Historically, young people with genetic heart diseases were discouraged from active sport due to concerns about the increased risk of sudden cardiac death during competitive or intensive exercise. The shock resulting from the sudden death of a young athlete, an event often highly publicised, tends to generate concern in the general population, and fear of litigation in a low-evidence area: both influence decision-making by the medical profession when discussing ‘restrictions’, especially in patients with genetic heart diseases, who by definition, are at increased risk of sudden cardiac death. In recent years, however, we have moved to a point where many athletes with certain genetic heart diseases can, with optimal medical therapy, be considered for involvement in various sporting and athletic pursuits. We are cautiously moving away from the assumption that exercise is contraindicated; we are factoring in the wishes of the patient-athlete (shared decision-making), and we are encouraging optimal protection for these athletes during their sporting endeavours (easily available automated external defibrillators [AEDs], and club personnel trained in basic life support [BLS]), while ensuring regular medical assessment to identify alterations in risk status. With dedicated follow-up of all such patient-athletes, we can refine our understanding of how best to advise (and protect) them in terms of exercise for enhanced quality of life.

Sporting activities in those with ICDs
Lampert and colleagues reported a prospective multi-national registry looking at the safety of sports for athletes with implantable cardioverter-defibrillators (ICDs) in 2013.1 At the time of inception in 2006, the international (American Heart Association [AHA] and European Society of Cardiology [ESC]) recommendations were that billiards, bowling and golf were acceptable activities for such patient athletes. Concerns related to potential failure of the ICD to defibrillate due to metabolic, autonomic or potentially ischaemic changes during intense exercise, potential death or harm due to momentary loss of control from arrhythmia or ICD shock, and damage to the device or lead system. Patients aged 10–60 years with ICDs taking part in organised sports were enrolled in 41 US and 18 European sites. A total of 372 (328 organised sports; 44 high-risk sports) were enrolled (most common long QT syndrome [LQTS] n=73; hypertrophic cardiomyopathy [HCM] n=63; arrhythmogenic right ventricular cardiomyopathy [ARVC, ACM] n=55). Notably, enrolment did not imply endorsement of the participants’ sports participation. Median follow-up was 31 months for the group, during which there were no tachyarrhythmic deaths or externally resuscitated tachyarrhythmias: 13% received at least one appropriate shock, and 11% at least one inappropriate one. More received shocks during competition/practice or other physical activity than at rest, and those with ARVC or idiopathic ventricular fibrillation (VF) were more likely than those with HCM or LQTS to receive appropriate shocks during competition/practice. There were no injuries related to shocks reported. Very few of the participants were involved in aggressive contact sports (where injury or ICD system damage could be higher). The authors concluded that many athletes with ICDs can engage in vigorous competitive sports without physical injury or failure to terminate an arrhythmia.
The same group subsequently reported on long-term follow-up of the total group,2 again reporting no deaths, and in 2018, undertook a post-hoc analysis of outcomes in younger people (incorporated from age 10–21 years) in the registry,3 thus, allowing for more informed shared decision-making for children and adolescents with ICDs, and their families. The registry, which completed enrolment in 2015, had 129 participants of 21 years or younger. Most had LQTS (n=49), HCM (n=30) and congenital heart disease (n=15). There were 117 young athletes who played competitive sport, and 12 who played dangerous sports. Median follow-up was 42 months. Seven participants withdrew (two due to worsening conditions) and 11 (all confirmed alive) were lost to follow-up. There were no deaths, nor was there any severe injury resulting from syncope or shock during sports. The four individuals who had appropriate shocks during competition or practice were in the highly competitive subgroup. Notably, 105 athletes stopped participation in some or all sports during follow-up, predominantly (82%) for non-medical reasons (graduation from high or middle school), and seven because of an ICD shock (three stopped all sports). The authors discuss the huge benefits of sport in young people and note that all the subjects benefitted from sports participation during their entire length of school. Of the total shocks received in the group (49 shocks in 35 subjects – 60% appropriate) less than 25% occurred during sport. The issue of implanting an ICD in a young person primarily to allow competition is discussed, but, as with the authors, all consensus documents recommend against this practice, especially with the recognised significant risks to ICD implantation in the young.
