Habitual physical activity improves cardiovascular health but there is a higher risk of atrial fibrillation (AF) in endurance athletes. The physiological processes underlying this observation are not fully understood, but adaptations to exercise, such as bradycardia and atrial dilatation, may contribute to arrhythmia susceptibility. Further data on long-term implications and individualised management strategies in athletes with AF are required.
Introduction
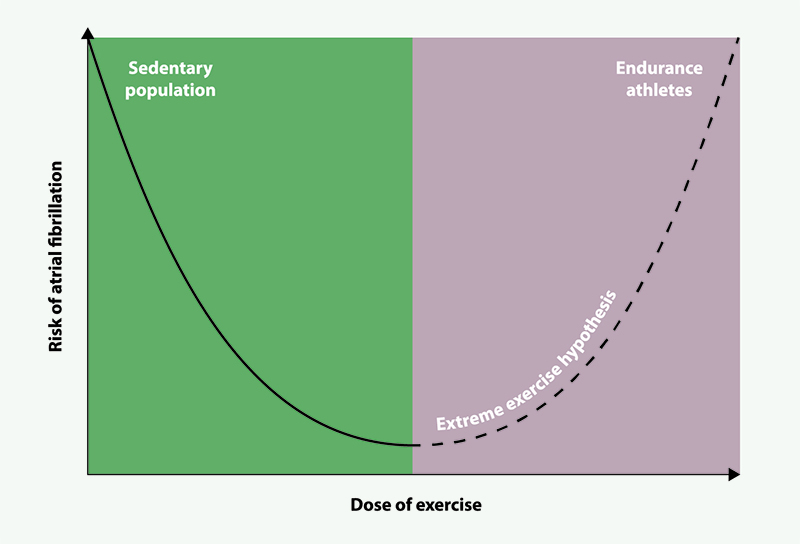
Atrial fibrillation (AF) is the most common cardiac arrhythmia with an estimated prevalence in the UK of 3%.1 Epidemiological studies have shown a 12–20% reduction in the risk of AF in individuals who engage in guideline-recommended physical activity levels.2,3 However, the reduction in AF risk appears to diminish with increasing doses of exercise, with contemporary data proposing a paradoxical rise in the risk of AF with the highest doses of exercise; suggesting a U-shaped dose-response relationship (figure 1).4
Andersen et al. were the first to robustly show that competitive endurance exercise paradoxically increases the risk of AF. In 52,000 cross-country skiers, athletes with the fastest finishing times (hazard ratio [HR] 1.30, 95% confidence interval [CI] 1.04 to 1.62) and the most number of races completed (HR 1.30, 95%CI 1.08 to 1.58) had the highest relative risk of developing AF.5 These observations are supported by a meta-analysis of 13 studies with 6,816 athletes and 63,662 controls, which found endurance athletes to have a two-fold risk of AF.6
Mechanisms of AF in endurance athletes
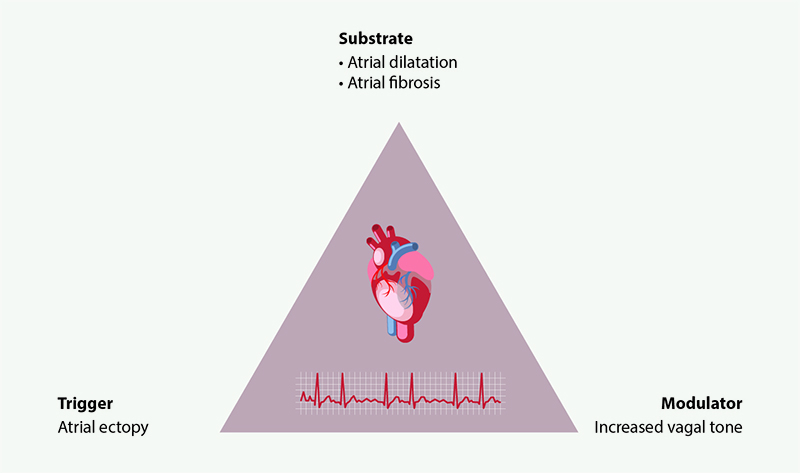
There are no unanimously accepted mechanisms to explain the observed risk of AF in endurance athletes. However, cardiovascular adaptations to endurance exercise are well described, and many of these are associated with arrhythmogenic potential. These can be described in the context of Coumel’s triangle of arrhythmogenesis, which describes three critical pathophysiological processes that generate arrhythmias: a substrate, modulator, and trigger (figure 2).7
Exercise induces autonomic modulation
Endurance exercise is commonly observed to result in a lower resting heart rate, which is thought to be a surrogate measure of parasympathetic cardiac tone exerted by the vagus nerve. High vagal tone slows heart rate through the sinoatrial node and slows the conduction through the atrioventricular (AV) node, leading to longer PR intervals on an electrocardiogram (ECG), which has been associated with individuals with higher aerobic fitness,8 and shortening of the atrial refractory period (the period of repolarisation and non-excitability after an impulse). It has been shown that increased vagal tone can lead to enhanced AF inducibility. In a rodent model, exercised rats displayed increased parasympathetic tone (measured by heart rate changes after pharmacological blockage) after 16 weeks of treadmill training. The right atrial refractory period was shortened to 34.4 ± 0.7 ms in exercised rats compared with 37.0 ± 0.9 ms in sedentary rats.9 Furthermore, a porcine model found larger atrial surface area and shorter effective refractory period were associated with an increase in sustained AF.10
AF vulnerability can also be enhanced in periods of higher vagal tone. A study of 15 AF patients found that 74% of atrial tachyarrhythmias occurred between 8pm and 8am.11 During slow-wave sleep, the body enters high vagal nerve activity, which may shorten the atrial refractory period, allowing atrial cells to be triggered more frequently, which may facilitate AF.12
Atrial ectopy triggers in endurance athletes
