A 79-year-old woman presents to the hospital with dyspnoea, fever, and hypotension, and is diagnosed with community-acquired pneumonia and septic shock. Resuscitation is initiated with fluids and vasopressors, and a central venous catheter is placed. However, during the procedure, the guide experiences resistance and cannot be removed, becoming trapped. This is confirmed with tomography and reconstruction, demonstrating intravascular position. The patient is then sent to interventional cardiology for extraction, which is successfully performed using the EN Snare (Merit Medical). The significance of this case lies in the complications of not guiding procedures with ultrasound and how to resolve them, such as the guide being trapped in this patient.
Introduction
Central venous line insertion is a common procedure in the hospital setting, but as an invasive procedure, it is not free from potential complications, which include infectious, thrombotic, and mechanical aspects. The latter include vascular perforation, arrhythmias, cardiac perforation, tamponade and, although exceptional, knotting of the guidewire has been documented.
Case
 |
 |
 |
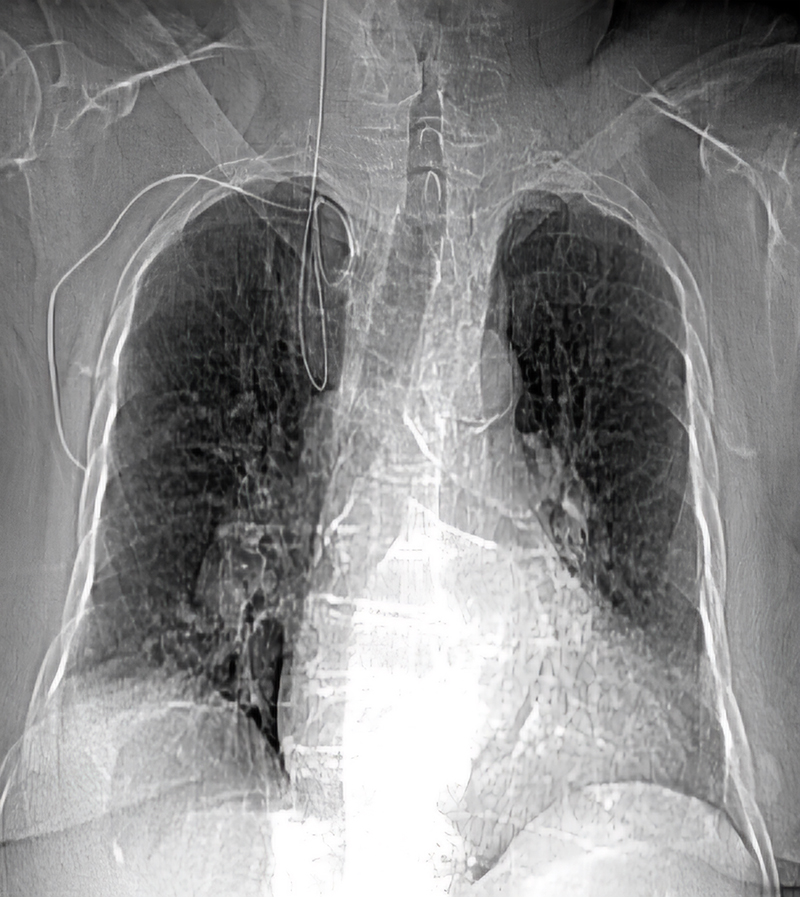
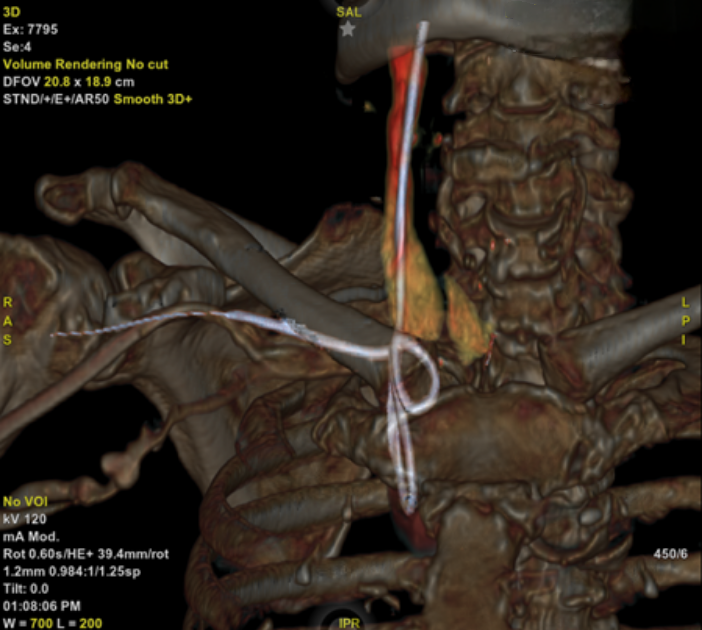
We present the case of a 79-year-old woman admitted to another hospital unit for dyspnoea at rest, fever and hypotension. The final diagnosis was community-acquired pneumonia and septic shock. Initiation of amines and placement of a right subclavian central venous catheter were required. During the procedure, resistance to the advancement of the guidewire was detected, which could not be extracted. The control X-ray revealed knotting that prevented the removal of the guidewire (figure 1), necessitating referral to the interventional cardiology service of our centre for percutaneous extraction. Prior to the decision to extract, a computed tomography (CT) with three-dimensional reconstruction was performed, which demonstrated the intravascular position of the guidewire (figure 2).
