is intended to offer some easy to follow ECG ‘refresher’ notes for clinicians who have previous, but somewhat rusty, knowledge. It also hopes to encourage less reliance on the often-inaccurate analysis by digital machines, now commonly found in many practices.
Social media is increasingly recognised as an important educational medium, allowing conversation and learning, while removing the constraints of a traditional classroom environment with computers, smartphones and tablets working like a virtual classroom. Participants can learn ‘on-the-move’ and can freely drop-in-and-out of conversations at their leisure.
The BJC series will be around the blog with the aim of keeping the learning atmosphere casual, non-threatening, and fun. Cardiologists will sometimes comment on further investigations and management of patients, and we will welcome feedback and questions from readers, as well as continuing some of the dialogue on Twitter.
All will be explained in the next issue of
the journal!
The European Society of Cardiology has said in a position paper that it welcomes the European Commission’s (EC) proposals for a new Regulation to govern the evaluation and approval of medical devices in Europe as an important step towards improving patient safety. The EC proposal document is available at http://ec.europa.eu/health/medical-devices/documents/revision/index_en.htm
New risk analysis scoring system
A new risk scoring system, based on the SMART study, allows doctors to determine more accurately the risk of cardiovascular disease patients developing a new event, such as heart attack or stroke.
Researchers from the University Medical Center (UMC) Utrecht, The Netherlands, developed the ‘SMART risk score’ by using data from 5,800 patients in the SMART (Secondary Manifestations of ARTerial disease) study.
Clinical details include gender, medical history, smoking behaviour, blood pressure and laboratory results. By using the model, doctors can now for the first time accurately predict a patient’s risk of a recurring vascular or cardiovascular event within the next 10 years. The results are published in Heart (doi: 10.1136/heartjnl-2013-303640).
Professor Yolanda van der Graaf, an epidemiologist at UMC Utrecht explains: “Patients and doctors do not gain anything from knowing what the average risk is. They want to know what their own individual risk is of disease recurrence”.
Sit less and move around more
Individuals at high risk of developing type 2 diabetes would benefit from being told to sit less and move around more often, rather than simply exercising regularly, according to research published in Diabetologia (doi: 10.1007/s00125-013-2845-9). Dr Joseph Henson and colleagues from the University of Leicester suggest that reducing sitting time by 90 minutes in total per day could lead to important health benefits.
Currently, at risk patients are advised to engage in moderate-to-vigorous physical activity for at least 150 minutes per week. But the new study suggests that patients should in fact be advised to reduce their sedentary time.
“Diabetes and cardiovascular prevention programmes concentrating solely on moderate-to-vigorous physical activity may overlook an area that is of fundamental importance to cardiometabolic health,” says Dr Henson who thinks there should be a paradigm shift in advice given to individuals at high risk of type 2 diabetes, who should be encouraged to think about the balance of sedentary behaviour and physical activity throughout the day.
New insulin available
Insulin degludec (Tresiba®), a new once-daily basal insulin for adult patients with type 1 and type 2 diabetes, is now available in the UK. According to the manufacturers Novo Nordisk UK, it is the first insulin to offer people with diabetes flexibility in the timing of insulin administration, on occasions when administration at the same time of day is not possible.
First UK chair in cardiorenal medicine
Professor David Goldsmith
Congratulations to Professor David Goldsmith (pictured above), Consultant Nephrologist at Guy’s King’s and St Thomas’ Medical School, King’s College London, who has recently been appointed to the first Chair in Cardiorenal Medicine in the UK. The appointment reflects the growing academic overlap between heart and kidney disease.
Professor Goldsmith has major interests in hypertension, cardiovascular disease and inflammation and calcification syndromes in renal patients. He is a founder member and active participant in the Cardiorenal Forum, which is holding their 8th Annual Scientific meeting on 4th October, this year (see www.cardiorenalforum.com).
Speaking to the BJC, Professor Goldsmith said, “I am delighted to have an opportunity to play a role in highlighting ever-increasing links between renal medicine, cardiology, diabetology and other clinical disciplines. I believe this reflects a growing trend towards doctors talking to each other across these different specialties in order to improve patient care and outcomes.”
We continue our series in which Consultant Interventionist Dr Michael Norell takes a sideways look at life in the cath lab…and beyond. In this column, he (or perhaps his trusty steed) consider the changing role of the medical secretary.
I should have thought about writing something like this years ago. Increasingly, I encounter a regular struggle to find a suitable topic upon which to muse that is readable, interesting, vaguely cardiological and – importantly – about which I have not written previously (as for the last on that list, I am relying somewhat upon my memory being better than yours). This topic was staring me in the face…
During my more than 20 years in consultant practice I have been privileged to work with a handful of medical secretaries. Previously, as a junior doctor, I recall my various bosses sitting in clinic and dictating letters directly to their secretary who, scribbling furiously, produced reams of shorthand in a spiral bound notepad.
The resulting bizarre hieroglyphics would later be translated into recognisable print (via a device termed a typewriter) that also generated one or more carbon copies. A process of checking, correction and signing would then precede enveloping, licking, franking and posting.
Dictaphones (a registered name, like Biro) saw the demise of such written skills, and technology ensured that these machines evolved from a Heath Robinson-type construction, derived seemingly from the era of Thomas Edison, to something you could more comfortably slip into your pocket.
At the same time, the constant drive towards efficiency meant that hospitals, like other organisations, were attracted to the concept of the typing pool. Whichever typist was up to date with their work, would then deal with your dictated correspondence. In one institution in which I worked this process was even more disconnected; in a secluded office and using one of a number of dedicated telephones, I dialled a specific extension number that allowed me to record onto the ether, as it were. A day or so later the printed results would appear in my cubbyhole for signing.
Succinct days
In registrar years my consultant would, on his ward rounds, dictate a short and succinct letter to each patient’s GP. This served a number of purposes: it documented him seeing the patient and making a contemporaneous note, it made the eventual production of the discharge summary much easier and it ensured that the GP was aware of what was happening to the patient.
I was sufficiently influenced by this approach to adopt and modify it when I took up my own consultant post. Rather than produce a ward round letter, I dictated only a paragraph summarising the course of the inpatient stay thus far and the proposed management plan. This would be typed and pasted into the notes, a system similar to that which our orthopaedic colleagues had been using for years. It proved extremely valuable as it was legible (useful) and, when scanning through a thick set of notes, I could rapidly find my own entry (probably less useful).
For years the combination of trusty tape recorder and accompanying mini-cassette served me well as a diary and memory prompt, and I can only recall two instances when this technology let me down…
My secretary had been off on maternity leave and for a few weeks my letters were typed by a less-than-able substitute. This resulted in constant checking and rechecking, correcting and re-correcting, such that our department ran out of Tipp-Ex and by the time any letter was actually sent out, the patient had got better.
Eventually my much-missed assistant returned. Basking in a sense of enormous relief shortly afterwards, and whilst dictating some outpatient letters, I muttered a brief preamble into the microphone along the lines of “For God’s sake don’t let what’s her name type this. I’m sure her typing consists of hitting keys at random!”
