Intravenous/subcutaneous anticoagulants
Heparin
Heparin is a polymer of repeating disaccharide units. Unfractionated heparin (UFH), as used pharmacologically, consists of a heterogenous mixture of chains of different lengths. Heparin binds antithrombin, inducing a conformational change which greatly increases its ability to inihibit factors Xa and IIa (thrombin). Heparin is rapidly cleared from the circulation by binding to endothelium/plasma proteins, with renal excretion becoming important once this mechanism is saturated. Although an effective anticoagulant, heparin has many undesirable features, such as the risk of heparin induced thrombocytopenia [HIT] and the need for intensive monitoring. Long-term use can also lead to osteoporosis. Heparin can be rapidly neutralised by protamine.
Low molecular weight heparin
Several of the problems with UFH have been resolved by the development of a ‘cleaner’ form, low molecular weight heparin (LMWH), by depolymerisation of heparin. The shorter chain means that principal anticoagulant activity is by anti Xa activity, but there is some residual antithrombin activity also – the several different LMWHs available differ in their ratio of anti Xa to antithrombin activity, according to their chain length.
LMWHs have much more predictable anticoagulant activity, so that monitoring is usually not required. LMWH also has a much lower incidence of HIT.
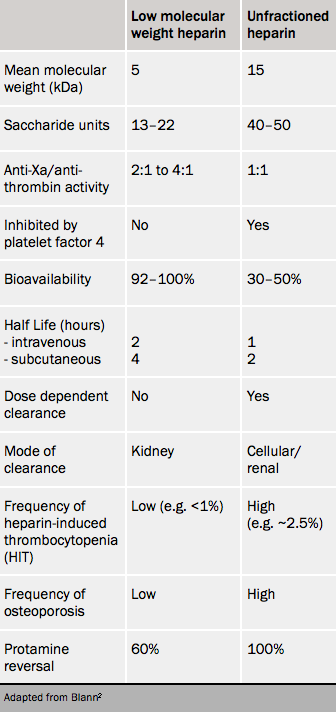
The main disadvantage of LMWHs is their greater reliance on renal excretion (although this varies between agents) making them unsuitable for use in severe renal impairment. LMWH also has a longer half life than UFH, and cannot be completely neutralised by protamine (although again this varies between agents), which can make the management of bleeding challenging.2
Differences between UFH and LMWHs are shown in table 1.
Fondaparinux
This may be described as a super-LMWH, being an engineered pentasaccharide that very precisely and reversibly binds the active site of factor Xa, providing very efficient inhibition.2 Other advantages are its inactivity towards platelets, and, with no activity against thrombin, that it has very predictable anticoagulant activity.
A relatively long plasma half-life of 14–21 hours permits once-daily injection. There is a rapid onset of action, with a peak activity reached in two hours, and no interactions with aspirin, warfarin or digoxin have been noted. Thrombocytopenia occurs even less commonly than with LMWH. In almost all cases, fondaparinux need not be routinely monitored in the laboratory.
Clearance is reduced in renal impairment; no reversal agent is available.
Fondaparinux has had a key role in the management of acute coronary syndromes since the OASIS-5 trial showed similar efficacy with reduced bleeding and lower mortality compared to enoxaparin.
Direct thrombin inhibitors (DTIs)
These operate by inhibiting the action of thrombin directly, that is (unlike heparin), independently of antithrombin. Bivalirudin is a hirudin, named after an anticoagulant purified from the mouthpart of a leech (see figure 2). Another parenteral hirudin, lepirudin, was recently discontinued by its manufacturer.

Argatroban is a synthetic, reversible, direct thrombin inhibitor. It has a short half life (50 minutes) and minimal renal clearance. Its main use is in the specialist management of acute HIT.4
Bivalirudin is an option instead of a heparin in patients with acute coronary syndromes having percutaneous coronary intervention (PCI) as an adjunct to aspirin and clopidogrel, and is approved by the National Institute for Health and Care Excellence (NICE) for patients with ST-elevation MI having PCI.5 Bivalirudin also has an important but specialist role in cardiac surgery in patients with a history of HIT, who cannot receive heparin.4
Dabigatran (discussed below) is an orally available direct thrombin inhibitor.
Monitoring intravenous/subcutaneous anticoagulants
UFH must be monitored in each patient using the activated partial thromboplastin time (APTT). Argatroban is also monitored by the APTT.
One of the major advantages of LMWHs and fondaparinux is that they do not routinely require monitoring. However, in cases where it is felt necessary to measure the degree of anticoagulation with these agents (for instance in patients with poor renal function, or with recurrent thrombosis despite anticoagulation) this can be done by measuring the anti Xa activity.
Anticoagulant monitoring will be considered further in module 4.
