The Scottish Heart and Arterial disease Risk Prevention (SHARP) charity has aimed to reduce and prevent premature morbidity and mortality from cardiovascular disease in Scotland since its formation. The recent SHARP Annual Scientific Meeting – held on November 22nd–23rd 2012 in Dunkeld – highlighted the SHARP prize, initiated two years ago to encourage young researchers. Dr Alan Begg reports.
Encouraging young researchers
![]() Death rates from coronary heart disease (CHD) are falling across the UK, but the rates remain high in Scotland with a slower rate of decline than the rest of the devolved nations.1 A recent Audit Scotland report has highlighted that although death rates of all types of heart disease have reduced by around 40% in the past 10 years, they remain the second highest cause of death after cancer.1 Between 1991 and 1996 the SHARP mobile screening unit successfully screened 19,400 Scots between the ages of 18 and 70 years, mainly at their place of work. Currently 14,694 people remain alive on this database, all of whom are available for data linking with the information available for SHARP members to use for their own research.
Death rates from coronary heart disease (CHD) are falling across the UK, but the rates remain high in Scotland with a slower rate of decline than the rest of the devolved nations.1 A recent Audit Scotland report has highlighted that although death rates of all types of heart disease have reduced by around 40% in the past 10 years, they remain the second highest cause of death after cancer.1 Between 1991 and 1996 the SHARP mobile screening unit successfully screened 19,400 Scots between the ages of 18 and 70 years, mainly at their place of work. Currently 14,694 people remain alive on this database, all of whom are available for data linking with the information available for SHARP members to use for their own research.
One of the most popular sessions of the recent meeting was the SHARP prize presentations, where a real sense of achievement was apparent in the young researchers. The prize is intended to help them develop their work, and presenting at our annual meeting gave them the opportunity to discuss developing their project further with other researchers attending the meeting.
Their six abstracts presented are published below. Congratulations to Naveed Akbar (Ninewells Hospital, Dundee) who was the 2012 SHARP Prize winner.
The enthusiasm for the SHARP organisation remains strong and promotion of the SHARP prize is an important component of our approach in reducing the long-term burden of cardiovascular disease. Although not unique, this prize will continue in 2013 with £500 being available to the winner to attend either national or international conferences. For further details, contact [email protected]
Strengthening long-term links between academic medicine and healthcare delivery has been highlighted in a report from the Academy of Medical Sciences.2 Our aim should be a clinical workforce able to utilise research for patient benefit and non-academic clinicians have an important role within their programmed activity, mentoring these aspiring researchers.
2012 SHARP prize abstracts
Chronic inflammation and cardiovascular disease: a need for better cholesterol management?
Presented by Naveed Akbar, PhD Student, Vascular and Inflammatory Diseases Research Unit, Ninewells Hospital and Medical School, University of Dundee
Chronic inflammation is associated with adverse cardiovascular events. However, significant disease heterogeneity exists within disease cohorts. Thus there is an urgent need to better understand the pathophysiology owing to these differences.
We demonstrate that a single protein mutation (ABIN-1), fundamental in the normal regulation of cytokine expression through nuclear factor kappa-beta (NF-κβ) induces autoimmune disease, cardiac hypertrophy, vascular dysfunction and produces increased oxidative stress in mice; which are further exacerbated by hypercholesterolaemia.
Our data provides a novel insight into cellular signalling in chronic inflammation and subsequent cardiovascular health, suggesting a need for more stringent management of cholesterol in inflammatory diseases.
Changing patterns in the diagnosis of ACS in Scotland since 2000
Presented by SJ Wilson (Royal Infirmary of Edinburgh) on behalf of NHS Information and Statistics Division
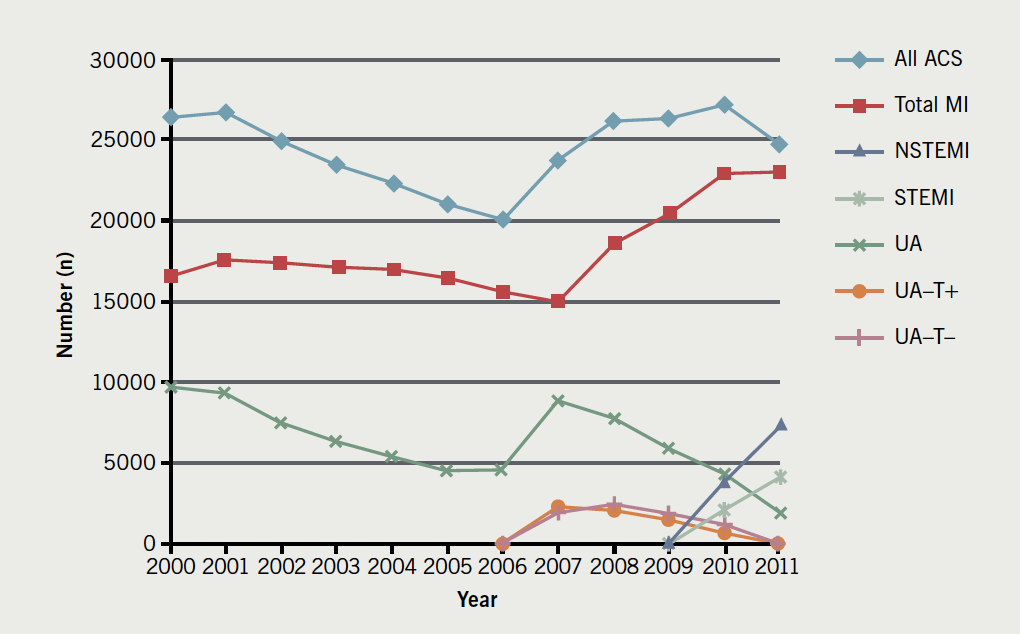
We assessed the impact of the publication of the European/American Universal Definition of Myocardial Infarction (2000 and 2007), the Scottish Cardiac Society vote (2008) to support this and the introduction of sensitive troponin assays (2007) on the epidemiology of acute coronary syndrome (ACS) in Scotland since 2000.