Somehow, and I suspect that higher beings on Mount Olympus played a part in this just to teach me a lesson, the tape found its way onto the desk of you know who…
The fallout was predictable; tears, counselling, hugs of support, more tears and quiet chats with managers, led to an apology along with some chocolates and a bunch of flowers. The anonymous lady in question never dealt with my letters again and I’m sure would have produced a letter tendering her resignation if she had actually been able to type the phrase.
In contrast to this sin of commission, the second episode was more one of omission. I tend not to write much (or indeed, anything) in outpatient notes, preferring to devote all my attention to observing and listening to the patient before assimilating my opinion into a letter that my primary care colleague would find helpful. From a medico-legal aspect I am assured that such a signed and dated contemporaneous communication is acceptable but it does rely on one small, but vital, link in the chain…specifically, not losing the tape.
Ten new patients, nothing written in the notes and no documented clue about what I thought or what I was planning to do. I managed to salvage the situation by producing somewhat more brief correspondence based on the referral letter, testimony from my outpatient nurse (provided under admittedly pressured interrogation), the various tests I had arranged as evidenced by completed request cards and to a minor extent, my memory. Never again…
Bluetooth era
Current digital technology has allowed any tape to be superfluous; my Dictaphone requires only to be docked with my office PC and voice files appear instantly on my secretary’s screen – or another’s in her absence. And way beyond one’s own office, some hospitals outsource such files to far off lands where typists will convert your words to typed text, then to be returned electronically for printing and signing.
Much of my day-to-day, non-clinical correspondence I deal with electronically which must release my secretary a fair bit. Otherwise, I am blessed with someone whose clinical letters do not require checking or signing so, as with other colleagues, my correspondence is finished with the line “dictated but unsigned to avoid delay” or a similar choice of words that smacks of efficiency as well as tacitly complimenting my loyal assistant.
The logical extension of these various developments will be the use of voice recognition software in conjunction with a paperless environment. Any dictated letters, summaries or reports will be converted to text and then sent electronically to primary care, hospital colleagues or to filing.
My own small contribution to this revolution is the social use of a Dragon app on my iPhone with which I can dictate particularly long texts or emails. It does, however, require a quiet environment and clear pronunciation otherwise some of the words or phrases displayed in response to the sounds it hears are truly astonishing – if not potentially illegal.
So where does this leave our loyal secretaries? What will be her (or his) function in the future? The role of many is much more that of a PA but I forget; such a title is reserved of course for the assistants of “senior managers” rather than just consultants.
In their absence who will be our public face; dealing with patients’ queries and concerns over the phone, making excuses as to why you can’t get to a meeting because you are embroiled in an emergency (allegedly) or telling an irritating and persistent caller that she “will check if I’m in my office” while she can plainly see me gesticulating wildly in front of her that I’m not available?
Who will check train or flight times, rearrange clinics or make last minute adjustments to next week’s PCI list, because I forgot to tell her about a meeting I want to attend, a talk I am scheduled to give or even some well earned (sic) annual leave?
They are worth their weight in gold so show interest and support them, ask about their family and remember their birthday or wedding anniversary. You will not regret it and as a reward she might not only type your Oblique View column for the BJC but also, as in this case, actually write it for you!
Highlights of the American College of Cardiology (ACC) meeting held in San Francisco last month included the first study to show a benefit of treating ST-elevation myocardial infarction (STEMI) patients in community hospitals with fibrinolysis before transfer for percutaneous coronary intervention (PCI), as well as evidence supporting the use of PCI in hospitals without surgical back up. There were also positive results for eplerenone in MI, ranolazine in diabetes, and a new IV anti-platelet agent – cangrelor – in PCI. But perhaps the biggest story of the meeting was the removal of the PREVAIL trial from the programme at the last minute because of an embargo break by the sponsor.
PREVAIL not presented but eases safety concerns on Watchman
The PREVAIL trial of a new device which closes the left atrial appendage in the heart (Watchman®, Boston Scientific) attracted huge controversy at the ACC meeting when it was removed from the programme within an hour of its presentation because of an embargo break by the sponsor, Boston Scientific.
But the slides and a press release were still made available to the media, and preliminary results appear to suggest some reassurance on safety concerns generated in a previous study.
The device, which is implanted via a trans-septal catheter-based delivery system, is already available in Europe for the prevention of stroke in atrial fibrillation (AF) patients, but it has not been approved by the USA Food and Drug Administration (FDA) because of safety concerns raised in the previous PROTECT-AF trial. These related to a high initial rate of pericardial effusions and procedure-related strokes. The PREVAIL trial was therefore conducted to give more information on safety and to confirm the efficacy results shown in PROTECT-AF.
The PREVAIL trial enrolled 407 patients who were randomised 2:1 to the device or warfarin. Device patients were given 45 days of warfarin therapy. The study had a Bayesian design, which means that the PROTECT results were also taken into account when assessing efficacy. Results showed that the device had a 95.1% implant success rate, up from the 91% rate in PROTECT.
The trial had three co-primary end points, one for safety and two for efficacy. The safety end point was met, as was one of the efficacy end points; the other efficacy end point was narrowly missed. The efficacy results are, however, very preliminary, with only 58 device patients and 30 controls having reached the 18 month follow-up time.
The main safety end point – acute (seven-day) occurrence of death, ischaemic stroke, systemic embolism and procedure, or device-related complications requiring major cardiovascular or endovascular intervention – occurred in six out of 269 patients (2.2%) who received the device. A second, broader, safety end point, including cardiac perforation, pericardial effusion with tamponade, ischaemic stroke, device embolisation, and other vascular complications, occurred in 4.4% of patients receiving the device in PREVAIL, compared with 8.7% in PROTECT.
Cardiac perforation requiring surgical repair occurred in 0.4% of PREVAIL patients receiving the device compared with 1.6% in PROTECT-AF. Pericardial effusion with cardiac tamponade requiring pericardiocentesis occurred in 1.5% of Watchman patients in PREVAIL vs. 2.4% of those in PROTECT AF.
Speaking to the media, lead investigator Dr David Holmes (Mayo Clinic, Minnesota, USA) said: “Despite inclusion of higher-risk patients in PREVAIL than in PROTECT, there were fewer complications, and results show the device can be safely implanted by new operators. The Watchman device therefore offers an alternative to oral anticoagulation therapy for thromboembolic prevention in patients with nonvalvular AF”.
Independent commentator, Dr Gordon Tomaselli (Johns Hopkins University, Baltimore, USA), said he was reassured by the safety data in PREVAIL, and said he would use the device in patients at high risk of stroke who can’t take anticoagulant drugs because of bleeding issues. He added that there were not enough data yet to recommend its use in patients who could take anticoagulants.
HPS-THRIVE shows no reduction in events with niacin
Full results of the large-scale HPS2-THRIVE (Heart Protection Study 2-Treatment of HDL to Reduce the Incidence of Vascular Events) trial have shown no success in the use of extended-release niacin and the antiflushing agent laropiprant for the reduction of major vascular events in patients with well-controlled low-density lipoprotein (LDL) levels, but an increased rate of adverse effects.
