Cardiac rehabilitation (ExCR) is an essential, evidence-based part of the management of people with chronic heart failure (CHF), but research indicates it is underused. This retrospective audit explores the eligibility of heart failure inpatients for ExCR, according to the European Society of Cardiology (ESC) consensus statement, and the impact of frailty on referral rates.
The first 100 patients admitted with a diagnosis of CHF from 1 February 2020 within one hospital trust were included in the audit. Only 54% of patients were eligible for ExCR at discharge and, of them, 43% were referred. Most patients (69%) admitted to cardiology wards were eligible for ExCR compared with 14% of those admitted to non-specialist care. Frail patients were less likely to be admitted to cardiology wards (43%) than their non-frail counterparts (93%).
Not all patients admitted to hospital with heart failure are eligible for ExCR, and assessing eligibility is important in identifying the true referral rate to allow national benchmarking. Interventions to improve referral are still important, but focus also needs to be directed to developing interventions for those individuals currently not eligible for standard ExCR programmes.
Introduction
Exercise-based cardiac rehabilitation (ExCR) is integral to the management of people with chronic heart failure (CHF).1 It not only improves quality of life (QoL), but is likely to reduce hospital admissions and mortality in this population.1 In response to this evidence, offering a personalised ExCR to all patients with stable CHF is included in the current National Institute for Health and Care Excellence (NICE) guidelines.2
Most CHF diagnoses (up to 80%) occur during an inpatient stay for acute decompensated heart failure (ADHF).3 An admission presents the opportunity for most people with CHF to be offered ExCR.
CHF is associated with increased age4 and high comorbidity burden,4 leaving individuals vulnerable to physical limitations and frailty (a syndrome characterised by physiological decline that leaves individuals less able to combat stressors, resulting in poor health outcomes).5 This is often exacerbated by an inpatient stay,6 and can make them unsuitable for an ExCR programme at the point of discharge. Two studies looking at outpatient referral to ExCR found high levels of ineligibility within CHF patients (up to 49%),7,8 and it is reasonable to suppose that this may be higher in the immediate post-discharge population, who are likely to be more symptomatic.
The annual National Heart Failure Audit (NHFA) on CHF admissions captures data on the proportion of patients referred to cardiac rehabilitation (CR) during their inpatient stay.9 They show significant variability from hospital to hospital (0 to 100%), with some notable high10 and low referral rates. The 2019/2020 NHFA average referral rate of inpatients with CHF to CR was 15%.9 These data do not take account of eligibility for ExCR, so it is difficult to compare them against NHS England’s Long Term Plan target of 85% uptake by eligible patients by 2028.11 The National Audit of Cardiac Rehabilitation (NACR) collects UK data (excluding Scotland) on referral and uptake of CR by people with CHF.12 Though they have no data on the total number of people eligible for CR, work by Jones et al.13 demonstrated that 52,273 patients with CHF were referred to the CR service in the period between April 2007 and November 2018. Of those, only 62.6% went on to be assessed for suitability for a CR programme, with 81.7% of those subsequently enrolled in a programme. It may well be that a proportion of individuals not enrolling on the programme were identified as not eligible for CR on assessment, but this number is not known.
This current audit aimed to identify the proportion of CHF patients admitted to a single NHS hospital trust who were eligible for an ExCR programme at the point of discharge, and identify how many of these patients were referred to the CR service. We also considered the factors commonly associated with ineligibility for an ExCR programme, including the admission frailty status.
Materials and method
Locally, the inpatient CR phase 1 assessment is delivered by the heart failure nursing service (HFNS).10 They aim to see all patients referred to the team before discharge from hospital to provide education, including a discussion about exercise and the ExCR programme. This approach is an effective way of delivering the phase 1 CR intervention and is reflected in the hospital level NHFA data.14 However, it has not translated into higher referral to the CR service for a phase 2 assessment.10 Not all CHF inpatients are referred to the HFNS, and the data gathered for the NHFA includes both those who have and have not been either referred or seen by the HFNS. Patients are admitted to either a general hospital, where the care is provided by non-specialist clinical teams, or a specialist tertiary hospital, where care is provided by a cardiology team.
Three sources of data were used in this audit.
- The local database collecting data for the NHFA.
- Case notes and electronic records for details of patient assessment and care.
- The CR database for referral of heart failure patients to the CR team.
