Platypnea-orthodeoxia syndrome (POS) is a rare condition which presents with positional dyspnoea and deoxygenation on an orthopneic position which resolves when supine. We present a rare presentation of POS in a 75-year-old man, who initially presented with mixed symptomology including dyspnoea on exertion and syncope. He was found to have intermittent symptomatic hypoxia and initial investigations ruled out infection, pulmonary embolism and interstitial lung disease. Pulse oximetry confirmed positional variations in oxygenation. A transthoracic echocardiogram and a transoesophageal bubble echocardiogram with positional manoeuvres confirmed the presence of a large patent foramen ovale (PFO) with shunting. The patient was referred to the tertiary centre for PFO closure which resulted in resolution of his symptoms. This case report highlights the importance of recognising POS as a rare differential in causes of unexplained dyspnoea and utilising multiple imaging techniques to confirm the diagnosis.
Introduction
Platypnea-orthodeoxia syndrome (POS) is a rare condition, the prevalence of which has yet to be estimated in the literature.1 It presents with positional dyspnoea and deoxygenation on an orthopneic position which resolves when the patient moves to a supine position. Diagnosis is often challenging and this syndrome is thought to be under-recognised.2
Its mechanisms are not fully understood but these can be classified into extracardiac and intracardiac causes. Extracardiac causes include pathology leading to intrapulmonary shunting or ventilation-perfusion mismatch, such as pulmonary arteriovenous malformations or severe intestinal lung disease. Intracardiac causes are more commonly reported and include atrial septal defects (ASD) or a patent foramen ovale (PFO).3 In cases of intracardiac shunting, a further abnormality which results in an increase in right-to-left shunting of blood is required to produce symptoms. This could be due to raised right atrial pressures, such as in pulmonary hypertension or after pneumonectomy, or to preferential blood flow across the defect with normal right atrial pressures, such as in aortic dilatation, elongation or aneurysm.4 The need for a further abnormality may explain why POS presents later in life, with one multicentre study reporting the average age of people requiring PFO closure secondary to POS is 67 years.5 We present here a rare case of POS secondary to a PFO and the diagnostic challenge that it presented.
Case report
A 75-year-old male patient presented to the emergency department with generalised weakness, dizziness, syncopal episodes, shortness of breath and chest discomfort on exertion. These symptoms had progressively worsened over the preceding 12 months and he now felt unable to cope. The patient had a past medical history of type 2 diabetes, controlled hypertension, chronic kidney disease (baseline eGFR 67) and was under surveillance for aortic root dilatation.
Prior to this admission, the patient had undergone multiple outpatient investigations for these progressive symptoms. Coronary angiogram showed moderate right coronary artery stenosis but subsequent stress echocardiogram did not demonstrate any inducible ischaemia. Isosorbide mononitrate was tried but had no effect. An echocardiogram showed good biventricular systolic function with mild aortic regurgitation and aortic root dilatation (sinus of Valsalva 41 mm). Holter monitor investigations showed no arrhythmias.
The patient suffered a pre-syncopal episode whilst awaiting review in the emergency department. On examination, he was found to have significant hypoxia, confirmed on arterial blood gas, which required 15 litres of oxygen to maintain normal saturations. Physical examination and initial investigations including respiratory viral screen, electrocardiogram, chest x-ray, computed tomography pulmonary angiogram, and full autoimmune screen showed no cause to explain his symptoms. He was commenced on empirical treatment for a chest infection with oral steroids and intravenous antibiotics, both stopped soon after, as an infective cause was excluded. The patient was reviewed multiple times for intermittent episodes of acute deoxygenation on pulse oximetry but always with subsequent normalisation. Pulse oximetry testing showed positional variations in oxygenation; saturations were 98% supine, 94% sitting, 93% standing and dropping to below 88% upon mobilisation in keeping with POS.
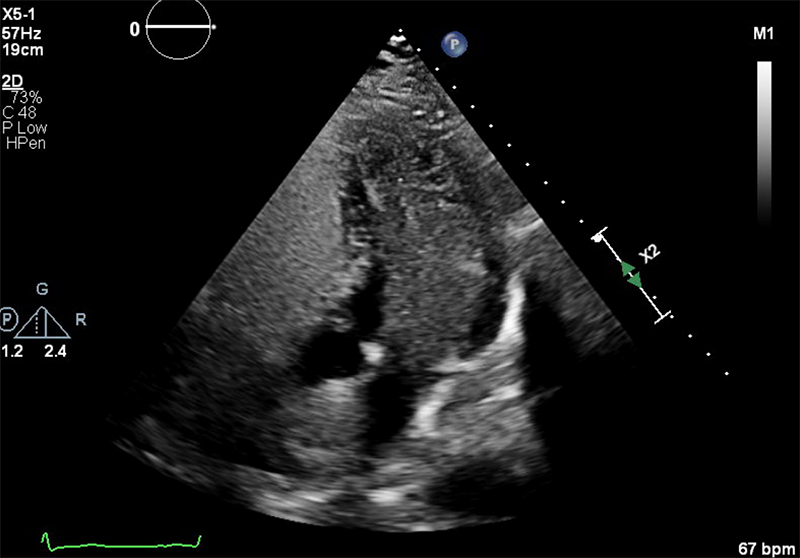
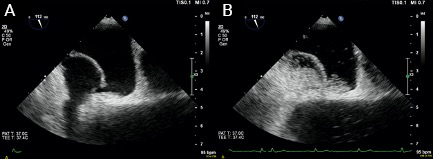
At this point, an intracardiac shunt was suspected and a bubble study with transthoracic echocardiography (TTE) was clearly positive with microbubbles almost completely filling the left heart chambers (figure 1). The dilated aortic root obscured the atrial septum so a PFO or ASD could not be identified. There was no evidence of a pulmonary arteriovenous malformation or hepatopulmonary shunt on CT scan. Transoesophageal echocardiography (TOE) with a bubble study confirmed a PFO measuring 40 mm maximally, causing a right-to-left shunt with large numbers of microbubbles crossing the interatrial septum when the patient was positioned at 45 degrees (semi upright) and less so when he was lying supine (figure 2).
