Physiological adaptation to exercise results in a series of electrical, structural, and functional cardiac changes, broadly named ‘athlete’s heart’. Symmetrical enlargement of all cardiac chambers and mild increase in wall thickness are common findings in highly trained athletes. Typical electrocardiogram (ECG) features include sinus bradycardia, first-degree atrioventricular (AV) block, isolated voltage criteria for right and left ventricular hypertrophy and early repolarisation. Cardiac remodelling may be marked in some athletes, and it may be challenging to distinguish physiological adaptation from cardiac conditions at risk of sudden cardiac death (SCD), such as cardiomyopathies. Differential diagnosis often requires a comprehensive assessment starting from a detailed personal and family history to baseline tests, such as ECG and echocardiogram. In some cases, second-line tests, such as prolonged ambulatory ECG monitoring, exercise tolerance test and cardiovascular magnetic resonance are required.
In this narrative review, we will explore the key features of physiological cardiac adaptation to exercise, and we will focus on differential diagnosis between ‘athlete’s heart’ and cardiomyopathies.
Introduction
Regular intense exercise often results in a series of electrical, structural and functional changes, collectively named as the ‘athlete’s heart’.1 These include mild harmonic increases in cardiac chamber size and in left ventricular wall thickness.2 Athletes often exhibit sinus bradycardia, first-degree atrioventricular (AV) block, isolated QRS voltage criteria for right and left ventricular hypertrophy and early repolarisation.3 These physiological changes can closely mimic serious cardiac conditions, such as cardiomyopathies.4 The differentiation between ‘athlete’s heart’ and cardiomyopathies is crucial to prevent unnecessary restriction from competitive sports, and to ensure those with underlying pathological conditions receive appropriate management in order to avoid potentially fatal ventricular arrhythmias and sudden cardiac death (SCD).5–10 In this narrative review, we will discuss the challenges in the differentiation between cardiac changes observed as part of physiological adaptation to exercise and cardiomyopathies. We will, therefore, focus on the strategies to accurately differentiate between benign and pathological entities.
The athlete’s heart: physiological adaptation to exercise
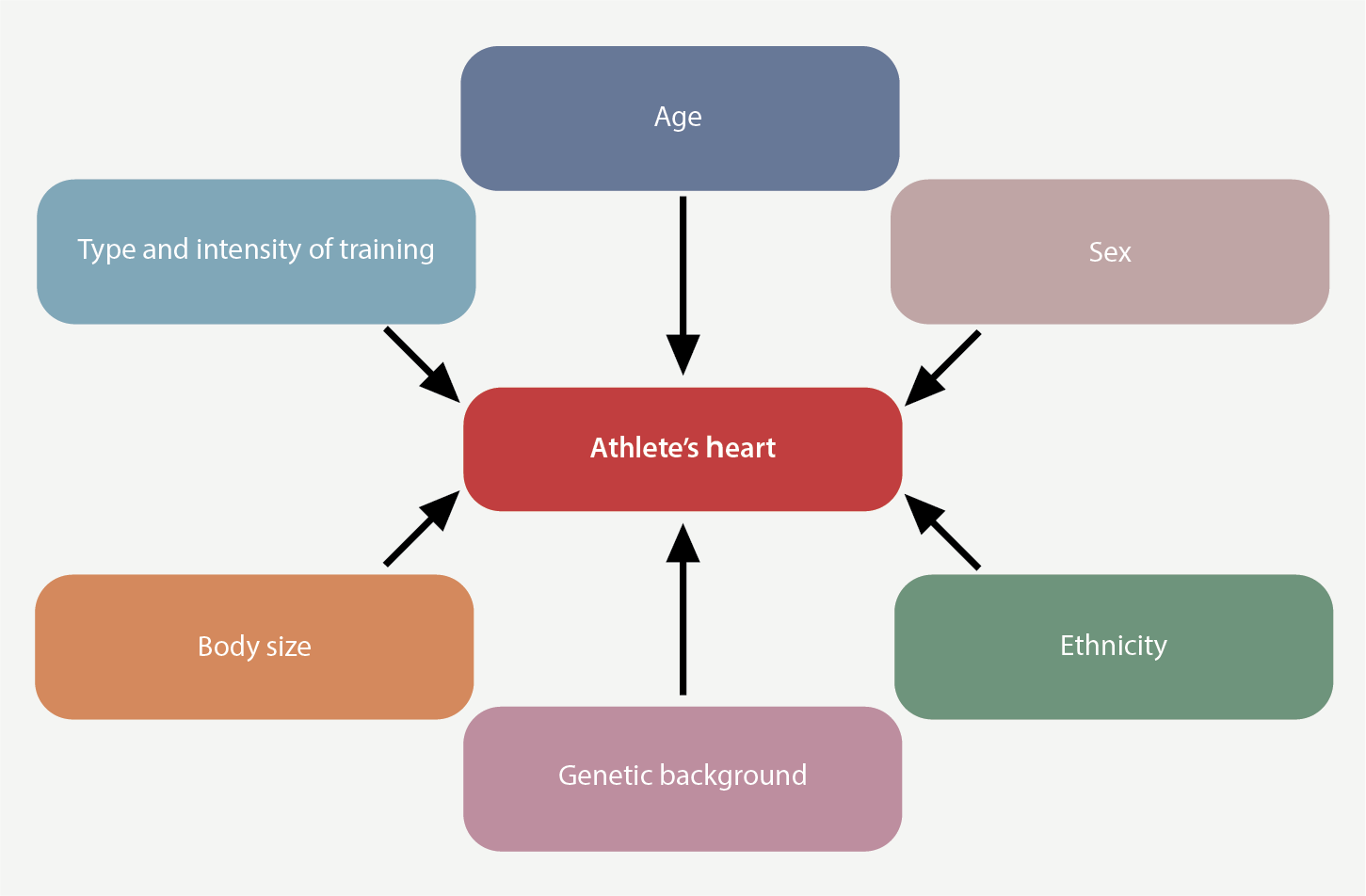
Cardiac adaptation to exercise in athletes is influenced by several factors, including the type and intensity of training, age, sex, ethnicity, and body size (figure 1). Knowledge of determinants of cardiac adaptation is crucial to ensure a learned and contextualised interpretation of cardiac investigations.