Saarel et al. suggest that the topic of return to play in young people is even more complex because of the added interplay between patient-athletes and parents, their emotional connections, and often divergent perceived value of sport in life, and, the burden of sudden cardiac death (SCD) in the young being disproportionately larger, because of their greater life-expectancy, and the tragic effects on families.3
Tobert et al. looked at a 20-year experience of athletes (n=125, mean age 19.8 years) with genetic heart disease (44.8% LQTS, 17.6% HCM, 13.6% catecholaminergic polymorphic ventricular tachycardia [CPVT]) and an ICD, who were evaluated at the Mayo Clinic and were approved for return to play.4 Over a mean 3.6-year follow-up, no sports-associated deaths or reports of sports-related ICD damage occurred. As expected, athletes who received an ICD were more likely to have events during their return-to-play (RTP) period than those within the original group without an ICD, reflecting the appropriate risk stratification. An equal number of patients received a shock during sport and out of sport. This underscores the importance of good evaluation, good risk stratification, and optimal treatment before shared decision-making (and subsequent RTP). They again emphasise that an athlete’s desire to continue participation in competitive sports should not be the only qualifying factor for implanting an ICD, and that guideline-based genetic heart disease (GHD)-specific ICD indications should always be followed. Because of the findings, the authors conclude that “an athlete with genetic heart disease and an ICD should no longer be viewed as an oxymoron but a mutually possible coexistence”.
In a recent comprehensive review on sudden cardiac arrest in athletes by Lampert and Harmon in the New England Journal of Medicine,5 they discussed the type of ICD (transvenous versus subcutaneous) that might be inserted in athletes, and the specific issues to be considered (such as repetitive upper extremity motion or collision sports). They mention the extravascular ICD which may well prove attractive for use in some of these patients.
Discussion
The importance of exercise cannot be overstated. Those who exercise regularly live five to seven years longer than those leading a sedentary life.6 Regular physical activity results in up to a 50% reduction in adverse events from coronary artery disease in middle-aged and older individuals.7 Exercise confers several health benefits, ranging from a positive influence on weight to modifying blood pressure and cholesterol. And so, when physicians advise against exercise for those with specific diseases, one needs as much information as possible on the relative risks and benefits to justify such an approach. We do not want to inadvertently add the long-term complications of a sedentary lifestyle to those specific diseases – we need, therefore, to find the safest ‘happy medium’ in order to try and ensure that young people with GHD live a long and healthy life. Martinez and coworkers, in their recent article on RTP for elite athletes with GHD predisposing to sudden death,8 summarise many of the negative effects of disqualifying athletes, ranging from depression, anger, frustration and stress, to suicidal tendencies and social isolation from primary friend groups (often teammates), and, of course, loss of scholarships and earning capacity for professional athletes.
Historically, young people with GHD were discouraged from active sport due to natural concerns about the increased risk of SCD during competitive or intensive exercise. The emotion and shock resulting from the sudden death of a young athlete, an event often highly publicised, tends to influence medical decision-making when discussing ‘restrictions’, especially as we know that patients with GHD are at increased risk of SCD. However, we have moved now to a point where many such athletes with certain GHD can be considered for involvement in various sporting and athletic pursuits. The concept of ‘shared decision-making’ has become key, where the athlete’s preferences are considered in conjunction with assessment of risk, a review of available evidence, and with a clear understanding that there will always be some risk involved, whatever the precautions taken. This shared decision-making should initially be between the athlete and the specialist cardiologist, after the introduction of optimal medical treatment as required for the diagnosed cardiac condition, and with the understanding that regular surveillance assessment to detect alterations in phenotype is in place going forward.