The primary end point of the 25,000 patient trial, the combination of coronary death, nonfatal MI, stroke, or coronary revascularisation occurred in 15.0% of patients in the control arm and 14.5% of patients in the niacin/laropiprant arm, a difference that was not statistically significant. There was a 10% reduction in the risk of coronary revascularisation with niacin and laropiprant that just reached statistical significance, but none of the other components of the primary end point reached significance.
In terms of adverse events, the niacin/laropiprant combination was associated with a significant 3.7% absolute excess risk of diabetic complications, a significant 1.8% excess risk of new-onset diabetes, as well as an excess 1.4% higher risk of infection and a 0.7% higher risk of bleeding, including an increased risk of haemorrhagic stroke.
Lead investigator Dr Jane Armitage (Oxford University) said: “In light of these findings the role of extended-release niacin for the prevention of cardiovascular disease should be reconsidered.”
Chair of the study, Dr Rory Collins (Oxford University) added that given the side effects of niacin and the increased risk of serious adverse events, the evidence clearly suggests no benefit of niacin therapy. He added that doctors should instead be using higher doses of statins in order to achieve low levels of LDL cholesterol.
Niacin products “under review”
In response to the HPS-THRIVE results, the European Medicines Agency (EMA) has suspended all niacin/laropiprant products from sale. It has also announced a review of nicotinic acid and related substances, saying that the HPS2-THRIVE data may “have implications for medicines containing only nicotinic acid or related substances,” and it plans to issue an opinion on whether the marketing authorisations for these medicines should be maintained, varied, suspended, or withdrawn across the European Union.
Intensive glycaemic control ups heart failure risk
Both intensive glycaemic control and poor glycaemic control were associated with an increased risk of heart failure in diabetes patients in a new case-control study.
The study was conducted in the diabetic population of the GoDARTS registry. Cases were patients with heart failure defined as either a hospital discharge code for chronic heart failure or systolic dysfunction requiring a loop diuretic. They were matched with controls for gender and age at diabetes diagnosis. Cox-regression analysis was used to examine the link between mean HbA1c and time to chronic heart failure, accounting for all possible confounders.
Of 8,890 patients with diabetes, 759 developed heart failure during the study. Those with poor glycaemic control (HbA1c >6.9%) were twice as likely to develop heart failure (odds ratio 2.26; p<0.01).
However, intensive glycaemic control (HbA1c <6%) also appeared to be associated with a similar increased risk for heart failure (OR 2.48; p<0.01).
The incidence of coronary artery disease and myocardial infarction also increased when mean HbA1c was outside the range of 6–7%.
Presenting the results, Dr Helen Parry (University of Dundee) recommended that type 2 diabetes patients should aim for tight glycaemic control, keeping an HbA1c in the range of 6.0% to 6.9% if they want to reduce their risk of heart failure. But she added that achieving this level of control is not easy.
Dr Parry said the mechanism behind heart failure risk with intensive glycaemic control was probably multifactorial. She noted that heart failure has been associated with several classes of diabetes drugs, which are probably used more in this with intensive control, and that patients with low levels of HbA1c more often experience acute hypoglycaemic events.
TACT: no effect of high dose vitamins on CV events
Taking high-doses of oral vitamins did not reduce the risk of cardiovascular events, new results from TACT (Trial to Assess Chelation Therapy) have shown.
The trial, in 1,700 post-myocardial infarction patients, had a two by two factorial design, and has already reported positive results with chelation therapy. For the vitamin investigation, patients were randomised to a treatment including high doses of vitamins A, B, C, D, E, K, niacin, folate, calcium, magnesium, and zinc, or placebo.
Results showed that the vitamin therapy did not significantly reduce the time to first occurrence of death, MI, stroke, coronary revascularisation, or hospitalisation for angina, although there was 11% non-significant reduction.
When the use of vitamin therapy was combined with chelation and compared with patients who received only placebo, there was a statistically significant 26% relative reduction in the risk of the primary end point.
Chelation results published
The chelation part of TACT, which showed an 18% reduction in events for chelation alone versus placebo, was first reported at last year’s American Heart Association meeting. It has now also been published in the March 26 issue of JAMA (http://dx.doi.org/10.1001/jama.2013.2107). However, the study has been dogged with controversy.
In an editorial accompanying the publication (http://dx.doi.org/10.1001/jama.2013.2778), Dr Steven Nissen (Cleveland Clinic, USA) concludes: “Given the numerous concerns with this expensive, federally funded clinical trial, including missing data, potential investigator or patient unmasking, use of subjective end points, and intentional unblinding of the sponsor, the results cannot be accepted as reliable and do not demonstrate a benefit of chelation therapy.
At the ACC meeting, lead researcher, Dr Gervasio Lamas (Mount Sinai Medical Centre, Miami, US) was cautious about how the chelation results should be interpreted. “We’ve moved something from alternative medicine into scientific inquiry and found some results that merit further research. We don’t think the results of any single trial are enough to carry this novel hypothesis into daily use for patients who have had an acute myocardial infarction.”
REMINDER: eplerenone beneficial in MI?
The aldosterone blocker, eplerenone, started within the first day after an acute myocardial infarction (MI) in patients without heart failure or left ventricular dysfunction can improve outcomes, according to the results of the REMINDER trial.
But the trial generated some controversy, in that the only component of the complex composite primary endpoint to be significantly reduced was the level of natriuretic peptides.
The primary endpoint of the study included cardiovascular mortality, rehospitalisation, prolonged heart failure hospitalisation, sustained ventricular tachycardia or ventricular fibrillation, left ventricular ejection fraction (LVEF) <40% after one month, or levels of natriuretic peptides.
REMINDER (Impact of Eplerenone on Cardiovascular Outcomes in Patients Post Myocardial Infarction) included 1,012 STEMI patients, who received eplerenone 25–50 mg/day or placebo. Treatment started within the first 24 hours of symptom onset and preferably before myocardial reperfusion.
At a mean of 10.5 months follow-up, the composite primary end point occurred in 29.6% of the placebo group versus 18.4% in the eplerenone group (p<0.0001). Most of the benefit was attributable to the natriuretic peptide biomarker, which was raised in 25.9% of the placebo groups versus 16% of the eplerenone group (p<0.0002). There were, however, trends in favour of eplerenone for heart-failure rehospitalisation and ventricular arrhythmias.
Safety was good, with similar rates of hyperkalemia in the eplerenone and placebo groups, and hypokalaemia occurring more often in the control group, noted lead investigator Dr Gilles Montalescot (Pitié-Salpêtrière University Hospital, France).
Discussing the trial, Dr Magnus Ohman (Duke University, Kansas City, USA) noted that eplerenone was not well used for heart failure because of concerns about hyperkalaemia. REMINDER could be considered more of a safety study for eplerenone rather than an efficacy study, showing that eplerenone is safe when you exclude patients with renal failure, he said.
