National Institute for Health and Care Excellence (NICE) guidance recommends routine early inpatient invasive coronary angiography (ICA) for patients presenting with non-ST-elevation acute myocardial infarction acute coronary syndrome (NSTEMI-ACS) within 72 hours of hospital admission. For patients admitted to hospitals without invasive cardiac facilities, completing interhospital transfer and investigation within this timeframe is challenging. This retrospective cohort study evaluated factors influencing time to ICA, diagnosis and treatment allocation decisions in 4,087 NSTEMI-ACS patients referred from five district general hospitals to the Royal Infirmary of Edinburgh over four years. The mean time from admission to coronary angiography was 5.0 ± 3.0 days, with the majority waiting longer than the 72-hour NICE target. Admission towards the end of the week, defined as Wednesday to Saturday, was associated with longer delay. Coronary revascularisation was not required in 34% of patients. The presence of obstructive coronary disease and use of coronary revascularisation varied with age and sex, with younger female patients more likely to have normal coronary arteries or mild non-obstructive plaque disease. Use of percutaneous coronary intervention (PCI) varied with supervising consultant operator. These findings highlight disparity between clinical practice and NICE guideline recommendations for NSTEMI-ACS patients admitted to hospitals without invasive cardiac facilities, and highlight the need for the development of treatment pathways that reduce delay and better identify patients who will benefit from coronary revascularisation.

Introduction
Clinical guidelines recommend routine early inpatient invasive coronary angiography (ICA) in patients presenting with non-ST-elevation acute myocardial infarction acute coronary syndrome (NSTEMI-ACS) who are considered at higher risk of future recurrent myocardial infarction (MI) and death. National Institute for Health and Care Excellence (NICE) guidance recommends early ICA in high-risk patients within three days of admission,1 and the European Society of Cardiology (ESC) recommends this investigation is completed within 24 hours.2 Most UK patients presenting with NSTEMI-ACS are admitted to hospitals that do not have invasive cardiac catheterisation facilities and experience treatment delays resulting from bed pressure and the need for interhospital transfer.3 Completing transfer to a cardiac centre for ICA within three days may not be feasible for most patients in this setting.
Randomised trials comparing invasive versus conservative treatment in NSTEMI-ACS have utilised invasive angiography within 72 hours. An early invasive strategy reduces recurrent MI and readmission with refractory angina, but not cardiovascular or all-cause mortality.4–6 More recent clinical trials have focused on the delay to ICA. For example, the VERDICT (Early Versus Standard Care Invasive Examination and Treatment of Patients With Non-ST-Segment Elevation Acute Coronary Syndrome) randomised-controlled trial compared invasive angiography within 12 hours to standard invasive angiography within 48 to 72 hours.7 A strategy of very early invasive angiography did not improve clinical outcomes. However, there appeared to be improved clinical outcomes in the subgroup of high-risk patients with a GRACE (Global Registry of Acute Coronary Events) score >140. A meta-analysis of 17 randomised-controlled trials involving more than 10,000 patients found that the benefits of earlier ICA were limited to reducing recurrent ischaemia and length of stay.8
Readmission with chest pain and a diagnosis of recurrent MI are impactful to the patient, but, following changes to diagnostic thresholds in the last 20 years, and the use of high-sensitivity troponin assays in particular, these diagnoses may not be associated with the mortality implications that shape the prevailing view about the need for immediate inpatient ICA.9 Recurrent or repeat episodes of ischaemic chest pain predict further symptoms and MI. The longer patients remain symptom free, the lower the risk of recurrent problems. The ICTUS (Early Invasive versus Selectively Invasive Management for Acute Coronary Syndromes) trial found no difference in major adverse cardiovascular events (MACE) between early ICA and initial conservative (medication only) therapy in patients admitted to hospital with NSTEMI-ACS who settled and had no further chest pain.10 In addition to lacking proven clinical benefit, the treatment delay for ICA is a source of frustration for patients waiting in hospital, increases hotel costs and places pressure on bed occupancy within hospitals that are struggling to manage the flow of emergency cases through the front door.