If the decision is made for an athlete to return to competitive sport or intensive exercise (figure 1), we need to ask: how do we maximise protection for that athlete should they suffer an acute cardiac event? This requires that the school, college or sports club must be part of the plan. There should be discussion and ‘buy-in’ with the club coach/club doctor. Herring and colleagues, in their consensus statement “Return to sport/return to play and the team physician”, state that the final return-to-sport decision should be led by the team physician, as part of a shared decision-making process.9 The club/centre needs to ensure easy access to automated external defibrillators (AEDs), and trained personnel to use them. Sports club members should be encouraged to partake in a basic life support course. Gray et al. discuss the development of a personalised emergency action plan for such athletes, involving the cardiologist, the athlete, and the club, with the goal of successful management of the worst-case scenario for the athlete.10 The athlete with GHD needs to ‘go into battle’, as it were, knowing that there is an increased risk of sudden death, but that, if everything is planned, that risk is reduced at least to what it would be during normal daily life. Some athletes will choose to continue their sporting activities despite advice against such an approach, but with a full understanding of the risks involved, and all back-up supports should be available for them.
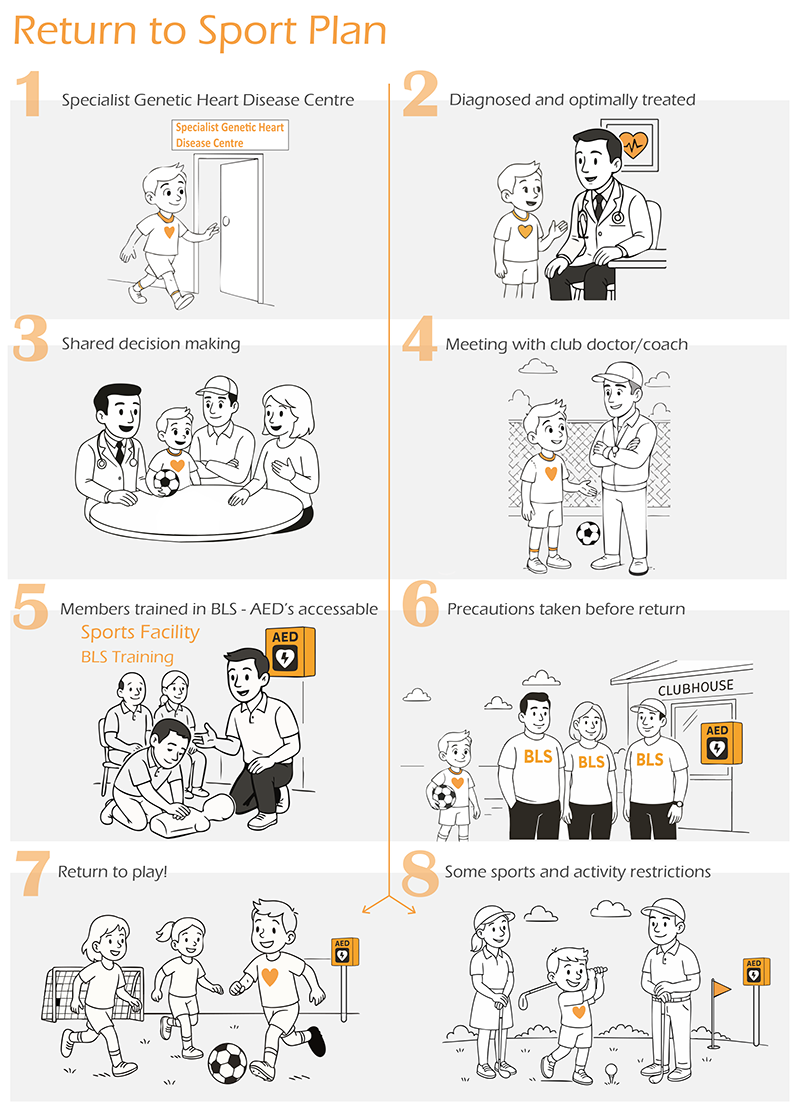
| Illustration by Noah Fingleton |
Patient-athletes with GHD who decide to return to sport should ensure some protection(s) around them. They should avoid circumstances where intensive sporting activities are performed alone, such as long-distance running or long-distance swimming. An available AED and trained personnel at hand should give comfort to all, and must be part of the cardiologist and team physician input into the shared decision-making. It should also be a part of the athlete’s programme plan, ensuring that ‘someone has your back’ should something go wrong. Running should be undertaken at a supervised facility, and swimming in a supervised pool. Although such advice may be seen as ‘restrictive’, one cannot avoid the fact that patients with GHD have an increased risk of sudden death, and genetic cardiac diseases (predominantly undiagnosed) are responsible for the majority of SCD during sporting activities in young people. The ESC 2022 guidelines for the management of patients with ventricular arrhythmias and the prevention of SCD11 notes the excellent rates of survival with favourable outcome after cardiac arrest in sports centres equipped with AEDs.12 This justifies the effort of implementing emergency programmes for SCD prevention, with the distribution of AEDs in sports and training arenas, and training of staff to perform cardiopulmonary resuscitation (CPR) and defibrillation.13
“SCA and SCD in athletes will never be prevented completely, underscoring the importance of an emergency action plan (EAP) to include cardiopulmonary resuscitation education for all stakeholders in the global sporting community and the availability of automated external defibrillators (AEDs) at all sporting venues”14
