Introduction
Patients diagnosed with atherosclerotic cardiovascular disease (CVD) are at very high risk of recurrent cardiac events.1 Appropriate management of risk factors and the implementation of healthy behaviours (including smoking cessation, recommended physical activity, a healthy diet, and maintaining a healthy weight) can significantly decrease the risk of future cardiovascular events; changes in lifestyle could reduce cardiovascular mortality by up to 75%.1 Commencing appropriate cardio-protective evidence-based medication can also improve quality of life, and reduce mortality and morbidity.2
Cardiac rehabilitation (CR) programmes provide structured education and activity for patients recovering from cardiovascular events, incorporating clinical assessments, medical management, supported physical activity, and psychosocial care. Despite strong evidence that attendance at such programmes can improve patient outcomes, challenges persist in improving uptake and completion rates.
Evidence for, and uptake of, cardiac rehabilitation
Patients admitted with acute coronary syndrome (ACS) should be offered a programme of cardiac rehabilitation (CR) within 10 days of discharge, according to guidelines from the British Association of Cardiovascular Prevention and Rehabilitation (BACPR)3 and the National Institute for Health and Care Excellence (NICE).4
There is a plethora of strong evidence to support the use of CR programmes,1–4 which have been shown to have improvements on mortality, quality of life, and reduction on further hospital admissions as well as being cost effective. Despite this, uptake of CR has plateaued over recent years to around 50%5 (figure 1) – some way from the NHS Long Term Plan target of 85% accessing CR by 2028.6 There may be a reluctance to refer certain groups, for example women, those from ethnic minorities or lower socioeconomic groups.7
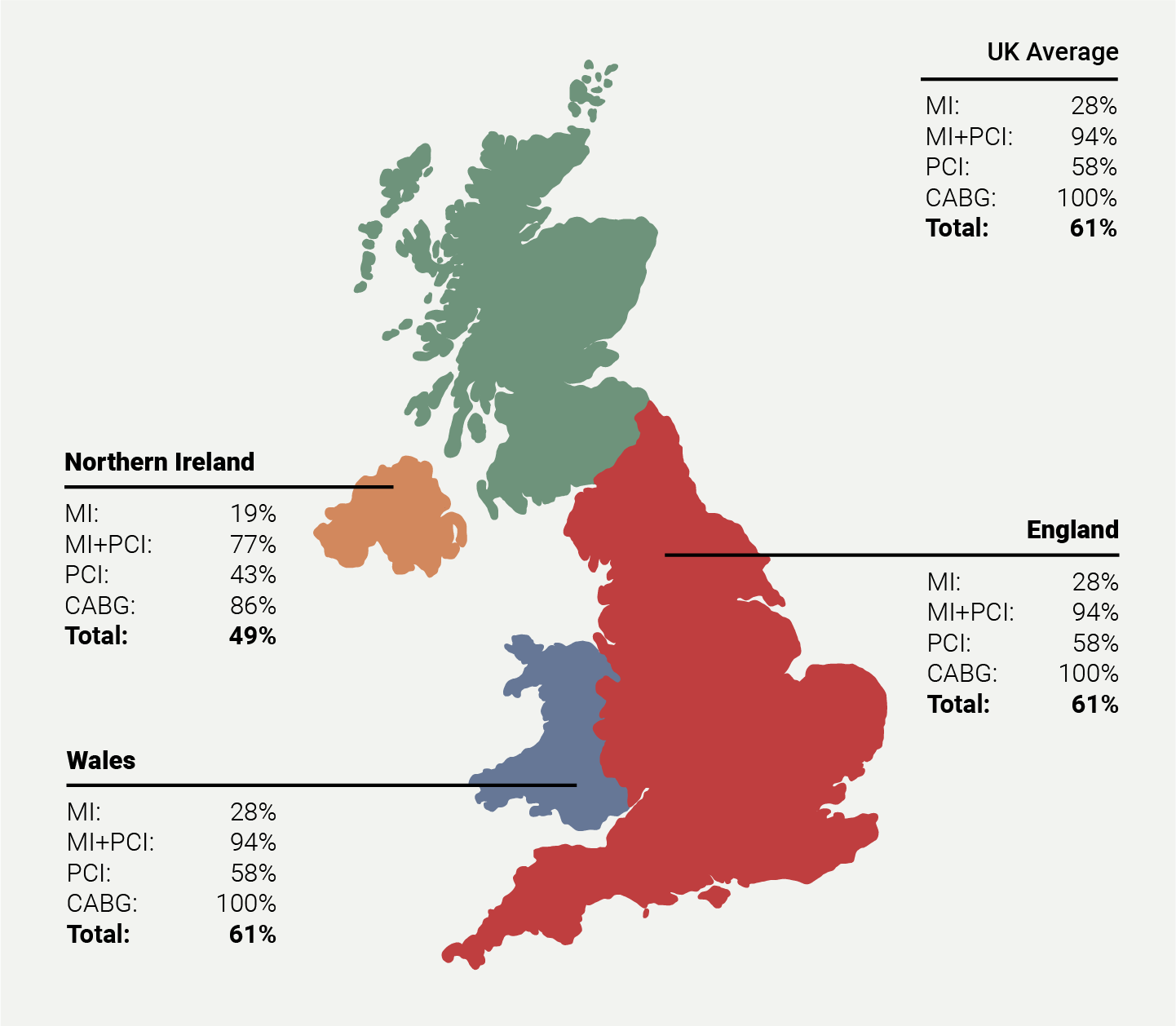
| Key: CABG = coronary artery bypass graft; MI = myocardial infarction; PCI = percutaneous coronary intervention The National Audit of Cardiac Rehabilitation collects data across England, Wales and Northern Ireland; it does not include data from Scotland, which is instead submitted to the Scottish Cardiac Audit Programme. |
Health inequalities and access to care
It is important to acknowledge that there are differences and heath inequalities within this population group. Analysis of the CVDPREVENT data recommends that integrated care boards (ICBs) should address health inequalities in CVD prevention targets – especially blood pressure control and lipid-lowering therapies – for example in females, those in black or mixed ethnicities and those in the most deprived quintiles.8