Electrocardiogram
Highly trained athletes display a plethora of electrocardiogram (ECG) changes, which typically result from physiological adaptation to exercise.3,11,12 Sinus bradycardia, sinus arrhythmia, first-degree and Mobitz type I second-degree AV blocks are common in athletes, and are due to increased vagal activity and intrinsic AV node changes. Prominent QRS voltages are frequently observed, especially in male athletes.3,13 Similarly, incomplete right bundle branch block (RBBB) and early repolarisation are common findings, which do not require any further investigation.3,14–16 T-wave inversion (TWI) ≥1 mm in depth in the anterior leads is a marker of physiological adaptation to exercise in some athletes, especially when preceded by J-point/coved ST-segment elevation.3,17 This pattern is more common in black athletes.18 The clinical significance of TWI varies according to its lead distribution on the ECG, namely anterior (leads V2–V4), lateral (V5 and/or V6, I and aVL) and inferior (II and aVF) leads. TWI may occasionally be more widespread, affecting the anterolateral and/or inferolateral leads.19 TWI is one of the most common ECG manifestations in individuals with cardiomyopathies and, therefore, differentiation between benign forms and pathological findings is crucial in this setting.3
Structural and functional adaptation
Elite athletes exhibit a series of structural and functional features, including increased left ventricular (LV) and right ventricular (RV) volumes, wall thickness and larger atrial dimensions.2,20
Endurance athletes, particularly males with a large body surface area (BSA), tend to exhibit a significant increase in ventricular size. This is especially evident in those who participate in high-intensity dynamic exercise, for example competitive cyclists, who often display a combination of enlarged cavity dimensions, with a left ventricular end-diastolic diameter (LVEDD) commonly >60 mm, and mild reduction in left ventricular ejection fraction (LVEF).21 A study on Italian Olympic athletes across 38 sports, particularly in endurance disciplines, showed that 14% of male Olympic athletes exhibit a LVEDD greater than 60 mm.22 In contrast, in healthy female athletes, a significant increase in absolute values of LV dimensions is rarely observed.22–26 Conversely, when indexed for BSA, LVEDD has been found to be significantly higher in female athletes compared with their male counterparts.27
A large observational study that enrolled 2,723 athletes (1,819 white, 904 black) demonstrated that an increased left ventricular wall thickness (>12 mm) is rarely observed in white male athletes but is more common in black athletes of African and Afro-Caribbean descent (respectively 1.6% and 12.4%).18 In contrast, female athletes rarely exhibit a left ventricular wall thickness >12 mm, and this finding should be considered a red flag, raising the suspicion of cardiomyopathy.23,25–27
Age is also a determinant of cardiac remodelling in athletes. Highly trained junior athletes typically exhibit only modest increase in LV cavity size and mass. In adolescent male athletes, for instance, LVEDD at echocardiography usually ranges between 40 and 60 mm, and less than 20% exceed 54 mm, with dimensions above 60 mm being uncommon.24 Additionally, while trained adolescent athletes tend to show greater absolute left ventricular wall thickness compared with their non-athlete counterparts, only a small fraction exhibit a left ventricular wall thickness >12 mm. When this degree of increased wall thickness is observed, it is almost always associated with concurrent enlargement of the LV cavity in healthy athletes.28
The RV is often dilated in endurance athletes, reflecting the high preload.2,29,30 Physiological dilatation of the RV may be erroneously interpreted as a sign of arrhythmogenic cardiomyopathy (ACM).31,32 Healthy athletes rarely show an RV end-diastolic volume/LV end-diastolic volume >1.2 and an RV ejection fraction (RVEF) <45% on cardiac magnetic resonance (CMR).33,34
Differential diagnosis with cardiomyopathies
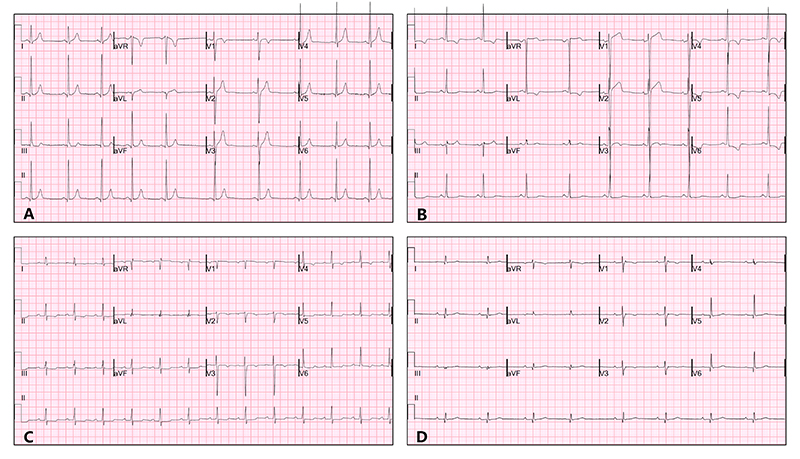
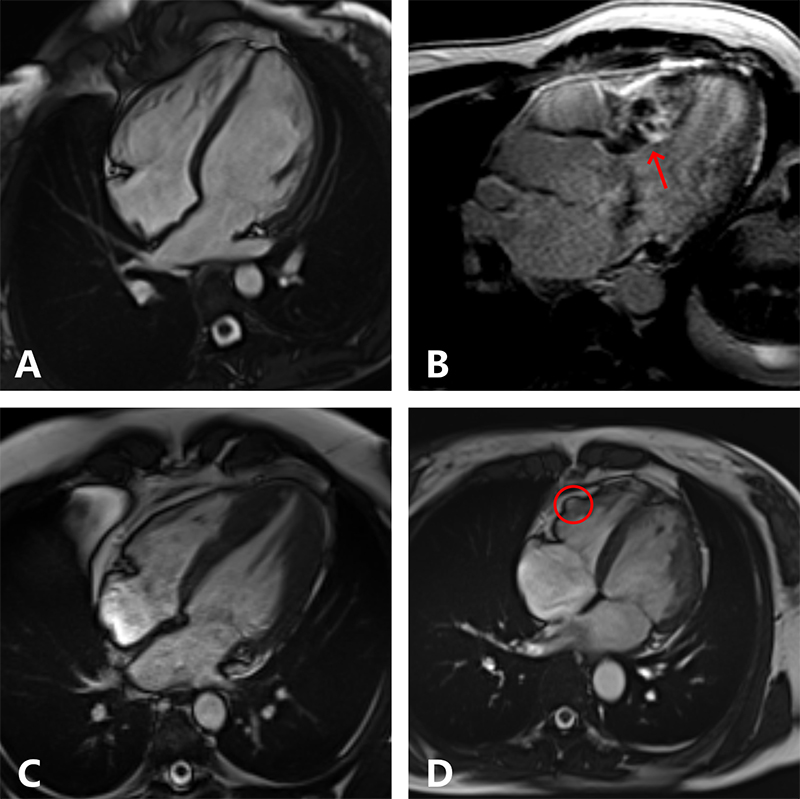
Cardiomyopathies are a heterogeneous group of conditions that affect the heart muscle, leading to structural and functional abnormalities.35 Cardiomyopathies are common aetiologies of SCD in young athletes.10 The most common types include hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy (DCM), and arrhythmogenic cardiomyopathy (ACM).36 Each type presents distinct pathophysiological features that may overlap with physiological cardiac adaptation to exercise (figure 2).37,38 Various diagnostic tools and criteria have been developed to aid clinicians in this process, including ECG, transthoracic echocardiography (TTE), CMR, and genetic testing.39 In the absence of symptoms, the diagnosis may be triggered by the detection of ECG abnormalities, for example, in the context of pre-participation screening (figure 3). TTE should be the primary imaging modality for athletes with suspected cardiac pathology. CMR imaging may provide further insights into differential diagnosis. Beyond the very high spatial and temporal resolution, CMR allows tissue characterisation and may reveal myocardial oedema, tissue infiltration and myocardial fibrosis (figure 4).