Against this background, this retrospective cohort study analysed factors influencing delay to ICA, diagnosis and treatment allocation for patients presenting with NSTEMI-ACS admitted to five acute receiving hospitals in South East Scotland that refer patients to Edinburgh Heart Centre for invasive cardiac tests and treatment. These hospitals serve regional populations and are located up to 40 miles from Edinburgh Heart Centre. This hub-and-spoke model for referrals and interhospital patient transfers into a tertiary centre with centralised expertise and invasive cardiology facilities is established within the UK and throughout the world.3,4 This study offers insight into ‘real-world’ application of NSTEMI-ACS management guidelines, and highlights the potential disparity in care pathways for patients admitted to hospitals without on-site cardiac catheterisation facilities. Understanding these dynamics will help develop optimised care pathways that minimise unnecessary delays, reduce hospital-bed occupancy, and ensure timely and appropriate management for NSTEMI patients, regardless of their initial point of care.
Materials and method
Study design, setting, and population
This retrospective cohort study included all patients with clinically confirmed or suspected NSTEMI-ACS referred for inpatient angiography from five district general hospitals (DGH: Victoria Hospital, Kirkcaldy, Western General Hospital, Edinburgh, Borders General Hospital, Melrose, Forth Valley Royal Hospital, Larbert, and St. John’s Hospital, Livingston) to Edinburgh Heart Centre (EHC) for ICA. The study included patients referred during a five-year period from April 2019 to March 2024.
Data collection and outcomes
Patients were identified from a database maintained by the cardiac liaison team at EHC. Patient demographics, dates of referral from the DGH, admission to EHC, first ICA, and supervising consultant and treatment allocation were recorded from electronic records. The date of initial admission to the DGH was not available and a one-day delay between DGH admission and referral to EHC was assumed when calculating total delay from admission to ICA. This assumption aligns with audits investigating referral delays for UK patients with NSTEMI-ACS.11 Patient diagnosis and treatment allocations following ICA for NSTEMI-ACS were classified in five categories:
- normal coronary arteries
- mild plaque disease/patent grafts and/or stent (for patients with previous coronary revascularisation) – abbreviated to non-obstructive disease
- moderate-to-severe obstructive disease (vessel stenosis >50%) with no revascularisation – abbreviated to obstructive disease, medical
- revascularisation with percutaneous coronary intervention (PCI) – abbreviated to obstructive disease, PCI ± stent
- revascularisation with coronary artery bypass grafting (CABG) – abbreviated to obstructive disease, CABG.
Statistical analysis
Data were compiled using Microsoft Excel, and statistical analyses were performed using IBM SPSS Statistics version 29.12 Descriptive statistics summarised the demographics and referral patterns. Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were presented as frequencies and percentages. Differences in treatment outcomes following angiography across sex, age (≤55 vs. >55 years), and duration of delay (≤72 vs. >72 hours) were assessed using the Mann-Whitney U test.13 The Kruskal-Wallis test was employed to compare outcomes between different DGHs and treatment outcomes across the study years.14 Mean durations from referral to ICA were evaluated using one-way analysis of variance (ANOVA), with post-hoc Tukey’s test to assess the statistical significance of annual variations.15 Significance was defined as p<0.05 for all analyses.
Results
Patient characteristics
A total of 4,664 patient records were identified, of which 4,087 were included for analysis after excluding incomplete data and patients who did not receive ICA. The mean age was 65.1 ± 11.3 (range 28–94) years and 67% were male.
Time to ICA
The mean duration from DGH admission to ICA was 5.0 ± 3.0 days. The mean time per calendar year varied between 2019 and 2024. The shortest duration of 4.1 ± 3.0 days in 2020–2021 was recorded during the COVID-19 pandemic (p<0.05 post-hoc Tukey). Overall, 2,687 (66%) patients waited longer than the NICE-recommended 72 hours for their first procedure, and 4,034 (99%) waited longer than the ESC-recommended 24 hours. Delay to ICA varied according to the day of the week the referral was made. Over the five-year study period, patients referred in the second half of the week (Wednesday to Saturday) waited 0.6 ± 0.1 days longer (p<0.05, independent samples t-test).