Dr Ohman added that the clinical significance of a natriuretic-peptide elevation after 30 days was not clear but that it might be a predictor of clinical outcomes in the future.
MASS COMM: elective PCI safe without surgical back up
Non-emergency percutaneous coronary intervention (PCI) can be performed safely in hospitals without on-site cardiac surgery, according to the results of the MASS COMM (PCI Outcomes in Community Versus Tertiary Settings) study.
The study, which was published online in the New England Journal of Medicine (http://dx.doi.org/10.1056/NEJMoa1300610) to coincide with its presentation at the ACC, included 3,691 patients who presented for elective PCI at a hospital without on-site cardiac surgery capabilities. They were randomised to receive PCI at the community hospital (2,774 patients) or to be transferred to a partner hospital with on-site cardiac surgery backup (917 patients).
Results showed that there was no difference in major adverse cardiac events (death, MI, repeat revascularisation, or stroke) at 30 days and 12 months when these patients were compared with those treated at hospitals with surgical back-up.
Presenting the data, Dr Alice Jacobs (Boston University School of Medicine, Boston, USA) said the results were in line with those of the C-PORT-E (Cardiovascular Patient Outcomes Research Team Elective Angioplasty) study. “These data suggest that PCI can be safely performed at hospitals without surgery on site, albeit with formal programmes and volume requirements, and that this could be an acceptable option for patients presenting to such hospitals,” she noted.
To participate in the study, hospitals had to perform a minimum of 300 diagnostic procedures in each of the previous two years, including 36 primary PCI procedures annually. The hospitals were also required to be within 60 minutes of a centre with 24 hour surgical backup, and physicians had to have performed a minimum of 75 PCI procedures annually.
Rivaroxaban: low risk of short treatment interruptions
Table 1. Clinical outcomes in patients with short treatment interruptions
Atrial fibrillation patients who stop taking rivaroxaban for a few days had a low risk of strokes or thrombotic events similar to that seen with similar interruptions of warfarin treatment, new results (see table 1) from the ROCKET-AF trial suggest.
In the analysis, a temporary interruption was defined as three days or more. Of the 14,236 patients in the study, 2,165 receiving rivaroxaban and 2,528 of those on warfarin stopped treatment at some point during the trial for an average duration of five days. The at -risk period was defined as three days after the drug was stopped until three days after the drug was restarted.
STREAM: success for fibrinolysis before transport for PCI
Fibrinolysis with tenecteplase and contemporary antithrombotic therapy given before transport to a hospital capable of percutaneous coronary intervention (PCI) is as effective as primary PCI in ST-elevation myocardial infarction (STEMI) patients presenting within three hours of symptom onset, according to the results of the STREAM (Strategic Reperfusion Early After Myocardial Infarction) trial.
Lead investigator, Dr Frans Van de Werf (University of Leuven, Belgium) said: “Fibrinolysis before transfer is at least as effective as PCI, and an urgent catheterisation was avoided in two-thirds of patients. This gives clinicians time to consider other options, such as coronary artery bypass graft (CABG) surgery and medical therapy.”
STREAM differs from other trials investigating fibrinolysis before transfer for PCI in that patients were only given urgent PCI on arrival at the tertiary hospital if they had not reperfused (as judged by the ECG). Because of this, the majority of patients avoided having to undergo PCI with fibrinolysis on board which has been associated with adverse outcomes in pervious studies.
Discussing the study, which was published online in the New England Journal of Medicine (http://dx.doi.org/10.1056/NEJMoa1301092) to coincide with the presentation, Dr Freek Verheugt (Nijmegen University, the Netherlands) said: ” I think this will change practice in certain parts of the world where there are long driving times to PCI hospitals.”
The trial involved 1,915 STEMI patients from 15 countries who were first seen in community hospitals or by emergency medical personnel, and for whom there was going to be a delay of over one hour before PCI could be performed. Before transfer, patients were randomised to PCI immediately after arrival or to tenecteplase plus enoxaparin, clopidogrel, and aspirin before arrival. Elderly patients had lower doses of clopidogrel (no loading dose) and enoxaparin.
When patients on tenecteplase reached a major medical centre, 36% needed urgent PCI. The other 64% of patients did not need urgent PCI and received an angiogram an average of 17 hours after arrival and, based on the results, received PCI or CABG under non-urgent circumstances.
Table 1. STREAM: primary endpoint
The primary end point (see table 1) – a composite of all-cause mortality, shock, congestive heart failure, and subsequent heart attack at 30 days – were similar between the immediate-PCI and tenecteplase groups.
Table 2. STREAM: ICH data
There was a significant increase in intracranial haemorrhage (ICH) in the fibrinolysis group, which led to the dose of tenecteplase being halved in people aged 75 years and older fairly early on in the course of the trial, after which the intracranial haemorrhage rate in the fibrinolysis group was reduced to 0.5% – not significantly different from the PCI group (see table 2). After the dosage amendment was made in the elderly, the primary end point almost reached significance in favor of the fibrinolysis group, Dr Van de Werf noted.
TERISA: ranolazine reduces angina in diabetics
The anti-anginal drug, ranolazine, is effective at reducing angina episodes specifically in patients with diabetes, the TERISA (Type 2 Diabetes Evaluation of Ranolazine in Subjects With Chronic Stable Angina) trial has shown.
Lead investigator, Dr Mikhail Kosiborod (Saint Luke’s Mid America Heart Institute, Kansas City, USA) noted that ranolazine is already approved as an anti-anginal but it was important to demonstrate a benefit in the particularly challenging diabetes population.
The study, which was simultaneously published online in the Journal of the American College Cardiology (http://dx.doi.org/10.1016/j.jacc.2013.02.011) to coincide with its ACC presentation, involved 949 type 2 diabetes patients who were randomised to a target dose of ranolazine 1,000 mg twice a day or placebo, for eight weeks. These patients had a high burden of angina, with around six to seven episodes per week, and were already receiving treatment with one or two anti-anginals.
The primary endpoint – average weekly angina frequency between weeks 2 and 8 – was significantly improved in the ranolazine group (3.8 episodes vs. 4.3 per week; p=0.008). Weekly use of rescue sublingual nitroglycerin was also lower among the ranolazine-treated patients (1.7 vs. 2.1 doses per week; p=0.003).
An editorial accompanying the publication (http://dx.doi.org/10.1016/j.jacc.2013.03.002) notes that the results confirm prior post hoc analyses of subgroups from the CARISA (Combination Assessment of Ranolazine in Stable Angina) and MERLIN-TIMI 36 (Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndromes) studies. But it adds that the absolute effects, although statistically significant, were small, with only 0.5 fewer episodes of angina and 0.4 fewer sublingual nitroglycerin tablets used per week. “The clinical relevance of such slight absolute differences may be questioned,” it concludes.
