In troubled times, in a sea of uncertainty, it is easy to forget that the UK remains the envy of the world in one aspect at least: the delivery of a national health service (NHS). The structure and organisation of UK general practice; the existence and authority of the National Institute for Health and Care Excellence (NICE) – with national guidance and local dissemination and structured implementation – remain the envy of the world. While our European neighbours stand by holding each other’s coats as Brexit rumbles on, we forget that each of these nations gazes at our health service and wishes they had one just like ours.
The Gospel of Matthew tells us, “…the last can be first…” Nowhere is this truer than the towering UK success of that fundamental cornerstone of cardiovascular prevention, cholesterol-lowering therapy.
In 2002, BJC published a paper showing how far the UK lagged behind other countries in Europe when it came to prescribing lipid-lowering drugs.1 At the same time, a number of other very large UK surveys were published.2 All showed that the UK was the sick man of Europe, with limited statin prescribing in the face of a huge burden of cardiovascular disease.
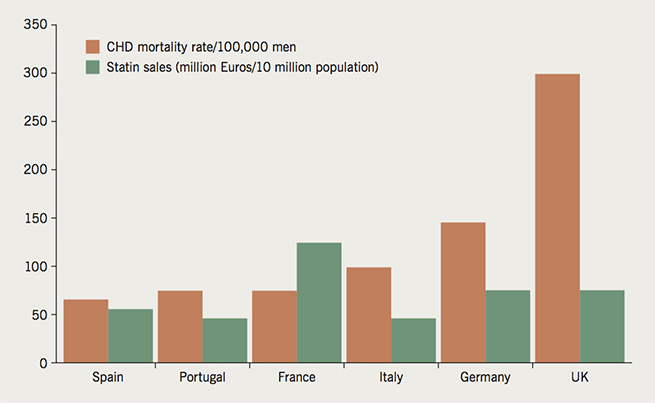
Three things then happened more or less simultaneously: NICE geared up its power and influence; consultant cardiologist Dr Roger Boyle (now Professor Sir Roger Boyle) was tasked as the ‘Heart Tsar’ for the NHS; and the Department of Health defined the Quality Outcomes Framework (QOF) as a practical way to achieve defined goals in healthcare. UK general practices, general practitioners (GPs) and cardiologists addressed, with growing zeal and confidence, the deficiencies in public awareness about cholesterol, and of prescribing drugs to lower it. Figure 1 shows where the UK was placed in 1999, lagging behind other countries in Europe. Figure 2 shows our success, built year upon year, so now the UK leads all the studied countries in Europe, and we are now the benchmark for lipid guidance and lipid prescribing within our continent.3 It can be seen that other countries have slowed their enthusiasm, or changed their priorities. Yet in the UK, the burden of cardiovascular disease is well recognised and treatment has grown steadily.
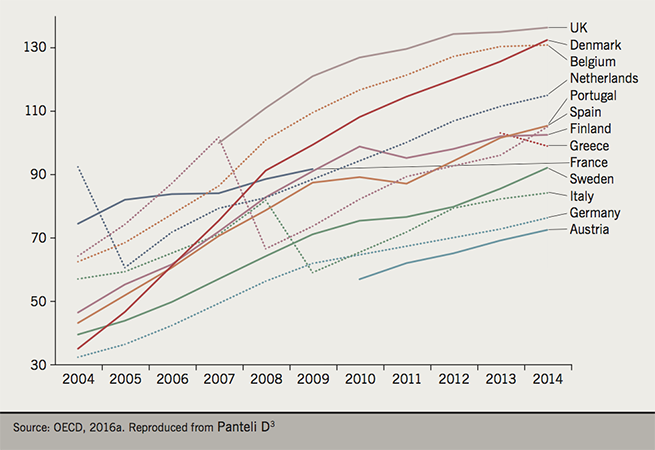
Lipid-modifying agents (defined daily doses per 1,000 inhabitants per day), 2004–2014
Medicine on a national and global scale is about awareness and about delivery. Over the last 15 years, the UK public has become increasingly aware of the importance of cholesterol. Information has come from multiple sources, from the British Heart Foundation and the Department of Health, to commercial interests, be it all with the same ultimate aim: an awareness of the importance of high cholesterol and the value of lowering it. Yet the platinum star goes to UK general practice, for its delivery and organisation of checking cholesterols and treating patients with high levels.
