Cardiac sarcoidosis is a rare but potentially deadly complication of systemic sarcoidosis, in which the heart is affected by immune dysregulation and granulomatous infiltration. We present a case of a 65-year-old woman who presented with worsening breathlessness and bradycardia secondary to complete heart block. Workup with cardiovascular magnetic resonance imaging showed an increased signal on late gadolinium enhancement sequences in the anteroseptum and inferoseptum consistent with active infiltration from cardiac sarcoidosis. High-resolution computed tomography of the chest showed multifocal ground-glass opacities with a peribronchovascular distribution in keeping with sarcoidosis. A dedicated CT scan of the chest showed bilateral hilar lymphadenopathy. A further positive emission tomography scan confirmed the diagnosis of cardiac sarcoidosis in the left ventricle. The findings were discussed in the cardiology multidisciplinary team meeting and it was decided the patient needed an implantable cardioverter defibrillator with further follow-up with the respiratory and cardiology team.
Introduction
Sarcoidosis is a multisystemic, granulomatous disease of unknown aetiology, frequently manifesting as a mild or even asymptomatic pulmonary disease.1
Cardiac sarcoidosis is the second most common cause of death in sarcoidosis patients globally and the first among Japanese sarcoidosis patients.1 The pathology consists of granulomatous inflammation of the pericardium, myocardium and endocardium with patchy, multifocal involvement. Several infectious organisms have been suggested as possible agents in the aetiology of sarcoidosis, although Propionibacterium acnes (P. acnes) is the only microorganism to be isolated from sarcoid lesions.1
The heart can be affected by sarcoidosis in two ways. Firstly, sarcoidosis can occur in the heart muscle, known as cardiac sarcoidosis. Secondly, the heart may be indirectly affected due to pulmonary hypertension caused by lung sarcoidosis.2 The accumulation of immune cells causes clumps of tissue (granulomas), which can occur in the heart.
In advanced cases, cardiac sarcoidosis can lead to an arrhythmia or heart failure.2
Cardiac sarcoidosis is known to cause atrioventricular block, ventricular arrhythmias, sudden cardiac death or heart failure.2
Case report
A 65-year-old woman with a past medical history of hypertension presented with progressive breathlessness and bradycardia of 38 bpm. The patient had been experiencing breathlessness on exertion over the preceding three months. The patient had no significant family history of note.
During a previous admission in July 2024, the patient presented with syncope and left-sided chest pain. The chest x-ray, transthoracic echocardiogram and coronary angiogram were normal. The patient was diagnosed with myocardial infarction with non-obstructive coronary arteries. The electrocardiogram (ECG) at that time showed a right bundle branch block and first-degree atrioventricular (AV) heart block. The patient was discharged with a plan for an urgent outpatient 24-hour ambulatory monitor, which showed occasional non-conducted P-waves with evidence of second-degree heart block Mobitz type I (Wenckebach). There was no evidence of a higher degree AV block and the patient remained asymptomatic of these findings at that time.
Following discharge, the patient had episodes of severe breathlessness on exertion, which was eased with rest. Episodes of palpitations and dizziness accompanied this.
During this admission, the patient presented feeling unwell with worsening breathlessness and dizziness. A home ambulatory monitor showed a fall in heart rate to 38 bpm. While in the emergency department, the patient suffered an episode of syncope, with further monitoring showing intermittent episodes of complete heart block.