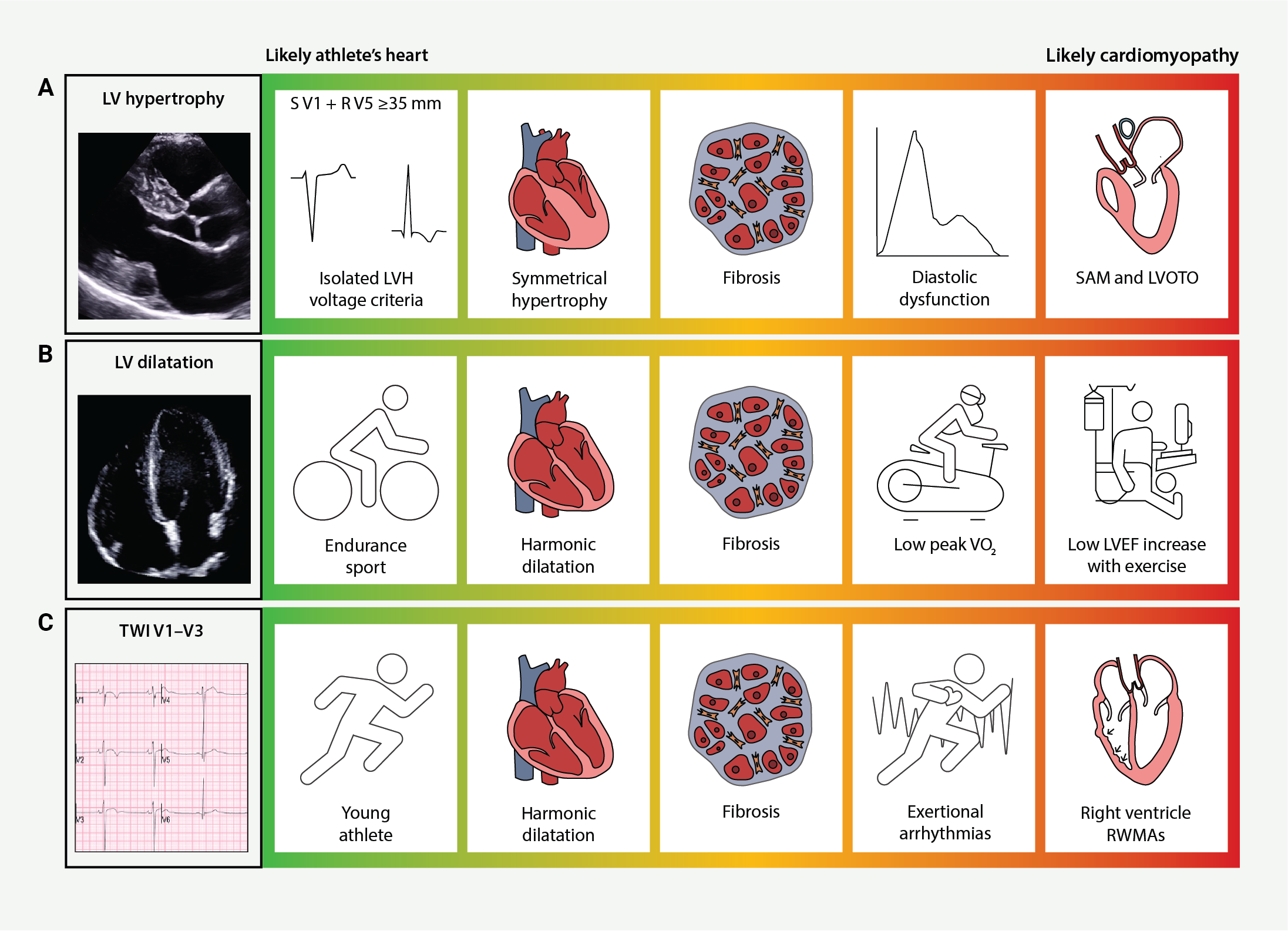
| Key: LV = left ventricle; LVEF = left ventricular ejection fraction; LVH = left ventricular hypertrophy; LVOTO = left ventricular outflow tract obstruction; RWMAs = regional wall motion abnormalities; SAM = systolic anterior motion; TWI = T-wave inversion |
Differential diagnosis with HCM
HCM is generally defined by the presence of left ventricular hypertrophy (LVH) with left ventricular wall thickness ≥15 mm in one or more myocardial segments, which is not explained by loading conditions.35,40 One of the most feared complications of HCM is SCD, which can be the first manifestation of the disease in otherwise asymptomatic individuals.41,42 Risk stratification in patients who are diagnosed with this condition is crucial for prevention and to instigate appropriate clinical management.43
Electrocardiogram
The ECG is abnormal in about 95% of patients with HCM.35 Pathological features that should raise suspicion of the disease include pathological Q-waves, ST-depression, and TWI, especially in the inferior and lateral leads.44 In contrast, the ECG of highly trained athletes often reveals isolated voltage criteria for LVH, which is unusual in patients with HCM.3 Particular care should be taken when assessing Q-waves, and specifically pathological Q-waves (≥40 ms in duration and/or Q/R ratio ≥0.25 in two or more contiguous leads, excluding leads III and aVR), and ‘benign’ Q-waves, which can often be found in healthy athletes.3,45,46 ST-segment depression ≥0.5 mm (relative to the isoelectric PR segment), in two or more leads, should be considered an abnormal finding and warrants further investigation to assess for underlying structural heart disease.3,45,47 Lateral TWI should always be considered pathological until proven otherwise. A normal echocardiography may not be of full reassurance, and further assessment with CMR is indicated.3
Echocardiogram
TTE is the first-line imaging test in individuals with suspected HCM. Diagnosis of HCM relies on the demonstration of LVH (wall thickness ≥15 mm or ≥13 mm when combined with ECG abnormalities or family history of HCM).35 A wall thickness of 16 mm or more is very rarely found in elite athletes, and this finding should always raise the suspicion of HCM.18 Therefore, the dilemma usually arises in asymptomatic athletes with mild asymmetric LVH of 13 to 15 mm, defined as ‘grey zone’. It is not just the absolute values of wall thickness that should be taken into consideration. Physiological LVH is often accompanied by enlargement of all four chambers and normal diastolic and longitudinal systolic functions.2 A relative wall thickness (RWT) exceeding 0.5 should raise the suspicion of HCM, regardless of ethnicity.48 The LVEDD has been proposed as a possible discriminator between physiological LVH and mild expression of HCM. Sheikh et al. compared 15 athletes with HCM in the ‘grey zone’ to 55 healthy athletes, both groups exhibiting concentric LVH with left ventricular wall thickness (LVWT) between 13 and 16 mm. A LVEDD ≤51 mm had good discriminating ability, but with a low sensitivity. Indeed, 13% of athletes with HCM in the ‘grey zone’ had a LVEDD >54 mm.49 Other factors that favour pathology include impaired diastolic function, a bizarre pattern of LVH, asymmetric LVH, and dynamic LV outflow obstruction.50
LV diastolic function is always normal, or even supranormal, in athletes, reflecting an enhanced ventricular filling pattern. Most diastolic function indicators have shown low sensitivity for detecting HCM in athletes. A retrospective analysis of LV diastolic function indices in 1,510 healthy young athletes, compared with 58 young patients with HCM, identified that the most sensitive diastolic markers for HCM include septal E wave <10 cm/s, lateral E wave <12 cm/s, average E/E’ >7.9, and E/A ratio <1.8.51
Finally, TTE may fail in the detection of apical HCM, due to poor visualisation of the LV apex.52,53
Further investigations
Athletes in the ‘grey zone’ should be investigated with more detailed tests. CMR is crucial in this setting, providing an accurate assessment of LVWT, chamber volumes, and LV mass. Due to its excellent spatial resolution, this test enables the evaluation of apical hypertrophy and of subtle LVH that may not be adequately visualised by echocardiography. Notably, CMR detects hypertrophy in approximately 12% of HCM patients who were not diagnosed through TTE due to segmental LVH.54 In addition, CMR allows a detailed assessment of possible architectural changes of the LV, including hypertrophic, accessory and anteriorly displaced papillary muscles and apical systolic obliteration.53,55 The presence of myocardial crypts, which are defined as narrow, deep, blood-filled invaginations within the compacted myocardial wall, may suggest an underlying genotype positive status, even in the absence of other phenotypic signs of HCM.56 Furthermore, CMR offers the possibility of tissue characterisation through late gadolinium enhancement (LGE) imaging. Patchy LGE suggests interstitial myocardial fibrosis, which is often present in HCM patients, especially within the hypertrophied segments.57 Other techniques, such as T1 mapping, allow quantification of the myocardial extracellular volume (ECV), which correlates with diffuse interstitial fibrosis.58 A study on 50 HCM patients and 40 highly trained healthy athletes demonstrated that as LVH increases, extracellular compartment decreases in athletes but increases in HCM patients.59 The negative correlation between ECV and wall thickness in athletes suggests that the increase in LV mass in healthy myocardium is driven by cellular hypertrophy, whereas in HCM, it is due to extracellular matrix expansion and myocardial disarray.60