Information retrieved from the data sources:
- Ineligibility for ExCR on clinical grounds based on the European Society of Cardiology (ESC) consensus document ‘Exercise training in heart failure’.15
- Admission frailty level taken in the emergency department (ED) on patients aged ≥65 years according to Rockwood clinical frailty score (CFS).16
- Documentation of contact with a healthcare professional (HCP) to discuss ExCR referral.
- Referral to ExCR.
Eligibility for ExCR was assessed using the criteria in the ESC consensus document ‘Exercise training in heart failure’.15 Documentation of a patient’s physical ability, level of independence and planned discharge location were reviewed and categorised together with any clinical exclusion criteria for ExCR at the point of discharge. Exclusion criteria identified in this cohort of patients are listed in table 1.
Documentation of discussion of ExCR with a HCP during admission; and referral to the CR team and by whom, was obtained from patient’s hospital notes or audit databases where possible.
Results
Data were obtained from the first 100 patients with CHF admitted with ADHF to the Leicester Hospitals University Trust hospitals from 1 February 2020 (prior to the first COVID-19 national lockdown). This cohort was similar to the national picture in the corresponding annual NHFA data with mean age 80 years, compared with mean NHFA age 78.4 years; 51% female compared with NHFA 44.8% female; non-white British 14% (NHFA does not currently publish these data)17 (table 2).
Data on CR referrals
In 54/100 of the patients’ records, no contraindications to CR were identified on clinical grounds based on the ESC consensus document (table 2).15 However, only 23/54 were referred. This represents 43% of the eligible population of this cohort.
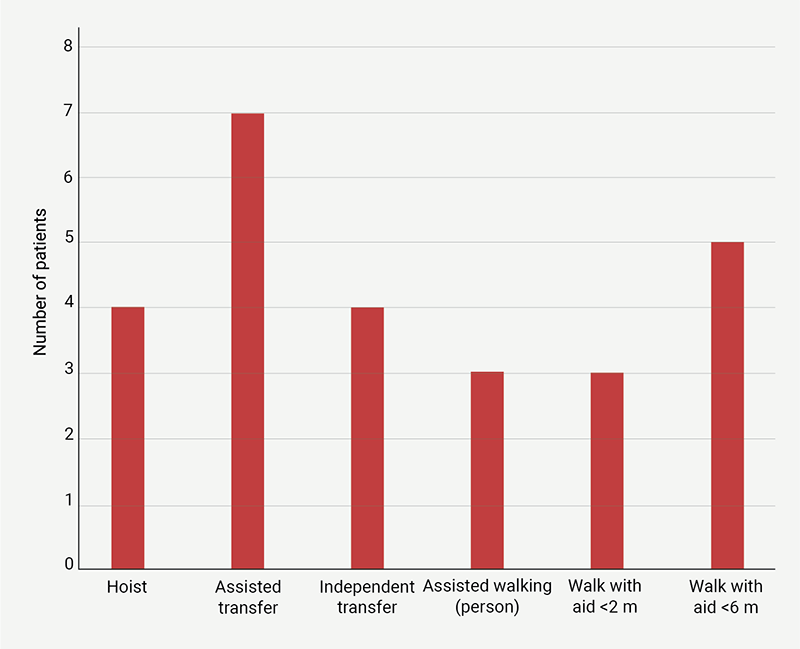
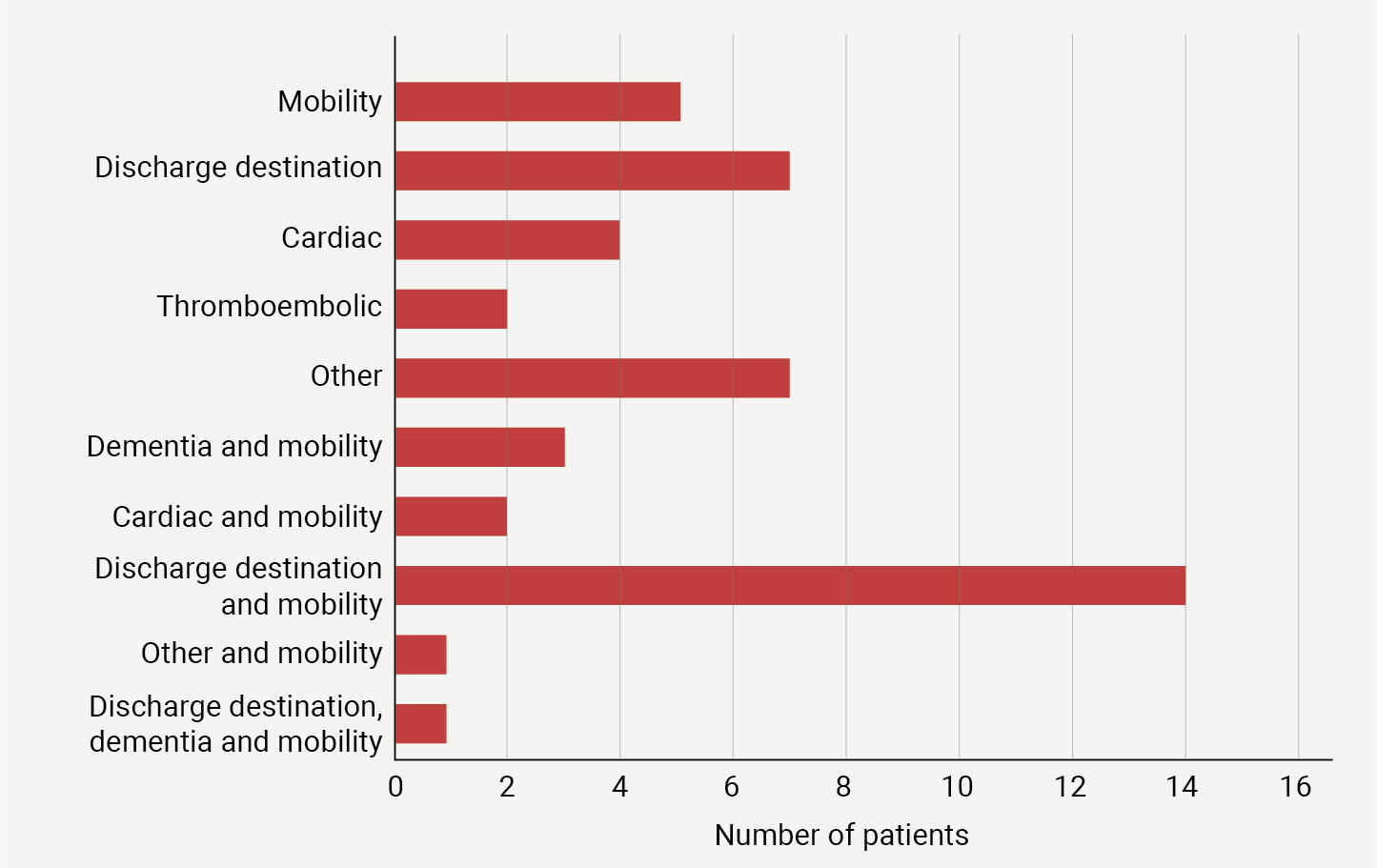