Evidence from the British Heart Foundation (BHF) recognises the strong associations between CVD and health inequalities in terms of prevalence, treatment and outcomes for CV disease and risk factors. There is also a deep connection to the wider determinants of health, for example, income, housing, education, the environment, and access to health and social care.9
Additional challenges have arisen around a growing population of people living with multiple long-term conditions with increased symptom burden, and older adults with frailty. These factors can affect the medical management of ACS and eligibility for CR programmes.10
Role of pharmacotherapy in CR
Another priority following an ACS event is the adherence to medication therapy, in particular antithromboembolic treatments, renin–angiotensin–aldosterone system blockers, beta blockers, and statins.2 However, data from the EUROASPIRE V survey identifies there is a wide gap between evidence-based guidelines and everyday clinical practice, with less than half of patients taking medication to help reduce their cardiovascular risk.11
Role of CR programmes
Box 1: Components of the ideal CR programme
style=”background-color: lightgrey; border-bottom: 2px solid grey; padding: 5px;
|
According to the BACPR standards and core components, CVD prevention and rehabilitation programmes (CPRP) should have an individualised approach, ideally designed in partnership with the patient, with agreed and co-produced manageable goals.3
UK guidelines acknowledge that patients should be offered a choice in how, when and where the CPRP is delivered, to help increase uptake and completion.3–5,12
CR programmes vary in their level of intensity and duration; this may be linked to the different modes of commissioning that currently exist across the UK. They should collaborate and engage with the patient’s wider care teams (primary, secondary, tertiary and voluntary) to create a comprehensive and integrated approach to CVD prevention.3
After hospital discharge
Patients should be provided with advice and support around their diagnosis and treatment prior to discharge.13 UK guidelines recommend that support should be provided by CR specialists whilst the patient is still in hospital.4,7 However, this provision is variable in different regions, with some CR providers starting their initial assessment immediately post-discharge – particularly for patients who have a short-duration admission and rapid discharge.