Other investigations can help in the differential diagnosis, such as cardiopulmonary exercise test (CPET) and ambulatory ECG monitoring. Athletes without pathological remodelling would be expected to have a high exercise tolerance (peak oxygen consumption [pVO2] >50 ml/kg/min or >20% above the predicted maximum value) and absence of arrhythmias on ambulatory ECG monitoring.49,61,62 Genetic testing should be reserved for those with high clinical suspicion or when the diagnosis remains uncertain.63–65
Differential diagnosis with DCM
DCM is currently defined by the presence of LV or biventricular dilatation and systolic dysfunction in the absence of abnormal loading conditions or coronary artery disease sufficient to cause global systolic impairment.35,36 DCM may cause SCD in athletes, and, therefore, it is extremely important to differentiate physiological adaptation to exercise from DCM. It is not uncommon, especially for endurance athletes, to exhibit a markedly dilated LV and low LVEF, features that are typically observed in DCM.21
Electrocardiogram
Abnormal ECG features are reported in up to 80% of cases of DCM.66 Various ECG abnormalities should raise the suspicion of DCM in an athlete with a dilated LV. Left bundle branch block (LBBB) is a common ECG feature, followed by left atrial enlargement, left axis deviation, low QRS voltages, TWI and pathological Q-waves.67 Although sinus bradycardia and first-degree AV block are normal in athletes, extreme bradycardia (<30 bpm) and advanced AV blocks suggest a pathological process and require further investigation.3 Some ECG abnormalities in this context may even suggest the underlying genetic substrate. Examples are sinus node disease, AV blocks, and LBBB which, in the appropriate clinical context, may suggest a lamin A/C (LMNA) cardiomyopathy, or low QRS voltages, in combination with inferolateral TWI, which may suggest filamin C (FLNC) or desmosomal disease.67
Echocardiogram
DCM is traditionally defined by the presence of LVEF <45% (>2 standard deviations [SD]) or fractional shortening <25% (>2 SD) and LVEDD >117% of predicted value corrected for age and BSA (>2 SD of the predicted normal limit +5%), in the absence of myocardial disease.68 Endurance athletes often exhibit increased biventricular dimensions.22 In highly trained endurance athletes, the LV dilatation may be accompanied by a mildly reduced LVEF (45–54%).69 An observational study of elite cyclists who participated in the Tour de France in 1995 and 1998, found that 51% of them exhibited LV dilatation (LVEDD >60 mm), and 18% a LVEF <55%.21
Further investigations
In athletes where the ECG and echocardiogram raise the suspicion of DCM, CMR may provide valuable insights, including an accurate assessment of LV volumes and the possible presence of mid-wall fibrosis, a feature that, if present, corroborates the diagnosis of DCM in the appropriate context.70 Moreover, ambulatory ECG monitoring, exercise stress echocardiogram and CPET may be helpful in the differential diagnosis. For instance, failure to augment cardiac output during exercise in athletes falling in the ‘grey zone’ (mild impairment of LV systolic function and significant LV dilatation at baseline echocardiography) is a red flag for DCM.71,72 Other features may suggest a pathological rather than physiological entity in this context, including high premature ventricular contractions (PVCs) burden (>2,000 per 24 hours) at ambulatory ECG monitoring, and propensity to develop frequent PVCs or non-sustained ventricular tachycardia (NSVT) during exercise tolerance test (ETT).73–76
Differential diagnosis with ACM
Arrhythmogenic cardiomyopathy is an inherited condition, reportedly affecting one in 1,000 of the general population.35 The disease is generally caused by mutations in genes encoding cardiac desmosomal proteins, with pathogenic or likely pathogenic variants identified in up to 60% of patients with a diagnosis of ACM.63,77 Although the initial description of the disease suggested an exclusive involvement of the RV, recent studies showed that the LV is involved in the majority of patients.78 The diagnosis of ACM is complex and traditionally based on the task force criteria (TFC), which include a series of clinical, ECG and structural/functional traits.79 The more recently proposed Padua criteria and the revised European task force consensus criteria also take into account myocardial abnormalities within the LV, such as, for example, mid-wall and subepicardial fibrosis at CMR.80,81 The disease hallmark is the replacement of healthy myocardium with fibrofatty tissue and a predilection for fatal arrhythmias, especially during exercise.5,82 Intensive exercise is thought to result in myocyte detachment with subsequent inflammation and abnormal repair, resulting in progressive fibrofatty replacement of the ventricular myocardium in predisposed individuals.83 SCD and progressive ventricular systolic dysfunction are the most feared complications.78
Electrocardiogram
The ECG is abnormal in ACM in up to 80% of cases. The most common ECG abnormality is anterior TWI, which is present in up to 50% of patients.81 This feature may be physiological in healthy athletes, especially young and of African or Afro-Caribbean descent.18 Certain features may suggest a pathological substrate in athletes with anterior TWI. These include ‘isoelectric or downward shift’ of J-point and ST-segment in V1–V3, low voltages in the limb and/or precordial leads, QRS duration ratio V2:V5 >1.2, S-wave prolongation in V1–V2 (>55 ms), multiple PVCs, and combination with TWI in the inferior and lateral leads.84 In contrast, in healthy athletes, anterior TWI is often accompanied by a J-point elevation of at least 1 mm.3 Patterns of PVCs may also be helpful in the differential diagnosis between ‘athlete’s heart’ and ACM. While PVCs originating from RV outflow tract are common in athletes and often disappear during exercise at the ETT, a RBBB pattern and superior axis with wide QRS may be a sign of ACM.85,86 Another typical ECG finding in ACM is the presence of an epsilon wave, defined as a small positive deflection or notch between the end of the QRS complex and onset of the T-wave in leads V1–V3.81 An epsilon wave is found in 8–10% of patients with ACM, being highly specific and poorly sensitive.87