The triggering event in exercise-induced AF is unclear, however, as atrial ectopy is thought to increase following physical activity in the general population, it has been proposed as a possible triggering event in exercise-induced AF. In a study of 60 runners, those with higher lifetime training hours (>4,500 hours) had an increased incidence of premature atrial contractions, along with increased parasympathetic tone and left atrial (LA) volume.13 However, a study of 134 endurance athletes with equal age and sex-matched controls found no difference in the burden of premature atrial beats between groups.14 Further research evaluating potential AF-triggering events in this population is needed.
The athlete’s heart as a substrate for arrhythmogenesis
Exercise-induced cardiac remodelling is a compensatory response to the haemodynamic demands associated with exercise. Typical adaptations include a proportional increase in cardiac volumes in all four chambers with a limited change in mass, described as the athlete’s heart phenotype.15 LA remodelling is of particular interest in the pathogenesis of exercise-induced AF. Due to their thin walls and elliptical shape, the atria are more susceptible to sheer wall stress and wall stretch, which may elicit a stronger signal for adaptive remodelling when compared with the ventricles. Furthermore, there is a decrease in diastolic time during exercise, which increases the relative time in which the mitral valve remains closed.16 The back pressure in the atria as a result of the closed mitral valve may contribute to a longer time in relatively higher LA pressure.16 These processes during exercise may increase the susceptibility of the atria to wall stress, causing subsequent remodelling.
Atrial dilatation may have a critical role in the pathogenesis of exercise-induced AF. A meta-analysis of 54 studies found athletes have a 4.1 mm longer LA diameter and 7 ml/m2 larger LA volume compared with sedentary controls.17 Larger LA volumes are associated with a higher risk of AF in the general population.18 In the Framingham Heart Study, each 5 mm increase in LA size was associated with a further 39% increase in the risk of AF.19
The mechanisms that underlie LA dilatation may also trigger atrial fibrosis formation. Myocardial fibrosis is the replacement of healthy functioning myocardium with extracellular connective tissue. Both atrial and ventricular fibrosis have been associated with athletes. Mean LA fibrosis scores were higher in 20 endurance athletes (15.5 ± 5.9%) compared with 20 healthy controls (9.6 ± 4.9%).20 Another study in a cohort of triathletes found 17% to have cardiac fibrosis, with regression analysis showing that the completion of 1,880 km of cycling was a significant predictor for fibrosis.21 Rodent models have shown increased fibrosis in 16-week intensely trained rats compared with sedentary rats, which was associated with increased arrhythmia inducibility.22 Myocardial fibrosis has been implicated in arrhythmogenesis due to its poor capacity for electrophysiological conduction when compared with native cardiac tissue.23
Clinical implications
Cerebrovascular thromboembolic disease, namely stroke, is a major cause of morbidity in AF. Prophylactic anticoagulation is offered following the calculation of thromboembolic risk using clinical risk scores such as CHA2DS2-VASc.24 However, these scores have not been validated in athletes. In a survey of nearly 1,000 athletes, there was an increased risk of stroke even in athletes who had a CHA2DS2-VASc score of zero or one, implying athletes’ true risk of stroke is not fully captured.25 Athletes demonstrate LA dilatation, which is associated with a graded risk of stroke in the general population. Deranged flow in a dilated LA may be further augmented by bradycardia, which may predispose them to intracardiac blood stasis. Importantly, these phenotypes are not well captured in currently utilised risk scores such as CHA2DS2-VASc.