Involvement of family and carers
There are a lot of adjustments for patients to consider following their ACS event, including:
- Concern about it happening again
- Uncertainty about which activities they can or can’t do
- Questions about managing medications
- Queries on returning to employment
- Managing emotions – symptoms of anxiety and depression are common14
The involvement of family and carers to help understand signs and symptoms is also crucial for aftercare support; partner support can help with adjustments post-event and aid a more successful recovery.15
Secondary preventative pharmacotherapy
For patients who have experienced their first event, there are additional challenges in regard to managing new secondary prevention medications,16 most commonly:4
- Angiotensin-converting enzyme (ACE) inhibition
- Dual antiplatelet therapy (aspirin plus a second antiplatelet agent) – unless there is a separate indication for anticoagulation
- Beta blockers
- High-dose statins
The ACE inhibitor and beta blocker will require uptitration to gain full optimisation of treatment; additional blood tests are required during uptitration of the ACE inhibitor to monitor renal function.
The shared management of patients following their event are usually between CR services and primary care teams. Good communication is essential between secondary and primary care to ensure that evidence-based practice is in place for this population.16
Discharge letter
Box 2. Minimum detail required in a discharge letter
style=”background-color: lightgrey; border-bottom: 2px solid grey; padding: 5px;
|
Effective discharge planning leads to an improvement in the patient’s long-term prognosis.17 The Royal College of Physicians recommend that patients should understand their diagnosis and treatment plan and strongly advise the use of patient advice leaflets prior to discharge.18
Written discharge communication from secondary care following an ACS event is crucial to inform the general practitioner (GP) of diagnosis, treatment and recommendations or actions. However, GPs often find discharge letters either lacking in information, too long or in a convoluted format. Patients are often given a copy of their discharge letter, which ideally needs explanation by a healthcare professional. It is important to not include any abbreviations, ‘unmet’ promises or unrealistic expectations.18
Following an ACS admission, the letter should also include follow up by a CR service, per UK and European guidelines.4,5,13
Role of non-medical prescribers (NMP) in CR
Advanced practice skills for nurses became increasingly widespread as a result of the European working time directive (which reduced the working hours of junior doctors), and the increased workforce demands caused by the complex health needs of an ageing population.19
CR specialist nurses can provide a high-quality service by reviewing the patient in a timely manner post-discharge, and ensuring that medications are titrated and monitored safely.20 They are also in the ideal position to liaise between cardiology consultants and primary care.
The BACPR Standards and Core Components (2023) for Cardiovascular Disease Prevention and Rehabilitation state that an NMP “should be part of the multidisciplinary team and should consider developing appropriate treatment algorithms for the wider team”. This would enable the optimisation of medical risk factors and improve long-term patient outcomes,3 in line with ESC guidance on post-ACS care, which states that lipid-lowering therapies should be started as early as possible post-discharge for both prognostic benefit and improved adherence.10,21
One year post-discharge
Following an ACS event, follow-up takes place around four to six weeks but there is no real evidence that 12-month follow up, which provides an opportunity to re-evaluate a patient’s risk factors, routinely takes place.
Sabouret et al.13 recommend follow up with cardiologists at four to six weeks, plus a further four to six weeks, and follow up from the GP on a regular three-monthly basis. Current workforce issues in primary care make this improbable and a dialogue between primary and secondary care would be desirable.