Echocardiogram
During exercise, the RV is subjected to significant wall stress, adapting to an increased preload. Athletes, especially the ones engaged in endurance exercise, often exhibit RV dilatation.29,30 Conventionally, echocardiography has a poor sensitivity for discriminating ACM from athlete’s heart due to the shortfall of a tri-dimensional view and lower spatial resolution in comparison to CMR.88 RV systolic dysfunction (RV fractional area change [FAC] <32%) with or without regional wall motion abnormalities in an athlete favours a diagnosis of ACM.32,89
Further investigations
When ACM is suspected, further investigations are warranted. CMR is the gold standard for the assessment of the RV and specifically to differentiate between normal and pathological findings.90 RV enlargement in athletes is usually accompanied by concomitant LV remodelling, reflecting a symmetrical adaptation of the heart to the haemodynamic changes induced by training.31 Regional wall motion abnormalities, such as dyskinesia, akinesia and aneurysms, as well as an RV/LV end-diastolic volumes ratio >1.2 and an impaired RV systolic function (RVEF ≤45%), are features that support ACM.33,34 Moreover, subepicardial and/or mid-wall LGE may corroborate the diagnosis.70 Other tests, such as ambulatory ECG monitoring and ETT can be helpful in the differential diagnosis. The presence of ventricular arrhythmias, such as a high burden of PVCs (>500 per 24 hours) and NSVT at ambulatory ECG monitoring are features that may point toward a diagnosis of ACM in the appropriate clinical context.33 In those with suspected ACM, ETT may reveal susceptibility to ventricular arrhythmias (either increased PVCs burden or NSVT) during exercise.33,91
Conclusion
Differential diagnosis between physiological cardiac adaptation to exercise in athletes and cardiomyopathies is often challenging. A comprehensive approach, integrating family and personal history, ECG, advanced imaging, and, in some cases, genetic testing, is essential to ensure an appropriate management of possible dilemmas. A deep understanding of the determinants of cardiovascular adaptation in athletes, including type and intensity of exercise, age, sex, and ethnicity is a first step to distinguish between physiological and pathological findings. A learned interpretation of the ECG and knowledge of the value of second-line cardiac investigations, such as echocardiogram, CMR, ETT and ambulatory ECG monitoring, is crucial to identify red flags that may lead to the correct diagnosis.
Key messages
- Intense exercise may result in a series of physiological electrical, structural and functional cardiac changes, which may mimic serious cardiac conditions, such as cardiomyopathies
- Differentiation between physiological adaptation to exercise and pathological findings suggestive of a cardiomyopathy is often challenging
- Differential diagnosis is crucial in this setting and usually requires a systematic approach, which starts from an accurate collection of personal and family history and electrocardiogram (ECG), with further tests dictated by the results of these
- Knowledge of determinants of physiological cardiac adaptation and of normal findings in athletes is key to distinguish them from pathological signs that raise the suspicion of an underlying cardiac disease
Conflicts of interest
None declared.
Funding
None.
Editors’ note
This is the first article in a series on sports cardiology.
References
1. Mills JD, Moore GE, Thompson PD. The athlete’s heart. Clin Sports Med 1997;16:725–37. https://doi.org/10.1016/S0278-5919(05)70050-8
2. Flanagan H, Cooper R, George KP et al. The athlete’s heart: insights from echocardiography. Echo Res Pract 2023;10:15. https://doi.org/10.1186/s44156-023-00027-8
3. Drezner JA, Sharma S, Baggish A et al. International criteria for electrocardiographic interpretation in athletes: consensus statement. Br J Sports Med 2017;51:704–31. https://doi.org/10.1136/bjsports-2016-097331
4. Pelliccia A, Maron BJ, Spataro A, Proschan MA, Spirito P. The upper limit of physiologic cardiac hypertrophy in highly trained elite athletes. N Engl J Med 1991;324:295–301. https://doi.org/10.1056/NEJM199101313240504
5. Corrado D, Basso C, Rizzoli G et al. Does sports activity enhance the risk of sudden death in adolescents and young adults? J Am Coll Cardiol 2003;42:1959–63. https://doi.org/10.1016/j.jacc.2003.03.002
6. Maron BJ, Doerer JJ, Haas TS et al. Sudden deaths in young competitive athletes – analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009;119:1085–92. https://doi.org/10.1161/CIRCULATIONAHA.108.804617
7. Finocchiaro G, Westaby J, Bhatia R et al. Sudden death in female athletes: insights from a large regional registry in the United Kingdom. Circulation 2021;144:1827–9. https://doi.org/10.1161/CIRCULATIONAHA.121.055535
8. Finocchiaro G, Radaelli D, D’Errico S et al. Sudden cardiac death among adolescents in the United Kingdom. J Am Coll Cardiol 2023;81:1007–17. https://doi.org/10.1016/j.jacc.2023.01.041
9. Petek BJ, Churchill TW, Moulson N et al. Sudden cardiac death in National Collegiate Athletic Association athletes: a 20-year study. Circulation 2024;149:80–90. https://doi.org/10.1161/CIRCULATIONAHA.123.065908
10. Finocchiaro G, Westaby J, Sheppard MN et al. Sudden cardiac death in young athletes: JACC state-of-the-art review. J Am Coll Cardiol 2024;83:350–70. https://doi.org/10.1016/j.jacc.2023.10.032
11. Dhutia H, Malhotra A, Finocchiaro G et al. Impact of the international recommendations for electrocardiographic interpretation on cardiovascular screening in young athletes. J Am Coll Cardiol 2017;70:805–07. https://doi.org/10.1016/j.jacc.2017.06.017