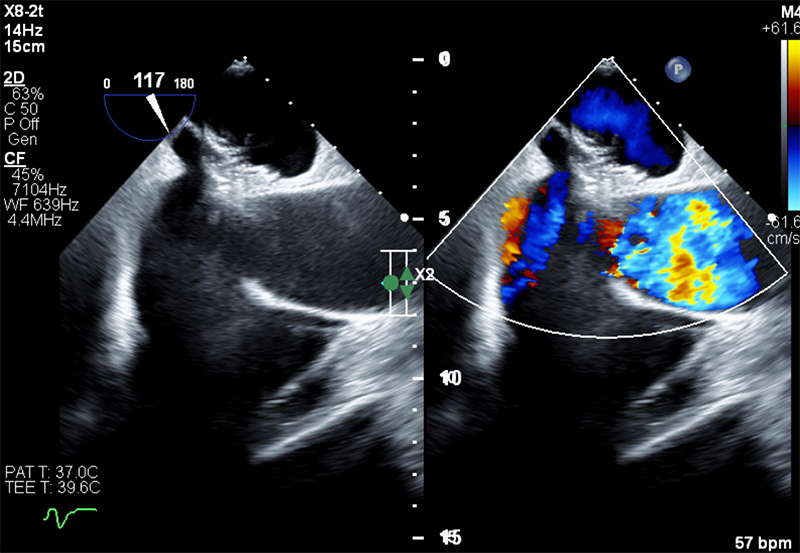
The patient was transferred to the tertiary cardiac centre for PFO closure (figure 3), which was completed with no complications using a Gore septal occluder device. Follow-up confirmed complete symptom resolution including positional hypoxia.
Discussion and conclusion
This case highlights the importance of recognising POS as a rare differential in recurrent unexplained dyspnoea and fluctuating hypoxia where no obvious alternative can be identified. The case also highlights that the diagnosis is predominantly clinical, where simple investigations such as pulse oximetry measurements with positional changes can help identify POS and prompt further imaging. In this case, a TTE and bubble study helped identify the presence of a right-to-left shunt and possibly contributing anatomical abnormalities. The utility of a bubble TOE was to confirm and visualise the size and location of the PFO. Syncope is not a typical symptom of POS but it has been implicated in the literature secondary to POS and PFOs.6,7 This patient’s syncopal symptoms resolved following the PFO closure, demonstrating the importance of recognising POS secondary to a PFO as a rare differential in unexplained syncope.
The postulated mechanism of syncope in relation to POS and PFO is believed to arise from a large right-to-left shunt resulting in deoxygenated venous blood entering the arterial circulation causing transient cerebral hypoxia.6 This raises the question of why the patient presented at this particular stage in life, since his PFO was likely present from birth. As previously mentioned, the patient was under surveillance for a dilated aortic root. Progression of this with increasing age may have precipitated his symptoms.4 The mechanism for this is not clearly understood but it is hypothesised that biomechanical changes from the enlarging aortic root may cause this – the enlarging root reduces the distance between the aorta and the posterior wall of the atria, subsequently increasing the mobility of the atrial septum and the flap valve of the fossa ovalis. This is thought to generate a ‘spinnaker effect’ and a billowing of venous flow which holds the PFO open, as described by Eicher et al.8 This effect is compounded in the upright position as this further repositions the atrial septum, causing preferential flow of deoxygenated blood from the inferior vena cava through the PFO.3
Conflicts of interest
None declared.
Funding
None declared.
Patient consent
Patient consent was obtained for the use of images, writing of the case and publication.
References
1. Khauli S, Chauhan S, Mahmoud N. Platypnea [Internet]. University of Wisconsin: StatPearls Publishing, Treasure Island (FL); 2022. Available from: http://europepmc.org/abstract/MED/30521255 (last accessed 9th April 2024)
2. Rodrigues P, Palma P, Sousa-Pereira L. Platypnea-orthodeoxia syndrome in review: defining a new disease? Cardiology 2012;123:15–23. https://doi.org/10.1159/000339872
3. Agrawal A, Palkar A, Talwar A. The multiple dimensions of platypnea-orthodeoxia syndrome: a review. Respir Med 2017;129:31–8. https://doi.org/10.1016/j.rmed.2017.05.016
4. Ahmed A, Rupal A, Walker A et al. Patent foramen ovale and ascending aortic dilatation causing platypnea-orthodeoxia syndrome. Cureus 2022;14:e26953. https://doi.org/10.7759/cureus.26953
5. Guérin P, Lambert V, Godart F et al. Transcatheter closure of patent foramen ovale in patients with platypnea-orthodeoxia: results of a multicentric French registry. Cardiovasc Intervent Radiol 2005;28:164–8. https://doi.org/10.1007/s00270-004-0035-3
6. Wang X, Liu X, Zheng L et al. Correlation between percutaneous patent foramen ovale closure and recurrence of unexplained syncope. Front Neurol 2023;14:1104621. https://doi.org/10.3389/fneur.2023.1104621
7. Pearman CM, Andron M. An unusual cause for collapse. BMJ 2010;341:c3975. Available from https://www.bmj.com/content/341/bmj.c3975.full (accessed 7th April 2025)
8. Eicher J-C, Bonniaud P, Baudouin N et al. Hypoxaemia associated with an enlarged aortic root: a new syndrome? Heart 2005;91:1030–5. https://doi.org/10.1136/hrt.2003.027839