Of the 46 who were not suitable for referral, the exclusion criterion most often associated with unsuitability for CR was the impact of comorbidities on mobility. They ranged from requiring hoisting, through to mobilising less than 6 metres (figure 1). It was common (21 out of the 46) for patients to have multiple exclusion criteria for ExCR (figure 2). Mobility issues were often associated with the discharge destination and ongoing plan, which included nursing home, home care, end-of-life care, etc. All five patients who were in the upper range of mobility (walking with aid <6 m) had other reasons for being ineligible for ExCR (severe dementia; required high level of support with activities of daily living [ADL]; severe aortic stenosis).
Association of frailty with CR eligibility and referral
Frailty data were only available for 80 of the patients in this audit, as the Rockwood CFS16 is not routinely collected if patients are aged <65 years or are admitted via the Clinical Decisions Unit. Following the recommendations from the developers of the CFS and its use in other studies, the cut-off point for frailty was considered as a CFS score >4.18 Overall, 45/80 patients with known frailty status were considered non-frail on admission, and the remaining 35/80 patients were considered frail (figure 3).
Of those known to be admitted to hospital without frailty, 26/45 (58%) had a documented discussion with a HCP about ExCR, and 16/45 (36%) went on to be referred to the CR team. In the group of patients who were frail on admission, only 14/35 (40%) had a documented discussion with a HCP about ExCR, and just 3/35 patients went on to be referred to the CR service.
Admission CFS score of >4 was associated with poor mobility and a reduced likelihood of being suitable for ExCR. However, people with frailty, but still eligible for ExCR (n=10), were less likely to receive a referral to CR than non-frail individuals eligible for ExCR (n=36) (figure 3).
