Sudden cardiac death (SCD) is a devastating and tragic occurrence that may affect individuals of all ages. It is defined as an unexpected death occurring within one hour of the onset of symptoms, if witnessed, or within 24 hours of last being seen alive and well, if unwitnessed. Athletes are considered to be the healthiest of all the population, and exercise is known to reduce the risk of atherosclerotic coronary artery disease. However, both amateur and highly trained athletes do die suddenly and unexpectedly, and this gets widespread media attention as it is so shocking and unexpected. This brings SCD, its frequency and causes into the spotlight. This review focuses on the epidemiology and aetiology of SCD in athletes from a pathological perspective.

Epidemiology
The incidence of sudden cardiac death (SCD) in athletes varies widely between studies, ranging between 0.24 and 6.8 per 100,000 person-years.1,2 This is partially explained by the differences in the populations studied, differences in the definition of an athlete, and the inclusion of sudden cardiac arrest into studies.
Age has been shown to be an important determinant of risk, with a nationwide Danish study showing that those aged 12 to 35 years were at a lower risk (0.43 to 2.95 per 100,000 person-years) compared with those aged 36 to 49 years (0.47 to 6.64 per 100,000 person-years).3 Interestingly, this study also showed that the risk of SCD is higher in the general population at 10.7 per 100,000 person-years, highlighting that most SCD in the young occurs in non-athletes.
It is well recognised that SCD occurs at a higher frequency in males, with a ratio of around 2:1 when compared with females.4 In athletes this is further exaggerated, with a similar study reporting a ratio of over 12:1.5 When female athletes are compared with males they are more likely to die at rest, as opposed to during exertion.6
In the US, black athletes have a higher risk of SCD than white athletes, with a reported incidence of 5.65 per 100,000 person-years compared with 3.02 per 100,000 person-years, respectively.7 Similarly, in a prospective cohort of elite adolescent soccer players in the UK, the risk of SCD was approximately seven times higher in black (25 per 100,000 person-years) compared with white (3.86 per 100,000 person-years) athletes.1
Type of sport has also been shown to have an effect, with ice hockey (4.25 per 100,000 person-years), basketball (2.51 per 100,000 person-years) and American football (1.21 per 100,000 person-years) having the greatest risks of SCD.8 In a UK cohort of 357 SCDs occurring in athletes, the most common sports disciplines were running (25%), football (25%), cycling (8%) and gymnastics (8%).5
Aetiology
SCD in athletes is caused by a wide variety of cardiac disease. While ischaemic heart disease (IHD) is common in older athletes, in younger athletes, genetic conditions, such as cardiomyopathy and channelopathy, are more common. It is important to eliminate causes such as hyperthermia, as this is one of the most common causes of sudden death in athletes. This is defined by a body temperature of over 40 °C.9 Hypothermia, with a body temperature of less than 32 °C, may also cause cardiac arrest, particularly in athletes exercising in cold weather or water.10 Both these conditions are usually identified by the first responders to cardiac arrest.
Role of the autopsy
Autopsy is the gold standard for identifying the cause of death.11 SCD is often the first manifestation of disease, and autopsy is the only opportunity to establish an accurate cause of death in the athlete. It is concerning that, in a recent worldwide International Federation of Association Football (FIFA) report into sudden death in young footballers, only 20% had an autopsy.12 A European survey has highlighted that up to 40% of SCD in those under 50 years did not have an autopsy.13 A full autopsy with detailed pathological examination of the heart should be undertaken in all young SCD to establish an accurate cause of death because of the implications of a diagnosis of a hereditary cardiac condition for blood relatives.14 Also, not all sudden deaths are due to cardiac causes, with 20–40% being unnatural or non-cardiac in origin after autopsy.15,16
The UK Royal College of Pathologists, and the Association for European Cardiovascular Pathology have published recommended guidelines for autopsy investigation of SCD cases.13,17,18 The Association for European Cardiovascular Pathology has also recently issued guidelines for diagnosis of genetic cardiomyopathies at autopsy.19 Blood for toxicology is essential,20 and fresh blood/spleen should routinely be saved for genetic testing, if deemed necessary, and the examinations may also include biochemistry and microbiology in selected cases.17