Occupational risks of trauma and major bleeding while taking anticoagulation medications may not reflect the risks of the general population, and the effects of living with AF in athletes are not well reported. A case report of a 75-year-old male cyclist with AF described the challenges of medical management. The individual could not be offered beta-blockers, a common treatment for AF, due to the athlete’s resting bradycardia and causing an unwanted reduction to their exercise capacity. Furthermore, anticoagulants were stopped due to their concern about crashing and bleeding.26 In a qualitative study of 10 athletes with AF, athletes described being told to cease sports participation or adapt to new training limits, which, for many of these individuals, would mean a significant reduction in their quality of life.27 The treatment goals in athletes should be managed on a case-to-case basis with individual risk-benefit options considered (table 1).
Table 1. Comparison of atrial fibrillation (AF) prognosis considerations between the general population and athletes
| General population | Athletes | |
| Rate/rhythm control | Beta-blockers to reduce heart rate | Unfavourable due to limiting exercise capacity and being bradycardic |
| Anticoagulants | Reduces stroke risk up to 80% | Avoided in impact sports due to the risk of bleeding from injuries |
| Detraining | Not applicable | Unfavourable due to the desire to maintain performance levels |
Conclusion
Exercise-induced AF is increasingly recognised. The mechanisms that underlie these observations are not fully understood. Stroke remains the most significant cause of morbidity in AF, and current risk scores may underestimate the risk of stroke in athletes. Future work should aim to provide more definitive evidence about the risk of AF and stroke in endurance athletes and offer more specific guidance for clinical teams caring for athletes with AF.
Key messages
- Guideline-recommended physical activity reduces the risk of atrial fibrillation (AF). However, this reduction appears to diminish with increasing doses of exercise, as seen in athletes
- Athletes often present with all three key pathophysiological processes of arrhythmogenic potential, promoting AF development
- Assessment of stroke risk using the CHA2DS2-VASc score may not fully capture the true risk of stroke in athletes with AF, highlighting a need for individualised treatment goals for athletes
Conflicts of interest
None declared.
Funding
CLD is funded through the British Heart Foundation (BHF) four-year PhD programme. AS is supported by an NIHR Advanced Fellowship (NIHR300867). GAN is supported by the BHF Research Excellence Award (RE/24/130031), BHF Programme Grant (RG/17/3/32774), Medical Research Council Biomedical Catalyst Developmental Pathway Funding Scheme (MR/S037306/1) and NIHR i4i grant (NIHR204553). GPM is supported by Leicester NIHR Biomedical Research Centre. SP is funded by the NIHR through the Academic Clinical Fellowship programme.
References
1. Adderley N, Ryan R, Nirantharakumar K, Marshall T. Prevalence and treatment of atrial fibrillation in UK general practice from 2000 to 2016. Heart 2019;105:27–33. https://doi.org/10.1136/heartjnl-2018-312977
2. de Keijzer AR, Kauling RM, Jørstad HT, Roos-Hesselink JW. Physical activity for cardiovascular prevention 2024. Council for Cardiology Practice. European Society of Cardiology, 2024. Available from: https://www.escardio.org/Councils/Council-for-Cardiology-Practice-(CCP)/Cardiopractice/physical-activity-for-cardiovascular-prevention
3. Jin M-N, Yang P-S, Song C et al. Physical activity and risk of atrial fibrillation: a nationwide cohort study in general population. Sci Rep 2019;9:13270. https://doi.org/10.1038/s41598-019-49686-w
4. Eijsvogels TMH, Thompson PD, Franklin BA. The “extreme exercise hypothesis”: recent findings and cardiovascular health implications. Curr Treat Options Cardiovasc Med 2018;20:84. https://doi.org/10.1007/s11936-018-0674-3
5. Andersen K, Farahmand B, Ahlbom A et al. Risk of arrhythmias in 52 755 long-distance cross-country skiers: a cohort study. Eur Heart J 2013;34:3624–31. https://doi.org/10.1093/eurheartj/eht188
6. Newman W, Parry-Williams G, Wiles J et al. Risk of atrial fibrillation in athletes: a systematic review and meta-analysis. Br J Sports Med 2021;55:1233–8. https://doi.org/10.1136/bjsports-2021-103994