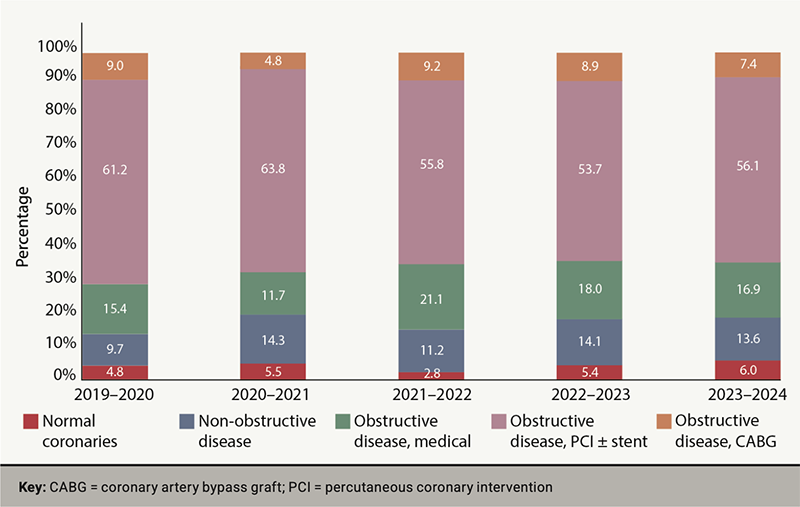
Diagnosis and treatment allocation following ICA
Figure 1 illustrates diagnosis and treatment allocation across the five years. There were variations in diagnosis and treatment outcomes in the years 2019–2020 versus 2022–2023, and 2023–2024 (p<0.05, Kruskal-Wallis test). In total, 66.1% received coronary revascularisation (follow-on PCI, staged PCI or referred for CABG). Patients not receiving coronary revascularisation had normal coronary arteries (4.9%), non-obstructive coronary artery disease (12.6%) or obstructive coronary disease for conservative management (16.4%). Patients receiving coronary revascularisation had PCI (58.3%) and CABG (7.8%).
Diagnosis and treatment allocation stratified by age, gender, duration of delay and supervising consultant operator
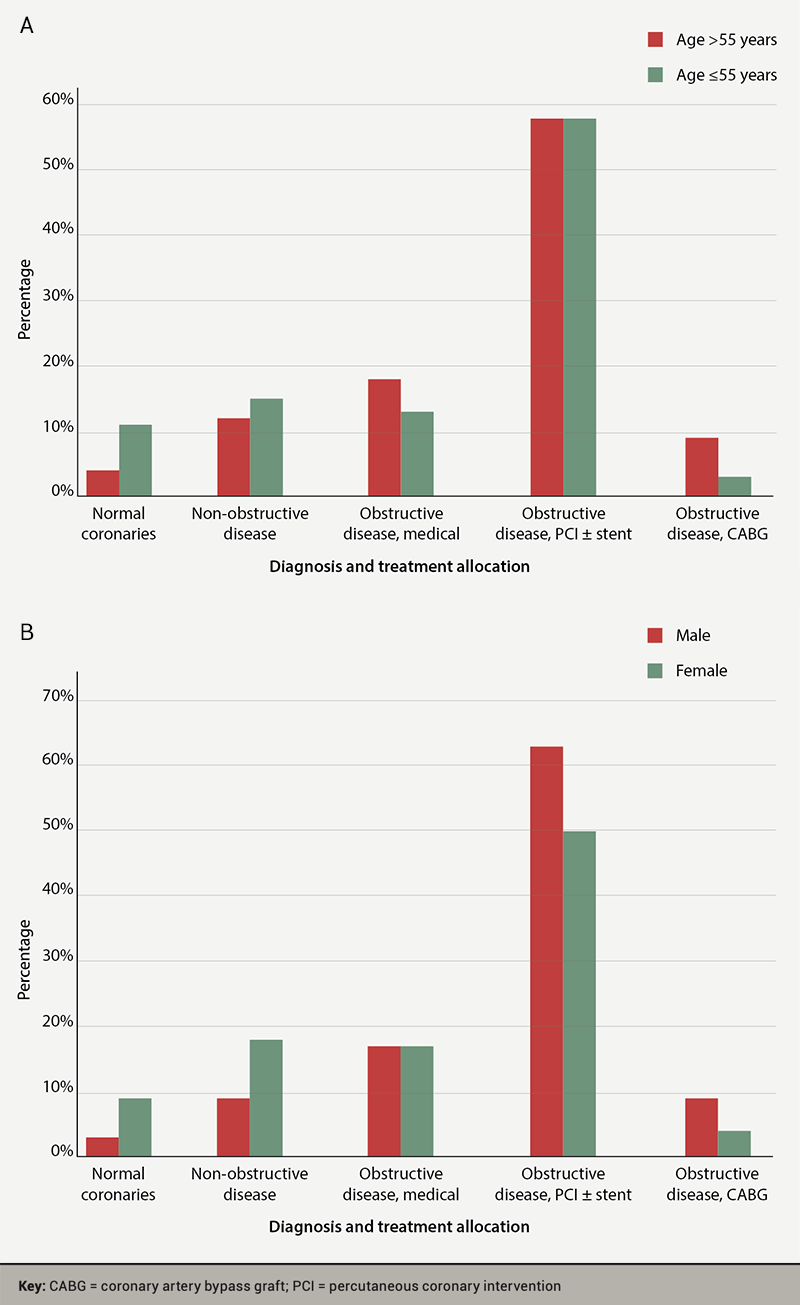
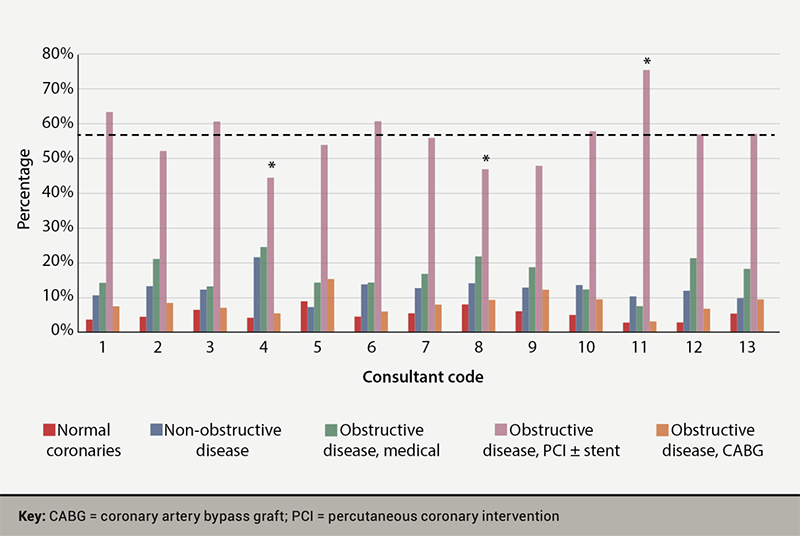
The prevalence of normal coronary arteries or non-obstructive plaque disease was higher in patients ≤55 compared with those >55 years (25.7% vs. 15.8%, p<0.05) (figure 2A), as well as female patients compared with male patients (28.9% vs. 12.1%, p<0.05) (figure 2B). Treatment allocation varied by consultant operator (figure 3). The mean rate of follow-on PCI was 56.7% (range 45–76%) among 13 supervising consultants. There was no variation in the distribution of diagnosis and treatment allocation between patients who received their ICA before or after 72 hours delay (p>0.05, Mann-Whitney U test).
Discussion
We recorded an average five-day delay from admission to ICA for 4,087 patients with NSTEMI-ACS referred to the South East Scotland regional cardiac centre between 2019 and 2024. The majority did not receive ICA within the NICE 72-hour guidance. This pattern of delay to treatment and disparity for patients admitted to acute hospitals without invasive facilities has been observed in other European countries.16 The clinical benefit of conducting ICA following a five-day inpatient wait is uncertain. This period of delay is longer than the delay to coronary angiography in randomised trials comparing invasive with conservative treatment in patients with NSTEMI-ACS, highlighting a major evidence gap underpinning a standard, resource-intensive healthcare pathway in the UK.