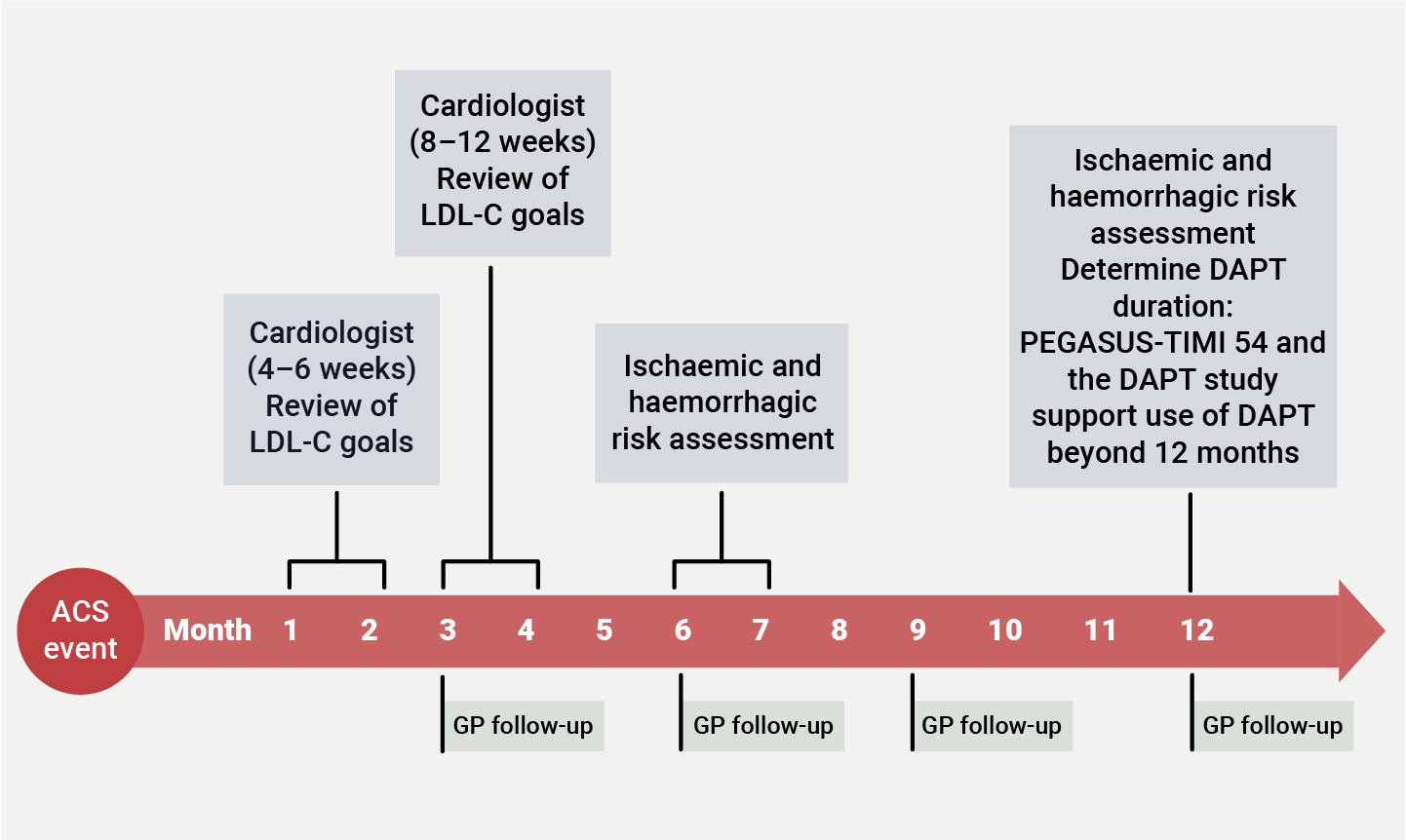
| Key: ACS = acute coronary syndrome; DAPT = dual antiplatelet therapy; LDL-C = low-density lipoprotein cholesterol; GP = general practitioner; PEGASUS-TIMI 54 = Prevention of cardiovascular events in patients with prior heart attack using ticagrelor compared to placebo on a background of aspirin-thrombolysis in myocardial infarction 54 |
In the UK, National Audit Cardiac Rehabilitation (NACR) encourage CR services to upload 12-month assessment data but the reporting from such assessment is low. ESC guidelines recommend that patients have an annual evaluation after their revascularisation event to re-assess medication compliance and adherence to targets.21
The BACPR minimum criteria for discharge summaries aim to support CR programmes in communicating long-term strategies for the patient’s management at the point of discharge.22
Case study
This is a real patient who has given permission to be included in this module
Presentation
- 48-year-old male
- Diagnosed with ST-elevation myocardial infarction and underwent percutaneous coronary intervention
- Echocardiogram shows severe left ventricular systolic dysfunction (ejection fraction: 30%)
Medication on discharge
- Aspirin 75 mg daily
- Prasugrel 10 mg daily
- Bisoproplol 2.5 mg daily
- Ramipril 1.25 mg daily
- Eplerenone 25 mg daily
- Dapagliflozin 10 mg daily
- Atorvastatin 80 mg daily
Initial CR assessment
- Assessment completed by a qualified NMP CR specialist by telephone
- Patient described feeling tired and lightheaded; no other symptoms noted
- No access to baseline bloods
- NMP liaised with patient’s GP to access new sample, and asked surgery to check blood pressure and heart rate
Second review
- In view of symptoms, ramipril dosing was moved to nighttime
- Eplerenone dosing moved to lunchtime
Third review (four weeks post-discharge)
- Patient reviewed in a face-to-face appointment as driving was now permitted
- Blood pressure, heart rate and renal function re-checked
- Uptitration of ramipril was considered the priority, due to the patient’s poor heart function
Ongoing follow up
- Patient is reviewed by the NMP every two to three weeks during their attendance at a CR exercise and education programme
- Symptoms have now settled
- Blood pressure and renal function are checked prior to patient attending the exercise sessions
- Ramipril uptitration to 10 mg daily was completed within two months of discharge
- Next priority is considered to be uptitration of the beta blocker bisoprolol, while keeping an eye on the patient’s heart rate
- GP is informed by email after every consultation to ensure the patient’s primary care records are updated
Key messages
- CR attendance rates currently fall short of national targets – This is in spite of strong evidence showing CR programmes are linked to improvements in mortality, quality of life, and reduction of rehospitalisation, as well as being cost effective. Health inequalities are evident, with some groups (for example, those in areas of high deprivation) being less likely to access CR.
