A coronary artery fistula (CAF) is an abnormal connection between a coronary artery and another structure. This rare condition has an incidence in the general population of 0.002%. A 57-year-old woman presented with angina, a normal electrocardiogram (ECG) and a peak troponin I of 0.22 µg/L (normal <0.04 µg/L). She was treated with a standard medical regimen for non-ST-elevation myocardial infarction. Coronary angiography revealed non-obstructed coronary arteries, with fistulae arising from the left anterior descending, left circumflex and right coronary arteries, all terminating in the pulmonary artery. Cardiac magnetic resonance (CMR) imaging was performed to investigate coronary steal syndrome. This confirmed there was no significant shunt or evidence of infarction. There was a small concentric pericardial effusion with a focal region of inferolateral epicardial fibrosis, suggesting a diagnosis of myopericarditis. The patient was treated with colchicine for three months.
CAF can cause patients to present with a variety of symptoms or potentially life-threatening complications, including fistula rupture and myocardial infarction. Early recognition, characterisation and shunt analysis are imperative to facilitate management. Although left/right heart catheterisation is considered the gold standard, CMR proved to be a useful diagnostic tool in our case, ruling out significant shunting and helping to identify a differential diagnosis.
Background
A coronary artery fistula (CAF) is an abnormal connection between a coronary artery and another blood vessel or heart chamber. There is a reported incidence of 0.002% in the general population,1,2 and up to 0.2% in angiographic series.1,3 CAF account for less than 1% of all congenital cardiac anomalies.1 Multiple bilateral coronary fistulae are even less common. We describe a rare case of three CAF, arising from each of the major vessels, and the management approach adopted.
Case
 |
 |
 |
A 57-year-old woman presented with angina. Her electrocardiogram (ECG) showed normal sinus rhythm without ischaemic changes. Initial troponin I was 0.01 µg/L (normal <0.04 µg/L) then rose to 0.22 µg/L on a repeat sample. Apart from a smoking history, she had no risk factors for coronary artery disease. She was initially treated with a standard medical regimen for non-ST- elevation myocardial infarction (NSTEMI).