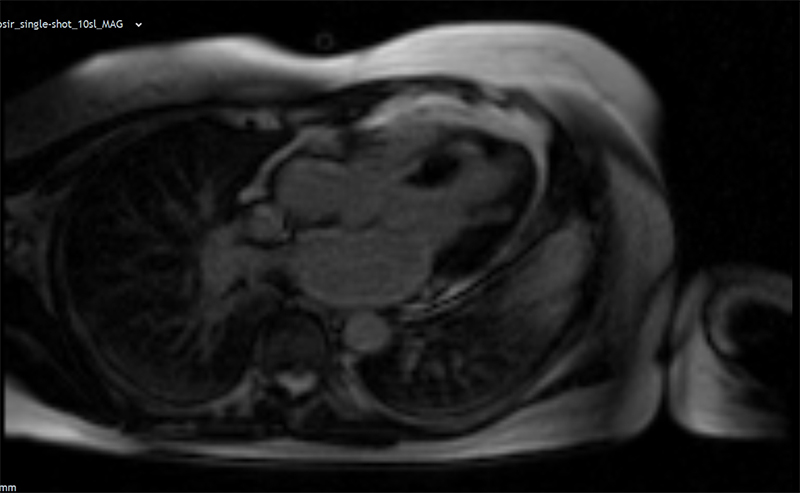
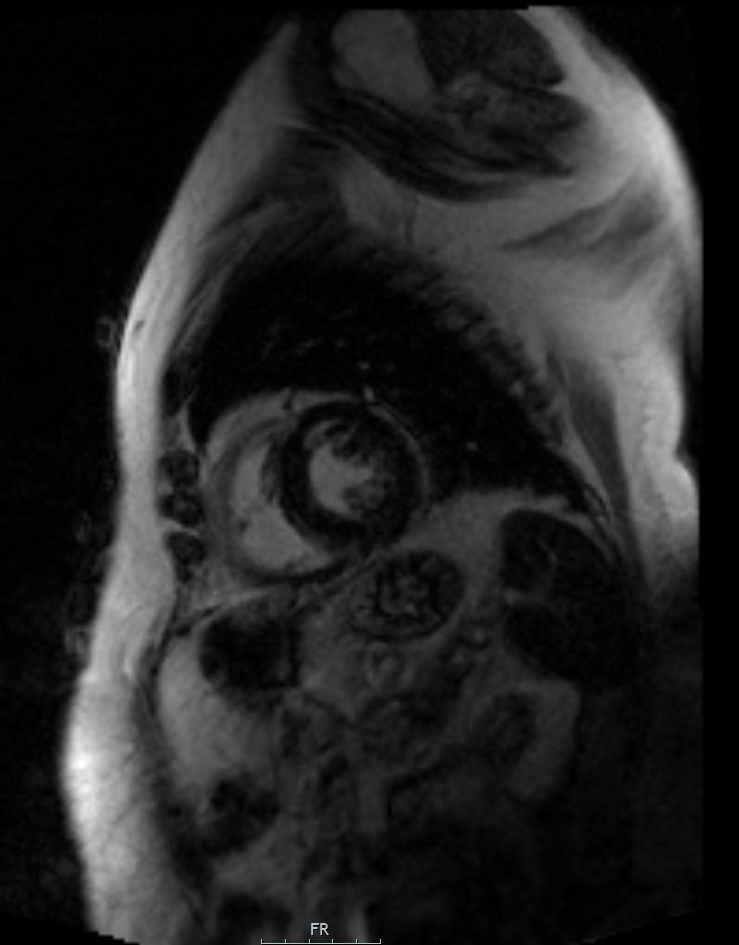
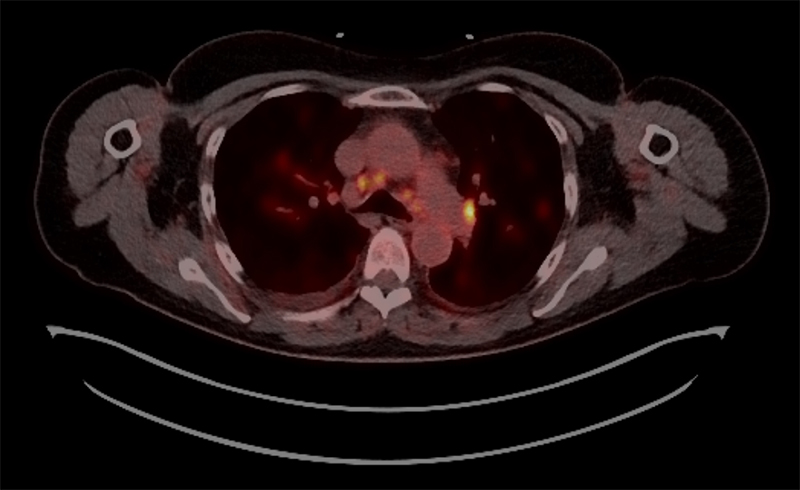
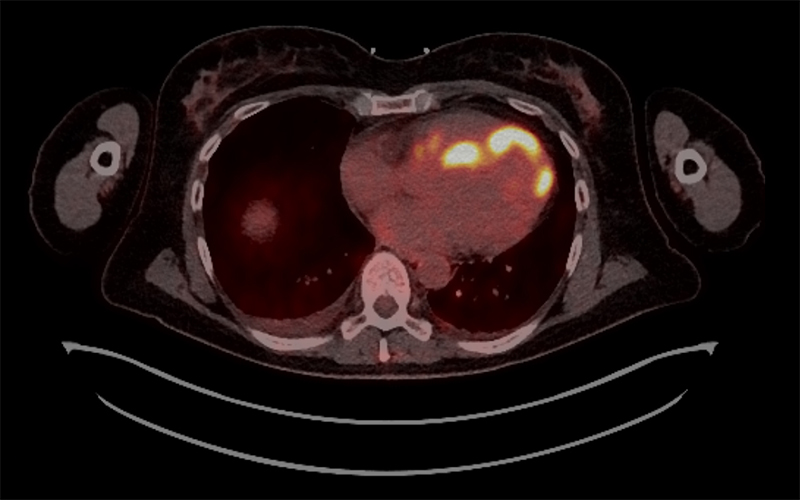
The patient proceeded to have cardiac magnetic resonance (CMR) and positive emission tomography (PET) imaging, which strongly suggested cardiac sarcoid infiltration (figures 1–4).