- Effective CR begins at discharge – Patients’ discharge letters should provide both patients and their GPs with clear, concise and coherent information about their medical management and long-term follow up. Both the cardiologist and GP should have regular touchpoints with patients in the first year post-discharge to monitor lipid-lowering and anticoagulation therapies, and review their progress towards goals.
- An individualised approach to CR is crucial, with agreed goals – Such an approach should take into consideration (among other factors) the patient’s lifestyle, cardiovascular risk factors, comorbidities, psychosocial health, exercise capacity, mood, and quality of life.
References
1. Panattoni G, Monzo L, Gugliotta M et al. Optimal management of patients after acute coronary syndrome. Eur Heart J 2023;25(Supplement C):C84–9. https://doi.org/10.1093/eurheartjsupp/suad039
2. Gray HH, Henderson RA, De Belder MA, Underwood SR, Camm AJ. Early management of unstable angina and non-ST-segment elevation myocardial infarction: summary of NICE guidance. Heart 2010;96:1662–8. https://doi.org/10.1136/hrt.2010.204511
3. Dawkes S, Samani NJ. The BACPR Standards and Core Components for Cardiovascular Disease Prevention and Rehabilitation 2023 (4th Edition) 2023. Available from: https://www.bacpr.org/s/BACPR-Standards-and-Core-Components-2023.pdf (Accessed August 2025)
4. National Institute for Health and Care Excellence (NICE). Acute coronary syndromes. NICE Guideline NG185. Published November 2020, last reviewed December 2024. https://www.nice.org.uk/guidance/ng185 (Accessed August 2025)
5. British Association for Cardiovascular Prevention and Rehabilitation, British Heart Foundation, NHS Digital. The National Audit of Cardiac Rehabilitation Quality and Outcomes Report 2019. 2019. Available from: https://www.bhf.org.uk/-/media/files/information-and-support/publications/hcps/nacr-quality-and-outcomes-report-2019.pdf?rev=8199a23df720465fb928be44cde83258 (Accessed August 2025)
6. NHS. NHS Long Term Plan (Published July 2025). Available from: https://www.longtermplan.nhs.uk/ (Accessed August 2025)
7. Taylor RS, Dalal HM, McDonagh STJ. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol 2021;19:180–94. https://doi.org/10.1038/s41569-021-00611-7
8. Health Quality Improvement Partnership (HQIP). CVD Prevent. Using data to drive cardiovascular disease prevention. HQIP, 2024. https://www.hqip.org.uk/resource/cvdprevent-dec2024/ (Accessed August 2025)
9. British Heart Foundation. How inequalities contribute to heart and circulatory diseases. Available from: https://www.bhf.org.uk/what-we-do/our-research/heart-statistics/health-inequalities-research/inequalities-in-heart-and-circulatory-diseases-in-england (Accessed August 2025)
10. Gilard RD. Follow-up management after an acute coronary syndrome. Available from: https://www.escardio.org/Councils/Council-for-Cardiology-Practice-(CCP)/Cardiopractice/follow-up-management-after-an-acute-coronary-syndrome (Accessed August 2025)
11. Santos RD. EUROASPIRE V and uncontrolled risk factors in primary prevention: atherosclerotic cardiovascular disease in the making. Eur J Prev Cardiol 2020;28:380–2. https://doi.org/10.1177/2047487320915662
