Measuring the N-terminal prohormone of brain natriuretic peptide (NT-proBNP) can help to triage patients with suspected acute heart failure (HF), towards confirmatory transthoracic echocardiography. It has a high negative-predictive value, however, it is not specific due to the influence on its levels by comorbidities. The British Society of Echocardiography (BSE) have published criteria for the triage of those with suspected HF, for inpatient echocardiography, using age-specific NT-proBNP cut-off values.
This study aims to evaluate the diagnostic utility of these recommendations for triaging inpatient echocardiography requests to diagnose acute HF. We analysed data from consecutive inpatients who had an echocardiogram requested between 1 and 15 March 2024, at two secondary care hospitals in the East of England. NT-proBNP results were paired to these requests. Patients were then grouped into the three BSE NT-proBNP cut-off levels and compared. The main outcome of interest was the diagnostic yield for HF using these criteria.
There were 159 patients included in the final analysis: 100 (62.9%) met the NT-proBNP BSE threshold; 65 (65.0%) of these had an inpatient echocardiogram, of which 39 (60.0%) were diagnosed with HF. There were 59 (37.1%) who did not meet the BSE threshold: 29 (49.2%), however, had an inpatient echocardiogram, with nine (31.0%) subsequently diagnosed with HF. Review of these nine patients revealed other valid reasons for echocardiography request: therefore, no cases were truly missed. Patients who had atrial fibrillation (AF) had a similar diagnostic yield for HF compared with those who did not (AF + HF diagnosis 54.0% vs. no AF + HF 67.9%; p=0.385).
In conclusion, the BSE’s age-related NT-proBNP criteria for inpatient echocardiography provides a safe and viable framework for triaging inpatient requests towards a diagnosis of HF. This approach could reduce the burden on stretched services, allowing resources to be directed more appropriately.
Introduction
Heart failure (HF) remains a leading cause of hospital admissions and healthcare expenditure worldwide, and is associated with substantial morbidity and mortality.1 HF is commonly classified into three subtypes based on left ventricular ejection fraction (LVEF)1 as heart failure with preserved ejection fraction (HFpEF), LVEF ≥50%; mildly reduced ejection fraction (HFmrEF), LVEF 41–49%; or with a reduced ejection fraction (HFrEF), LVEF ≤40%.
Patients with HF are at risk of decompensation due to the inability of the heart to sustain a functional cardiac output. Compensatory mechanisms, such as neurohormonal activation and salt and water retention, initially beneficial, become deleterious long term. This can lead to adverse cardiac remodelling and worsening cardiac function, increasing symptoms that could result in a hospital admission.
When this happens, early and accurate diagnosis is essential for the immediate management and initiation of guideline-recommended therapies known to reduce mortality and reduce the risk of rehospitalisation. Symptoms and signs of HF are neither sensitive nor specific, therefore, they can mimic other conditions. A confirmatory diagnosis of HF is, therefore, usually predicated on cardiac imaging, such as transthoracic echocardiography (TTE). The cardiac biomarker N-terminal pro-B-type natriuretic peptide (NT-proBNP) is recommended as a useful rule-out tool, as when raised, the pre-test probability of making a diagnosis of HF is increased.2
B-type natriuretic peptide (BNP) is a protein, produced in cardiac myocytes and released in response to myocardial stretch caused by volume expansion. Functionally, BNP exerts several counter-regulatory effects to reduce cardiac workload and limit disease progression. These include promoting natriuresis and diuresis, leading to increased sodium and water excretion by the kidneys, which in turn helps reduce intravascular volume and ventricular preload. Additionally, BNP inhibits the sympathetic nervous system and the renin–angiotensin–aldosterone system (RAAS), both of which contribute to vasoconstriction, sodium retention, and myocardial remodelling. BNP also induces vasodilation, reducing peripheral vascular resistance and afterload, thereby, improving cardiac output.3,4
The N-terminal of BNP (NT-proBNP), cleaved during activation, is a stable and useful biomarker. It is recommended in National Institute for Health and Care Excellence (NICE) guidance to triage outpatients towards a diagnostic echocardiogram,5 and has value for prognosis, and monitoring response to therapy.2 NT-proBNP levels can, however, be confounded by a number of factors, including age, given that older individuals tend to exhibit higher baseline concentrations.6 Other comorbidities may also contribute to elevating natriuretic peptide levels. These include cardiac causes, such as acute coronary syndrome (ACS), valvular heart disease, myocarditis, and atrial fibrillation (AF). Non-cardiac causes include chronic kidney disease (CKD) and anaemia.1,4 Consequently, using absolute thresholds, without taking into account these other factors, may lead to many unnecessary investigations and misallocation of echocardiography resources.