7. Coumel P. Paroxysmal atrial fibrillation: a disorder of autonomic tone? Eur Heart J 1994;15(suppl A):9–16. https://doi.org/10.1093/eurheartj/15.suppl_A.9
8. Dorey TW, O’Brien MW, Kimmerly DS. The influence of aerobic fitness on electrocardiographic and heart rate variability parameters in young and older adults. Auton Neurosci 2019;217:66–70. https://doi.org/10.1016/j.autneu.2019.01.004
9. Guasch E, Benito B, Qi X et al. Atrial fibrillation promotion by endurance exercise: demonstration and mechanistic exploration in an animal model. J Am Coll Cardiol 2013;62:68–77. https://doi.org/10.1016/j.jacc.2013.01.091
10. Lee AM, Aziz A, Didesch J, Clark KL, Schuessler RB, Damiano RJ. Importance of atrial surface area and refractory period in sustaining atrial fibrillation: testing the critical mass hypothesis. J Thorac Cardiovasc Surg 2013;146:593–8. https://doi.org/10.1016/j.jtcvs.2012.04.021
11. Mitchell ARJ, Spurrell PAR, Sulke N. Circadian variation of arrhythmia onset patterns in patients with persistent atrial fibrillation. Am Heart J 2003;146:902–07. https://doi.org/10.1016/S0002-8703(03)00405-8
12. Verrier RL, Josephson ME. Impact of sleep on arrhythmogenesis. Circ Arrhythm Electrophysiol 2009;2:450–9. https://doi.org/10.1161/CIRCEP.109.867028
13. Wilhelm M, Roten L, Tanner H, Wilhelm I, Schmid J-P, Saner H. Atrial remodeling, autonomic tone, and lifetime training hours in nonelite athletes. Am J Cardiol 2011;108:580–5. https://doi.org/10.1016/j.amjcard.2011.03.086
14. Cipriani A, Vio R, Mastella G et al. Burden of premature atrial beats in middle-aged endurance athletes with and without lone atrial fibrillation versus sedentary controls. Eur J Prev Cardiol 2019;27:1555–63. https://doi.org/10.1177/2047487319880042
15. Prior DL, La Gerche A. The athlete’s heart. Heart 2012;98:947–55. https://doi.org/10.1136/heartjnl-2011-301329
16. La Gerche A, Claessen G. Increased flow, dam walls, and upstream pressure: the physiological challenges and atrial consequences of intense exercise. JACC Cardiovasc Imaging 2016;9:1389–91. https://doi.org/10.1016/j.jcmg.2016.06.008
17. Iskandar A, Mujtaba MT, Thompson PD. Left atrium size in elite athletes. JACC Cardiovasc Imaging 2015;8:753–62. https://doi.org/10.1016/j.jcmg.2014.12.032
18. Habibi M, Samiei S, Ambale Venkatesh B et al. Cardiac magnetic resonance-measured left atrial volume and function and incident atrial fibrillation: results from MESA (Multi-Ethnic Study of Atherosclerosis). Circ Cardiovasc Imaging 2016;9:e004299. https://doi.org/10.1161/CIRCIMAGING.115.004299
19. Vaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. Circulation 1994;89:724–30. https://doi.org/10.1161/01.CIR.89.2.724
20. Peritz DC, Catino AB, Csecs I et al. High-intensity endurance training is associated with left atrial fibrosis. Am Heart J 2020;226:206–13. https://doi.org/10.1016/j.ahj.2020.05.015
21. Tahir E, Starekova J, Muellerleile K et al. Myocardial fibrosis in competitive triathletes detected by contrast-enhanced CMR correlates with exercise-induced hypertension and competition history. JACC Cardiovasc Imaging 2018;11:1260–70. https://doi.org/10.1016/j.jcmg.2017.09.016
22. Benito B, Gay-Jordi G, Serrano-Mollar A et al. Cardiac arrhythmogenic remodeling in a rat model of long-term intensive exercise training. Circulation 2011;123:13–22. https://doi.org/10.1161/CIRCULATIONAHA.110.938282
23. Platonov PG. Atrial fibrosis: an obligatory component of arrhythmia mechanisms in atrial fibrillation? J Geriatr Cardiol 2017;14:233–7. https://doi.org/10.11909/j.issn.1671-5411.2017.04.008
24. Camm AJ, Lip GY, De Caterina R et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012;33:2719–47. https://doi.org/10.1093/eurheartj/ehs253
25. Pallikadavath S, Richards C, Bountziouka V et al. The AFLETES study: atrial fibrillation in veteran athletes and the risk of stroke. Clin J Sport Med 2023;33:209–16. https://doi.org/10.1097/JSM.0000000000001115
26. Patel R, Pallikadavath S, Graham-Brown MPM, Singh A. Shared decision making in athletes with cardiovascular disease: what we can learn from a masters athlete. BMJ Case Rep 2021;14:e245822. https://doi.org/10.1136/bcr-2021-245822
27. Galloway CSL, Simonetto D, Shave R et al. The experiences of endurance athletes with atrial fibrillation: tensions and takeaways. Heart Lung Circ 2023;32:1207–14. https://doi.org/10.1016/j.hlc.2023.08.009