CHAMPION-PHOENIX: cangrelor looks good for acute use in PCI
The new intravenous antiplatelet agent, cangrelor, reduced the risk of periprocedural complications of percutaneous coronary intervention (PCI) compared with clopidogrel in CHAMPION-PHOENIX (Clinical Trial Comparing Cangrelor to Clopidogrel Standard Therapy in Subjects Who Require PCI).
The trial, which was simultaneously published online in the New England Journal of Medicine (http://dx.doi.org/10.1056/NEJMoa1300815), randomised 11,145 patients undergoing urgent or elective PCI to receive cangrelor (30 µg/kg bolus followed by a 4 µg/kg/min infusion for at least two hours) or a 600-mg or 300-mg loading dose of clopidogrel.
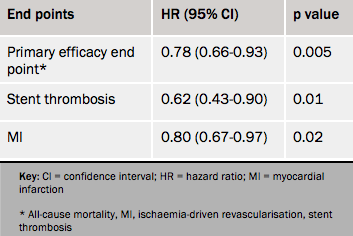
Table 1. Efficacy outcomes at 48 hours, cangrelor vs. clopidogrel
Results (see table 1) showed a 22% reduction in the composite efficacy end point with cangrelor, driven by reductions in myocardial infarction and stent thrombosis.
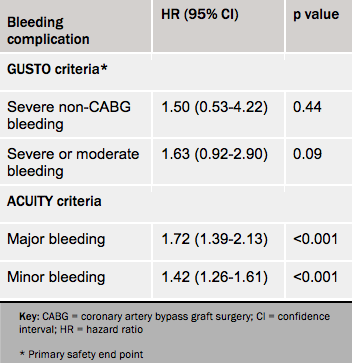
Bleeding complications as prospectively defined according to the GUSTO criteria were not increased, but when defined using the more sensitive ACUITY definitions, there was more bleeding with cangrelor than with clopidogrel (see table 2).
Co-principal investigator, Dr Deepak L Bhatt (Brigham and Women’s Hospital, Boston, USA) told a press conference that one of the main advantages of cangrelor was its short-acting nature which gave the flexibility to initiate and rapidly stop platelet inhibition, in case the patient requires surgery or develops bleeding complications.
Table 2. Bleeding complications by different bleeding criteria, cangrelor vs. clopidogrel
However, an editorial accompanying the publication (http://dx.doi.org/10.1056/
NEJMe1302504) points out some problems with the study – namely that the full antiplatelet effects of cangrelor were operative before and during PCI, whereas 37% of patients in the clopidogrel group received the drug during or after PCI; and that many patients received clopidogrel at the inferior 300 mg dose. Given these points, the routine use of cangrelor for all patients undergoing PCI is not yet justified, it concludes.
The Scottish Heart and Arterial disease Risk Prevention (SHARP) charity has aimed to reduce and prevent premature morbidity and mortality from cardiovascular disease in Scotland since its formation. The recent SHARP Annual Scientific Meeting – held on November 22nd–23rd 2012 in Dunkeld – highlighted the SHARP prize, initiated two years ago to encourage young researchers. Dr Alan Begg reports.
Encouraging young researchers
Death rates from coronary heart disease (CHD) are falling across the UK, but the rates remain high in Scotland with a slower rate of decline than the rest of the devolved nations.1 A recent Audit Scotland report has highlighted that although death rates of all types of heart disease have reduced by around 40% in the past 10 years, they remain the second highest cause of death after cancer.1 Between 1991 and 1996 the SHARP mobile screening unit successfully screened 19,400 Scots between the ages of 18 and 70 years, mainly at their place of work. Currently 14,694 people remain alive on this database, all of whom are available for data linking with the information available for SHARP members to use for their own research.
One of the most popular sessions of the recent meeting was the SHARP prize presentations, where a real sense of achievement was apparent in the young researchers. The prize is intended to help them develop their work, and presenting at our annual meeting gave them the opportunity to discuss developing their project further with other researchers attending the meeting.
Their six abstracts presented are published below. Congratulations to Naveed Akbar (Ninewells Hospital, Dundee) who was the 2012 SHARP Prize winner.
The enthusiasm for the SHARP organisation remains strong and promotion of the SHARP prize is an important component of our approach in reducing the long-term burden of cardiovascular disease. Although not unique, this prize will continue in 2013 with £500 being available to the winner to attend either national or international conferences. For further details, contact [email protected]
Strengthening long-term links between academic medicine and healthcare delivery has been highlighted in a report from the Academy of Medical Sciences.2 Our aim should be a clinical workforce able to utilise research for patient benefit and non-academic clinicians have an important role within their programmed activity, mentoring these aspiring researchers.
2012 SHARP prize abstracts
Chronic inflammation and cardiovascular disease: a need for better cholesterol management?
Presented by Naveed Akbar, PhD Student, Vascular and Inflammatory Diseases Research Unit, Ninewells Hospital and Medical School, University of Dundee
Chronic inflammation is associated with adverse cardiovascular events. However, significant disease heterogeneity exists within disease cohorts. Thus there is an urgent need to better understand the pathophysiology owing to these differences.
We demonstrate that a single protein mutation (ABIN-1), fundamental in the normal regulation of cytokine expression through nuclear factor kappa-beta (NF-κβ) induces autoimmune disease, cardiac hypertrophy, vascular dysfunction and produces increased oxidative stress in mice; which are further exacerbated by hypercholesterolaemia.
Our data provides a novel insight into cellular signalling in chronic inflammation and subsequent cardiovascular health, suggesting a need for more stringent management of cholesterol in inflammatory diseases.
Changing patterns in the diagnosis of ACS in Scotland since 2000
Presented by SJ Wilson (Royal Infirmary of Edinburgh) on behalf of NHS Information and Statistics Division
We assessed the impact of the publication of the European/American Universal Definition of Myocardial Infarction (2000 and 2007), the Scottish Cardiac Society vote (2008) to support this and the introduction of sensitive troponin assays (2007) on the epidemiology of acute coronary syndrome (ACS) in Scotland since 2000.