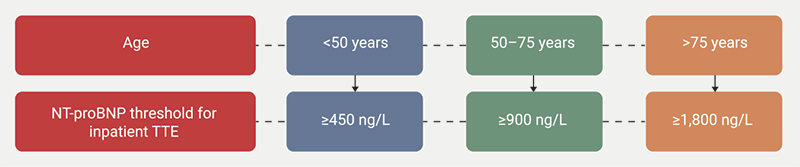
Recognising these limitations, the British Society of Echocardiography (BSE) introduced an age-adjusted NT-proBNP threshold to triage inpatient TTE requests.7 This was intended to enrich the patient population most likely to benefit from inpatient echocardiography, therefore, improving diagnostic efficiency and optimising use of the service (figure 1).
The aim of this study was to assess the diagnostic accuracy and clinical utility of the BSE’s new age-adjusted NT-proBNP thresholds within a regional inpatient setting.
Materials and method
We analysed data from consecutive inpatients who had an echocardiogram requested between 1 and 15 March 2024, at two secondary care hospitals in the East of England. Data on patient demographics, NT-proBNP values, echocardiography results, and clinical indications for imaging, were extracted from electronic health records.
Patients were subsequently grouped and compared according to the BSE NT-proBNP threshold criteria (figure 1), and whether they subsequently underwent an inpatient TTE. The diagnosis of HF was based on the echocardiogram report.
Statistical analysis
Descriptive statistics were used to summarise the patient demographics and baseline characteristics. Continuous variables were reported as mean ± standard deviation (SD) or median with interquartile range (IQR). Comparison between groups was by a two-sample t-test for means or χ2 test to compare proportions. A p value <0.05 was considered statistically significant. All statistical analysis was performed using IBM SPSS (Statistical Package for the Social Sciences) software version 27.0.1.0.
Results
A total of 159 inpatients were included in the final analysis. The mean age was 84.6 ± 5.4 years, 43.4% were women and 12.6% were non-white. Of the cohort, 57.2% and 42.1% were comorbid with CKD and AF, respectively, and 57.7% were overweight or obese (table 1).
Table 1. Patient demographics
| Demographic | N=159 |
| Mean age ± SD, years | 84.6 ± 5.4 |
| Male, n (%) | 90 (56.6) |
| Ethnicity, n (%) | |
| White British | 139 (87.4) |
| Asian or Asian British | 2 (1.3) |
| Black or Black British | 4 (2.5) |
| Unknown | 14 (8.8) |
| Comorbidities, n (%) | |
| Hypertension | 87 (54.7) |
| Diabetes mellitus | 41 (25.8) |
| Chronic kidney disease (eGFR <60 ml/min/1.73 m2) | 91 (57.2) |
| Atrial fibrillation | 67 (42.1) |
| Previous myocardial infarction | 31 (19.5) |
| Overweight (BMI 25.0–29.9 kg/m2) | 49 (30.8) |
| Obese (BMI ≥30 kg/m2) | 44 (27.7) |
| Presenting symptoms, n (%) | |
| Shortness of breath | 66 (41.5) |
| Chest pain | 34 (21.4) |
| Cough | 22 (13.8) |
| Fall | 11 (6.9) |
| Leg swelling | 11 (6.9) |
| Dizziness | 7 (4.4) |
| Syncope | 3 (1.9) |
| Confusion | 3 (1.9) |
| Incidental | 3 (1.9) |
| Laboratory values, median (IQR) | |
| Haemoglobin, g/L | 123.5 (103.5–137.0) |
| Platelet count, 109/L | 233.0 (189.0–324.0) |
| Haematocrit, L/L | 0.4 (0.3–0.4) |
| Mean corpuscular volume, (fL) | 89.6 (85.9–94.9) |
| C-reactive protein, mg/L | 25.0 (5.5–90.0) |
| Creatinine, μmol/L | 91.0 (75.8–128.3) |
| eGFR, ml/min/1.73m2 | 57.0 (38.0–73.5) |
| Sodium, mmol/L | 137.0 (134.3–140.0) |
| Total cholesterol, mmol/L | 4.0 (3.3–4.6) |
| LDL, mmol/L | 2.03 (1.55–2.7) |
| Triglycerides, mmol/L | 1.2 (0.9–1.6) |
| Troponin T, ng/L | 40.0 (15.0–94.0) |
| NT-proBNP, ng/L | 2,282 (934–7,074) |
| HbA1c, mmol/mol | 40.0 (37.0–46.0) |
| Echocardiographic results, n (%)* | |
| LVEF ≥50% | 11 (11.7) |
| LVEF 41–49% | 10 (10.6) |
| LVEF ≤40% | 28 (29.8) |
| Not heart failure | 45 (47.9) |
| * Total number of inpatient echocardiograms was 94 Key: BMI = body mass index; eGFR = estimated glomerular filtration rate; HbA1c = glycated haemoglobin; IQR = interquartile range; LDL = low-density lipoprotein; LVEF = left ventricular ejection fraction; NT-proBNP = N-terminal pro-B-type natriuretic peptide; SD = standard deviation |
|
The most common reason for an inpatient TTE request was suspected HF (52.2%, n=83). Other reasons were chest pain (12.6%, n=20), arrhythmia (3.1%, n=5), suspected valve disease (2.5%, n=4), syncope (2.5%, n=4), ACS (1.9%, n=3), infective endocarditis (1.9%, n=3), pulmonary embolism (1.3%, n=2), right heart assessment (1.3%, n=2), and stroke (0.6%, n=1).