The recently published international guidelines from the AHA/American College of Cardiology (ACC),14 the ESC15 and Heart Rhythm Society (HRS),16 published as recently as June 2025, help guide our decision-making when considering RTP in patients with GHD. They are, however, only guidelines, some recommendations based on the findings of retrospective single-centre observational studies, but should serve as helpful guidance when ensuring that optimal assessment and treatment is performed prior to RTP, and on a regular basis thereafter, and when trying to sift through information on what kind of exercise is best (if any) for specific disease types. From all the available evidence, it seems reasonable for athletes who are genotype-positive but phenotype-negative for HCM to take part in all sporting activities, but with regular surveillance. Hopefully, a clearer understanding of the relationship between exercise, genotype and phenotypic expression in ARVC will allow for a more liberal approach to exercise in future. It seems reasonable to advise those at risk of syncope to avoid disciplines that could lead to fatal injury to oneself or danger to others,17 and for some athletes with ICDs to take part in sporting activities, while avoiding collision sports. It seems reasonable for those with genotype-positive phenotype-negative LQTS, when optimally treated, to participate in sporting activities.
Overall, we are cautiously moving away from the historical assumption that exercise is a ‘no-no’ for those with GHD, and with increased identification and follow-up of such patient-athlete groups, we should get an ever-greater understanding of how best to advise them in terms of exercise for improving quality of life. Hopefully, also the collection of prospective data on the benefits of readily available trained personnel and AEDs at all sporting venues will crystalise our thinking and advice further.
“Capture of prospective multicentre registry data, inclusive of a diverse population of athletes with CVD, who have chosen to either continue or cease competitive sports participation, is a scientific imperative.”14
Key messages
- All sporting centres should ideally have basic life support (BLS) training for their membership, and easily accessible and maintained automated external defibrillators (AEDs)
- Patients with genetic heart diseases returning to sport, should ensure protection(s) around them (planning for ‘worst case scenario’). They should avoid circumstances where their sports are performed alone, e.g. long-distance running or swimming. An available AED (perhaps even their own) and trained personnel should ideally be at hand
- Athletes who have any ‘episode’ or ‘event’ should avoid sporting activities until their clinical status is reassessed and stabilised over a three-month period
- Final eligibility decisions for organised sports participation may involve third parties (e.g. team physicians, consultants, institutional leadership) acting on behalf of schools or teams
Conflicts of interest
None declared.
Funding
None.
Editors’ note
This is the second part of a two-part review, the first part was published in the last issue (issue 1, 2026) http://doi.org/10.5837/bjc.2026.010. This article is also part of the Sports Cardiology series.