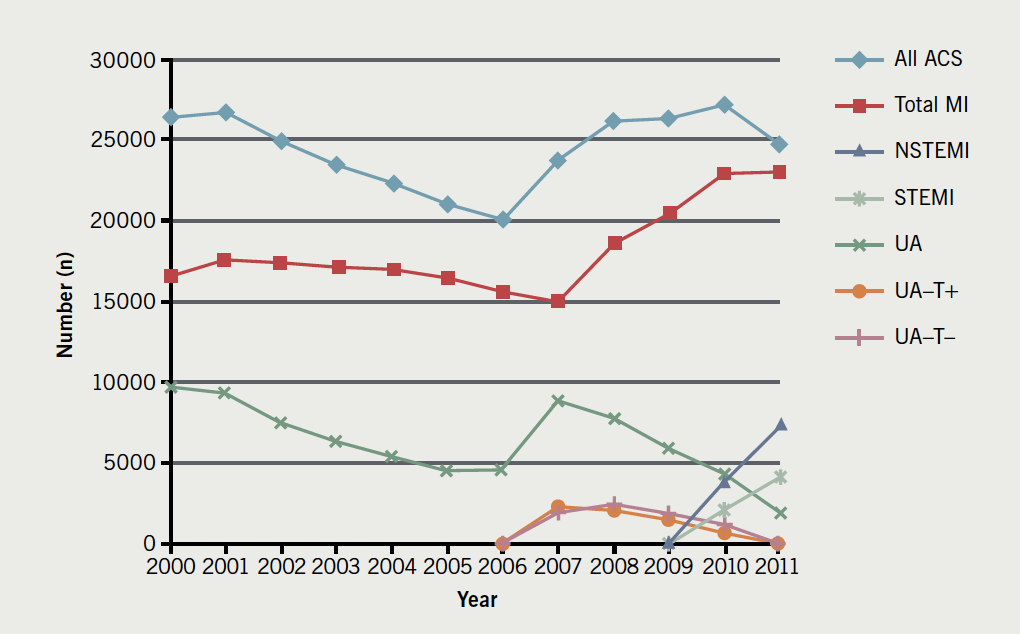
Figure 1 shows that between 2000–2011 the incidence of myocardial infarction (MI) increased by 38% and unstable angina decreased by 81%, most dramatically following the majority of these changes in practice between 2007–2008. During this time, 30-day mortality for MI fell from 16.2 to 9.26%. These changes in the diagnosis/classification of patients with ACS correlate with major reductions in mortality.
Figure 1. Annual hospital admissions in Scotland for acute coronary syndrome
Improving the palliative care pathway for patients with chronic heart failure
Presented by A Ness, Western General Nurse, Crewe Road South, Edinburgh
We aimed to ensure that patients with chronic heart failure, who have palliative care needs are identified early in their disease trajectory and to promote a multi-disciplinary, anticipatory approach to patient care.
A communication tool, utilising clinical indicators adapted from the existing Gold Standards Framework, was developed to identify patients who would benefit from a palliative care approach. This was then shared with the care team.
The use of a communication tool was shown to prompt clinicians to deliver palliative care to patients with advanced heart failure and ensured earlier, open discussion between patients/carers/clinicians regarding future treatment options.
Preliminary investigation into the benefits of imaging myocardial fat using MRI
Presented by DB Cassidy, SJ Gandy, P Martin, S Mathew, RS Nicholas and JG Houston, Ninewells Hospital and Medical School, University of Dundee
Lipid over-storage in human cardiac myocytes is an early manifestation in the pathogenesis of type 2 diabetes mellitus. Magnetic resonance imaging (MRI) has become gold standard in cardiac functional and structural assessments but other novel fat imaging techniques may provide additional prognostic information.
This study involved the investigation of multiecho fat-water separation technique in cardiac MRI using a healthy volunteers and diabetes cohort.
The ability of MRI to discriminate between water and fat in cardiac imaging may prove beneficial for characterising conditions such as cardiac masses, myocardial lipomatous infiltration and evaluation of inflammatory responses such as pericarditis leading to improvements in heart and diabetes management.
Observer reproducibility in WB-MRA cardiovascular analysis
Presented by L McCormick, the Institute of Cardiovascular Research, University of Dundee
Contrast-enhanced whole-body magnetic resonance angiography (WB-MRA) enables cardiovascular analysis of the entire arterial tree excluding the coronary vessels, enabling characterisation of atherosclerotic disease on a systemic level. As part of on-going work in WB-MRA analysis, this study examines reproducibility and variability in radiological stenosis quantification between four observers, and therefore the extent to which different observers influence cardiovascular assessment of images in both single site and whole-body atherosclerosis scoring. Analysis was performed on 159 sites for each of 20 patients. Reproducibility between observers was substantial, while a significant degree of variability between observers was found, suggesting a need for improved analysis techniques.
Sensitive troponin assays and clinical specificity for the diagnosis of myocardial infarction
Presented by ASV Shah, BHF Centre for Cardiovascular Science, Edinburgh University
Lowering the diagnostic threshold for myocardial infarction (MI) using more sensitive troponin assays will reduce clinical specificity. As such, the universal definition of MI recommends classification to differentiate between primary and secondary causes of myocardial injury.
At a regional cardiac centre all consecutive patients with elevated cardiac troponin concentrations (>0.05 ng/mL; n=2,930), irrespective of clinical presentation, were classified as type I-V MI by two independent cardiologists before (validation phase; six months) and after (implementation phase; six months) lowering the threshold of detection for myocardial necrosis from 0.20 to 0.05 ng/mL with a sensitive troponin I assay. During the validation phase, only concentrations above the original diagnostic threshold of ≥0.20 ng/mL were reported to clinicians.
Results showed 50% of patients (n=1,171) had a primary MI (type I), 48% (n=1,108) had secondary causes of MI (type II) and 2% (n=43) had sudden cardiac death or procedural related MI (type III-V). Lowering the diagnostic threshold from 0.20 to 0.05 ng/mL increased the diagnosis of type I MI by 22% (259/1,171) and type II MI by 61% (673/1,108). At one year, patients with type II MI were less likely than patients with type I MI to have a recurrent MI (4% versus 12%, OR 0.30, 95% CI 0.21–0.42), but more likely to be dead (37% versus 16%, OR 2.52, 95% CI 3.07–3.74). In patients with troponin 0.05–0.19 ng/mL lowering the diagnostic threshold in the implementation phase was associated with a reduction in recurrent MI and death at one year in patients with type I MI (31% versus 17%, p=0.009), but no significant change in outcome for patients with type II MI (36% versus 29%, p=0.090).
We conclude that secondary myocardial injury is as common as primary myocardial infarction in clinical practice. Whilst implementation of a sensitive troponin assay was associated with better clinical outcomes for patients with type I MI, the number of patients with type II MI increased by more than 50% with a major impact on cardiac services and no clear benefit for these patients.
2. Building clinical academic capacity and the allocation of resources across academic specialties. The Academy of Medical Sciences 2009. ISBN: 978-1903401194
Authors: Dr Justin Williamson; Drs Toby Rogers, Jonathan Hill, and Khaled Alfakih
First published online April 23rd 2013
Correspondence from the world of cardiology
Feasibility of using CTCA in patients with acute low-to-intermediate likelihood chest pain in a DGH
Dear Sirs,
I would like to make three points about this paper:1
1. The summary states “results suggest that it is feasible to use computed tomography coronary angiography (CTCA)…in place of exercise tolerance testing (ETT) at no extra cost”. The body of the article shows “CTCA had a higher cost compared with ETT. The overall cost per patient was £375 with CTCA vs. £309 with ETT, but this was not statistically significant (p=0.28)”. The lack of significance is attributable to the small size of the data-set, and it does not allow a contrary conclusion to be drawn. The statement in the summary is not an acceptable conclusion to draw from the results in the body of the paper.
Furthermore, the cost analysis was based on guesswork about the cost of CTCA. The analysis for CTCA is much more complicated than for CT pulmonary angiogram (CTPA). As a result the cost would be expected to be higher. To guess that it would be the same makes the entire cost analysis suspect.