We know from previous studies that expert cardiac pathology evaluation is essential, as this significantly improves the post-mortem diagnostic accuracy.14,21 A UK study found that the initial diagnosis of cause of SCD, made by the referring pathologist, was altered after expert evaluation in 41% of cases.14 For arrhythmogenic cardiomyopathy, only two out of 20 were confirmed by the expert cardiac pathologist.14
Sudden arrhythmic death syndrome
Sudden arrhythmic death syndrome (SADS) is the term used in the post-mortem setting to describe an individual who has died suddenly and unexpectedly, where no cause of death is found at autopsy or on toxicology, and detailed histology of the heart shows it to be morphologically normal. This is the so-called negative autopsy. This is the most common cause of SCD in European athletes, and accounts for between 20% and 40% in this population.5,22 When this diagnosis is made, the family must be screened for underlying channelopathies, a group of disorders affecting the ion channels of the heart, which include long-QT syndrome (LQTS), short-QT syndrome, Brugada and catecholaminergic polymorphic ventricular tachycardia (CPVT), conduction disease and idiopathic ventricular fibrillation. The main role of the autopsy is to establish that the heart is normal, and that minor abnormalities or mild coronary artery disease are not erroneously considered the cause of death.21 Toxicology should always be done in all cases, as we have shown that it can be positive in 10% of potential SADS cases.20
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is cardiologically defined as a left ventricular wall thickness of 15 mm or more in any myocardial segment that is not explained solely by loading conditions. The disease is estimated to have a prevalence of one in 500 in the general population.23 HCM is reported to cause between 2% and 36% of SCD in athletes,5,16,24 and is reported as the most common cause of SCD in athletes in the US, making up 36%.16 Contrastingly, in the UK, HCM causes 6% of SCDs.5 Most HCM patients die suddenly at rest, rather than on exertion.25,26 The differences in the proportion of SCD caused by HCM in all these studies may be explained by how the diagnosis is made.4 At autopsy, on macroscopic examination there is frequently increased heart weight with asymmetric left ventricular hypertrophy27 (figure 1A) and normal coronary arteries. It is important to state that the heart can appear normal in 30% of cases, so pathologists need to be aware that histology should be taken on all normal hearts in individuals with SCD.25
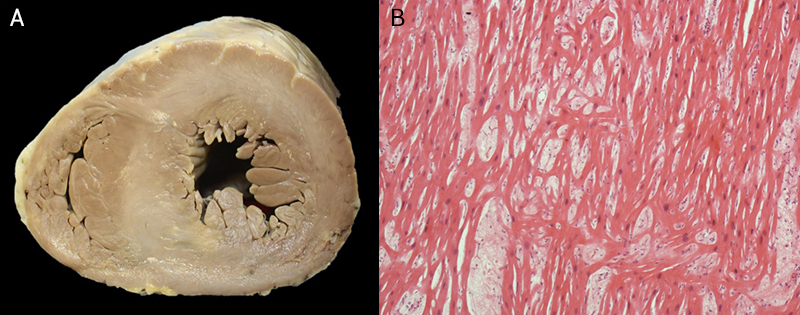
The diagnosis is made histologically with the detection of widespread myocyte disarray in the left ventricle (figure 1B). Pathologists need to be strict in their definition of myocyte disarray and guidelines should be carefully followed.19 There is a genetic cause in up to 70% of cases. Once the diagnosis is made, then the pathologist informs the medical examiner and coroner who will inform the family that they need cardiological screening in view of the SCD. Sudden death is the first presentation with the diagnosis made at autopsy in 79% of cases in our HCM series, emphasising the role of the autopsy and pathologist.25,28
Arrhythmogenic cardiomyopathy
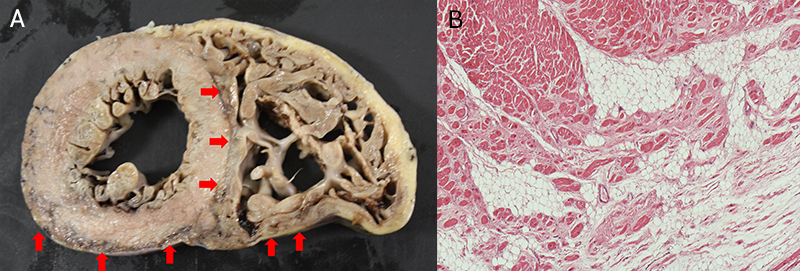
Arrhythmogenic cardiomyopathy (ACM) is a mainly inherited cardiac disease characterised by progressive replacement of the myocardium by fibrofatty tissue, with a subepicardial distribution in both ventricles. This can lead to cardiac arrhythmia, ventricular dysfunction, and SCD.29 ACM has an estimated prevalence of one in 1,000 to one in 5,000,30,31 and the genes underlying arrhythmogenic right ventricular cardiomyopathy (ARVC) mainly encode proteins of the cardiac desmosome.32 Originally denoted as ARVC, it is now recognised to affect both ventricles, with a recent study showing left ventricular (LV) involvement in 87% of cases.29 ACM is emerging as one of the most common causes of death in athletes, ranging from 4% to 22% in SCD studies.5,16,33 SCD with ACM is frequently associated with exertion. At autopsy, the diagnosis is made based upon both the macroscopic and microscopic findings in the heart. Macroscopically, there can be fat and fibrous tissue in a subepicardial distribution in both ventricles in the absence of significant coronary artery disease (figure 2A). Again, as in HCM, the heart can look macroscopically normal. Microscopically, fibrous tissue and fat replace the myocardium (figure 2B).29 There are mimics of ACM, such as cardiac sarcoid,34 so again, histology is essential in all cases for correct diagnosis.
