Mitral regurgitation
The criteria for surgery differ crucially depending on whether:
- primary or secondary.
- repairable or not
- the surgical risk including comorbidity
Primary regurgitation
If repairable at low risk then this should be considered in an asymptomatic patient if:
- LVEF <60%
- LVSD ≥45 mm (class I) (or even ≥40 mm) (Class I AHA and IIa ESC)
- PA pressure >50 mmHg at rest (IIa)
- New onset AF (IIa)
It is vital if such an early referral is made that the surgeon is a specialist in repair and that the assessment of preoperative likelihood of repair is performed by an expert.
The decision between repair or replacement depends on the anatomy and function of the valve. The characteristic on echocardiography determining feasibility of repair are:
- Mechanism (e.g. prolapse, perforation, restriction)
- Site of prolapse
- Direction of jet compatible with site
- Annulus diameter
- Presence of calcium in posterior annulus.
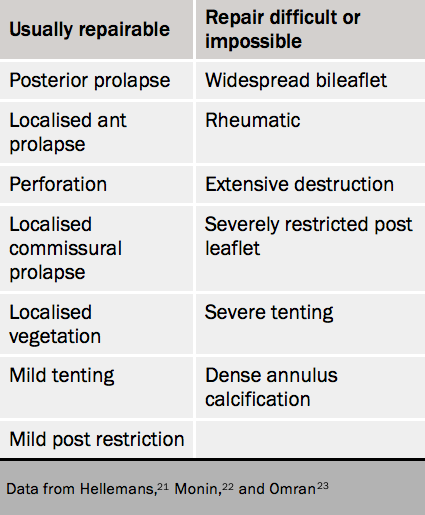
The features that favour or discriminate against repair can be seen in table 4.21–3 Prophylactic surgery is usually acceptable for P2 prolapse but not always where repair is difficult e.g. medial commissure or extensive bileaflet prolapse.
The mitral valve is composed of two leaflets, anterior and posterior. Echocardiography is the most useful method of detecting mitral prolapse and identifying the segments affected (see figure 18) and the grade of mitral regurgitation as well as the LV response. It also assesses the annulus diameter. Mitral prolapse is defined as leaflet displacement behind the plane of the annulus by >2 mm.
Repair is more successful if there is limited damage to areas of the mitral valve leaflets or to the chordae tendineae. But replacement is usually preferred for people who have a hard, calcified mitral valve ring (annulus) or widespread damage to the valve and surrounding tissue.

Valve repair may involve reshaping the valve by removing excess valve tissue then strengthening the annulus with an annuloplasty ring to reduce tension on the repair. It may also be possible to avoid valve resection by improving support with artificial chordae or, less commonly, chordal transposition.
If not repairable (e.g. rheumatic) then replacement is indicated for symptoms.
If the LV is poor with EF <30% then surgery is indicated, especially if repair is feasible, if the patient has symptoms despite full medical therapy.
Other indications (IIb) if risk low and repair likely:
- LA dilated ≥60 ml/m2 in sinus rhythm
- PA systolic pressure >60 mmHg on exercise