2. The discussion states “CTCA is a safe and non-invasive diagnostic tool”. There is no statement about complications (or lack of) in the results. Clearly there is a small but real risk of contrast nephropathy and contrast allergy. This risk is absent in the ETT arm.
Furthermore, the effectiveness of diagnostic tools ideally needs assessment against outcome. This is entirely missing in the study. Instead, some of the patients received invasive coronary angiography (ICA). Catheter angiography is not a good gold standard – patients have significant cardiac events with normal coronary artery angiography2 and subgroups of patients with abnormal coronary artery angiography have excellent outcomes without intervention.3
3. The discussion states: “Prospective gating, which is available on all modern 64-slice CT scanners, reduces the radiation dose to 2–3 mSv. This is a fraction of the radiation dose of single-photon emission computed tomography (SPECT) perfusion.” This is not correct. Just as CTCA has progressed to prospective gating, there have been technical changes in SPECT perfusion scanning. SPECT scanners currently being sold and commonly in use have radiation dose as little as 1 mSv per scan.4
My personal opinion is that any multi-centre trial needs to be based on outcome data, rather than an imperfect gold standard.
Justin Williamson
Nuclear Medicine Specialist
Hastings Memorial Hospital, Hastings, New Zealand ([email protected])
References
1. Michael Michail, Shubra Sinha, Mohamed Albarjas, et al. Feasibility of using CTCA in patients with acute low-to-intermediate likelihood chest pain in a DGH. Br J Cardiol 2013;20:39. http://dx.doi.org/10.5837/bjc.2013.002
2. Larsen A, et al. Long-term prognosis of patients presenting with ST-segment elevation myocardial infarction with no significant coronary artery disease (from the HORIZONS-AMI trial). Am J Cardiol 2013;111:643–8. http://dx.doi.org/10.1016/j.amjcard.2012.11.011
3. Kostkiewicz M, et al. The prognostic value of normal myocardial perfusion SPECT with positive coronary angiography. Nuclear Med Rev 2012;15:22–5. http://dx.doi.org/10.5603/nmr-18726
4. Jeffrey A, Ron E, Howard B, et al. Comparison of image quality, myocardial perfusion, and left ventricular function between ultra-low-dose imaging using a high-efficiency solid-state SPECT camera and standard low-cose imaging using an Anger SPECT camera: results from the multicenter nuclear low-dose imaging at a millisievert study. J Am Coll Cardiol 2013;61:E1007. http://dx.doi.org/10.1016/S0735-1097(13)61007-4
The authors’ reply
We are grateful to Dr Williamson for his comments. In response:
1. We acknowledge that our study was a feasibility study in a single centre with retrospective comparison of ETT vs. CTCA. The cost analysis demonstrates that the overall cost of using CTCA as an initial test is similar to ETT, because ETT leads to more second-line testing, which offsets the difference in cost of the actual test. Furthermore, if all the patients with equivocal ETT were investigated further, the overall cost of the ETT strategy would have been higher. Our pricing of CTCA was a local estimate based on the cost of CT scanner time, contrast, radiographer and the radiologist/cardiologist time.
With a good quality study and modern semi-automated coronary analysis tools, reporting time is short, particularly in patients with normal coronary arteries. The National Institute of Health and Clinical Excellence (NICE) estimated the cost of CTCA in a recent cost analysis to be £175, which is close to our estimate.1
2. We did not collect long-term outcome data. However, there are several on-going large multi-centre clinical trials comparing CTCA vs. SPECT, including outcomes, which will report over the coming few years.2
3. The new developments in SPECT perfusion which Dr Williamson describes are clearly very important, particularly as another publication by Einstein et al. describes patients undergoing multiple SPECT studies over a 20 year period, accumulating a total of 121 msv of radiation in the process.3
Dr Toby Rogers
SpR in Cardiology
Dr Jonathan Hill
Consultant Cardiologist
Dr Khaled Alfakih
Consultant Cardiologist
King’s College Hospital, Denmark Hill, London, SE5 9RS
References
1. Chest pain of recent onset, CG95. Costing report: implementing NICE guidance. National Institute of Health and Clinical Excellence (NICE) 2011. Available from http://www.nice.org.uk/nicemedia/live/12947/55738/55738.pdf (accessed 09/04/13)
2. PROspective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE). Study record detail, ClinicalTrials.gov (Last updated: February 21, 2013). Available from http://clinicaltrials.gov/ct2/show/NCT01174550 (accessed 09/04/13)
3. Einstein AJ, Weiner SD, Bernheim A, et al. Multiple testing, cumulative radiation dose, and clinical indications in patients undergoing myocardial perfusion imaging. J Am Med Assoc 2010;304:2137–44. http://dx.doi.org/10.1001/jama.2010.1664 (accessed 09/04/13)
Treatment of chronic heart failure (HF) is underpinned by a firm evidence base. The same cannot be said for most acute HF but this may be set to change, as discussed at the British Society for Heart Failure (BSH) Annual Day for Training and Revalidation. Held on February 7th 2013, at the Wellcome Collection Conference Centre, London, this meeting included a number of excellent presentations and interactive case-based discussions focussing on particularly challenging and controversial issues. Dr Michael Pope reports on some of the highlights.
A new treatment for acute heart failure?
The recently published RELAX-AHF (Efficacy and Safety of Relaxin for the Treatment of Acute Heart Failure) study was a prospective, randomised, double-blind, placebo-controlled trial carried out in a targeted population of patients with acute HF.1 Relaxin is a physiological hormone that regulates maternal adaptations to pregnancy, increasing cardiac output, renal blood flow, and arterial compliance, alongside decreased peripheral vascular resistance.2,3 Serelaxin is a recombinant human relaxin-2 shown to have beneficial effects on symptoms and outcomes in early studies.4
The primary end points in this study were measures of patient reported dyspnoea at six, 12, and 24 hours. According to the visual analogue scale area under the curve (AUC), serelaxin significantly improved symptoms. Most intriguing was the unexpected finding that serelaxin was associated with significantly reduced cardiovascular and all-cause mortality at 180 days. Furthermore, serelaxin was associated with decreased use of intravenous loop diuretics, decreased length of initial hospital stay, and of intensive care or cardiac care days.
Many aspects of these results, however, preclude us from declaring serelaxin the new ‘wonder drug’. Professor Theresa McDonagh (King’s College London) pointed out that this HF patient population, by nature of the exclusion of patients with a systolic blood pressure ≤125 mmHg creates a fairly low risk population making it difficult to extrapolate the findings to other patients.
Equally, it’s difficult to translate statistical significance into actual clinical significance. In particular, a “448 mm x h” increase in AUC seems an obscure measurement of genuine improvement in dyspnoea. Nonetheless, the finding is supported by the decreased use of diuretics, and fewer patients experiencing worsening heart failure in the serelaxin-treated group. The data regarding 180-day mortality also needs to be interpreted cautiously.