An implantable cardioverter defibrillator (ICD) was placed because of her complete heart block and syncopal episodes. Due to the active involvement of sarcoidosis seen on the scan, the patient was commenced on prednisolone 30 mg daily for a month, with a plan to then taper this down. The patient will have ongoing regular follow-up.
Epidemiology
The incidence and prevalence of sarcoidosis varies widely across the globe and has been reported to be higher in populations of northern European and African American descent.3 The highest incidence has been reported in Scandinavian countries, with an estimated 11.5 cases per 100,000 individuals. In the United States, it ranges from eight to 11 per 100,000 people and is reported to be lower in other parts of the world, including Canada (6.8 per 100,000) and East Asian countries such as South Korea (0.5–1.3 per 100,000). The highest prevalence has been noted among Black American women (178.5 per 100,000).3
Discussion
This case reinforces the importance of detailed workup in patients with suspected cardiac sarcoidosis, including an ECG, high-resolution computed tomography, CMR and PET scans.
In daily practice, decisions leading to permanent pacemaker (PPM) versus ICD implantation are not always so straightforward.4 Advantages of directly proceeding with an ICD include avoidance of undue additional procedural risk (initial PPM implantation, followed by an upgrade to ICD) and to allow for protection against arrhythmia during diagnostic workup. The disadvantages are increased risks of complications compared to PPM, such as the additional risk of inappropriate shocks, and increased unnecessary costs if, on further diagnostic testing, the patient is found not to have sarcoidosis.4 ICD placement is highly recommended in patients with sarcoidosis and a history of non-sustained ventricular tachycardia.5
The multisystem involvement of sarcoidosis warrants a multidisciplinary team approach for accurate diagnosis, treatment, and comprehensive care.6 Patient preferences and input are essential to the process of deciding when and how to treat. Patients should be made aware of the progressive nature of the disease and the need for repeat evaluation and imaging to guide timely therapy.
Corticosteroids are the first-line treatment. They may improve survival but they do not reduce the incidence of ventricular arrhythmias.5 Most experts suggest an initial dose of 30–40 mg/day of prednisolone7 with the response to treatment evaluated after one to three months. If there has been a response, the prednisolone dose should be tapered to 5 to 15 mg/day, with treatment planned for an additional nine to 12 months.7
Patients should be followed for at least three years after discontinuing treatment to assess for relapse. Methotrexate is often used as a second-line agent in refractory cases and/or if there are significant steroid side effects. Other therapies that have been used in cardiac sarcoidosis include azathioprine, cyclophosphamide, and infliximab.7
Corticosteroids have been reported to reduce the burden of ventricular tachycardia, reverse AV block, and improve left ventricular ejection fraction (LVEF). The goal of corticosteroid immunosuppression is early initiation of therapy before the LVEF decreases and to reduce corticosteroid exposure.3
Conflicts of interest
None declared.
Funding
None.
Patient consent
Written consent was granted by the patient for publication of this case report.
References
1. Markatis E, Afthinos A, Antonakis E, Papanikolaou IC. Cardiac sarcoidosis: diagnosis and management. Rev Cardiovasc Med 2020;21:321–38. https://doi.org/10.31083/j.rcm.2020.03.102
2. Hussain K, Shetty M. Cardiac sarcoidosis. [Updated 2024 Mar 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK578192/
3. Mathai SV, Patel S, Jorde UP, Rochlani Y. Epidemiology, pathogenesis, and diagnosis of cardiac sarcoidosis. Methodist DeBakey Cardiovasc J 2022;18:78–93. https://doi.org/10.14797/mdcvj.1057
4. Uzunoglu EC, Liu K, Spragg D et al. Skipping sarcoidosis: when ventricular arrhythmia arises immediately post-permanent pacemaker implantation. HeartRhythm Case Rep 2023;9:844–7. https://doi.org/10.1016/j.hrcr.2023.09.003
5. Doughan AR, Williams BR. Cardiac sarcoidosis. Heart 2006;92:282–8. https://doi.org/10.1136/hrt.2005.080481
6. Cheng RK, Kittleson MM, Beavers CJ et al. on behalf of the American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology, and Council on Cardiovascular and Stroke Nursing. Diagnosis and management of cardiac sarcoidosis: a scientific statement from the American Heart Association. Circulation 2024;149:e1197–e1216. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001240
7. Birnie DH, Nery PB, Ha AC, Beanlands RSB. Cardiac sarcoidosis. J Am Coll Cardiol 2016;68:411–21. https://doi.org/10.1016/j.jacc.2016.03.605
