There is growing support, in the form of data from national multi-centre registries, for extending the indications for TAVI to include intermediate-risk patients. One such report is the retrospective three-centre BERMUDA (BERn, MUnich, rotterDAm) Triangle Study in which 510 patients were propensity-score-matched to either TAVI (n=255) or surgical aortic valve replacement, SAVR, (n=255). Their Society of Thoracic Surgeons predicted risk of operative mortality (STS PROM) score ranged from 3−8%. This study revealed a comparable one-year all-cause mortality outcome for TAVI (n=43, 16.5%) compared to SAVR (n=42, 16.9%) (HR: 0.90, 95% CI: 0.57-1.42, p = 0.64).36
The STACCATO (transapical transcatheter aortic valve implantation vs. surgical aortic valve replacement in operable elderly patients with aortic stenosis) trial was a prospective, randomised clinical trial deigned to evaluate TAVI in intermediate-risk patients. It was discontinued after recruiting 70 patients due to a high adverse event rate among the TAVI group compared to the surgery group. The study’s primary end point was the composite all-cause mortality, cerebral stroke and/or renal failure requiring hemodialysis at 30 days. The TAVI group recorded the following adverse effects: deaths (n=2), stroke (n=2), renal failure with haemodialysis (n=1) vs. stroke (n=1) in the SAVR cohort (p=0.07). Four patients in the TAVI group required cardiac surgery following ruptured annulus (n=1), severe paravalvular leak (n=2), and left coronary artery blockage (n=1).37,40 Non-randomised, multi-centre studies have also shown similar 30-day all-cause mortality TAVI vs. SAVR (1.8%, p=1.00); 38 (3.8%, p=1.00).39 However, the peri-procedural spectrum of complications between TAVI and surgical replacement were different with TAVI patients reporting a higher incidence of major vascular damage (5.3% vs. 0.0%, p=0.007) and pacemaker implantation (0.8% vs. 12.0%; p=0.001), whereas a higher requirement for blood transfusion was reported across the surgical cohort (49.6% vs. 36.1%, p=0.026).39
The non-inferiority of TAVI in lower risk cohorts compared to conventional surgical aortic valve replacement has not been established in randomised trials. Two such randomised trials: the SURTAVI (Surgical Replacement and Transcatheter Aortic Valve Implantation) trial and the PARTNER II (Placement of Aortic Transcatheter Valves II) trial, have completed enrolment as at October 2013 and study results are awaited.41,42 Currently, European Society of Cardiologists (ESC) guidelines recommend TAVI for patients with severe symptomatic aortic stenosis who are high risk surgical candidates, determined by a multidisciplinary heart team, and who are likely to experience improved quality of life, and life expectancy greater than one year regardless of comorbidities.2 Consensus guidelines also recommend that TAVI be performed in a facility with a cardiac surgeon onsite.
Mitral valve repair (MVr)
Transcatheter mitral valve repair (TMVr) is a minimally invasive technique for treatment of chronic mitral regurgitation. While a number of technologies are in clinical development, an edge-to-edge leaflet repair device (the MitraClip®, Abbott) is currently the only United States Food and Drug Administration (FDA) – approved device for TMVr. The MitraClip®, as well as the Carillon® mitral annuloplasty device (Kardia), have CE Mark approval.27-29 In comparison to aortic valve disease, however, percutaneous therapy for mitral valve pathology remains in its early stages. Abbott’s MitraClip® has the largest clinical experience and has been shown to have similar improvements in clinical outcomes but was associated with superior safety outcomes compared to surgery at one year.14,27,30. The MitraClip® is discussed later in this module.
Percutaneous mitral valve repair devices
Normal function of the mitral valve depends on six components of the mitral apparatus: left atrial wall, mitral annulus, mitral leaflet, chordae tendinea, papillary muscles and left ventricular wall. Not surprisingly, therefore, percutaneous approaches at percutaneous mitral repair aim to address pathologies affecting any of the above areas just like open operative repairs. The mitral device technologies used are grouped as follows:20-27
- Interventions addressing the leaflets
- Direct annuloplasty
- Indirect annuloplasty (via the coronary sinus)
- Chordal implantation
- Left ventricular remodeling.
Table 3 summarises percutaneous mitral valve repair and replacement technologies 21
Table 3. Percutaneous mitral valve repair and replacement technologies21
This table can be viewed as table 1 in Chiam21

The MitraClip®
The MitraClip® mitral valve repair system (figure 8) is finding a role in the percutaneous treatment of mitral regurgitation in select patients. It has been available in Europe since 2008, when it gained CE Mark approval and approved more recently in the USA with the indication for symptomatic mitral regurgitation (MR≥ 3+) in patients deemed too high risk for open mitral valve surgery.