ICA is the gateway to coronary revascularisation with coronary angioplasty and stenting or planning for CABG surgery. This test also provides important information that may lead to a change in diagnosis. Our study found that 34% of patients receiving ICA did not receive coronary revascularisation, and 18% of these cases had normal or non-obstructed coronary arteries. As expected, younger patients and female patients were more likely to have normal or non-obstructive coronary plaque disease. Specifically, 26% of patients under 55 years and 29% of female patients had normal or non-obstructed coronary arteries. We found no association between delay to ICA (≥72 or <72 hours) and diagnosis or treatment allocation. This represents a large cohort of patients who may be suitable for non-invasive diagnostic imaging modalities, such as computed tomography (CT) coronary angiography, potentially avoiding the need for, and risks associated with, ICA.17
Furthermore, we found that treatment allocation at the time of angiography varied according to the consultant performing the coronary angiogram. The decision to proceed with ad-hoc PCI is made with the patient lying on the catheter laboratory table. We found conversion rates from diagnostic angiography to coronary intervention between 45% and 76% across 13 interventional cardiology consultants. This finding possibly indicates the impact of individual interpretation of clinical data and variation in interventional practice and expertise, and is in alignment with previous studies that have reported operator-dependent variations in NSTEMI-ACS treatment.18 Our data do not capture the additional clinical factors, including coronary anatomy and patient comorbidity, that influence decisions on coronary revascularisation, and this finding may be considered hypothesis generating.
