Surgery for truly asymptomatic AS still excites controversy. The annual mortality in AS is less than one per cent when patients are truly asymptomatic. However there is a rapid increase in death rate to 3–4% within three months of the onset of symptoms and a further 7% on a six month waiting list (see figure 1418).
Adapted from Otto(18)
There is therefore an approximate 10% risk of dying in the early symptomatic period producing a great need to identify patients who are ‘pre-symptomatic’. The most accepted are:
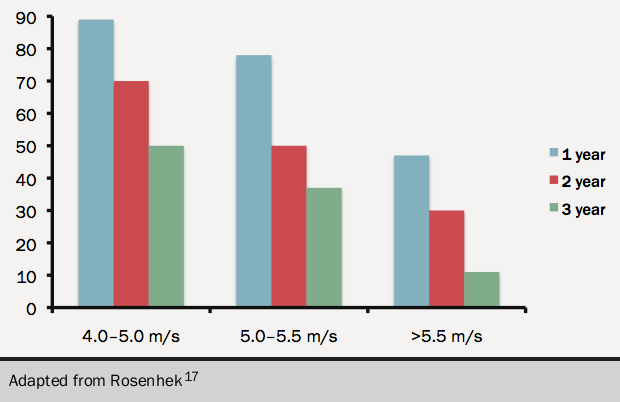
- Critical AS V max >5.5 m/s since the progression is rapid (see figure 1517)
- Rapid rate of progression >0.3 m/s per year with additional heavy valve calcification
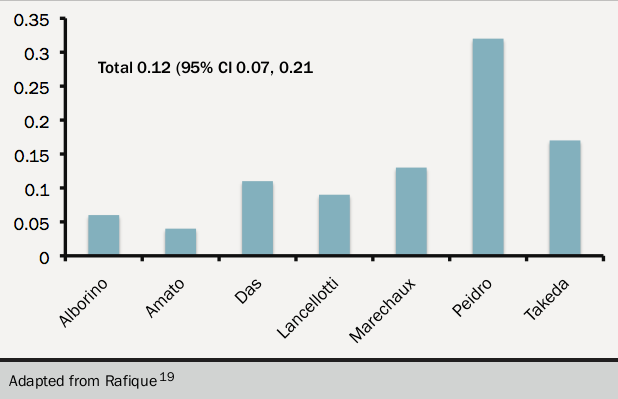
- Symptoms on exercise testing (see figure 1619). This is a class I ESC recommendation and a class IIa AHA recommendation. The data on exercise testing are mainly European. The effect of blunted blood pressure rise is less tight
Other criteria for surgery are:
- Rising BNP, while not yet accepted although it may corroborate other indications.
- Severe LV hypertrophy. A septal width >15 mm is an indication for surgery.2 Severe hypertrophy is associated with higher mortality at the time of surgery and it may take many years for diastolic dysfunction to improve. There is evidence that diastolic dysfunction, especially a change from slow filling to pseudonormal, is a better criterion for early surgery.
- An increase in mean gradient by 20 mmHg on exercise is cited in the ESC guidance as a marker of severe AS but this rests on little published data and should not be used as a sole criterion for surgery.