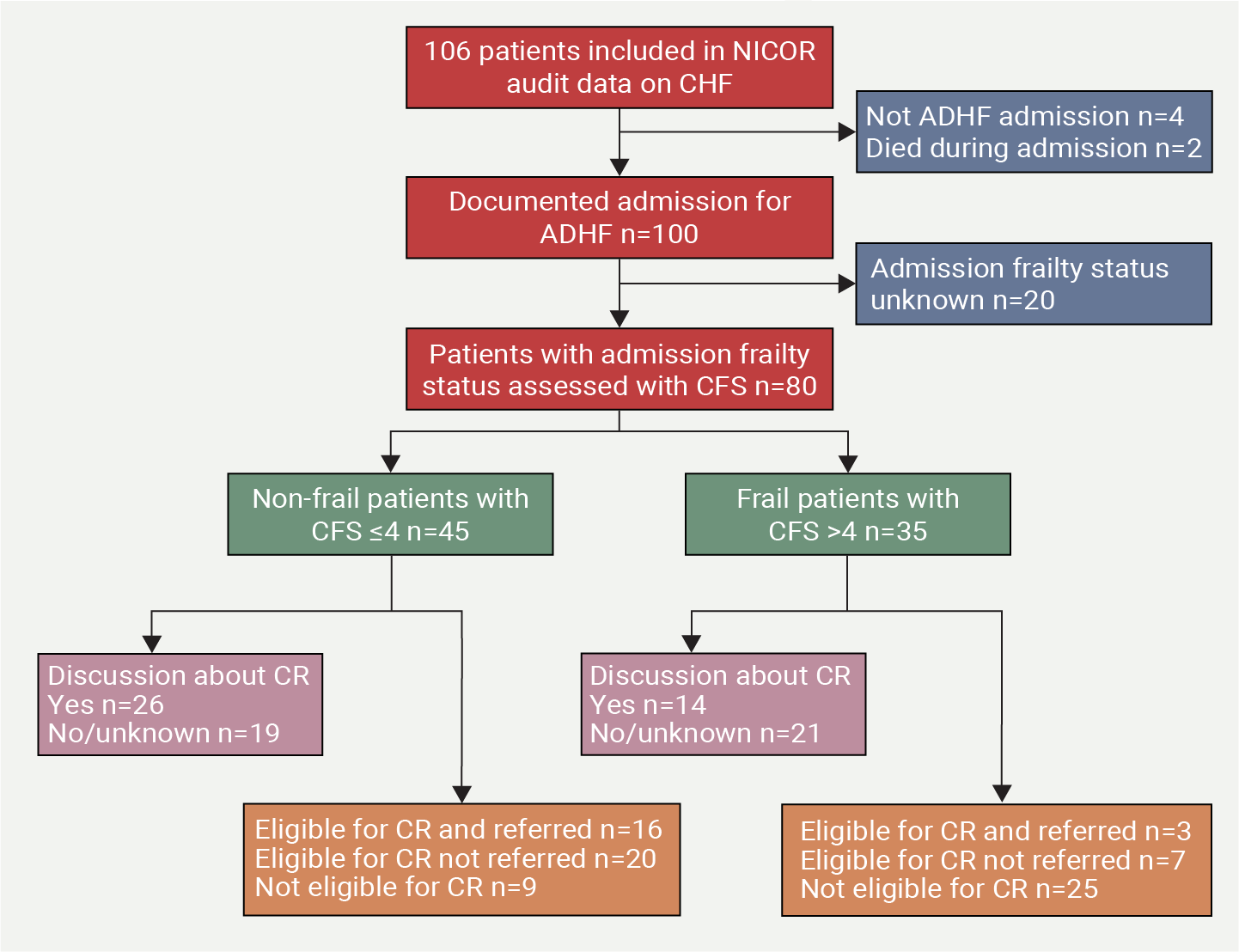
| Key: ADHF = acute decompensated heart failure; CFS = clinical frailty score; CHF = chronic heart failure; CR = cardiac rehabilitation; NICOR = National Institute for Cardiovascular Outcomes Research |
Most non-frail patients (93%) were admitted to the specialist tertiary hospital, whereas only 43% of frail patients received this specialist care. However, those admitted to the tertiary hospital were also more likely to be considered suitable for ExCR (69%) compared with those admitted to non-specialist care (14%), which reflects the association between frailty and a lower likelihood of eligibility for an ExCR programme (figure 3).