12. NHS England. NHS England commissioning standards for cardiovascular rehabilitation. Available from: https://www.england.nhs.uk/long-read/commissioning-standards-for-cardiovascular-rehabilitation/
13. Sabouret P, Lemesle G, Bellemain-Appaix A et al. Post-discharge and long-term follow-up after an acute coronary syndrome: International Collaborative Group of CNCF position paper. Arch Med Sci 2022;18:839–54. https://doi.org/10.5114/aoms/150321
14. Jackson AC, Grande MRL, Rogerson MC et al. The cardiac distress inventory: a new measure of psychosocial distress associated with an acute cardiac event. BMC Cardiovasc Dis 2022;22:460. https://doi.org/10.1186/s12872-022-02897-y
15. Randall G, Molloy GJ, Steptoe A. The impact of an acute cardiac event on the partners of patients: a systematic review. Health Psych Rev 2009;3:1–84. https://doi.org/10.3389/fpsyg.2017.01265
16. McCormack T, Mills J. The post-ACS patient: shared care to improve outcomes. Br J Cardiol 2017;24(supplement 1):S16–20. https://doi.org/10.5837/bjc.2017.s03
17. Lu M, Tang J, Wu J, Yang J, Yu J. Discharge planning for acute coronary syndrome patients in a tertiary hospital: a best practice implementation project. JBI Database System Rev Implement Rep 2015;13:318–34. https://doi.org/10.11124/jbisrir-2015-2078
18. Royal College of General Practitioners. Best Practice Guideline: Discharge to general practice. 2022. Available from: https://rcem.ac.uk/wp-content/uploads/2022/10/Discharge_to_General_Practice_Updated_Oct22.pdf (Accessed August 2025)
19. Nie W. Exploring the role of advanced clinical practitioners in the UK. Int J Adv Pract 2025;3:21–5. https://doi.org/10.12968/ijap.2024.0004
20. Conway B. The role of independent nurse prescribers in a cardiac rehabilitation service. Br J Cardiac Nurs 2011;6:406–7. https://doi.org/10.12968/bjca.2011.6.8.406
21. Byrne RA, Rossello X, Coughlan JJ et al. 2023 ESC Guidelines for the management of of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J 2023;44:3720–826. https://doi.org/10.1093/eurheartj/ehad191
22. British Association of Cardiac Prevention and Rehabilitation (BACPR). BACPR Guidance: Minimum criteria for discharge summaries. Available from: https://bacpr.org/resources/publications

All rights reserved. No part of this programme may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publishers, Medinews (Cardiology) Limited.
It shall not, by way of trade or otherwise, be lent, re-sold, hired or otherwise circulated without the publisher’s prior consent.
Medical knowledge is constantly changing. As new information becomes available, changes in treatment, procedures, equipment and the use of drugs becomes necessary. The editors/authors/contributors and the publishers have taken care to ensure that the information given in this text is accurate and up to date. Readers are strongly advised to confirm that the information, especially with regard to drug usage, complies with the latest legislation and standards of practice.
Healthcare professionals should consult up-to-date Prescribing Information and the full Summary of Product Characteristics available from the manufacturers before prescribing any product. Medinews (Cardiology) Limited cannot accept responsibility for any errors in prescribing which may occur.