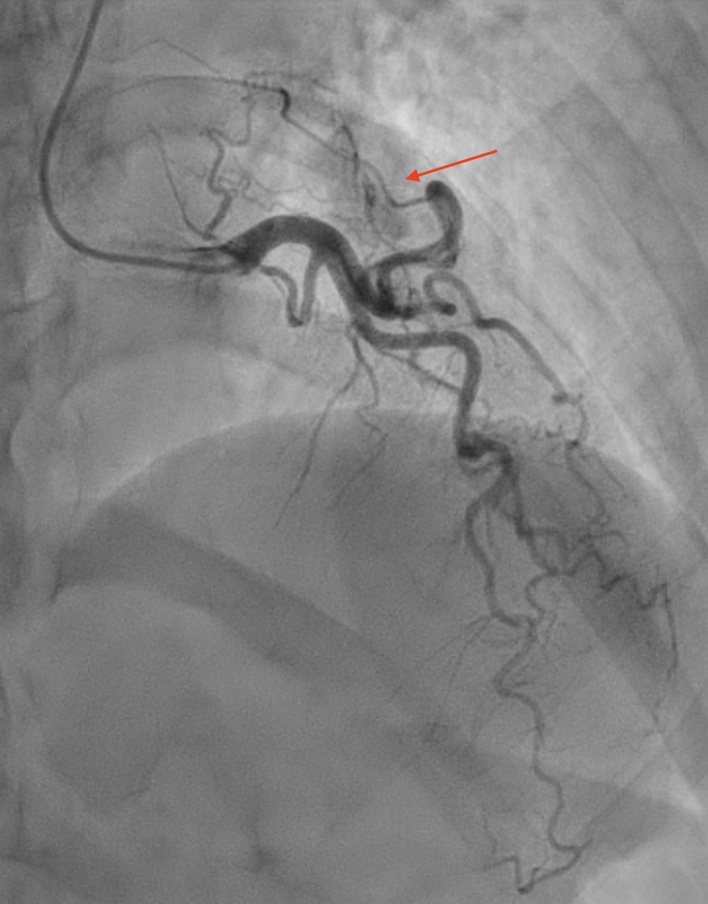
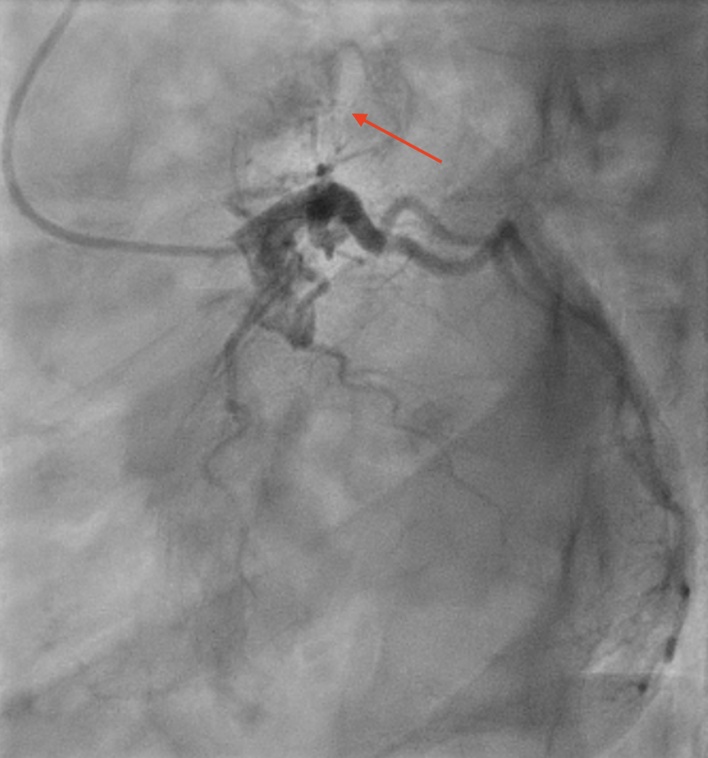
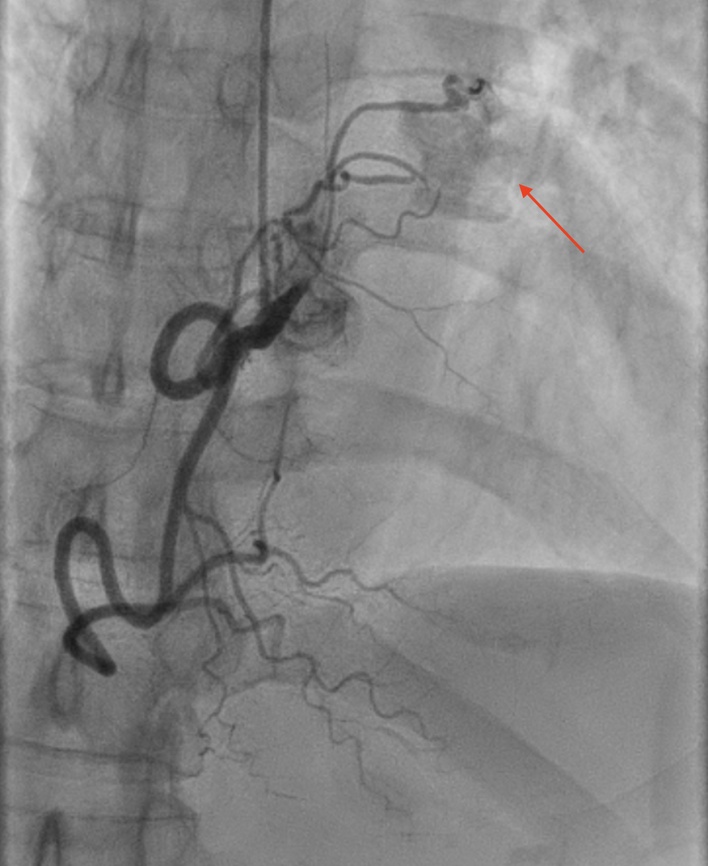
Coronary angiography showed very tortuous coronary arteries with three fistulae from the left anterior descending, left circumflex and right coronary arteries, all terminating in the pulmonary artery (figures 1–3). There was no evidence of obstructive coronary artery disease. Initial presumed diagnosis was myocardial infarction due to coronary steal syndrome. Cardiac magnetic resonance (CMR) imaging was performed. A standard protocol of white blood and cine image sequences with late gadolinium enhancement was used. Shunt assessment via formal volumetric analysis and flow analysis through the valves was performed. True forward stroke volume through the aortic valve was 99 ml/beat with a peak gradient across the valve of 8 mmHg and a regurgitant fraction of 1%. True forward flow through the pulmonary valve was 102 ml/beat. This confirmed that there was no significant shunt. Normal biventricular size and function, with no prior infarction, was also demonstrated. There was a small concentric pericardial effusion with a focal region of inferolateral epicardial fibrosis, suggesting a diagnosis of myopericarditis. The patient was treated with regular colchicine for three months, and ibuprofen, as required. Her troponin and symptoms settled and she was discharged.
Discussion
Typically CAF are singular and unilateral, arising most commonly from the right coronary artery (60%).4 The majority drain into right-sided heart structures, including heart chambers, pulmonary trunk and coronary sinus.4,5 While CAF are mostly congenital in origin, they can rarely be acquired as a consequence of coronary artery catheterisation.6 Hackensellner’s involution persistence theory has been proposed as the embryological basis for coronary–pulmonary fistulae.7 The truncus arteriosus is a single vessel that originates from the embryonic heart, which subsequently gives rise to six anlages, and forms the aortic and pulmonary arteries. Normally, only two of the six anlages persist, arising from the aortic sinuses to form the left and right coronary arteries. The other four, usually originating from the pulmonary sinus, are expected to degrade. If one of these four anlages fail to involute, they may persist and connect with the aortic sinuses, resulting in abnormal fistulous communications.