Within our cohort, a HF diagnosis using the age-adjusted NT-proBNP thresholds, was more prevalent among patients aged over 75 years (figure 2).
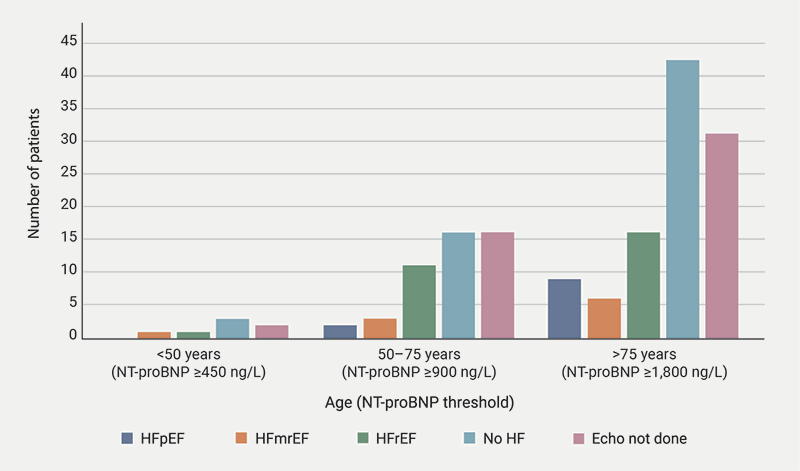
| Key: echo = echocardiography; HF = heart failure; HFmrEF = heart failure with mildly reduced ejection fraction; HFpEF = heart failure with preserved ejection fraction; HFrEF = heart failure with reduced ejection fraction; NT-proBNP = N-terminal pro-B-type natriuretic peptide |
There were 100 patients (62.9%) who met the BSE NT-proBNP threshold for an inpatient TTE. Of these, 65 (65.0%) subsequently had a TTE, of whom, 39 (60.0%) patients had a final diagnosis of HF. Of the 59 patients who did not meet the BSE threshold, 29 (49.2%) still underwent inpatient TTE and nine (31.0%) patients were diagnosed with HF. There was a statistically significant difference in the diagnostic yield based on meeting the BSE criteria but subsequently having an echocardiogram (p=0.014) (table 2). Using a HF diagnosis as the outcome, the BSE criteria demonstrated a sensitivity and specificity of 81% and 43%, respectively.
Table 2. Results summary
| Number of patients | Met BSE criteria for inpatient TTE (n=100) | Did not meet BSE criteria for inpatient TTE (n=59) | p value |
| Had echo | 65 (65%) | 29 (49.2%) | |
| Positive HF diagnosis | 39 (60%) | 9 (31.0%) | 0.014 |
| Key: BSE = British Society of Echocardiography; HF = heart failure; TTE = transthoracic echocardiography | |||
Out of the entire cohort (n=159), 67 (42.1%) patients had AF. Of these, 48 (71.6%) met the NT-proBNP threshold to trigger inpatient echocardiography, compared with 52 (56.5%) patients without AF. While there was a trend towards a higher proportion of patients with AF meeting the NT-proBNP threshold, this was not statistically significant (AF 71.6% vs. no AF 56.5%, p=0.075).
Among the 100 patients meeting the NT-proBNP threshold for inpatient echocardiography, 48 (48.0%) had AF. Of these, 37 (77.1%) underwent inpatient TTE. HF was diagnosed in 20 (54.1%) of these patients, while 17 (45.9%) had no echocardiographic evidence of HF. Among the remaining 52 patients (52.0%) without AF, 28 (53.8%) underwent TTE, with HF diagnosed in 19 (67.9%) and no HF in nine (32.1%). There was no statistically significant difference in the diagnostic yield of HF between these groups (AF + HF diagnosis 54.1% vs. no AF + HF diagnosis 67.9%, p=0.385).