Professor John McMurray (University of Glasgow) highlighted the delicacy of the statistical significance when the number of events is small, the trial not powered for this analysis, and this was not a pre-specified primary end point. Furthermore, this result is not supported by the hospitalisation statistics, which show no significant difference in death or readmission at either 30 or 60 days.
Professor McMurray also contrasted these results with that of the ASCEND-HF (Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure) trial of the novel drug nesiritide, a recombinant B-type natriuretic peptide.5 This demonstrated no significant difference in dyspnoea or 30 day outcomes between nesiritide and placebo, in combination with standard therapies. Nesiritide however was associated with increased rates of hypotension.
The measurement used for dyspnoea here was the Likert scale, which although showing a trend towards improved dyspnoea, did not reach statistical significance. This was also found with serelaxin, which only reached statistical significance when measured using the AUC on the visual analogue scale.
Nevertheless, the findings are potentially exciting, demonstrate the clinical safety of serelaxin, and suggest interesting potential for this new therapy. Further studies are awaited with considerable interest.
The next Heart Failure Day for Training and Revalidation will take place on 20th March 2014, in Glasgow.
The BSH also gratefully acknowledges the support provided by the Friends of BSH: Alere, Edwards Lifesciences, HeartWare, Medtronic, Novartis, Pfizer, Servier, St. Jude Medical and Thoratec.
If you would like more information about the British Society for Heart Failure, please contact [email protected], or visit the website at www.bsh.org.uk
1. Teerlink JR, Cotter G, Davison BA, et al. Serelaxin, recombinant human relaxin-2, for treatment of acute heart failure (RELAX-AHF): a randomised, placebo-controlled trial. Lancet 2013;381:5–11. http://dx.doi.org/10.1016/S0140-6736(12)61855-8
2. Conrad KP. Maternal vasodilation in pregnancy: the emerging role of relaxin. Am J Physiol Regul Integr Comp Physiol 2011;301:R267–R275. http://dx.doi.org/10.1152/ajpregu.00156.2011
3. Teichman SL, Unemori E, Teerlink JR, Cotter G, Metra M. Relaxin: review of biology and potential role in treating heart failure. Curr Heart Fail Rep 2010;7:75–82. http://dx.doi.org/10.1007/s11897-010-0010-z
4. Teerlink JR, Metra M, Felker GM et al. Relaxin for the treatment of patients with acute heart failure (Pre-RELAX-AHF): a multicentre, randomised, placebo-controlled, parallel-group, dose-finding phase IIb study. Lancet 2009;373:1429–39. http://dx.doi.org/10.1016/S0140-6736(09)60622-X
5. O’Connor CM, Starling RC, Hernandez AF, et al. Effect of nesiritide in patients with acute decompensated heart failure. N Engl J Med 2011;365:32–43. http://dx.doi.org/10.1056/NEJMoa1100171
Practical handbook of advanced interventional cardiology: tips and tricks (4th edition)
Authors: Nguyen T, Hu D, Chen SL, et al.
Publisher: Wiley-Blackwell, 2012
ISBN: 9780470670477
Price: £62.99
This helpful, practical guide to interventional cardiology focuses on procedural and technical aspects rather than the overall clinical practice approach usually seen in larger textbooks. It assumes that clinical decision-making prior to starting the procedure has been sound, and approaches things from the perspective of already having a patient on the table.
The content and chapters are fairly comprehensive and logical in their order, with increasingly complex or less commonly performed procedures towards the end of the book. I would have liked a specific chapter on rotational atherectomy and also perhaps one on some adjunctive methods to evaluate stenoses.
The style is generally easy to read and, although the descriptions of certain practical manoeuvres could be hard to follow (and are at times quite lengthy), stepwise illustrations help to explain these. I do think that extensive descriptions were required to adequately explain the use of certain equipment and so on. Despite their length, these probably improve the readers’ chances of successfully employing the techniques themselves.
The ‘tricks and tips’ suggested have sometimes been ranked according to cost, safety, and technical difficulty, which are delineated by symbols throughout the book. Although I didn’t feel this was particularly necessary, as such things may be obvious to most practitioners, I did appreciate this more in the ‘tactical move’ sections. These illustrate a stepwise technical problem-solving approach, starting with the simplest/cheapest and escalating appropriately. The ‘caveat’ sections are also relevant, helpful, and would be of particular use to less experienced operators.
Probably the best aspect of this book is the unbiased and detailed descriptions of contemporary interventional cath lab equipment, with illustrations in many cases. I was impressed with the range of devices that are discussed and the level of detail and practical information regarding their use/limitations. This really was an outstanding feature and would be useful both to trainees employing these for the first time as well as for experienced operators as an ‘aide-mémoire’.
Overall, this is an excellent practical handbook. It is both easy and useful to read sequentially for educational purposes but also has a role as a quick-reference guide. I would certainly recommend it to other interventional trainees and consultants.
Dr Kristel C Longman ST7 Cardiology Department of Cardiology, Portsmouth Hospitals NHS Trust
This book provides a state-of-the-art review of the theoretical and practical aspects of bifurcation stenting. The editors have successfully brought together 54 contributors to compile an extensive body of evidence that takes the reader through basic bifurcation techniques, major clinical trials in bifurcation stenting, adjunctive imaging modalities and the rapidly expanding field of dedicated bifurcation stents. The organisation is meticulous, the layout is exquisite and the text is packed with robust scientific evidence.
The first chapter introduces the reader to the classification of bifurcation stenting. This is followed by five chapters on the several available techniques and landmark trials that have helped shape clinical practice in recent years. Importantly, a separate chapter is dedicated to left main stem bifurcation stenting. All major trials are described in a careful, structured manner, educating the reader about the evidence that each trial contributed.
The following seven chapters describe the use of adjunctive imaging modalities – for example, intravascular ultrasound and optical coherence tomography – in bifurcation stenting. Other chapters cover the basic pathophysiology of plaque development at coronary bifurcations, principles of bench model testing, and the role of quantitative angiography.
The final six chapters take the reader through the exciting and rapidly expanding field of dedicated bifurcation platforms. Each dedicated bifurcation stent has a separate chapter that describes the device, the method of deployment and indications for use. As these devices are relatively new, careful attention has been given to provide a step-bystep approach on the methodology and indications for each dedicated bifurcation stent. Each chapter also includes up-to-date scientific evidence summarising mechanistic and population-based prospective studies.
My only criticism is that some of the black and white angiogram images can be difficult to appreciate and perhaps can be improved upon in any subsequent editions. Finally, a notable omission from the book is the TrytonTM stent which has gained approval for clinical use in bifurcation lesions and is currently being investigated in a left main stem registry.
The editors and contributors ought to be congratulated in providing such an in-depth yet easy-to-read book on this subject, which will undoubtedly serve as an excellent and timely addition to the field of interventional cardiology.
Dr Omar Rana Fellow in Interventional Cardiology Royal Bournemouth Hospital, Bournemouth BH7 7DW
You are not logged in
You need to be a member to print this page.
Find out more about our membership benefits