Dilated cardiomyopathy
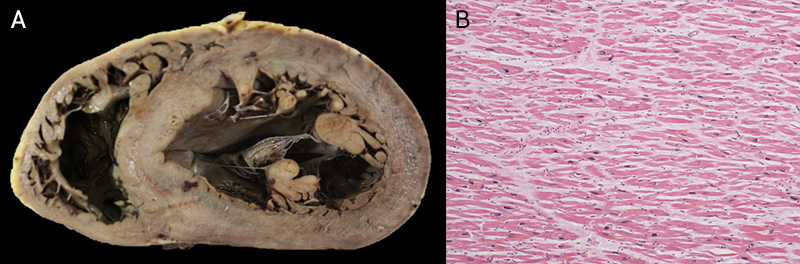
Dilated cardiomyopathy (DCM) is cardiologically defined by the presence of LV dilatation and contractile dysfunction not explained by coronary artery disease or abnormal loading conditions.35 There are several genes that are causative of DCM, which encode structural components of the sarcomere and desmosome. Some are associated with a higher risk of SCD, such as FLNC, DES, DSP, PLN, LMNA, TMEM43 or RMB20.23 Other causes include myocarditis, exposure to drugs, toxins or allergens, endocrine or autoimmune disease. DCM is a rarer cause of SCD in athletes, occurring in just 1–3%.5,7,16 Classically, on pathological examination, the heart shows enlargement, increased weight, dilation of the left ventricle with wall thinning and mural thrombi in atria and ventricles with dilated valve annulus (figure 3A). Histology usually shows interstitial and replacement fibrosis, but this may be absent (figure 3B).
Idiopathic left ventricular hypertrophy
Idiopathic left ventricular hypertrophy (ILVH) is an emerging entity that accounts for 16–17% of SCD in athletes, and in more recent studies, is the predominant cardiomyopathy.5,22 It is defined by an increased heart weight in the absence of significant coronary artery disease, valvular disease, other cardiomyopathy, hypertension, obesity, alcohol misuse and diabetes. It is histologically distinct from HCM by the absence of myocyte disarray on histology.4 A recent study on decedents with ILVH, utilising post-mortem genetic testing and comprehensive screening of direct blood relatives, found that there were no variants associated with HCM and no evidence of HCM in relatives. This suggests that ILVH is an entity that is distinct from HCM.36 Further evaluation of families and genetic testing will clarify this entity and its causes.
Idiopathic left ventricular fibrosis
Left ventricular fibrosis is usually explained by coronary artery disease, toxic causes such as alcohol, or cardiomyopathy. In a small proportion it remains unexplained and does not reach the criteria for a diagnosis of dilated, arrhythmogenic or hypertrophic cardiomyopathy. These are labelled as idiopathic left ventricular fibrosis (ILVF), which is another emerging entity. In studies where it is diagnosed, it accounts for up to 8% of SCD in athletes.5 Recent studies of decedents with ILVF have shown that variants associated with cardiomyopathy, but also channelopathy, may be found in these individuals,37,38 replicating what has been found on cardiological screening of blood relatives.21
Ischaemic heart disease
Ischaemic heart disease (IHD) is the world’s biggest killer and, despite exercise being protective against coronary artery atheroma, it is still a well-recognised cause of SCD in mainly older athletes. A nationwide Danish study of individuals aged 12–49 years reported that IHD was the most common cause of SCD, accounting for 43%.3 In younger individuals, such as US athletes at collegiate level with an average age of 19 years, IHD accounts for a much lower proportion of SCD (6%),22 and in our study, 2% in a mainly younger cohort.5 We have reported on premature atheroma in younger patients, the youngest being 11 years old.39 Findings at post-mortem include significant atheromatous narrowing of the coronary arteries, atheromatous plaque rupture and thrombosis, acute infarction of the myocardium and myocardial fibrosis. Blood relatives should be screened for familial hypercholesterolaemia when IHD occurs in young athletes.