Finally, treatment delay was longer for patients referred in the second half of the week, possibly reflecting the impact of weekend working, when there are no routine cardiac catheterisation lists.19 The weekend effect has been linked previously to worse clinical outcomes.20 This may not be evident in centres that run weekend angiography lists. Treatment delay was also reduced by one day during the COVID pandemic, when service provision and non-urgent elective work were disrupted.
Acute hospital wards are uncomfortable places for ambulant and well patients to stay. Noise and shared bays lead to sleep disruption.21 There is the potential for exposure to hospital-acquired infection, such as norovirus and COVID infection.22 Our daily experience looking after these patients records the frustration for the patient and clinical team surrounding delays and uncertainty regarding timing of transfer to EHC.
The strengths of this study include the large sample size and data completeness over five years, providing a picture of NSTEMI-ACS referral and treatment in a UK regional hub-and-spoke model. There are several important limitations. First, its observational retrospective design restricts the available variables, making the data insufficiently detailed to build informative models on factors influencing time-to-angiography or treatment allocation. We, therefore, report predominantly descriptive results. Second, the diagnosis of NSTEMI is based upon clinical records, and the final diagnosis at discharge was not available. There will be a subgroup of patients in whom the final diagnosis was not NSTEMI. Finally, clinical outcome data were not available.
Conclusion
This study outlines substantial disparities between clinical practice and NICE guideline recommendations for ICA in patients with NSTEMI-ACS. The 72-hour target was not delivered in the majority of patients. Our findings highlight variation in the presence of obstructive coronary disease and use of coronary revascularisation according to patient age, sex and supervising consultant operator. The clinical benefit of a strategy of delayed ICA in stable patients with NSTEMI-ACS is uncertain. Treatment delay is associated with negative patient experience and increased hospital costs. Taken together, these findings indicate a need for the development of clinical pathways that avoid unnecessary inpatient stay, reduce delays to diagnosis and treatment and better identify patients with NSTEMI-ACS who will benefit from ICA and coronary revascularisation.
Key messages
- This retrospective cohort study examined factors influencing delay to invasive coronary angiography, diagnosis and treatment allocation in 4,087 patients admitted to district general hospitals in South East Scotland with no invasive cardiac facilities with a non-ST-elevation acute myocardial infarction acute coronary syndrome (NSTEMI-ACS) diagnosis
- The mean delay from admission to invasive coronary angiography was five days. The majority (65.7% of patients) waited longer than the 72-hour National Institute for Health and Care Excellence (NICE) guidance. Coronary revascularisation was not required in 34% of patients and diagnosis and treatment allocation varied with age, sex and supervising consultant operator
- Delay to invasive coronary angiography for patients with NSTEMI-ACS is associated with doubtful clinical benefit and negative experience. These findings highlight the need to develop treatment pathways that reduce delay and better identify patients who will benefit from coronary revascularisation
Conflicts of interest
None declared.
Funding
None.
Study approval
Permission for this service review and audit was given by the hospital audit committee with no requirement to seek ethical approval.
