Radiation
Radiation-induced valve disease may be seen after high-dose, high-volume mediastinal radiation given typically for Hodgkin’s disease, and less commonly for breast cancer. Valve changes are more likely to affect the left-sided valves, probably because of higher mechanical stresses. The tricuspid and less commonly the pulmonary valve may also be involved, the aortic and mitral valve equally.
Failing biological valves
Biological valves have acceptable durability in older patients, with failures uncommon before five years in the mitral position and eight years in the aortic position.5 However, durability is limited in younger patients, particularly those aged under 40.
Biological valves are implanted in younger patients if anticoagulation control may be uncertain or to allow pregnancy without the potential teratogenic and bleeding complications of oral anticoagulants. This is common in industrially underdeveloped countries (see figure 2) so that redo surgery is frequently necessary.6
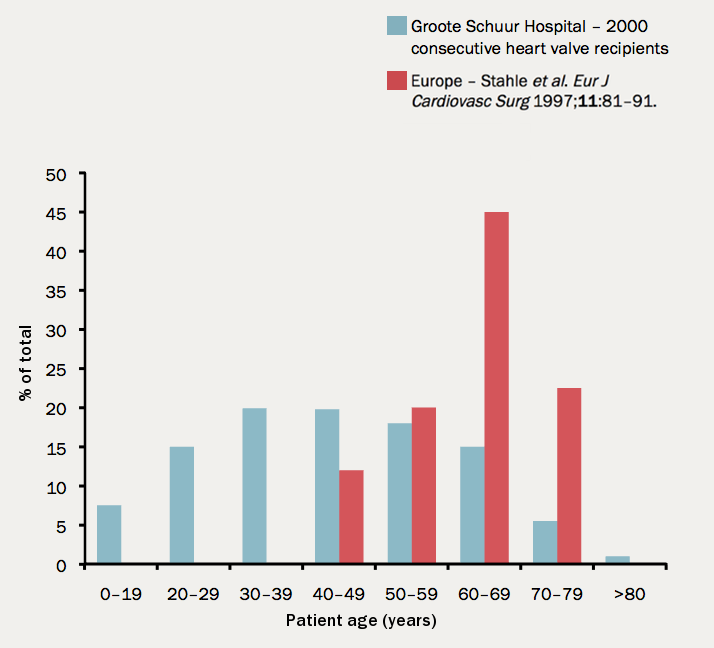
This is also a problem in developed countries as patients survive longer.
In the UK, 7% of aortic valve operations are redo procedures.7
Endocarditis
The incidence of infective endocarditis is between three and 10 episodes per 100,000 patient years,8 but there are major geographical variations depending largely on the age of the population and the frequency of medical devices or intravenous drug use. The incidence increases with age and is 14.5 episodes per 100,000 patient years in those aged 70–80. There is a male to female ratio of over 2:1.
In the industrially underdeveloped regions, patients with endocarditis are young, with about three quarters having rheumatic heart disease and oral streptococci being the main infecting organisms.
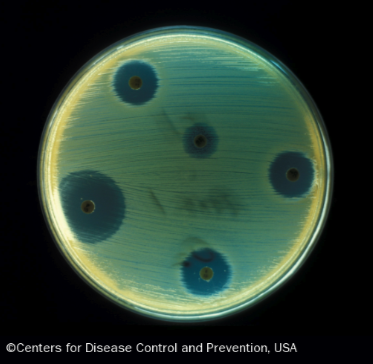
In fully industrialised regions, most patients are older and endocarditis is increasingly associated with replacement heart valves, pacemakers or haemodialysis. Prosthetic valves have a 50 times increased risk of endocarditis compared with the rest of the population. Early infection within one year of implantation occurs in 4% usually caused by coagulase negative staphylococci or Staphylococcus aureus (see figure 3). Late infection has an incidence of 0.5% p.a.4 and is most commonly caused by oral commensals.
With intravenous drug use endocarditis is most commonly caused by S. aureus. Predisposing factors are diabetes and immune-deficiency including human immunodeficiency virus (HIV).