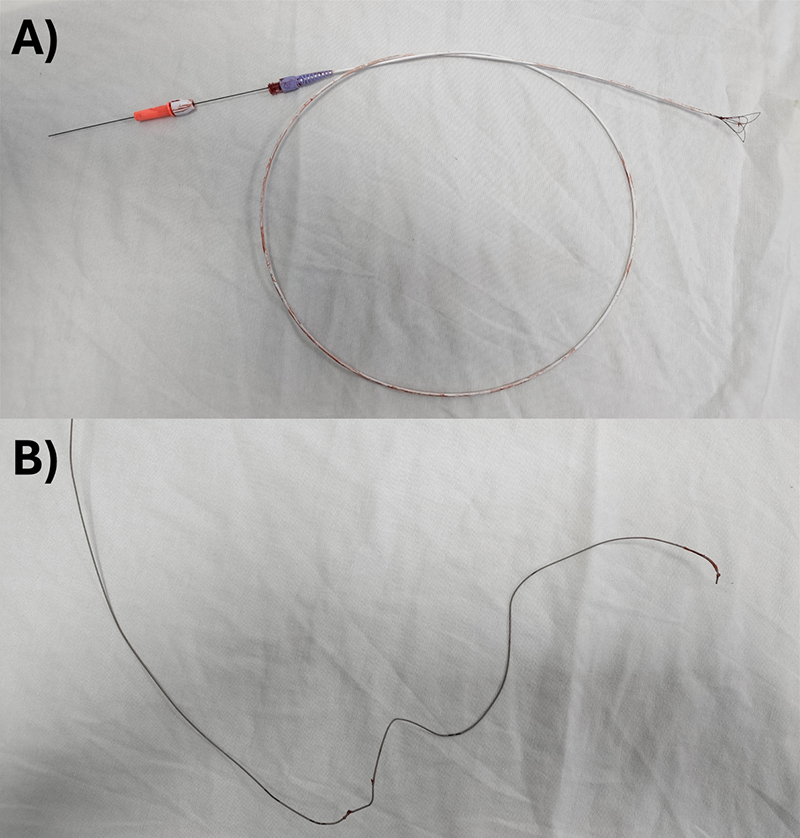
A right femoral venipuncture was performed using an 8 French introducer, and fluoroscopy was employed to visualise the distal end of the knotted guide. The EN Snare 12–20 mm three-loop snare wire extraction device (Merit Medical, Salt Lake City, US) was utilised to snare the tip of the wire under fluoroscopic guidance and extract it completely via the right femoral route. It was removed without complications (figure 3).
