Severe mitral regurgitation (MR), when complicated by a co-existing lung abscess, is a management challenge, as both conventional cardiac and thoracic surgical interventions may be contraindicated. In the case described below, transcatheter edge-to-edge mitral valve repair (TEER) was utilised to achieve haemodynamic stability, permitting subsequent thoracic surgical lung abscess resection.
We report the case of a 60-year-old man with torrential MR secondary to chordal rupture presenting with recurrent pulmonary oedema, complicated by lung sepsis and abscess formation resistant to antibiotic therapy and precluding open valvular repair. The presence of a lung abscess contraindicated open mitral valve repair, and the severity of MR precluded thoracic surgical treatment of the lung abscess, precluding any form of surgical intervention.
A successful TEER procedure resulted in a reduction of MR from severe to no more than mild-to-moderate, enabling haemodynamic stabilisation and permitting subsequent thoracic surgical treatment of the lung abscess.
Our case demonstrates the possibility of treating severe MR with TEER in the presence of a lung sepsis and abscess, when both conventional cardiac and thoracic surgical interventions were considered contraindicated. This later enabled thoracic surgery and treatment of the lung abscess.
Introduction
Mitral regurgitation (MR) is one of the most common valvular pathologies affecting around 2% of the Western population, and is classified into primary and secondary causes.1,2 Primary causes involve degenerative changes due to ageing and/or mitral valve prolapse. Secondary causes are described as functional and are commonly caused by annular enlargement secondary to structural changes of the left ventricle and left atrium.3
Case presentation
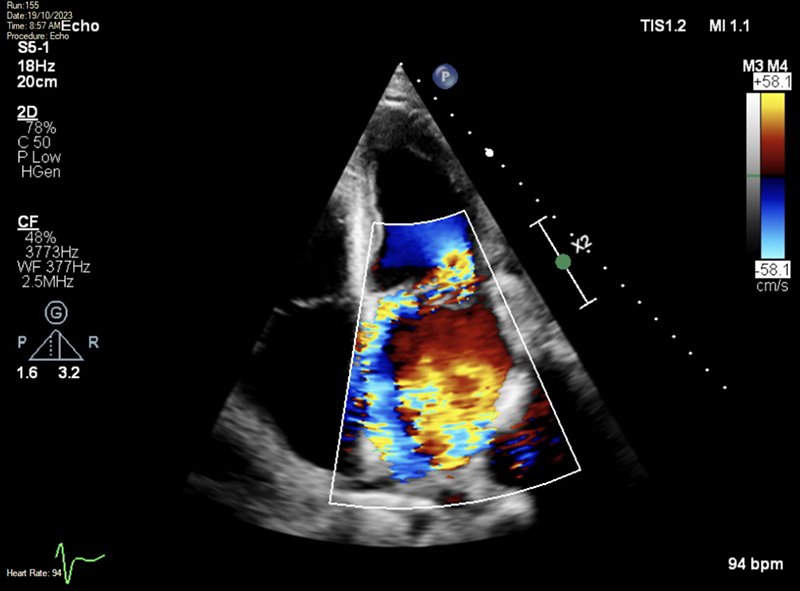
A previously fit and healthy 60-year-old man presented with recurrent and severe pulmonary oedema. Clinical assessment and an initial transthoracic echocardiogram (TTE) showed a flail posterior mitral valve (MV) leaflet (P2) associated with chordal rupture and torrential eccentric MR (figure 1). Left ventricular (LV) function, in this off-loaded state, was preserved with an ejection fraction (EF) of 60%.
Initially, the patient was treated with intravenous furosemide and intravenous antibiotics, but did not respond to these interventions, demonstrating a continuing supplemental oxygen requirement and ongoing evidence of infection. The antibiotics, initially started empirically, were clarithromycin and combination piperacillin and tazobactam (Tazocin) for 20 days due to raised inflammatory markers and temperature spikes.
A repeat TTE, two weeks after admission, was unchanged from the previous study and there was no improvement in the patient’s clinical status. Blood cultures were sterile and viral tests were negative. Results for sputum samples from bronchial wash came back positive for Pseudomonas aeruginosa, antibiotics were then switched to meropenem for five days, with two stat doses of amikacin during that period based on sensitivities. A repeat chest X-ray and subsequent thoracic computed tomography (CT) scan showed evidence of new pulmonary consolidation and possible lung abscess formation.