Recommended reading
Martinez KA, Bos JM, Baggish AL et al. Return-to-play for elite athletes with genetic heart diseases predisposing to sudden cardiac death. J Am Coll Cardiol 2023;82:661–70. https://doi.org/10.1016/j.jacc.2023.05.059
Gray B, Lampert R, Papadakis M. Return to play with genetic heart disease: the importance of developing a personalized emergency action plan. Circulation 2025;151:893–5. https://doi.org/10.1161/CIRCULATIONAHA.124.072830
Lampert R, Harmon KG. Sudden cardiac arrest in athletes. N Engl J Med 2026;394:268–80. https://doi.org/10.1056/NEJMra2312555
References
1. Lampert R, Olshansky B, Heidbuchel H et al. Safety of sports for athletes with implantable cardioverter-defibrillators: results of a prospective, multinational registry. Circulation 2013;127:2021–30. https://doi.org/10.1161/CIRCULATIONAHA.112.000447
2. Lampert R, Olshansky B, Heidbuchal H et al. Safety of sports for athletes with implantable cardioverter-defibrillators: long-term results of a prospective multinational registry. Circulation 2017;135:2310–12. https://doi.org/10.1161/CIRCULATIONAHA.117.027828
3. Saarel EV, Law I, Berul CL et al. Safety of sports for young patients with implantable cardioverter-defibrillators: long-term results of the multinational ICD sports registry. Circ Arrhythm Electrophysiol 2018;11:e006305. https://doi.org/10.1161/CIRCEP.118.006305
4. Tobert KE, Bos JM, Cannon BC, Ackerman MJ. Outcomes of athletes with genetic heart diseases and implantable cardioverter-defibrillators who choose to return to play. Mayo Clin Proc 2022;97:2028–39. https://doi.org/10.1016/j.mayocp.2022.03.024
5. Lampert R, Harmon KG. Sudden cardiac arrest in athletes. N Engl J Med 2026;394:268–80. https://doi.org/10.1056/NEJMra2312555
6. Clausen JSR, Marott JL, Holtermann A, Gyntelberg F, Jensen MT. Midlife cardio-respiratory fitness and the long-term risk of mortality: 46 years of follow-up. J Am Coll Cardiol 2018;72:987–95. https://doi.org/10.1016/j.jacc.2018.06.045
7. Tanasescu CM, Leitzmann MF, Rimm EB, Willett WC, Stempfer MJ, Hu FB. Exercise type and intensity in relation to coronary heart disease in men. JAMA 2002;288:1994–2000. https://doi.org/10.1001/jama.288.16.1994
8. Martinez KA, Bos JM, Baggish AL et al. Return-to-play for elite athletes with genetic heart diseases predisposing to sudden cardiac death. J Am Coll Cardiol 2023;82:661–70. https://doi.org/10.1016/j.jacc.2023.05.059
9. Herring SA, Putukian M, Kibler WB et al. Team physician consensus statement: return to sport/return to play and the team physician. A team physician consensus statement: 2023 update. Med Sci Sports Exerc 2024;56:767–75. https://doi.org/10.1249/MSS.0000000000003371
10. Gray B, Lampert R, Papadakis M. Return to play with genetic heart disease: the importance of developing a personalized emergency action plan. Circulation 2025;151:893–5. https://doi.org/10.1161/CIRCULATIONAHA.124.072830
11. Zeppenfeld K, Tfelt-Hansen J, de Riva M et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. https://doi.org/10.1093/eurheartj/ehac262
12. Drezner JA, Rogers KJ, Horneff JG. Automated external defibrillator use at NCAA division 11 and 111 universities. Br J Sports Med 2011;45:1174–8. https://doi.org/10.1136/bjsm.2009.070052
13. Borjesson M, Serratosa L, Carre F et al. Consensus document regarding cardiovascular safety at sports arenas: position stand from the European Association of Cardiovascular Prevention and Rehabilitation (EACPR) section of sports cardiology. Eur Heart J 2011;32:2119–24. https://doi.org/10.1093/eurheartj/ehr178
14. Kim JH, Baggish AL, Levine BD et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation 2025;151:e716–e761. https://doi.org/10.1161/CIR.0000000000001326
15. Pelliccia A, Sharma S, Gahi S et al. 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease: the task force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur Heart J 2021;42:17–96. https://doi.org/10.1093/eurheartj/ehaa605
16. Lampert R, Chung EH, Ackerman MJ et al. 2024 HRS expert consensus statement on arrhythmias in the athlete: evaluation, treatment, and return to play. Heart Rhythm 2024;21:e151–e252. https://doi.org/10.1016/j.hrthm.2024.05.018
17. Arbelo E, Protonotarios A, Gimeno JR et al. 2023 ESC guidelines for the management of cardiomyopathies: developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur Heart J 2023;44:3503–626. https://doi.org/10.1093/eurheartj/ehad194