Figure 1 shows that between 2000–2011 the incidence of myocardial infarction (MI) increased by 38% and unstable angina decreased by 81%, most dramatically following the majority of these changes in practice between 2007–2008. During this time, 30-day mortality for MI fell from 16.2 to 9.26%. These changes in the diagnosis/classification of patients with ACS correlate with major reductions in mortality.
Improving the palliative care pathway for patients with chronic heart failure
Presented by A Ness, Western General Nurse, Crewe Road South, Edinburgh
We aimed to ensure that patients with chronic heart failure, who have palliative care needs are identified early in their disease trajectory and to promote a multi-disciplinary, anticipatory approach to patient care.
A communication tool, utilising clinical indicators adapted from the existing Gold Standards Framework, was developed to identify patients who would benefit from a palliative care approach. This was then shared with the care team.
The use of a communication tool was shown to prompt clinicians to deliver palliative care to patients with advanced heart failure and ensured earlier, open discussion between patients/carers/clinicians regarding future treatment options.
Preliminary investigation into the benefits of imaging myocardial fat using MRI
Presented by DB Cassidy, SJ Gandy, P Martin, S Mathew, RS Nicholas and JG Houston, Ninewells Hospital and Medical School, University of Dundee
Lipid over-storage in human cardiac myocytes is an early manifestation in the pathogenesis of type 2 diabetes mellitus. Magnetic resonance imaging (MRI) has become gold standard in cardiac functional and structural assessments but other novel fat imaging techniques may provide additional prognostic information.
This study involved the investigation of multiecho fat-water separation technique in cardiac MRI using a healthy volunteers and diabetes cohort.
The ability of MRI to discriminate between water and fat in cardiac imaging may prove beneficial for characterising conditions such as cardiac masses, myocardial lipomatous infiltration and evaluation of inflammatory responses such as pericarditis leading to improvements in heart and diabetes management.
Observer reproducibility in WB-MRA cardiovascular analysis
Presented by L McCormick, the Institute of Cardiovascular Research, University of Dundee
Contrast-enhanced whole-body magnetic resonance angiography (WB-MRA) enables cardiovascular analysis of the entire arterial tree excluding the coronary vessels, enabling characterisation of atherosclerotic disease on a systemic level. As part of on-going work in WB-MRA analysis, this study examines reproducibility and variability in radiological stenosis quantification between four observers, and therefore the extent to which different observers influence cardiovascular assessment of images in both single site and whole-body atherosclerosis scoring. Analysis was performed on 159 sites for each of 20 patients. Reproducibility between observers was substantial, while a significant degree of variability between observers was found, suggesting a need for improved analysis techniques.
Sensitive troponin assays and clinical specificity for the diagnosis of myocardial infarction
Presented by ASV Shah, BHF Centre for Cardiovascular Science, Edinburgh University
Lowering the diagnostic threshold for myocardial infarction (MI) using more sensitive troponin assays will reduce clinical specificity. As such, the universal definition of MI recommends classification to differentiate between primary and secondary causes of myocardial injury.
At a regional cardiac centre all consecutive patients with elevated cardiac troponin concentrations (>0.05 ng/mL; n=2,930), irrespective of clinical presentation, were classified as type I-V MI by two independent cardiologists before (validation phase; six months) and after (implementation phase; six months) lowering the threshold of detection for myocardial necrosis from 0.20 to 0.05 ng/mL with a sensitive troponin I assay. During the validation phase, only concentrations above the original diagnostic threshold of ≥0.20 ng/mL were reported to clinicians.
Results showed 50% of patients (n=1,171) had a primary MI (type I), 48% (n=1,108) had secondary causes of MI (type II) and 2% (n=43) had sudden cardiac death or procedural related MI (type III-V). Lowering the diagnostic threshold from 0.20 to 0.05 ng/mL increased the diagnosis of type I MI by 22% (259/1,171) and type II MI by 61% (673/1,108). At one year, patients with type II MI were less likely than patients with type I MI to have a recurrent MI (4% versus 12%, OR 0.30, 95% CI 0.21–0.42), but more likely to be dead (37% versus 16%, OR 2.52, 95% CI 3.07–3.74). In patients with troponin 0.05–0.19 ng/mL lowering the diagnostic threshold in the implementation phase was associated with a reduction in recurrent MI and death at one year in patients with type I MI (31% versus 17%, p=0.009), but no significant change in outcome for patients with type II MI (36% versus 29%, p=0.090).
We conclude that secondary myocardial injury is as common as primary myocardial infarction in clinical practice. Whilst implementation of a sensitive troponin assay was associated with better clinical outcomes for patients with type I MI, the number of patients with type II MI increased by more than 50% with a major impact on cardiac services and no clear benefit for these patients.
References
1. Begg A. Men’s health: a tale of two nations. Trends in Urology & Men’s Health 2012;3:19–22. http://dx.doi.org/10.1002/tre.296
2. Building clinical academic capacity and the allocation of resources across academic specialties. The Academy of Medical Sciences 2009. ISBN: 978-1903401194