Data on whether or not an inpatient physiotherapy (PT) or occupational therapy (OT) review occurred were available for 53 patients. Of these, 45% were reviewed by a PT or OT inpatient team. These reviews were more likely to occur in frail patients (72%) than non-frail patients (21%), and they were not associated with increased referral to the CR service.
Discussion
Not everyone admitted to hospital with CHF will be eligible for ExCR at the point of discharge, and there is a need for data to help identify the magnitude of this population. Currently, this is not reported in either the NHFA or the NACR data, which limits the ability of the research and clinical community to establish appropriate benchmarks or targets for uptake of CR in the CHF population. In our audit, 46% of patients were identified as ineligible for ExCR, which is comparable with the work done on outpatient populations.7,8 However, our work was looking specifically at an inpatient population, which links with the data currently presented in the NHFA.
Within our locality, the HFNS reviews 80% of the patients coded as admitted with CHF. They provide the phase 1 CR discussion about the patient’s condition and how to manage it in the immediate post-discharge period, including advice about exercise and ExCR.10
Frailty is a condition for which the international CR community has been considering making provision, first in terms of identifying patients with frailty at enrolment, and second, in adapting the programme to address specific needs.19,20 There is evidence that physical activity interventions can improve elements of frailty (mobility, strength) in frail individuals over 65 years of age.21 Consequently, frailty alone should not be a deterrent to the offer or uptake of ExCR, though adapted programmes may be required to mitigate for the challenges people with frailty may face.22–24 The REHAB-HF (Rehabilitation Therapy in Older Acute Heart Failure Patients) trial demonstrated both the possibility to retain frail CHF participants within an exercise-based intervention, and the association with greater improvement in physical indicators of frailty (strength, speed and balance) compared with usual care.25
In our audit, though frail patients were admitted to both specialist and non-specialist settings, those admitted to the non-specialist setting had a higher prevalence of frailty. They had a lower likelihood of eligibility for a standard ExCR programme, but were more likely to be seen by inpatient PT or OT. The presence of higher comorbid frailty rates in CHF patients on general wards is corroborated by data from other researchers,26 as is a lower referral rate to CR.27
Different models of delivery of ExCR are advocated to help engage different sections of the population.28–30 These include: remote programmes, such as web-based and telehealth;31 programmes provided closer to, or within, participants homes, such as the REACH-HF (Rehabilitation Enablement in Chronic Heart Failure) programme;32 a modified chair-based exercise or alternative format of programmes.29 It may be that a bridging physical activity intervention, or a modified ExCR programme, could be beneficial to this group of frail patients,24,25 who are currently not eligible for the standard ExCR programme, which may be facilitated by closer interdisciplinary education and working with the PT and OT ward-based teams.33,34
Study strengths and limitations
There were limitations due to missing data, which prevented all the audit data being used in the analysis of the impact of frailty. As the number of records reviewed in the audit was limited to 100, the inferences made need to be supported by further research. However, as the case notes were hand-searched for data, the audit did not rely on data transfer into a database and a comprehensive account of a hospital admission was available. Information about mobility was often well reported, particularly if the patient had been reviewed by the PT/OT teams, but mobility was more difficult to ascertain if a formal mobility assessment had not been done.
Conclusion
Recruiting patients with CHF to an ExCR programme following an inpatient stay presents many challenges. However, unlike the NHFA data, which suggests an average of 15% of patients are referred to CR prior to discharge, this audit indicates the true value is up to 43% of eligible CHF patients are referred at our hospital trust. Though there is significant room for improvement, we have also identified a high proportion of patients who are not eligible for referral. There is some uncertainty as to when, if ever, they would be considered suitable to access a centre-based programme, but multiple points of referral along the patient journey may be needed to facilitate uptake of ExCR.
Progress towards the current national target of 85% uptake of ExCR by eligible patients is difficult to monitor in the CHF population if data on eligibility are not currently established and agreed for benchmarking. National reports of a referral rate of 15% do not reflect an accurate picture, as they do not account for those patients who are ineligible for the standard ExCR programmes currently available. The role of nationally gathered data, either via the NHFA or NACR, should not be underestimated, and it should aim to contribute to identifying the true size of the eligible population, rather than presenting incomplete data that does not take adequate account of eligibility.