Myocarditis
 |
 |
 |
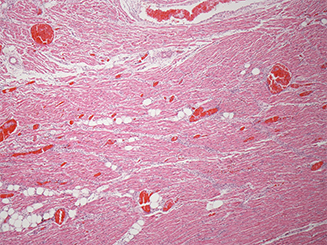
Myocarditis is histologically defined as an inflammatory infiltrate associated with myocyte necrosis not caused by ischaemia.40 The process is generally diffuse with widespread involvement of the myocardium in both left and right ventricles. Originally thought to be induced by viruses, bacteria, protozoa and fungi, as well as a variety of toxic substances and drugs and systemic immune-mediated diseases, it is now recognised that a myocarditis picture may be seen in inherited cardiomyopathy.41 Myocarditis is reported to be the cause of 2–7% of SCD in athletes.3,5,22 At autopsy, the heart may appear normal macroscopically or have dilated ventricles with colour variegation of the myocardium. Histologically, there must be myocyte necrosis with an associated inflammatory infiltrate, which can be subcategorised as lymphohistiocytic (56%), neutrophilic (17%), eosinophilic (16%), toxic (7%) or giant cell (4%) (figure 4).42
Coronary artery anomalies
Anomalous coronary arteries are a rare cause of SCD in athletes, accounting for 3–9%, and frequently occurring with exertion and first presenting at post-mortem.3,5,22 The left or right coronary artery arises in the wrong sinus (figure 5). The course is considered to be malignant when it passes within the aortic wall and between the pulmonary trunk and the aorta, which can cause compression of the proximal coronary artery resulting in ischaemia and SCD.43
Mitral valve prolapse
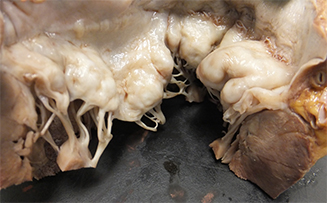
Mitral valve prolapse (MVP) has been reported as the cause of SCD in 2% of athletes.5,22 The condition affects both males and females equally. In a cohort of 120 cases of MVP identified following SCD, 11 (9%) died associated with exertion.44 Both valve leaflets show ballooning, thickening, elongation and annular disjunction at autopsy, with or without ventricular scarring (figure 6).
Commotio cordis
This is a rare cause of SCD in athletes, generally occurring in younger individuals because of the pliability of the chest wall.45 It is due to the impact of an object, usually a baseball or football, into the chest over the left intercostal space with immediate collapse and death. It is believed to occur in a vulnerable time in the cardiac cycle leading to cardiac arrest.46 The heart is normal at post-mortem, but there may be evidence of impact on the skin. The diagnosis is reliant on the circumstances of being hit in the chest shortly prior to SCD.45
Contusio cordis
Contusio cordis is a similar entity to commotio cordis, but is distinguished as the blow to the chest results in structural cardiac injury.47 There may simply be contusion of myocardial muscle, but there can be more severe injuries, such as rupture of a cardiac chamber, or disruption of a heart valve. Contusion may cause ventricular arrhythmia or conduction abnormalities resulting in SCD. Ventricular rupture can be rapidly fatal, and tamponade may occur. When rupture is through the septum, this leads to shunting with right ventricular hypertrophy, heart failure and death.
Conclusion
The incidence of SCD in athletes varies widely between studies, ranging between 0.24 and 6.8 per 100,000 person-years. It has diverse causes and is potentially heritable in over 75% of cases. Autopsy and thorough histopathological cardiac evaluation are essential to determine the causes of SCD.