It is important to note that CAF are rare abnormalities and result in no clinical sequelae in the vast majority of cases; despite that, some patients can present with a diversity of symptoms.4 Angina has been reported in up to a quarter of patients with CAF without obstructive coronary artery disease.4 Symptoms are caused by shunts across these fistulae resulting in a coronary steal syndrome. CAF can also be associated with life-threatening complications, including fistula rupture, myocardial infarction and congestive cardiac failure, although the risk of these complications is very low.5
In our case, CMR proved a useful diagnostic tool. Shunt calculations were performed using two robust assessments of Qp:Qs, ruling out steal syndrome. CMR has been used to characterise CAF for many decades now, but appears to be less frequently reported as the diagnostic tool chosen.8 Compared with other diagnostic tools used for assessment of CAF, CMR offers many benefits; it is non-invasive and avoids the need for large doses of nephrotoxic contrast used in computed tomography. Furthermore, this imaging modality is useful for ruling out infarction and identifying other potential diagnoses and/or associated cardiac anomalies. While left and right heart catheterisation may be considered the gold standard for pressure analysis and shunt calculations, CMR provided a thorough assessment of the fistulae and helped identify an alternative diagnosis in our case.
Management of CAF is a contentious and controversial topic. Apart from the heterogeneity of fistula morphology and patient presentation, there is no high level evidence supporting management recommendations. Treatment options include conservative management, transcatheter procedures and surgical closure. A paper by Al-Hijji et al. proposed treatment indications and management algorithms.6 While small CAF tend to close spontaneously and are better managed conservatively, larger CAFs are at risk of dilatation and closure should be considered in the presence of attributable symptoms, complications or cardiac remodelling.6 Percutaneous treatment options include delivery of embolisation coils, vascular occluding plugs and covered stents. There are various considerations to be taken into account with these options, not least the associated complications of invasive procedures and the need for antiplatelet therapy when using stents. Consequently, decision-making in this area can be challenging.
Conclusion
Multiple CAF is a rare congenital cardiac anomaly with limited data. CMR can prove to be a useful diagnostic tool in this clinical context.
Conflicts of interest
None declared.
Funding
None.
Patient consent
Informed consent was obtained from the patient for the publication of this case.
Editors’ note
Videos of the CAF are available on request from the authors.
References
1. De Roeck F, Franssen C, De Wolf D, Haine S. Exercise-induced ventricular arrhythmia due to bilateral coronary to pulmonary artery fistulas. Catheter Cardiovas Interv 2019;94:112–16. https://doi.org/10.1002/ccd.28108
2. Yildiz A, Okcun B, Peker T, Arslan C, Olcay A, Bulent Vatan M. Prevalence of coronary artery anomalies in 12,457 adult patients who underwent coronary angiography. Clin Cardiol 2010;33:E60–E64. https://doi.org/10.1002/clc.20588
3. Vaidyanathan KR, Theodore SAC, Sankar MN, Cherian KM. Coronary artery to pulmonary artery fistula with dual origin – embryological, clinical and surgical significance. Eur J Cardiothorac Surg 2007;31:318–19. https://doi.org/10.1016/j.ejcts.2006.11.018
4. Said SAM, van der Werf T. Dutch survey of coronary artery fistulas in adults: congenital solitary fistulas. Int J Cardiol 2006;106:323–32. https://doi.org/10.1016/j.ijcard.2005.01.047
5. Shyam Sunder KR, Balakrishnan KG, Tharakan JA et al. Coronary artery fistula in children and adults: a review of 25 cases with long-term observations. Int J Cardiol 1997;58:47–53. https://doi.org/10.1016/S0167-5273(96)02792-1
6. Al-Hijji M, Sabbagh AE, Hajj SE et al. Coronary artery fistulas. JACC Cardiovasc Interv 2021;14:1393–406. https://doi.org/10.1016/j.jcin.2021.02.044
7. Heifetz SA, Robinowitz M, Mueller KH, Virmani R. Total anomalous origin of the coronary arteries from the pulmonary artery. Pediatr Cardiol 1986;7:11–18. https://doi.org/10.1007/BF02315476
8. Rathi VK, Mikolich B, Patel M, Doyle M, Yamrozik J, Biederman RW. Coronary artery fistula; non-invasive diagnosis by cardiovascular magnetic resonance imaging. J Cardiovasc Magn Reson 2005;7:723–5. https://doi.org/10.1081/JCMR-200065643