Discussion
Mechanical complications associated with central venous catheterisation (CVC), such as embolisation, migration, fracture or vascular entrapment of the guidewire, occur in 1% of patients.1 However, knotting and intravascular entrapment are even more infrequent, with only one case report. Potential risk factors include operator inexperience,2 history of multiple CVCs at the same site, and subclavian catheter placement associated with costoclavicular pinch syndrome.3
Vascular guidewire embolism is a serious complication with a high mortality rate (60–71%),4 resulting in vascular blockage, myocardial perforation,3 thromboembolism, arrhythmias, endocarditis and sepsis.5 Extraction, even in asymptomatic patients, is recommended due to its severity. The percutaneous technique, introduced in the 1960s, offers a success rate of 80–100% in fragment removal.6
Percutaneous extraction, through femoral venous access, is consolidated as the gold standard in the removal of intravascular foreign bodies, highlighting the preference for right femoral access. This choice is based on key advantages, such as the ergonomics of handling the instruments, the possibility of using larger calibre sheaths, the ease of puncture, and the ability to apply an effective and safe compression at the end of the procedure. In addition, the adequacy of the calibre for various diameters of the device used is highlighted, as well as the option of using the contralateral femoral vein in challenging situations.4
Success rates for percutaneous intravascular foreign body removal are a remarkable 97.8%,4 although it is imperative to consider complications, which include transient ventricular tachycardia, tricuspid valve instability and possible haematoma formation at the puncture site.7
Various materials are currently available for foreign body removal, ranging from loop catheters and basket devices to more specialised instruments, such as biotomes. The choice among these materials is guided by the preferences and expertise of the medical personnel involved in the procedure.5
In the rare scenario of a failed percutaneous extraction, consideration of alternative access through the internal jugular vein is suggested.5 As a last resort, and reserved for exceptional circumstances, surgical approach via median sternotomy is contemplated.2 This approach, while less common, is reserved to ensure safe resolution of the situation, preserving the patient’s health with minimal morbidity.
It is crucial to highlight the substantial and consistent evidence demonstrating the advantages of ultrasound guidance in CVC procedures. This approach significantly minimises the risk of complications, including failed cannulation, arterial puncture, haematoma, pneumothorax, and haemothorax.8
Conclusion
Guidewire-related complications during CVC are mostly mechanical and may include fracture, leakage, knotting, and intravascular entrapment. In this case, one patient had a guidewire-related complication during CVC, specifically retention, knotting and coiling. This is an uncommon mechanical complication, with few cases reported in the literature. Possible risk factors for this rare complication include operator inexperience, previous CVC at the same site, multiple punctures, physical fatigue, night shifts and demanding situations.
It is crucial to approach the diagnosis and management of these cases in a multi-disciplinary manner, often involving a vascular surgeon, given the potential risks involved in guidewire removal. In this case, the patient was referred to the haemodynamics department for removal by percutaneous extraction using the Merit Medical EN Snare guidewire successfully.
It is important to note that the use of ultrasound guidance for CVC has been shown to significantly reduce complications.
Conflicts of interest
None declared.
Funding
None.
Patient consent
Written informed consent was obtained from the patient for publication of this case report, including accompanying images.
References
1. Motta Leal Filho JM, Carnevale FC, Nasser F et al. Endovascular techniques and procedures, methods for removal of intravascular foreign bodies. Rev Bras Cir Cardiovasc 2010;25:202–08. https://doi.org/10.1590/S0102-76382010000200012
2. Corzo RJ, Parra R, Meléndez HJ. Guía retenida y anudada extravascular durante un cateterismo venoso central: reporte de un caso. Salud UIS 2014;46:61–4. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0121-08072014000100007&lng=en
3. Polderman KH, Girbes AR. Central venous catheter use part 1: mechanical complications. Intensive Care Med 2002;28:1–17. https://doi.org/10.1007/s00134-001-1154-9
4. Leite TFO, Pazinato LV, Bortolini E, Pereira OI, Nomura CH, Filho JMDML. Endovascular removal of intravascular foreign bodies: a single-center experience and literature review. Ann Vasc Surg 2022;82:362–76. https://doi.org/10.1016/j.avsg.2021.12.003
5. Chiesa P, Ríos M, Giúdice J. Captura y extracción percutánea de cuerpos extraños intravasculares. Arch Pediatr Urug 2019;90:270–5. https://doi.org/10.31134/AP.90.5.3
6. de Castro Bienert IR, Chiozzi RLLAF, Mota CEC, Braga JS, Bombonato R, Kajita LJ. Percutaneous removal of intravascular catheter fragment – an adaptation of the toolbox. Revista Brasileira de Cardiologia Invasiva (English Edition) 2013;21:291–4. https://doi.org/10.1016/S2214-1235(15)30147-2
7. Intagliata E, Basile F, Vecchio R. Totally implantable catheter migration and its percutaneous retrieval: case report and review of the literature. G Chir 2017;37:211–15. https://doi.org/10.11138/gchir/2016.37.5.211
8. Wu SY, Ling Q, Cao LH, Wang J, Xu MX, Zeng WA. Real-time two-dimensional ultrasound guidance for central venous cannulation: a meta-analysis. Anesthesiology 2013;118:361–75. https://doi.org/10.1097/ALN.0b013e31827bd172