Key messages
- The incidence of sudden cardiac death (SCD) in athletes is between 0.24 and 6.8 per 100,000 person-years
- SCD in athletes has diverse aetiology and is caused by potentially heritable cardiac conditions in over 75%
- SCD is frequently the first presentation of cardiac disease in athletes
- Autopsy and thorough histopathological cardiac evaluation are essential to determine the causes of SCD
Conflicts of interest
None declared.
Funding
Cardiac Risk in the Young (CRY) fund the cardiovascular pathology laboratories. JW is funded by the National Institute for Health and Care Research.
Patient consent
Example images are provided from a large anonymised dataset.
References
1. Malhotra A, Dhutia H, Finocchiaro G et al. Outcomes of cardiac screening in adolescent soccer players. N Engl J Med 2018;379:524–34. https://doi.org/10.1056/NEJMoa1714719
2. Risgaard B, Winkel BG, Jabbari R et al. Burden of sudden cardiac death in persons aged 1 to 49 years nationwide study in Denmark. Circ Arrhythm Electrophysiol 2014;7:205–11. https://doi.org/10.1161/CIRCEP.113.001421
3. Risgaard B, Winkel BG, Jabbari R et al. Sports-related sudden cardiac death in a competitive and a noncompetitive athlete population aged 12 to 49 years: data from an unselected nationwide study in Denmark. Heart Rhythm 2014;11:1673–81. https://doi.org/10.1016/j.hrthm.2014.05.026
4. Sheppard MN, Westaby J, Zullo E, Fernandez BVE, Cox S, Cox A. Sudden arrhythmic death and cardiomyopathy are important causes of sudden cardiac death in the UK: results from a national coronial autopsy database. Histopathology 2023;82:1056–66. https://doi.org/10.1111/his.14889
5. Finocchiaro G, Papadakis M, Robertus JL et al. Etiology of sudden death in sports: insights from a United Kingdom regional registry. J Am Coll Cardiol 2016;67:2108–15. https://doi.org/10.1016/j.jacc.2016.02.062
6. Finocchiaro G, Westaby J, Bhatia R et al. Sudden death in female athletes: insights from a large regional registry in the United Kingdom. Circulation 2021;144:1827–9. https://doi.org/10.1161/CIRCULATIONAHA.121.055535
7. Harmon KG, Asif IM, Maleszewski JJ et al. Incidence, cause, and comparative frequency of sudden cardiac death in National Collegiate Athletic Association athletes: a decade in review. Circulation 2015;132:10–19. https://doi.org/10.1161/CIRCULATIONAHA.115.015431
8. Peterson DF, Kucera K, Thomas LC et al. Aetiology and incidence of sudden cardiac arrest and death in young competitive athletes in the USA: a 4-year prospective study. Br J Sports Med 2021;55:1196–203. https://doi.org/10.1136/bjsports-2020-102666
9. Roberts WO, Armstrong LE, Sawka MN, Yeargin SW, Heled Y, O’Connor FG. ACSM expert consensus statement on exertional heat illness: recognition, management, and return to activity. Curr Sports Med Rep 2021;20:470–84. https://doi.org/10.1249/JSR.0000000000000878
10. Fudge J. Exercise in the cold: preventing and managing hypothermia and frostbite injury. Sports Health 2016;8:133. https://doi.org/10.1177/1941738116630542
11. Paratz ED, Rowe SJ, Stub D, Pflaumer A, La Gerche A. A systematic review of global autopsy rates in all-cause mortality and young sudden death. Heart Rhythm 2023;20:607–13. https://doi.org/10.1016/j.hrthm.2023.01.008
12. Egger F, Scharhag J, Kästner A, Dvořak J, Bohm P, Meyer T. FIFA sudden death registry (FIFA-SDR): a prospective, observational study of sudden death in worldwide football from 2014 to 2018. Br J Sports Med 2022;56:80–7. https://doi.org/10.1136/bjsports-2020-102368
13. Banner J, Basso C, Tolkien Z, Kholova I, Michaud K, Gallagher PJ. Autopsy examination in sudden cardiac death: a current perspective on behalf of the Association for European Cardiovascular Pathology. Virchows Arch 2021;478:687–93. https://doi.org/10.1007/s00428-020-02949-8