By highlighting the eligibility for ExCR in this patient population, it is hoped that an estimation of the true referral rate can be established. With more focus placed on reporting eligibility for ExCR in the CHF population, interventions can be targeted, not only to those who may choose not to engage with an ExCR programme, but also those who find themselves ineligible for the standard ExCR programme when it is being offered, particularly those with co-existing frailty.
Key messages
- Many patients with heart failure are not eligible for exercise-based cardiac rehabilitation (ExCR) at the point of hospital discharge
- Frail patients are less likely to be eligible for ExCR compared with their non-frail counterparts
- Interventions need to be developed to, not only improve uptake of ExCR in eligible patients, but also to help those who are currently not eligible for the standard programme
Conflicts of interest
None declared.
Funding
HW received a BHF Nursing and Allied Health Professional PhD Fellowship, which funded this work.
Study approval
The audit was approved and registered on the clinical audit programme at University Hospitals Leicester NHS Trust.
References
1. Long L, Mordi IR, Bridges C et al. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst Rev 2019;1:CD003331. https://doi.org/10.1002/14651858.CD003331.pub5
2. National Institute for Health and Care Excellence (NICE). Chronic heart failure in adults: diagnosis and management. NG106. London: NICE, 2018. Available from: https://www.nice.org.uk/guidance/ng106
3. Bottle A, Kim D, Aylin P, Cowie MR, Majeed A, Hayhoe B. Routes to diagnosis of heart failure: observational study using linked data in England. Heart 2018;104:600. https://doi.org/10.1136/heartjnl-2017-312183
4. Conrad N, Judge A, Tran J et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet 2018;391:572–80. https://doi.org/10.1016/S0140-6736(17)32520-5
5. World Health Organization. World report on ageing and health. Geneva: WHO, 2015. Available from: http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf
6. Krumholz HM. Post-hospital syndrome – an acquired, transient condition of generalized risk. N Engl J Med 2013;368:100–02. https://doi.org/10.1056/NEJMp1212324
7. Contractor A, O’Sullivan K, Pack QR et al. Cardiac rehabilitation among hospitalized patients with heart failure: eligibility, enrollment, and participation. Circ Heart Fail 2022;15:e009403. https://doi.org/10.1161/CIRCHEARTFAILURE.121.009403
8. Rengo JL, Savage PD, Barrett T, Ades PA. Cardiac rehabilitation participation rates and outcomes for patients with heart failure. J Cardiopulm Rehabil Prev 2018;38:38–42. https://doi.org/10.1097/HCR.0000000000000252
9. National Institute for Cardiovascular Outcomes Research. National Cardiac Audit Programme. National heart failure audit (NHFA): 2021 summary report (2019/20 data). London: Healthcare Quality Improvement Partnership (HQIP), 2021. Available from: https://www.hqip.org.uk/resource/national-heart-failure-audit-nhfa-2021-summary-report/
10. Waterhouse H, Squire I, Clayton L, Gardiner N, Singh S. P215. Is the delivery of inpatient cardiac rehabilitation review by heart failure nurses an effective strategy? Eur J Cardiovasc Nurs 2020;19(suppl 1):S44. https://doi.org/10.1177/1474515120952021
11. National Health Service. The NHS long term plan. London: NHS, 2019. Available from: https://www.longtermplan.nhs.uk/
12. NHS England. National Audit of Cardiac Rehabilitation. Available at: https://digital.nhs.uk/data-and-information/clinical-audits-and-registries/national-audit-of-cardiac-rehabilitation
13. Jones AV, Evans RA, Harrison AS et al. Exercise rehabilitation in COPD and heart failure: comparison of two national audits. ERJ Open Res 2022;8:00131-2022. https://doi.org/10.1183/23120541.00131-2022
14. National Institute for Cardiovascular Outcomes Research. Heart failure hospital level tables report 2019 2020 (revised). Available at: https://www.nicor.org.uk/national-cardiac-audit-programme/previous-reports/heart-failure-3/2021-4
15. Piepoli MF, Conraads V, Corra U et al. Exercise training in heart failure: from theory to practice. A consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur J Heart Fail 2011;13:347–57. https://doi.org/10.1093/eurjhf/hfr017