12. Dhutia H, Malhotra A, Finocchiaro G et al. Diagnostic yield and financial implications of a nationwide electrocardiographic screening programme to detect cardiac disease in the young. Europace 2021;23:1295–301. https://doi.org/10.1093/europace/euab021
13. Zaidi A, Ghani S, Sheikh N et al. Clinical significance of electrocardiographic right ventricular hypertrophy in athletes: comparison with arrhythmogenic right ventricular cardiomyopathy and pulmonary hypertension. Eur Heart J 2013;34:3649–56. https://doi.org/10.1093/eurheartj/eht458
14. Kim JH, Noseworthy PA, McCarty D et al. Significance of electrocardiographic right bundle branch block in trained athletes. Am J Cardiol 2011;107:1083–9. https://doi.org/10.1016/j.amjcard.2010.11.037
15. Noseworthy PA, Weiner R, Kim J et al. Early repolarization pattern in competitive athletes: clinical correlates and the effects of exercise training. Circ Arrhythm Electrophysiol 2011;4:432–40. https://doi.org/10.1161/CIRCEP.111.962852
16. Brosnan M, La Gerche A, Kalman J et al. Comparison of frequency of significant electrocardiographic abnormalities in endurance versus nonendurance athletes. Am J Cardiol 2014;113:1567–73. https://doi.org/10.1016/j.amjcard.2014.01.438
17. Pelliccia A, Quattrini FM. Clinical significance of J-wave in elite athletes. J Electrocardiol 2015;48:385–9. https://doi.org/10.1016/j.jelectrocard.2015.03.012
18. Papadakis M, Carre F, Kervio G et al. The prevalence, distribution, and clinical outcomes of electrocardiographic repolarization patterns in male athletes of African/Afro-Caribbean origin. Eur Heart J 2011;32:2304–13. https://doi.org/10.1093/eurheartj/ehr140
19. Milman A, Keren G. Diagnostic and clinical significance of T wave inversion in athletes. Isr Med Assoc J 2018;20:114–18. Available from: https://www.ima.org.il/MedicineIMAJ/viewarticle.aspx?year=2018&month=02&page=114
20. Martinez MW, Kim JH, Shah AB et al. Exercise-induced cardiovascular adaptations and approach to exercise and cardiovascular disease: JACC state-of-the-art review. J Am Coll Cardiol 2021;78:1453–70. https://doi.org/10.1016/j.jacc.2021.08.003
21. Abergel E, Chatellier G, Hagege AA et al. Serial left ventricular adaptations in world-class professional cyclists: implications for disease screening and follow-up. J Am Coll Cardiol 2004;44:144–9. https://doi.org/10.1016/j.jacc.2004.02.057
22. Pelliccia A, Culasso F, Di Paolo FM et al. Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med 1999;130:23–31. https://doi.org/10.7326/0003-4819-130-1-199901050-00005
23. Pelliccia A, Maron BJ, Culasso F et al. Athlete’s heart in women – echocardiographic characterization of highly trained elite female athletes. JAMA Cardiol 1996;276:211–15. https://doi.org/10.1001/jama.276.3.211
24. Makan J, Sharma S, Firoozi S et al. Physiological upper limits of ventricular cavity size in highly trained adolescent athletes. Heart 2005;91:495–9. https://doi.org/10.1136/hrt.2004.035121
25. Rawlins J, Carre F, Kervio G et al. Ethnic differences in physiological cardiac adaptation to intense physical exercise in highly trained female athletes. Circulation 2010;121:1078–85. https://doi.org/10.1161/CIRCULATIONAHA.109.917211
26. Colombo CSSS, Finocchiaro G. The female athlete’s heart: facts and fallacies. Curr Treat Options Cardiovasc Med 2018;20:101. https://doi.org/10.1007/s11936-018-0699-7
27. Finocchiaro G, Dhutia H, D’Silva A et al. Effect of sex and sporting discipline on LV adaptation to exercise. JACC Cardiovasc Imaging 2017;10:965–72. https://doi.org/10.1016/j.jcmg.2016.08.011
28. Sharma S, Maron BJ, Whyte G et al. Physiologic limits of left ventricular hypertrophy in elite junior athletes: relevance to differential diagnosis of athlete’s heart and hypertrophic cardiomyopathy. J Am Coll Cardiol 2002;40:1431–6. https://doi.org/10.1016/S0735-1097(02)02270-2
29. D’Ascenzi F, Pelliccia A, Corrado D et al. Right ventricular remodelling induced by exercise training in competitive athletes. Eur Heart J Cardiovasc Imaging 2016;17:301–07. https://doi.org/10.1093/ehjci/jev155
30. D’Ascenzi F, Pisicchio C, Caselli S et al. RV remodeling in Olympic athletes. JACC Cardiovasc Imaging 2017;10:385–93. https://doi.org/10.1016/j.jcmg.2016.03.017
31. Bauce B, Frigo G, Benini G et al. Differences and similarities between arrhythmogenic right ventricular cardiomyopathy and athlete’s heart adaptations. Br J Sports Med 2010;44:148–54. https://doi.org/10.1136/bjsm.2007.042853
32. D’Ascenzi F, Solari M, Corrado D et al. Diagnostic differentiation between arrhythmogenic cardiomyopathy and athlete’s heart by using imaging. JACC Cardiovasc Imaging 2018;11:1327–39. https://doi.org/10.1016/j.jcmg.2018.04.031
33. Zaidi A, Sheikh N, Jongman JK et al. Clinical differentiation between physiological remodeling and arrhythmogenic right ventricular cardiomyopathy in athletes with marked electrocardiographic repolarization anomalies. J Am Coll Cardiol 2015;65:2702–11. https://doi.org/10.1016/j.jacc.2015.04.035
34. Moccia E, Papatheodorou E, Miles CJ et al. Arrhythmogenic cardiomyopathy and differential diagnosis with physiological right ventricular remodelling in athletes using cardiovascular magnetic resonance. Int J Cardiovasc Imaging 2022;38:2723–32. https://doi.org/10.1007/s10554-022-02684-y
35. Arbelo E, Protonotarios A, Gimeno JR et al. ESC guidelines for the management of cardiomyopathies: developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur Heart J 2023;44:3503–626. https://doi.org/10.1093/eurheartj/ehad194
36. Thiene G, Corrado D, Basso C. Revisiting definition and classification of cardiomyopathies in the era of molecular medicine. Eur Heart J 2008;29:144–6. https://doi.org/10.1093/eurheartj/ehm585
37. Brosnan M, Rakhit D. Differentiating athlete’s heart from cardiomyopathies – the left side. Heart Lung Circ 2018;27:1052–62. https://doi.org/10.1016/j.hlc.2018.04.297
38. Prior D. Differentiating athlete’s heart from cardiomyopathies – the right side. Heart Lung Circ 2018;27:1063–71. https://doi.org/10.1016/j.hlc.2018.04.300