Review of the false negatives
Nine patients whose NT-proBNP levels were below the BSE thresholds, had an echocardiogram that demonstrated HF. A review of these cases, however, revealed that there was additional clinical justification for an inpatient TTE, that would have resulted in a HF diagnosis. Three patients had a known diagnosis of HF, and a repeat scan was deemed clinically indicated. Two patients had subsequent inpatient cardiac magnetic resonance imaging (MRI) excluding HF and disproving the prior abnormal echocardiogram result. One patient presented with ACS, and another with ventricular tachycardia, both warranting inpatient TTE for this clinical indication. One patient had a clinical presentation highly suggestive of HF, justifying inpatient TTE despite NT-proBNP not meeting the diagnostic threshold, and one patient was a duplicate case. These patients were not excluded from analysis as the aim was to evaluate the BSE NT-proBNP thresholds in a real-world setting, in which indications for an echocardiogram are not always stand-alone and can overlap; including them avoids selection bias.
Discussion
This study provides real-world evidence that the current BSE age-specific NT-proBNP thresholds correctly identify most inpatients who have HF with a high sensitivity (81%). It is, therefore, appropriate as a rule-out screening tool to help reduce unnecessary inpatient echocardiograms in patients with a low pre-test probability of HF. The observed specificity (43%), reflects the well-recognised limitations of NT-proBNP as a rule-in test, due to its elevation in a variety of non-cardiac conditions, reinforcing the need for clinical interpretation alongside biomarker use.8,9
These findings are consistent with a previous study, including a retrospective analysis assessing the European Society of Cardiology’s (ESC’s) age-adjusted natriuretic peptide thresholds, which similarly demonstrated a higher sensitivity but lower specificity.10 Notably, in our cohort, no true cases of HF were missed when applying the BSE criteria. The few patients with NT-proBNP levels below threshold who were ultimately diagnosed with HF had alternative clinical indications for inpatient echocardiography, suggesting that the criteria allow sufficient flexibility to accommodate complex presentations or co-existing pathologies.
While age correlates with NT-proBNP levels, our data show that other factors, particularly CKD, obesity and AF were prevalent in this cohort; 36.5% (n=58) of the cohort had two or more of these comorbidities (table 1). These are known to influence NT-proBNP concentrations and may reduce test specificity. Consequently, we observed a non-significant association between a diagnosis of AF and the likelihood of meeting the NT-proBNP threshold to trigger inpatient TTE. However, the diagnostic yield for HF in patients with AF who underwent TTE, while proportionally higher, was statistically non-significant when compared with a non-AF population. This finding reflects the recognised association between AF and elevated levels of NT-proBNP, even in the absence of ventricular dysfunction, potentially leading to false-positive triage results. Nevertheless, the observation that a substantial proportion of patients with AF and an elevated NT-proBNP had a diagnosis of HF, supports the continued clinical value of this biomarker, even within this subgroup, in the acute inpatient setting.
Future research should explore the feasibility of incorporating additional adjustment factors for comorbidities into the threshold algorithm to improve diagnostic accuracy.
TTE remains an essential, non-invasive tool in HF assessment, however, inappropriate requesting is common. Adoption of the BSE criteria could help curb unnecessary TTEs, optimising resource allocation and ensuring that imaging is prioritised for those with the highest likelihood of diagnostic benefit.13 While NT-proBNP testing may further aid triage, it should be interpreted alongside clinical assessment, as elevated levels can occur in the absence of HF and reliance on the biomarker alone could inadvertently increase demand on TTE services.
Limitations
The study’s retrospective design, small cohort size, short duration, and single-region sampling may limit generalisability.
Conclusion
This study demonstrates the BSE’s age-specific NT-proBNP thresholds for triaging inpatient echocardiography requests is a safe and effective approach to support the diagnosis of HF. By enhancing diagnostic efficiency, it has the potential to alleviate pressure on echocardiography services and facilitate more appropriate allocation of imaging resources. Our findings support broader adoption of this framework in clinical practice.
Further research is warranted to validate these results prospectively across diverse healthcare settings. Future studies should assess the impact of this approach on diagnostic timelines, clinical outcomes, and healthcare costs. Additionally, incorporating other clinical and biochemical risk factors into triage algorithms, such as renal function and body mass index (BMI), may improve specificity and refine the utility of NT-proBNP in HF diagnosis.