What about blood pressure?
So, we are top at cholesterol lowering. What about high blood pressure? In May of this year we will have a chance to be top of Europe again, during May Measurement Month. This is a global initiative led by Professor Neil Poulter at Imperial College, President of the International Society of Hypertension. In the UK, we aim to measure 250,000 blood pressures in ordinary people, at hundreds of blood pressure stations across the country. If you are able to measure blood pressure, download the app for May Measurement Month, and get measuring. Practically everybody over 18 is eligible to be a participant in this trial. The British and Irish Hypertension Society has tasked its members each to measure 1,000 blood pressures during May.
UK lipid lowering over the next five years
So we lead Europe in lipid lowering, yet that is still not enough. We must not cease in our push for universal global awareness of the importance of cholesterol, blood pressure and blood sugar. This is the ‘Holy Trinity’ of cardiovascular prevention, and our work is not finished.
So what about the new drugs – the proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors? Recently, at the American College of Cardiology, the results of the FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) trial were announced: 27,000 patients randomised to the PCSK9 inhibitor evolocumab or placebo.4 The results of this enormous trial were warm rather than red hot. There was a reduction in some cardiovascular end points but no benefit on mortality. The trial reported after two years, probably too early to see a sustained benefit. Longer-term follow-up results will appear, and the ODYSSEY outcome trial (Long-term Safety and Tolerability of Alirocumab) of the other PCSK9 inhibitor alirocumab, which does have longer follow-up, is coming, results due 2018.
Ezetimibe will come off patent next year, and the growing familiarity and comfort with this unassuming, safe, evidence-based and effective drug may mean that combination therapy for cholesterol lowering, like blood-pressure lowering and blood-sugar lowering, becomes the norm. Then, the PCSK9 drugs and other monoclonal antibodies, will have to unseat an accepted, safe and evidence-based combination therapy if the new drugs are to become prominent.
And the last of the cholesterol ester transfer protein (CETP) inhibitors may yet be first. Anacetrapib, being tested in over 30,000 patients, will report later this year. The other CETP inhibitors have all fallen by the wayside, yet the huge HPS3/TIMI 55-REVEAL (Randomised EValuation of the Effects of Anacetrapib through Lipid-modification) trial passed a futility test last year, and is set to report at the European Society of Cardiology (ESC) in Barcelona. This unusual drug, with unique pharmacokinetics and a half-life measured in years, may yet prove to be fruitful.
Conclusion
Cholesterol-lowering therapy in the UK is a huge triumph of dogged British determination, initiative, drive and perseverance. UK general practice, in its delivery and organisational care, remains supreme. We have the structure, we have the implementation, and we are the envy of the world. For the future, we have a great health service, great GPs, good drugs, and much to look forward to. Keep going!
Conflict of interest
AJBB has received research grants and honoraria from Astra Zeneca, Bayer, MSD, Roche and Servier.
References
1. Brady AJB. Britain: still the sick man of Europe? Br J Cardiol 2002;9:1–3. Available from: https://bjcardio.co.uk/2002/01/britain-still-the-sick-man-of-europe/
2. Brady AJB, Oliver MA, Pittard JB. Secondary prevention in 24,431 patients with coronary heart disease: survey in primary care. BMJ 2001;322:1463. https://doi.org/10.1136/bmj.322.7300.1463
3. Panteli D, Arickx F Cleemput I et al. Pharmaceutical regulation in 15 European countries. Health Systems in Transition 2016;18:15, Fig. 2.9. Available from: http://www.euro.who.int/en/about-us/partners/observatory/publications/health-system-reviews-hits/full-list-of-country-hits/special-edition-pharmaceutical-regulation-in-15-european-countries-2016
4. Sabatine MS, Giugliano RP, Keech AC et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017;online first. https://doi.org/10.1056/NEJMoa1615664