39. Maron BJ, Pelliccia A, Spirito P. Cardiac disease in young trained athletes: insights into methods for distinguishing athlete’s heart from structural heart disease, with particular emphasis on hypertrophic cardiomyopathy. Circulation 1995;91:1596–601. https://doi.org/10.1161/01.CIR.91.5.1596
40. Maron BJ, Maron MS. Hypertrophic cardiomyopathy. Lancet 2013;381:242–55. https://doi.org/10.1016/S0140-6736(12)60397-3
41. Finocchiaro G, Papadakis M, Tanzarella G et al. Sudden death can be the first manifestation of hypertrophic cardiomyopathy: data from a United Kingdom pathology registry. JACC Clin Electrophysiol 2019;5:252–4. https://doi.org/10.1016/j.jacep.2018.11.004
42. Finocchiaro G, Bhatia RT, Westaby J et al. Sudden cardiac death during exercise in young individuals with hypertrophic cardiomyopathy. JACC Clin Electrophysiol 2023;9:865–7. https://doi.org/10.1016/j.jacep.2022.12.007
43. O’Mahony C, Jichi F, Pavlou M et al. A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM Risk-SCD). Eur Heart J 2014;35:2010–20. https://doi.org/10.1093/eurheartj/eht439
44. Sheikh N, Papadakis M, Ghani S et al. Comparison of electrocardiographic criteria for the detection of cardiac abnormalities in elite black and white athletes. Circulation 2014;129:1637–49. https://doi.org/10.1161/CIRCULATIONAHA.113.006179
45. Lakdawala NK, Thune JJ, Maron BJ et al. Electrocardiographic features of sarcomere mutation carriers with and without clinically overt hypertrophic cardiomyopathy. Am J Cardiol 2011;108:1606–13. https://doi.org/10.1016/j.amjcard.2011.07.019
46. Bent RE, Wheeler MT, Hadley D et al. Computerized Q wave dimensions in athletes and hypertrophic cardiomyopathy patients. J Electrocardiol 2015;48:362–7. https://doi.org/10.1016/j.jelectrocard.2015.01.009
47. Bent RE, Wheeler MT, Hadley D et al. Systematic comparison of digital electrocardiograms from healthy athletes and patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 2015;65:2462–3. https://doi.org/10.1016/j.jacc.2015.03.559
48. Basu J, Finocchiaro G, Miles C et al. The effect of ethnicity on left ventricular adaptation to exercise. Eur J Prev Cardiol 2023;30:E69–E71. https://doi.org/10.1093/eurjpc/zwad126
49. Sheikh N, Papadakis M, Schnell F et al. Clinical profile of athletes with hypertrophic cardiomyopathy. Circ Cardiovasc Imaging 2015;8:e003454. https://doi.org/10.1161/CIRCIMAGING.114.003454
50. Abulí M, de la Garza MS, Sitges M. Differentiating athlete’s heart from left ventricle cardiomyopathies. J Cardiovasc Transl Res 2020;13:265–73. https://doi.org/10.1007/s12265-020-10021-8
51. Finocchiaro G, Dhutia H, D’Silva A et al. Role of Doppler diastolic parameters in differentiating physiological left ventricular hypertrophy from hypertrophic cardiomyopathy. J Am Soc Echocardiogr 2018;31:606.e1–613.e1. https://doi.org/10.1016/j.echo.2017.11.022
52. Moon JCC, Fisher NG, McKenna WJ et al. Detection of apical hypertrophic cardiomyopathy by cardiovascular magnetic resonance in patients with non-diagnostic echocardiography. Heart 2004;90:645–9. https://doi.org/10.1136/hrt.2003.014969
53. Hughes RK, Shiwani H, Rosmini S et al. Improved diagnostic criteria for apical hypertrophic cardiomyopathy. JACC Cardiovasc Imaging 2024;17:501–12. https://doi.org/10.1016/j.jcmg.2023.07.012
54. Maron MS, Maron BJ, Harrigan C et al. Hypertrophic cardiomyopathy phenotype revisited after 50 years with cardiovascular magnetic resonance. J Am Coll Cardiol 2009;54:220–8. https://doi.org/10.1016/j.jacc.2009.05.006
55. Harrigan CJ, Appelbaum E, Maron BJ et al. Significance of papillary muscle abnormalities identified by cardiovascular magnetic resonance in hypertrophic cardiomyopathy. Am J Cardiol 2008;101:668–73. https://doi.org/10.1016/j.amjcard.2007.10.032
56. Goyal N, Keir G, Esterson YB et al. Hypertrophic cardiomyopathy – phenotypic variations beyond wall thickness. Clin Imaging 2023;95:80–9. https://doi.org/10.1016/j.clinimag.2023.01.003
57. Maron MS. The current and emerging role of cardiovascular magnetic resonance imaging in hypertrophic cardiomyopathy. J Cardiovasc Transl Res 2009;2:415–25. https://doi.org/10.1007/s12265-009-9136-3
58. Puntmann VO, Voigt T, Chen Z et al. Native T1 mapping in differentiation of normal myocardium from diffuse disease in hypertrophic and dilated cardiomyopathy. JACC Cardiovasc Imaging 2013;6:475–84. https://doi.org/10.1016/j.jcmg.2012.08.019
59. Swoboda PP, McDiarmid AK, Erhayiem B et al. Assessing myocardial extracellular volume by T1 mapping to distinguish hypertrophic cardiomyopathy from athlete’s heart. J Am Coll Cardiol 2016;67:2189–90. https://doi.org/10.1016/j.jacc.2016.02.054
60. Finocchiaro G, Sheikh N, Leone O et al. Arrhythmogenic potential of myocardial disarray in hypertrophic cardiomyopathy: genetic basis, functional consequences and relation to sudden cardiac death. Europace 2021;23:985–95. https://doi.org/10.1093/europace/euaa348
61. Sharma S, Elliott PM, Whyte G et al. Utility of metabolic exercise testing in distinguishing hypertrophic cardiomyopathy from physiologic left ventricular hypertrophy in athletes. J Am Coll Cardiol 2000;36:864–70. https://doi.org/10.1016/S0735-1097(00)00816-0
62. Boraita A, Heras M-E, Valenzuela PL et al. Holter-determined arrhythmias in young elite athletes with suspected risk: insights from a 20-year experience. Front Cardiovasc Med 2022;9:896148. https://doi.org/10.3389/fcvm.2022.896148
63. Charron P, Arad M, Arbustini E et al. Genetic counselling and testing in cardiomyopathies: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2010;31:2715–28. https://doi.org/10.1093/eurheartj/ehq271
64. Ackerman MJ, Priori SG, Willems S et al. HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies: this document was developed as a partnership between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA). Heart Rhythm 2011;8:1308–39. https://doi.org/10.1016/j.hrthm.2011.05.020
65. Sheikh N, Papadakis M, Wilson M et al. Diagnostic yield of genetic testing in young athletes with T-wave inversion. Circulation 2018;138:1184–94. https://doi.org/10.1161/CIRCULATIONAHA.118.034208