Delivery method
The device has a catheter-based delivery system, that is advanced over a guide-wire through the femoral vein. The left atrium is accessed through a trans-septal puncture (see figure 9A) which is dilated before removal of the guidewire and dilator. The device is then advanced through the catheter and positioned over the mitral valve annulus under tranoesophageal echocardioraphic guidance (see figure 9B).
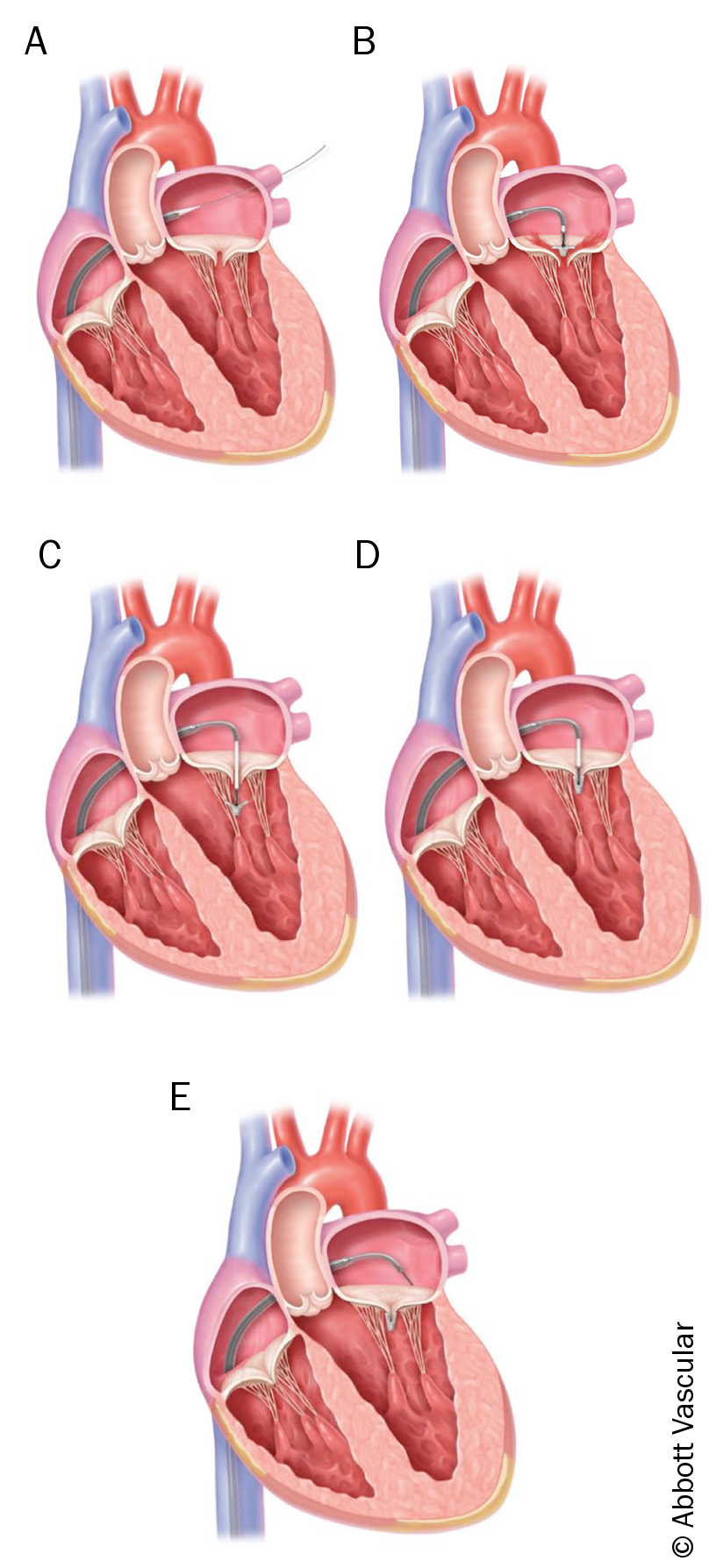
The two arms of the clip are opened in the left atrium and positioned over the area of origin of the regurgitant jet. The extended clip is then advanced across the annulus into the left ventricle and satisfactory positioning is obtained (see figure 9C). The device is retracted back towards the atrium and closed, thereby approximating the anterior and posterior leaflet of the mitral valve with a result that is similar to the edge-to-edge surgical technique (see figures 9D, and 9E).
The degree of mitral regurgitation is assessed intraprocedurally and the device may be repositioned or a second device may be deployed to achieve optimal reduction in regurgitant flow. With clip in place, the mitral valve becomes a double orifice valve with anterior and posterior leaflets bound to one another at the center of their free margins (see figure 10)