14. de Noronha SV, Behr ER, Papadakis M et al. The importance of specialist cardiac histopathological examination in the investigation of young sudden cardiac deaths. Europace 2014;16:899–907. https://doi.org/10.1093/europace/eut329
15. Risgaard B, Lynge TH, Wissenberg M et al. Risk factors and causes of sudden noncardiac death: a nationwide cohort study in Denmark. Heart Rhythm 2015;12:968–74. https://doi.org/10.1016/j.hrthm.2015.01.024
16. Maron BJ, Haas TS, Ahluwalia A, Murphy CJ, Garberich RF. Demographics and epidemiology of sudden deaths in young competitive athletes: from the United States national registry. Am J Med 2016;129:1170–7. https://doi.org/10.1016/j.amjmed.2016.02.031
17. Basso C, Aguilera B, Banner J et al. Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows Archiv 2017;471:691–705. https://doi.org/10.1007/s00428-017-2221-0
18. Sheppard MN, Suvarna K. Guidelines on autopsy practice: sudden death with likely cardiac pathology. London: Royal College of Pathologists, 2022. Available from: https://www.rcpath.org/static/823dfcf4-8eba-40f7-81b7e174675ecdd9/482ebe54-91c8-4961-bff76b1c01f642cc/Guidelines-on-autopsy-practice-Sudden-death-with-likely-cardiac-pathology.pdf
19. Sheppard MN, van der Wal AC, Banner J et al. Genetically determined cardiomyopathies at autopsy: the pivotal role of the pathologist in establishing the diagnosis and guiding family screening. Virchows Archiv 2023;482:653–69. https://doi.org/10.1007/s00428-023-03523-8
20. Radaelli D, Westaby J, Finocchiaro G, Sinagra G, D’Errico S, Sheppard MN. Sudden cardiac death with morphologically normal heart: always do toxicology. J Clin Pathol 2024;77:645–6. https://doi.org/10.1136/jcp-2023-209351
21. Papadakis M, Raju H, Behr ER et al. Sudden cardiac death with autopsy findings of uncertain significance: potential for erroneous interpretation. Circ Arrhythm Electrophysiol 2013;6:588–96. https://doi.org/10.1161/CIRCEP.113.000111
22. Petek BJ, Churchill TW, Moulson N et al. Sudden cardiac death in National Collegiate Athletic Association athletes: a 20-year study. Circulation 2024;149:80–90. https://doi.org/10.1161/CIRCULATIONAHA.123.065908
23. Arbelo E, Protonotarios A, Gimeno JR et al. 2023 ESC guidelines for the management of cardiomyopathies: developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur Heart J 2023;44:3503–626. https://doi.org/10.1093/eurheartj/ehad194
24. Corrado D, Basso C, Rizzoli G, Schiavon M, Thiene G. Does sports activity enhance the risk of sudden death in adolescents and young adults? J Am Coll Cardiol 2003;42:1959–63. https://doi.org/10.1016/j.jacc.2003.03.002
25. Finocchiaro G, Papadakis M, Tanzarella G et al. Sudden death can be the first manifestation of hypertrophic cardiomyopathy: data from a United Kingdom pathology registry. JACC Clin Electrophysiol 2019;5:252–4. https://doi.org/10.1016/j.jacep.2018.11.004
26. Maron BJ, Mackey-Bojack S, Facile E, Duncanson E, Rowin EJ, Maron MS. Hypertrophic cardiomyopathy and sudden death initially identified at autopsy. Am J Cardiol 2020;127:139–41. https://doi.org/10.1016/j.amjcard.2020.04.021
27. Finocchiaro G, Sheikh N, Leone O et al. Arrhythmogenic potential of myocardial disarray in hypertrophic cardiomyopathy: genetic basis, functional consequences and relation to sudden cardiac death. Europace 2021;23:985–95. https://doi.org/10.1093/europace/euaa348
28. Finocchiaro G, Bhatia RT, Westaby J et al. Sudden cardiac death during exercise in young individuals with hypertrophic cardiomyopathy. JACC Clin Electrophysiol 2023;9:865–7. https://doi.org/10.1016/j.jacep.2022.12.007
29. Miles C, Finocchiaro G, Papadakis M et al. Sudden death and left ventricular involvement in arrhythmogenic cardiomyopathy. Circulation 2019;139:1786–97. https://doi.org/10.1161/CIRCULATIONAHA.118.037230