References
1. National Institute for Health and Care Excellence. Acute coronary syndromes. NG185. London: NICE, 2020. Available from: https://www.nice.org.uk/guidance/ng185/chapter/Recommendations#nstemi-and-unstable-angina-early-management
2. Byrne RA, Rossello X, Coughlan JJ et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J 2023;44:3720–826. https://doi.org/10.1093/eurheartj/ehad191
3. Thein EKK, Blunt C, Saleem M. 70 Delays in invasive angiography in non-ST elevation ACS patients from district general hospital and action plans to reduce these delays. Heart 2023;109:A10. https://doi.org/10.1136/heartjnl-2023-BCS.70
4. O’Donoghue M, Boden WE, Braunwald E et al. Early invasive vs conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction. JAMA 2008;300:71. https://doi.org/10.1001/jama.300.1.71
5. Fox KA, Clayton TC, Damman P et al. Long-term outcome of a routine versus selective invasive strategy in patients with non-ST-segment elevation acute coronary syndrome: a meta-analysis of individual patient data. J Am Coll Cardiol 2010;55:2435–45. https://doi.org/10.1016/j.jacc.2010.03.007
6. Fanning JP, Nyong J, Scott IA, Aroney CN, Walters DL. Routine invasive strategies versus selective invasive strategies for unstable angina and non-ST elevation myocardial infarction in the stent era. Cochrane Database Syst Rev 2016;2016:CD004815. https://doi.org/10.1002/14651858.CD004815.pub4
7. Kofoed KF, Kelbaek H, Hansen PR et al. Early versus standard care invasive examination and treatment of patients with non-ST-segment elevation acute coronary syndrome. Circulation 2018;138:2741–50. https://doi.org/10.1161/CIRCULATIONAHA.118.037152
8. Kite TA, Danchin N, Keeley EC et al. Timing of invasive strategy in non-ST-elevation acute coronary syndrome: a meta-analysis of randomized controlled trials. Eur Heart J 2022;43:3148–61. https://doi.org/10.1093/eurheartj/ehac213
9. O’Fee K, Deych E, Ciani O, Brown DL. Assessment of nonfatal myocardial infarction as a surrogate for all-cause and cardiovascular mortality in treatment or prevention of coronary artery disease. JAMA Intern Med 2021;181:1575–87. https://doi.org/10.1001/jamainternmed.2021.5726
10. de Winter RJ, Windhausen F, Cornel JH et al. Early invasive versus selectively invasive management for acute coronary syndromes. N Engl J Med 2005;353:1095–104. https://doi.org/10.1056/NEJMoa044259
11. Society of Cardiovascular Intervention, National Institute for Cardiovascular Outcomes Research (NICOR). National Audit of Percutaneous Coronary Interventions (NAPCI): 2020 summary report (2018/19 data). London: Healthcare Quality Improvement Partnership, 2020. Available from: https://www.nicor.org.uk/national-cardiac-audit-programme/previous-reports/pci-1/2020-3
12. IBM Corp. IBM SPSS Statistics for Windows, version 29.0. Armonk, NY: IBM Corp, 2022.
13. McKnight PE, Najab J. Mann-Whitney U test. In: Weiner IB, Craighead WE, eds. The Corsini Encyclopedia of Psychology. Hoboken, NJ: John Wiley & Sons, 2010. https://doi.org/10.1002/9780470479216.corpsy0524
14. Kruskal WH, Wallis WA. Use of ranks in one-criterion variance analysis. J Am Stat Assoc 1952;47:583–621. https://doi.org/10.1080/01621459.1952.10483441
15. Kaufmann J, Schering A. Analysis of variance ANOVA. In: Balakrishnan N, Colton T, Everitt B, Piegorsch W, Ruggeri F, Teugels JL, eds. Wiley StatsRef: Statistics Reference Online, 2014. https://doi.org/10.1002/9781118445112.stat06938
16. van Steenbergen GJ, Demandt JPA, Schulz DN et al. Direct admission versus interhospital transfer for revascularisation in non-ST-segment elevation myocardial infarction. Clin Cardiol 2023;46:997–1006. https://doi.org/10.1002/clc.24060
17. Maurovich-Horvat P, Bosserdt M, Kofoed KF et al. CT or invasive coronary angiography in stable chest pain. N Engl J Med 2022;386:1591–602. https://doi.org/10.1056/NEJMoa2200963
18. Naranjo D, Doll J, Maynard C, Beaver K, Bansal A, Helfrich CD. Practice pattern variation in adoption of new and evolving percutaneous coronary intervention procedures. J Interv Cardiol 2023;2023:2488045. https://doi.org/10.1155/2023/2488045
19. Kwok CS, Al-Dokheal M, Aldaham S et al. Weekend effect in acute coronary syndrome: a meta-analysis of observational studies. Eur Heart J Acute Cardiovasc Care 2018;8:432–42. https://doi.org/10.1177/2048872618762634
20. Kostis WJ, Demissie K, Marcella SW, Shao YH, Wilson AC, Moreyra AE. Weekend versus weekday admission and mortality from myocardial infarction. N Engl J Med 2007;356:1099–109. https://doi.org/10.1056/NEJMoa063355
21. Pilkington S. Causes and consequences of sleep deprivation in hospitalised patients. Nurs Stand 2013;27:35–42. https://doi.org/10.7748/ns2013.08.27.49.35.e7649
22. Manoukian S, Stewart S, Graves N et al. Bed-days and costs associated with the inpatient burden of healthcare-associated infection in the UK. J Hosp Infect 2021;114:43–50. https://doi.org/10.1016/j.jhin.2020.12.027