66. Zaffalon D, Papatheodorou E, Merghani A et al. Role of the electrocardiogram in differentiating genetically determined dilated cardiomyopathy from athlete’s heart. Eur J Clin Invest 2022;52:e13837. https://doi.org/10.1111/eci.13837
67. Finocchiaro G, Merlo M, Sheikh N et al. The electrocardiogram in the diagnosis and management of patients with dilated cardiomyopathy. Eur J Heart Fail 2020;22:1097–107. https://doi.org/10.1002/ejhf.1815
68. Mestroni L, Maisch B, Mckenna WJ et al. Guidelines for the study of familial dilated cardiomyopathies. Eur Heart J 1999;20:93–102. https://doi.org/10.1053/euhj.1998.1145
69. Claessen G, De Bosscher R, Janssens K et al. Reduced ejection fraction in elite endurance athletes: clinical and genetic overlap with dilated cardiomyopathy. Circulation 2024;149:1405–15. https://doi.org/10.1161/CIRCULATIONAHA.122.063777
70. Meier C, Eisenblätter M, Gielen S. Myocardial late gadolinium enhancement (LGE) in cardiac magnetic resonance imaging (CMR) – an important risk marker for cardiac disease. J Cardiovasc Dev Dis 2024;11:40. https://doi.org/10.3390/jcdd11020040
71. Claessen G, Schnell F, Bogaert J et al. Exercise cardiac magnetic resonance to differentiate athlete’s heart from structural heart disease. Eur Heart J Cardiovasc Imaging 2018;19:1062–70. https://doi.org/10.1093/ehjci/jey050
72. Millar LM, Fanton Z, Finocchiaro G et al. Differentiation between athlete’s heart and dilated cardiomyopathy in athletic individuals. Heart 2020;106:1059–65. https://doi.org/10.1136/heartjnl-2019-316147
73. Biffi A, Pelliccia A, Verdile L et al. Long-term clinical significance of frequent and complex ventricular tachyarrhythmias in trained athletes. J Am Coll Cardiol 2002;40:446–52. https://doi.org/10.1016/S0735-1097(02)01977-0
74. Cipriani A, Zorzi A, Sarto P et al. Predictive value of exercise testing in athletes with ventricular ectopy evaluated by cardiac magnetic resonance. Heart Rhythm 2019;16:239–48. https://doi.org/10.1016/j.hrthm.2018.08.029
75. Volpato G, Falanga U, Cipolletta L et al. Sports activity and arrhythmic risk in cardiomyopathies and channelopathies: a critical review of European guidelines on sports cardiology in patients with cardiovascular diseases. Medicina (Kaunas) 2021;57:308. https://doi.org/10.3390/medicina57040308
76. Lampert R, Chung EH, Ackerman MJ et al. 2024 HRS expert consensus statement on arrhythmias in the athlete: evaluation, treatment, and return to play. Heart Rhythm 2024;21:e151–e252. https://doi.org/10.1016/j.hrthm.2024.05.018
77. Groeneweg JA, Bhonsale A, James CA et al. Clinical presentation, long-term follow-up, and outcomes of 1001 arrhythmogenic right ventricular dysplasia/cardiomyopathy patients and family members. Circ Cardiovasc Genet 2015;8:437–46. https://doi.org/10.1161/CIRCGENETICS.114.001003
78. Miles C, Finocchiaro G, Papadakis M et al. Sudden death and left ventricular involvement in arrhythmogenic cardiomyopathy. Circulation 2019;139:1786–97. https://doi.org/10.1161/CIRCULATIONAHA.118.037230
79. Marcus FI, McKenna WJ, Sherrill D et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the task force criteria. Circulation 2010;121:1533–41. https://doi.org/10.1161/CIRCULATIONAHA.108.840827
80. Corrado D, Perazzolo Marra M, Zorzi A et al. Diagnosis of arrhythmogenic cardiomyopathy: the Padua criteria. Int J Cardiol 2020;319:106–14. https://doi.org/10.1016/j.ijcard.2020.06.005
81. Corrado D, Anastasakis A, Basso C et al. Proposed diagnostic criteria for arrhythmogenic cardiomyopathy: European Task Force consensus report. Int J Cardiol 2024;395:131447. https://doi.org/10.1016/j.ijcard.2023.131447
82. Corrado D, Basso C, Judge DP. Arrhythmogenic cardiomyopathy. Circ Res 2017;121:785–802. https://doi.org/10.1161/CIRCRESAHA.117.309345
83. Meraviglia V, Alcalde M, Campuzano O et al. Inflammation in the pathogenesis of arrhythmogenic cardiomyopathy: secondary event or active driver? Front Cardiovasc Med 2021;8:784715. https://doi.org/10.3389/fcvm.2021.784715
84. Finocchiaro G, Papadakis M, Dhutia H et al. Electrocardiographic differentiation between ‘benign T-wave inversion’ and arrhythmogenic right ventricular cardiomyopathy. Europace 2019;21:332–8. https://doi.org/10.1093/europace/euy179
85. Calò L, Panattoni G, Tatangelo M et al. Electrocardiographic characteristics of right-bundle-branch-block premature ventricular complexes predicting absence of left ventricular scar in athletes with apparently structural normal heart. Europace 2023;25:euad217. https://doi.org/10.1093/europace/euad217
86. Laredo M, Tovia-Brodie O, Milman A et al. Electrocardiographic findings in patients with arrhythmogenic cardiomyopathy and right bundle branch block ventricular tachycardia. Europace 2023;25:1025–34. https://doi.org/10.1093/europace/euac267
87. Pérez-Riera AR, Barbosa-Barros R, Daminello-Raimundo R et al. Epsilon wave: a review of historical aspects. Indian Pacing Electrophysiol J 2019;19:63–7. https://doi.org/10.1016/j.ipej.2019.02.003
88. Zholshybek N, Khamitova Z, Toktarbay B et al. Cardiac imaging in athlete’s heart: current status and future prospects. Cardiovasc Ultrasound 2023;21:21. https://doi.org/10.1186/s12947-023-00319-3
89. D’Ascenzi F, Pelliccia A, Solari M et al. Normative reference values of right heart in competitive athletes: a systematic review and meta-analysis. J Am Soc Echocardiogr 2017;30:845–58. https://doi.org/10.1016/j.echo.2017.06.013
90. Galea N, Carbone I, Cannata D et al. Right ventricular cardiovascular magnetic resonance imaging: normal anatomy and spectrum of pathological findings. Insights Imaging 2013;4:213–23. https://doi.org/10.1007/s13244-013-0222-3
91. Finocchiaro G, Barra B, Molaro S et al. Prevalence and clinical correlates of exercise-induced ventricular arrhythmias in arrhythmogenic right ventricular cardiomyopathy. Int J Cardiovasc Imaging 2022;38:389–96. https://doi.org/10.1007/s10554-021-02395-w