30. Corrado D, Basso C, Judge DP. Arrhythmogenic cardiomyopathy. Circ Res 2017;121:784–802. https://doi.org/10.1161/CIRCRESAHA.117.309345
31. McKenna WJ, Maron BJ, Thiene G. Classification, epidemiology, and global burden of cardiomyopathies. Circ Res 2017;121:722–30. https://doi.org/10.1161/CIRCRESAHA.117.309711
32. Gandjbakhch E, Redheuil A, Pousset F, Charron P, Frank R. Clinical diagnosis, imaging, and genetics of arrhythmogenic right ventricular cardiomyopathy/dysplasia: JACC state-of-the-art review. J Am Coll Cardiol 2018;72:784–804. https://doi.org/10.1016/j.jacc.2018.05.065
33. Corrado D, Basso C, Thiene G. Sudden cardiac death in young people with apparently normal heart. Cardiovasc Res 2001;50:399–408. https://doi.org/10.1016/S0008-6363(01)00254-1
34. Bagwan IN, Hooper LVB, Sheppard MN. Cardiac sarcoidosis and sudden death. The heart may look normal or mimic other cardiomyopathies. Virchows Arch 2011;458:671–8. https://doi.org/10.1007/s00428-010-1003-8
35. Weintraub RG, Semsarian C, Macdonald P. Dilated cardiomyopathy. Lancet 2017;390:400–14. https://doi.org/10.1016/S0140-6736(16)31713-5
36. Finocchiaro G, Dhutia H, Gray B et al. Diagnostic yield of hypertrophic cardiomyopathy in first-degree relatives of decedents with idiopathic left ventricular hypertrophy. Europace 2020;22:632–42. https://doi.org/10.1093/europace/euaa012
37. Lahrouchi N, Raju H, Lodder EM et al. The yield of postmortem genetic testing in sudden death cases with structural findings at autopsy. Eur J Hum Genet 2020;28:17–22. https://doi.org/10.1038/s41431-019-0500-8
38. Iglesias M, Ripoll-Vera T, Perez-Luengo C et al. Diagnostic yield of genetic testing in sudden cardiac death with autopsy findings of uncertain significance. J Clin Med 2021;10:1806. https://doi.org/10.3390/jcm10091806
39. Green AC, Sheppard MN. Sudden cardiac death associated with premature atheroma in the young: an autopsy study emphasising single-vessel lesions. Cardiol Young 2016;26:743–8. https://doi.org/10.1017/S1047951115001286
40. Aretz HT. Myocarditis: the Dallas criteria. Hum Pathol 1987;18:619–24. https://doi.org/10.1016/S0046-8177(87)80363-5
41. Monda E, Bakalakos A, Cannie D et al. Prevalence of pathogenic variants in cardiomyopathy-associated genes in acute myocarditis: a systematic review and meta-analysis. JACC Heart Fail 2024;12:1101–11. https://doi.org/10.1016/j.jchf.2024.02.012
42. Bhatia RT, Finocchiaro G, Westaby J et al. Myocarditis and sudden cardiac death in the community: clinical and pathological insights from a national registry in the United Kingdom. Circ Arrhythm Electrophysiol 2023;16:e012129. https://doi.org/10.1161/CIRCEP.123.012129
43. Finocchiaro G, Behr ER, Tanzarella G et al. Anomalous coronary artery origin and sudden cardiac death: clinical and pathological insights from a national pathology registry. JACC Clin Electrophysiol 2019;5:516–22. https://doi.org/10.1016/j.jacep.2018.11.015
44. Westaby J, Bicalho L, Zullo E, Sheppard MN. Insights into malignant mitral valve degenerative disease from a sudden cardiac death cohort highlighting significant measurement differences from normal. Histopathology 2024;84:960–6. https://doi.org/10.1111/his.15142
45. Cooper S, Woodford NW, Maron BJ, Harris KM, Sheppard MN. A lethal blow to the chest as an underdiagnosed cause of sudden death in United Kingdom sports (football, cricket, rugby). Am J Cardiol 2019;124:808–11. https://doi.org/10.1016/j.amjcard.2019.05.050
46. Maron BJ, Estes NAM 3rd. Commotio cordis. N Engl J Med 2010;362:917–27. https://doi.org/10.1056/NEJMra0910111
47. Farrokhian AR. Commotio cordis and contusio cordis: possible causes of trauma-related cardiac death. Arch Trauma Res 2016;5:e41482. https://doi.org/10.5812/atr.41482