Key messages
- The British Society of Echocardiography’s (BSE’s) age-adjusted N-terminal pro-B-type natriuretic peptide (NT-proBNP) thresholds are a safe and effective tool for triaging inpatient transthoracic echocardiogram (TTE) requests in suspected heart failure (HF), maintaining high diagnostic sensitivity (81%)
- No cases of HF were missed when applying the BSE criteria retrospectively; all patients with low NT-proBNP and a subsequent HF diagnosis had alternative clinical indications for TTE
- This strategy improves diagnostic efficiency and reduces unnecessary echocardiography, with a significantly higher diagnostic yield in patients meeting BSE NT-proBNP thresholds (60.0% vs. 31.0%, p=0.014)
- Implementation of the BSE framework may help alleviate pressure on overstretched echocardiography services, while ensuring high-risk patients are appropriately prioritised
Conflicts of interest
None declared.
Funding
None.
Study approval
This was a retrospective service evaluation with the use of anonymised patient data. Formal ethical approval and individual patient consent were therefore not required. The study received approval from the Mid and South Essex NHS Foundation Trust clinical governance board and was conducted according to the principles outlined in the Declaration of Helsinki.
References
1. McDonagh TA, Metra M, Adamo M et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021;42:3599–726. https://doi.org/10.1093/eurheartj/ehab368
2. Januzzi JL Jr, Chen-Tournoux AA, Christenson RH. Natriuretic peptides for the diagnosis and management of heart failure. J Am Coll Cardiol 2018;72:1181–93. https://doi.org/10.1016/j.jacc.2018.06.020
3. Easa J, Chappell J, Warriner D. Understanding the pathogenesis of heart failure. Pract Nurs 2021;32:54–8. https://doi.org/10.12968/pnur.2021.32.2.54
4. Doust J, Lehman R, Glasziou P. The role of BNP testing in heart failure. Am Fam Physician 2006;71:1893–900. Available from: https://www.aafp.org/pubs/afp/issues/2006/1201/p1893.html
5. National Institute for Health and Care Excellence (NICE). Heart failure – chronic: diagnosis – how to assess. Clinical Knowledge Summaries. London: NICE. Available from: https://cks.nice.org.uk/topics/heart-failure-chronic/diagnosis/how-to-assess/
6. Welsh P, Campbell RT, Mooney L et al. Reference ranges for NT-proBNP (N-terminal pro-B-type natriuretic peptide) and risk factors for higher NT-proBNP concentrations in a large general population cohort. Circ Heart Fail 2022;15:e009427. https://doi.org/10.1161/circheartfailure.121.009427
7. British Society of Echocardiography. Clinical indications and triaging for emergency, inpatient and critical care echocardiography. London: BSE, 2023. Available from: https://www.bsecho.org/common/Uploaded%20files/Education/Posters/PUE006_Clinical-indications-triaging_emergency-inpatient-critical-care.pdf
8. Maisel A, Mueller C, Adams K Jr et al. State of the art: using natriuretic peptide levels in clinical practice. Eur J Heart Fail 2008;10:824–39. https://doi.org/10.1016/j.ejheart.2008.07.007
9. Horwich TB, Hamilton MA, Fonarow GC. B-type natriuretic peptide levels in chronic heart failure. J Am Coll Cardiol 2006;47:52–5. https://doi.org/10.1016/j.jacc.2005.07.070
10. Taylor CJ, Taylor KS, Ordonez-Mena JM et al. ESC heart failure association age-adjusted natriuretic peptide thresholds for a new diagnosis of heart failure: diagnostic accuracy study. Eur Heart J 2024;45(suppl 1):ehae666.949. https://doi.org/10.1093/eurheartj/ehae666.949
11. Richards M, Di Somma S, Mueller C et al. Atrial fibrillation impairs the diagnostic performance of cardiac natriuretic peptides in dyspneic patients: results from the BACH study (Biomarkers in ACute Heart Failure). JACC Heart Fail 2013;1:192–9. https://doi.org/10.1016/j.jchf.2013.02.004
12. Mehrabi EN, Toupchi‐Khosroshahi V, Athari SS. Relationship of atrial fibrillation and N terminal pro brain natriuretic peptide in heart failure patients. ESC Heart Fail 2023;10:3250–7. https://doi.org/10.1002/ehf2.14542
13. Khalili A, Drummond J, Ramjattan N et al. Diagnostic and treatment utility of echocardiography in the management of the cardiac patient. World J Cardiol 2020;12:262–8. https://doi.org/10.4330/wjc.v12.i6.262