16. Rockwood K, Song X, MacKnight C et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005;173:489–95. https://doi.org/10.1503/cmaj.050051
17. National Institute for Cardiovascular Outcomes Research. National Cardiac Audit Programme. National heart failure audit (NHFA): 2022 summary report (2020/21 data). London: Healthcare Quality Improvement Partnership (HQIP), 2022. Available from: https://www.nicor.org.uk/national-cardiac-audit-programme/previous-reports/heart-failure-3/2022-4/nhfa-doc-2022-final?layout=file
18. Church S, Rogers E, Rockwood K, Theou O. A scoping review of the clinical frailty scale. BMC Geriatr 2020;20:393. https://doi.org/10.1186/s12877-020-01801-7
19. Vigorito C, Abreu A, Ambrosetti M et al. Frailty and cardiac rehabilitation: a call to action from the EAPC cardiac rehabilitation section. Eur J Prev Cardiol 2017;24:577–90. https://doi.org/10.1177/2047487316682579
20. Flint KM, Stevens-Lapsley J, Forman DE. Cardiac rehabilitation in frail older adults with cardiovascular disease: a new diagnostic and treatment paradigm. J Cardiopulm Rehabil Prev 2020;40:72–8. https://doi.org/10.1097/HCR.0000000000000492
21. Racey M, Ali MU, Sherifali D et al. Effectiveness of physical activity interventions in older adults with frailty or prefrailty: a systematic review and meta-analysis. CMAJ Open 2021;9:e728–e743. https://doi.org/10.9778/cmajo.20200222
22. Hillier T, MacEachern E, Kehler DS, Giacomantonio N. Contribution of individual and cumulative frailty-related health deficits on cardiac rehabilitation completion. BMC Geriatr 2023;23:34. https://doi.org/10.1186/s12877-022-03624-0
23. Afilalo J. Evaluating and treating frailty in cardiac rehabilitation. Clin Geriatr Med 2019;35:445–57. https://doi.org/10.1016/j.cger.2019.07.002
24. Ijaz N, Buta B, Xue QL et al. Interventions for frailty among older adults with cardiovascular disease: JACC state-of-the-art review. J Am Coll Cardiol 2022;79:482–503. https://doi.org/10.1016/j.jacc.2021.11.029
25. Kitzman DW, Whellan DJ, Duncan P et al. Physical rehabilitation for older patients hospitalized for heart failure. N Engl J Med 2021;385:203–16. https://doi.org/10.1056/NEJMoa2026141
26. Sharma Y, Horwood C, Hakendorf P, Thompson C. Characteristics and outcomes of patients with heart failure discharged from different speciality units in Australia: an observational study. QJM 2022;115:727–34. https://doi.org/10.1093/qjmed/hcac051
27. Buttery AK, Carr-White G, Martin FC, Glaser K, Lowton K. Cardiac rehabilitation for heart failure: do older people want to attend and are they referred? Eur Geriatr Med 2014;5:246–51. https://doi.org/10.1016/j.eurger.2014.04.011
28. Iliou MC. How can we increase the participation of patients in cardiac rehabilitation programmes? Eur J Prev Cardiol 2018;25:1923–4. https://doi.org/10.1177/2047487318806698
29. Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiol 2015;22:35–74. https://doi.org/10.1177/2047487313501093
30. Chindhy S, Taub PR, Lavie CJ, Shen J. Current challenges in cardiac rehabilitation: strategies to overcome social factors and attendance barriers. Expert Rev Cardiovasc Ther 2020;18:777–89. https://doi.org/10.1080/14779072.2020.1816464
31. Wongvibulsin S, Habeos EE, Huynh PP et al. Digital health interventions for cardiac rehabilitation: systematic literature review. J Med Internet Res 2021;23:e18773. https://doi.org/10.2196/18773
32. Dalal HM, Taylor RS, Jolly K et al. The effects and costs of home-based rehabilitation for heart failure with reduced ejection fraction: the REACH-HF multicentre randomized controlled trial. Eur J Prev Cardiol 2019;26:262–72. https://doi.org/10.1177/2047487318806358
33. Shoemaker MJ, Dias KJ, Lefebvre KM, Heick JD, Collins SM. Physical therapist clinical practice guideline for the management of individuals with heart failure. Phys Ther 2020;100:14–43. https://doi.org/10.1093/ptj/pzz127
34. Dean E, Lomi C. A health and lifestyle framework: an evidence-informed basis for contemporary physical therapist clinical practice guidelines with special reference to individuals with heart failure. Physiother Res Int 2022;27:e1950. https://doi.org/10.1002/pri.1950