The patient’s presentation, clinical course, and imaging were discussed at the local joint surgical and cardiology multi-disciplinary meeting (MDT). The MDT consensus was that open surgical repair was contraindicated by the presence of the pulmonary abscess. Similarly, thoracic surgical intervention for the lung abscess was considered contraindicated by the presence of severe MR, leading to a therapeutic impasse.
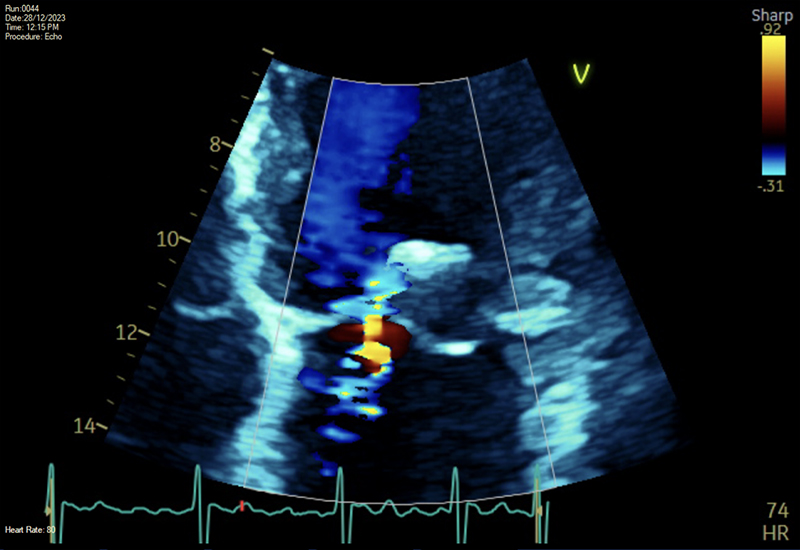
To break this impasse, an uncomplicated transcatheter edge-to-edge mitral valve repair (TEER) was undertaken under general anaesthesia using Pascal with a reduction of the left atrial (LA) V-wave from 50 mmHg to only 17 mmHg following double-clip deployment (figure 2). A post-procedural TTE demonstrated Pascals in situ with only mild-to-moderate residual MR, a mean transmitral gradient of only 3 mmHg, and just modest LV impairment with an EF of 49%. The patient was subsequently switched to oral diuretics and remained haemodynamically stable.
Thoracic surgical intervention was now successfully undertaken utilising video-assisted thoracic surgery (VATS) with wedge resection of his right lower lobe encompassing the lung abscess, along with a lymph node dissection. These showed consolidation, in keeping with organising pneumonia and necrosis, with granulomatous inflammation, respectively. Post-TEER and VATS he continued oral clindamycin and ciprofloxacin for five days and then oral linezolid for another five days. The patient was discharged home subsequently without complications. He continued to be followed-up for four months post-TEER and VATS and has remained well since.
Conclusion
TEER facilitated the successful management of severe MR in an individual who was simultaneously haemodynamically compromised and septic, and, thus, considered untreatable by conventional surgical technologies. This case demonstrated the utility of TEER when both conventional cardiac and thoracic surgical interventions were considered contraindicated.
Conflicts of interest
None declared.
Funding
None.
Patient consent
The patient provided written consent for publication.
References
1. Douedi S, Douedi H. Mitral Regurgitation. Treasure Island (FL): StatPearls Publishing, 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553135/
2. NHS England. Evidence review: clinical and cost-effectiveness and adverse events associated with percutaneous mitral valve leaflet repair for severe degenerative mitral regurgitation (MitraClip). London: NHS England, May 2018. Available from: https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2019/07/Evidence-Review_Percutaneous-mitral-valve-leaflet-repair-for-primary-degenerative-mitral-regurgitation-in-adul.pdf
3. O’Gara PT, Mack MJ. Secondary mitral regurgitation. N Engl J Med 2020;383:1458–67. https://doi.org/10.1056/NEJMcp1903331
